Embed Size (px)
Citation preview

Co-occurring Conditions and Change in Diagnosis inAutism Spectrum Disorders
WHAT’S KNOWN ON THIS SUBJECT: Mixed prevalence rates of co-occurring psychiatric and neurodevelopmental conditions havebeen reported in children diagnosed with an autism spectrumdisorder (ASD). ASD diagnoses remain fairly stable withina continuum, but some do not meet criteria for an ASD diagnosisyears after initial diagnosis.
WHAT THIS STUDY ADDS: Co-occurring neurodevelopmental andpsychiatric conditions may explain, in part, why the diagnosis ofan ASD may change with age.
abstractOBJECTIVE: This study aimed to investigate descriptive characteristicsand co-occurring neurodevelopmental and psychiatric conditions inyoung children, children, and adolescents with a current andconsistent or past but not current (PBNC) diagnosis of autismspectrum disorder (ASD) and how such characteristics and conditionsmay engender a change in diagnosis of an ASD.
METHODS: Cross-sectional data of 1366 children with a parent-reportedcurrent or PBNC ASD diagnosis were obtained from the National Surveyof Children’s Health 2007 data set across 3 developmental stages: youngchildren (aged 3–5 years), children (aged 6–11 years), and adolescents(aged 12–17 years). Multinomial logistic regression was used toexamine demographic characteristics and co-occurring conditionsthat differentiate the groups with a current ASD from groups witha PBNC ASD.
RESULTS: Results indicated the co-occurring conditions that distinguishgroups currently diagnosed with an ASD from groups with a PBNC ASDdiagnosis. In young children, current moderate/severe learningdisability, and current moderate/severe developmental delay; inchildren, past speech problem, current moderate/severe anxiety,and past hearing problem; and in adolescents, current moderate/severe speech problem, current mild seizure/epilepsy, and pasthearing problem.
CONCLUSIONS: These findings suggest that the presence of co-occurring psychiatric and neurodevelopmental conditions are associatedwith a change in ASD diagnosis. Questions remain as to whetherchanges in diagnosis of an ASD are due to true etiologic differencesor shifts in diagnostic determination. Pediatrics 2012;129:e305–e316
AUTHORS: Heather A. Close, BS,a Li-Ching Lee, PhD, ScM,a
Christopher N. Kaufmann, MHS,a and Andrew W.Zimmerman, MDb
aCenter for Autism and Developmental Disabilities Epidemiology,Johns Hopkins Bloomberg School of Public Health, Baltimore,Maryland; and bLurie Family Autism Center, MassachusettsGeneral Hospital for Children, Lexington, Massachusetts
KEY WORDSautism spectrum disorder, co-occurring conditions, diagnosischange
ABBREVIATIONSaOR—adjusted odds ratioASD—autism spectrum disorderCI—confidence intervalIEP—individualized education planNSCH—National Survey of Children’s HealthPBNC—past but not currentPDD-NOS—pervasive developmental disorder, not otherwisespecified
All 4 authors had full access to the total data set used andguarantee the integrity of the study and study findings. Ms Closedeveloped the study design, acquired the data set, performedportions of data analysis, and drafted/revised the manuscript;Dr Lee also developed the study design and oversaw reportedstatistical findings and preparation/revisions of the manuscriptfor important intellectual content; Mr Kaufmann completedstudy data analysis and assisted in drafting the initialmanuscript; and Dr Zimmerman assisted in understanding theclinical implications of the findings and final edits of the draft.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1717
doi:10.1542/peds.2011-1717
Accepted for publication Sep 28, 2011
Address correspondence to Heather A. Close, BS, Center forAutism and Developmental Disabilities Epidemiology, JohnsHopkins Bloomberg School of Public Health E6036, Baltimore, MD21209. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
PEDIATRICS Volume 129, Number 2, February 2012 e305
ARTICLE

Autism spectrum disorders (ASD), in-cluding autistic disorder; pervasivedevelopmental disorder, not otherwisespecified (PDD-NOS); and Aspergerdisorder, were formerly believed tooccur in 4 to 5 cases out of 10 000.1
However, this prevalence rate has risenin recent years, and reports now in-dicate that ∼1% of children aged 8 inthe United States alone are diagnosedwith some form of ASD.2 Differentiationbetween the core features of an ASD andother co-occurring neurodevelopmental(eg, ADHD, learning disability)3 andpsychiatric conditions can be challeng-ing.4 Diagnostic confusion may delay ap-propriate diagnosis and lead to missedopportunities for early intervention witheffective therapies.5
Researchers have begun to understandthe importance of co-occurring neu-rodevelopmental and psychiatric con-ditions when diagnosing and treatingchildren with ASDs.4,6 Previous studieshave shown higher rates of co-occurringdevelopmental and psychiatric con-ditions in children with ASDs.3,7–11 Co-occurring conditions occur morefrequently in children with an ASDcompared with typically developingchildren12 or children with devel-opmental delays or genetic disorderswithout an ASD.5 Prevalence of each co-occurring condition differs withindevelopmental age groups for thosediagnosed with an ASD. Children andadolescents with an ASD have shownhigh rates of co-occurring ADHD,13
whereas adolescents and adults withan ASD are frequently diagnosed withco-occurring depression.14 In addi-tion, there have been variable reportsof prevalence rates for co-occurringconduct disorder, phobias, and anxi-ety with ASDs.7,8,11
Stability of an ASD diagnosis seems tovary over time.15,16 One prospectivestudy found that .10% of 2 year oldsoriginally diagnosed with an ASD nolonger had an ASD diagnosis at age 9.17
More recently, a study using the USNational Survey of Children’s Health(NSCH) 2007 data set found that 40% ofchildren (aged 3–17), with an ASD di-agnosis ever, no longer had a diagnosisof ASD at time of parent report.18 Ourunderstanding of the extent to which co-occurring conditions are associatedwith diagnostic changes in ASDs will im-prove the accuracy and timeliness of di-agnosis and thereby optimize the efficacyof early intervention and treatments.
This study aimed to investigate the ex-tent to which commonly co-occurringconditions differentiate children witha current ASD diagnosis from childrenwhohadapastbutnotcurrent(PBNC)ASDdiagnosis (ie, no longer meeting criteriafor an ASD diagnosis), across 3 de-velopmental stages: young children (aged3–5 years), children (aged 6–11 years),and adolescents (aged 12–17 years).
METHODS
Data from the US NSCH 2007 were usedto complete this study. Cross-sectional,parent-reported data of NSCH 2007were collected by one-time random-digit-dial phone interviews to house-holds between April 2007 and July2008. Households with at least 1 childbetween the ages of 0 and 17 wereeligible to participate. Survey questionsincluded the child’s demographics;physical and mental health, includingcurrent and past medical, behavioral,and developmental diagnoses; healthcare needs and services; and parentaland family health and behaviors. Thefinal NSCH 2007 data set comprised91 642 completed surveys. More in-formation regarding the administra-tion and data collection are describedelsewhere.19
Study Sample
This study focused on the responses tothe following questions: “Has a doctoror other health care provider evertold you that [study child] had Autism,
Asperger disorder, pervasive develop-mental disorder, or other autism spec-trum disorder?” and “Does [study child]currently have autism or ASD?” A vari-able was thus created that defined the2 study groups: (1) current ASD di-agnosis and (2) PBNC ASD diagnosis,based on the responses to thesequestions. Omissions to this variable,including “refusal” or “don’t know”responses, no current or past ASDdiagnoses, and children ,3 years ofage, were excluded from the studysample. Data were analyzed acrossthe following 3 developmental stages:(1) young children (aged 3–5), (2)children (aged 6–11), and (3) adoles-cents (aged 12–17). Age groups wereallocated on the basis of the charac-teristics of each. Autism diagnosisusually occurs by age 517,20 whileother confounding diagnoses havebecome apparent. From age 3 to 5,brain plasticity is maximal and theeffects of early intervention and thera-pies are optimal.21 ASD diagnoses inchildren, aged 6 to 11, have been shownto change22 from autism to PDD-NOS (orthe reverse).17 Also, learning capa-bilities and individual needs becomeclearer during this period. ASD di-agnoses usually stabilize during ado-lescence, ages 12 to 17, and educationalneeds are clarified. Psychiatric co-occurring conditions often become evi-dent during adolescence as well. Thefinal data set used in this study included1366 study children and comprised 154young children, 373 children, and 386adolescents reported having a currentASD diagnosis and 53 young children,189 children, and 211 adolescentsreported having a PBNC ASD diagnosis.Altogether, 453 children, or 33.2% of ourstudy sample, were reported havinga PBNC ASD diagnosis at time of surveyadministration.
Study Variables
Sociodemographic variables assessedincluded child sex, race (white, black,
e306 CLOSE et al
multiracial, and other single race), eth-nicity (Hispanic, non-Hispanic), mother’sand father’s education (less than highschool diploma, high school diploma,greater than high school diploma),poverty level (#100%, 101%–200%,201%–300%, .300% of the federalpoverty level), current health insurancecoverage (insured, uninsured), consis-tency of health coverage during thepast year (consistent, inconsistent), andwhether the study child had a currentindividualized education plan (IEP) (yes,no). Co-occurring conditions of interestincluded attention-deficit/hyperactivitydisorder, learning disability, develop-mental delay, speech problems, hearingproblems, anxiety, depression, behav-ioral or conduct problems, and seizuresor epilepsy (seizures/epilepsy). Responsesfor each co-occurring condition weredivided into the following categories:past diagnosis, current mild diagnosis,current moderate or severe (moderate/severe) diagnosis, and never diagnosed.
Statistical Analysis
Descriptive statistics of both un-weighted andweightedpercentagesofvarioussociodemographicvariables,andprevalence rates for each co-occurringcondition were stratified by the devel-opmental age groups. Multinomial lo-gistic regression was carried out toexamine the associations between theASD diagnosis status (current ASDversus PBNC ASD) and demographiccharacteristics and co-occurring con-ditions. The multinomial logistic re-gressionmodel is a simple extension ofthe binomial logistic regression modelin which the dependent variable has.2 unordered nominal categories.
Odds ratios and the 95% confidenceintervals (CI) were reported to indicatethe associations. All regression analy-ses used weighted data. Methods ofvariance estimation accounting for thecomplex sampling design were appliedto correct standard errors by using the
Taylor-series approximation. Two setsof confounders were included in themultivariate analyses. The first set in-cluded race, ethnicity, and mother’s edu-cation. Because children with learningdisabilities, including an ASD, are coveredunder the Individuals with DisabilitiesAct,23 which may alter the associationbetween ASD diagnosis and the co-occurring conditions, we conducted thesecond set of analyses by adding IEP asone of the confounders in addition torace, ethnicity, and mother’s education.
RESULTS
Sample Demographics
Demographic characteristics for the 2study groups, those with a current andPBNCdiagnosis of anASD, are presentedin Table 1 by developmental stages. Themajority of children included in oursample were male, of white race, and ofnon-Hispanic ethnicity. Most were cov-ered by health insurance and had con-sistent health insurance coverageduring the past year before adminis-tration of the survey. Approximatelythree-fourths of children were on a cur-rent IEP. Approximately 70% of parentshad education beyond high school, andnearly half of the children’s families inthe survey had household incomes.300% of the federal poverty level.
Co-occurring Conditions
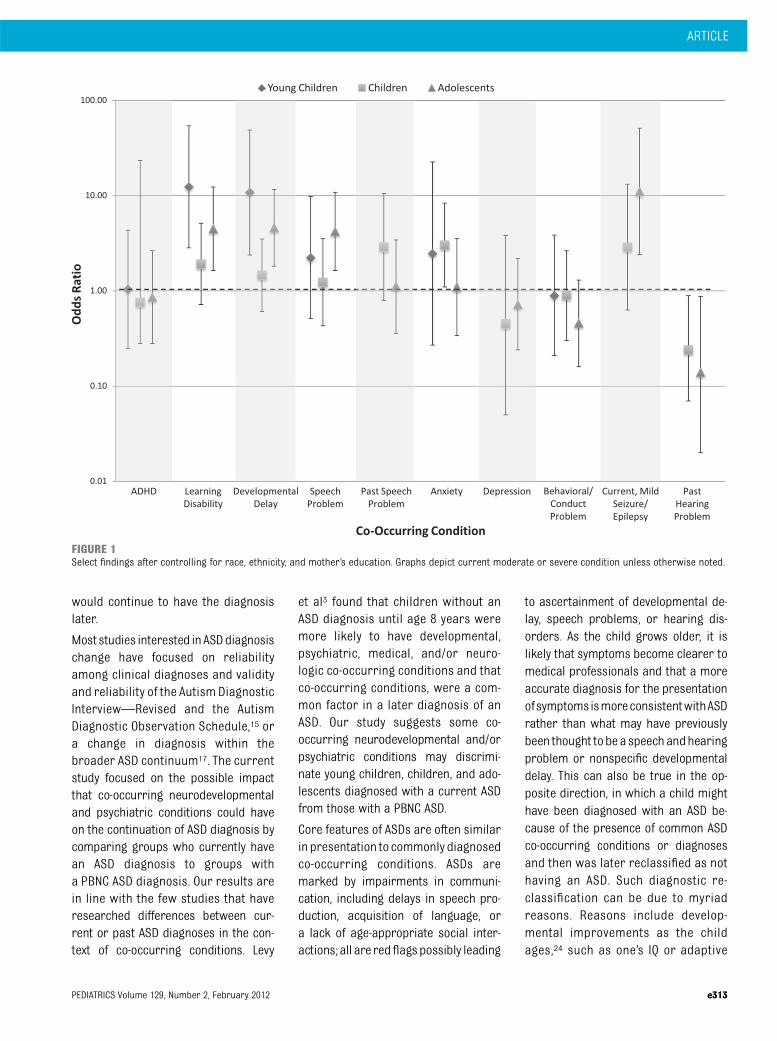
Table 2 presents unadjusted and ad-justed associations between ASD diag-nosis status (current versus PBNC)and co-occurring neurodevelopmentaland psychiatric conditions. Figures 1and 2 show select results of adjustedodds ratios; the y axis is in logarithmicformat.
Young Children (Aged 3–5 Years)
After adjusting for race, ethnicity,mother’s education, and IEP, youngchildren with a current diagnosis ofASD had 11.07 (95% CI: 2.48–49.49)times higher odds of having a current
moderate/severe learning disabilityand 9.20 (95% CI: 1.90–44.42) timesgreater odds of having a currentmoderate/severe developmental delaythan the young children with a PBNCASD diagnosis. Young children witha current ASD diagnosis were 4.76(95% CI 1.46–15.51) timesmore likely tohave $2 current co-occurring con-ditions than children with a PBNC ASDdiagnosis. Statistical analysis was notperformed for cells with a sample size,5 because it did not provide suffi-cient statistical power to calculateprecise effect estimates.
Children (Aged 6–11 Years)
Children with a current ASD diagnosiscompared with those with a PBNC ASDdiagnosis showed differences in pastspeech problem (5.3% vs 2.1%), currentmoderate/severe anxiety (21.1%vs8.9%),and past hearing problem (3.8% vs12.8%). After adjusting for confounders,childrenwith a current diagnosis of ASDhad 3.85 (95% CI: 1.09–13.67) timesgreater odds of having a past speechproblem, 3.51 (95% CI: 1.28–9.65)greater odds of having currentmoderate/severe anxiety, but lowerodds of having past hearing problems(adjusted odds ratio [aOR] = 0.23, 95%CI: 0.06–0.83) compared with childrenwith a PBNC diagnosis of ASD. Childrenwith a current ASD diagnosis were 3.19(95% CI: 1.25–8.16) times more likely tohave $2 current co-occurring con-ditions when controlling for all con-founders except IEP. When IEP wasadded as a confounder, the effect wasno longer significant.
Adolescents (Aged 12–17 Years)
Adolescents with a current diagnosisof ASD had almost 4 times (aOR = 3.91,95% CI: 1.56–9.75) greater oddsof having current moderate/severespeech problems, 10 times (aOR =10.48, 95% CI: 2.25–48.87) greater oddsof current mild seizures/epilepsy, andsignificant lower odds (aOR = 0.11, 95%
ARTICLE
PEDIATRICS Volume 129, Number 2, February 2012 e307
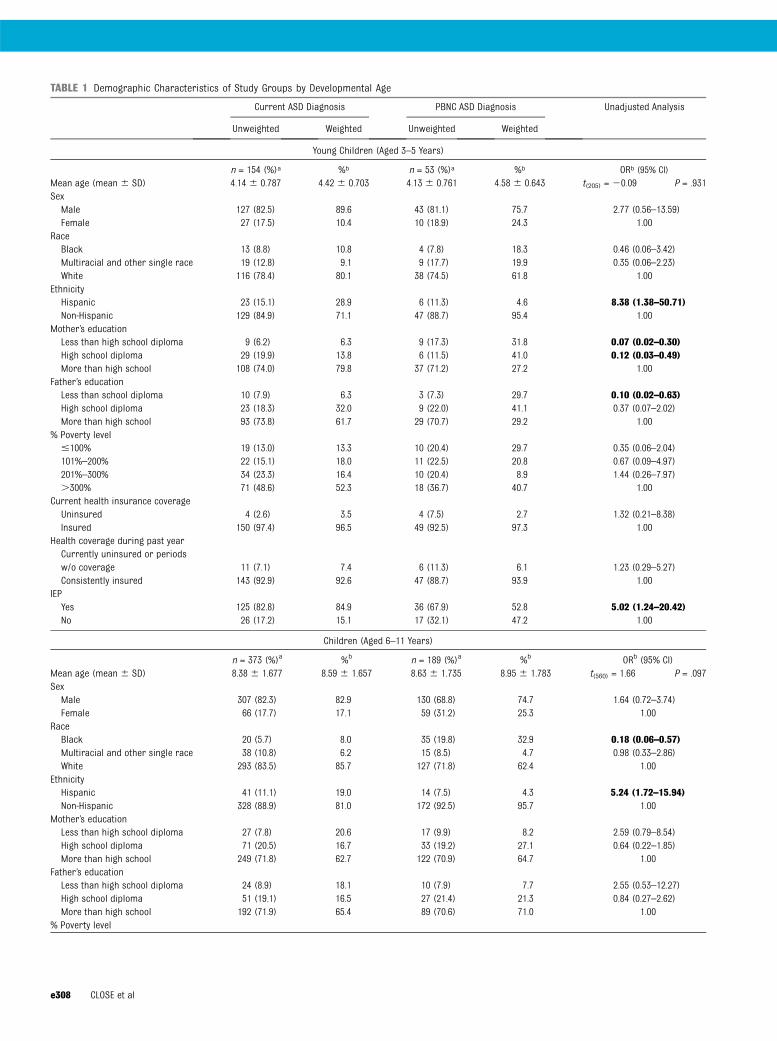
TABLE 1 Demographic Characteristics of Study Groups by Developmental Age
Current ASD Diagnosis PBNC ASD Diagnosis Unadjusted Analysis
Unweighted Weighted Unweighted Weighted
Young Children (Aged 3–5 Years)
n = 154 (%)a %b n = 53 (%)a %b ORb (95% CI)Mean age (mean 6 SD) 4.14 6 0.787 4.42 6 0.703 4.13 6 0.761 4.58 6 0.643 t(205) = 20.09 P = .931SexMale 127 (82.5) 89.6 43 (81.1) 75.7 2.77 (0.56–13.59)Female 27 (17.5) 10.4 10 (18.9) 24.3 1.00
RaceBlack 13 (8.8) 10.8 4 (7.8) 18.3 0.46 (0.06–3.42)Multiracial and other single race 19 (12.8) 9.1 9 (17.7) 19.9 0.35 (0.06–2.23)White 116 (78.4) 80.1 38 (74.5) 61.8 1.00
EthnicityHispanic 23 (15.1) 28.9 6 (11.3) 4.6 8.38 (1.38–50.71)Non-Hispanic 129 (84.9) 71.1 47 (88.7) 95.4 1.00
Mother’s educationLess than high school diploma 9 (6.2) 6.3 9 (17.3) 31.8 0.07 (0.02–0.30)High school diploma 29 (19.9) 13.8 6 (11.5) 41.0 0.12 (0.03–0.49)More than high school 108 (74.0) 79.8 37 (71.2) 27.2 1.00
Father’s educationLess than school diploma 10 (7.9) 6.3 3 (7.3) 29.7 0.10 (0.02–0.63)High school diploma 23 (18.3) 32.0 9 (22.0) 41.1 0.37 (0.07–2.02)More than high school 93 (73.8) 61.7 29 (70.7) 29.2 1.00
% Poverty level#100% 19 (13.0) 13.3 10 (20.4) 29.7 0.35 (0.06–2.04)101%–200% 22 (15.1) 18.0 11 (22.5) 20.8 0.67 (0.09–4.97)201%–300% 34 (23.3) 16.4 10 (20.4) 8.9 1.44 (0.26–7.97).300% 71 (48.6) 52.3 18 (36.7) 40.7 1.00
Current health insurance coverageUninsured 4 (2.6) 3.5 4 (7.5) 2.7 1.32 (0.21–8.38)Insured 150 (97.4) 96.5 49 (92.5) 97.3 1.00
Health coverage during past yearCurrently uninsured or periodsw/o coverage 11 (7.1) 7.4 6 (11.3) 6.1 1.23 (0.29–5.27)Consistently insured 143 (92.9) 92.6 47 (88.7) 93.9 1.00
IEPYes 125 (82.8) 84.9 36 (67.9) 52.8 5.02 (1.24–20.42)No 26 (17.2) 15.1 17 (32.1) 47.2 1.00
Children (Aged 6–11 Years)
n = 373 (%)a %b n = 189 (%)a %b ORb (95% CI)Mean age (mean 6 SD) 8.38 6 1.677 8.59 6 1.657 8.63 6 1.735 8.95 6 1.783 t(560) = 1.66 P = .097SexMale 307 (82.3) 82.9 130 (68.8) 74.7 1.64 (0.72–3.74)Female 66 (17.7) 17.1 59 (31.2) 25.3 1.00
RaceBlack 20 (5.7) 8.0 35 (19.8) 32.9 0.18 (0.06–0.57)Multiracial and other single race 38 (10.8) 6.2 15 (8.5) 4.7 0.98 (0.33–2.86)White 293 (83.5) 85.7 127 (71.8) 62.4 1.00
EthnicityHispanic 41 (11.1) 19.0 14 (7.5) 4.3 5.24 (1.72–15.94)Non-Hispanic 328 (88.9) 81.0 172 (92.5) 95.7 1.00
Mother’s educationLess than high school diploma 27 (7.8) 20.6 17 (9.9) 8.2 2.59 (0.79–8.54)High school diploma 71 (20.5) 16.7 33 (19.2) 27.1 0.64 (0.22–1.85)More than high school 249 (71.8) 62.7 122 (70.9) 64.7 1.00
Father’s educationLess than high school diploma 24 (8.9) 18.1 10 (7.9) 7.7 2.55 (0.53–12.27)High school diploma 51 (19.1) 16.5 27 (21.4) 21.3 0.84 (0.27–2.62)More than high school 192 (71.9) 65.4 89 (70.6) 71.0 1.00
% Poverty level
e308 CLOSE et al
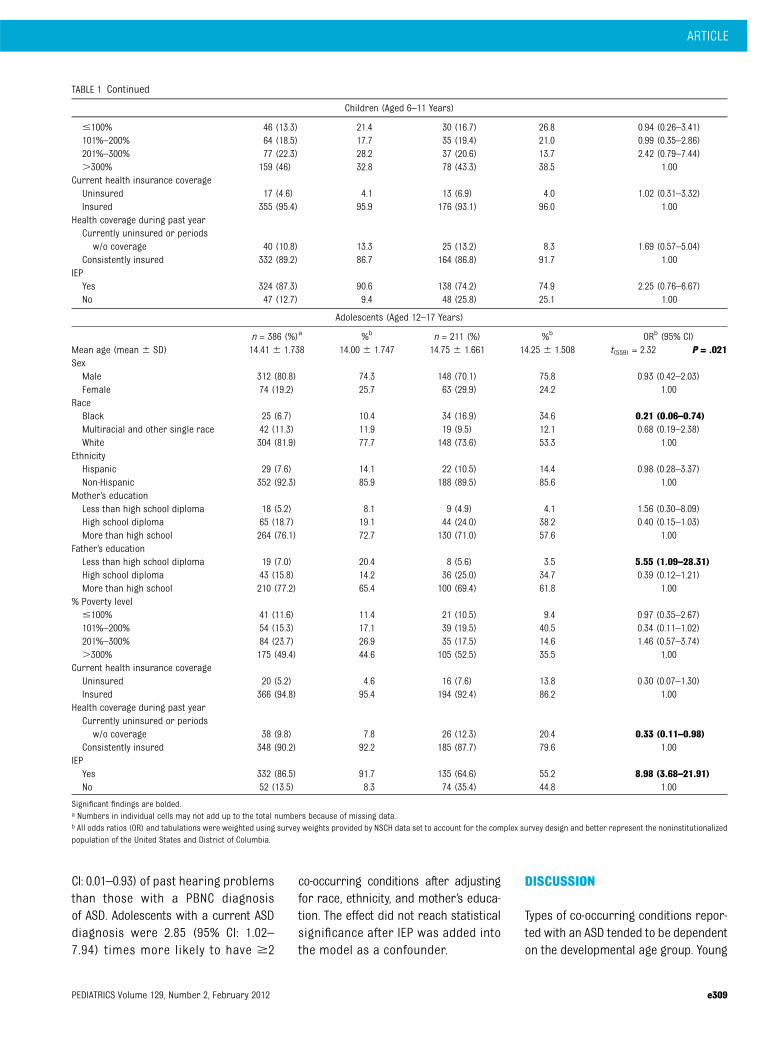
CI: 0.01–0.93) of past hearing problemsthan those with a PBNC diagnosisof ASD. Adolescents with a current ASDdiagnosis were 2.85 (95% CI: 1.02–7.94) times more likely to have $2
co-occurring conditions after adjustingfor race, ethnicity, and mother’s educa-tion. The effect did not reach statisticalsignificance after IEP was added intothe model as a confounder.
DISCUSSION
Types of co-occurring conditions repor-ted with an ASD tended to be dependenton the developmental age group. Young
TABLE 1 Continued
Children (Aged 6–11 Years)
#100% 46 (13.3) 21.4 30 (16.7) 26.8 0.94 (0.26–3.41)101%–200% 64 (18.5) 17.7 35 (19.4) 21.0 0.99 (0.35–2.86)201%–300% 77 (22.3) 28.2 37 (20.6) 13.7 2.42 (0.79–7.44).300% 159 (46) 32.8 78 (43.3) 38.5 1.00
Current health insurance coverageUninsured 17 (4.6) 4.1 13 (6.9) 4.0 1.02 (0.31–3.32)Insured 355 (95.4) 95.9 176 (93.1) 96.0 1.00
Health coverage during past yearCurrently uninsured or periodsw/o coverage 40 (10.8) 13.3 25 (13.2) 8.3 1.69 (0.57–5.04)
Consistently insured 332 (89.2) 86.7 164 (86.8) 91.7 1.00IEPYes 324 (87.3) 90.6 138 (74.2) 74.9 2.25 (0.76–6.67)No 47 (12.7) 9.4 48 (25.8) 25.1 1.00
Adolescents (Aged 12–17 Years)
n = 386 (%)a %b n = 211 (%) %b ORb (95% CI)Mean age (mean 6 SD) 14.41 6 1.738 14.00 6 1.747 14.75 6 1.661 14.25 6 1.508 t(559) = 2.32 P = .021SexMale 312 (80.8) 74.3 148 (70.1) 75.8 0.93 (0.42–2.03)Female 74 (19.2) 25.7 63 (29.9) 24.2 1.00
RaceBlack 25 (6.7) 10.4 34 (16.9) 34.6 0.21 (0.06–0.74)Multiracial and other single race 42 (11.3) 11.9 19 (9.5) 12.1 0.68 (0.19–2.38)White 304 (81.9) 77.7 148 (73.6) 53.3 1.00
EthnicityHispanic 29 (7.6) 14.1 22 (10.5) 14.4 0.98 (0.28–3.37)Non-Hispanic 352 (92.3) 85.9 188 (89.5) 85.6 1.00
Mother’s educationLess than high school diploma 18 (5.2) 8.1 9 (4.9) 4.1 1.56 (0.30–8.09)High school diploma 65 (18.7) 19.1 44 (24.0) 38.2 0.40 (0.15–1.03)More than high school 264 (76.1) 72.7 130 (71.0) 57.6 1.00
Father’s educationLess than high school diploma 19 (7.0) 20.4 8 (5.6) 3.5 5.55 (1.09–28.31)High school diploma 43 (15.8) 14.2 36 (25.0) 34.7 0.39 (0.12–1.21)More than high school 210 (77.2) 65.4 100 (69.4) 61.8 1.00
% Poverty level#100% 41 (11.6) 11.4 21 (10.5) 9.4 0.97 (0.35–2.67)101%–200% 54 (15.3) 17.1 39 (19.5) 40.5 0.34 (0.11–1.02)201%–300% 84 (23.7) 26.9 35 (17.5) 14.6 1.46 (0.57–3.74).300% 175 (49.4) 44.6 105 (52.5) 35.5 1.00
Current health insurance coverageUninsured 20 (5.2) 4.6 16 (7.6) 13.8 0.30 (0.07–1.30)Insured 366 (94.8) 95.4 194 (92.4) 86.2 1.00
Health coverage during past yearCurrently uninsured or periodsw/o coverage 38 (9.8) 7.8 26 (12.3) 20.4 0.33 (0.11–0.98)
Consistently insured 348 (90.2) 92.2 185 (87.7) 79.6 1.00IEPYes 332 (86.5) 91.7 135 (64.6) 55.2 8.98 (3.68–21.91)No 52 (13.5) 8.3 74 (35.4) 44.8 1.00
Significant findings are bolded.a Numbers in individual cells may not add up to the total numbers because of missing data.b All odds ratios (OR) and tabulations were weighted using survey weights provided by NSCH data set to account for the complex survey design and better represent the noninstitutionalizedpopulation of the United States and District of Columbia.
ARTICLE
PEDIATRICS Volume 129, Number 2, February 2012 e309

TABLE 2 Associations Between ASD Diagnosis Status and Co-occurring Developmental and Psychiatric Conditions by Developmental Age
Co-occurring Condition Current ASD Diagnosis PBNC ASD Diagnosis Unadjusted Analysis Adjusted Analysisb Adjusted Analysisc
Unweighted Weighted Unweighted Weightedn (%)a % n (%)a % OR (95% CI) OR (95% CI) OR (95% CI)
Young Children (Aged 3–5 Years)
ADHDPast 8 (5.2) 3.1 2 (3.8) 0.3 NA NA NACurrent, mild 6 (3.9) 6.6 2 (3.8) 2.0 NA NA NACurrent, moderate/severe 19 (12.4) 8.0 7 (13.2) 10.9 0.77 (0.18–3.26) 1.04 (0.25–4.35) 0.90 (0.21–3.93)None 120 (78.4) 82.3 42 (79.2) 86.8 1.00 1.00 1.00
Learning disabilityPast 3 (2.0) 1.7 3 (5.9) 1.3 NA NA NACurrent, mild 32 (21.2) 17.1 8 (15.7) 12.1 4.16 (1.01–17.11) 4.09 (0.95–17.63) 3.31 (0.70–15.72)Current, moderate/severe 70 (46.4) 56.0 12 (23.5) 12.9 12.67 (3.13 -51.22) 12.37 (2.83–54.03) 11.07 (2.48–49.49)None 46 (30.5) 25.2 28 (54.9) 73.7 1.00 1.00 1.00
Developmental delayPast 9 (5.9) 7.3 3 (5.8) 3.1 NA NA NACurrent, mild 38 (25.0) 19.4 14 (26.9) 19.4 2.52 (0.61–10.36) 3.75 (0.87–16.22) 2.99 (0.63–14.22)Current, moderate/severe 67 (44.1) 49.6 17 (32.7) 18.0 6.92 (1.68–28.55) 10.79 (2.38–48.84) 9.20 (1.90–44.42)None 38 (25.0) 23.7 18 (34.6) 59.5 1.00 1.00 1.00
Speech problemPast 5 (3.3) 4.8 4 (7.5) 15.7 NA NA NACurrent, mild 25 (16.4) 30.6 9 (17.0) 30.1 1.26 (0.19–8.45) 0.96 (0.18–5.00) 0.71 (0.15–3.47)Current, moderate/severe 66 (43.4) 38.0 20 (37.7) 21.3 2.20 (0.60–8.04) 2.23 (0.51–9.82) 1.73 (0.46–6.46)None 56 (36.8) 26.7 20 (37.7) 32.9 1.00 1.00 1.00
AnxietyPast 8 (5.2) 7.0 2 (3.8) 1.5 NA NA NACurrent, mild 8 (5.2) 1.6 4 (7.5) 8.5 NA NA NACurrent, moderate/severe 13 (8.4) 22.3 5 (9.4) 5.4 5.09 (0.63–41.47) 2.46 (0.27–22.58) 2.53 (0.26–25.05)None 125 (81.2) 69.1 42 (79.2) 84.6 1.00 1.00 1.00
DepressionPast 2 (1.3) 0.5 0 0.0 NA NA NACurrent, mild 0 0.0 0 0.0 NA NA NACurrent, moderate/severe 1 (0.7) 0.3 0 0.0 NA NA NANone 150 (98.0) 99.3 52 (100.0) 100.0 NA NA NA
Behavioral/conduct problemPast 1 (0.7) 0.3 1 (1.9) 0.2 NA NA NACurrent, mild 7 (4.6) 1.9 4 (7.5) 4.6 NA NA NACurrent, moderate/severe 23 (15.2) 12.0 10 (18.9) 15.1 0.74 (0.19–2.84) 0.89 (0.21–3.86) 0.82 (0.18–3.74)None 120 (79.5) 85.8 38 (71.7) 80.0 1.00 1.00 1.00
Seizure/epilepsyPast 2 (1.3) 1.9 0 0.0 NA NA NACurrent, mild 5 (3.3) 2.3 0 0.0 NA NA NACurrent, moderate/severe 3 (2.0) 2.8 3 (5.7) 1.9 NA NA NANone 143 (93.5) 92.9 50 (94.3) 98.1 NA NA NA
Hearing problemPast 10 (6.5) 7.4 3 (5.9) 4.8 NA NA NACurrent, mild 3 (2.0) 1.5 3 (5.9) 4.1 NA NA NACurrent, moderate/severe 3 (2.0) 1.1 1 (2.0) 4.0 NA NA NANone 137 (89.5) 90.0 44 (86.3) 87.0 NA NA NA
Total no. of current co-occurring conditions$2 116 (75.3) 77.5 32 (60.4) 38.5 9.95 (2.33–42.47) 7.16 (1.78–28.75) 4.76 (1.46–15.51)1 20 (13.0) 14.8 9 (17.0) 23.8 3.08 (0.36–25.98) 1.08 (0.12–9.62) 0.73 (0.10–5.52)None 18 (11.7) 7.7 12 (22.6) 37.7 1.00 1.00 1.00
Total no. of past co-occurring conditions$2 12 (7.8) 6.6 4 (7.6) 2.5 2.71 (0.46–15.92) 2.84 (0.54–15.05) 4.31 (0.41–45.11)1 20 (13.0) 18.3 8 (15.1) 21.3 0.87 (0.15–5.15) 1.01 (0.24–4.27) 1.57 (0.38–6.44)None 122 (79.2) 75.1 41 (77.4) 76.2 1.00 1.00 1.00
Children (Aged 6–11 Years)
ADHDPast 24 (6.5) 3.5 13 (7.0) 5.8 0.61 (0.18–2.09) 0.63 (0.18–2.23) 0.66 (0.18–2.38)
e310 CLOSE et al

TABLE 2 Continued
Children (Aged 6–11 Years)
Current, mild 40 (10.8) 16.1 17 (9.1) 4.1 3.95 (0.96–16.33) 4.28 (0.78–23.46) 5.20 (0.84–32.20)Current, moderate/severe 101 (27.3) 36.5 50 (26.7) 46.5 0.78 (0.30–2.08) 0.76 (0.28–2.04) 0.76 (0.28–2.06)None 205 (55.4) 43.9 107 (57.2) 43.7 1.00 1.00 1.00
Learning disabilityPast 13 (3.6) 7.3 19 (10.2) 8.9 1.35 (0.20–9.31) 1.46 (0.21–10.39) 2.15 (0.38–12.16)Current, mild 74 (20.2) 18.2 27 (14.5) 11.2 2.67 (0.79–9.04) 2.66 (0.78–9.06) 2.68 (0.79–9.07)Current, moderate/severe 185 (50.5) 53.3 75 (40.3) 45.0 1.95 (0.70–5.43) 1.91 (0.72–5.13) 1.94 (0.72–5.21)None 94 (25.7) 21.2 65 (34.9) 34.9 1.00 1.00 1.00
Developmental delayPast 25 (6.8) 4.0 20 (10.6) 8.8 0.46 (0.15–1.39) 0.44 (0.15–1.30) 0.65 (0.25–1.71)Current, mild 74 (20.3) 19.9 26 (13.8) 28.9 0.71 (0.19–2.57) 0.79 (0.22–2.82) 0.77 (0.22–2.77)Current, moderate/severe 148 (40.5) 46.8 69 (36.7) 32.1 1.50 (0.59–3.80) 1.46 (0.61–3.51) 1.45 (0.61–3.46)None 118 (32.3) 29.3 73 (38.8) 30.1 1.00 1.00 1.00
Speech problemPast 30 (8.2) 5.3 8 (4.2) 2.1 3.01 (0.82–11.09) 2.89 (0.79–10.58) 3.85 (1.09–13.67)Current, mild 64 (17.4) 12.6 35 (18.5) 13.1 1.16 (0.41–3.30) 1.24 (0.42–3.62) 1.25 (0.42–3.71)Current, moderate/severe 85 (23.2) 33.1 42 (22.2) 25.8 1.55 (0.51–4.65) 1.23 (0.43–3.53) 1.21 (0.42–3.51)None 188 (51.2) 48.9 104 (55.0) 58.9 1.00 1.00 1.00
AnxietyPast 24 (6.5) 8.3 18 (9.6) 11.1 0.90 (0.18–4.48) 0.72 (0.22–2.32) 0.96 (0.25–3.70)Current, mild 49 (13.2) 10.3 15 (8.0) 7.5 1.65 (0.47–5.74) 1.75 (0.50–6.11) 2.35 (0.80–6.90)Current, moderate/severe 73 (19.7) 21.1 29 (15.4) 8.9 2.84 (1.04–7.76) 3.03 (1.10–8.36) 3.51 (1.28–9.65)None 225 (60.6) 60.3 126 (67.0) 72.4 1.00 1.00 1.00
DepressionPast 16 (4.3) 12.8 12 (6.3) 3.4 3.86 (0.94–15.82) 2.52 (0.64–9.88) 3.21 (0.75–13.78)Current, mild 13 (3.5) 3.0 9 (4.8) 3.6 0.85 (0.22–3.34) 0.89 (0.22–3.55) 0.90 (0.22–3.68)Current, moderate/severe 17 (4.6) 8.4 12 (6.3) 16.5 0.52 (0.07–3.93) 0.45 (0.05–3.81) 0.45 (0.05–3.98)None 322 (87.5) 75.8 156 (82.5) 76.6 1.00 1.00 1.00
Behavioral/conduct problemPast 18 (4.9) 8.7 13 (6.9) 3.9 2.05 (0.67–6.29) 2.09 (0.69–6.29) 2.10 (0.74–5.97)Current, mild 33 (8.9) 12.3 20 (10.6) 24.4 0.46 (0.12–1.73) 0.47 (0.13–1.77) 0.42 (0.11–1.62)Current, moderate/severe 67 (18.2) 28.3 28 (14.8) 25.4 1.02 (0.34–3.09) 0.90 (0.30–2.64) 0.83 (0.28–2.49)None 251 (68.0) 50.7 128 (67.7) 46.3 1.00 1.00 1.00
Seizure/epilepsyPast 5 (1.3) 1.9 5 (2.6) 3.1 0.58 (0.09–3.68) 0.62 (0.09–4.08) 0.60 (0.09–4.11)Current, mild 15 (4.0) 2.5 6 (3.2) 0.9 2.81 (0.60–13.16) 2.88 (0.63–13.21) 2.91 (0.62–13.52)Current, moderate/severe 10 (2.7) 1.2 10 (5.3) 3.2 0.37 (0.09–1.61) 0.39 (0.10–1.56) 0.39 (0.09–1.68)None 342 (91.9) 94.4 168 (88.9) 92.7 1.00 1.00 1.00
Hearing problemPast 12 (3.2) 3.8 15 (8.0) 12.8 0.24 (0.07–0.83) 0.24 (0.07–0.89) 0.23 (0.06–0.83)Current, mild 6 (1.6) 2.0 7 (3.7) 5.8 0.28 (0.05–1.59) 0.23 (0.03–1.56) 0.24 (0.03–1.62)Current, moderate/severe 10 (2.7) 5.6 4 (2.1) 9.8 0.46 (0.04–4.83) 0.16 (0.02–1.61) 0.16 (0.02–1.62)None 343 (92.5) 88.6 162 (86.2) 71.6 1.00 1.00 1.00
Total no. of current co-occurring conditions$2 289 (77.5) 83.9 121 (64.0) 74.4 3.48 (1.39–8.72) 3.19 (1.25–8.16) 1.92 (0.79–4.64)1 55 (14.8) 11.3 33 (17.5) 10.9 3.22 (1.06–9.80) 3.13 (0.99–9.87) 1.86 (0.57–6.10)None 29 (7.8) 4.8 35 (18.5) 14.8 1.00 1.00 1.00
Total no. of past co-occurring conditions$2 34 (9.1) 10.9 31 (16.4) 14.2 0.80 (0.22–2.87) 0.64 (0.23–1.80) 0.95 (0.33–2.74)1 92 (24.7) 32.7 45 (23.8) 27.3 1.24 (0.48–3.17) 1.32 (0.53–3.30) 1.34 (0.53–3.35)None 247 (66.2) 56.5 113 (59.8) 58.5 1.00 1.00 1.00
Adolescents (Aged 12–17 Years)
ADHDPast 39 (10.5) 8.0 24 (11.5) 6.2 1.16 (0.41–3.34) 1.10 (0.39–3.08) 0.85 (0.34–2.10)Current, mild 46 (12.4) 12.5 35 (16.7) 17.7 0.65 (0.20–2.06) 0.59 (0.17–1.98) 0.32 (0.10–1.03)Current, moderate/severe 110 (29.6) 27.3 62 (29.7) 28.5 0.87 (0.30–2.57) 0.86 (0.28–2.64) 0.46 (0.16–1.36)None 176 (47.4) 52.2 88 (42.1) 47.5 1.00 1.00 1.00
Learning disabilityPast 14 (3.7) 1.6 22 (10.6) 7.9 0.40 (0.09–1.70) 0.43 (0.10–1.79) 0.36 (0.08–1.63)Current, mild 88 (23.2) 21.0 42 (20.2) 23.7 1.76 (0.49–6.32) 1.73 (0.46–6.44) 0.56 (0.17–1.85)Current, moderate/severe 201 (52.9) 60.4 93 (44.7) 34.7 3.44 (1.28–9.27) 4.49 (1.63–12.34) 1.37 (0.61–3.09)
ARTICLE
PEDIATRICS Volume 129, Number 2, February 2012 e311

children with a current ASD diagnosishad higher rates of current, moderate/severe learning disability and moderate/severe developmental delays than youngchildren with a PBNC ASD diagnosis.Children with a current ASD diagnosis,compared with children with a PBNCASD, had higher rates of past speechproblems and/or current, moderate/severe anxiety. Finally, adolescents with
a current ASD diagnosis, comparedwithadolescents with a PBNC ASD diagnosis,had higher rates of current, moderate/severe speech problems and current,mild seizures/epilepsy. Both childrenandadolescentswithacurrentASDwereless likely to have had hearing problemsin the past than those with a PBNC ASD.Overall, participants with a current ASD,in all 3 developmental age groups, were
found to be more likely to have $2co-occurring conditions than thosewith a PBNC ASD diagnosis. Seizures/epilepsy were more than 10 timesmore likely to be a co-occurring condi-tion in adolescents with a current ASDdiagnosis than those with a PBNC ASDdiagnosis; this implies that epilepsy isa strong discriminator as to whetheradolescents with a current ASD diagnosis
TABLE 2 Continued
Adolescents (Aged 12–17 Years)
None 77 (20.3) 17.0 51 (24.5) 33.7 1.00 1.00 1.00Developmental delayPast 51 (13.4) 11.0 34 (16.1) 16.7 1.27 (0.44–3.66) 1.74 (0.62–4.86) 1.57 (0.58–4.24)Current, mild 58 (15.2) 13.3 19 (9.0) 9.0 2.85 (0.67–12.10) 2.74 (0.65–11.60) 1.36 (0.28–6.50)Current, moderate/severe 155 (40.6) 48.7 69 (32.7) 22.0 4.28 (1.74–10.50) 4.60 (1.82–11.64) 2.26 (0.78–6.56)None 118 (30.9) 27.0 89 (42.2) 52.3 1.00 1.00 1.00
Speech problemPast 34 (8.9) 7.1 31 (14.8) 8.1 1.16 (0.40–3.41) 1.12 (0.36–3.43) 1.02 (0.32–3.23)Current, mild 44 (11.5) 9.0 13 (6.2) 11.0 1.08 (0.20–5.75) 0.98 (0.16–6.14) 0.83 (0.11–6.13)Current, moderate/severe 75 (19.5) 30.8 23 (11.0) 11.1 3.67 (1.29–10.43) 4.22 (1.63–10.87) 3.91 (1.56–9.75)None 231 (60.2) 53.0 143 (68.1) 69.8 1.00 1.00 1.00
AnxietyPast 30 (7.9) 4.2 15 (7.1) 11.3 0.37 (0.11–1.28) 0.41 (0.11–1.49) 0.35 (0.08–1.48)Current, mild 48 (12.6) 16.4 27 (12.8) 9.2 1.81 (0.65–4.98) 1.79 (0.63–5.08) 1.74 (0.58–5.21)Current, moderate/severe 108 (28.4) 27.6 49 (23.2) 27.2 1.02 (0.32–3.27) 1.10 (0.34–3.53) 1.04 (0.35–3.05)None 194 (51.1) 51.8 120 (56.9) 52.3 1.00 1.00 1.00
DepressionPast 39 (10.2) 11.7 26 (12.5) 7.4 1.39 (0.51–3.78) 1.53 (0.59–3.91) 1.87 (0.74–4.74)Current, mild 40 (10.4) 9.8 21 (10.1) 18.1 0.48 (0.13–1.78) 0.43 (0.11–1.69) 0.34 (0.08–1.50)Current, moderate/severe 41 (10.7) 7.9 24 (11.5) 12.6 0.55 (0.16–1.86) 0.72 (0.24–2.20) 0.60 (0.22–1.68)None 263 (68.7) 70.5 137 (65.9) 61.9 1.00 1.00 1.00
Behavioral/conduct problemPast 23 (6.0) 4.6 15 (7.1) 4.6 0.75 (0.25–2.25) 0.90 (0.30–2.73) 1.18 (0.49–2.83)Current, mild 40 (10.5) 7.0 18 (8.6) 4.4 1.19 (0.38–3.74) 1.51 (0.59–3.84) 1.32 (0.53–3.33)Current, moderate/severe 73 (19.1) 25.0 52 (24.8) 43.6 0.43 (0.15–1.19) 0.46 (0.16–1.30) 0.41 (0.15–1.13)None 246 (64.4) 63.4 125 (59.5) 47.4 1.00 1.00 1.00
Seizure/epilepsyPast 16 (4.2) 2.6 8 (3.8) 2.0 1.57 (0.49–5.01) 1.20 (0.37–3.83) 1.23 (0.26–5.77)Current, mild 19 (5.0) 14.8 8 (3.8) 1.6 11.01 (2.20–55.22) 11.07 (2.40–51.16) 10.48 (2.25–48.87)Current, moderate/severe 9 (2.4) 6.6 7 (3.3) 4.2 1.93 (0.38–9.65) 1.82 (0.37–9.04) 1.66 (0.32–8.74)None 338 (88.5) 76.0 188 (89.1) 92.2 1.00 1.00 1.00
Hearing problemPast 15 (3.9) 2.1 12 (5.7) 10.7 0.18 (0.03–1.09) 0.14 (0.02–0.88) 0.11 (0.01–0.93)Current, mild 13 (3.4) 2.6 7 (3.3) 0.8 3.06 (0.84–11.11) 2.97 (0.77–11.42) 2.60 (0.65–10.39)Current, moderate/severe 16 (4.2) 4.0 12 (5.7) 4.9 0.74 (0.17–3.14) 0.95 (0.27–3.34) 1.04 (0.33–3.35)None 340 (88.5) 91.3 180 (85.3) 83.6 1.00 1.00 1.00
Total no. of current co-occurring conditions$2 305 (79.0) 80.2 150 (71.1) 71.4 2.67 (0.95–7.53) 2.85 (1.02–7.94) 0.75 (0.26–2.13)1 49 (12.7) 13.6 29 (13.7) 13.9 2.33 (0.61–8.91) 2.38 (0.61–9.32) 0.99 (0.29–3.34)None 32 (8.3) 6.2 32 (15.2) 14.8 1.00 1.00 1.00
Total no. of past co-occurring conditions$2 54 (14.0) 10.4 52 (24.6) 16.0 0.52 (0.21–1.29) 0.55 (0.23–1.35) 0.74 (0.33–1.63)1 118 (30.6) 25.1 55 (26.1) 32.4 0.62 (0.23–1.63) 0.69 (0.24–1.94) 0.68 (0.23–1.99)None 214 (55.4) 64.5 104 (49.3) 51.6 1.00 1.00 1.00
ADHD, attention-deficit/hyperactivity disorder; NA, not analyzed due to small sample size for precise effect estimates (ie, OR and CI); OR, odds ratio. Significant findings are bolded.a Numbers in individual cells may not add up to the total numbers because of missing data.b Adjusting for race, ethnicity, and mother’s education.c Adjusting for race, ethnicity, mother’s education, and IEP.
e312 CLOSE et al
would continue to have the diagnosislater.
Most studies interested inASDdiagnosischange have focused on reliabilityamong clinical diagnoses and validityand reliability of the Autism DiagnosticInterview—Revised and the AutismDiagnostic Observation Schedule,15 ora change in diagnosis within thebroader ASD continuum17. The currentstudy focused on the possible impactthat co-occurring neurodevelopmentaland psychiatric conditions could haveon the continuation of ASD diagnosis bycomparing groups who currently havean ASD diagnosis to groups witha PBNC ASD diagnosis. Our results arein line with the few studies that haveresearched differences between cur-rent or past ASD diagnoses in the con-text of co-occurring conditions. Levy
et al3 found that children without anASD diagnosis until age 8 years weremore likely to have developmental,psychiatric, medical, and/or neuro-logic co-occurring conditions and thatco-occurring conditions, were a com-mon factor in a later diagnosis of anASD. Our study suggests some co-occurring neurodevelopmental and/orpsychiatric conditions may discrimi-nate young children, children, and ado-lescents diagnosed with a current ASDfrom those with a PBNC ASD.
Core features of ASDs are often similarin presentation to commonly diagnosedco-occurring conditions. ASDs aremarked by impairments in communi-cation, including delays in speech pro-duction, acquisition of language, ora lack of age-appropriate social inter-actions; all are redflagspossibly leading
to ascertainment of developmental de-lay, speech problems, or hearing dis-orders. As the child grows older, it islikely that symptoms become clearer tomedical professionals and that a moreaccurate diagnosis for the presentationofsymptomsismoreconsistentwithASDrather than what may have previouslybeen thought tobe a speech andhearingproblem or nonspecific developmentaldelay. This can also be true in the op-posite direction, in which a child mighthave been diagnosed with an ASD be-cause of the presence of common ASDco-occurring conditions or diagnosesand then was later reclassified as nothaving an ASD. Such diagnostic re-classification can be due to myriadreasons. Reasons include develop-mental improvements as the childages,24 such as one’s IQ or adaptive
FIGURE 1Select findings after controlling for race, ethnicity, and mother’s education. Graphs depict current moderate or severe condition unless otherwise noted.
ARTICLE
PEDIATRICS Volume 129, Number 2, February 2012 e313

social abilities,25 or a child no longermeeting the diagnostic criteria asa result of early intervention.22 Im-provements leading to a loss of an ASDdiagnosis also occur more commonlyin children diagnosed at an early agewith PDD-NOS rather than with autisticdisorder.22
The natural history of co-occurringconditions may explain the likelihoodof their being diagnosed in conjunctionwith current and constant ASDs. Anxietyis a commonly researched and repor-ted co-occurring condition in childrenwith an ASD.8,26 The anxiety experiencedby a child diagnosed with an ASD isfrequently associated with the need forrigidity in schedules, fear of change, orin response to the child’s own aware-ness of social expectations and becomes
more pronounced with age.27 In addi-tion, the onset of epilepsy not only peaksduring early adolescence but alsooccurs in a significant portion of ado-lescents diagnosed with an ASD.28,29
Therefore, not surprisingly, our studyalso found that children and adoles-cents with a current ASD were morelikely to have current anxiety and cur-rent moderate/severe epilepsy, respec-tively, compared with children andadolescents with a PBNC ASD diagnosis.
Our results should be interpretedwithin the context of the study’s limi-tations. First, we relied on parent-reported diagnoses through 1 phonecall interview. Numerous studies haveresearched the validity of self-reportwith respect to sensitive informationand foundmany factors that impact the
validity of responses. Such factors in-clude the participant’s anonymity andconfidentiality of responses, as well asthe respondent’s health, social, andpsychological conditions.30 Becausethe NSCH does not ask caregiverswhether the study child has an in-tellectual disability, we could notdiscriminate between children re-portedly diagnosed with a learningdisability who may actually have in-tellectual disability. Similarly, NSCHdid not ask parents to report thespecific ASD diagnosis of each studychild. Children and adolescents withautism, Asperger disorder, and PDD-NOS have been found to have differentoutcomes,31 and this lack of specificityprovides another limitation of our study.Another important consideration is
FIGURE 2Select findings after controlling for race, ethnicity, mother’s education, and IEP.
e314 CLOSE et al

the small sample size for some vari-ables of interest in young children.Therefore, results for this group maynot be representative of young chil-dren with PBNC and current ASD di-agnoses. Additionally, the currentstudy lacks information on individualinterventions for each child outsideof IEPs. Lastly, this study only in-vestigated children with a current ASDdiagnosis or PBNC ASD diagnosis, butnot the change from never having anASD diagnosis to having an ASD di-agnosis. It is important to note thatthe change of an ASD diagnosis can goin either direction. Nonetheless, thestudy analyzed data from a largenational population-based sample,which offers great statistical powerto investigate the study questionsthat could not have been answered by
other studies with smaller samplesizes.
Our study provides a basis for futuredirections for research in this area.Although a prospective longitudinalapproach would be ideal, a population-based retrospective study of adultsasking similar questions from the NSCHabout co-occurring conditions couldbenefit our understanding of a child’sPBNC diagnosis of an ASD. Throughthis, one could establish a more de-tailed profile about the ages of diag-nosis change, co-occurring conditions,and the interventions and treatmentsreceived. There would be consider-able value in future research studiesthat focus on the factors that dis-criminate the co-occurring condi-tions whose symptoms overlap withASD.
CONCLUSIONS
The findings of this study suggest spe-cific co-occurring conditions that maylead to a change in an ASD diagnosis:whether an ASD diagnosis would becurrent and constant or be reclassifiedas having a PBNC ASD diagnosis. How-ever, themechanisms that underlie thischange are unclear. Symptoms of co-occurring conditions similar to char-acteristics of ASDs may initially impedean ASD diagnosis until later develop-mental stages. Future research needsto focus on changes of ASD diagnoses inthe context of co-occurring conditionsrather than solely within the continuumof the autism spectrum.
ACKNOWLEDGMENTWe thank Ryne Yarger for proofreadingthis article.
REFERENCES
1. Wing L. The definition and prevalence ofautism: A review. Eur Child Adolesc Psy-chiatry. 1993;2(2):61–74
2. Autism and Developmental DisabilitiesMonitoring Network Surveillance Year 2006Principal Investigators; Centers for DiseaseControl and Prevention (CDC). Prevalenceof autism spectrum disorders—Autismand Developmental Disabilities MonitoringNetwork, United States, 2006. MMWR Sur-veill Summ. 2009;58(10):1–20
3. Levy SE, Giarelli E, Lee L-C, et al. Autismspectrum disorder and co-occurring devel-opmental, psychiatric, and medical condi-tions among children in multiple populationsof the United States. J Dev Behav Pediatr.2010;31(4):267–275
4. Hess JA, Matson JL, Dixon DR. Psychiatricsymptom endorsements in children andadolescents diagnosed with autism spec-trum disorders: a comparison to typicallydeveloping children and adolescents. J DevPhys Disabil. 2010;22(5):485–496
5. Fodstad JC, Rojahn J, Matson JL. Emergentcomorbidity in at risk children with andwithout autism spectrum disorder—a cross-sectional study. J Dev Phys Disabil. 2010;22(4):381–400
6. Gargaro BA, Rinehart NJ, Bradshaw JL,Tonge BJ, Sheppard DM. Autism and ADHD:
how far have we come in the comorbiditydebate? Neurosci Biobehav Rev. 2011;35(5):1081–1088
7. Simonoff E, Pickles A, Charman T, ChandlerS, Loucas T, Baird G. Psychiatric disordersin children with autism spectrum dis-orders: prevalence, comorbidity, and as-sociated factors in a population-derivedsample. J Am Acad Child Adolesc Psychia-try. 2008;47(8):921–929
8. Leyfer OT, Folstein SE, Bacalman S, et al.Comorbid psychiatric disorders in childrenwith autism: interview development andrates of disorders. J Autism Dev Disord.2006;36(7):849–861
9. Joshi G, Petty C, Wozniak J, et al. The heavyburden of psychiatric comorbidity in youthwith autism spectrum disorders: a largecomparative study of a psychiatrically re-ferred population. J Autism Dev Disord.2010;40(11):1361–1370
10. Mukaddes NM, Hergüner S, Tanidir C.Psychiatric disorders in individuals withhigh-functioning autism and Asperger’s dis-order: similarities and differences. WorldJ Biol Psychiatry. 2010;11(8):964–971
11. Matson JL, Nebel-Schwalm MS. Comorbidpsychopathology with autism spectrumdisorder in children: an overview. Res DevDisabil. 2007;28(4):341–352
12. Gurney JG, McPheeters ML, Davis MM. Pa-rental report of health conditions andhealth care use among children with andwithout autism: National Survey of Child-ren’s Health. Arch Pediatr Adolesc Med.2006;160(8):825–830
13. Sinzig J, Walter D, Doepfner M. Attentiondeficit/hyperactivity disorder in childrenand adolescents with autism spectrumdisorder: symptom or syndrome? J AttenDisord. 2009;13(2):117–126
14. Witwer AN, Lecavalier L. Validity of comor-bid psychiatric disorders in youngsterswith autism spectrum disorders. J DevPhys Disabil. 2010;22(4):367–380
15. Kleinman JM, Ventola PE, Pandey J, et al.Diagnostic stability in very young childrenwith autism spectrum disorders. J AutismDev Disord. 2008;38(4):606–615
16. van Daalen E, Kemner C, Dietz C, SwinkelsSHN, Buitelaar JK, van Engeland H. Inter-rater reliability and stability of diagnosesof autism spectrum disorder in childrenidentified through screening at a veryyoung age. Eur Child Adolesc Psychiatry.2009;18(11):663–674
17. Lord C, Risi S, DiLavore PS, Shulman C,Thurm A, Pickles A. Autism from 2 to 9years of age. Arch Gen Psychiatry. 2006;63(6):694–701
ARTICLE
PEDIATRICS Volume 129, Number 2, February 2012 e315

18. Kogan MD, Blumberg SJ, Schieve LA, et al.Prevalence of parent-reported diagnosis ofautism spectrum disorder among childrenin the US, 2007. Pediatrics. 2009;124(5):1395–1403
19. Blumberg SJ, Foster EB, Skalland BJ,Chowdhury SR, O’Connor KS. Design andOperation of the National Survey of Child-ren’s Health, 2007 (Vital Health Stat 1).Hyattsville, MD: National Center for HealthStatistics; 2009
20. Moore V, Goodson S. How well does earlydiagnosis of autism stand the test of time?Follow-up study of children assessed forautism at age 2 and development of anearly diagnostic service. Autism. 2003;7(1):47–63
21. Corsello CM. Early intervention in autism.Infants Young Child. 2005;18(2):74–85
22. Sutera S, Pandey J, Esser EL, et al. Predictorsof optimal outcome in toddlers diagnosed
with autism spectrum disorders. J AutismDev Disord. 2007;37(1):98–107
23. Williams BB, Armistead L. Applying law andethics in professional practice. In: LionettiTM, Snyder EP, Christner RW, eds. A Prac-tical Guide to Building Professional Com-petencies in School Psychology. New York,NY: Springer Science and Business Media;2011:13–33
24. Fecteau S, Mottron L, Berthiaume C, BurackJA. Developmental changes of autisticsymptoms. Autism. 2003;7(3):255–268
25. Anderson DK, Oti RS, Lord C, Welch K. Pat-terns of growth in adaptive social abilitiesamong children with autism spectrumdisorders. J Abnorm Child Psychol. 2009;37(7):1019–1034
26. Matson JL, Hess JA, Boisjoli JA. Comorbidpsychopathology in infants and toddlerswith autism and pervasive developmentaldisorders-not otherwise specified (PDD-NOS).
Res Autism Spectr Disord. 2010;4(2):300–304
27. Gillott A, Furniss F, Walter A. Anxiety in high-functioning children with autism. Autism.2001;5(3):277–286
28. Giovanardi Rossi P, Posar A, Parmeggiani A.Epilepsy in adolescents and young adultswith autistic disorder. Brain Dev. 2000;22(2):102–106
29. Hara H. Autism and epilepsy: a retrospec-tive follow-up study. Brain Dev. 2007;29(8):486–490
30. Del Boca FK, Noll JA. Truth or consequences:the validity of self-report data in healthservices research on addictions. Addic-tion. 2000;95(suppl 3):S347–S360
31. Cederlund M, Hagberg B, Billstedt E,Gillberg IC, Gillberg C. Asperger syndrome andautism: a comparative longitudinal follow-upstudy more than 5 years after original diag-nosis. J Autism Dev Disord. 2008;38(1):72–85
e316 CLOSE et al





























