Embed Size (px)
Citation preview

clinicaloptions.com/oncology
FRANCESCO BOCCARDO
Professore Ordinario di Oncologia Professore Ordinario di Oncologia Medica, Università di GenovaMedica, Università di Genova
Direttore Oncologia Medica BDirettore Oncologia Medica BIST .GenovaIST .Genova
Presidente NazionalePresidente Nazionale Associazione Italiana Oncologia Medica Associazione Italiana Oncologia Medica
INIBITORI DELL’AROMATASI(back from San Antonio)
clinicaloptions.com/oncology
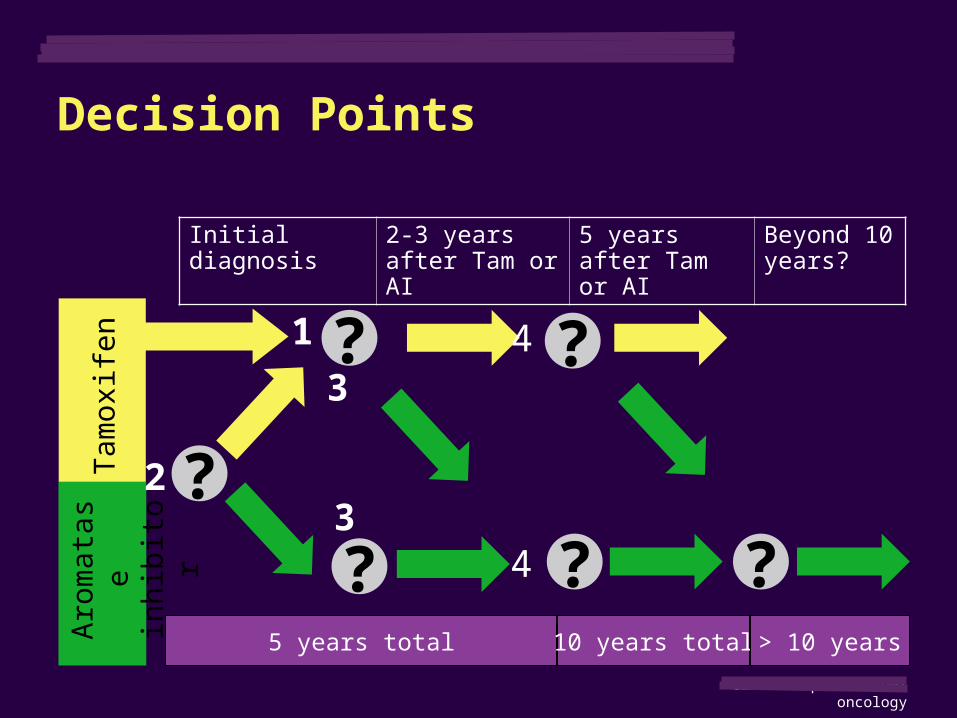
Initial diagnosis 2-3 years after Tam or AI
5 years after Tam or AI
Beyond 10 years?
Tam
oxife
nA
rom
atas
e in
hibi
tor
5 years total 10 years total > 10 years
Decision Points
?
?
?
?
?
1
2
34
4?3
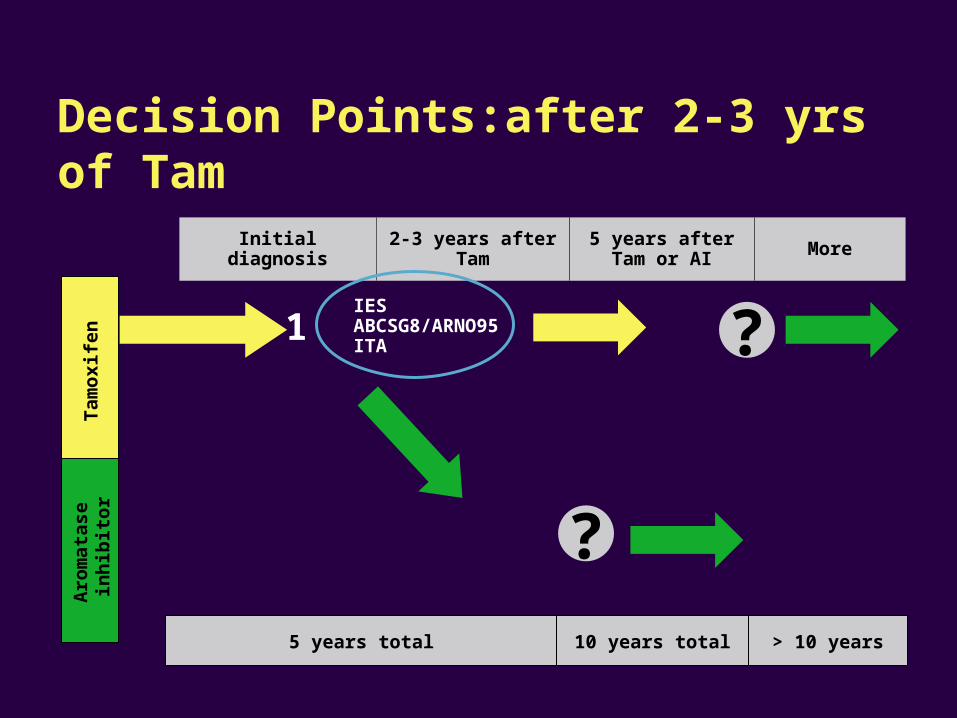
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More
Tam
oxi
fen
Aro
mat
ase
in
hib
ito
r
5 years total 10 years total > 10 years
Decision Points:after 2-3 yrs of Tam
?
?IESABCSG8/ARNO95ITA
1
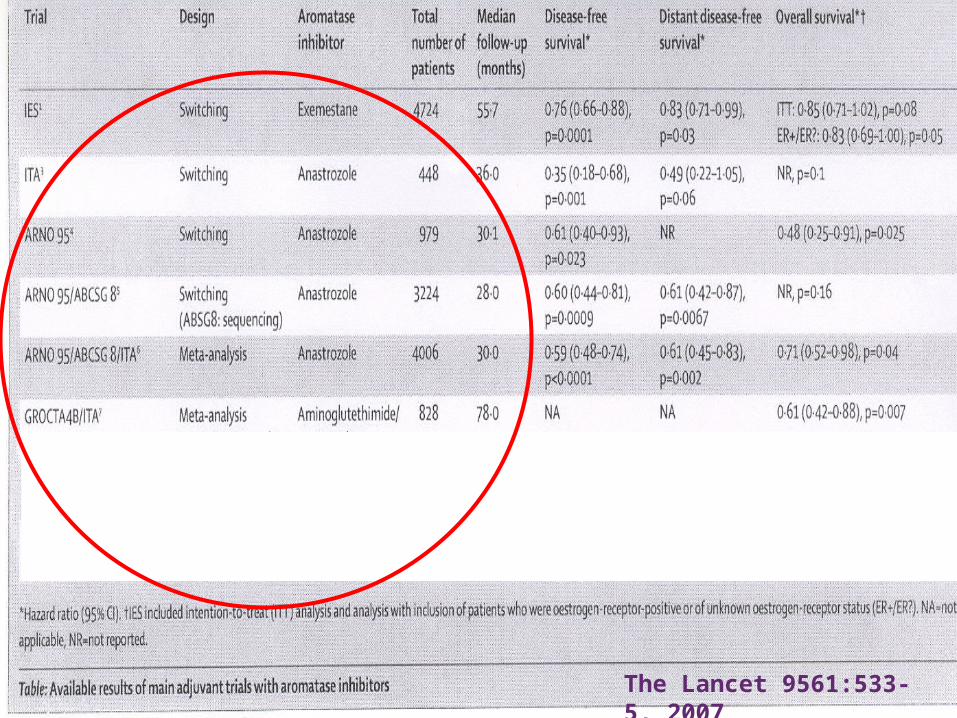
The Lancet 9561:533-5, 2007
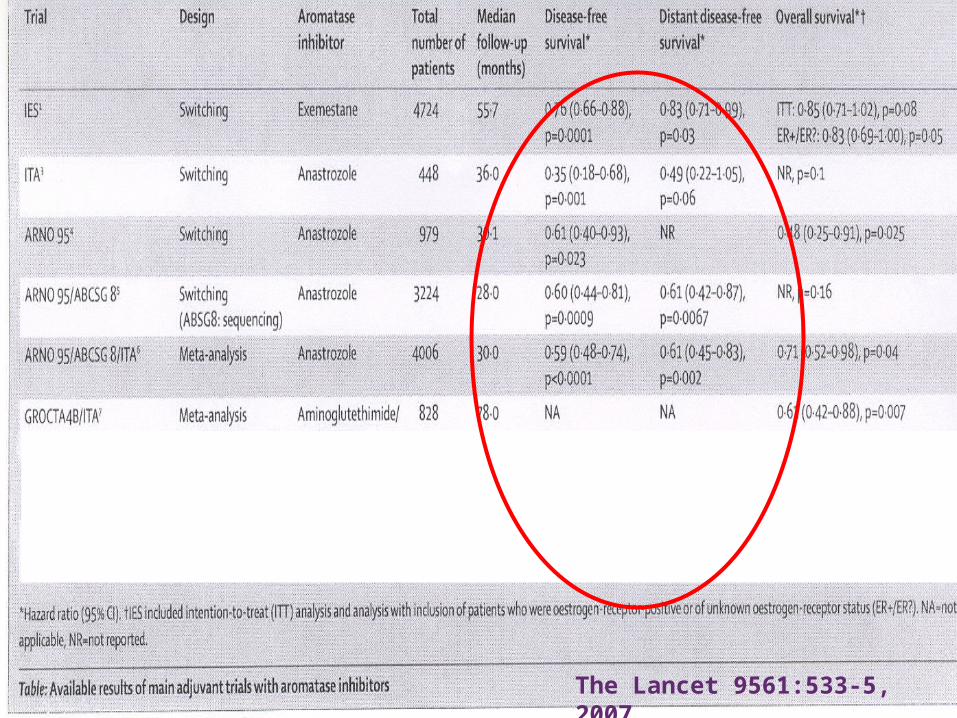
The Lancet 9561:533-5, 2007
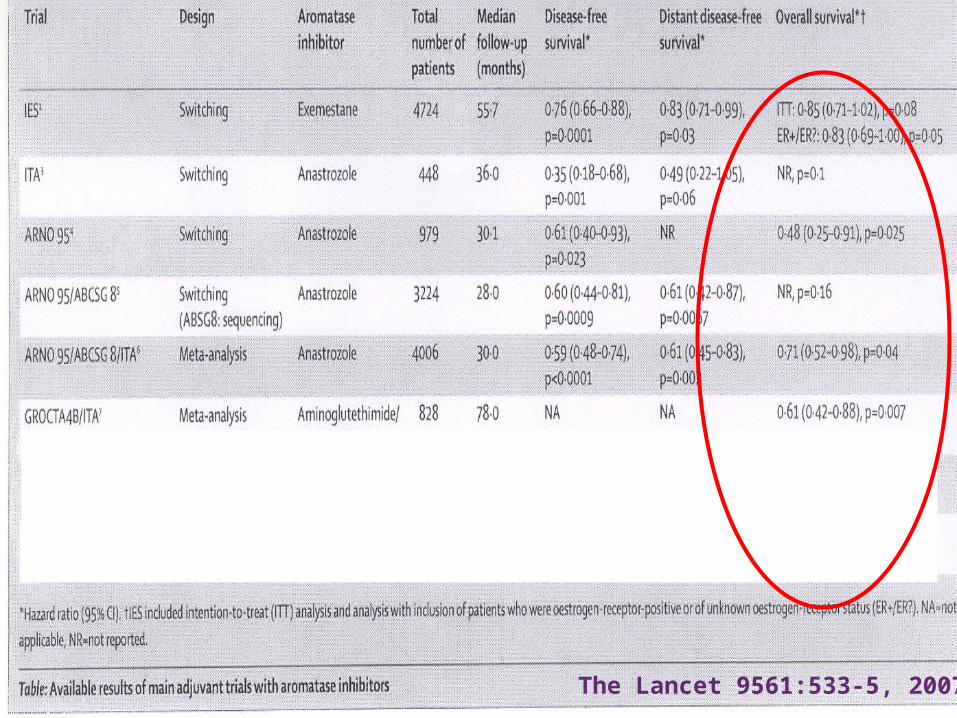
The Lancet 9561:533-5, 2007
clinicaloptions.com/oncology
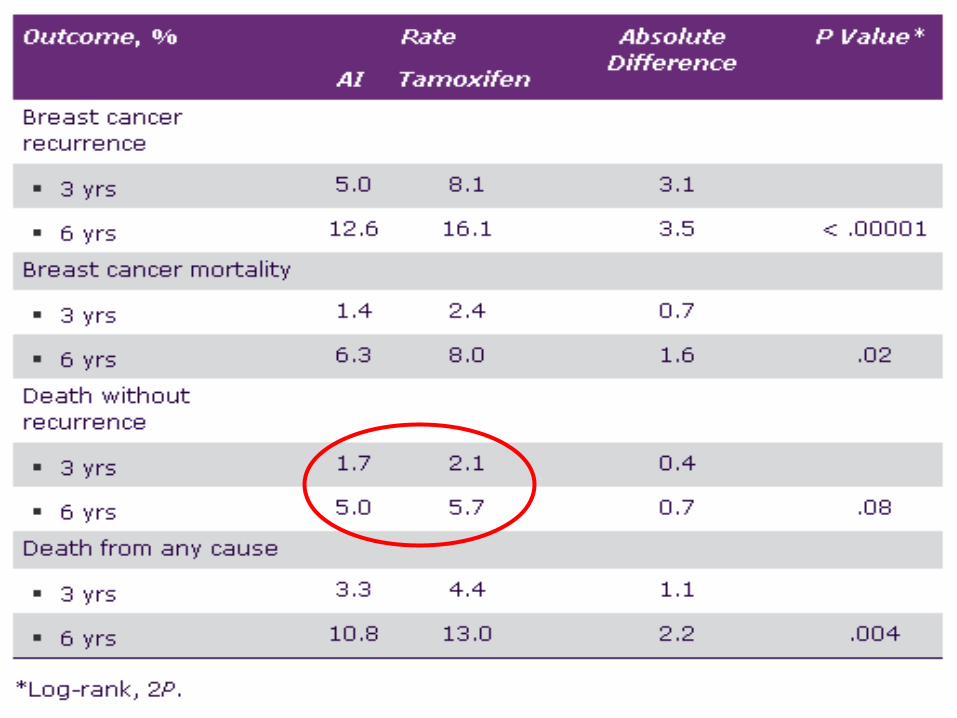
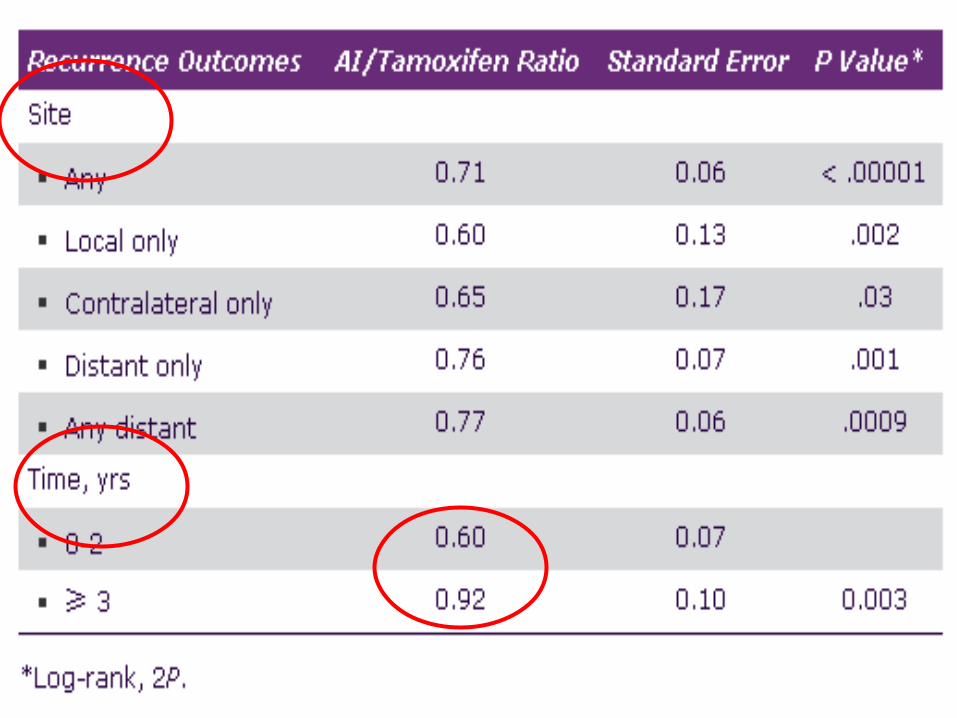
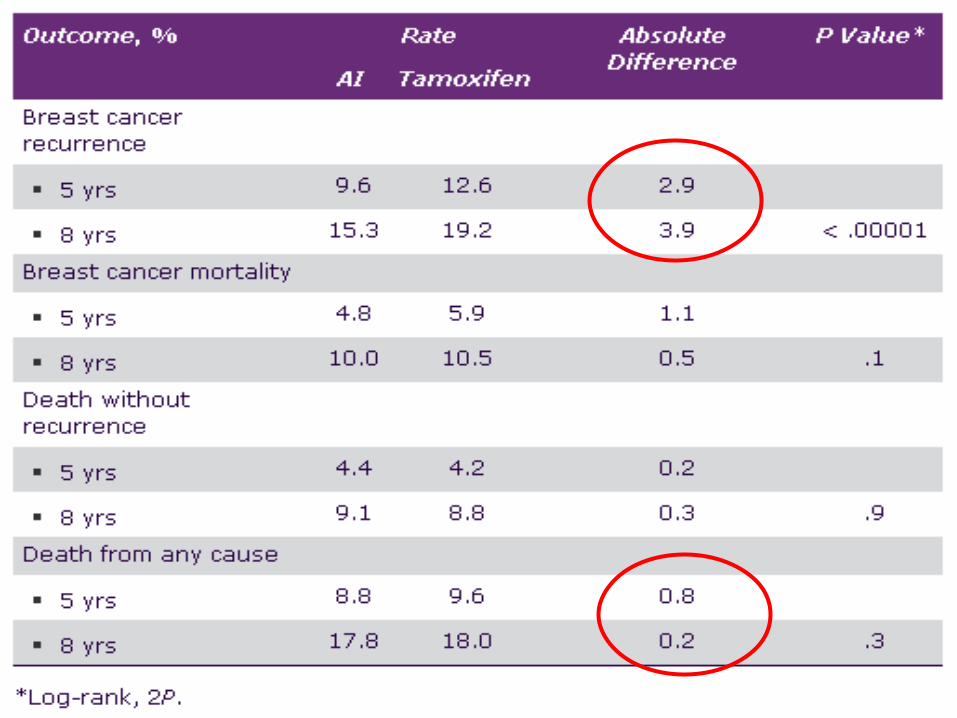
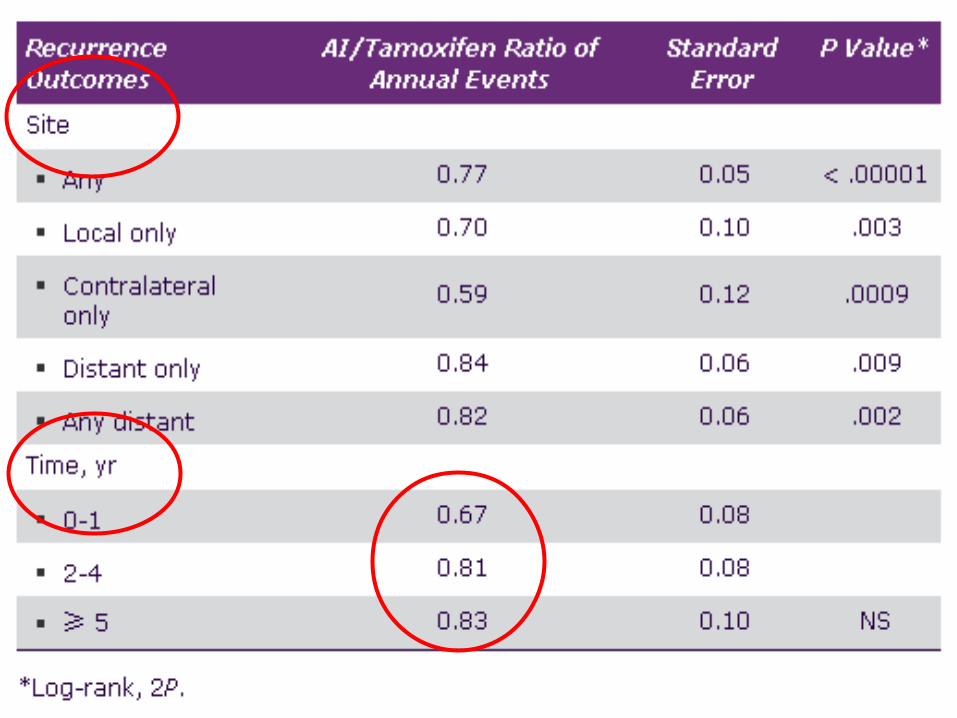
AIOG Metanalysis
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
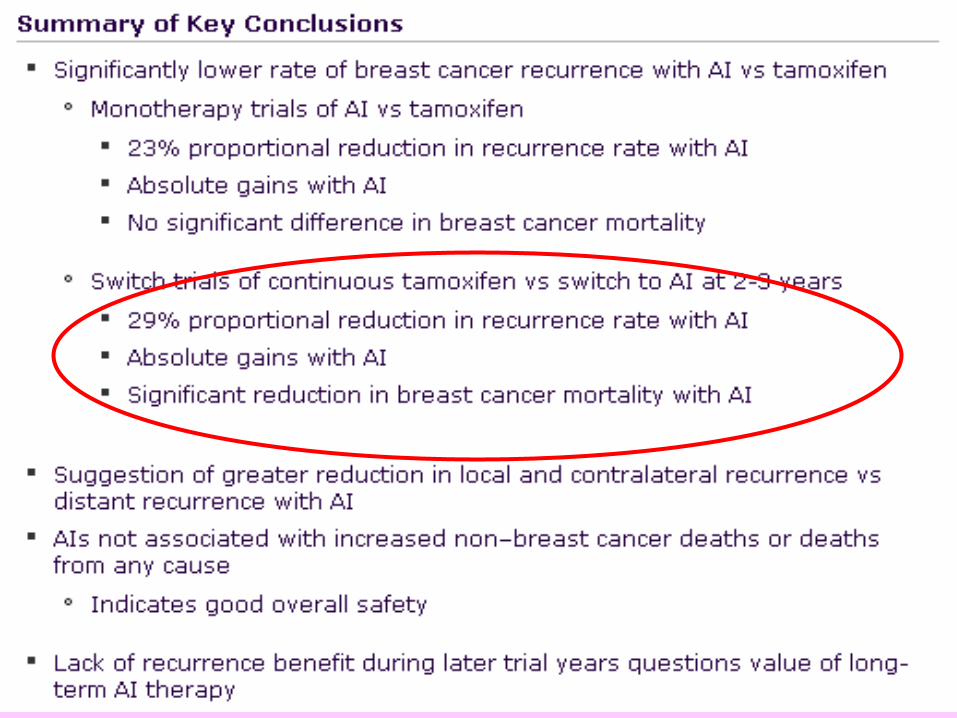
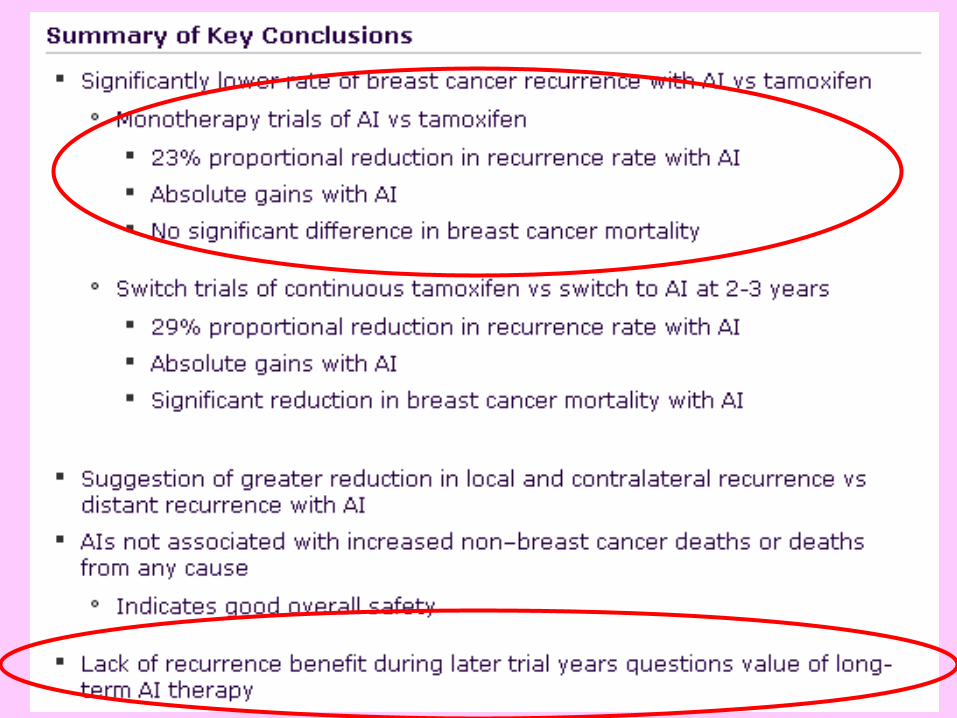
……….back from San Antonio 2008: take home #1
“There is a clear benefit (including a S benefit) in switching women already on treatment with Tam to an AI (anastrozole,exemestane) unless AI therapy is contraindicated”
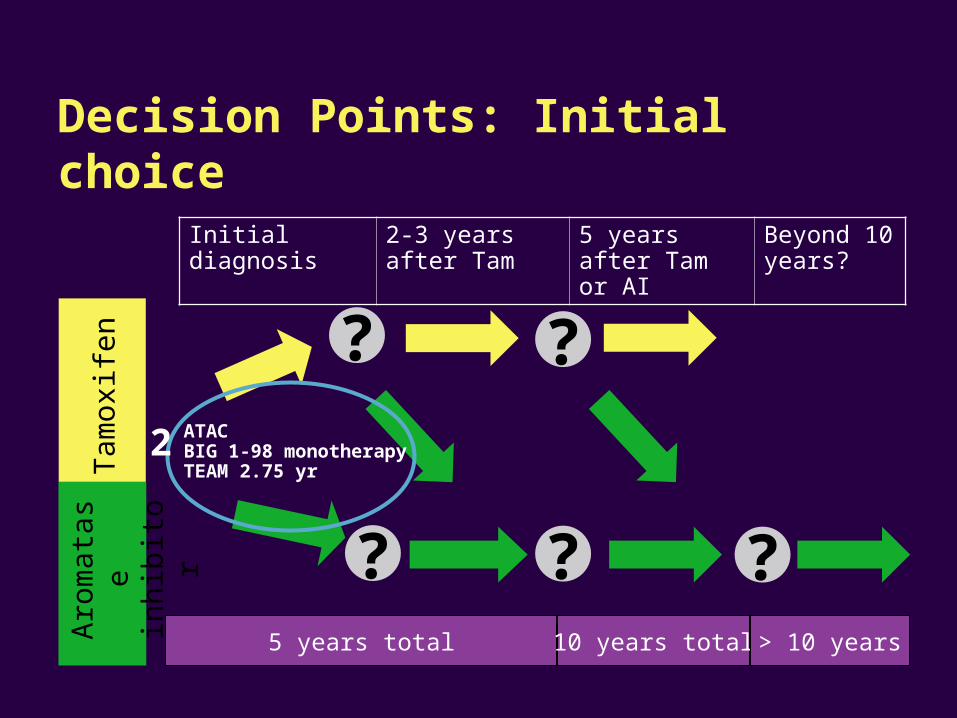
Decision Points: Initial choice
?
?
?
?
Initial diagnosis 2-3 years after Tam
5 years after Tam or AI
Beyond 10 years?
Tam
oxife
nA
rom
atas
e in
hibi
tor
5 years total 10 years total > 10 years
ATACBIG 1-98 monotherapy TEAM 2.75 yr
?
2
clinicaloptions.com/oncology
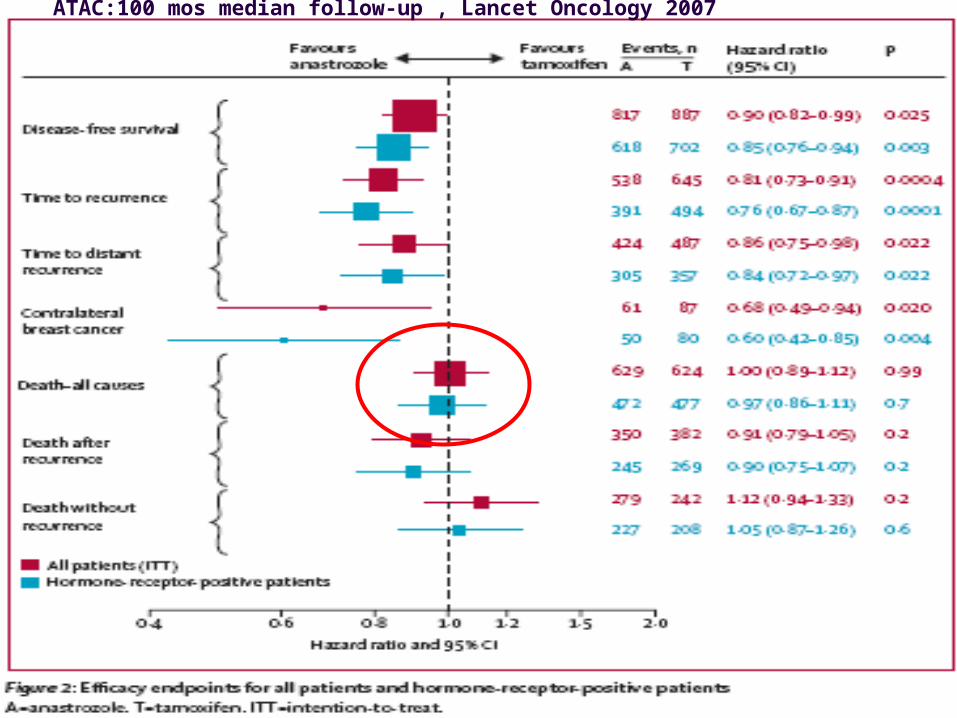
ATAC:100 mos median follow-up , Lancet Oncology 2007
clinicaloptions.com/oncology
AIOG Metanalysis
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
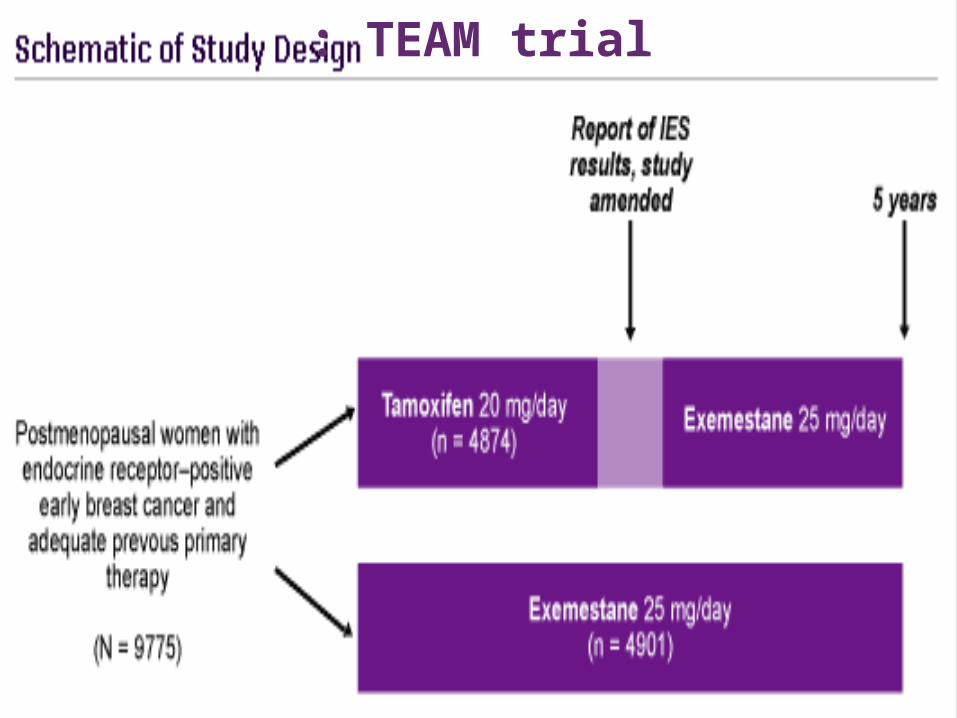
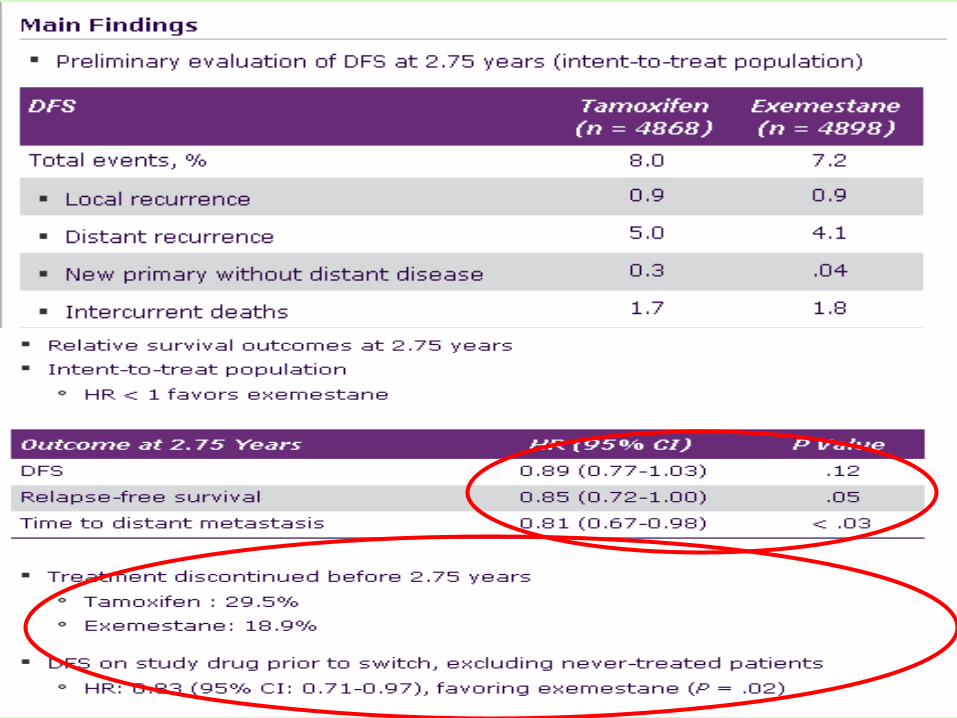
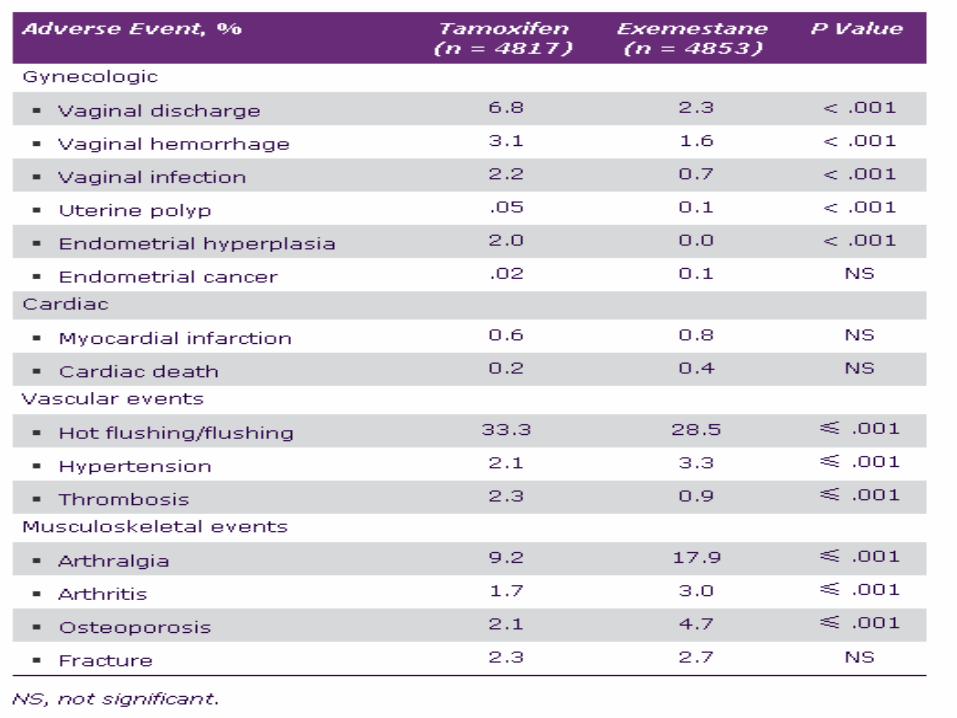
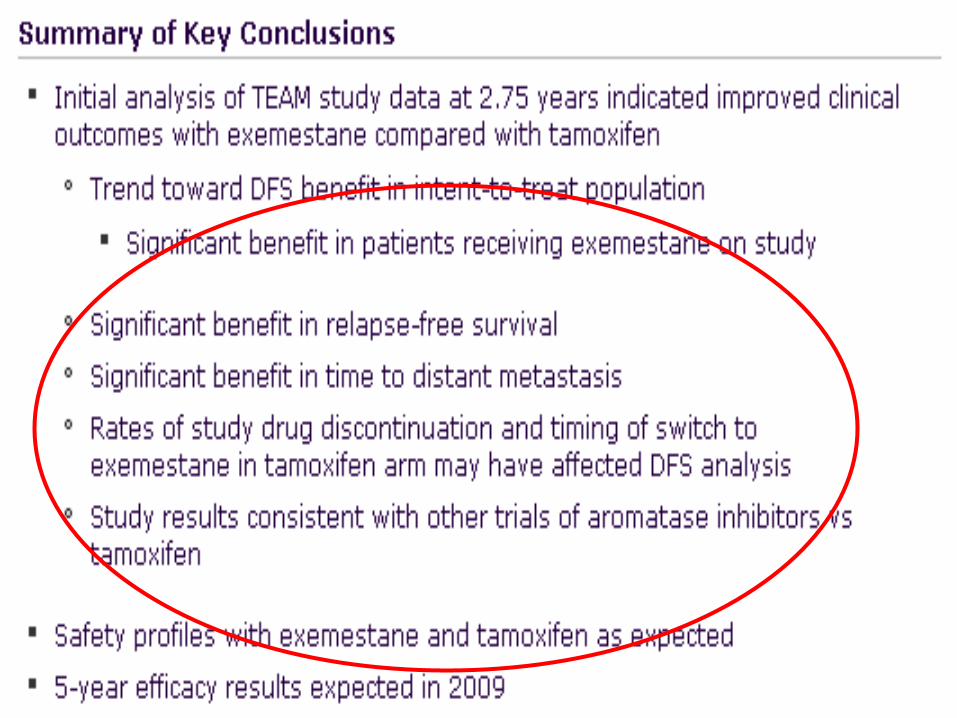
: TEAM trial
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
……….back from San Antonio 2008: take home #2
“Three drugs now available as front line
treatment:
Which drug or which patients?”
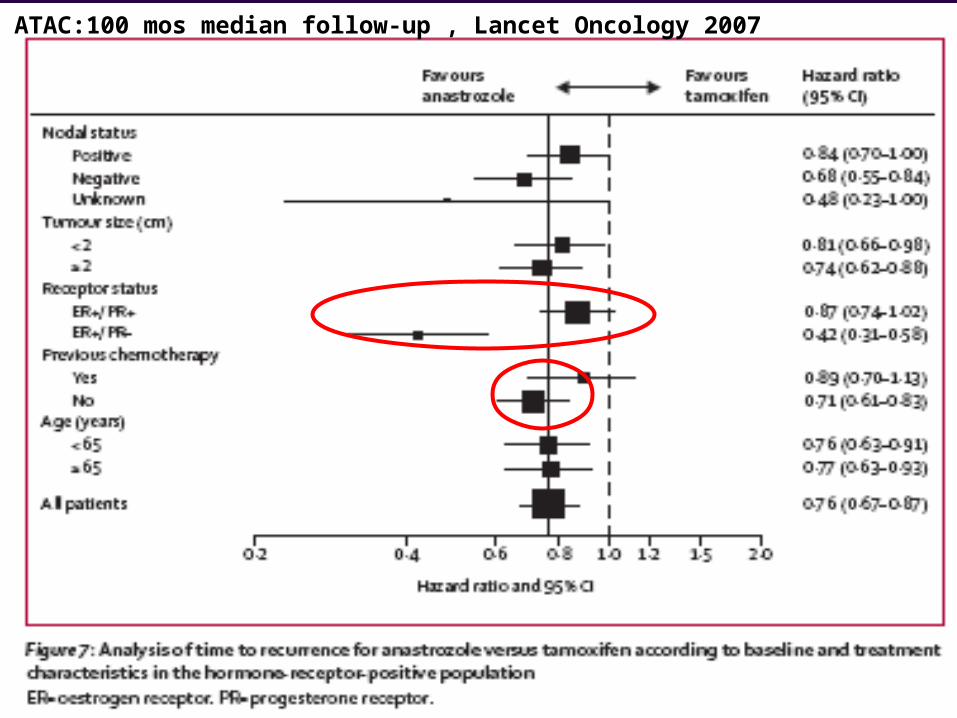
ATAC:100 mos median follow-up , Lancet Oncology 2007
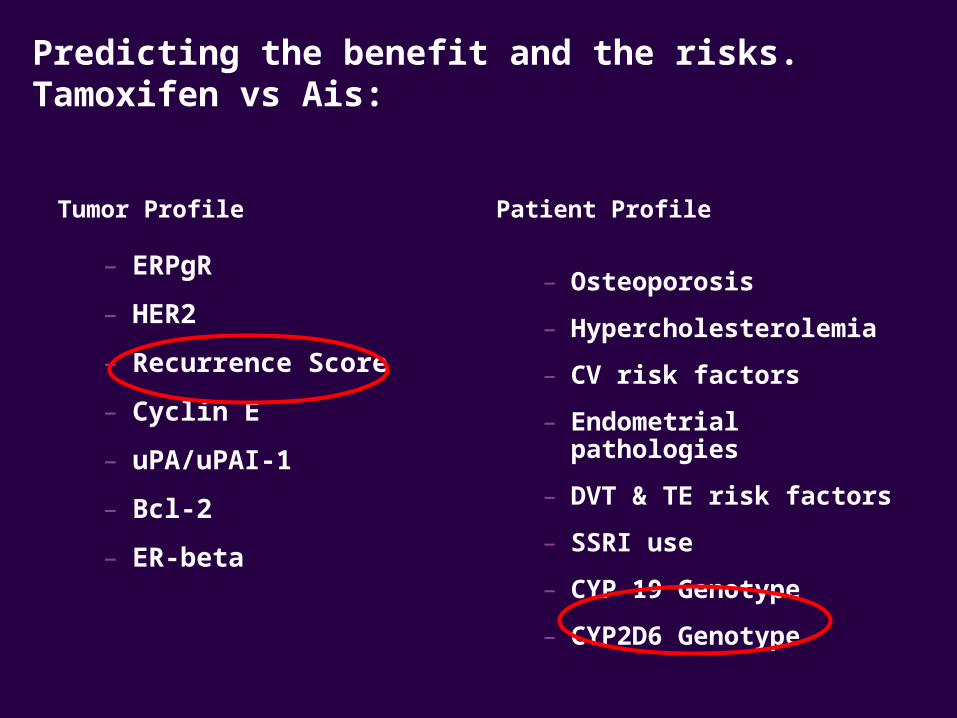
Predicting the benefit and the risks. Tamoxifen vs Ais:
Tumor Profile
– ERPgR
– HER2
– Recurrence Score
– Cyclin E
– uPA/uPAI-1
– Bcl-2
– ER-beta
Patient Profile
– Osteoporosis
– Hypercholesterolemia
– CV risk factors
– Endometrial pathologies
– DVT & TE risk factors
– SSRI use
– CYP 19 Genotype
– CYP2D6 Genotype
clinicaloptions.com/oncology
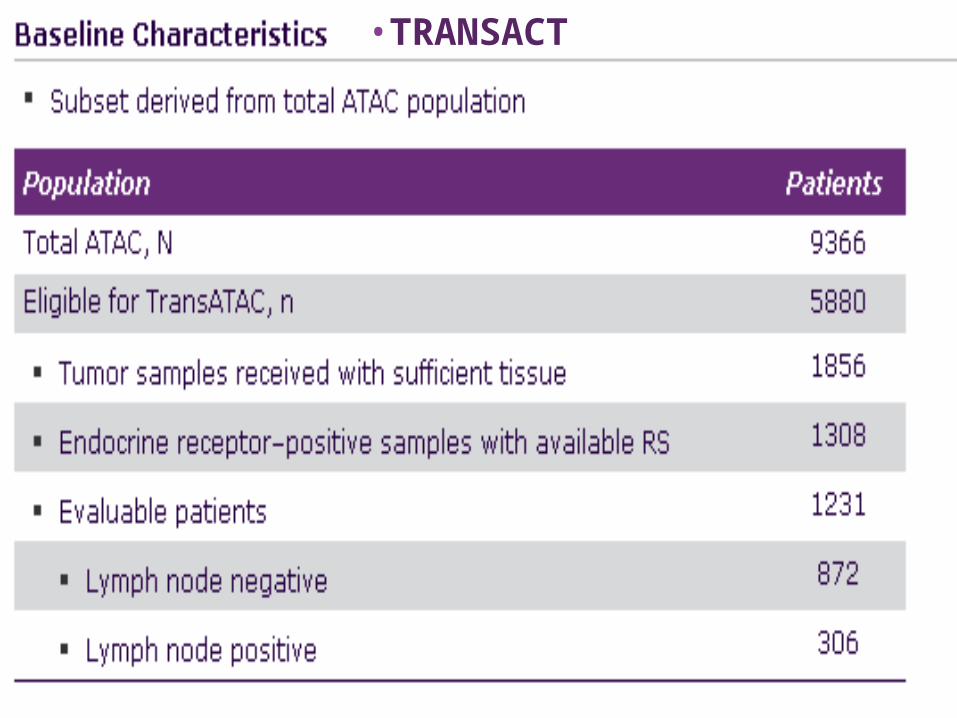
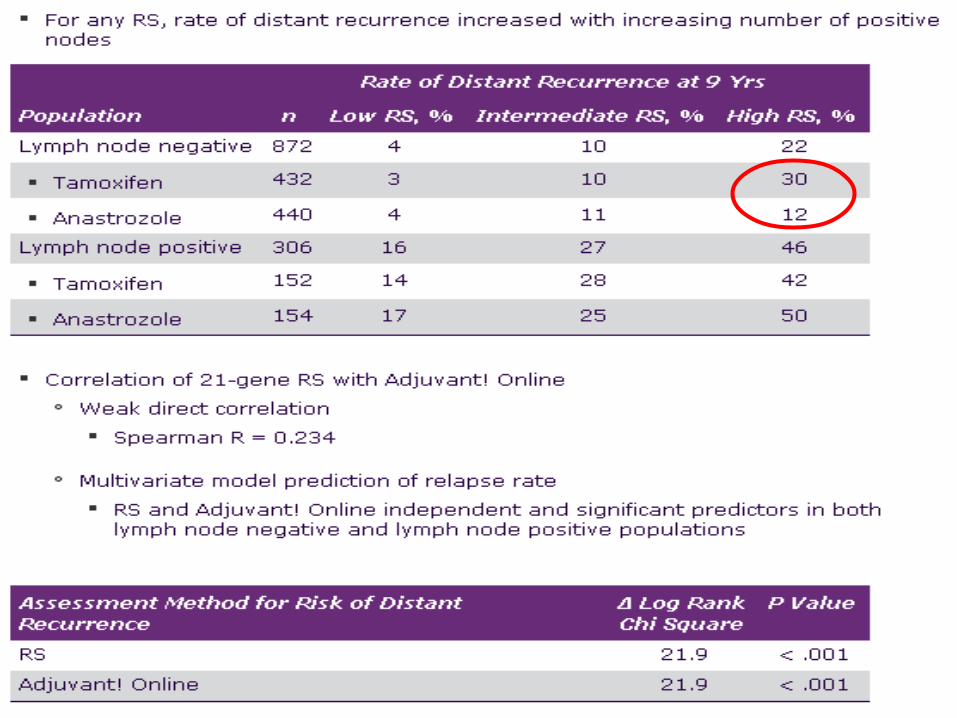
•TRANSACT
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
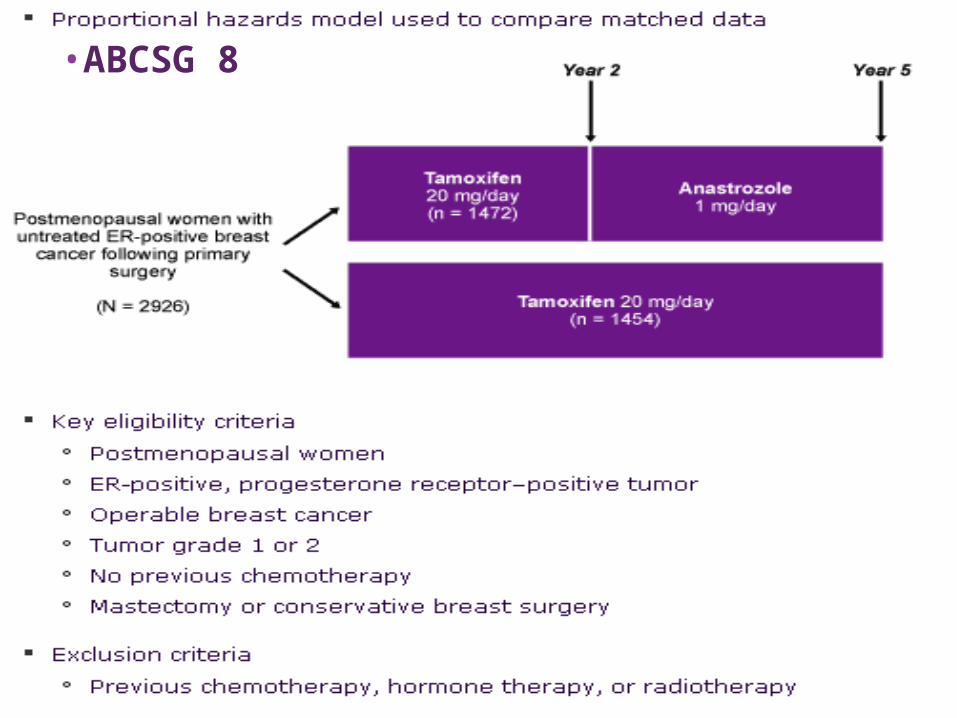
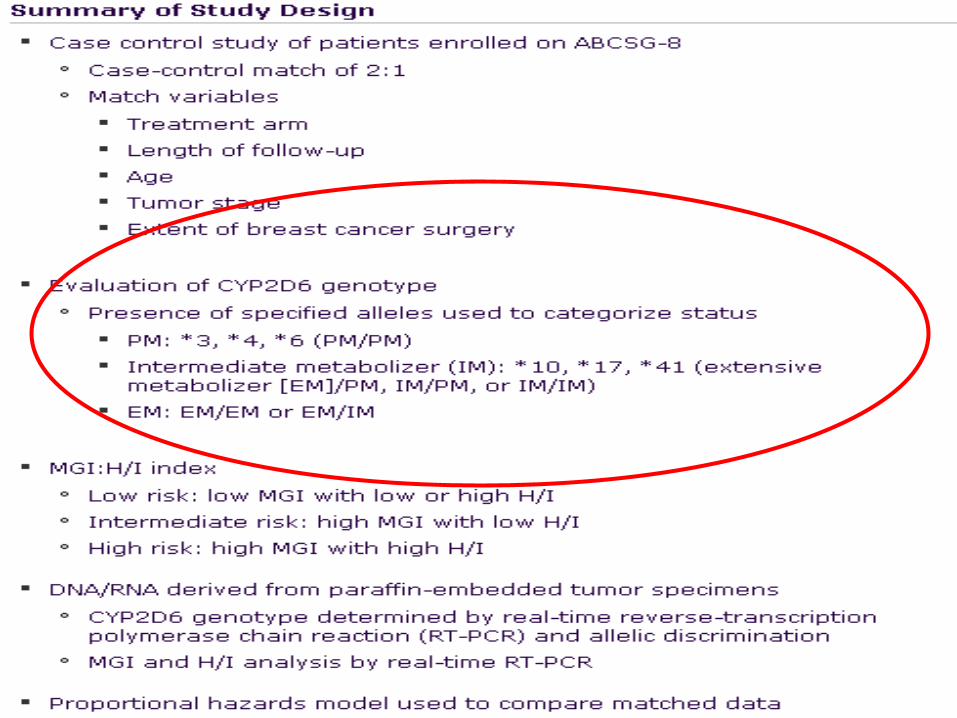
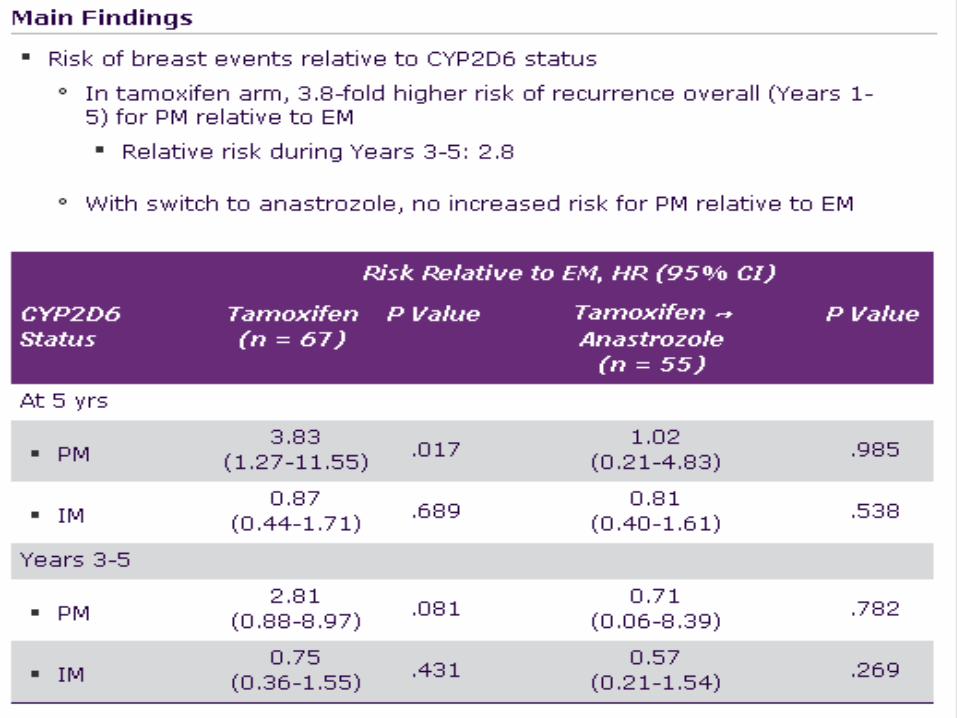
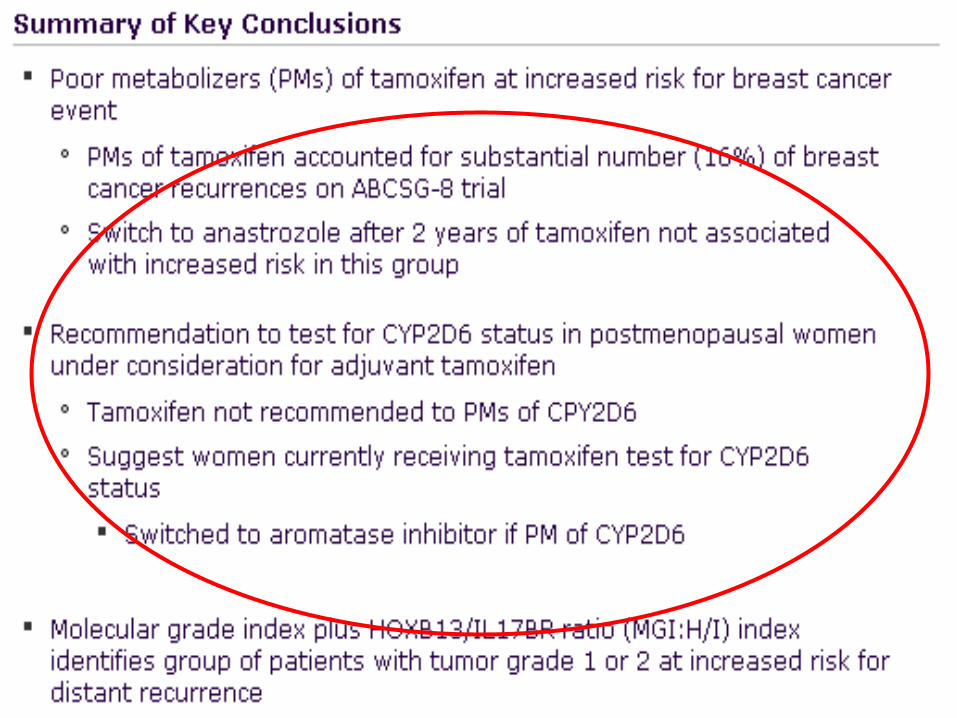
•ABCSG 8
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
……….back from San Antonio 2008: take home #3
“Starting with an Ai is a reasonable choice especially in certain patient subsets (i.e. PgRneg,HER2 pos,HRScore Node neg,poor metabolizers of CYP2D6….!):however:
1) no major mortality advantge
2) No over rate in selecting patients “

clinicaloptions.com/oncology
Initial diagnosis 2-3 years after Tam or AI
5 years after Tam or AI
Beyond 10 years?
Tam
oxife
nA
rom
atas
e in
hibi
tor
5 years total 10 years total > 10 years
Decision Points:sequencing
?
?
?
?
?
1
2
34
4?3
ABCSG8TEAM 5-yr: n.a. yet
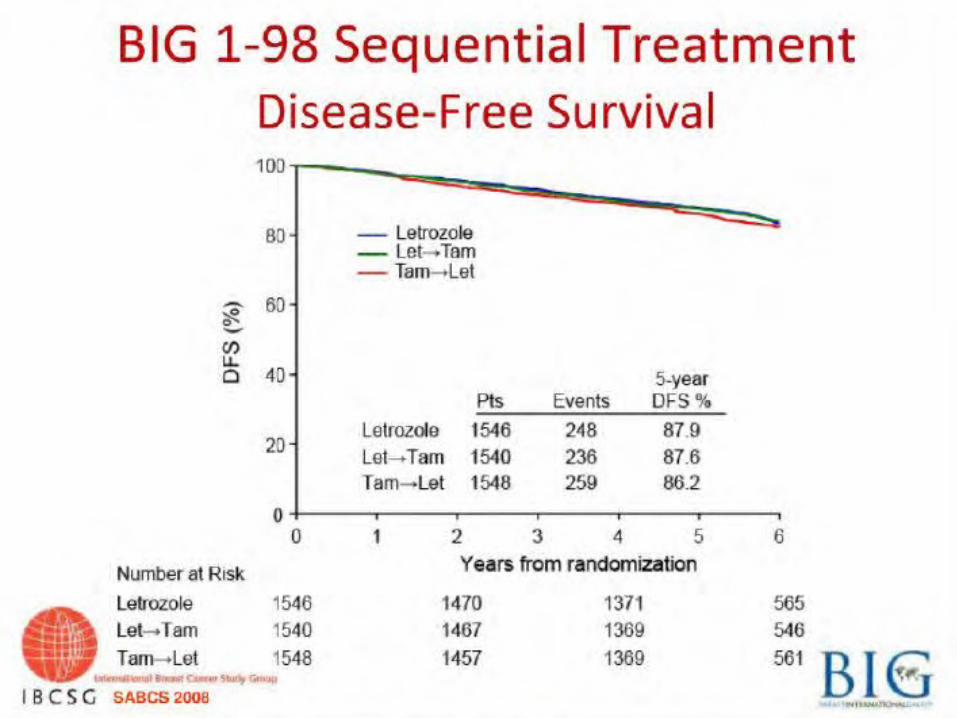
BIG-1-98
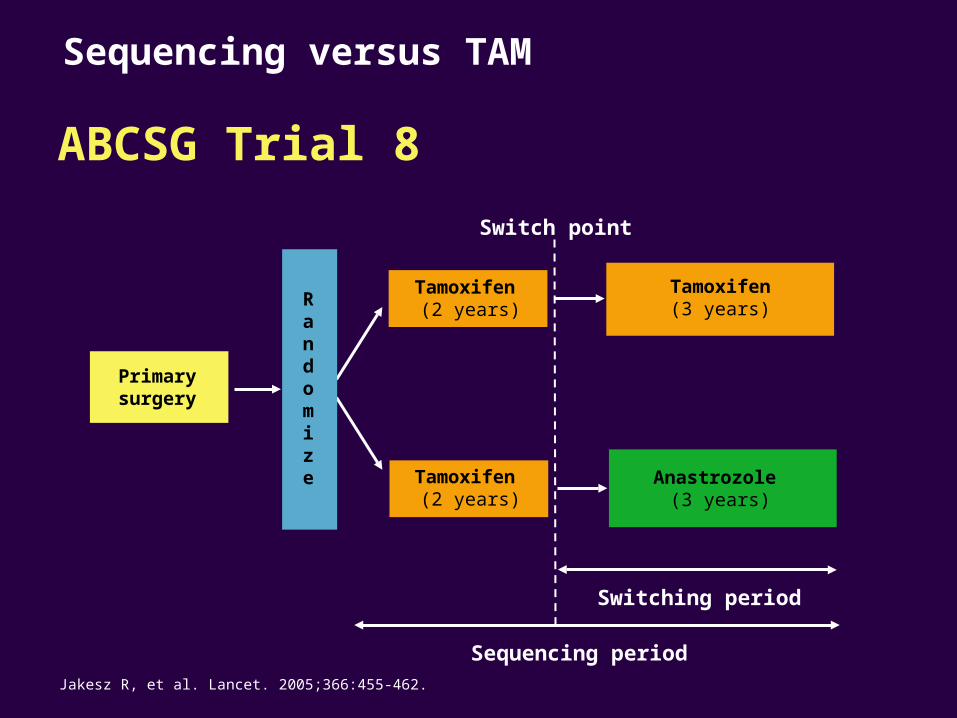
Primarysurgery
Randomize Anastrozole
(3 years)
Switching period
Sequencing period
Switch point
Tamoxifen(3 years)
Tamoxifen (2 years)
Jakesz R, et al. Lancet. 2005;366:455-462.
Tamoxifen (2 years)
ABCSG Trial 8
Sequencing versus TAM
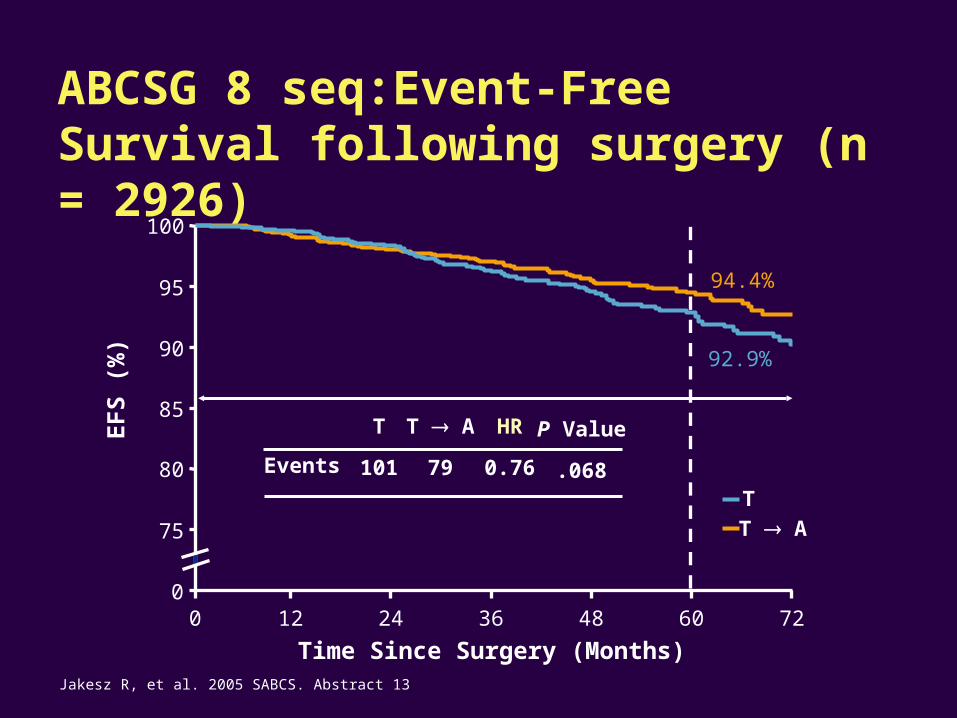
0
75
80
85
90
95
100
0 12 24 36 48 60 72
HR
0.76Events
P Value
.068
T
101
T A
79
94.4%
92.9%
ABCSG 8 seq:Event-Free Survival following surgery (n = 2926)
T A
T
EF
S (
%)
Time Since Surgery (Months)Jakesz R, et al. 2005 SABCS. Abstract 13
clinicaloptions.com/oncology
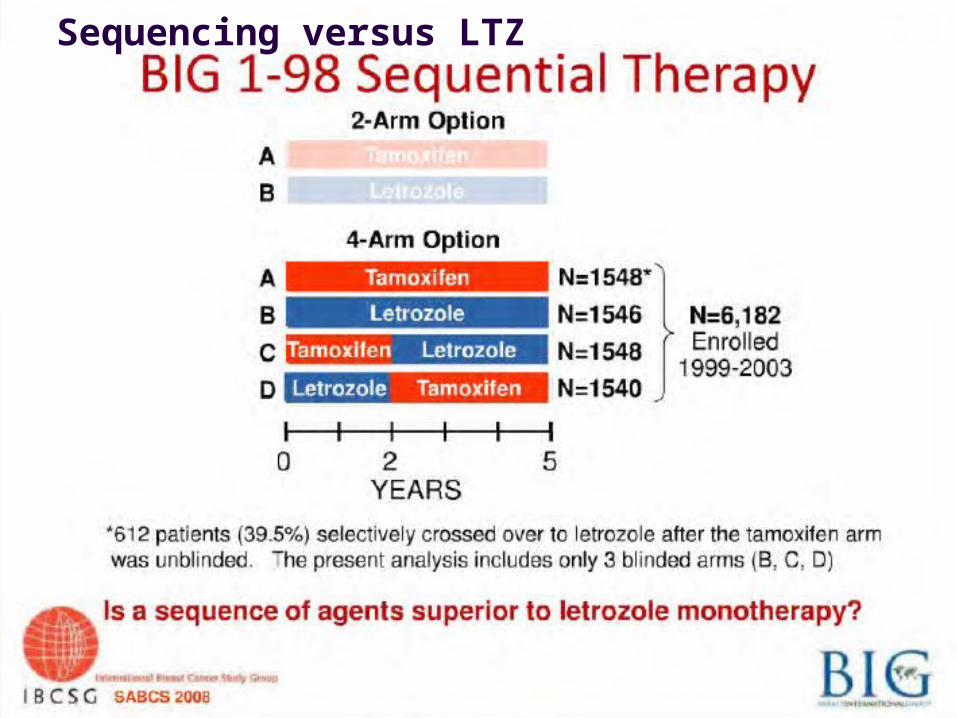
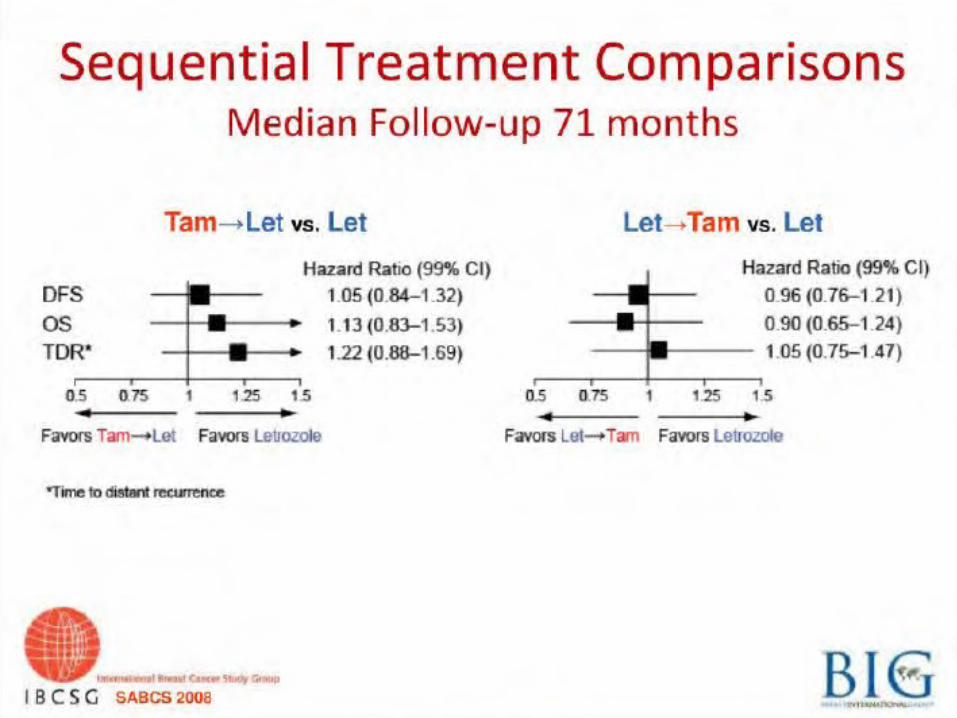
Sequencing versus LTZ
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
clinicaloptions.com/oncology
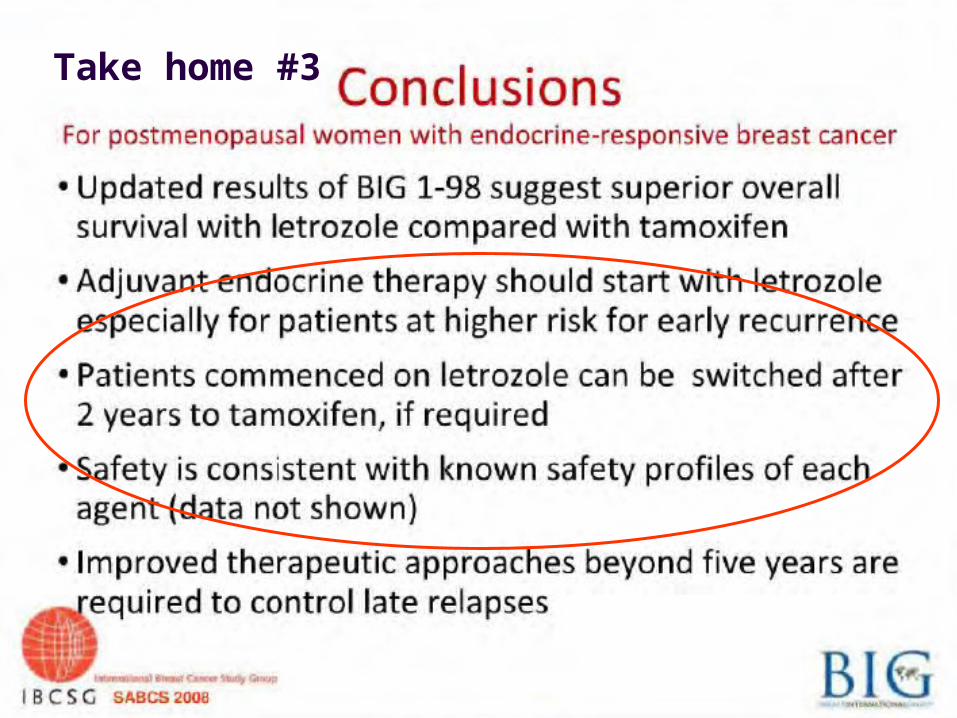
Take home #3
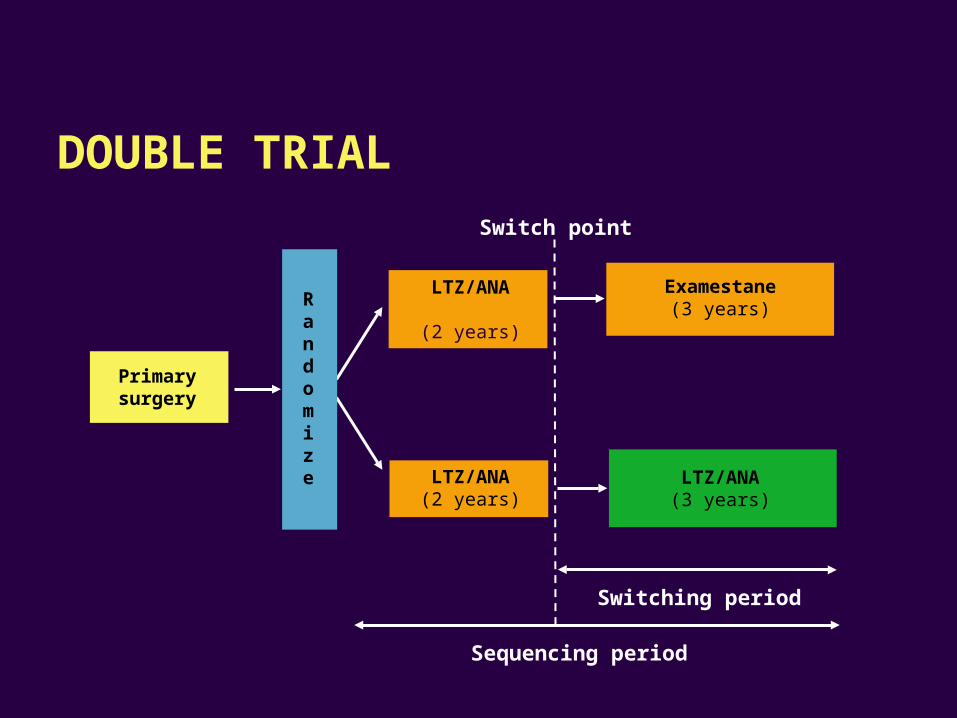
Primarysurgery
Randomize LTZ/ANA
(3 years)
Switching period
Sequencing period
Switch point
Examestane(3 years)
LTZ/ANA
(2 years)
LTZ/ANA(2 years)
DOUBLE TRIAL
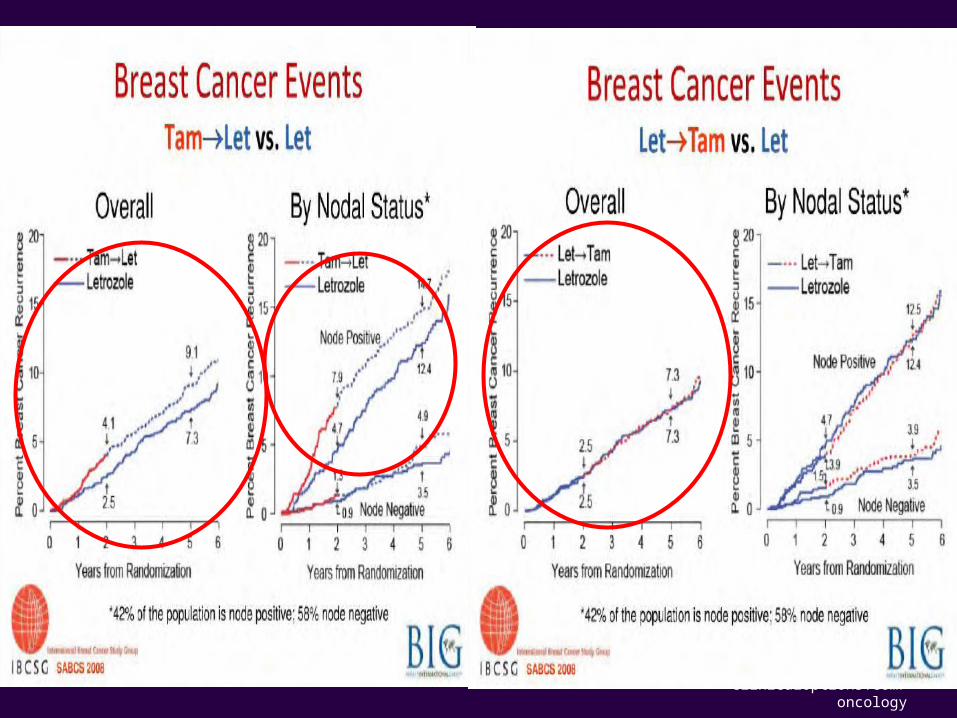
……….back from S. Antonio 2008: Take home #4
“sequencing TAM with an Ai is probably better
than TAM alone,but does not offer major
advantages vs Ai alone; switching from an
Ai to TAM is possible if required… “
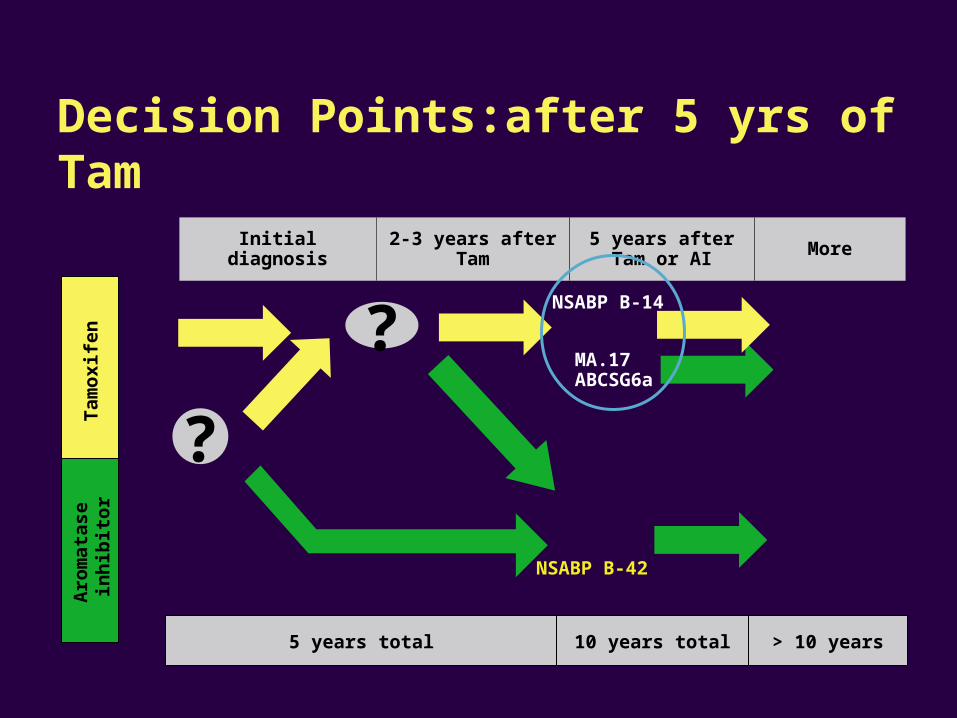
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More
Tam
oxi
fen
Aro
mat
ase
in
hib
ito
r
5 years total 10 years total > 10 years
Decision Points:after 5 yrs of Tam
MA.17ABCSG6a
NSABP B-42
?
?
NSABP B-14
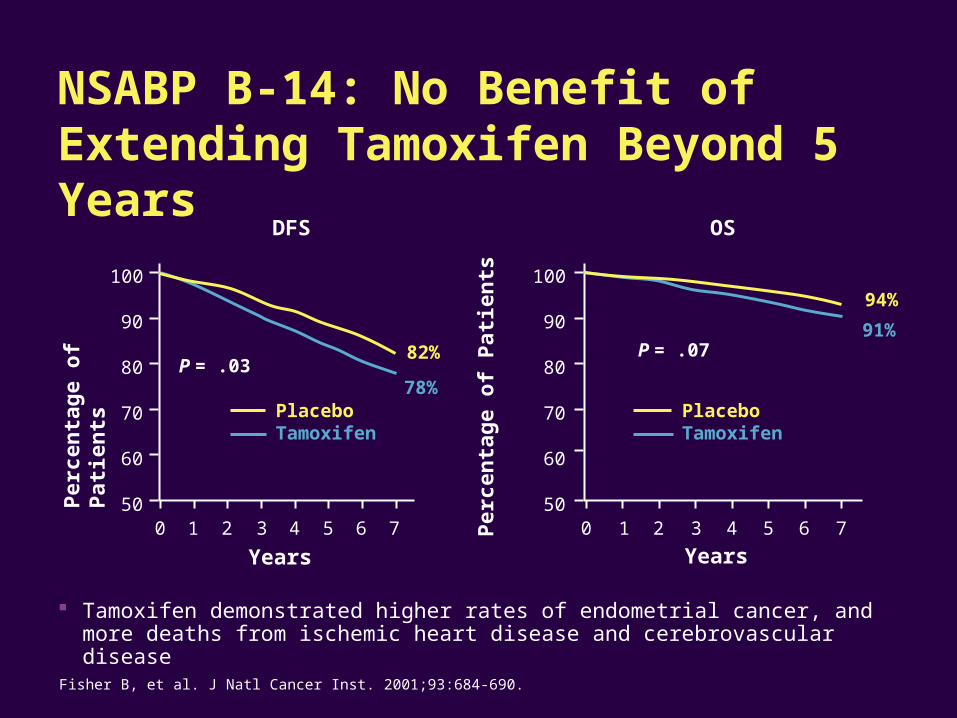
DFS
Years
OS
Years
Tamoxifen demonstrated higher rates of endometrial cancer, and more deaths from ischemic heart disease and cerebrovascular disease
100
90
80
70
60
50Per
cen
tag
e o
f P
atie
nts
0 5
PlaceboTamoxifen
7
82%
78%P = .03
1 2 4 63 0 5
100
90
80
70
60
507
Per
cen
tag
e o
f P
atie
nts
PlaceboTamoxifen
94%
91%P = .07
1 32 4 6
Fisher B, et al. J Natl Cancer Inst. 2001;93:684-690.
NSABP B-14: No Benefit of Extending Tamoxifen Beyond 5 Years
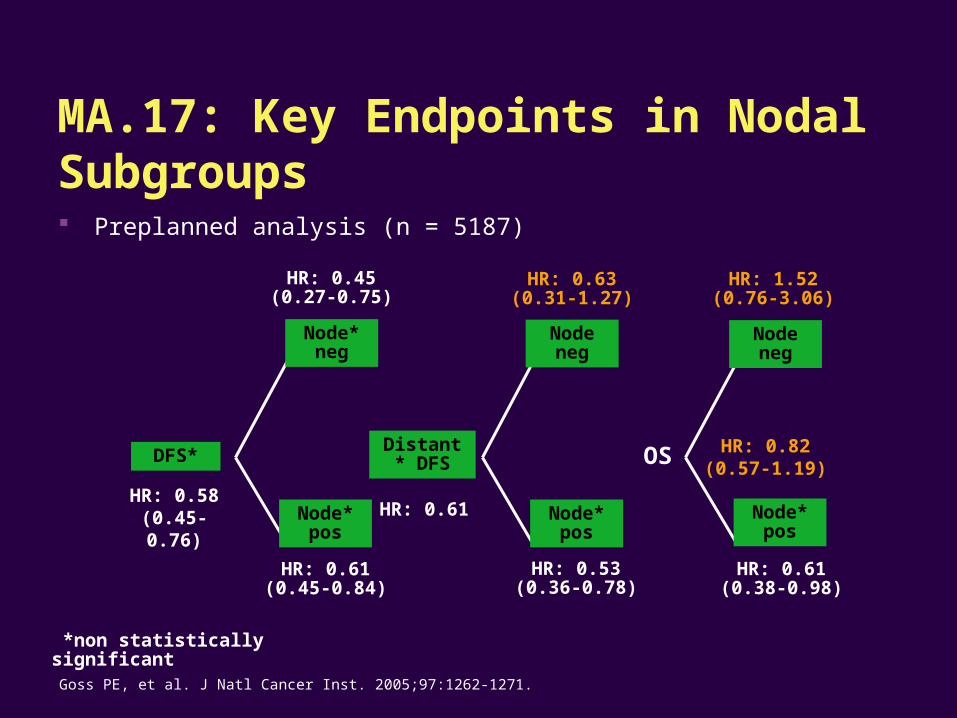
DFS*Distant*
DFS
Node*pos
Node* pos
Node* neg
Node neg
Node neg
Node* pos
*non statistically significant
HR: 0.61(0.45-0.84)
HR: 0.45(0.27-0.75)
HR: 0.63(0.31-1.27)
HR: 0.53(0.36-0.78)
HR: 1.52(0.76-3.06)
HR: 0.61(0.38-0.98)
HR: 0.58(0.45-0.76) HR: 0.61
HR: 0.82(0.57-1.19)
OS
Goss PE, et al. J Natl Cancer Inst. 2005;97:1262-1271.
Preplanned analysis (n = 5187)
MA.17: Key Endpoints in Nodal Subgroups
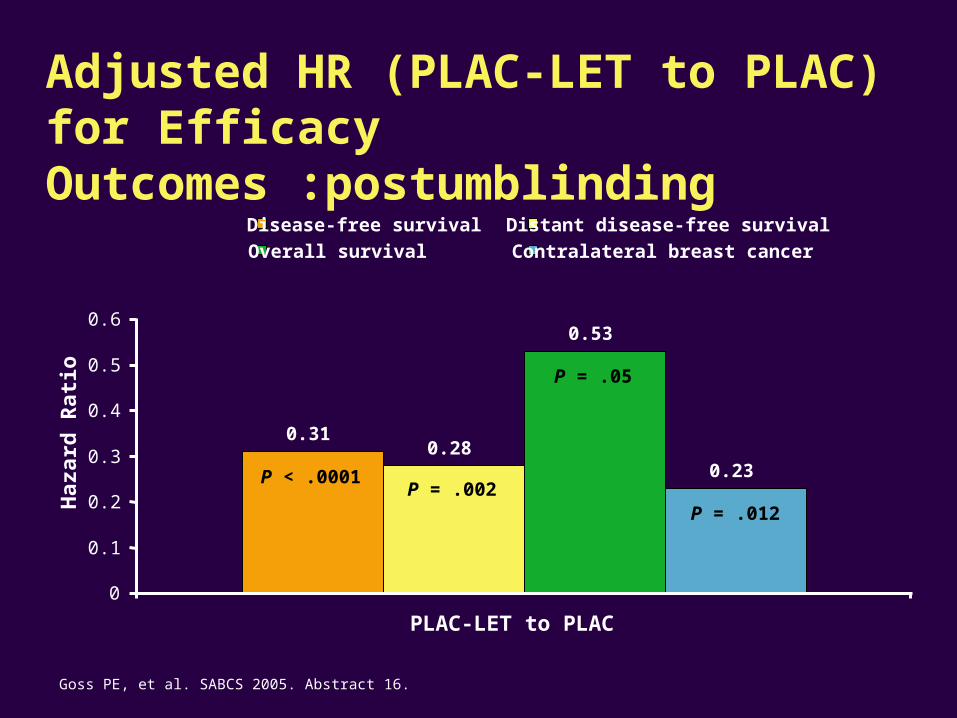
Adjusted HR (PLAC-LET to PLAC) for Efficacy Outcomes :postumblinding
Goss PE, et al. SABCS 2005. Abstract 16.
p<0.0001
p=0.002
p=0.05
p=0.012
0.310.28
0.53
0.23
0
0.1
0.2
0.3
0.4
0.5
0.6
PLAC-LET to PLAC
Disease-free survival Distant disease-free survival
Overall survival Contralateral breast cancer
Haz
ard
Rat
io
P < .0001P = .002
P = .05
P = .012
………back from S.Antonio 2008: Take home #5
“ Late switching after 5 yrs of TAM: no news “
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More
Tam
oxi
fen
Aro
mat
ase
in
hib
ito
r
5 years total 10 years total > 10 years
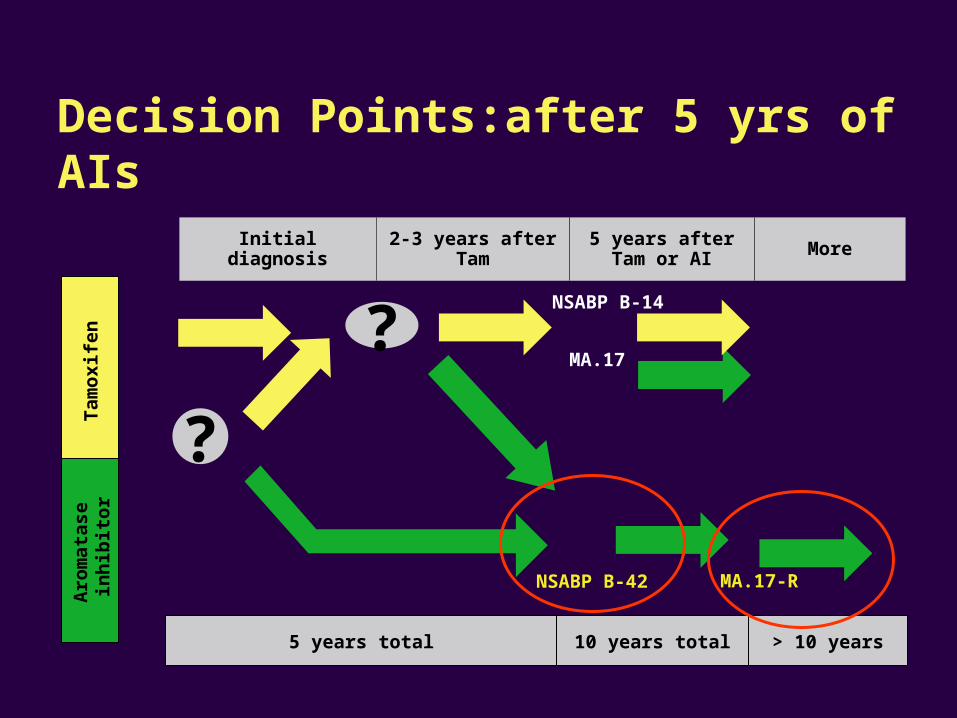
Decision Points:after 5 yrs of AIs
MA.17
MA.17-RNSABP B-42
?
?
NSABP B-14
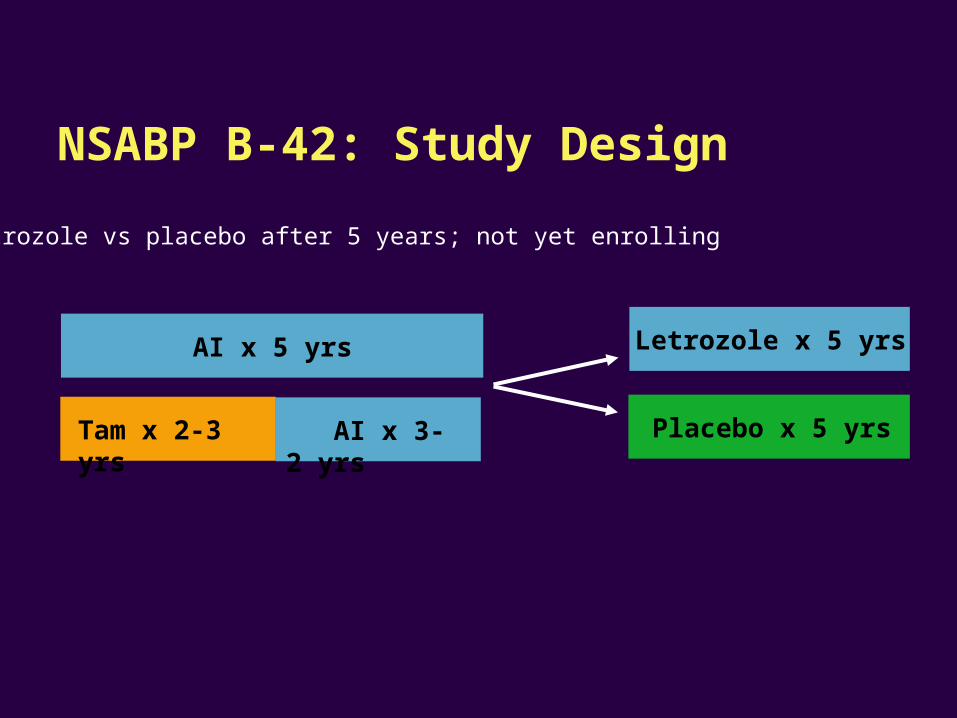
AI x 5 yrs
AI x 3-2 yrs
Tam x 2-3 yrs
Letrozole x 5 yrs
Placebo x 5 yrs
Letrozole vs placebo after 5 years; not yet enrolling
NSABP B-42: Study Design
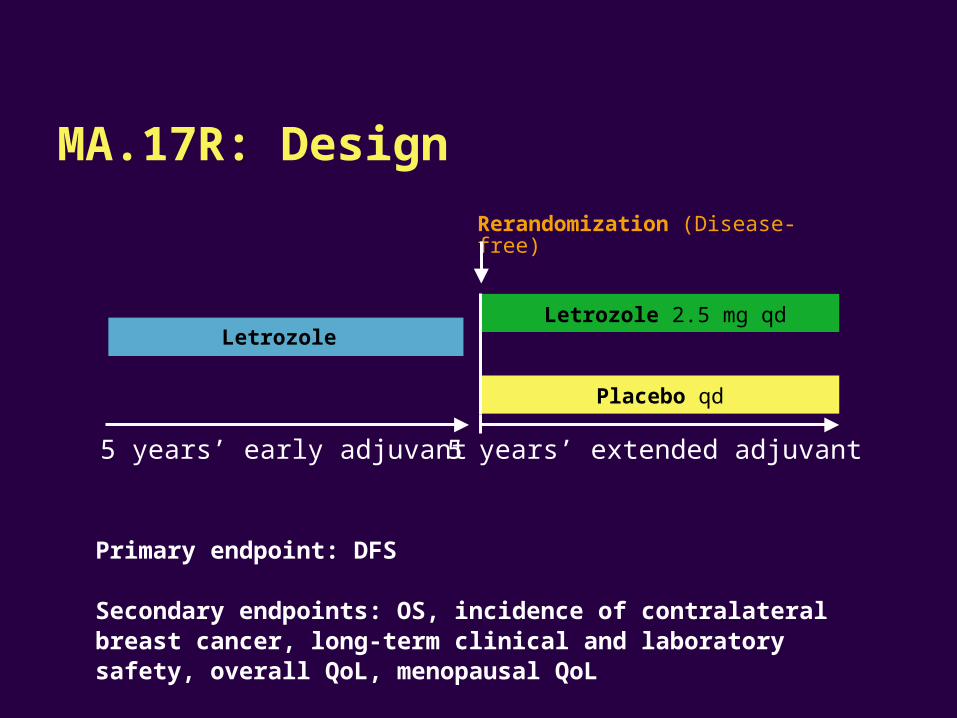
Primary endpoint: DFS
Secondary endpoints: OS, incidence of contralateral breast cancer, long-term clinical and laboratory safety, overall QoL, menopausal QoL
MA.17R: Design
Rerandomization (Disease-free)
Letrozole
Placebo qd
Letrozole 2.5 mg qd
5 years’ early adjuvant 5 years’ extended adjuvant
…….back from S. Antonio 2008: Take home #6
“ are trials concerning Ai optimal duration still
justified? “
clinicaloptions.com/oncology
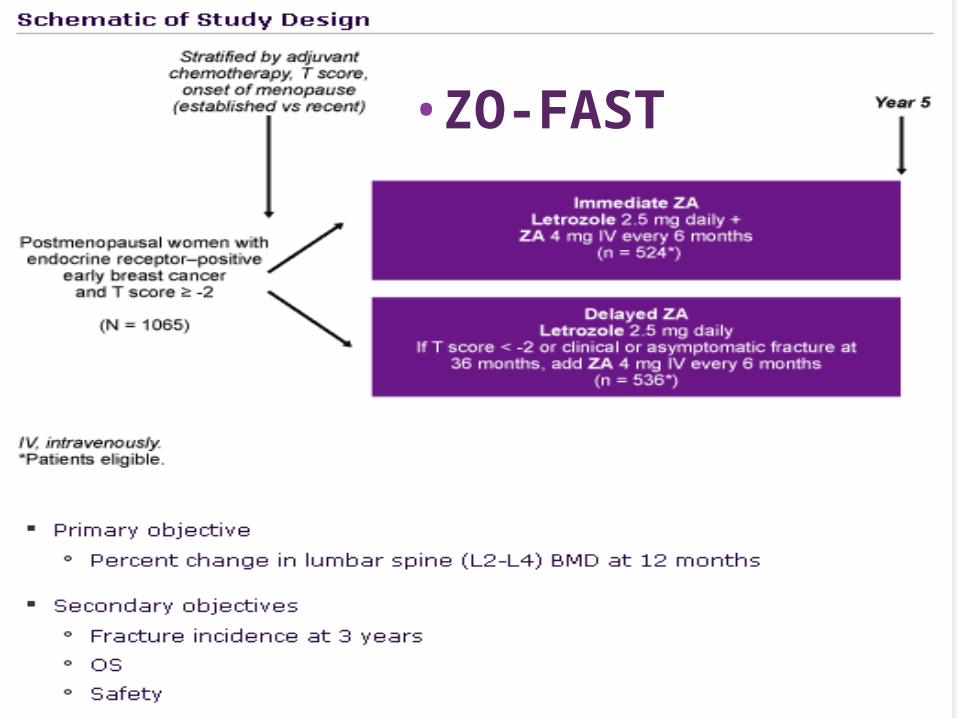
•ZO-FAST
clinicaloptions.com/oncology
clinicaloptions.com/oncology
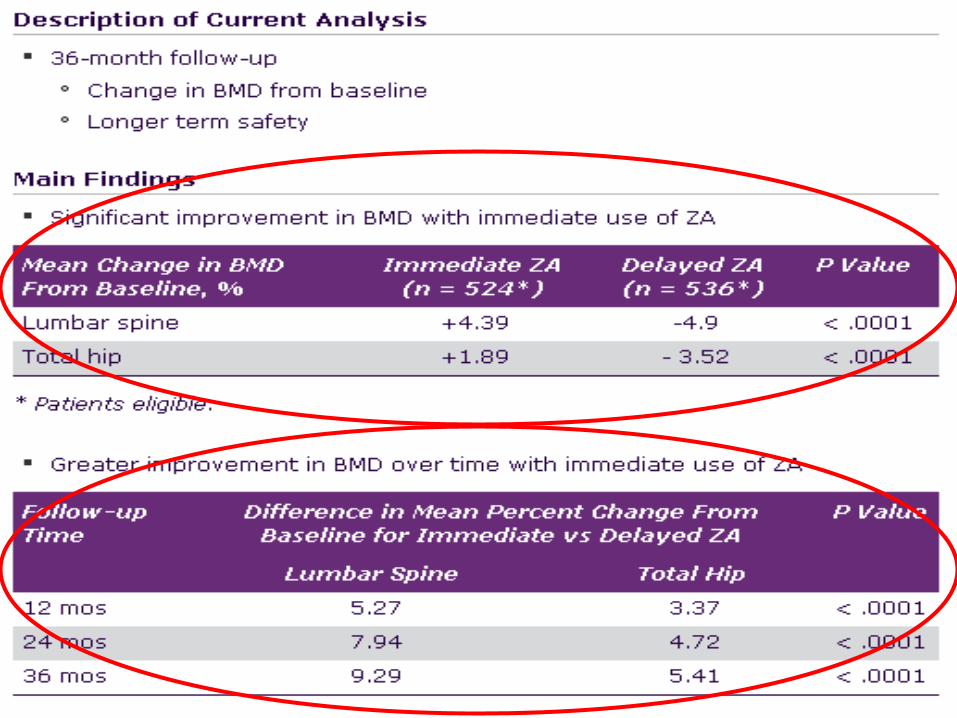
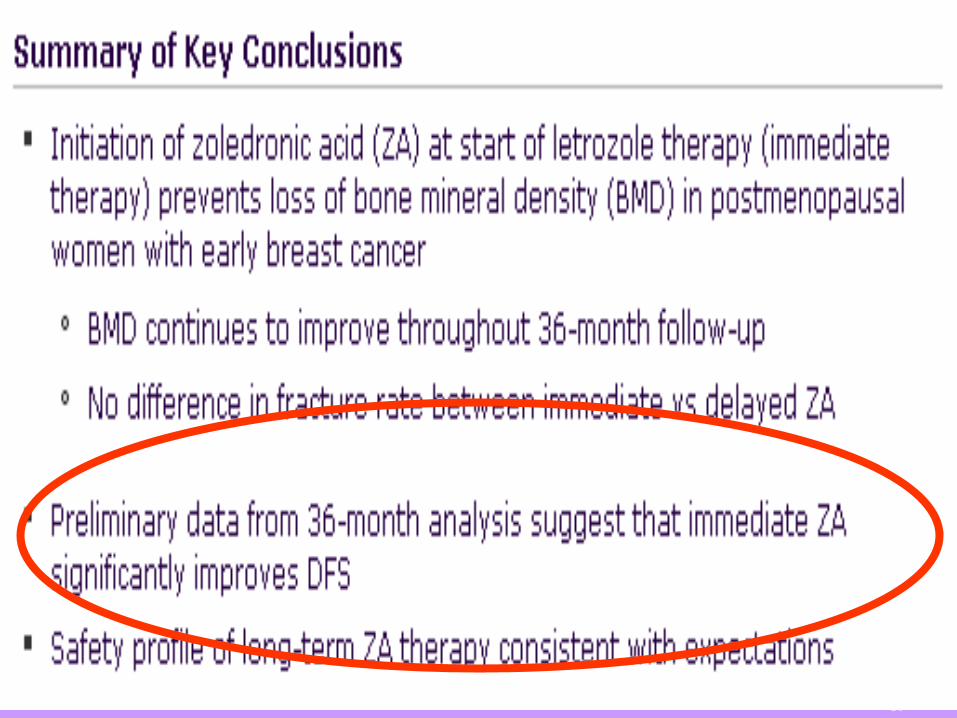
Immediate Therapy With Zoledronic Acid Prevents Bone Loss and Improves DFS in Women With Early Breast Cancer Receiving Letrozole
Zometa-Femara Adjuvant Synergy Trial (ZO-FAST): 36-month follow-up results of multicenter, randomized phase III trial[1]
…….back from S. Antonio 2008: Take home #7
“ the seed and soil theory likely to work: data
from ABCSG 12 confirmed!”
EARLYSWITCHING : 1) the new standard for the patients already on treatment with TAM from 2 or 3 yrs 2) switching from LTZ to TAM after 2-3 yrs possible if requiredLATE SWITCHING : a reasonable option for patients at the completion of 5 yrs of
TAM, namely for N pos (no news from San Antonio)
UPFRONT : the choice for the patients who have contraindications to the use of TAM. A reasonable choice for the patients at higher risk of relapse (HR score) or for whom a suboptimal response to TAM might be predicted (CYPD26) : cost/benefit to be defined in the individual patient (no S advantage on the average)
SEQUENCING : 1) no better /no worse than LTZ 2) no evidence yet in respect to TAM
AIs IN THE ADJUVANT SETTING,back from AIs IN THE ADJUVANT SETTING,back from San Antonio 2008:San Antonio 2008:
………back from S.Antonio 2008: Take home #8
“ THANK YOU! ”





























