Embed Size (px)
Citation preview

Diabetic Retinopathy Into Practice
INTEGRATINGNEW TREATMENTS for
Jointly sponsored by The New York Eye and Ear Infirmaryand MedEdicus LLC
This continuing medical education activity is supported throughan unrestricted educational grant from Genentech, Inc.
Distributed with Ophthalmology Times
ORIGINAL RELEASE: November 15, 2012LAST REVIEW: October 15, 2012EXPIRATION: November 30, 2013
CME MONOGRAPH

Learning Method and MediumThis educational activity consists of a supplement and ten (10) study questions. The partici-pant should, in order, read the learning objectives contained at the beginning of this supple-ment, read the supplement, answer all questions in the post test, and complete theevaluation form. To receive credit for this activity, please follow the instructions provided onthe post test and evaluation form. This educational activity should take a maximum of 1.5 hours to complete.
Content SourceThis continuing medical education (CME) activity captures content from CME meetings,which took place in June and July 2012.
Activity DescriptionLaser has been the clinical standard for treating diabetic macular edema (DME) for the past25 years. However, its limitations include destruction to macular tissue, limited improve-ment, and limited effectiveness in treating advanced disease. Recently a number of clinicaltrials have suggested a role for anti-vascular endothelial growth factor (VEGF) therapies inthe management of DME. The integration of these therapies into clinical practice is underway. New data about all the anti-VEGF agents have implications for dosing, patient selection,patient monitoring, and practice management. This educational activity provides an updateon the current approaches to the management of DME.
Learning ObjectivesUpon completion of this activity, participants will be better able to:• Recognize the treatment classes of drugs for glycemic control• Describe the pathophysiology of diabetic retinopathy (DR) and DME• Describe the current and emerging treatment options for DME• Choose appropriate treatment regimens for various patients with DME• Successfully integrate new practice management procedures into their practices
Target AudienceThis activity intends to educate retina specialists, comprehensive ophthalmologists, andophthalmology practice managers.
Accreditation StatementThis activity has been planned and implemented in accordance with the Essential Areas andPolicies of the Accreditation Council for Continuing Medical Education through the jointsponsorship of The New York Eye and Ear Infirmary and MedEdicus LLC. The New YorkEye and Ear Infirmary is accredited by the ACCME to provide continuing medical education for physicians.
AMA Credit Designation StatementThe New York Eye and Ear Infirmary designates this enduring material for a maximum of 1.5 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensuratewith the extent of their participation in the activity.
Grantor StatementThis continuing medical education activity is supported through an unrestricted educationalgrant from Genentech, Inc.
2
David S. Boyer, MD (Co-Chair)Clinical ProfessorKeck School of MedicineUniversity of Southern CaliforniaLos Angeles, CaliforniaSenior PartnerRetina-Vitreous Associates Medical GroupBeverly Hills, California
David M. Brown, MD, FACS (Co-Chair)Retina Consultants of HoustonClinical Associate ProfessorThe Methodist Hospital–Weill Cornell Medical CollegeHouston, Texas
Mary Vouyiouklis, MDStaff PhysicianDepartment of Endocrinology, Diabetes and Metabolism Cleveland ClinicCleveland, Ohio
David Baczewski, MBAAdministratorIllinois Retina AssociatesDirectorIrwin Retina CenterIngalls Memorial HospitalHarvey, Illinois
Jamieson R. Holmes, CEORetina Consultants of Southwest FloridaNational Ophthalmic Research InstituteFort Myers, Florida
FACULTY Disclosure Policy StatementIt is the policy of The New York Eye and Ear Infirmary that the faculty and anyone in a posi-tion to control activity content disclose any real or apparent conflicts of interest relating tothe topics of this educational activity, and also disclose discussions of unlabeled/unap-proved uses of drugs or devices during their presentation(s). The New York Eye and EarInfirmary has established policies in place that will identify and resolve all conflicts of inter-est prior to this educational activity. Full disclosure of faculty/planner and their commercialrelationships, if any, follows.
Faculty DisclosuresDavid J. Baczewski, MBA, had a financial agreement or affiliation during the past year withthe following commercial interests in the form of Consultant/Advisory Board: Alimera Sciences; Genentech, Inc; and Regeneron Pharmaceuticals, Inc; Fees for promotional,advertising, or non-CME services received directly from commercial interests or their Agents(eg, Speakers Bureaus): Genentech, Inc.
David S. Boyer, MD, had a financial agreement or affiliation during the past year with thefollowing commercial interests in the form of Consultant/Advisory Board: Allergan, Inc;Bayer; Genentech, Inc; Novartis; and Regeneron Pharmaceuticals, Inc; Fees for promotional,advertising, or non-CME services received directly from commercial interests or their Agents(eg, Speakers Bureaus): Alcon, Inc; Allergan, Inc; and Genentech, Inc; Contracted Research:Alcon, Inc; Allergan, Inc; Genentech, Inc; Ophthotech Corporation; Quark Pharmaceuticals,Inc; and Regeneron Pharmaceuticals, Inc.
David M. Brown, MD, had a financial agreement or affiliation during the past year with the following commercial interests in the form of Honoraria: Genentech, Inc; and Regeneron Pharmaceuticals, Inc; Consultant/Advisory Board: Alimera Sciences, Allergan, Inc; Genentech,Inc; Novartis; Regeneron Pharmaceuticals, Inc; and ThromboGenics, Inc; Contracted Research:Alcon, Inc; Alimera Sciences; Allergan, Inc; Bayer; Eli Lilly and Company; Genentech, Inc; GlaxoSmithKline; Novartis; Regeneron Pharmaceuticals, Inc; and ThromboGenics, Inc.
Jamieson R. Holmes had a financial agreement or affiliation during the past year with the following commercial interests in the form of Honoraria: Genentech, Inc; Consultant/AdvisoryBoard: Genentech, Inc; Fees for promotional, advertising, or non-CME services receiveddirectly from commercial interests or their Agents (eg, Speakers Bureaus): Genentech, Inc.
Mary Vouyiouklis, MD, has no relevant commercial relationships to disclose.
Peer Review DisclosuresJohn Sorenson, MD, has no relevant commercial relationships to disclose.
Editorial Support DisclosuresTony Realini, MD, MPH; Cynthia Tornallyay, RD, MBA, CCMEP; Kimberly Corbin, CCMEP;Barbara Lyon; and Vivian Fransen, MPA, have no relevant commercial relationships to disclose.
Disclosure AttestationThe contributing faculty listed above have attested to the following:1) that the relationships/affiliations noted will not bias or otherwise influence their involve-ment in this activity; 2) that practice recommendations given relevant to the companies withwhom they have relationships/affiliations will be supported by the best available evidence or,absent evidence, will be consistent with generally accepted medical practice; and 3) that allreasonable clinical alternatives will be discussed when making practice recommendations.
Off-Label DiscussionThis educational activity includes off-label discussion of aflibercept, bevacizumab, dexamethasone implant, pegaptanib, and triamcinolone for the treatment of DME.
For Digital EditionsIf you are viewing this activity online, please ensure the computer you plan to usemeets the following requirements:
System Requirements• Operating System: Windows or Macintosh• Media Viewing Requirements: Flash Player or Adobe Reader• Supported Browsers: Microsoft Internet Explorer, Firefox, Google Chrome, Safari, and Opera• A good Internet connection
The New York Eye and Ear Infirmary Privacy & Confidentiality Policyhttp://www.nyee.edu/cme-enduring.html
CME Provider ContactFor questions about this activity call 212-979-4383
To Obtain AMA PRA Category 1 Credit™To obtain AMA PRA Category 1 Credit™ for this activity, read the material in its entirety andconsult referenced sources as necessary. We offer instant certificate processing and supportGreen CME. Please take this post test and evaluation online by going to www.MedEdicus.comand clicking the Educational Activities & Post Test Center box. Upon passing, you will receiveyour certificate immediately. You must score 70% or higher to receive credit for this activity,and may take the test up to 2 times. Upon registering and successfully completing the posttest, your certificate will be made available online and you can print it or file it. There are nofees for participating and receiving CME credit for this activity.
Alternatively, you may complete the evaluation form along with the post test answer boxwithin this supplement. Remove the Activity Evaluation page from the printed supplement orprint the Activity Evaluation page from the Digital Edition. Return via mail or fax to Kim Corbin,Director, ICME, The New York Eye and Ear Infirmary, 310 East 14th Street, New York, NY10003 or fax to (212) 353-5703. Your certificate will be mailed to the address that you pro-vide on the evaluation form. Please allow 3 weeks for mailed/faxed forms to be processed.
DisclaimerThe views and opinions expressed in this educational activity are those of the faculty and donot necessarily represent the views of The New York Eye and Ear Infirmary; MedEdicusLLC; Genentech; or Ophthalmology Times. Please refer to the official prescribing informationfor each product for discussion of approved indications, contraindications, and warnings.
This CME activity is copyrighted to MedEdicus LLC ©2012. All rights reserved.

Modern Medical Management of DiabetesMary Vouyiouklis, MD
More systemic diabetes medications are available today than everbefore in medical history. Most of these agents are relatively newand may not have been introduced yet when many clinicians now inpractice were in medical school. Table 1 summarizes these drugs byclass; both brand and generic names, as well as the mechanisms ofaction and key side effects, are listed.1
While this large selection of drugs may seem bewildering to the oph-thalmologist, the variety of drugs—which have diverse mechanisms ofaction and safety profiles—allows endocrinologists to individualizetherapy for patients with diabetes. In some cases, the potential sideeffects may be ocular in nature. For instance, pioglitazone is knownto cause macular edema in some patients.2 Clinicians would notwant to confuse a medication side effect with making a diagnosis ofdiabetic macular edema (DME) because the appropriate treatmentfor these patients would be to discontinue pioglitazone, not toadminister therapies for DME.
Maintaining open lines of communication between the ophthalmol-ogist and the endocrinologist is very important, especially whenpatients are struggling with diabetic retinopathy (DR). The ophthal-mologist should make sure the endocrinologist knows that annualeye exams are occurring, as well as the results of these examina-tions. Similarly, the endocrinologist should keep the ophthalmolo-gist informed about the adequacy of blood glucose control,hemoglobin A1c levels, compliance and nonadherence issues, andany changes in therapy for each patient. Working together, thisimportant health care team can provide each patient with the bestpossible outcomes.
The Management of DMEDavid S. Boyer, MD, and David M. Brown, MD
Pathophysiology of DMEIn simplest terms, diabetic macular edema (DME) occurs due tobreakdown of the blood-retinal barrier. Increased vascular permeabil-ity leads to expansion of the retinal extracellular space. The fluidaccumulation results in macular thickening.
The precise etiology of DME is not known, but many of the contribut-ing factors have been elucidated. Hyperglycemia, hyperlipidemia,and hypertension are all contributors to the development of DME.3-6
Vascular endothelial growth factor (VEGF) is an important driver ofthe process,7 as well as inflammation.8 Thus, both anti-VEGF mole-cules and corticosteroids are useful therapies, as will be discussed.VEGF is upregulated by both hyperglycemia and hypoxia, leading tovascular disruption and increased permeability of vascular endothe-lial cells by damaging the pericytes lining the capillaries.9,10 Thesechanges lead to increased basement membrane thickness andincreased extracellular matrix deposition,11,12 which, in turn, leads tocapillary closure and further hypoxia with more VEGF upregulationthat perpetuates a vicious cycle.
The inflammatory component involves leukocytes.8,13 Patients withdiabetes have less easily deformable leukocytes, which tend to
adhere to the vascular endothelium. This process generates superradicals and proteolytic enzymes, which lead to hypoxia, capillarynonperfusion, and upregulation of VEGF; again, this action perpetu-ates the cycle already described.
Imaging in DMEClinicians use imaging to confirm the diagnosis of macular edema,document the diagnosis, guide the therapy choices, and assess andmonitor the patient’s response to therapy. Several imaging modalitiesare available, each of which has advantages and disadvantages.14
Fundus photography is the most basic option. Clinicians can take animage of only the posterior pole or the full 7-field Early TreatmentDiabetic Retinopathy Study (ETDRS) field or perform ultrawide fieldphotography or even obtain stereoscopic images to attempt to capture the retinal thickening in DME.
Fluorescein angiography is also an important imaging modality. Clini-cians can perform standard fluoresce in angiography or ultrawide fieldangiography. The latter option can reveal more peripheral areas of cap-illary nonperfusion and capillary dropout that may play a role in increas-ing VEGF production, which may offer a potential treatment target.
Optical coherence tomography (OCT) has become an importantimaging modality for DME. The OCT platform has evolved from timedomain to spectral domain OCT, and swept-source OCT—which willprovide faster imaging at greater depths—is on the horizon. Most clinicians are using spectral domain OCT now, but it is important toremember that most of the studies that are currently shaping clinicalpractice patterns were conducted using time domain OCT.
The advantages and disadvantages of the various imaging modalitiesfor DME are provided (Table 2).
Management of DMELaserLaser photocoagulation was established as the clinical standard ofcare through a series of studies conducted in the 1980s. TheETDRS confirmed that prompt versus deferred macular grid lasertherapy showed a 50% reduction in moderate vision loss; however,very few patients gained 3 lines or more.15 This study also gave usthe classic concept of clinically significant macular edema.
Laser therapy does have disadvantages. Scotomata are common,and over time it appears that the chorioretinal scars and their atten-dant scotomata may enlarge and coalesce. Too-heavy treatment canpenetrate Bruch’s membrane and result in choroidal neovasculariza-tion. Subretinal fibrosis and subpigment epithelial membranes canalso occur, all of which can lead to a decrease in visual acuity.
New therapies have rendered laser as an adjunctive therapy for DME.The role of laser therapy in combination with pharmacotherapy forDME will be further discussed. New lasers are also being developedthat may reposition laser therapy in the current treatment algorithm.
SteroidsSteroids are effective for DME because there is an inflammatorycomponent to its pathophysiology. Numerous steroids are availablefor therapy, including triamcinolone as an injectable solution, as wellas fluocinolone acetonide and dexamethasone in implant form.
3
INTEGRATING NEW TREATMENTS for Diabetic Retinopathy Into Practice

Several studies have been conducted showing the benefit of steroidsfor DME. The Diabetic Retinopathy Clinical Research (DRCR) Net-work conducted a study comparing the outcomes of patient groupstreated with laser therapy versus 1 mg of triamcinolone versus 4 mgof triamcinolone with retreatment up to every 4 months based onprespecified criteria.16 In the short term, the 4-mg triamcinolone-treated group had the best visual recovery compared with the othergroups. Over time, however, both steroid-treated groups developedcataracts, which reduced visual acuity after 12 to 16 months, and thepatients who received laser treatment had the best long-term visualoutcome. Cataracts and glaucoma were much more common in thegroups treated with steroids than the laser-treated group, and the
lower dose of triamcinolone was associated with a better safety pro-file than the larger dose with no efficacy difference.
The dexamethasone implant was also evaluated in the eyes ofpatients with DME, but also in combination with laser treatment.17 Thecontrol group received laser treatment plus sham implantation of thedexamethasone device. Although the dexamethasone-treated grouphad better visual outcomes at several time points throughout thestudy, both groups experienced similar results at the 12-month mark.
As with laser treatment, new anti-VEGF drugs have recast steroidsinto an adjunctive therapy role. The fluocinolone implant Iluvien® wassubmitted for approval by the US Food and Drug Administration
4
Brand Name Generic Name Mechanism of Action Key Side Effects
Insulin Secretagogues
Micronase® Glyburide Stimulate the pancreas torelease more insulin right after a meal and then overmany hours
Potential for hypoglycemia
Glucotrol® Glipizide
Amaryl® Glimepride
Prandin® Repaglinide Stimulate the pancreas torelease more insulin right after a meal
Potential for hypoglycemia
Starlix® Nateglinide
Biguanides (Glucose Suppressors)
Glucophage® Metformin Reduce the amount of glucose the liver releasesbetween meals
Gas, diarrhea, nausea, abdominal painor discomfort, lactic acidosis
Glucophage® XR
Fortamet®
Glumetza®
Riomet®
α-Glucosidase InhibitorsPrecose® Acarbose Delay the absorption and
breakdown of carbohydratesfrom intestines
Gas, diarrhea, stomach upset
Glyset® Miglitol
Thiazolidinediones (Insulin Sensitizers)
Actos® Pioglitazone Make the body more sensitiveto the effects of insulin
Weight gain, fluid retention, osteopenia,increase in congestive heart failure in those at risk, macular edema. Pioglitazone only: US Food and DrugAdministration warning regarding a pos-sible association with bladder cancer.Rosiglitazone only: Possible increasedcardiovascular events in those at riskAvandia® (restricted use) Rosiglitazone
Dipeptidyl Peptidase-4 (DPP-4) Inhibitors
Januvia® Sitagliptin Improve the level of the body’sinsulin after a meal and lowerthe amount of glucose madeby the body; prolong endoge-nous GLP-1 action
Stuffy nose, sore throat, occasionaldiarrhea, stomach discomfort; rarecases of pancreatitis have beenreported
Onglyza® Saxagliptin
Tradjenta® Linagliptin
Glucagon-Like Peptide (GLP) Agonists
Byetta® Exenatide Increase insulin secretion, suppress glucagon
Weight loss, gastrointestinal symptoms,rare pancreatitis. Bydureon™ and Victoza® only: Black box warningfor C-cell hyperplasia, which was seen in rodents
Bydureon™ Exenatide once weekly
Victoza® Liraglutide
Others
Symlin® Amylin Slows gastric emptying, suppresses glucagon
Reduces postprandial glycemia, weight loss, nausea, hypoglycemia
Cycloset® Bromocryptine mesylate Reduces postprandial glucose Nausea, dizziness, fatigue
Table 1. Current systemic diabetes medications, their mechanisms of action, and key side effects.1

(FDA) as an indication for the treatment for DME but at this time hasnot been approved for DME. Another fluocinolone implant, Retisert™,is approved for the treatment of uveitis. Thus, all steroid treatment forDME is off-label use.
Anti-VEGF AgentsAnti-VEGF agents have revolutionized the management of manyimportant posterior segment diseases, from macular degeneration toretinal venous occlusive disease. The rationale for anti-VEGF therapyin DME is supported by the finding that VEGF levels are elevated inthe eyes of patients with DR. Numerous studies have evaluated thebenefits of all currently-available anti-VEGF agents: ranibizumab,bevacizumab, pegaptanib, and aflibercept. Recently, ranibizumab wasapproved for the treatment of DME; the other anti-VEGF agents areused off-label for DME.
Ranibizumab. RISE and RIDE were a pair of Phase III prospective,multicenter studies of identical design that enrolled patients with clinically significant macular edema and central retinal thickness inexcess of 275 microns based on time domain OCT.18 Patients withproliferative diabetic disease were excluded, and the primary out-come was the proportion of patients with 3 lines of visual gain at 24 months. Patients were randomized to receive either sham injec-tions or 0.3 mg of ranibizumab or 0.5 mg of ranibizumab monthly,with rescue laser therapy available to all groups starting at month 3based on prespecified criteria.
In the 2 studies, the proportion of patients achieving at least a 3-linevisual gain in the 0.3-mg ranibizumab groups was 33% to 45%. Inthe 0.5-mg ranibizumab groups, 39% to 45% of the patients madethe same gains. In contrast, the sham (laser only) group achieved a3-line gain in 12% to 18% of the patients. Both ranibizumab-treatedgroups were statistically better than the laser-treated groups andequivalent to one another. The average number of letters gained wasaround 12 letters in the ranibizumab-treated groups versus 2 to 3 let-ters in the sham (laser) group. OCT analysis corresponded to thevisual outcomes, with reductions in retinal thickness occurring asearly as 1 week after the first treatment and being maintainedthroughout the study.
From a safety perspective, the safety profile of ranibizumab in peo-ple with diabetes was very similar to what we observed in the age-related macular degeneration (AMD) trials. The observed adverseevents were quite similar between all 3 groups, although there wasa slightly higher rate of cerebrovascular accident in the 0.5-mg
ranibizumab-treated group (2%) compared tothe other 2 groups (1.2% for sham, 0.8% for0.3-mg ranibizumab) in the pooled safety analy-sis. The studies were not powered to assess thesignificance of differences in safety profilesbetween the groups. Treatment at the 0.3-mgdose of ranibizumab has recently beenapproved by the FDA for the treatment of DME.
Bevacizumab. The evidence supporting beva-cizumab for the treatment of DME is somewhatless robust than for ranibizumab. The BOLT studyenrolled 80 subjects with residual nonischemicsubfoveal clinically significant macular edemaafter at least 1 grid laser treatment.19 These sub-jects were randomized to receive either beva-cizumab injections every 6 weeks for 3 injectionsfollowed by retreatment as needed based onprespecified criteria or focal macular laser ther-apy as needed up to every 4 months. The primary endpoint was the change in vision at 12 months; 2-year data are also now available.
After 2 years of protocol-based therapy, the eyesof patients in the bevacizumab-treated group had
gained an average of 8.6 letters compared to an average loss of 0.5 letters in the laser-treated group. Interestingly, both groups expe-rienced significant reductions of central retinal thickness on timedomain OCT, but this outcome was associated with visual gains onlyin the bevacizumab-treated group. The safety profile of both groupswas similar, although with only a total of 80 patients enrolled, thisstudy was not adequately powered to evaluate safety.
Pegaptanib. A Phase III trial of pegaptanib for DME was conductedin the eyes of patients with center-involving edema that was inexcess of 250 microns thick and experienced visual acuity between20/50 and 20/200.20 Subjects were randomized to receive either0.3-mg pegaptanib injections or sham injections every 6 weeks, withrescue laser therapy available at week 18 based on prespecified cri-teria; in year 2, both groups switched to only injections as neededbased on prespecified retreatment criteria. The primary outcomemeasure was the proportion of eyes gaining 10 or more letters ofacuity at 12 months; 2-year data are now available.
At 12 months, 37% of the pegaptanib-treated eyes and 20% of theeyes in the sham group had gained 10+ letters. Visual gains wereapparent by the first 6 weeks and remained stable throughout thestudy, with the pegaptanib-treated group gaining an average of 6.1 letters versus 1.3 letters in the sham group. No safety issueswere noted in either group.
Aflibercept. VEGF Trap-Eye has been evaluated in 1 Phase II trialcalled DA VINCI; another Phase III trial called VISTA is now underway. DA VINCI was a randomized, multicenter, double-masked trial inpatients with clinically significant center-involving macular edemaexceeding 250 microns on time domain OCT whose acuity wasbetween 20/40 and 20/320.21 With a total of 5 arms, this study had4 arms with various dosing regimens of aflibercept: 0.5 mg adminis-tered every 4 weeks, 2 mg administered every 4 weeks, 2 mgadministered every 8 weeks, and 2 mg administered as needed asoften on a monthly basis according to prespecified retreatment crite-ria; all patients received 3 monthly loading doses at the start. Thecontrol group received macular laser therapy up to every 4 months.The primary endpoint was the mean change in acuity at 24 weeks;52-week data are also available.
In all 4 aflibercept-treated arms of this study, visual acuity improvedimmediately and quite similarly between groups. At 24 and 52 weeks,gains in the aflibercept-treated groups were in the range of 10 to 12 letters, compared to a mean loss of approximately 1 letter in thelaser-treated group. Central retinal thickness also began to improve
5
Modality Advantages Disadvantages
Fundus photography • Readily available• Easy to perform• Documents disease status• May reveal clinically inapparent lesions (especially microaneurysms)
• Does not reveal all relevantanatomy• No perfusion information• Of limited use if dense cataract or media opacities are present
Fluorescein angiography • Readily available• Identifies ischemia, leakage,and proliferative retinopathy
• Relatively invasive• Not diagnostic of clinically significant macular edema
Ultrawide field angiography
• May detect peripheral nonperfusion
• Unclear if treating the peripheryimproves outcomes• Relatively invasive
Optical coherencetomography
• Reveals the presence orabsence of center-involvingedema• Useful for assessingresponse to treatment
• May not correlate with clinically significant macular edema• Platform development has outpaced major clinical trialsmethodology
Table 2. Advantages and disadvantages of the various imaging modalities used in evaluating DME.

immediately and correlated with the observed acuity gains. The safetyprofile of aflibercept was consistent with other anti-VEGF agents.
Similar to study findings on AMD, these results with anti-VEGF ther-apy represent such a vast improvement over the current standard ofcare—laser and steroids—that we are in the midst of a new paradigmshift. Anti-VEGF therapy offers not only stabilization of vision but alsoa favorable opportunity for significant visual gains for most patients.As new drugs enter the marketplace, clinical practice patterns arestill being optimized. Future head-to-head studies will clarify the opti-mal drugs, doses, and dosing frequencies for DME treatment. Animportant upcoming study coordinated by the DRCR Network is protocol T, in which 3 of the anti-VEGF agents—ranibizumab, beva-cizumab, and aflibercept—will be compared on a head-to-head basisin a DME study.
The Safety of Anti-VEGF TherapyTwo major trials focusing on patients with AMD—CATT and IVAN—found some safety signals. In the IVAN trial, bevacizumab was foundto suppress systemic VEGF much more than ranibizumab.22 In CATT,more systemic adverse events requiring hospitalization were found inthe bevacizumab-treated groups compared to the ranibizumab-treated groups.23 Yet these were more common in the administer asneeded group than in the scheduled monthly dose group, whichmakes causality difficult to understand given that the administer asneeded group had lower drug exposure. In addition, these eventswere scattered throughout the various organ systems. Furthermore,this finding was not confirmed in systemic cancer trials in whichmuch higher doses of bevacizumab were given.
It might be hypothesized that anti-VEGF therapy would have moresafety signals in people with diabetes than in patients with maculardegeneration because people with diabetes are more vasculopathicand may be more susceptible to the consequences of VEGF sup-pression. However, no significant safety signals were reported withthe anti-VEGF agents in these DME trials. In the absence of a plausi-ble biologic mechanism by which anti-VEGF therapy could producesystemic safety issues, it is reasonable to conclude that they are safefor use in patients with retinal vascular disease.
Combination TherapyAs the studies described conclusively demonstrate, anti-VEGF ther-apy has driven a paradigm shift in the management of DME. But aseach study also shows, not every patient achieves an adequateresponse to anti-VEGF monotherapy. Laser and steroids may nolonger be the first-line treatment in the new paradigm, but they stillhave an important place in the comprehensive management of DME.
Numerous studies have explored the additivity of steroids and laser toanti-VEGF therapy, with the goals of either improving visual acuity orreducing the frequency of injections. Most of these studies were relatively small, but despite their shortcomings they can guide theselection of combination therapy. It is important to realize that all randomized controlled trials had eliminated patients who may haveresponded to previous laser treatment. Laser treatment still plays arole in the treatment of DME although the timing has to be elucidated.
The DRCR Network conducted a trial of nearly 800 eyes of patientswith DME involving the foveal center in excess of 250 microns on timedomain OCT.24 Subjects were randomized to 1 of 4 groups: 0.5 mg ofranibizumab plus prompt laser (within 1 week), 0.5 mg of ranibizumabplus deferred laser (performed at 24 weeks), 4 mg of intravitreal triam-cinolone, or sham injection plus prompt laser. All groups received 4 monthly injections as a loading dose; subsequent injections weregiven as needed based on prespecified retreatment criteria.
At 52 weeks, the 2 ranibizumab-treated groups had produced similarmean acuity gains—on the order of 9 letters—while the steroid-treatedand sham groups were essentially equal with 3-letter gains. After ayear, no incremental benefit was found for prompt laser in conjunc-tion with ranibizumab treatment. In fact, in the deferred laser group,
72% of the patients never needed a single laser treatment, and 20%of the patients received a single laser treatment. Another importantcaveat is that the relatively poor outcomes in the triamcinolone-treated group are likely attributable to cataract formation; 60% ofphakic patients needed cataract surgery, compared to 14% in theother groups. In a subset of pseudophakic eyes, the triamcinolone-treated group did almost as well as the 2 ranibizumab-treated groups.Glaucoma was also common in the steroid-treated group, with 28%of the patients needing glaucoma medications but only 1% of thepatients needing glaucoma surgery. Given that cataracts are easy toaddress and glaucoma medications are generally well tolerated, theseissues should not be a reason to avoid triamcinolone, especially in apatient who seems to respond poorly to anti-VEGF therapy.
The RESTORE trial also evaluated the combination of ranibizumaband laser as effective DME treatment. RESTORE was a Phase III trial—randomized, multicenter, and double-masked—that enrolled patientswith DME and randomized them to 1 of 3 treatment groups: 0.5 mgof ranibizumab plus laser; ranibizumab with sham laser; and shamranibizumab plus laser.25 In all cases, ranibizumab or sham injectionwas administered every month for 3 months and then as neededbased on prespecified retreatment criteria; laser or sham laser wasalso performed at baseline and then up to every 3 months asneeded beginning in month 3.
By month 12, both ranibizumab-treated groups (with and withoutlaser) had the same mean gains in visual acuity—approximately 6.5 letters in each group—while the laser only group had gainedabout 1 letter on average. All 3 groups had equal average numbersfor active or sham injections and active or sham laser treatments.Anatomic outcomes correlated with the acuity outcomes with nosafety differences between groups.
Both of these combination studies support the paradigm changetoward pharmacotherapy for DME. Adding laser or steroids toranibizumab did not improve visual acuity or anatomic outcomes inthese 2 studies. Given the potential side effects of these 2 adjunctivetherapies, the paradigm that is best supported by the data is initialmonotherapy. Anti-VEGF monotherapy is safer than steroidmonotherapy due to the relatively high risk of cataracts and glau-coma with steroid monotherapy. Only patients who respond poorly toanti-VEGF monotherapy should be considered candidates for steroidmonotherapy or combination therapy.
Practice Management Pearls for DMEDavid Baczewski, MBA, and Jamieson Holmes
The logistics of DME management touch many aspects of clinicalpractice. Among these considerations are the management of druginventory, storage of drugs, and patient education to ensure optimalclinical outcomes.
The most common method of anti-VEGF drug management in theprivate practice setting is the buy and bill model. Clinicians buy drugsdirectly from the manufacturer or pharmacy supply, and then clini-cians bill the patients when they use the drugs. However, thismethod involves risk. The drugs can be expensive, and once clini-cians buy them, they either use the drugs, bill for them, and collectthe fee or they accept the loss. Each practice needs a key personmanaging drug inventory; this person ensures that an adequate sup-ply of drugs is always on hand to avoid being caught short whilemaking sure an excess of drugs will not lead to having drugs that willexpire before being used.
Some insurance companies do not allow the clinician to bill for thesedrugs. The drugs must come from a pharmacy, commonly referred toas a specialty pharmacy. Specialty pharmacies may require a patientcopay that is separate from any office-based examinations and pro-cedures. This requirement can complicate patient care because nowthe patient must be made aware of their financial obligations at boththe specialty pharmacy and the medical practice. Falling behind on
6

either obligation may disincentivize the patient to follow his or hertreatment plan. It is important to note that most manufacturers ofanti-VEGF therapies for AMD have patient assistance programs tohelp individuals who otherwise cannot afford the cost of treatment.Awareness of these programs and their criteria can help ensure thatall patients obtain the appropriate therapy regardless of their abilityto pay for it.
Once any drug arrives at the practice, it must be inspected to insureits acceptable condition, then stored properly. Drugs that requirerefrigeration should not sit on the countertop for several hours. Forthis reason, the person responsible for managing the drug inventorywithin the practice should be clearly identified and well trained.
Many practices store drugs in a small college dorm-style refrigerator,the type one can buy inexpensively at a shopping warehouse. How-ever, this may not be adequate for maintaining the quality of thedrugs. Temperature fluctuations can occur with these refrigerators.Clinicians have switched to medical grade refrigerators and freezersto address this concern. These refrigerators and freezers are sepa-rate, not combined units with a small freezer compartment in the cor-ner of the refrigerator. In combined units, any drugs stored too closelyto the freezer compartment could still freeze. Medical grade refrigera-tors have thicker walls and no storage space in the doors, where ittends to be too warm. They have built-in temperature monitors thatare located in places that are relatively insensitive to the opening andclosing of the door, resulting in improved temperature stability.
If clinicians have multiple offices and/or high volumes and keep largequantities of drugs on hand, they are susceptible to substantiallosses in the event of power outages. It is important to monitor thepower grid where practices are located. In the event of a power out-age, clinicians can arrange to immediately send people to the officeto retrieve the drugs, place them into coolers, and move them toanother satellite office or to a hospital, which has more reliablebackup power and is less susceptible to power outages.
The coding sequence for billing is very important and may varybased upon the region of the country or insurance company. It isimportant to monitor claims for the best coding in one’s area.
For example, in one region, the preferred sequence when treatingthe eye of a patient with DME is to select the DME code (362.07)first followed by the Specificity or Severity code for PDR, mild, mod-erate, or severe diabetic retinopathy (362.02 – 362.06), and finallythe Manifestation code (250.50). In another region, the preferredsequence is to use the Manifestation code (250.50) first followed bythe DME code (362.07) and then the Specificity or Severity codes(362.02 – 362.06). Follow the payer’s preferred sequence and mon-itor claims for prompt and correct payment. .
The importance of patient satisfaction in ensuring optimal clinical out-comes cannot be overemphasized. New patients typically becomeinformed about the nature of their disease and their treatment plan;they are motivated and satisfied when they initiate therapy. Ongoingeducation is equally important to maintain an understanding of theirclinical course and their motivation to continue follow-up as sched-uled. A large component of patient satisfaction is expectations man-agement. Patients must understand what the reasonable clinicaloutcome should be. They should anticipate a long series of visits,each with testing that will likely include OCT imaging; many patientswill require an intravitreal injection. Patients need to be informedabout the consequences of nonadherence with follow-up. Further-more, it is important for them to understand the financial aspects oftherapy at the outset so that bills do not disincentivize their follow-upcare. It is human nature to become unsatisfied with processes thatare long and drawn out, which is often the case in managing DME.
Education is linked to patient satisfaction. Education is a process, notan event. In our experience, explaining the medical and financial
processes, as well as the rationale, to patients at the outset of therapydoes not mean that they comprehend all of the details at first men-tion, or even remember everything 6 months later. Optimizing patientsatisfaction requires ongoing education and follow-up. It is importantto remind patients how much better they are seeing now than beforetreatment. It is also important to remind them that the drugs onlywork for 1 or 2 months at a time. Furthermore, it is important toremind patients that if they do not return for follow-up care, the visualgains they have made can be lost. These steps will help them to stayengaged in the process.
Patient CasesDavid S. Boyer, MD, and David M. Brown, MD
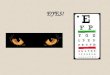
Case 1A 63-year-old male with type 2 diabetes mellitus whose baselinevisual acuities were 20/40 and 20/32 in the right and left eyes,respectively, and had been stable for 6 months presents for evalua-tion and treatment. When he had some issues with blood glucosecontrol, his endocrinologist made some medication adjustments.Shortly thereafter, he returned with significantly reduced visual acuitylasting 4 weeks. His OCT reveals bilateral macular edema (Figure 1).Therapeutic options include anti-VEGF therapy or focal macular laser.Before either of these treatments was undertaken, we carefullyreviewed his medication list and discovered that when the endocri-nologist adjusted his systemic diabetes medications, pioglitazonewas added. After communicating with the endocrinologist, pioglita-zone was stopped and the edema was resolved. This patientregained his 20/40 and 20/32 vision, which matched his visual acuity before he started taking pioglitazone.
7
Case 1: OCT of thepatient’s decreasedvision lasting 4 weeksafter pioglitazone therapystarted (OD 20/60, OS 20/40)
A
B
Figure 1. (A and B) Optical coherence tomography of right and left eyes of thepatient described in Case 1, showing bilateral macular edema; (C and D) thispatient’s eyes 6 weeks after discontinuing pioglitazone.
Photos Courtesy of David M. Brown, MD
Case 1: OCT of thepatient’s vision 6 weeksafter pioglitazone discontinued (OD 20/40,OS 20/32)
C
D

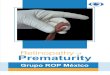
Case 2A 60-year-old male has background DR in both eyes and focal DMEin his left eye. He has had a few focal laser treatments in the past.His uncorrected vision is 20/40 in the left eye and pin holes at20/25. As noted in his OCT (Figure 2A), he has some mild leakage,but it is very close to the fovea. It is likely attributable to a singlemicroaneurysm. Treatment options include focal laser or anti-VEGFtherapy. It would likely only take 1 shot with the laser, but the clini-cian must be steady and the patient must stay very still because ofthe proximity to the fovea. This patient underwent focal laser therapy.The posttreatment OCT (Figure 2B) clearly shows significant resolu-tion of the edema, and the patient’s vision remained stable.
Case 3A 58-year-old female has PDR in the right eye and nonproliferativeretinopathy in the left eye. Her left eye has had a single prior focallaser treatment; she was subsequently enrolled in a trial for DMEusing high-dose ranibizumab. Her visual acuity in the left eye is20/40. Her posterior pole reveals multiple cotton wool spots andhemorrhages as well as DME in an ultrawide field fundus photograph(Figure 3). OCT confirms significant DME (Figure 4). Several treat-ment options are available. Because there is so much visible leakage,initial laser is reasonable to consider. Alternatively, a series of 3 monthly anti-VEGF treatments would also be reasonable. At anypoint after either of these selections, one could add the other therapy if the response is suboptimal. For this patient we opted forcombination treatment with anti-VEGF therapy plus laser treatment.We prefer to give the anti-VEGF agent first to help dry out the maculaso that lower laser energy can be used for the subsequent lasertreatment. She received an anti-VEGF injection, followed 6 weekslater by macular laser therapy, and she continues to do well withongoing anti-VEGF injections.
Case 4A 71-year-old female has glaucoma in both eyes. She also has PDRand clinically significant macular edema in the left eye. She has previ-ously had both panretinal photocoagulation and focal macular laser aswell as 3 bevacizumab injections—all to the left eye. Her fluoresceinangiogram reveals both mild macular edema and some leaky neovas-cularization along the inferonasal arcade (Figure 5). In this case, weelected to add some focal laser in the area of the neovascularizationand also restarted anti-VEGF therapy. Anti-VEGF therapy alone wouldtreat both the macular edema and regress the proliferative retinopathy.But the neovascularization will continue to recur because there isischemia in that area driving the process. We would need to adminis-ter injections on an ongoing basis to keep the VEGF coming from thatischemic tissue suppressed. Laser therapy to address the neovascular-ization will allow us to use an as-needed retreatment schedule with theanti-VEGF agent for the macular edema.
Case 5A 71-year-old female has glaucoma, clinically significant macularedema, vitreomacular traction, and an epiretinal membrane in theright eye (Figure 6). She has previously received bevacizumab, pan-retinal photocoagulation, and 2 focal laser treatments. Options hereinclude anti-VEGF therapy or a vitrectomy. One point worth making is that once the clinician performs a vitrectomy in an eye like this,anti-VEGF agents will not be as efficacious as before because ofincreased vitreous clearance following vitrectomy.
8
A
Figure 2. (A) Optical coherence tomography of the patient described in Case2, showing macular edema near the foveal center; (B) this patient’s same eyeafter focal macular laser therapy.
Photos Courtesy of David M. Brown, MD
B
Figure 3. Ultrawide fieldfundus photograph of thepatient in Case 3 showsdiffuse DME.
Photo Courtesy of David M. Brown, MD
Figure 4. Optical coherence tomography of the patient in Case 3 showsdiffuse macular edema.
Photo Courtesy of David M. Brown, MD
Figure 6. Optical coherence tomography of the patient in Case 5 showsmacular edema and vitreomacular traction.
Photo Courtesy of David M. Brown, MD
Figure 5. Fluoresceinangiogram of thepatient in Case 4shows DME.
Photo Courtesy ofDavid M. Brown, MD

References1. Standards of medical care in diabetes—2012. Diabetes Care.2012;35(suppl 1):S11-63.
2. Ryan EH, Jr, Han DP, Ramsay RC, et al. Diabetic macular edemaassociated with glitazone use. Retina. 2006;26:562-570.
3. Chew EY, Klein ML, Ferris FL, 3rd, et al. Association of elevatedserum lipid levels with retinal hard exudate in diabetic retinopa-thy. Early Treatment Diabetic Retinopathy Study (ETDRS) Report22. Arch Ophthalmol. 1996;114:1079-1084.
4. Klein R, Klein BE, Moss SE, Cruickshanks KJ. The Wisconsin Epidemiologic Study of Diabetic Retinopathy: XVII. The 14-yearincidence and progression of diabetic retinopathy and associatedrisk factors in type 1 diabetes. Ophthalmology. 1998;105:1801-1815.
5. Vitale S, Maguire MG, Murphy RP, et al. Clinically significant macular edema in type I diabetes. Incidence and risk factors.Ophthalmology. 1995;102:1170-1176.
6. Klein R, Klein BE, Moss SE, Davis MD, DeMets DL. Glycosylatedhemoglobin predicts the incidence and progression of diabeticretinopathy. JAMA. 1988;260:2864-2871.
7. Nguyen QD, Tatlipinar S, Shah SM, et al. Vascular endothelialgrowth factor is a critical stimulus for diabetic macular edema.Am J Ophthalmol. 2006;142:961-969.
8. Miyamoto K, Ogura Y. Pathogenetic potential of leukocytes in diabetic retinopathy. Semin Ophthalmol. 1999;14:233-239.
9. Ciulla TA, Harris A, Latkany P, et al. Ocular perfusion abnormali-ties in diabetes. Acta Ophthalmol Scand. 2002;80:468-477.
10. Ansari NH, Zhang W, Fulep E, Mansour A. Prevention of pericyteloss by trolox in diabetic rat retina. J Toxicol Environ Health A.1998;54:467-475.
11. Mogensen CE, Osterby R, Gundersen HJ. Early functional andmorphologic vascular renal consequences of the diabetic state.Diabetologia. 1979;17:71-76.
12. Koya D, King GL. Protein kinase C activation and the develop-ment of diabetic complications. Diabetes. 1998;47:859-866.
13. Stewart MW. Corticosteroid use for diabetic macular edema: oldfad or new trend? Curr Diab Rep. 2012;12:364-375.
14. American Academy of Ophthalmology Retina Panel. PreferredPractice Pattern Guidelines. Diabetic Retinopathy. San Francisco,CA: American Academy of Ophthalmology; 2008.http://www.aao.org/ppp. Accessed September 24, 2012.
15. Early Treatment Diabetic Retinopathy Study research group. Photocoagulation for diabetic macular edema. Early TreatmentDiabetic Retinopathy Study report number 1. Arch Ophthalmol.1985;103:1796-1806.
16. Beck RW, Edwards AR, Aiello LP, et al. Three-year follow-up of arandomized trial comparing focal/grid photocoagulation andintravitreal triamcinolone for diabetic macular edema. Arch Ophthalmol. 2009;127:245-251.
17. Callanan D, Gupta S, Giulla TA, et al. Efficacy and safety of combi-nation therapy with dexamethasone intravitreal implant (DEXimplant) plus laser photocoagulation versus monotherapy withlaser for treatment of diffuse diabetic macular edema (DDME).Paper presented at: American Academy of Ophthalmology 2010Retina Subspecialty Meeting; October 16, 2012; Chicago, IL.
18. Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for dia-betic macular edema: results from 2 phase III randomized trials:RISE and RIDE. Ophthalmology. 2012;119:789-801.
19. Michaelides M, Kaines A, Hamilton RD, et al. A prospective ran-domized trial of intravitreal bevacizumab or laser therapy in themanagement of diabetic macular edema (BOLT study) 12-monthdata: report 2. Ophthalmology. 2010;117:1078-1086 e2.
20. Sultan MB, Zhou D, Loftus J, Dombi T, Ice KS. A phase 2/3, multi-center, randomized, double-masked, 2-year trial of pegaptanibsodium for the treatment of diabetic macular edema. Ophthalmology. 2011;118:1107-1118.
21. Do DV, Nguyen QD, Boyer D, et al. One-year outcomes of theDA VINCI study of VEGF Trap-Eye in eyes with diabetic macularedema. Ophthalmology. 2012;119:1658-1665.
22. Chakravarthy U, Harding SP, Rogers CA, et al. Ranibizumab versus bevacizumab to treat neovascular age-related maculardegeneration: one-year findings from the IVAN randomized trial.Ophthalmology. 2012;119:1399-1411.
23. Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ.Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364:1897-1908.
24. Elman MJ, Aiello LP, Beck RW, et al. Randomized trial evaluatingranibizumab plus prompt or deferred laser or triamcinolone plusprompt laser for diabetic macular edema. Ophthalmology.2010;117:1064-1077 e35.
25. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTOREstudy: ranibizumab monotherapy or combined with laser versuslaser monotherapy for diabetic macular edema. Ophthalmology.2011;118:615-625.
9
Acronyms of Studies Evaluating Anti-VEGF Therapy for Posterior Segment Conditions
BOLT A Prospective Randomized Trial of Intravitreal Bevacizumab or Laser Therapy in the Management of Diabetic Macular Edema19
CATT Comparison of Age-Related Macular Degeneration Treatment Trials23
DA VINCI Diabetic Macular Edema and VEGF Trap-Eye: Investigation of Clinical Impact21
IVAN A Randomized Controlled Trial of Alternative Treatments to Inhibit VEGF in Patients with Age-Related Choroidal Neovascularization22
RESTORE A Randomized, Double-masked, Multicenter, Laser-controlled Phase III Study Assessing the Efficacy and Safety of Ranibizumab (Intravitreal Injections) as Adjunctive and Mono-therapy in Patients With Visual Impairment Due to Diabetic Macular Edema25
RIDE A Phase III, Double-Masked, Multicenter, Randomized, Sham Injection-Controlled Study of the Efficacy and Safety of Ranibizumab Injection in Subjects With Clinically Significant Macular Edema With Center Involvement Secondary to Diabetes Mellitus18
RISE A Phase III, Double-Masked, Multicenter, Randomized, Sham Injection-Controlled Study of the Efficacy and Safety of Ranibizumab Injection in Subjects With Clinically Significant Macular Edema With Center Involvement Secondary to Diabetes Mellitus18
VISTA VEGF Trap-Eye: Investigation of Safety, Treatment Effect, and Anatomic Outcomes in Diabetic Macular Edema

1. Which of the following systemic diabetes medications can beassociated with macular edema?a. Glipizideb. Metforminc. Pioglitazoned. Liraglutide
2. Which of the following is not a known contributor to the pathophysiology of DME?a. Hyperglycemiab. Hyperalbuminemiac. Hyperlipidemiad. Hypertension
3. Which of the following is a disadvantage of fundus photography?a. It is readily availableb. It documents disease statusc. It provides no perfusion informationd. It poses a high risk of complications
4. Which of the following is true regarding optical coherence tomography (OCT)?a. OCT does not reveal if the patient’s edema involves thefoveal center
b. OCT is useful for assessing the patient’s response to treatment
c. The edema visualized by OCT often correlates with thedegree of vision loss
d. The results of studies using time domain OCT can be directlyapplied to clinical practice using spectral domain OCT
5. Which of the following is false regarding laser therapy for DME?a. Laser therapy halves the risk of losing 2+ lines of visionb. Most people gain 3 or more lines of vision after laserc. Scotomata are common complications of laser therapy for DME
d. Primary laser therapy for DME remains the gold standard for most patients
6. Which of the following is true regarding steroid therapy for DME?a. Intravitreal triamcinolone at a dose of 4 mg is less effectivethan laser therapy in restoring short-term visual acuity
b. Cataracts are rare in eyes treated with intravitreal steroidsc. Glaucoma is common following intravitreal steroid therapyd. Steroids are superior to anti-VEGF agents in restoring visual acuity
7. Which of the following is true regarding the RISE and RIDE PhaseIII trials evaluating ranibizumab for DME?a. The control group received intravitreal steroid injectionsb. Fewer than 25% of the patients receiving ranibizumabgained 3+ lines of vision
c. Both the 0.3 mg and 0.5 mg doses of ranibizumab producedsuperior visual outcomes for the control group
d. None of the above is true
8. Which of the following is false regarding the DA VINCI trial ofaflibercept for DME?a. The control group received intravitreal bevacizumabb. Visual acuity slowly improved after several months of aflibercept therapy
c. Central retinal thickness remained unchanged from baselinein the aflibercept treatment groups
d. All of the above are false
9. Which of the following is true regarding combination therapy for DME?a. Laser therapy should be the first-line therapy for mostpatients
b. Use of anti-VEGF therapy can reduce the frequency withwhich laser must be performed
c. If combination therapy is warranted, both treatments shouldbe administered simultaneously
d. Patients who achieve rapid vision gains on anti-VEGFmonotherapy should then receive steroids to further increase vision gains
10. The preferred billing coding sequence for DME treatment is:a. DME, specificity, manifestationb. DME, specificityc. Manifestation, specificity, DMEd. Depends on your region
10
We offer instant certificate processing and support Green CME. Please take this post test and evaluation online by going to www.MedEdicus.com and clicking the Educational Activities & Post TestCenter box. Upon registering and successfully completing the post test, your certificate will be madeavailable online and you can print it or file it immediately. Alternatively, you may complete and submitthe ACTIVITY EVALUATION/CREDIT REQUEST on the next page.
CME POST TEST

To receive AMA PRA Category 1 Credit™, you must complete this Evaluation form and the Post Test. Record your answers to the Post Test in the Answer Boxlocated below. Mail or Fax this completed page to The New York Eye and Ear Infirmary–ICME, 310 East 14th Street, New York, NY 10003 (Fax: 212-353-5703).Your comments help us to determine the extent to which this educational activity has met its stated objectives, assess future educational needs, and create timelyand pertinent future activities. Please provide all the requested information below. This ensures that your certificate is filled out correctly and is mailed to the properaddress. It also enables us to contact you about future CME activities. Please print clearly or type. Illegible submissions cannot be processed.
PARTICIPANT INFORMATION (Please Print) � Home � Office
Last Name _____________________________________________________________________ First Name ________________________________________
Specialty ____________________________________________ Degree � MD � DO � PharmD � RPh � NP � RN � PA � Other ____________
Institution _________________________________________________________________________________________________________________________
Street Address ____________________________________________________________________________________________________________________
City ________________________________________ State _____________________ ZIP Code ____________________ Country ______________________
E-mail ______________________________________ Phone ______________________________________ Fax _____________________________________
Please note: We do not sell or share e-mail addresses. They are used strictly for conducting post-activity follow-up surveys that are required by the Accreditation Council for Continuing Medical Education (ACCME).
Learner Disclosure: To ensure compliance with the US Centers for Medicare and Medicaid Services regarding gifts to physicians, The New York Eye and EarInfirmary Institute for CME requires that you disclose whether or not you have any financial, referral, and/or other relationship with our institution. CME certificatescannot be awarded unless you answer this question. For additional information, please call NYEE ICME at 212-979-4383. Thank you.
�Yes � No I and/or my family member have a financial relationship with The New York Eye and Ear Infirmary and/or refer Medicare/Medicaid patients to it.
o I certify that I have participated in the entire activity and claim 1.5 AMA PRA Category 1 Credits™.
Signature Required __________________________________________________________________ Date Completed ______________________________
OUTCOMES MEASUREMENT
�Yes � No Did you perceive any commercial bias in any part of this activity? IMPORTANT! If you answered “Yes,” we urge you to be specific about where the bias occurred so we can address the perceived bias with the contributor and/or in the subject matter in future activities.
_________________________________________________________________________________________________________________________________
Circle the number that best reflects your opinion on the degree to which the following learning objectives were met:5 = Strongly Agree 4 = Agree 3 = Neutral 2 = Disagree 1 = Strongly Disagree
Upon completion of this activity, I am better able to:
• Recognize the treatment classes of drugs for glycemic control 5 4 3 2 1
• Describe the pathophysiology of diabetic retinopathy (DR) and diabetic macular edema (DME) 5 4 3 2 1
• Describe the current and emerging treatment options for DME 5 4 3 2 1
• Choose appropriate treatment regimens for various patients with DME 5 4 3 2 1
• Successfully integrate new practice management procedures into my practice 5 4 3 2 1
1. Please list one or more things, if any, you learned from participating in this educational activity that you did not already know. ____________________________
_________________________________________________________________________________________________________________________________
2. As a result of the knowledge gained in this educational activity, how likely are you to implement changes in your practice?4=definitely will implement changes 3=likely will implement changes 2=likely will not implement any changes 1=definitely will not make any changes
5 4 3 2 1
Please describe the change(s) you plan to make: __________________________________________________________________________________________
_________________________________________________________________________________________________________________________________
3. Related to what you learned in this activity, what barriers to implementing these changes or achieving better patient outcomes do you face?_________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________
4. Please check the Core Competencies (as defined by the Accreditation Council for Graduate Medical Education) that were enhanced for you through participationin this activity. � Patient Care � Practice-Based Learning and Improvement � Professionalism
� Medical Knowledge � Interpersonal and Communication Skills � Systems-Based Practice
5. What other topics would you like to see covered in future CME programs? ___________________________________________________________________________
_________________________________________________________________________________________________________________________________
ADDITIONAL COMMENTS __________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________
ACTIVITY EVALUATION/CREDIT REQUEST
ORIGINAL RELEASE: November 15, 2012LAST REVIEW: October 15, 2012
EXPIRATION: November 30, 2013
1 2 3 4 5 6 7 8 9 10
POST TEST ANSWER BOX
INTEGRATING NEW TREATMENTS for Diabetic Retinopathy Into Practice

INTEGRATING NEW TREATMENTS for Diabetic Retinopathy Into Practice