Embed Size (px)
Citation preview

CLOFIBRATE IN INSULIN-DEPENDENT DIABETES
C. Two,mey* and A. Bloom
Departments of Medicine and Geriatrics, Whittington Hospita/, London N19.
Summary FORTY-FOUR diabetic patients main-
tained on insulin entered a double- blind crossover trial. They were given clofibrate 2 g daily for 6 weeks, either before or after a period of 6 weeks on placebo.
Clofibrate did not cause any material change in insulin requirements and there was no change in body weight. Drug tolerance was good.
The mean blood glucose was signific- antly lowered while taking clofibrate. Plasma fibrinogen and pre-beta-lipopro- tein concentrations were also signific- antly decreased following clofibrate therapy.
Introduction The use of clofibrate in hyperlipopro-
teinaemias is well established (Best and Duncan, 1963). It has been used in the treatment of exudative diabetic retino- pathy (Duncan eta[, 1968) and has been shown to suppress the ketonaemia asso- ciated with insulin dependent diabetes (Schade and Eaton, 1975). Diabetic patients, treated or untreated, have a higher incidence of lipoprotein abnorm- alities than non-diabetics (Albrink e t al, 1963).
Patients with high blood lipids fre- quently have abnormally high plasma fibrinogen levels as well. Both are low- ered following clofibrate therapy (Hart et al, 1974; Cotton and Wade, 1966). Hypertriglyceridaemia is associated with insulin resistance (Davidson and Albrink, 1965). Theoretically, therefore, a reduc- tion of blood lipids by clofibrate might decrease insulin requirements and lead to better diabetic control. This study was
undertaken in an attempt to test this hypothesis.
Patients and Methods Fifty-two insulin-dependent diabetic
patients attending the diabetic clinic at Whittington Hospital were randomly sel- ected for a double-blind crossover trial using clofibrate 2 g per day, in divided doses and a placebo, 2 capsules twice daily. These patients attended a separ- ate clinic on the same day in the early afternoon for 12 consecutive weeks. Blood samples were collected at the the same time each week. Patient com- pliance was monitored by capsule count- ing and estimation of serum clofibrate concentrations.
Forty-four patients (16 male, 28 female) completed the trial. Their ages ranged from 14 years to 78 years (mean 47 years). The duration of diabetes ranged from 3 months to 38 years (mean 12 years). The length of time on insulin ranged from 3 months to 26 years. Conventional insulin preparations were used including monocomponent insulins. Twenty patients were having insulin twice a day, 24 once daily.
At the first, seventh and final visits each patient was weighed and had blood glucose, triglyceride, cholesterol, SML lipid profile, fibrinogen and clofibrate concentrations estimated. Each patient completed a questionnaire which inclu- ded questions on diabetic control and possible side effects at these 3 visits. Furthermore, 10 of the 44 patients, ran- domly selected had, in addition to the above, serum aspartic transaminase (AST), creatine phosphokinase (CPK) and creatinine levels estimated. (Clofib-
*Present address: Cork Regional Hospital, Wilton, Cork.
31

32 IRISH JOURNAL OF MEDICAL SCIENCE
rate has been reported to cause in- creases in these enzymes in some pat- ients (Oliver, 1962; Langer and Levy, 1968)).
On the other 10 visits blood glucose only was estimated. It was estimated from venous blood using the automa- ted guaiacum glucose oxidase method (Gutteridge and Wright, 1968). Meas- urement of CPK was performed using a commercially a.yailable kit (Boer',- ringer Mannheim, 1977). The other tests were performed using standard techniq- ues (lipid profile Thorpe et al, 1967; f ibr inogen-- Stirland, 1956; clofibrate assay---Thorp, 1962; AST--Bergmeyer and Bernt, 1974; creatinine--Technicon method).
Results Twenty-one patients received clofib-
rate for the first 6 weeks, the remaining 23 received placebo first. Cumulative probability plotting showed the distribu- tion of the biochemical estima,tions to be log-normal. All values were therefore logged prior to analyses.
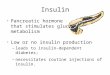
The mean blood glucose for the 44 patients over 6 weeks on clofibrate was significantly lower than when on placebo (Fig. 1). The difference in log means between the two groups corresponded to a difference of 1 mmol/I (paired t test, t = 3.37, p<0.005).
Plasma fibrinogen levels were also significantly lowered on c[ofibrate com- pared with placebo (paired t test, t = 4.81, p<0.001) (Fig. 1). The difference in log means correspond to a difference of approximately 1.04 g/I between the 2 groups.
The concentrations of M particles of the lipid profile representing pre-beta- lipoproteins were significantly lowered by clofibrate (paired t test, t = 2.42, p<0.02).
There was no significant difference in the concentrations of cholesterol, trigly- cerides, S or L particles in the 2 groups.
Fig.I MEAN PLASMA GLUCOSE & FIBRINOGEN LEVELS FOR THE 44 PATIENTS ON PLACEBO (P) & CLOFIBRATE (C)
.= .
P C P C PLASMA PLASMA GLUCOSE FIBRINOGEN (mmol/I) (mg/lOOml)
A possible relationship between initial levels of blood glucose, fibrinogen, chol- esterol, triglycerides and SML lipid par- ticles and the subsequent magnitude of fall in blood glucose after c[ofibrate ,ther- apy was examined. Simple correlation analysis showed a significant positive correlation between initial blood glucose and the subsequent fall in blood glucose (r = +0.3865, p < 0.01). There were weaker correlations with fibrinogen (+0.1684), cholesterol (-0.2932), tfigly- cerides (-0.2639), M (-0.1843) and L (-0.2861) particles, but none reached statistical significance.
The 4 lipid measurements, cholesterol, triglycerides, M and L correlated signific- antly with each other as did plasma fib- rinogen and L particles. In view of these complex inter-relationships , multiple re- gression analysis, using a step down technique, was performed to see if sev- eral of the initial test results together could improve the correlation obtained between the fall in blood glucose on clofibrate and ,the initial blood glucose alone. The analysis showed that none of the other variables gave a statistically significant improvement.

CLOFIBRATE IN INSULIN-DEPENDENT DIABETES 33
The insulin requirements of 21 patients remained the same throughout the study. Although 14 patients reduced their daily insulin dosage by at least 8 units while on clofibrate, 8 patients made a similar adjustment on placebo.
No significant change in weight occur- red in any patient. No elevation in aspar- tic transaminase or creatine phospho- kinase was observed. Serum creatinine was normal in the 10 patients on whom these enzyme tests were done.
There was no difference in the fre- quency of diabetic symptoms between those on clofibrate and those on pla- cebo. Side effects generally were re- corded most frequently before taking either capsule on the patients' first visit.
Eight patients did not complete the trial. Four withdrew for personal reasons. Three patients, on placebo, were with- drawn from the trial, 2 having been admitted to hospital, the third because of intolerance of the placebo. The re- maining patient had a severe hypogly- caemic reaction 5 days after commenc- ing clofibrate. He had completed his 6 weeks on placebo without ill effects. His diabetes had been stable for over 12 months and there was no obvious ex- planation for this attack.
Discussion The use of oral agents in addition to
insulin to produce lowering of blood glucose and of insulin requirements is not a new concept, and has been shown to occur with phenformin (Bloom and Kolbe, 1970).
CIofibrate lowered blood glucose when given to treated maturity onset diabetic patients (Barnett and Craig, 1975). This effect was demonstrated regardless of the type of antidiabetic therapy or the presence of hypertriglyceridaemia. Halo- fenate, a synthetic anti-lipaemic agent, has been shown to potentiate the hypo- glycaemic action of sulphonylureas in diabetic patients. This did not occur with clofibrate (Jain et al, 1975). More re-
cently, Ferrari and colleagues have re- ported that clofibrate improves glucose tolerance in non-diabetic patients with hypertriglyceridaemia and in previously untreated diabetic patients, with or with- out lipid abnormalities (Ferrari et al, 1977). Furthermore, the effect was de- monstrable after only one week's treat- ment. The fall in blood glucose was preceded by significant reductions in serum triglycerides. They also showed that insulin resistance, as indicated by serum immunoreactive insulin response to glucose, was significantly reduced after clofibrate.
In Miller's study on 18 patients with post-climacteric diabetes, it was possible to withhold or reduce insulin require- ments in 16 of the 18 patients following clofibrate treatment (Miller, 1963). It has already been pointed out that some of these patients, being in the adult-onset age group, may not have been truly insulin dependent. Danowski and col- leagues failed to show any' .significant effect on fasting blood glucose, glucose tolerance or 24 hour urinary glucose in 18 insulin dependent juvenile-onset dia- betics given clofibrate for 3 months (Donowski et al, 1965). Two years later, Narduzzi and colleagues reported on the effect of clofibrate on glucose tolerance in 14 juvenile-onset diabetics (Narduzzi et at, 1967). These patients had clofibrate for over 12 months. Five-hour oral gluc- ose tolerance tests were performed. Clofibrate reduced the peak hypergly- caemia at 2 and 3 hours following the glucose load.
This study has shown that clofibra.te had a statistically significant hypogly- caemic effect. Clofibrate also lowered plasma fibrinogen and pre-betalipopro- teins in the same patients. No significant correlation between the effect of clofib- rate on blood sugar and on plasma fibrinogen or blood lipids was demon- strated.
In addition to lowering plasma fibrino- gen and blood lipids, clofibrate has been

34 IRISH JOURNAL OF MEDICAL SCIENCE
shown to lower free fatty acids, plasma ketones and serum insulin levels (Schade and Eaton, 1975; Fenderson eta[ , 1974). It is not known how clofibrate exerts its effect on blood glucose. Clearly it can- not be solely the displacement of hypo- glycaemic agents from their protein bind- ing sites as occurred with halofenate (Jain eFt al, 1975), as Ferrari and col- leagues demonstrated the effect of clo- fibrate in untreated chemical diabetics, and this study has shown a definite, albeit mild, hypoglycaemic effect in in- sulin dependent diabetic patients. The role glucogon may play in the complex inter-actions is as yet unclear (Tiengo et al, 1975).
No patient developed muscle weak- ness, tenderness or raised serum creat- ine phosphokinase. The patients studied had normal renal function in marked contrast to the 5 patients reported by Pierides and colleagues (Pierides et al, 1975).
In conclusion, clofibrate has a hypo- glycaemic effect in diabetes mellitus regardless of the severity of the diabetes, but the benefits of this have yet to be determined.
We would like to acknowledge, with thanks, the help of Sister Clarke and her staff in the diabetic clinic; Dr. Joyce Bell, Royal Free Hospital, for doing the lipid profiles; Dr. T. Dormandy and his staff in the Clinical Chemistry Department, Whit- tington Hospital, for the other biochemical results; Dr. A. Hart, Medical Department, Imperial Chemi- cal Industries, for supplying the capsules, for doing the clofibrate assay and helping in some of the analyses; and Dr. H. M. Hodkinson, Hammer- smith Hospital, for assistance in the statistical analyses.
References
Albrink, M. J., Lavietes, P. H. and Man, E. 1963. Vascular disease and serum lipids in diabetes mellitus. Ann. Int, Med. 58, 305.
Anon. 1977. "Automated Analysis". Boehringer Mannheim GmbH Diagnostica. March issue.
Barnett, D. and Craig, J. G. 1975. Effect of clofibrate on glucose tolerance in maturity- onset diabetes. Proceedings of Autumn Meet- ing, British Diabetic Association.
Bergmeyer, H. U. and Bernt, E. 1974. Method of Enzymatic Analysis. New York and London. Academic Press Inc. p. 727.
Best, M. M. and Duncan, C. H. 1963. Hypogly- ceridemic effect of ethyl-oz-p-chlorophenoxyiso- butyrate with and without androsterone. Circu- lation, 28, 690.
Bloom, A. and Kolbe, R. J. 1970. Phenformin in insulin-dependent diabetics. Brit. Med. J. i, 660.
Cotton, R. C. and Wade, E. G. 1966. Further ob- servations on the effect of ethyl-(x-p-chlorophen- oxyisobutyrate and androsterone (Atromid) on plasma fibrincgen and serum cholesterol in patients with ischaemic heart disease. J. Ath- erosclerosis Res. 6, 98.
Danowski, T. S., Cohn, R. E., Limage, N. R., Novak, J. F., Saul, R., Sunder, J. H. and Moses, C. 1965. Ethylchlorophenoxyisobutyrate (CPIB) effects in juvenile-onset diabetes mellitus. Clin. Pharm. Therapeut. 6, 716.
Davidson, P. C. and Aibrink, M. J. 1965. Insulin resistance in hyperglyceridemia. Metabolism, 14, 1059.
Duncan, L. J. P., Cullen, J. F., Ireland, J. T., Nolan, J., Clarke, B. F. and Oliver, M. F. 1968. A three-year trial of Atromid therapy in exud- ative diabetic retinopathy. Diabetes, 17, 458.
Fenderson, Ralph W., Sekowski, Ignancy, Mohan, J. Chandra, Deutsch, Stanley, Benjamin, Fred and Samuel, Paul. 1974. Effect of ciofibrate on plasma glucose and serum immunoreactive insulin in patients with hyperlipoproteinemia~ Amer. J. Clin. Nutrit. 27, 22.
Ferrari, C., Frezzati, S., Romussi, M., Bertuzzoni, A., Testori, G. P., Antonini, S. and Raracchi, A. 1977. Effects of short-term clofibrate adminis- tration on glucose tolerance and insulin secre- tion in patients with chemical diabetes or hypertrigiyceridemia. Metabolism, 26, 129.
Gutteridge, J. M. C. and Wright, E. B. 1968. J. Med. Lab. Tech. 25, 385.
Hart, A., Cohen, H. and Thorp, J. M. 1974. Effect of clofibrate in lowering plasma fibrinogen and lipoproteins in diabetic patients with vascular complications. Proc. 12th Int. Congr. Internal Meal., Tel Aviv. Basel. Kanger. p. 106.
Jain, A. K., Ryan, J. R. and McMahon, F. G. 1975. Potentiation of hypoglycemic effect of sulfonyl- ureas by halofenate. New Eng. J. Med. 293, 1283.
Langer, T. and Levy, R. I. 1968. Acute muscular syndrome associated with administration of clofibrate. New Eng. J. Med. 279, 856.
Miller, R. D. 1963. Atromid in the treatment of post-climacteric diabetes. J. Athersclerosis Res. 3, 694.
Narduzzi, J. V., Danowski, T. S., Weir, T. F., Allen, R. A., Verth, J. W. and Moses, C. 1967. Laboratory indices in clofibrate therapy of juvenile-onset diabetes. Clin. Pharm. Ther. 8, 817.

CLOFIBRATE IN INSULIN-DEPENDENT DIABETES 35
Oliver, M. M. 1962. Reduction of serum-lipid and uric-acid levels by an orally active androster- one. Lancet, i, 1321.
Pierides, A. M., Alvarez-Ude, F. and Kerr, D. N. S. 1975. Clofibrate-induced muscle damage in patients with chronic renal failure. Lancet, ii, 1279.
Schade, D. S. and Eaton, R. P. 1975. Clofibrate suppression of ketonemia in insulin deficient diabetes. Diabetes, 24, Suppl. 2, 442.
Stirland, R. 1956. A rapid method of estimating fibrinogen. Lancet, i, 672.
Technicon Method, Autoanalyser, Sheet N-116. Thorp, J. M., Horsfall, G. B. and Stone, M. C.
1967. A new red-sensitive micronephelometer. Med. Biol. Eng. 5, 51.
Thorp, J. M. 1962. Experimental evaluation of an orally active combination of androsterone with ethyl chlorophenoxyisobutyrate. Lancet, i, 1323.
Tiengo, A., Muggeo, M., Assan, R., Fedde, D. and Crepaldi, G. 1975. Glucagon secretion in prim- ary endogenous hypertriglyceridemia before and after clofibrate treatment. Metabolism, 24, 901.