Embed Size (px)
Citation preview

Co-creating Health Systems
WHO Geneva, May 2006
Dr Shaun Conway
Sharon White

Expectations
1. Explore the potential of Co-creation as an innovative approach to strengthening health systems
2. Advocate for Human Scale Development in pursuing development goals & poverty reduction
3. Present our PPM project (under development) as an example to apply these concepts and focus the discussion
4. Identify lessons for improving our work

Problems with traditional services
Providers - resist centrally derived targets & performance improvement
Professionals - de-motivated by poor pay; heavy workload
Users - poor quality, impersonal experience Products - singular, high cost consumptive Public-private divide Little accountability for care outcomes & impact Innovation difficult to propagate Fragmented - not efficient and lacks synergy Centralized - discourages creativity and self-efficacy in
decision making

HS challenges for Development Goals
Inadequate coverage (limited supply) Variable quality (reduced effectiveness) Fragmentation (Lack of efficiency & ‘absorptive
capacity’) No sustainability (consumptive vs productive) Failing prevention Systems not meeting the needs of people Treat affected populations vs develop healthy
communitiesThese challenges will not be solved by just increasing aid or
achieving economic growth (i.e. traditional development approaches)

Human Scale Development
“Development is a process that happens inside people as a consequence of what happens between people and their life support systems, as they satisfy their fundamental human needs by fashioning an infinite range of diverse satisfiers”.
Manfred Max-Neef

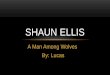
The Chronic Care Model (Adapted from: Wagner EH. Effective Clinical Practice, 1998)

Components of Health Systems
1. Rules2. People3. Money4. Supplies5. Information6. Management7. Community
Traditionally health systems are ‘closed’ and operate within parallel public and private domains

Drivers of Public Health Benefit
Most health benefit accrues from changes outside the “health system”
Family and individuals (through self-care) provide majority of healthcare, +traditional healers
Cumulative changes result from health trends (especially if increasing self-efficacy for health action)

A “7th element” of health systemsSustainable systems need cohesion = “community”
Social cohesion Shared goals Shared values Identity Participation Creativity...
Types of community User community Provider community Professional community…
Social support and a sense of belonging (being part of a social network) are a vital part of good health

Co-creating Open Systems
By enabling collaboration across sectoral, organizational and public/private boundaries this creates communities that can grow as distributive networks to make sustainable contributions that address local health needs.
These communities ‘co-create’ health systems through new combinations of financing, knowledge, human resources, etc.

Changing Paradigms
‘Prevailing strategies rely largely on outmoded theories of control and standardisation of work.
More modern, and much more effective, theories of production seek to harness the imagination and participation of the workforce [health providers] in reinventing the system’
Don Berwick, Quality & Safety in Health Care,
December 2003

Desirable characteristics of Open Systems…
Accessible by being distributed across communities & households
Collaborative so resources, know-how, effort & expertise are shared
Creative building on what is already available and more adaptive to local needs
High-Impact with greater potential to generate long-term public health benefits
Sustainable when participants in care are seen as producers, rather than consumers

Unlocking the potential to co-create health
Create conditions for co-creation Help providers become organized, motivated
and equipped Activate communities / networks and help them to
become better organised Introduce interventions that have the greatest
potential to synergistically satisfy fundamental human needs
Distribute information, resources, know-how

Public-Private Mix
A design that establishes the conditions for co-creating health systems:
Purpose (shared goals) Participants “Operating platform” Tools & processes Resources Agency


Shared Public Health Goals
AvailabilityQualitySustainabilityService Integration

Participants in the mix
Private Companies Medical practitioners Public Sector employees CBO’s (Home-based care) Traditional Healers Care supporters Dispensaries Workforce (esp. Peer Educators) Church groups, School teachers…These are active communities that have the energy, people and
potential to co-create health services

Examples of corporate contributions
Health of the workforce community Advocacy & political influence Corporate Social Responsibility Leveraging Core competency Funding / donations (including co-investment)
“CSR is business response to sustainability”

Operating Platform
‘Public Health Approach’ “Package of essential public health
interventions” Guidelines Training Monitoring tools …
“A franchise for public health care”

Tools & processes
Contracting (including MoU) Accreditation Training (eg. IMAI) Monitoring & reporting …
Wherever possible, use National Programme tools, processes, standards, etc. BUT difference here is in how these are operationalized (for sustainability)

Resources
Co-investment Drug supply Knowledge Expertise …

Agency Roles Create conditions
Advocacy (alignment of public health goals) Tools and processes Public Health Approach (programme alignment) Resources (investment, allocation, management)
Organise, motivate & equip providers Community-building (mobilise participation, establish
partnerships) Developmental interventions Distribute information, resources, know-how
Manage sustainable development of system Learning and knowledge management (incl reporting) etc.

What motivates co-creation?
Interventions that satisfy fundamental Human Needs can drive sustainable participation :
+ Subsistence + Understanding+ Protection (health) + Creation+ Participation + Identity+ Idleness (recuperation)+ Affection (care) + Freedom (choice)
Needs Theory is central to understanding Human Scale Development


‘I Know!’ intervention meeting Human Needs
Need Having Being Doing
Subsistence Stipend Employed Peer Support
Protection Treatment Supported Adhering
Understanding Training Tx Literate Learning
Participation Role In Team Train others
Creation Opportunity Resourceful Communicating
Identity Expert Patient Disclosed Advocacy
Freedom Choice Able Deciding

Early experiences Opportunities: Risks:
CSR (linked to workplace responses) GBC, WEF, GCSD
Co-investment PEPFAR, GFATM
PLHA Advocacy for participation
Political declarations about Private Sector
More organised providers Developing markets Local action (building on
workplace programme)
Establishing legitimacy Aligning corporate partner Defining governance Feasibility? Political processes ROLES & INFLUENCES
OF LOCAL/PROVINCIAL GOVERNMENT…

Government Roles
How to exercise stewardship over ‘open systems’? PPP policy Levels of decision-making Resource allocation Regulation Relationship with Agency