Embed Size (px)
Citation preview
Clinically Significant Gastrointestinal Bleedingin Critically Ill Patients in an Era of ProphylaxisMark Pimentel, M.D., Daniel E. Roberts, M.D., Charles N. Bernstein, M.D., Michael Hoppensack, B.Sc., andDonald R. Duerksen, M.D.Department of Medicine, University of Manitoba, Winnipeg, Manitoba, Canada
OBJECTIVE: Clinical studies examining stress-related gastro-intestinal bleeding in critically ill patients vary in theirclinical definitions and assessment of clinical significance.Although there is evidence that routine prophylaxis de-creases stress-related gastrointestinal bleeding, recent stud-ies indicate a decreasing incidence, independent of the useof prophylactic medications. The purpose of this study wasto determine the incidence of and risk factors for clinicallysignificant, endoscopically proven gastrointestinal bleedingin critically ill patients.
METHODS: A database (prospectively collected data) of8338 patients admitted to the surgical and medical intensivecare units at major tertiary care center from July 1988 toApril 1995 was examined. All patients with significantupper gastrointestinal bleeding as defined by a drop inhemoglobin of.20 g/L and endoscopic evidence of anupper GI tract source were identified. Risk factors for GIbleeding from stress ulceration were compared in bleedingand nonbleeding patients. A case-control study analyzingrisk factors for bleeding in the abdominal aortic aneurysmsubgroup was performed.
RESULTS: After exclusion criteria, 12/7231 (0.17%) patientshad clinically significant, endoscopically proven bleeding.Significant risk factors included age, septic shock, abdom-inal aortic aneurysm repair, and nutritional support. Inten-sive care unit stay was prolonged in patients with stress-related bleeding. There was no difference in incidence ofhypotension, clamp time, APACHE score, or operatingroom time in patients with abdominal aortic aneurysm repairas compared with controls.
CONCLUSIONS: In an intensive care unit where stress pro-phylaxis is widely used, clinically important gastrointestinalbleeding is uncommon. Further study is needed to define theoptimal prophylaxis regimen and the role for its selectiveuse in high-risk patients. (Am J Gastroenterol 2000;95:2801–2806. © 2000 by Am. Coll. of Gastroenterology)
INTRODUCTION
Stress ulceration in critically ill patients may result in clin-ically significant gastrointestinal bleeding associated withan increased intensive care unit mortality (1, 2). Specific
factors that place critically ill patients at increased risk forgastrointestinal bleeding include sepsis, burns, coagulopa-thy, mechanical ventilation, and neurological events (3–8).Because of the increased morbidity and mortality associatedwith stress ulceration, clinical trials have been performedthat have demonstrated the benefit of various forms ofpharmacological prophylaxis, including histamine-2 recep-tor antagonists (H2RAs), sucralfate, and antacids. The re-sults of these studies have been summarized in a meta-analysis (9).
More recent literature suggests that the risk for clinicallysignificant gastrointestinal bleeding is decreasing—an effectthat is independent of gastrointestinal prophylaxis (10).Prophylaxis for all critically ill patients may not be cost-effective (8), and it has been suggested that prophylaxisshould be used only in patients with factors that convey highrisk.
There is great variation in the definition of gastrointesti-nal bleeding in studies examining the incidence and riskfactors for gastrointestinal bleeding. Criteria for significantgastrointestinal bleeding such as hemodynamic instabilityand a drop in hemoglobin have not been consistent. Some ofthe studies examining the incidence and demographics ofstress ulceration in critically ill patients have based thediagnosis on heme-positive nasogastric aspirates (3, 4),which are insensitive and not specific for stress-relatedbleeding (11). Other studies have used only endoscopiccriteria and have not considered clinically significant end-points (5, 7). Finally, when clinically significant endpointshave been used, these have not been correlated with endo-scopic confirmation of stress ulceration (1, 2, 6, 8).
Since 1988, the intensive care unit (ICU) at the HealthScience Centre in Winnipeg has prospectively entered allpatients into a database. Based on clinical studies of phar-macological prophylaxis, it has been the practice of this unitto administer prophylaxis with H2RAs or sucralfate to pa-tients who remain in the ICU.24 h. The objective of thisstudy was to examine, in patients receiving stress prophy-laxis, the incidence and demographics of endoscopicallyproven, clinically significant stress-induced bleeding in crit-ically ill patients. In addition, risk factors for developingsignificant bleeding were examined.
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 95, No. 10, 2000© 2000 by Am. Coll. of Gastroenterology ISSN 0002-9270/00/$20.00Published by Elsevier Science Inc. PII S0002-9270(00)01982-1

MATERIALS AND METHODS
Critically ill patients admitted to the medical and surgicalintensive care units at the Health Sciences Centre, Univer-sity of Manitoba since July 1, 1988, have been prospectivelyenrolled into a computer database. This database was de-signed to accumulate demographics, information on phar-maceutical use, admitting and acquired diagnoses, a thera-peutic intervention scoring system (TISS), and variousoutcome and severity of illness measures during the first 5days of the ICU stay. In addition, TISS scoring was done ona daily basis during the complete stay in the ICU. The detailsof the database have previously been described (12, 13).
Since 1988, when the data collection first started, it hasbeen the philosophy of the ICU to provide stress ulcerationprophylaxis for any patient anticipated to be admitted to theICU for a period.24–48 h. If patients were anticipated tohave a short duration of stay, stress prophylaxis was notgiven. The decision regarding the type of pharmacologicalprophylaxis has been left to the individual attending physician.
Using this database, an analysis of patients admitted toeither of the critical care units (surgical or medical) wasperformed to assess the incidence of clinically significantbleeding as well as risk factors important in the developmentof stress ulceration. The database was examined from July1988 to April 1995. All patients admitted during this timewere considered for entry into the study. Patients wereexcluded if they were admitted with any of the problemsoutlined in Table 1. Exclusion criteria were applied to elim-
inate any patients who might have significant gastrointesti-nal bleeding from a source other than stress ulceration.These include recent GI surgery, potential blood loss distalto the duodenum, admission with an upper GI bleed, andbleeding related to portal hypertension. Information onwhether patients had an endoscopic procedure performedduring their ICU admission was included in the TISS score.Using the search mode of the database program, the recordsof all patients with a gastroscopy during the first 5 days inthe ICU were obtained. A manual search of all TISS sheetson patients with an ICU stay.5 days was performed toidentify patients who had gastroscopies performed.
All patients who had a gastroscopy performed.24 h afteradmission to the ICU were considered. To be included in thestudy, a bleeding site needed to be identified on gastroscopywith either one or both of the following: a drop in hemo-globin.20 g/L, or a drop in systolic blood pressure of.20mm Hg (or 10 mm Hg diastolic). These criteria were appliedto select only those patients who had documented clinicallysignificant gastrointestinal bleeding. Similar criteria forclin-ically significant bleeding have been previously defined (8).
The patients who met the criteria for clinically significantgastrointestinal bleeding were assessed for a number ofvariables. These variables included demographic factorssuch as age and sex, an acuity index score (APACHE II) onpresentation to the ICU (14), admitting and discharge diag-noses, the type and duration of stress ulceration prophylaxisused, the presence of tube feeding (enteral nutrition), thelength of stay in the ICU, mortality, the change in hemo-globin (the number of units of blood required), the presenceof a coagulopathy (as determined by a platelet count,100,000/ml or elevated prothrombin and partial thrombo-plastin times) and the findings at endoscopy.
Using the criteria defined above, a small number of casesof clinically significant bleeding were identified. To deter-mine whether any cases of significant bleeding may havebeen missed, the database was validated using the endos-copy database at the Health Science Centre. This databasedocuments all gastrointestinal endoscopies performed in thehospital and has been validated in other clinical studies (15).The records from the last 2 yr of the study period wereexamined and no additional patients who met the studycriteria using this log were identified. Based on this analysis,it was assumed that the database was accurate in identifyingcritically ill patients with significant gastrointestinal bleeding.
Case-Control Study for Aortic Aneurysm PatientsBecause of the over-representation of postoperative abdom-inal aortic aneurysms in the group of patients with con-firmed stress ulceration, a case-control study of these pa-tients was performed. Two patients admitted to the ICUafter abdominal aortic aneurysm surgery without stress ul-ceration were chosen for every abdominal aortic aneurysmpatient who met the criteria for clinically significant gastro-intestinal bleeding and were matched for age, sex, APACHEII score, and date of surgery (within 3 months of the case).
Table 1. Exclusion Criteria
Upper gastrointestinal bleedingEsophageal variceal bleedingIschemic bowelBowel obstructionToxic megacolonParalytic ileusAppendicitisBowel perforation, nontraumaticCaustic injury, esophagusMesenteric infarct/thrombosisHernia, incarceratedAcetylsalicylic acid poisoningAnoxic encephalopathy, poor prognosisBrain deathNeck/thoracic injuriesMalignancy of esophagus, stomach, colonHIV infectionBone marrow transplantPost chemotherapyDeath in,24 hOrgan donorAbdominal traumaFacial fracturesEsophagectomyTracheoesophageal fistula resectionGastrectomyPyloroplastyWhipple’s procedureOversew of gastric or duodenal ulcer
2802 Pimentel et al. AJG – Vol. 95, No. 10, 2000
The records of these patients were also examined forfactors that might be important in conferring an additionalrisk for significant gastrointestinal bleeding. Specifically,the patients were assessed for aortic clamp times, the loca-tion of the clamp, the duration and severity of hypotensionduring surgery, the need for inotropic support, and thenumber of inotropic agents required. The number of units ofblood required and the use of anticoagulant during surgerywere also assessed. Finally, the length of the surgery and thepresence of a ruptured aorta at surgery were noted.
Statistical AnalysisAll results are expressed as mean6 standard deviation.Qualitative variables were compared by using ax2 test forsets of data with absolute numbers in.20. Fisher’s exacttest was used to compare qualitative variables in whichsmall numbers were involved in each group being com-pared. Continuous variables were compared using a two-tailed t test. Statistical significance was established at apvalue of ,0.05. For variables in Table 2, a Bonferroniadjustment was applied. When statistically analyzing thepaired data obtained in the comparison of abdominal aorticaneurysms that bled compared to those that did not, quali-tative data was analyzed using McNemar’s test. Quantitativedata was compared in these two groups using a pairedt test.
RESULTS
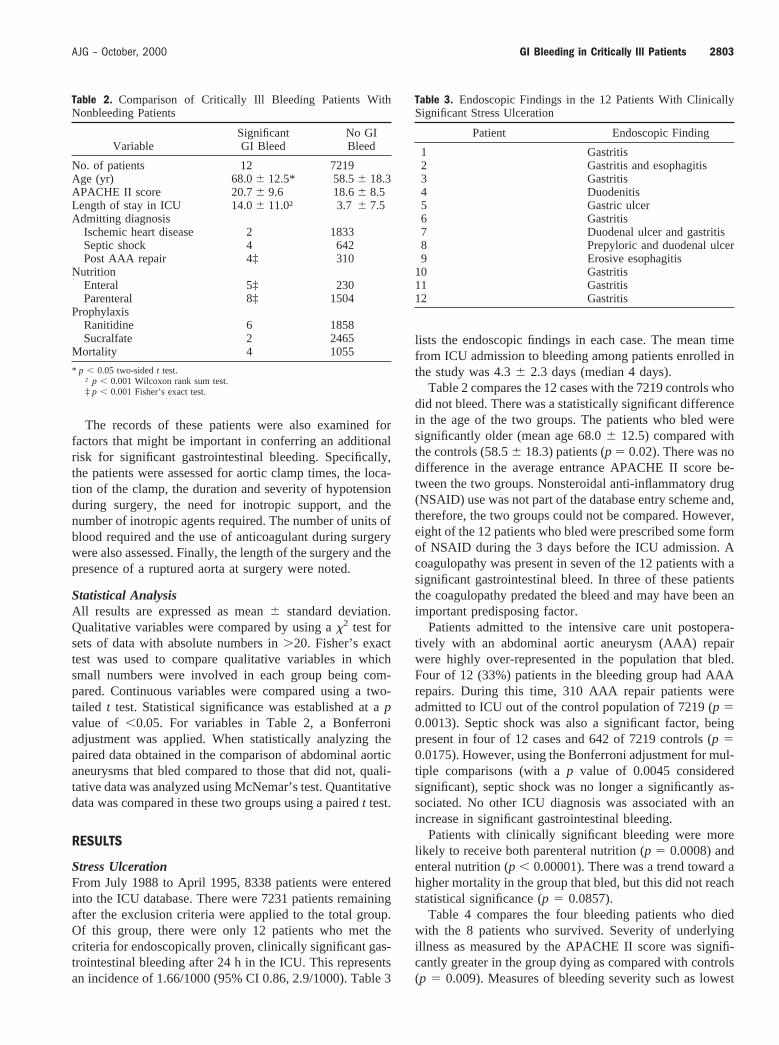
Stress UlcerationFrom July 1988 to April 1995, 8338 patients were enteredinto the ICU database. There were 7231 patients remainingafter the exclusion criteria were applied to the total group.Of this group, there were only 12 patients who met thecriteria for endoscopically proven, clinically significant gas-trointestinal bleeding after 24 h in the ICU. This representsan incidence of 1.66/1000 (95% CI 0.86, 2.9/1000). Table 3
lists the endoscopic findings in each case. The mean timefrom ICU admission to bleeding among patients enrolled inthe study was 4.36 2.3 days (median 4 days).
Table 2 compares the 12 cases with the 7219 controls whodid not bleed. There was a statistically significant differencein the age of the two groups. The patients who bled weresignificantly older (mean age 68.06 12.5) compared withthe controls (58.56 18.3) patients (p 5 0.02). There was nodifference in the average entrance APACHE II score be-tween the two groups. Nonsteroidal anti-inflammatory drug(NSAID) use was not part of the database entry scheme and,therefore, the two groups could not be compared. However,eight of the 12 patients who bled were prescribed some formof NSAID during the 3 days before the ICU admission. Acoagulopathy was present in seven of the 12 patients with asignificant gastrointestinal bleed. In three of these patientsthe coagulopathy predated the bleed and may have been animportant predisposing factor.
Patients admitted to the intensive care unit postopera-tively with an abdominal aortic aneurysm (AAA) repairwere highly over-represented in the population that bled.Four of 12 (33%) patients in the bleeding group had AAArepairs. During this time, 310 AAA repair patients wereadmitted to ICU out of the control population of 7219 (p 50.0013). Septic shock was also a significant factor, beingpresent in four of 12 cases and 642 of 7219 controls (p 50.0175). However, using the Bonferroni adjustment for mul-tiple comparisons (with ap value of 0.0045 consideredsignificant), septic shock was no longer a significantly as-sociated. No other ICU diagnosis was associated with anincrease in significant gastrointestinal bleeding.
Patients with clinically significant bleeding were morelikely to receive both parenteral nutrition (p 5 0.0008) andenteral nutrition (p , 0.00001). There was a trend toward ahigher mortality in the group that bled, but this did not reachstatistical significance (p 5 0.0857).
Table 4 compares the four bleeding patients who diedwith the 8 patients who survived. Severity of underlyingillness as measured by the APACHE II score was signifi-cantly greater in the group dying as compared with controls(p 5 0.009). Measures of bleeding severity such as lowest
Table 2. Comparison of Critically Ill Bleeding Patients WithNonbleeding Patients
VariableSignificantGI Bleed
No GIBleed
No. of patients 12 7219Age (yr) 68.06 12.5* 58.56 18.3APACHE II score 20.76 9.6 18.66 8.5Length of stay in ICU 14.06 11.0† 3.76 7.5Admitting diagnosis
Ischemic heart disease 2 1833Septic shock 4 642Post AAA repair 4‡ 310
NutritionEnteral 5‡ 230Parenteral 8‡ 1504
ProphylaxisRanitidine 6 1858Sucralfate 2 2465
Mortality 4 1055
* p , 0.05 two-sidedt test.† p , 0.001 Wilcoxon rank sum test.‡ p , 0.001 Fisher’s exact test.
Table 3. Endoscopic Findings in the 12 Patients With ClinicallySignificant Stress Ulceration
Patient Endoscopic Finding
1 Gastritis2 Gastritis and esophagitis3 Gastritis4 Duodenitis5 Gastric ulcer6 Gastritis7 Duodenal ulcer and gastritis8 Prepyloric and duodenal ulcer9 Erosive esophagitis
10 Gastritis11 Gastritis12 Gastritis
2803AJG – October, 2000 GI Bleeding in Critically Ill Patients
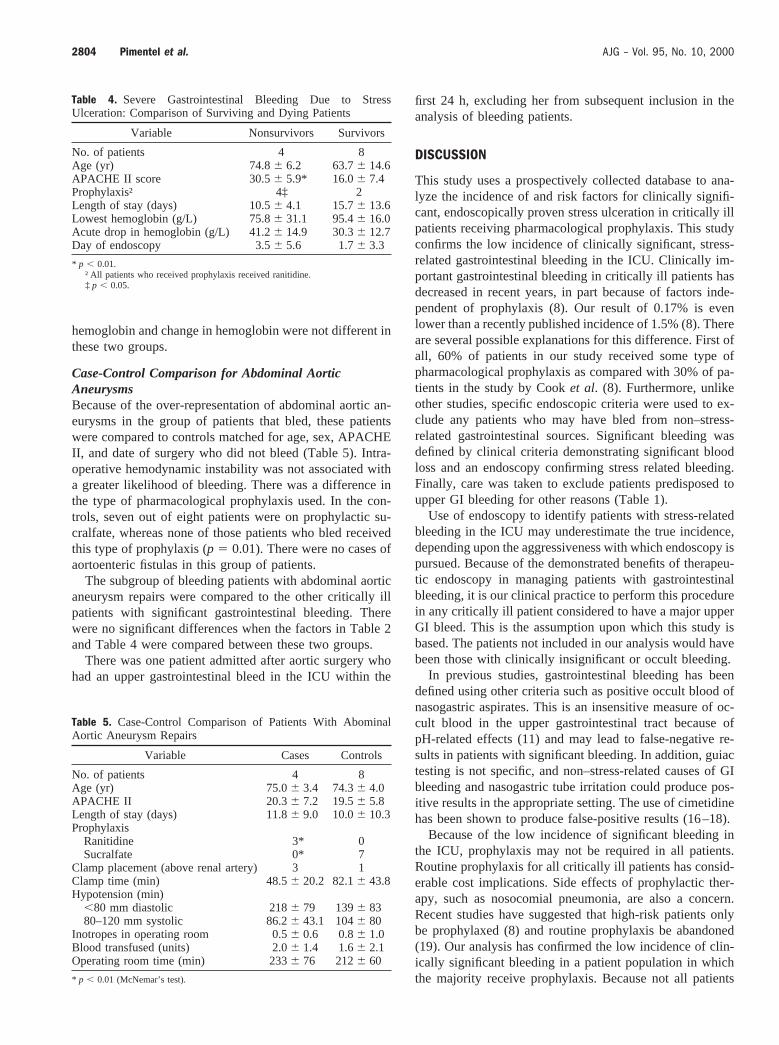
hemoglobin and change in hemoglobin were not different inthese two groups.
Case-Control Comparison for Abdominal AorticAneurysmsBecause of the over-representation of abdominal aortic an-eurysms in the group of patients that bled, these patientswere compared to controls matched for age, sex, APACHEII, and date of surgery who did not bleed (Table 5). Intra-operative hemodynamic instability was not associated witha greater likelihood of bleeding. There was a difference inthe type of pharmacological prophylaxis used. In the con-trols, seven out of eight patients were on prophylactic su-cralfate, whereas none of those patients who bled receivedthis type of prophylaxis (p 5 0.01). There were no cases ofaortoenteric fistulas in this group of patients.
The subgroup of bleeding patients with abdominal aorticaneurysm repairs were compared to the other critically illpatients with significant gastrointestinal bleeding. Therewere no significant differences when the factors in Table 2and Table 4 were compared between these two groups.
There was one patient admitted after aortic surgery whohad an upper gastrointestinal bleed in the ICU within the
first 24 h, excluding her from subsequent inclusion in theanalysis of bleeding patients.
DISCUSSION
This study uses a prospectively collected database to ana-lyze the incidence of and risk factors for clinically signifi-cant, endoscopically proven stress ulceration in critically illpatients receiving pharmacological prophylaxis. This studyconfirms the low incidence of clinically significant, stress-related gastrointestinal bleeding in the ICU. Clinically im-portant gastrointestinal bleeding in critically ill patients hasdecreased in recent years, in part because of factors inde-pendent of prophylaxis (8). Our result of 0.17% is evenlower than a recently published incidence of 1.5% (8). Thereare several possible explanations for this difference. First ofall, 60% of patients in our study received some type ofpharmacological prophylaxis as compared with 30% of pa-tients in the study by Cooket al. (8). Furthermore, unlikeother studies, specific endoscopic criteria were used to ex-clude any patients who may have bled from non–stress-related gastrointestinal sources. Significant bleeding wasdefined by clinical criteria demonstrating significant bloodloss and an endoscopy confirming stress related bleeding.Finally, care was taken to exclude patients predisposed toupper GI bleeding for other reasons (Table 1).
Use of endoscopy to identify patients with stress-relatedbleeding in the ICU may underestimate the true incidence,depending upon the aggressiveness with which endoscopy ispursued. Because of the demonstrated benefits of therapeu-tic endoscopy in managing patients with gastrointestinalbleeding, it is our clinical practice to perform this procedurein any critically ill patient considered to have a major upperGI bleed. This is the assumption upon which this study isbased. The patients not included in our analysis would havebeen those with clinically insignificant or occult bleeding.
In previous studies, gastrointestinal bleeding has beendefined using other criteria such as positive occult blood ofnasogastric aspirates. This is an insensitive measure of oc-cult blood in the upper gastrointestinal tract because ofpH-related effects (11) and may lead to false-negative re-sults in patients with significant bleeding. In addition, guiactesting is not specific, and non–stress-related causes of GIbleeding and nasogastric tube irritation could produce pos-itive results in the appropriate setting. The use of cimetidinehas been shown to produce false-positive results (16–18).
Because of the low incidence of significant bleeding inthe ICU, prophylaxis may not be required in all patients.Routine prophylaxis for all critically ill patients has consid-erable cost implications. Side effects of prophylactic ther-apy, such as nosocomial pneumonia, are also a concern.Recent studies have suggested that high-risk patients onlybe prophylaxed (8) and routine prophylaxis be abandoned(19). Our analysis has confirmed the low incidence of clin-ically significant bleeding in a patient population in whichthe majority receive prophylaxis. Because not all patients
Table 4. Severe Gastrointestinal Bleeding Due to StressUlceration: Comparison of Surviving and Dying Patients
Variable Nonsurvivors Survivors
No. of patients 4 8Age (yr) 74.86 6.2 63.76 14.6APACHE II score 30.56 5.9* 16.06 7.4Prophylaxis† 4‡ 2Length of stay (days) 10.56 4.1 15.76 13.6Lowest hemoglobin (g/L) 75.86 31.1 95.46 16.0Acute drop in hemoglobin (g/L) 41.26 14.9 30.36 12.7Day of endoscopy 3.56 5.6 1.76 3.3
* p , 0.01.† All patients who received prophylaxis received ranitidine.‡ p , 0.05.
Table 5. Case-Control Comparison of Patients With AbominalAortic Aneurysm Repairs
Variable Cases Controls
No. of patients 4 8Age (yr) 75.06 3.4 74.36 4.0APACHE II 20.36 7.2 19.56 5.8Length of stay (days) 11.86 9.0 10.06 10.3Prophylaxis
Ranitidine 3* 0Sucralfate 0* 7
Clamp placement (above renal artery) 3 1Clamp time (min) 48.56 20.2 82.16 43.8Hypotension (min)
,80 mm diastolic 2186 79 1396 8380–120 mm systolic 86.26 43.1 1046 80
Inotropes in operating room 0.56 0.6 0.86 1.0Blood transfused (units) 2.06 1.4 1.66 2.1Operating room time (min) 2336 76 2126 60
* p , 0.01 (McNemar’s test).
2804 Pimentel et al. AJG – Vol. 95, No. 10, 2000

received pharmacological prophylaxis, the true failure rateof prophylactic therapy cannot be determined from our study.
A second objective of this study was to determine possi-ble risk factors for gastrointestinal bleeding in critically illpatients. This study found age and septic shock as signifi-cant risk factors for the development of gastrointestinalbleeding. APACHE II score, as a measure of acuity ofillness, did not predict bleeding. This is consistent withprevious studies (8). Bleeding patients who died tended tohave a higher APACHE II score than bleeding patients whosurvived. The APACHE II score is known to be a predictorof mortality. Bleeding patients had a high incidence ofcoagulopathy and NSAID use. The database could not de-termine the use of NSAIDs in all patients and, therefore, thiscould be a confounding variable affecting the incidence ofbleeding. Similarly, it was not possible to examine forcoagulopathy in all patients. A systemic coagulopathy hasbeen associated with an increased risk for stress-relatedbleeding (8). However, in four of the seven patients who hadabnormal coagulation parameters, the coagulation profilewas normal on the day immediately preceding the bleedingevent, suggesting that consumption may have played a rolein the laboratory abnormality.
This study also found a significant increase in GI bleedingin postoperative abdominal aortic aneurysm repair patients.There are several possible explanations for this. There isevidence that patients undergoing aortic surgery have anincreased incidence of peptic ulcer disease (20, 21). Inpreoperative assessments of 106 patients undergoing AAAsurgery, Chenget al. found that 38 patients had evidence ofpeptic ulcer disease (20). They also found a rate of bleedingthat was higher in those with a pre-existing peptic ulcer (20).Other studies have confirmed this (21). There also is a highprevalence of endoscopic stress ulceration in this group ofpatients. Martin (22) demonstrated an 80% incidence ofstress ulceration in 42 postoperative patients undergoingaortic surgery. There is a high mortality among patients withthis complication after aortic surgery (23). Therefore, thesestudies suggest that this group of patients has an increasedincidence of underlying peptic ulcer disease and is also morelikely to develop postoperative stress ulceration. The reasonfor the latter is unclear, but underlying diffuse small vesselatherosclerosis may predispose to mucosal ischemia. Therelationship ofHelicobacter pylorito the development ofulceration in these patients is unknown. Given the associa-tion of Helicobacter pyloriwith peptic ulceration (24), itmay be reasonable to consider exploringH. pylori status inpatients before aortic surgery.
When AAA patients who had significant bleeding werecompared with matched controls, there were no significantintraoperative factors that predicted bleeding. The groupsdid differ, however, with respect to the type of prophylaxisused. Previous studies have demonstrated that sucralfate isas effective as histamine receptor antagonists (9, 25–29)when studied in large heterogeneous populations of criti-cally ill patients and may confer the additional benefit of a
lower incidence of nosocomial pneumonias (27). The num-bers included in our study are small, but demonstrate thatsucralfate may be a more effective prophylactic agent thanH2RAs in this high-risk subgroup. A larger group will needto be studied to determine the optimal prophylaxis in thishigh-risk subgroup of patients, as the selection of prophy-lactic agents in this study was nonrandomized.
The association of enteral nutrition with the developmentof stress-related bleeding was unexpected. A retrospectivestudy by Pingleton and Hadzima (30) suggested that enteralnutrition protects against gastrointestinal bleeding. Al-though the etiology of stress ulceration is likely multifac-torial, gastric acid is an important factor (31). Enteral nu-trition could potentially decrease stress ulceration by raisingintragastric pH. Recent studies in critically ill patients, how-ever, have demonstrated that enteral feeding does not havea significant effect on increasing gastric pH (32, 33) and,therefore, may be ineffective in affording gastroprotection.In our analysis, the use of enteral nutrition may have se-lected a more malnourished population predisposed tostress-related bleeding on the basis of underlying malnutri-tion. The association of TPN with stress-related bleeding inour study could be explained with similar reasoning. Theassociation of malnutrition with stress-related gastrointesti-nal bleeding in critically ill patients has not been studiedprospectively or retrospectively. A criticism of our dataregarding nutritional supplementation is that it was notadministered in either a randomized or controlled fashion.Thus, it may be patient factors that dictated the nutritionalsupplementation that placed the patients at increased risk,rather than the nutrition itself. The effects of nutrition onICU-related bleeding needs to be studied prospectively.
In conclusion, we have shown that the incidence of clin-ically significant, endoscopically proven stress ulceration inthe ICU is very low in the setting of current prophylaxisprotocols. Risk factors for bleeding include age, sepsis, andadmission after aortic surgery for AAA repair. Stress-relatedbleeding is associated with an increased mortality, particu-larly in association with high APACHE scores. The mosteffective prophylactic protocol is unknown, but bolus intra-venous H2RAs are not optimal in a subgroup of patientswith AAA repair. Further study is needed to define theoptimal prophylaxis regimen and the role for its selectiveuse in high-risk patients.
Reprint requests and correspondence:Donald R. Duerksen,M.D., Department of Medicine, Division of Gastroenterology,C5120 409 Tache Avenue, St. Boniface Hospital, Winnipeg, Mani-toba, Canada R2H 2A6.
Received May 14, 1998; accepted May 3, 2000.
REFERENCES
1. Brown RB, Janelle K, Teres D, et al. Prospective study ofclinical bleeding in intensive care unit patients. Crit Care Med1988;16:1171–6.
2805AJG – October, 2000 GI Bleeding in Critically Ill Patients
2. Martin LF, Booth FVM, Reines D, et al. Stress ulcers andorgan failure in incubated patients in surgical intensive careunits. Ann Surg 1991;215:332–7.
3. Harris SK, Bone RC, Ruth WE. Gastrointestinal hemorrhagein patients in a respiratory care unit. Chest 1977;72:301–4.
4. Hastings PR, Skillman JJ, Bushnell LS, et al. Antacid titrationin the prevention of acute gastrointestinal bleeding. N EnglJ Med 1978;298:1041–5.
5. Czaja AJ, McAlhanny JC, Pruitt BA. Acute gastroduodenaldisease after thermal injury. N Engl J Med 1974;291:925–9.
6. Schuster DP, Rowley H, Feinstein S, et al. Prospective eval-uation of the risk of upper gastrointestinal bleeding afteradmission to a medical intensive care unit. Am J Med 1984;76:623–30.
7. Brown TH, Davidson PF, Larson GM. Acute gastritis occur-ring within 24 hours of severe head injury. Gastrointest En-dosc 1989;35:37–40.
8. Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors forgastrointestinal bleeding in critically ill patients. N Engl J Med1994;330:377–81.
9. Cook DJ, Witt LG, Cook RJ, et al. Stress ulcer prophylaxis inthe critically ill: A meta-analysis. Am J Med 1991;91:519–27.
10. Cook DJ, Pearl RG, Cook RJ, et al. The incidence of clinicallyimportant bleeding in ventilated patients. J Intensive Care Med1991;6:167–74.
11. Layne EA, Mellow MH, Lipman TO. Insensitivity of guaiacslide tests for detection of blood in gastric juice. Ann InternMed 1981;94:774–6.
12. Roberts D, Ostryzniuk P, Loewen E, et al. Control of blood gasmeasurements in intensive-care units. Lancet 1991;337:1580–2.
13. Roberts DE, Bell DD, Ostryzniuk T, et al. Eliminating need-less testing in intensive care—An information-based teammanagement approach. Crit Care Med 1993;21:1452–8.
14. Knaus WA, Draper EA, Wagner DP, et al. APACHE II: Aseverity of disease classification system. Crit Care Med 1985;13:818–28.
15. Patel Y, Pettigrew NM, Grahame GR, et al. The diagnosticyield of lower endoscopy plus biopsy in nonbloody diarrhea.Gastrointest Endosc 1997;46:338–43.
16. Norfleet RG, Rhodes RA, Saviage K. False positive “hemoc-cult” reaction with cimetidine. N Engl J Med 1980;302:467.
17. Schentag JJ. False positive “hemoccult reaction” with cimeti-dine. N Engl J Med 1980;303:110.
18. Hauser A, Quigley ML, Driever CW, et al. More on false
positive “hemoccult” reaction with cimetidine. N Engl J Med1981;304:847–8.
19. Eddleston JM, Pearson RC, Holland J, et al. Prospective en-doscopic study of stress erosions and ulcers in critically illadult patients treated with either sulcrate or placebo. Crit CareMed 1994;22:1949–54.
20. Cheng SWK, Fok M, Wong J. Peptic ulcers and abdominalaortic aneurysms. J Gastroenterol Hepatol 1992;7:302–4.
21. Zotti G, Giancarlo B, Sfarzo A, et al. Postoperative gastriccomplications in vascular patients. Int Surg 1984;69:129–31.
22. Martin LF. Stress ulcers are common after aortic surgery.Endoscopic evaluation of prophylactic therapy. Am Surg1994;60:169–74.
23. Goodman AA, Frey CF. Massive upper gastrointestinal hemor-rhage following surgical operations. Ann Surg 1967;167:180–4.
24. Soll A. Medical treatment of peptic ulcer disease. JAMA1996;275:622–9.
25. Tryba M, Zevounou F, Torok M, et al. Prevention of acutestress bleeding with sulcrate, antacids, or cimetidine. Am JMed 1985;79:55–61.
26. Tryba M. Sulcrate versus antacids or H2-antagonists for stressulcer prophylaxis: A meta-analysis on efficacy and pneumoniarate. Crit Care Med 1991;19:942–9.
27. Tryba M. Prophylaxis of stress ulcer bleeding. J Clin Gastro-enterol 1991;13(suppl 2):S44–55.
28. Grau JM, Casademont J, Fernandez-Sola J, et al. Prophylaxisof gastrointestinal tract bleeding in patients admitted to ageneral hospital ward. Scand J Gastroenterol 1993;28:244–8.
29. Ben-Menachem T, Fogel R, Patel RV, et al. Prophylaxis forstress-related gastric hemorrhage in the medical intensive careunit. Ann Intern Med 1994;121:568–75.
30. Pingleton SK, Hadzima, SK. Enteral alimentation and gastro-intestinal bleeding in mechanically ventilated patients. CritCare Med 1983;11:13–6.
31. Hastings PR, Skillman JJ, Bushnell LS, Silen W. Antacidtitration in the prevention of acute gastrointestinal bleeding: Acontrolled, randomized trial in 100 critically ill patients.N Engl J Med 1978;298:1041–5.
32. Valentine RJ, Turner WW, Borman KR, Weigelt JA. Doesnasoenteral feeding afford adequate gastrodudenal stress pro-phylaxis? Crit Care Med 1986;14:599–601.
33. Bonten MJ, Gaillard CA, van der Hulst R, et al. Intermittententeral feeding: The influence in respiratory and digestive tractcolonization in mechanically ventilated intensive care unitpatients. Am J Respir Crit Care Med 1996;154:394–9.
2806 Pimentel et al. AJG – Vol. 95, No. 10, 2000





























