Embed Size (px)
Citation preview

CO-TRIMOX AZOLE PROPHYLA XIS FOR HIV-EXPOSED
AND HIV-INFECTED INFANTS AND CHILDREN
Pract ical approaches to implementat ion and scale up

WHO Library Cataloguing-in-Publication Data
Co-trimoxazole prophylaxis for hiV-exposed and hiV-infeCted infants and Children: practical approaches to implementation and scale up
1. Trimethoprim-sulfamethoxazole combination - therapeutic use. 2. HIV infections - drug therapy. 3. AIDS-related opportunistic infections - prevention and control. 4. Child. 5. Infant. I. World Health Organization. II. UNICEF.
ISBN 978 92 4 159863 7 (NLM classification: WC 503.2)
© World Health Organization and UNICEF 2009
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]).
The World Health Organization and UNICEF welcome requests for permission to reproduce or translate their publications – whether for sale or for noncommercial distribution. Applications and enquiries should be addressed to WHO, Office of Publications, at the above address (fax: +41 22 791 4806; email: [email protected] or to UNICEF.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization or UNICEF concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization, UNICEF or other organizations that have contributed to this work in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization, UNICEF and other organizations that have contributed to this work do not warrant that the information contained in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use.
Cover photo credit: © UNICEF/NYHQ2006-1375/PirozziAll text photo credits: © Smiley N.Pool

CO-TRIMOX AZOLE PROPHYLA XIS FOR HIV-EXPOSED
AND HIV-INFECTED INFANTS AND CHILDREN
Pract ical approaches to implementat ion and scale up
This document was written on behalf of the Expanded Inter-Agency Task Team (IATT) on Prevention of HIV Infection in Pregnant Women, Mothers and their Children and with the collaboration of multiple organizations working to improve pediatric HIV prevention, care and treatment.


iii
ACKNOWLEDGEMENTS
We gratefully acknowledge the work of Elizabeth Preble for research associated with this guide and for providing the first complete drafts.
The contributions of the following individuals who assisted in further developing, reviewing and editing this document are also gratefully acknowledged: Elaine Abrams, Stephen Arpadi, Jane Briggs, Nancy Calles, Miriam Chipimo, Siobhan Crowley, Patricia Doughty, René Ekpini, Gloria Ekpo, Shaffiq Essajee, Kathy Ferrer, Robert Ferris, Mary Lyn Field-Nguer, Robert Gass, Janet Kayita, Mary Lou Lindegren, Ronnie Lovich, Chewe Luo, Bandana Malhotra, Justin Mandala, Elizabeth Preble, Emilia Rivadeneira, Paul Roux, Peter Salama, Nathan Shaffer, Diana Silimperi, Michael Tolle, Renee van de Weerdt and Helena Walkowiak.
UNICEF and WHO on behalf of the Inter-Agency Task Team on Prevention of HIV Infection in Pregnant Women, Mothers and their Children would like to express special gratitude to the writing committee that worked to develop successive drafts of this publication: Siobhan Crowley, Mary Lyn Field-Nguer and Robert Gass.
UNICEF and WHO also acknowledge the efforts and dedication of Siobhan Crowley and Robert Gass for their overall coordination of this project and bringing this publication to fruition.

iv
ACRONYMS AND ABBREVIATIONS
ANC antenatal care
ARI acute respiratory infection
ART antiretroviral therapy
ARV antiretroviral
BIPAI Baylor International Pediatric AIDS Initiative
BUFMAR Bureau des Formations Médicales Agréées au Rwanda
CAMERWA Centrale d’Achat de Médicaments Essentiels du Rwanda
CBO community-based organization
CHAP Children with HIV Antibiotic Prophylaxis (study)
CHER Children with HIV Early Antiretroviral Therapy (study)
CPDS Coordinated Procurement and Distribution System
DBS dried blood spot
EML essential medicines list
GMP Good Manufacturing Practices
HMIS health management information systems
IMAI Integrated Management of Adolescent and Adult Illness
IMCI Integrated Management of Childhood Illness
IMNCI Integrated Management of Neonatal and Childhood Illness
MCH maternal and child health
MNCH maternal, newborn and child health
MNH maternal and newborn health
MOH Ministry of Health
MSH Management Sciences for Health
MTCT mother-to-child transmission
NGO nongovernmental organization
NVP nevirapine
OI opportunistic infection
PCP Pneumocystis jiroveci pneumonia
PEPFAR US President’s Emergency Plan for AIDS Relief
PITC provider-initiated HIV testing and counselling
PMTCT prevention of mother-to-child transmission (of HIV)
UNAIDS Joint United Nations Programme on HIV/AIDS
UNICEF United Nations Children’s Fund
WHO World Health Organization

v
CONTENTS
ACKNOWLEDGEMENTS ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . i i i
ACRONYMS AND ABBREVIATIONS ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
EXECUTIVE SUMMARY.... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .v i i
I . INTRODUCTION ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
I I . HIV INFECTION IN INFANTS AND CHILDREN ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
A. Epidemiology and clinical overview .......................................................................................................................................................................... 3
B. Access to diagnosis and treatment of HIV ...................................................................................................................................................... 3
C. Access to co-trimoxazole prophylaxis for infants and children ........................................................................................... 4
I I I . RATIONALE AND RECOMMENDATIONS ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
A. Rationale ........................................................................................................................................................................................................................................................ 5
B. WHO recommendations ........................................................................................................................................................................................................... 6
C. Adherence ................................................................................................................................................................................................................................................... 6
D. Discontinuation of co-trimoxazole prophylaxis .......................................................................................................................................... 7
IV. CHALLENGES ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
V. KEY STRATEGIES FOR SCALING UP ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Government leadership, ownership and accountability ......................................................................................................................... 9
Integration of co-trimoxazole prophylaxis into existing services .............................................................................................12
Use of available entry points to initiate co-trimoxazole prophylaxis....................................................................................15
Reliable procurement and supply management mechanisms ...................................................................................................19
Strengthened community-based capacity ........................................................................................................................................................... 22
Strengthened monitoring and evaluation systems .....................................................................................................................................24

vi
VI. CONCLUSION ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26APPENDICES .......................................................................................................................................................................................................................................................... 27
Appendix A: WHO recommendations for co-trimoxazole prophylaxis for infants and children ...............27
Appendix B: Generic HIV algorithm used for the Integrated Management of Childhood Illness (IMCI) programme .......................................................................................................................................30
Appendix C: Zambia child health card ..................................................................................................................................................................................31
Appendix D: Sample dosing card for co-trimoxazole prophylaxis (Columbia University) ............................... 33
Appendix E: Rapid assessment tool for scaling up co-trimoxazole prophylaxis ........................................................ 34
Appendix F: Assessment of staffing needs .................................................................................................................................................................. 38
Appendix G: Resources for co-trimoxazole prophylaxis .............................................................................................................................. 39
REFERENCES ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40

vii
EXECUTIVE SUMMARY
Co-trimoxazole prophylaxis is safe, inexpensive and highly effective in reducing morbidity and mortality among HIV-infected infants and children. The World Health Organization (WHO) recommends that all HIV-exposed infants be started on co-trimoxazole prophylaxis at four to six weeks of age, in order to provide adequate prevention against early opportunistic infections (OIs). This is particularly critical for HIV-infected infants. Data from a randomized clinical trial conducted in Zambia demonstrated the effectiveness of co-trimoxazole prophylaxis in reducing mortality and morbidity among HIV-infected children, despite high levels of bacterial resistance. Other studies have also demonstrated the effectiveness of co-trimoxazole prophylaxis in HIV-infected children, adolescents and adults across the spectrum of CD4 counts, and across varying levels of bacterial resistance. Benefits to be accrued from co-trimoxazole prophylaxis are particularly important in resource-limited settings where access to effective services for prevention of mother-to-child transmission (PMTCT) of HIV, effective infant-feeding interventions, early diagnostic services and antiretroviral therapy (ART) for children remain limited.
Globally, in 2007, about 2 million children below the age of 15 years were living with HIV. In that year alone, 370 000 children were newly infected with HIV, more than 90% of them as a result of mother-to-child transmission (MTCT) of HIV, and 270 000 children died of HIV-related causes. While HIV care and treatment services for HIV-infected children are slowly expanding in resource-constrained settings, they are still very limited and lag behind treatment services available for adults.
An important component of the HIV care and treatment package for children is the provision of co-trimoxazole prophylaxis. This widely available, inexpensive antibiotic is recommended for HIV-exposed or -infected children to prevent the development of serious, often fatal, OIs, notably Pneumocystis jiroveci pneumonia (PCP) in young HIV-infected infants. However, despite the fact that countries have developed and put in place policies to support the scale up and implementation of co-trimoxazole prophylaxis for infants and children, and that it is inexpensive, life-saving, safe and theoretically simple to deliver, the United Nations Children’s Fund (UNICEF), WHO and partners estimate that in 2008, only 8% of children exposed to HIV were initiated on co-trimoxazole prophylaxis by two months of age.
One of the main challenges countries must address in order to scale up co-trimoxazole prophylaxis is the absence of mechanisms to systematically identify and follow up HIV-exposed infants at and after birth. If HIV-infected children are to be identified early in the course of their disease – a prerequisite for receiving co-trimoxazole prophylaxis and early ART – systems need to be in place to ensure that health workers consider the possibility of HIV infection in infants at birth and at all clinic or other health encounters thereafter. Antenatal messages for HIV-infected women need to routinely include anticipatory guidance aimed at improving postnatal follow up of mother–infant pairs through education and information of parents and caregivers It is also critical to inform and mobilize communities to ensure that HIV-exposed infants and children are identified and families are aware of available services for prevention and treatment for young infants and children, and the benefits of early use of care services.

viii
This document provides a brief review of evidence supporting the use of co-trimoxazole prophylaxis in children and summarizes common barriers to implementation. It proposes specific actions and strategies needed for scaling up co-trimoxazole prophylaxis, including the following:
1. Government leadership, ownership and accountability for provision of co-trimoxazole prophylaxis to HIV-exposed and -infected infants and children. This entails developing policies, setting national targets and making budgeted national plans to reach infants and children in need;
2. Delivery of co-trimoxazole prophylaxis for children through such existing services as HIV and maternal, newborn and child health (MNCH), and decentralization of delivery to the lowest appropriate, effective and feasible level of the health-care system;
3. Maximized use of all available entry points to ensure timely initiation of co-trimoxazole prophylaxis. This will be facilitated through the use of provider-initiated HIV testing and counselling (PITC) to identify HIV-exposed and -infected infants and children, use of child health cards with HIV-specific information, and outreach services including immunization and home-based care;
4. Developing reliable national- and district-level procurement and supply management mechanisms that ensure a consistent supply of co-trimoxazole for paediatric co-trimoxazole prophylaxis needs;
5. Strengthened community-based capacity to identify HIV-exposed and -infected infants and children, and provide referrals for testing, care (including initiation and continuation of co-trimoxazole prophylaxis) and treatment;
6. Strengthened monitoring and evaluation systems to support the provision of high-quality care for children who are HIV-infected or -exposed, including the provision of co-trimoxazole prophylaxis.

1
II. INTRODUCTION
Co-trimoxazole prophylaxis is safe, inexpensive and highly effective in reducing morbidity and mortality among HIV-infected infants and children, as well as in adolescents and adults. Ideally, all infants exposed to HIV should be started on co-trimoxazole prophylaxis during the first four to six weeks of life, as recommended by the World Health Organization (WHO). This period is particularly critical for HIV-infected infants. Providing co-trimoxazole prophylaxis protects against serious, often fatal, opportunistic infections (OIs) and leads to improvement in the quality of life of HIV-infected infants while reducing the burden of care on health-care systems and caregivers. In situations where antiretroviral therapy (ART) is not readily available, the use of co-trimoxazole prophylaxis will increase the chances of survival of HIV-infected infants until ART can be initiated. This is particularly important in resource-limited settings where access to effective services for prevention of mother-to-child transmission (PMTCT) and ART remains limited.
Key points
• Co-trimoxazole prophylaxis can cut mortality in half and reduce hospital admissions of children.
• Co-trimoxazole prophylaxis is inexpensive, and costs about US$ 0.03 per child per day, or about US$ 10/child/year.
• In 2008, 1.4 million women with HIV gave birth in low- and middle-income countries.
• All babies born to these mothers with HIV should receive co-trimoxazole prophylaxis but the estimated coverage of such infants is only 8%.
Globally, in 2007, about 2 million children below the age of 15 years were living with HIV. In that year alone, 370 000 children were newly infected with HIV, over 90% as a result of mother-to-child transmission (MTCT), and 270 000 children died of HIV-related causes.1 Most of these deaths occurred in sub-Saharan African countries where seroprevalence rates among women of reproductive age are extremely high and where health services, including programmes that can prevent and treat paediatric HIV, are still limited.
In resource-rich settings, the rate of HIV transmission from HIV-infected pregnant women who have access to a comprehensive package of PMTCT services to their infants is less than 2%.2 Unfortunately, in 2008, antiretrovirals (ARVs) or ART to prevent MTCT, a crucial component of PMTCT services, reached only about 45% of pregnant women with HIV in low- and middle-income countries.4 In addition, most women received prophylaxis with only single-dose nevirapine (NVP), a regimen that is less effective than combination ARV regimens in reducing MTCT.
While HIV care and treatment services for HIV-infected children in resource-constrained settings are slowly expanding, they are still very limited and lag behind treatment services available for adults. The widely available antibiotic co-trimoxazole is an important preventive element of HIV care and is recommended for the prevention of OIs, notably Pneumocystis jiroveci pneumonia (PCP), and its use for this indication is referred to as co-trimoxazole prophylaxis.

2
IDespite the existence of national policies for co-trimoxazole prophylaxis and the fact that it is inexpensive, lifesaving, widely available, safe and theoretically easy to deliver, the United Nations Children’s Fund (UNICEF), WHO and partners estimate that in 2008, only about 8% of children exposed to HIV were initiated on co-trimoxazole prophylaxis by two months of age.4
This document proposes actions needed to scale up co-trimoxazole prophylaxis. It is intended:
• to provide practical information on the role of co-trimoxazole prophylaxis in maternal and child health (MCH) and HIV programming,
• to review current barriers to rapid, effective scaling up of co-trimoxazole prophylaxis, and
• to provide strategies and tools to facilitate scale up.
The principal audiences for this document include national, provincial and district-level programme managers, planners, trainers and implementing partners.

3
I I . HIV INFECTION IN INFANTS AND CHILDREN
A. Epidemiology and cl inical overview
Globally, over 90% of children with HIV live in sub-Saharan Africa, where seroprevalence rates among women of reproductive age remain high. The vast majority of these infants were infected in utero, during delivery or after birth through breastfeeding. For infants infected during pregnancy or delivery, HIV disease progression is particularly rapid, with mortality rates exceeding 50% in the first year of life. Access to co-trimoxazole prophylaxis and early ART is life-saving for such infants.
Just as in adults, HIV in children damages the immune system; thus, opportunistic and other infections are more common and more severe. In addition, children in resource-limited settings are exposed to a greater burden of pathogens associated with early morbidity and mortality, irrespective of HIV status. Co-trimoxazole prophylaxis can prevent the development of some of the most serious opportunistic and common childhood infections.
HIV-uninfected infants born to HIV-infected women also have greater morbidity and mortality than HIV-unexposed infants and children. Many infections in children born to mothers with HIV, regardless of the infant’s eventual HIV status, can be prevented by timely initiation of co-trimoxazole prophylaxis.
To maximize the benefits of co-trimoxazole prophylaxis, it should be started before HIV infection can be confirmed and prior to the development of HIV-related signs or symptoms.
B. Access to diagnosis and treatment of HIV
It is essential to institute systems which ensure that infants known to be HIV exposed are followed regularly and tested using an HIV viral test at four to six weeks after birth to identify HIV infection before it becomes symptomatic. This would enable early initiation of ART for HIV-infected infants. Exposed infants also need to have adequate infant-feeding support and counselling, as well as other important HIV care and treatment interventions.
Access to HIV viral tests (which are recommended for the diagnosis of HIV in infants) has increased in recent years, largely as a result of the introduction of dried blood spot (DBS) specimen collection on filter paper. When test results are promptly provided and acted upon, and treatment is initiated early in infancy, HIV-infected infants experience significantly reduced morbidity and mortality (Children with HIV Early Antiretroviral Therapy [CHER] study).5 In most settings, however, health workers continue to wait and test only at 18 months with HIV antibody tests. Initiation of co-trimoxazole prophylaxis is particularly important in these settings as it affords the possibility of delaying the onset of OIs in HIV-infected infants prior to confirmatory diagnosis and subsequent initiation of ART.
HIV antibody testing conducted early in life can confirm HIV exposure as it detects persisting maternal HIV antibody in the infant. Antibody testing is therefore useful in identifying infants not previously known to be HIV exposed so that they too may benefit from the protection from OIs afforded by co-trimoxazole prophylaxis. It is also useful in identifying HIV-uninfected and -unexposed infants.6 HIV antibody testing is therefore an important intervention to screen infants and young children for HIV
II

4
IIexposure in high HIV-burden settings, so as to identify those in need of co-trimoxazole prophylaxis and HIV viral testing.
Of the 2 million children infected with HIV in 2007, the vast majority of those estimated to be in need of ART were not receiving it,7 despite the UNICEF/Joint United Nations Programme on HIV/AIDS (UNAIDS) target of providing ART, co-trimoxazole prophylaxis or both to 80% of children in need by 2010.7 While access to ART remains limited for children, use of co-trimoxazole prophylaxis may be lifesaving.
C. Access to co-tr imoxazole prophylaxis for infants and chi ldren
Data regarding the current need for and uptake of co-trimoxazole prophylaxis globally for both HIV-exposed and -infected infants are difficult to obtain as many countries have only recently begun to collect and report data on this intervention. UNICEF and WHO, however, are working with countries to develop systems that support more accurate reporting on this in the future. Data regarding initiation of co-trimoxazole prophylaxis in HIV-exposed infants were first reported in 2007. Approximately 1.4 million women with HIV gave birth in low- and middle-income countries and all of these children should have been initiated on co-trimoxazole prophylaxis by four to six weeks of age. However, 2008 estimates reveal that only about 8% of infants needing co-trimoxazole prophylaxis had been started on it by two months of age.4

5
I I I . RATIONALE AND RECOMMENDATIONS
A. Rat ionale
Co-trimoxazole is a combination of two antibiotics – sulfamethoxazole and trimethoprim. It is widely available in a number of forms and is known by several brand names. The most common use of co-trimoxazole is for the first-line management of acute respiratory infections (ARI) in children, but it is also used to treat diarrhoea and PCP, as well as infections of the urinary tract and middle ear.
To prevent PCP in HIV-infected individuals, co-trimoxazole has been the standard of care in high-income countries for many years, based on a number of studies that have demonstrated its benefits, primarily in HIV-infected adults.8 There were initial concerns by some policy-makers and MCH experts that widespread use of co-trimoxazole as prophylaxis would undermine its efficacy in the management of ARI, and would lead to problems of antibiotic resistance in common pathogens. More recent studies have not substantiated such fears and have demonstrated population-level benefit. These studies are discussed in the WHO co-trimoxazole prophylaxis guidelines.8
It has also been recognized that co-trimoxazole prophylaxis provides benefits beyond the prevention of PCP. A randomized controlled trial among HIV-infected children in Zambia demonstrated that mortality was reduced by half and the number of hospital admissions was significantly reduced among children using co-trimoxazole.9 These findings, along with other evidence of efficacy and cost-effectiveness, as well as fewer deaths due to ARI in HIV-infected infants under the age of six months,10,11 have highlighted the benefits of co-trimoxazole prophylaxis for infants and children with HIV.
Co-trimoxazole prophylaxis also protects against episodes of malaria (estimated 99.5% protection from pooled data).12 Mortality from malaria in HIV-infected children and adults is also reduced if they are on co-trimoxazole (pooled data estimates RR 0.62 [0.51–0.74] comparing HIV-infected persons on co-trimoxazole with HIV-infected subjects not on co-trimoxazole).13 A similar reduction in mortality was seen in a subgroup of children below five years of age (RR 0.68, 0.51–0.91) in the Children with HIV Antibiotic Prophylaxis (CHAP) study from Zambia.9
In addition to the clinical benefits of co-trimoxazole prophylaxis for the prevention of OIs associated with HIV disease, other benefits include the following:14
• it can be delivered to children at levels of the heath-care system that cannot yet offer ART.
• it can be provided through a family-based approach as the benefits of co-trimoxazole prophylaxis are important for both adults and children.
• it encourages drug adherence behaviours before initiation of ART.
• it can reduce the burden of communicable diseases in the index case and other family members, and;
• it can prevent malaria.
Finally, co-trimoxazole prophylaxis is a low-cost intervention, with a unit cost of only about US$ 0.03 per child per day, or about US$ 10/year.15
III

6
IIIB. WHO recommendat ions
The WHO guidelines provide recommendations and related evidence for the use of co-trimoxazole prophylaxis.8
• HIV-exposed infants and children: In settings with a high prevalence of HIV, high infant mortality due to infectious diseases and limited health-care infrastructure, WHO recommends co-trimoxazole prophylaxis for all HIV-exposed infants and children, starting at four to six weeks after birth and maintained until at least six weeks after cessation of risk of HIV transmission and definitive exclusion of HIV infection in infants.
• HIV-infected infants and children:
> For infants with confirmed HIV infection who are less than one year of age, co-trimoxazole prophylaxis is indicated regardless of the CD4 percentage or clinical status.
> For infants and children one through four years of age, initiation of co-trimoxazole prophylaxis is recommended if the child has WHO clinical stages 2, 3 or 4, regardless of CD4 percentage, or if the child has a CD4 percentage <25 at any WHO stage. Countries are advised that they may choose to institute universal co-trimoxazole prophylaxis for all HIV-infected infants and children irrespective of the clinical or immunological stage.
> For children 5 years of age or older, WHO’s adult guidelines should be followed.8
Children with a history of treated PCP should be administered the same regimen of co-trimoxazole prophylaxis as that recommended for primary prevention.
More detailed recommendations from WHO on eligibility, formulations and dosages, initiation of secondary co-trimoxazole prophylaxis, and discontinuation of co-trimoxazole prophylaxis can be found in Appendix A.8
C. Adherence
Adherence may be challenging when co-trimoxazole prophylaxis is given to very small infants, and in infants who need to take co-trimoxazole prophylaxis for long periods of time. Ensuring good adherence is an ongoing process that begins at the first clinical encounter and continues at every subsequent interaction with the caregiver. Adequate initial and ongoing counselling is critical to achieving good adherence. Initial counselling can help caregivers identify factors that may interfere with adherence, while ongoing counselling both reinforces positive trends and allows for the detection of emerging issues. Helping caregivers develop cues based on daily life activities that trigger medication administration is a particularly useful technique for improving long-term adherence.
Emphasis on adherence training and implementation of adherence strategies need to be as strong in community-based programmes as in clinical programmes. Community-based organizations (CBOs), existing home-based care services and women’s groups will require comprehensive training in treatment literacy and adherence support.
Imperfect adherence to co-trimoxazole prophylaxis should not, however, be a reason to discontinue it, as prevention efficacy is maintained even with thrice-weekly dosing. While the benefits may be reduced with less-than-perfect adherence, it is likely that there will still be some benefit.

7
IIIImproving adherence through once-daily dosing
Baylor International Pediatric AIDS Initiative (BIPAI) initiated once-daily dosing of co-trimoxazole prophylaxis at its Center of Excellence in Gaborone, Botswana. Families have reported that this has made adherence to co-trimoxazole prophylaxis easier as they no longer have to think about which days of the week they need to administer co-trimoxazole prophylaxis to their infants.
D. Discont inuat ion of co-tr imoxazole prophylaxis
Co-trimoxazole prophylaxis may need to be discontinued in the event of an adverse drug reaction. Although severe reactions to co-trimoxazole are uncommon, these may include extensive exfoliative rash, Stevens–Johnson syndrome, or severe anaemia or pancytopenia.
Guardians and caregivers should be provided with verbal or written information on the potential adverse effects, and advised to stop the drug and report to their nearest health facility if co-trimoxazole-related adverse events are suspected. Current evidence is insufficient to recommend discontinuation of co-trimoxazole prophylaxis once the child is stable on effective ART.

8
IV. CHALLENGES
Several barriers have been identified to effective, broad national scale up of co-trimoxazole prophylaxis. These include the following:
1. Inadequate policies, operational guidelines and plans for co-trimoxazole prophylaxis: By 2008, while most resource-limited countries had integrated co-trimoxazole prophylaxis into national policy documents on PMTCT, ART and maternal, newborn and child health (MNCH), there remained a lack of sufficiently detailed operational guidance to advise national programme managers on exactly how co-trimoxazole prophylaxis is to be scaled up at the health-service level.
2. Limited integration of PMTCT services within MCH and ART programmes, and weak links between these programmes and other child health services: PMTCT services are the crucial link to timely identification of HIV-exposed infants who are eligible for co-trimoxazole prophylaxis. However, because of the traditional practice of vertical programming, PMTCT services are often not sufficiently integrated into MCH programmes, making it difficult to monitor mothers and infants.16 Mothers and infants are often seen separately at clinics, even when they are both in need of HIV services, bringing other factors such as time, transportation and cost into play as additional barriers.
3. Missed opportunities to identify infants and children in need of co-trimoxazole prophylaxis and other HIV services: Many infants born to HIV-infected mothers do not receive appropriate interventions, including co-trimoxazole prophylaxis, because they are not identified as being HIV-exposed. Such missed opportunities are the result of a lack of appropriate training of health-care workers, limited use of clinic tools such as child health cards documenting HIV exposure status, or absence of systems whereby health workers providing care to children make HIV assessment a routine part of their initial interaction with the child. In addition, many other children showing early signs and symptoms of HIV infection remain untested for HIV infection because of lack of training or absence of facilitative policies. Frequently, communities have also not been sufficiently informed or sensitized to identify HIV-exposed infants and children so that they can be referred to care.
4. Other barriers: Other constraints that limit health workers’ ability to implement co-trimoxazole prophylaxis include limited policy support for lower-level workers to dispense co-trimoxazole prophylaxis, insufficient training on the importance of co-trimoxazole prophylaxis of those allowed to prescribe and dispense it, and failure to include co-trimoxazole prophylaxis in training materials for HIV care and treatment.
In terms of supplies, barriers include insufficient quantities of co-trimoxazole made available for prophylaxis, a lack of clarity on sharing of supplies across programmes, inadequate procurement policies and procedures, and problems with storage and distribution.
IV

9
V. KEY STRATEGIES FOR SCALING UP
Six key strategies are essential for scaling up co-trimoxazole prophylaxis for HIV-exposed and -infected children.
1. Ensure government leadership, ownership and accountability for the provision of co-trimoxazole prophylaxis to HIV-exposed and -infected infants and children. These are demonstrated by the formulation of supportive policies, setting of national targets and development of budgeted national plans for scaling up, directed towards reaching all children in need.
2. Integrate co-trimoxazole prophylaxis for children into existing services. These include services such as HIV and MNCH, and decentralized delivery to the lowest appropriate, effective and feasible level of the health-care system.
3. Maximize the use of all available entry points to ensure timely initiation of co-trimoxazole prophylaxis. This can be facilitated through the use of child health cards with HIV-specific information as well as through PITC to identify HIV-exposed and HIV-infected infants and children as part of outreach services, immunization and home-based care.
4. Develop reliable national- and district-level procurement and supply management mechanisms. These ensure a consistent supply of co-trimoxazole for prophylaxis of infants and children in need.
5. Strengthen community-based capacity to identify HIV-exposed and -infected infants and children. This is necessary for referral to testing, care (including initiation and continuation of co-trimoxazole prophylaxis) and treatment.
6. Strengthen monitoring and evaluation systems. Such systems support the provision of high-quality care for children who are exposed to or infected with HIV, including the provision of co-trimoxazole prophylaxis.
The action steps needed to incorporate each of these strategies into national programmes are outlined below.
Strategy 1
Ensure government leadership, ownership and accountability for provision of co-trimoxazole prophylaxis for HIV-exposed and -infected infants and children, demonstrated by the formulation of supportive policies, setting of national targets and development of budgeted national plans for scaling up co-trimoxazole prophylaxis so as to reach all children in need.
Effective leadership, ownership, programme management and coordination capacity are needed at the national and subnational levels (such as districts) to promote and support the scaling up of co-trimoxazole prophylaxis for eligible children.
V

10
VRelevant actions
1.1 Conduct a situational analysis
An initial rapid, brief but systematic situational analysis should be performed1 to assess current levels of programming. This should include key health system bottlenecks to provision of co-trimoxazole prophylaxis so that national MNCH and/or HIV strategic plans can revised and/or adapted to better address the provision of co-trimoxazole prophylaxis.
A tool for such an assessment can be found in Appendix E. Key elements to be assessed in the situational analysis include the following:
• Epidemiological profile (e.g. number of HIV-infected pregnant women giving birth annually, number of children exposed to or infected by HIV, proportion of eligible children currently receiving co-trimoxazole prophylaxis);
• Health system capacity to provide co-trimoxazole for prophylaxis (e.g. level of health facility able to provide co-trimoxazole prophylaxis, training provided, level of decentralization of PMTCT and other HIV care delivery);
• National policies and guidelines that refer to co-trimoxazole prophylaxis (e.g. indications for use of co-trimoxazole prophylaxis in national policies and guidelines, including who can prescribe and dispense);
• Operational plans to complement policies and guidelines (e.g. existence of a paediatric HIV care and treatment plan, and inclusion of co-trimoxazole prophylaxis in the plan, a system for identifying children requiring co-trimoxazole prophylaxis, provision of training, and development and distribution of job aids for co-trimoxazole prophylaxis);
• Financial, logistical and human resources available to implement co-trimoxazole prophylaxis; and
• Monitoring and evaluation system (e.g. use of national-level indicators for co-trimoxazole prophylaxis, data analysis and quality improvement activities focused on co-trimoxazole prophylaxis).
1.2 Establish co-trimoxazole prophylaxis-related targets
Time-bound targets are essential to scale up interventions as learned from recent experience (i.e. WHO’s 3 by 5 Initiative, the US President’s Emergency Plan for AIDS Relief [PEPFAR’s] 2-7-10 goals) because they set a tone of urgency and motivate national programme managers to take action. Population-based or geographically based targets can also be used locally to drive planning: for example, co-trimoxazole prophylaxis targets for urban areas will probably differ from the targets for rural areas. Setting district-level targets is also important, since it assigns expectations and accountability, and assists in coordinating supportive technical assistance, including targeted training for health-care providers and ensuring that appropriate quantities of supplies reach the sites in need. Decisions regarding district- and subdistrict-level targets will need to be based on considerations of local capacity to prescribe co-trimoxazole prophylaxis, particularly in areas where health centres do not have a medical doctor or officer on the staff, and nurses or other health-care workers do not have the capacity to prescribe and dispense co-trimoxazole prophylaxis. Establishing targets can also be useful for leveraging and mobilizing resources as they provide a quantifiable and measurable understanding of the country’s expectations for scaling up.
27 Ideally, information regarding usage of co-trimoxazole prophylaxis should be collected as part of existing situational
analyses addressing HIV care and MCH to expedite implementation and maximize the use of valuable resources.

11
V1.3 Ensure that existing management and coordination structures focus on the needs
of children affected by HIV (exposed and infected) and address co-trimoxazole prophylaxis for children.
The relevant management and coordinating body should:
• Include co-trimoxazole prophylaxis for children in national scale-up plans for PMTCT of HIV as well as those for care and treatment.
• Develop appropriate policies to facilitate the initiation of co-trimoxazole prophylaxis for children. Examples of such policies include but are not limited to:
> PITC recommended for sick children in sites likely to have large numbers of children who have HIV such as paediatric wards, tuberculosis units and malnutrition clinics, as well as all children of adults receiving ART to identify those eligible for co-trimoxazole prophylaxis;
> using mechanisms to communicate a child’s HIV exposure or infection status both within facilities as well as between sites, such as with child health cards on which HIV exposure status is documented to facilitate initiation of co-trimoxazole prophylaxis;
> utilizing well-baby services such as clinics providing immunization or growth monitoring to routinely assess infants and young children for HIV-exposure status;
> providing co-trimoxazole prophylaxis and other paediatric HIV services free of user charges for children;
> revising national scopes of practice to permit additional types of health workers to prescribe and dispense co-trimoxazole prophylaxis for children;
> using community case management programmes addressing pneumonia, malaria and diarrhoea to identify HIV-exposed children in need of co-trimoxazole prophylaxis; and
> using community-based HIV testing and counselling programmes to identify exposed and infected infants and children in need of co-trimoxazole prophylaxis.
These policies should be incorporated into site preparation processes, standard operating procedures and personnel expectations, and actively disseminated so that they are implemented.
• Review and adapt existing guidelines pertinent to delivering co-trimoxazole prophylaxis to children. WHO has developed guidelines specifically focused on co-trimoxazole prophylaxis for adults and children, which can be adapted for national use.8 Other guidelines developed by WHO17 also refer to co-trimoxazole prophylaxis for children and may be of use in revising national guidelines on the following:
> PITC and infant diagnosis18
> services for PMTCT2
> ART for children19
> patient monitoring guidelines19
> infant and young child feeding20
> tuberculosis21
> malaria22,23
> Integrated Management of Childhood Illness (IMCI)24

12
VWhere co-trimoxazole is currently recommended, national management guidelines for ARI, malaria, diarrhoea and dysentery may need to be reviewed and aligned to incorporate this.
• Develop dissemination and communication strategies/materials to raise awareness of revised policies and guidelines. Ensure that the reach of communication materials extends to community and other local care providers.
• Coordinate the training of health-care workers. As governments move to decentralize the delivery of paediatric HIV care and treatment including co-trimoxazole prophylaxis, there will be a need for coordinated national training. District-level coordination is essential to ensure that training is applied consistently across sites and reaches all the providers who need it. Supportive supervision is also essential to ensure that the knowledge and skills obtained during training sessions are effectively translated into their day-to-day work.
1.4 Ensure district-level leadership, ownership and accountability for the scale up of co-trimoxazole prophylaxis.
To ensure effective increases in the uptake of co-trimoxazole prophylaxis, it is essential that critical government functions extend beyond the national level to much lower levels of the government such as the district level. District-level managers should be involved in district-level planning and implementation of the national policy on co-trimoxazole prophylaxis, coordination of local training, setting of site-specific targets, provision of supportive supervision, and monitoring of the quality of care delivered.
• Integrate commodity needs specific to co-trimoxazole prophylaxis for infants and children who are exposed to or have HIV into national procurement and supply management systems (see the section on supply management [Strategy 4]).
• Integrate indicators on co-trimoxazole prophylaxis for children into monitoring and evaluation systems (see the section on monitoring and evaluation [Strategy 6]).
Strategy 2
Integrate co-trimoxazole prophylaxis for children into existing services such as HIV and MNCH, and decentralize delivery to the lowest appropriate and feasible level of the health-care system.
Decentralized delivery of co-trimoxazole prophylaxis and other HIV care through an integrated package of services for the child and family offers several advantages:
• It delivers care for all family members at the same time and place;
• It minimizes costly and time-consuming transport to and from tertiary centres;
• It facilitates the continuity of care between the home, community and health centre; and
• It maximizes efforts to improve adherence and overcome barriers to long-term engagement in care.

13
VIncreasing the provision of co-trimoxazole prophylaxis in five districts in Rwanda: the impact of district planning, training and supportive supervision
Following a district action planning exercise as part of the National Conference on Paediatric HIV in Rwanda in 2007, BASICS has provided support to five selected districts to improve the performance of PMTCT and paediatric HIV services. The provision of co-trimoxazole prophylaxis to HIV-exposed and -infected children has been integrated into the national Integrated Management of Neonatal and Childhood Illness (IMNCI)–HIV–Birth Spacing training module in 25 districts and in the district paediatric HIV action plans in five districts in Rwanda. A co-trimoxazole prophylaxis indicator has been integrated into the IMNCI supervision and monitoring tool for the districts. In a review of 16 health facilities in five districts after implementation of the action plan training for paediatric HIV, the number of children receiving co-trimoxazole prophylaxis increased from 522 in September 2007 to 715 by March 2008. This indicated a 36% increase in the number of children who received co-trimoxazole prophylaxis following training of health-care workers to identify HIV-exposed and -infected children and place them on co-trimoxazole prophylaxi. Source: Mary Lyn Field-Nguer, BASICS
Relevant actions
2.1 Integrate initiation of co-trimoxazole prophylaxis into existing MNCH programmes.
Existing MNCH programmes include specific services such as immunization, which are well established, well attended and have high penetration into the communities being targeted. MNCH clinics therefore provide the greatest potential for expanding services for co-trimoxazole prophylaxis, as virtually all HIV-exposed infants will be there during their first year of life. Ministries of health interested in increasing the coverage and uptake of co-trimoxazole prophylaxis should concentrate initial efforts on ensuring that MNCH settings are able to identify HIV-exposed children, start co-trimoxazole prophylaxis and refer for other essential HIV services.
At present, however, these programmes often do not address the HIV-related needs of children such as co-trimoxazole prophylaxis. Health-care workers can more effectively recognize when infants and children need HIV testing and co-trimoxazole prophylaxis if the child health card includes information related to services for PMTCT. In addition to recognizing HIV-exposed children who appear otherwise well, health-care workers should also be trained and directed to ensure that HIV infection is considered in the diagnosis of infants and young children who present with an illness to child health services. Acute care services for infants and children must be able to provide age-appropriate HIV testing and counselling and initiate co-trimoxazole prophylaxis (see also 3.1).

14
VApproach to HIV diagnosis, care, support and treatment through Integrated Management of Childhood Illness (IMCI)
Several countries (Botswana, Ethiopia, Kenya, Lesotho, Namibia, Rwanda, South Africa, Swaziland, Uganda, Zambia and Zimbabwe) have adapted their IMCI materials to include HIV and AIDS. The IMCI HIV guidelines are similar to the existing syndromic guidelines for common childhood illnesses, since they provide health-care workers with a checklist to determine whether a child might be either exposed to or infected with HIV. The first question during the child assessment is whether the mother received an HIV test during antenatal care (ANC). Depending on the answer received and the presence or absence of other symptoms including pneumonia, persistent diarrhoea or severe malnutrition, the health-care worker can classify the child into different HIV exposure and infection categories, and determine the next steps to follow in the child’s care plan, including initiation of co-trimoxazole prophylaxis.25
Swaziland: Improving early postnatal care
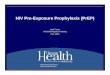
Early postnatal care is the most neglected area of maternal and newborn health (MNH) in developing countries. It provides an opportunity to identify and address problems, including infection with HIV in postpartum women and exposure of their newborn babies. In Swaziland, one of the countries with the highest HIV prevalence in the world (39% among pregnant women in 2007), BASICS and partners implemented the integration of focused, quality postnatal care for all postpartum women and their newborn babies. One of the objectives of this intervention was to improve the follow up and care of HIV-positive mothers and their exposed babies, who were being lost to care after being identified by the national PMTCT programme during ANC. This facility-based programme included training of health staff involved in MNH care, facilitation of organizational changes needed to provide the new postnatal care services, and supportive supervision of personnel providing the care. An evaluation carried out one year after initiation of the service showed a significant increase in the proportion of both HIV-positive postpartum women and their infants started on co-trimoxazole prophylaxis as a result of counselling during the early postnatal visits (within one week of birth), from 47% to 65%, and from 13% to 37%, respectively (P<0.01). Providers also confirmed that HIV-positive postpartum women received the relevant or appropriate follow-up care and treatment.

15
VCotrimoxazole prophylaxis in HIV positive mothers
and their exposed infants
100
47
65
Mother******p<0.01 Baby***
13
37
80
Per
cent
of
mo
ther
s &
bab
ies
rece
ivin
g c
otr
imo
xazo
le
du
rin
g P
P p
erio
d
60
40
20
Baseline 2006
Endline 2007
Source: Mazia G et al. Integrating quality postnatal care into PMTCT in Swaziland. Global Public Health Journal, 2009 (in press).26
2.2 Decentralize delivery of co-trimoxazole prophylaxis to the lowest levels of the health system.
Health-care workers with minimal clinical background or experience in HIV care and treatment can effectively deliver co-trimoxazole prophylaxis. Community leaders and health-care workers need to understand that co-trimoxazole preventive treatment is a low-cost and easy-to-deliver intervention that can dramatically reduce morbidity and mortality. By using community-based channels or health outreach services, as well as local pharmacies and drug vendors, co-trimoxazole prophylaxis can be provided much closer to where children who need it live.
Decentralization of co-trimoxazole prophylaxis requires district-level planning. District-level managers will need to be involved in implementation of the national policy for co-trimoxazole prophylaxis, development of site-specific targets, coordination of local training, provision of supportive supervision and ensuring the quality of care delivered.
Strategy 3
Maximize the use of all available entry points to ensure timely initiation of co-trimoxazole prophylaxis. This will be facilitated through the use of PITC to identify HIV-exposed and -infected infants and children, as well as through outreach services including immunization and home-based care.
A. Optimize the follow up of known HIV-exposed infants identified through services for PMTCT.
Although many countries are moving towards national coverage of services for PMTCT, most children born to women known to be living with HIV are not being systematically monitored and followed up during the postpartum period. HIV-exposed children must be followed up to minimize the risk of postpartum HIV transmission and improve infant health outcomes through provision of co-trimoxazole prophylaxis and other essential services including ARV prophylaxis for the infant, early infant diagnosis, and infant-feeding counselling and support.

16
VRelevant actions
3.1 Ensure the availability of policy and technical guidance supporting the follow up of infants known to be exposed to HIV through their connection to PMTCT services so that co-trimoxazole prophylaxis may be initiated and they may receive other essential interventions in a timely manner.
3.2 Document information on the child’s HIV exposure/infection status including receipt of PMTCT services by the mother and child on MNCH cards to facilitate initiation of co-trimoxazole prophylaxis for eligible infants.
Health-care workers providing care to either the mother or the infant can use health cards with HIV exposure and infection status documented on it to facilitate initiation of HIV-related follow up of the infant. Health cards, in addition to carrying information such as height, weight, immunization history, should note whether the child is known to be HIV exposed or infected, and can contain some or all of the following information:
• HIV status of the mother;
• ARVs provided to the mother and/or infant;
• HIV testing status of the infant; and
• whether co-trimoxazole prophylaxis was initiated for the mother or infant.
Lesotho: Optimizing follow up on HIV-exposed infants
Lesotho’s example of creating a stamp that can be stamped at birth into the child’s bukana (portable health record) is illustrative. The stamp is designed to be applied to the bukanas of all children born to mothers known to be HIV-infected. It is the size of one of the bukana’s small pages, and includes a prompt to the paediatric care provider to ensure that the child is initiated on co-trimoxazole prophylaxis at four to six weeks after birth or as soon thereafter as the child’s first encounter takes place. The stamp may even be placed in a bukana to be given to a child after birth, providing a critical opportunity for the maternal care provider to ensure, at the moment the mother tests positive, that the newborn infant will be identified as HIV exposed. All of this helps link the need for co-trimoxazole prophylaxis from the prenatal or delivery setting to the initial clinical setting in which the child is cared for – even when these are space- and time-separated, as is commonly the case. Lesotho has shown a strong commitment to this concern at the central level by incorporating the information on the stamp into a permanent page in the new bukana.
Source: Michael A. Tolle, Lineo Thahane, Tony Garcia-Pratts, Baylor International Pediatric AIDS Initiative (BIPAI)
This approach has also been successfully used in several other countries, including Zambia and Zimbabwe. Health-care workers are made aware by looking at either the mother’s or child’s health card that the child has been exposed to HIV and are prompted to ensure that important interventions including provision of co-trimoxazole prophylaxis and early diagnostic testing are implemented. In addition, this ensures that both the mother and the child are followed more carefully to monitor for any signs suggestive of HIV infection. The health-care worker who provides the first set of immunizations

17
Vto the child at six weeks of age is ideally positioned to review the child’s HIV status and provide the necessary HIV-related services such as co-trimoxazole prophylaxis or HIV testing, or refer the child for it. For this mechanism to work, at a minimum, the following must be in place.
• Information on services for PMTCT, including the child’s HIV exposure status, must be documented on the child’s health card and included on the mother’s health card (Figure 1).
• Children’s health cards must be distributed in a timely fashion at or around delivery. Some countries now provide the pregnant woman living with HIV with a child health card documenting HIV exposure status at the time she receives her HIV result.
• Information on the child health card or mother–baby booklet must be standardized nationally and follow nationally agreed-upon guidelines.
• Health-care workers must be oriented to and vested in the utility of this information.
• Measures must be taken to ensure patient confidentiality.
Health-care workers in ANC should also sensitize pregnant women with HIV to inform the child’s health-care provider of the child’s exposure status so that he/she can receive the necessary interventions at the six-week clinic visit.
Figure 1. PMTCT panel from child health card used in Zambia
CHILD’S PARTICULARS IMMUNISATION RECORD
Boy/Girl
NRC no.
NRC no.
Birth weightDate of Birth
Mother’s or Guardian’s Name
Father’s or Guardian’s Name
Where the family lives: address
IMMUNISATION against Tuberculosis (TB)BCG (at birth) Date ..............................
Date .......................................
Date ....................................
Date ...........................................
Date ..........................................
Date Date Dosage Dosage
Dosage: 0-5 months, 50,000 IU only if not breastfed; 6-11 months,100,000 IU; 12-59 months, 200,000 IU every six months
Date ....................................................
Date ....................................
Date .....................................................
Date .....................................................
Date ..............................................
(at least 4 weeks after DPT-HepB-Hib1)
(at least 4 weeks after OPV 2)
(at 9 months, only if OPV 0 was not given)
(at 9 months, or soon after. Unless symptomatic HIV)
(at least 4 weeks after OPV 1)
(at least 4 weeks after DPT-HepB-Hib 2)
OPV 0 (at birth to 13 days)
OPV 1 (at 6 weeks)
OPV 2
OPV 3
OPV 4
Date
Date
VITAMIN A SUPPLEMENTATION
OTHER IMMUNISATIONS
Measles
DPT-HepB-Hib 1 (at 6 weeks)
DPT-HepB-Hib 3
DPT-HepB-Hib 2
Date ..............................If no scar after 12 weeks, repeat dose. Unless symptomatic HIV
IMMUNISATION against Polio (OPV), Diphtheria, Whooping Cough, Tetanus, Hib, Hepatitis B, Meningitis, Pneumonia(DPT-HepB-Hib) & Measles
DEWORMING
Date Medication
Vitamin A (1 dose of 200,000 IU) to be given soon after birth or within two months of delivery.
MOTHER
Date Vit. A given to the mother
Birth weight less than 2.5kg
Born within 2 years of last delivery
Fully protected against Tetanus at birth
Number of brothers and sisters
Any other reason for special attention:
Dead
Dead
Alive
Alive
For children aged 12 months and above, 500 mg Mebendazole every six months
Name of Health Facility
Child’s No.
Child’s Name
Date first seen
Place of Birth:
Date Medication
Tick if the child has/is:
Birth defect/handicap
Mother dead
Father dead
Twin child
CHILDREN’S CLINIC CARD
IF THE CHILD HAS DIARRHOEA
Note: (dilute 1 sachet of ORS in 1 litre of boiled cooled water)
� If the child is still on breast milk, continue breast feeding.
After each loose stool, do the following:
� Give ORS � Give extra fluids � Continue to feed the child.
Go immediately to the nearest Health Centre.
PNEUMONIAIf a child has a cough with: � Fast Breathing � Difficulties in breathing� Difficulties in breast-feeding The child may have Pneumonia, Go immediately to the nearest Health Centre.
IMPORTANT: � All infants and young children should be breastfed exclusively for
the first six months of life and continue to breastfeed up to two years and beyond with adequate complementary feeding from six months of age unless medically indicated.
� Babies born to HIV positive mothers have special feeding needs. Discuss with a health worker.
� Feeding during and after illness � Safe food and drinking water� Treatment of diarrhoea� HIV/AIDS� Malaria
� Breastfeeding� Complementary feeding� Immunisation� Vitamin A supplementation� Family planning
DISCUSSFollow up time
Infant feeding code
Follow up time
Infant feeding code
Feeding Code:
1) Exclusive breast feeding (in the first 6 months, breast-feeding only, no water,
no other fluids except medicines indicated by medical personnel)
2) Exclusive Alternative Infant Formula
3) Animal Milk
4) Mixed feeding (breast milk and other foods)
5) Continued breast feeding after six months in addition to other foods
6) Milk based feed after six months in addition to other foods
7) Other, specify
.......................................................................................................................
......................................................................................................................
MONITORING OF INFANT AND YOUNG CHILD FEEDING
Birth
7M
6 Days
8M
6W
9M
1M
10M
2M
11M
3M
12M
4M 5M 6M
15M 18M 24M
Date baby referred for ART............/.........../..........
Date initiated on ART............../.............../.............
Age at initiation of ART.........................................
CE
MGA
Rapid Test
Rapid Test
PCR
R NR IDATE
IGA
Follow up time
Cotrimoxazole
Follow up time
Cotrimoxazole
MSU CNE
Test by:
PMTCT
8M
2 Months6 Weeks
9M
3M
10M
4M
12M
5M
15M
6M
18M
7M
24M
652
1212
1812
Ministry of Health
Source: Ministry of Health, Government of Zambia

18
VB. Identify infants and children who have HIV and are eligible for co-trimoxazole
prophylaxis.
The vast majority of infants who have HIV are currently not identified through PMTCT or routine MCH services but are diagnosed when they present to inpatient and outpatient health services with signs and symptoms suggestive of HIV infection. A large number of children who have HIV have been identified through PITC in acute care settings in many countries including Cameroon, Uganda, Zambia and others.
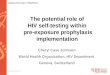
For example, a study on the referral patterns of HIV care and treatment for children in Malawi found that only 1% of the children referred for ART come from services for PMTC. The vast majority (80%) are identified as a result of HIV testing conducted in children’s wards or nutritional rehabilitation units (Figure 2).27 These children should usually be immediately initiated on ART and co-trimoxazole prophylaxis.
Figure 2. Referral sources for antiretroviral therapy for children in Malawi
Wards, nutritional rehabilitation units (80%)
Clinic of person receiving ART (1%)
Follow up of preventionof mother-to-child transmission (1%)
Antiretroviraltherapy clinic for children
Clinic for childrenyounger than 5 years (18%)
Source: Report of a country-wide survey of HIV/AIDS services in Malawi for the year 2006.27
Relevant actions
3.3 Implement PITC at sites likely to yield a high volume of positive HIV test results to identify infants and children in need of co-trimoxazole prophylaxis and other HIV services.
Protocols and systems should be established for routinely recommending HIV testing for hospitalized children, those attending malnutrition clinics, those with TB and those younger than five years with other signs and symptoms suggestive of HIV infection such as severe pneumonia, severe persistent diarrhoea, ear discharge or very low weight for age. Infants and children identified as exposed to or infected with HIV should be promptly initiated on co-trimoxazole prophylaxis and ART, if indicated.

19
VUse of PITC to identify HIV-infected infants and children
In all of its African sites, BIPAI promotes PITC in multiple clinical settings where children are cared for, particularly inpatient wards and outpatient clinics. In Lesotho, BIPAI helped to institute PITC of all children admitted to the inpatient paediatric ward at the national hospital in Maseru. This has helped identify HIV-exposed and HIV-infected children who would otherwise have escaped detection, and ensure their enrolment in HIV/AIDS care, treatment and support services, including the administration of co-trimoxazole prophylaxis.
Source: Michael A. Tolle, Baylor International Pediatric AIDS Initiative (BIPAI)
3.4 Institutionalize a family-centred approach and secure HIV testing for all additional family members once an index case is identified.
If one family member is identified as having HIV infection, it is very important to recommend HIV testing and counselling for the other family members. In many families, more than one person has HIV. Programmes can help ensure that all family members are tested by requiring information on all other family members on a person’s health card, including information on HIV testing. Ensure co-trimoxazole prophylaxis for mother and baby/child as indicated.
3.5 Use approaches such as the IMCI and Integrated Management of Adolescent and Adult Illness (IMAI) to identify infants and children at peripheral sites in need of HIV testing and co-trimoxazole prophylaxis.
IMCI has a modified algorithm for assessing children presenting to primary health facilities.25 The algorithm is designed to optimize management of infants and children exposed to or infected with HIV. For the HIV-exposed child, health-care workers are guided to ensure that the child receives appropriate interventions including co-trimoxazole prophylaxis and early testing. First-level health-care workers should be trained to improve their ability to recognize a child who may have HIV (as in the HIV-adapted IMCI approach). This involves training health workers including private sector pharmacists and drug sellers to recognize signs and symptoms that are common among children who have HIV, and provide basic care and appropriate referrals. The generic IMCI HIV algorithm is given in Appendix B.
3.6 Use community health workers to facilitate entry to diagnosis and care services.
Ensure that the community health workers providing community-based case management or treatment for common childhood infections such as diarrhoea, pneumonia, malaria and fever are able to recognize the signs of HIV infection, refer for HIV testing, and provide co-trimoxazole prophylaxis as required.
Strategy 4Develop reliable national- and district-level procurement and supply management mechanisms that ensure a consistent supply of co-trimoxazole for paediatric prophylaxis needs.
In the context of HIV care and treatment for children, a well-functioning supply system is critically important to ensure that children who need commodities and other material resources for routine HIV care (including medicines to prevent and treat common OIs) can access them when and where they need them.

20
VAs for all health-care commodities, the steps for establishing a functioning supply management system can be structured according to the processes in the supply cycle: selection, procurement (including quantification), distribution (including inventory management), use, and the organizational and managerial functions underpinning them.
Relevant actions
4.1 Ensure that supply management is appropriately coordinated among supply stakeholders and also linked to the overall implementation plan. Where there is a working group on procurement and supply management of drugs for HIV, integrate co-trimoxazole prophylaxis for infants and children into the existing mechanism.
4.2 Develop estimates of need and determine additional resource requirements for co-trimoxazole products taking into account:
• Requirements for HIV and non-HIV use, and current national and partner contributions to both
• National guideline recommendations for starting and continuing co-trimoxazole prophylaxis in infants and children
• Formulation and dosage requirements for each age/weight group
• Co-trimoxazole prophylaxis targets disaggregated by age/weight group
• Other providers such as faith-based organizations, implementing partners and accredited private providers providing services on behalf of the government
• Areas where interruptions in co-trimoxazole supply for non-HIV use commonly occur. Identify requirements and funding to fill the gap to avoid depleting stocks ordered for co-trimoxazole prophylaxis.
For determination of budget requirements and potential procurement sources, the following sources may be consulted:
1. International drug indicator price guide28 (Management Sciences for Health [MSH]), which provides an indication of pharmaceutical prices on the international market, and
2. Global Price Reporting Mechanism (WHO).29
4.3 Select products containing co-trimoxazole and confirm registration status.
• Select appropriate formulations (syrup, paediatric tablets or adult tablets), minimizing, where possible, the number of products that will need to be procured, stored and distributed.
• Determine if soluble, scored tablets and/or products that are formulated to be cut will be needed.
• Confirm that the products are registered in-country and determine if the essential medicines list (EML) will need to be revised to include co-trimoxazole for prophylaxis.
• Determine criteria to assure the quality of co-trimoxazole products (e.g. those manufactured according to Good Manufacturing Practices [GMP], or have undergone post-test evaluation).

21
V4.4 Plan for procurement and distribution.
• Foster integration of co-trimoxazole supply systems for HIV and non-HIV use where possible by building on what exists and strengthen capacity where it is lacking.
• Define the procurement strategy for co-trimoxazole prophylaxis. Consider the availability of donations, and whether procurement for co-trimoxazole prophylaxis can be integrated into existing procurement methods, for example, for essential medicines.
• Consider sourcing and pricing (see resources listed above under section 4.2).
• Regularly update procurement and distribution plans to match revised co-trimoxazole prophylaxis targets and distribution at new sites.
• Determine the distribution mechanisms for reaching sites and ensure that the supply of co-trimoxazole reaches the level of the community-based worker.
• Secure adequate storage space in warehouses and facilities.
• Ensure that reporting systems provide up-to-date data on co-trimoxazole consumption for HIV and non-HIV use to inform demand forecasting and supply management.
4.5 Plan for co-trimoxazole use.
• Determine what quantities of co-trimoxazole will be given at the first and subsequent clinic visits; and the procedure to be used for evaluating the infant for resupply.
• Review practice codes and laws related to who can dispense co-trimoxazole. Ensure that nurses, medical officers and community health workers are able to dispense co-trimoxazole prophylactically.
• Disseminate guidelines and develop job aids for all staff responsible for dispensing and providing medication counselling to clients and caregivers.
• Review local knowledge on the determinants of adherence to other paediatric medicines and take appropriate steps to promote adherence to co-trimoxazole prophylaxis.
• Issue guidance on sharing supplies across programmes to respond to stock-outs.

22
VRwanda: Managing procurement and supply to support scaling up of co-trimoxazole prophylaxis
In Rwanda, the Government and Ministry of Health have adopted a policy of providing co-trimoxazole prophylaxis to all HIV-exposed and -infected children. Infants born to HIV-positive mothers receive co-trimoxazole prophylaxis for six months following birth. At this point, co-trimoxazole prophylaxis is discontinued for those infants who test negative for HIV. The Ministry of Health uses the Coordinated Procurement and Distribution System (CPDS) established in 2006 for ARV medicines to coordinate the procurement of co-trimoxazole products among funders, including the Rwandan Government and its partners. CPDS coordinates the national quantification of co-trimoxazole products for HIV use and pooled procurement through Centrale d’Achat de Médicaments Essentiels du Rwanda (CAMERWA), the national public sector medicine procurement and supply agency, and the leader of the CPDS Implementation Committee. These estimates are then approved by the Resource Management Commission, which is chaired by the Permanent Secretary of the Ministry of Health. CAMERWA is also responsible for quantifying and procuring co-trimoxazole for non-HIV use for public and faith-based health facilities. Procurements are coordinated with the Bureau des Formations Médicales Agréées au Rwanda (BUFMAR), which also procures and distributes co-trimoxazole to faith-based facilities for non-HIV use. Although the quantification and procurement processes are not yet integrated, CAMERWA stores and distributes co-trimoxazole supplies for both HIV and non-HIV use, and the same products are used for both. Public and faith-based health facilities and district pharmacies report co-trimoxazole consumption for each programme to the central level in two separate monthly reports to facilitate quantification and reporting to funders.
Source: Personal communications from the Pharmacy Task Force of the Ministry of Health (MOH), the Treatment and
AIDS Research Center (TRAC Plus), CAMERWA, the Permanent Secretary of the MOH and Management Sciences for
Health Strengthening Pharmaceutical Services (MSH/SPS) Rwanda office.
Strategy 5
Strengthen community-based capacity to identify HIV-exposed and -infected infants and children and refer for testing, care (including initiation and continuation of co-trimoxazole prophylaxis) and treatment.
Community-based strategies are an important way of optimizing initiation and continued delivery of co-trimoxazole prophylaxis for children who are exposed to or who have HIV, particularly for families living far from health centres. Infants and children with HIV will only gain access to diagnosis, care and treatment if their parents and caregivers, and the frontline health-care workers and nongovernmental organizations (NGOs) serving the households where they live are informed about how HIV affects infants and children, that there is hope through early treatment, and how to access these services.

23
VRelevant actions
5.1 Integrate community-based approaches into MNCH and HIV programming strategies.
For community-based strategies for co-trimoxazole delivery to be effective, several components must be in place. These include:
• Incorporating community strategies for basic HIV care and support, such as monitoring of co-trimoxazole prophylaxis, in national treatment and care plans;
• Establishing policies that support the role of community health-care workers to provide basic HIV-related care such as initiation and monitoring of co-trimoxazole prophylaxis; and
• Incorporating co-trimoxazole prophylaxis in the core educational content of community health workers.
In planning for community-based strategies, the time commitment and caseloads of community health workers, particularly those who work as volunteers or receive a small stipend, cannot be expected to be the same as those for full-time workers, who may also earn more substantial financial compensation for their efforts. For community health workers to be effective, their workload must be manageable and fit in with their other responsibilities.
5.2 Accelerate case-finding through integration into community health programmes for other childhood illnesses.
Identifying young children with HIV infection or exposure is important so that they can be given appropriate care, including co-trimoxazole prophylaxis, and can benefit from life-saving ART. Community options for case-finding can be built into existing community health services such as regularly scheduled outreach MNCH services and delivery of integrated services through child health days, community IMCI, home-based care, community nutrition programmes and other child care activities driven by NGOs and CBOs. Infants and young children identified as HIV exposed or suspected of being HIV infected should be initiated on co-trimoxazole prophylaxis and referred for HIV testing to the nearest facility. Where community IMCI is in place, integrate HIV case-finding and follow up into protocols, training and referral processes.
5.3 Enhance community capacity to provide co-trimoxazole prophylaxis and other HIV-related care and support.
Community health workers can be instrumental in sustaining long-term delivery of co-trimoxazole prophylaxis and ART, as well as other interventions for HIV-infected children such as nutritional and adherence counselling, psychosocial support , and the management of simple, common side-effects. The use of peer-to-peer approaches, maternal support groups and community health workers can help support adherence to co-trimoxazole prophylaxis and ART by ensuring a resupply of medications and routinely reviewing the health plans with caregivers. Community health workers currently doing community case management for pneumonia, malaria and diarrhoea are an excellent source of provision for co-trimoxazole prophylaxis to infants and young children who are HIV-exposed or -infected.

24
VStrategy 6
Strengthen monitoring and evaluation systems to support the provision of high-quality care for children who are exposed to or who have HIV, including the provision of co-trimoxazole prophylaxis.
WHO and UNICEF have recently reviewed and revised existing guidance on monitoring and evaluation of services for PMTCT, ART, and HIV care and support.30 The guidance was revised to better reflect the recent technical revisions to recommendations on ART and HIV care and support, including co-trimoxazole prophylaxis.
The indicator specific to co-trimoxazole prophylaxis reads as follows: Percentage of infants born to women living with HIV started on co-trimoxazole prophylaxis before two months of age.
6.1 National programmes should ensure that registers used in the HIV and MNCH programmes contain entry points to capture and record initiation and monitoring of co-trimoxazole prophylaxis.
Relevant actions
These registers are instrumental in prompting health workers to provide the appropriate service in a timely manner. They also assist governments in monitoring progress in terms of scale up, and identifying better- and poorer-performing facilities for documentation of best practices or provision of supportive supervision.
6.2 Child health cards should be modified to allow for recording of co-trimoxazole prophylaxis for all HIV-exposed infants.
Child health cards containing HIV-specific information are essential to ensure appropriate follow-up care for HIV-exposed infants, and can therefore contribute significantly to reduced infant and child morbidity and mortality (see Appendix C).
6.3 Initiation and adherence monitoring of co-trimoxazole prophylaxis should be selected as a quality improvement indicator and prioritized as an area for improvement.
Problems with the quality of care being delivered are frequently linked to systems. The quality of HIV care for children can often be improved by simply introducing basic documentation tools. For example, introducing a basic checklist into a child health chart can help remind health-care providers about the importance of specific interventions such as initiation and continuation of co-trimoxazole prophylaxis.

25
VA quality improvement initiative for co-trimoxazole prophylaxis
The following graphical presentation shows the results of a quality improvement initiative focused on the administration of co-trimoxazole prophylaxis for HIV-exposed children at three sites in Lesotho during the period October 2007 to September 2008. Coverage with co-trimoxazole prophylaxis for HIV-exposed infants improved dramatically, with all sites achieving over 85% coverage during this period.
CTX Prophylaxis Oct-07 – Sept-08
700
Ntsekhe
500
600
Nu
mb
er o
f ch
ildre
n
400
200
300
100
0
Exposed Children
CTX Prophylaxis
134 127
Mabote
586513
Mafeteng
436382
Improvement was attributed to the following:
• Improved logistics supply management of co-trimoxazole syrup for infants
• Ongoing training of staff in the follow up/care of HIV-exposed children
• Regular supportive supervision in the Under-5 Clinics
• Creation of a one-stop shopping centre for early infant diagnosis and co-trimoxazole dispensing in MCH settings
Source: Personal communication, International Center for AIDS Care and Treatment Programs, Lesotho
Many facilities in a geographical area may experience similar challenges to the provision of co-trimoxazole prophylaxis. Sharing of experiences between different health facilities can lead to sharing of successful strategies and overall group learning.

26
VI. CONCLUSION
Co-trimoxazole prophylaxis is safe, inexpensive and highly effective in reducing morbidity and mortality among HIV-infected infants and children. Ideally, all infants exposed to HIV should be started on co-trimoxazole prophylaxis in the first four to six weeks of life. Coverage, however, remains unacceptably low. One of the main challenges countries face in scaling up uptake is the absence of mechanisms to systematically identify and follow up HIV-exposed infants at and after birth. Systems need to be in place to ensure that health workers consider the possibility of HIV infection in infants at birth, and at all clinic or other health encounters thereafter, so that this intervention can be provided on a timely basis.
This guide was developed to assist national programme managers and implementing partners to effectively implement and rapidly scale up the uptake of co-trimoxazole prophylaxis within the context of existing HIV and MNCH programmes. The specific actions proposed include: (1) enhance government leadership; (2) deliver co-trimoxazole prophylaxis through existing services; (3) optimize identification and follow up of HIV-exposed infants and sick infants of unknown HIV status; (4) develop reliable national- and district-level procurement and supply management mechanisms; (5) strengthen community capacity to identify HIV-exposed and -infected infants; and (6) strengthen monitoring and evaluation systems for co-trimoxazole prophylaxis.
VI

27
APPENDICES
APPENDIX A : WHO RECOMMENDATIONS FOR CO-TRIMOX AZOLE PROPHYLA XIS FOR INFANTS AND CHILDREN
Table 1. Initiation of co-trimoxazole prophylaxis in infants and children
Situation
HIV-exposed infants and childrena
Infants and children confirmed to be living with HIVb
<1 year 1–4 years >5 years
Co-trimoxazole prophylaxis is universally indicated, starting at four to six weeks after birth and maintained until risk of HIV transmission ceases and HIV infection is excluded
Co-trimoxazole prophylaxis is indicated regardless of CD4 percentage or clinical statusc
WHO clinical stages 2, 3 and 4 regardless of CD4 percentage
OR
Any WHO stage and CD4 <25%
Follow adult recommendations
OR
Universal option: prophylaxis for all infants and children born to mothers confirmed to be or suspected of living with HIV. This strategy may be considered in settings with a high prevalence of HIV, high infant mortality due to infectious diseases and limited health infrastructure.
a. Defined as a child born to a mother living with HIV or a child breastfeeding from a mother living with HIV until HIV exposure stops (six weeks after complete cessation of breastfeeding) and infection can be excluded.
b. Among children younger than 18 months, HIV infection can only be confirmed by HIV viral testing.
c. Once a child is started on co-trimoxazole, prophylaxis should continue until five years of age regardless of clinical symptoms or CD4 percentage. Specifically, infants who begin co-trimoxazole prophylaxis before the age of one year and are subsequently asymptomatic and/or have CD4 levels >25% should remain on co-trimoxazole prophylaxis until they reach the age of five years.
APPENDICES

28
APPENDICES
Table 2. Dosages of commonly used co-trimoxazole formulations for infants and children living with or exposed to HIV
Recommended daily dosagea
Suspension
(5 ml of syrup 200 mg/40 mg)
Child tablet
(100 mg/20 mg)
Single-strength adult tablet
(400 mg/80 mg)
Double-strength
adult tablet
(800 mg/ 160 mg)
<6 months or <5 kg
100 mg sulfamethoxazole/ 20 mg trimethoprim
2.5 ml One tablet mixed with feed or small amount of milk or water
¼ tablet, possibly mixed with feed or small amount of milk or waterb
–
6 months–5 years or 5–15 kg
200 mg
sulfamethoxazole/ 40 mg trimethoprim
5 mlc Two tablets Half tablet –
6–14 years or 15–30 kg
400 mg sulfamethoxazole/ 80 mg trimethoprim
10 mlc Four tablets One tablet Half tablet
>14 years or >30 kg
800 mg sulfamethoxazole/ 160 mg trimethoprim
– – Two tablets One tablet
Frequency – once a day
a. Some countries may use weight bands rather than age to determine dosing.
b. Splitting tablets into quarters is not considered best practice. This should be done only if syrup is not available.
c. Children of these ages (6 months–14 years) may swallow crushed tablets.
Source: World Health Organization. Guidelines on co-trimoxazole prophylaxis for HIV-related infections among children,
adolescents and adults. Recommendations for a public health approach. Geneva, WHO, 2006:15 (Table 3). http://www.who.
int/hiv/pub/guidelines/ctxguidelines.pdf8
(Two tables have been combined to include both age and weight).

29
APPENDICES
Children with a history of treated PCP should be administered secondary co-trimoxazole prophylaxis with the same regimen recommended for primary prophylaxis.
Table 3. Summary of recommendations for discontinuing primary co-trimoxazole prophylaxis among infants and children
Target population Recommendations
HIV-exposed children Discontinue co-trimoxazole prophylaxis after HIV infection is excluded
Infants and children living with HIV
Maintain on co-trimoxazole prophylaxis until the age of five years, irrespective of clinical and immune response
Children older than five years can be reassessed and consideration given to discontinuing co-trimoxazole prophylaxis in accordance with the recommendations for adults and adolescents
The general recommendation is that secondary co-trimoxazole prophylaxis should not be discontinued, irrespective of the clinical and immune response to ART.
Source: World Health Organization. Guidelines on co-trimoxazole prophylaxis for HIV-related infections among children,
adolescents and adults. Recommendations for a public health approach. Geneva, WHO, 2006.Available at: http://www.who.
int/hiv/pub/guidelines/ctxguidelines.pdf (accessed on 28 July 2009).8

30
APPENDICES
APPENDIX B : GENERIC HIV ALGORITHM USED FOR THE INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS ( IMCI )
Source: World Health Organization/United Nations Children’s Fund. Integrated Management of Childhood Illness for high HIV
settings: chart booklet. Geneva, WHO Department of Child and Adolescent Health, 2008:20–21.25
SIGNS CLASSIFY IDENTIFY TREATMENTS
• Positive HIV antibody test for child 18 months and above
OR
• HIV positive virological test
CONFIRMEDHIV INFECTION
¾ Treat, counsel and follow-up existing infections
¾ Give co-trimoxazole prophylaxis
¾ Give vitamin A supplement from 6 months of age every 6 months
¾ Assess the child’s feeding and provide appropriate counseling to the mother
¾ Refer for further assessment including HIV care/ART
¾ Follow-up in 14 days, then monthly for 3 months then every three months or as per immunization schedule
One or both of the following
• Mother HIV positive and no test result for child
OR
• Child less than 18 months with positive antibody test
HIV EXPOSED/POSSIBLE HIV
¾ Treat, counsel and follow-up existing infections
¾ Give co-trimoxazole prophylaxis
¾ Give vitamin A supplement from 6 months of age every 6 months
¾ Assess the child’s feeding and provide appropriate counseling to the mother
¾ Confirm HIV infection status of child as soon as possible with best available test
¾ Follow-up in 14 days, then monthly for 3 months then every three months or as per immunization schedule
• 2 or more conditions
AND
• No test results for mother and child
SUSPECTEDSYMPTOMATICHIV INFECTION
¾ Treat, counsel and follow-up existing infections
¾ Give co-trimoxazole prophylaxis
¾ Give vitamin A supplement from 6 months of age every 6 months
¾ Assess the child’s feeding and provide appropriate counseling to the mother
¾ Test to confirm HIV infection
¾ Refer for further assessment including HIV care/ART
¾ Follow-up in 14 days, then monthly for 3 months then every three months or as per immunization schedule
• Less than two conditions
AND
• No test result for mother or child
SYMPTOMATIC HIV INFECTIONUNLIKELY
¾ Treat, counsel and follow-up existing infections
¾ Advise the mother about feeding and about her own health
¾ Encourage HIV testing
• Negative HIV test result in mother or child AND not enough signs to classify as suspected symptomatic HIV infection
HIV INFECTIONUNLIKELY
¾ Treat, counsel and follow-up existing infections
¾ Advise the mother about feeding and about her own health
THEN CHECK FOR HIV INFECTION*
¾ Has the mother or child had an HIV test?
OR
¾ Does the child have one or more of the following conditions?:
• Pneumonia**
• Persistent diarrhoea**
• Ear discharge (acute or chronic)
• Very low weight for age**
If yes to one of the two questions above, enter the box below and look for the following conditions suggesting HIV infection:
Classify for HIV Infection
NOTE OR ASK:
LOOK AND FEEL :
• PNEUNOMIA?
• PERSISTENT
• DIARRHOEA?
• EAR DISCHARGE?
• VERY LOW WEIGHT?
• Oral Thrush
• Parotid enlargement
• Generalized persistent lymphadenopathy
*A child who has already been put on ART does not need to be assessed with this HIV box
**Includes severe forms such as severe pneumonia... In the case of severe forms, complete assessment quickly and refer child URGENTLY

31
APPENDICES
APPENDIX C : ZAMBIA CHILD HEALTH CARD
CH
ILD
’S P
AR
TIC
UL
AR
SIM
MU
NIS
AT
ION
RE
CO
RD
Boy/
Girl
NR
C n
o.
NR
C n
o.
Birth
weig
ht
Date
of B
irth
Moth
er’s
or
Guard
ian’s
Nam
e
Fath
er’s
or
Guard
ian’s
Nam
e
Where
the fam
ily li
ves:
addre
ss
IMM
UN
ISA
TIO
N a
ga
inst
Tu
be
rcu
losi
s (T
B)
BC
G (
at
birth
)D
ate
..............................
Date
.......................................
Da
te
....
....
....
....
....
....
....
....
....
Da
te .
....
....
....
....
....
....
....
....
....
....
..
Da
te
....
....
....
....
....
....
....
....
....
....
..
Da
te
Da
te
Do
sa
ge
Do
sa
ge
Do
sag
e:
0-5
mo
nth
s, 5
0,0
00
IU
on
ly if
no
t b
rea
stfe
d;
6
-11
mo
nth
s,1
00
,00
0 I
U;
1
2-5
9 m
on
ths,
20
0,0
00
IU
eve
ry s
ix m
on
ths
Da
te
....
....
....
....
....
....
....
....
....
....
....
....
....
Date
....................................
Da
te .
....
....
....
....
....
....
....
....
....
....
....
....
....
Da
te .
....
....
....
....
....
....
....
....
....
....
....
....
....
Date
..............................................
(at le
ast
4 w
eeks
after
DP
T-H
epB
-Hib
1)
(at
lea
st 4
we
eks
aft
er
OP
V 2
)
(at 9
mon
ths,
onl
y if
OP
V 0
w
as n
ot g
iven
)(a
t 9 m
onth
s, o
r so
on a
fter.
U
nle
ss s
ympto
matic
HIV
)
(at
lea
st 4
we
eks
aft
er
OP
V 1
)
(at le
ast
4 w
eeks
after
DP
T-H
epB
-Hib
2)
OP
V 0
(a
t b
irth
to
13
da
ys)
OP
V 1
(
at
6 w
ee
ks)
OP
V 2
OP
V 3
OP
V 4
Date
Date
VIT
AM
IN A
SU
PP
LE
ME
NT
AT
ION
OT
HE
R I
MM
UN
ISA
TIO
NS
Measl
es
DP
T-H
epB
-Hib
1 (
at 6 w
eeks
)
DP
T-H
epB
-Hib
3
DP
T-H
epB
-Hib
2
Date
..............................
If n
o s
car
aft
er
12
we
eks
, re
pe
at
do
se.
Un
less
sym
pto
ma
tic H
IV
IMM
UN
ISA
TIO
N a
gain
st P
olio
(O
PV
), D
iphth
eria, W
hoopin
g
Cough, T
eta
nus,
Hib
, H
epatit
is B
, M
enin
giti
s, P
neum
onia
(DP
T-H
epB
-Hib
) &
Measl
es
DE
WO
RM
ING
Da
teM
ed
ica
tion
Vit
am
in A
(1
do
se o
f 2
00
,00
0 I
U)
to b
e g
ive
n s
oo
n a
fte
r b
irth
or
wit
hin
tw
o m
on
ths
of
de
liv
ery
.
MO
TH
ER
Da
te V
it. A
giv
en
to
th
e m
oth
er
Bir
th w
eig
ht
less t
han
2.5
kg
Bo
rn w
ith
in 2
years
of
last
delivery
Fu
lly p
rote
cte
d a
gain
st
Teta
nu
s a
t b
irth
Nu
mb
er
of
bro
thers
an
d s
iste
rs
An
y o
ther
reaso
n f
or
sp
ecia
l att
en
tio
n:
De
ad
De
ad
Aliv
e
Aliv
e
Fo
r ch
ildre
n a
ge
d 1
2 m
on
ths
an
d a
bo
ve,
50
0 m
g M
eb
en
da
zole
eve
ry s
ix m
on
ths
Na
me
of
He
alth
Fa
cilit
y
Child
’s N
o.
Child
’s N
am
e
Date
first
seen
Pla
ce o
f B
irth
:
Da
teM
ed
ica
tion
Tic
k if
the c
hild
has/is:
Bir
th d
efe
ct/
han
dic
ap
Mo
ther
dead
Fath
er
dead
Tw
in c
hild
CH
ILD
RE
N’S
CLIN
IC C
AR
D
IF T
HE
CH
ILD
HA
S D
IAR
RH
OE
A
Note
: (d
ilute
1 s
achet of O
RS
in 1
litr
e o
f boile
d c
oole
d w
ate
r)
�If the c
hild
is s
till
on b
reast m
ilk, continue b
reast fe
edin
g.
Aft
er
each
lo
ose s
too
l, d
o t
he f
ollo
win
g:
�G
ive O
RS
�
G
ive e
xtr
a flu
ids
� C
ontinue to feed the c
hild
.
Go
im
med
iate
ly t
o t
he n
eare
st
Healt
h C
en
tre.
PN
EU
MO
NIA
If a
child
has a
cough w
ith:
�F
ast B
reath
ing
�D
iffic
ulti
es in
bre
ath
ing
�D
iffic
ulti
es in
bre
ast-
feedin
g T
he c
hild
may h
ave P
neum
onia
, G
o im
med
iate
ly t
o t
he n
eare
st
Healt
h C
en
tre.
IMP
OR
TA
NT
: �
All
infa
nts
and y
oung c
hild
ren s
hould
be b
reastfed e
xclu
siv
ely
for
the first six
month
s o
f lif
e a
nd c
ontinue to b
reastfeed u
p to tw
o
years
and b
eyond w
ith a
dequate
com
ple
menta
ry feedin
g fro
m s
ix
month
s o
f age u
nle
ss m
edic
ally
indic
ate
d.
�B
abie
s b
orn
to H
IV p
ositiv
e m
oth
ers
have s
pecia
l feedin
g n
eeds.
Dis
cuss w
ith a
health w
ork
er.
�F
ee
din
g d
urin
g a
nd
aft
er
illn
ess
�S
afe
fo
od
an
d d
rin
kin
g w
ate
r�
Tre
atm
en
t o
f d
iarr
ho
ea
�H
IV/A
IDS
�M
ala
ria
�B
rea
stfe
ed
ing
�C
om
ple
me
nta
ry fe
ed
ing
�Im
mu
nis
atio
n�
Vita
min
A s
up
ple
me
nta
tio
n�
Fa
mily
pla
nn
ing
DIS
CU
SS
Fol
low
up
tim
e
Infa
nt f
eedi
ng c
ode
Fol
low
up
tim
e
Infa
nt f
eedi
ng c
ode
Fee
din
g C
ode:
1)E
xclu
sive
bre
ast
feed
ing
(in
the
firs
t 6
mon
ths,
bre
ast-
feed
ing
only
, no
wat
er,
no o
ther
flu
ids
exce
pt m
edic
ines
ind
icat
ed b
y m
edic
al p
erso
nnel
)
2)E
xclu
sive
Alt
erna
tive
Inf
ant
For
mul
a
3)A
nim
al M
ilk
4)M
ixed
fee
ding
(br
east
mil
k an
d ot
her
food
s)
5)C
onti
nued
bre
ast
feed
ing
afte
r si
x m
onth
s in
add
itio
n to
oth
er f
oods
6)M
ilk
base
d fe
ed a
fter
six
mon
ths
in a
ddit
ion
to o
ther
foo
ds
7)O
ther
, sp
ecif
y
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
...
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
..
MO
NIT
OR
ING
OF
IN
FA
NT
AN
D Y
OU
NG
CH
ILD
FE
ED
ING
Bir
th
7M
6 D
ays
8M
6W
9M1M
10M
2M 11M
3M 12M
4M5M
6M
15M
18M
24M
Dat
e ba
by r
efer
red
for
AR
T..
....
....
../.
....
....
../.
....
....
.
Dat
e in
itia
ted
on A
RT
....
....
....
../.
....
....
....
../.
....
....
....
Age
at
init
iati
on o
f A
RT
....
....
....
....
....
....
....
....
....
....
.
CE MG
A
Rapid
Test
Rapid
Test
PC
R
RN
RI
DA
TE
IGA
Fol
low
up
tim
e
Cot
rim
oxaz
ole
Fol
low
up
tim
e
Cot
rim
oxaz
ole
MS
UC
NE
Test
by:
PM
TC
T
8M
2 M
onth
s6
Wee
ks
9M
3M 10M
4M 12M
5M 15M
6M 18M
7M 24M
6 52
12
12
18
12
Min
istr
y of
Hea
lth

32
APPENDICES
Birth Weight Birth Date
3 m
ea
ls p
er
da
y
Weight (Kgs)
5 y
ears
3 m
ain
me
als
an
d 2
sn
ack
s p
er
da
y
3-5
year
s
2-3
year
s
3 m
ain
me
als
an
d 2
sn
acks p
er
da
y
+
++
4 ye
ars
5 ye
ars
WA
TC
H T
HE
DIR
EC
TIO
N O
F T
HE
LIN
E S
HO
WIN
G T
HE
CH
ILD
’S G
RO
WT
HG
OO
DM
ea
ns
the
ch
ildis
gro
win
g w
ell.
DA
NG
ER
SIG
NS
ug
ge
st f
ee
din
g t
he
child
at
lea
st 5
tim
es
ea
ch d
ay.
VE
RY
DA
NG
ER
OU
SC
hild
ma
y b
e il
l,n
ee
ds
ext
ra c
are
.
If inadequate
weig
ht
gain
for
2 m
onth
s or
more
, se
ek
medic
al
attentio
n
from
a
health
ca
re
pro
vider.
If
oedem
a o
n b
oth
feet, p
oin
t an a
rrow
on t
he g
row
th
curv
e a
nd t
hen s
eek
medic
al
attentio
n f
rom
neare
st
health
centr
e.
Bir
th -
6 m
on
ths
- 1
year
Kg
Kg
Kg
Kg
1 -
2 ye
ars
NU
TR
ITIO
N R
EC
OR
DR
ec
ord
of
vis
its
an
d n
utr
itio
n c
ou
ns
ell
ing
fo
llo
w u
p28
28
2727
2626
2525
2424
2323
23
2222
22
2121
212223
2121
2020
2020
20
1919
1919
19
1818
1818
18
1717
1717
1717
1616
1616
1616
1515
1515
1515
1414
1414
1414
1313
1313
1313
1212
1212
1212
1111
1111
11
1010
1010
10
99
99
88
88
77
7
66
6
55
44
33
22
11
00
Co
ntin
ue
bre
ast
fee
din
g a
nd
fe
ed
th
e c
hild
with
3 m
ain
me
als
a
nd
2 s
na
cks
pe
r d
ay.
Milk
Ric
e
Add these
oth
er
foods
to the
baby’
s porr
idge
or
giv
e w
ith
nsh
ima.
+
Use
a v
ariety
of lo
cally
ava
ilable
foods
such
as
vegeta
ble
s, k
apenta
, beans,
gro
undnuts
, sw
eet pota
toes,
cass
ava
, m
illet, r
ice, fr
esh
milk
or
sour
milk
, fr
uits
, oil.
Da
teN
utr
itional
statu
s A
dvic
eg
ive
nF
ollo
w u
pd
ate
1314
1516
1718
1920
2122
2324
2526
2728
2930
3132
3334
3536
3738
3940
4142
4344
4546
4748
4950
5152
5354
5556
5758
5960
11
22
33
44
55
66
77
88
99
1010
1111
1212
1325
3749
1426
3850
1527
3951
1628
4052
1729
4153
1830
4254
1931
4355
2032
4456
2133
4557
2234
4658
2335
4759
2436
4860

33
APPENDICES
APPENDIX D : SAMPLE DOSING CARD FOR CO-TRIMOX AZOLE PROPHYLA XIS
Trimethoprim/sulfamethoxazoleCTX/SMZ, Cotrimoxazole, Septrim®, Bactrim®
Age Suspension40 mg TMP/200 mg SMZ per 5ml
Single-Strength Tablet80 mg TMP/400 mg SMZ
< 6 months 2.5 ml daily 1/4 tab daily
6 months-5 years 5 ml daily 1/2 tab daily
6-14 years 10 ml daily 1 tab daily
> 14 years 2 single-strength orone double-strength tab daily
COTRIMOXAZOLE PROPHYLAXIS FOR INFANTS AND CHILDRENDOSING RECOMMENDATIONS
Updated June 2006
PEDIATRIC COTRIMOXAZOLE PROPHYLAXIS
Important prescribing information:
aCotrimoxazole is usually well-tolerated but should be regularlymonitored. Tolerance and adherence should be assessed atevery visit.
aThe most common side effects are gastrointestinal (nausea,vomiting, diarrhea); these are usually seen within two weeks ofinitiation.
aRash and fever are rare but reported side effects in children.
aMarrow suppression may lead to neutropenia and anemia,and caution is warranted when using cotrimoxazole with otherdrugs known to have hematologic toxicity. Where possible,initiation of cotrimoxazole and zidovudine (AZT, ZDV) should beseparated by 4-6 weeks.
aCotrimoxazole can also cause hepatitis, or asymptomaticincrease in liver enzymes (transaminitis). Where possible,initiation of cotrimoxazole and nevirapine-containing ARTshould be separated by 8-12 weeks.
aContraindications to cotrimoxazole include:
– Sulfa allergy– Severe renal insufficiency (creatinine > 3 times normal)– Severe hepatic insufficiency (LFTs > 5 times normal)
aDapsone may be used in place of cotrimoxazole whennecessary. The appropriate dose for children > 4 weeks of age is2 mg/kg/day.
Important information for parents:
aCotrimoxazole prevents serious infections in children with HIVand can help them feel better and live longer. It is not anantiretroviral drug, and does not treat or cure the HIV virus.
aCotrimoxazole may be given with or without food.
The prophylactic use of cotrimoxazole (Septrim®, Bactrim®,TMP/SMX, CTX, trimethoprim/sulfamethoxazole) is a criticallyimportant component of HIV care.
Pneumocystis pneumonia is a common and deadly infection,frequently seen in infants with HIV. It generally occurs betweenthree and six months of life, often as the first sign of HIVinfection and before the child’s HIV status has been determined.
Cotrimoxazole prophylaxis has been clearly shown to preventPneumocystis pneumonia and to save lives, and national andinternational treatment guidelines strongly support its use.
Pediatric cotrimoxazole prophylaxis is recommended for:
aAll HIV-exposed infants (e.g. all infants whose mothers areknown to have HIV) from 4-6 weeks of age until the child isno longer breast feeding and is determined to be uninfected
aAll HIV-infected infants < 12 months
aAll HIV-infected children 1- 4 years with:
• Clinical stage 2, 3 or 4 disease• CD4 < 25 %
aAll HIV-infected children > 5 years with:
• Clinical stage 3 or 4 disease• CD4 < 350
aAll HIV-infected infants and children with priorPneumocystis pneumonia.
All programs providing HIV/AIDS care should follow local and national treatment guidelines,which remain the final authority for country-specific protocols.
PEDIATRIC COTRIMOXAZOLE PROPHYLAXIS
www.columbia-icap.org
Source: International Center for AIDS Care and Treatment Programs (ICAP). Mailman School of Public Health, Columbia
University, New York, June 2006.

34
APPENDICES
APPENDIX E : RAPID ASSESSMENT TOOL FOR SCALING UP CO-TRIMOX AZOLE PROPHYLA XIS
The following rapid assessment tool is designed for use at the national and/or local and/or facility level, and ideally at all three levels. Ideally, specific relevant information from this assessment should be incorporated into routine assessments related to HIV and/or MNCH care. Information from this assessment should form the basis for improving policies, operations, training, and community education and mobilization so that more infants and children are reached with co-trimoxazole prophylaxis.
PROCESS
It is recommended that a review be conducted at sample sites where it is most likely that HIV-infected children are being seen. In most countries, this will include the following:
• ART sites
• General paediatric outpatient clinics
• Inpatient hospital units
• Homes visited by home-based care programmes
• PMTCT sites
• Health centres in high HIV-prevalence communities
• Tuberculosis clinics that see children
• Immunization and other child health outreach services.
A. Policy and planning
Answer yes (Y) or no (N) or respond as indicated.
1. Is co-trimoxazole prophylaxis for children addressed in national roll-out plans for HIV care, PMTCT and/or MNCH?
Insert funding total: 2. Which programme is responsible for funding co-trimoxazole products for prophylaxis? How much funding is available in total?
3. Have adequate resources for the co-trimoxazole prophylaxis roll-out/phase-in been identified, taking into account the number of eligible infants, current consumption and patterns of use?
4. Does a mechanism exist to coordinate co-trimoxazole prophylaxis roll-out/phase-in among stakeholders?
5. Do national ART guidelines, PMTCT guidelines and clinical care guidelines include co-trimoxazole prophylaxis for HIV-exposed and HIV-infected children?
6. Have these guidelines been disseminated to front-line health workers?

35
APPENDICES
7. Does the national treatment or case management guidelines for malaria, ARI, diarrhoea or dysentery include co-trimoxazole?
8. Are all required co-trimoxazole products registered in-country?
9. Is co-trimoxazole for prophylaxis included in the Essential Medicines List? What are the formulations listed for infants and children?
10. What is the cost of co-trimoxazole prophylaxis to the patient in public and private sector pharmacies and health service sites?
11. Is there a policy for user fees and waivers/exemptions for co-trimoxazole prophylaxis for infants and children?
12. Do policies allow for services that extend access to co-trimoxazole supply to the community level (for example, community case management of ARI or malaria?)
B. Systems, health management information systems (HMIS) and operations
Documentation and procedures available to identify and follow up HIV-exposed infants
1. Is maternal HIV status included on child health cards, maternal and paediatric record forms and registers?
2. Is provision of co-trimoxazole prophylaxis included on child health cards, maternal and paediatric record forms and registers?
Pharmaceutical management
a)______
b)______
c)______
3. How are co-trimoxazole supplies procured:
a) for use as an essential medicine?
b) for use as PCP prophylaxis?
c) Are the procurement mechanisms for different uses functionally integrated?
a)______
b)______
4. a) Are there annual quantification exercises that include management and prophylaxis use?
b) Is the process inclusive of programmes and partners for both HIV and non-HIV use?
a)______
b)______
c)______
5. How are co-trimoxazole supplies distributed:
a) for use as an essential medicine?
b) for use as prophylaxis?
c) Is the storage and distribution of co-trimoxazole products for different uses functionally integrated?

36
APPENDICES
6. Are there any issues with the procurement and distribution of co-trimoxazole formulations for infants and children?
a1)___ a2)___
b1)__ b2)___
7. Availability of co-trimoxazole products in warehouses and facilities visited
a) for use as an essential medicine
b) for use as prophylaxis
(1) at the time of visit (percentage of facilities where each product was available at the time of visit) and
(2) over the past year (average percentage of time out of stock in the past 6–12 months)
a)______
b)______
8. Have all orders for the past 6 months been received in full:
a) for use as an essential medicine?
b) for use as prophylaxis?
a)______
b)______
9. What percentage of stock records correspond with physical counts for co-trimoxazole products in (a) warehouses and (b) facilities visited?
10. Is there a policy/guidance on sharing supplies across programmes to fill gaps in availability?
11. Have requisition and reporting forms been updated to include co-trimoxazole for prophylactic use?
Prescribing and dispensing practices
12. Which health workers in which facilities are allowed to dispense co-trimoxazole to infants and children?
a)______
b)______
13. Are community health workers allowed to
(a) initiate co-trimoxazole prophylaxis?
(b) resupply co-trimoxazole prophylaxis after it has been initiated?
14. Are prescriptions required?

37
APPENDICES
a)______
b1)______
b2)______
b3)______
15. What are the current prescribing practices?
a) For which conditions is co-trimoxazole commonly prescribed?
b) Are prescriptions aligned with guideline recommendations (1) for government facilities, (2) for the NGO and private sectors, and (3) for community health workers?
16. Have job aids been developed to assist pharmacy and other dispensing staff to check the doses prescribed, and counsel patients and caregivers on medication use?
C. Health provider training
_____Nursing
_____Medical
_____Pharmacy
1. Is content on co-trimoxazole prophylaxis for infants and children included in the pre-service nursing, medical and pharmacy school curricula?
a. _______
b. _______
2. Is content on co-trimoxazole prophylaxis for infants and children included in
a) continuing education/in-service training?
b) If so, for which cadres of health workers?
a. __________
b. __________
3. Is content on co-trimoxazole prophylaxis for infants and children included in
a) adult and paediatric ART training?
b) What is the duration of training?
D. Knowledge and attitudes of clients and health workers
1. Please describe ongoing or planned community education and mobilization activities that include information on co-trimoxazole prophylaxis. Please attach related job aids or materials.
2. Describe PMTCT and other facility-based patient education efforts around co-trimoxazole prophylaxis for HIV-exposed and -infected children and non-HIV use of co-trimoxazole.

38
APPENDICES
APPENDIX F: ASSESSMENT OF STAFFING NEEDS
Existing staff will need to be assigned specific tasks to ensure all aspects of delivery of co-trimoxazole prophylaxis, from ordering to prescribing and ensuring adherence. Questions you need to ask to identify staffing needs include the following:
Who will be responsible for
• procuring supplies: assessing stock, placing orders, receiving and storing stock, accounting for materials?
• identifying HIV-exposed infants for initiation of co-trimoxazole prophylaxis and HIV testing (DBS)?
• prescribing and dispensing co-trimoxazole, and counselling regarding co-trimoxazole adherence?
• data collection and/or data entry, and preparation of summary reports?
• evaluating data and presenting feedback to staff on site performance?
• training new staff on programme activities and providing supportive supervision?
Adapted from: Abrams EJ, Fayorsey R, Gonzalez LF. Diagnosis of HIV infection in infants: a comprehensive implementation and clinical manual. New York, Columbia University, Mailman School of Public Health, International Center for AIDS Care and Treatment Programs, 2007.32

39
APPENDICES
APPENDIX G : RESOURCES FOR CO-TRIMOX AZOLE PROPHYLA XIS
I. WHO/UNITED NATIONS POLICY STATEMENTS, RECOMMENDATIONS AND GUIDELINES ON CO-TRIMOXAZOLE PROPHYLAXIS
WHO. Guidelines on co-trimoxazole prophylaxis for HIV-related infections among children, adolescents and adults. Recommendations for a public health approach. Geneva, WHO, 2006. http://www.who.int/hiv/pub/guidelines/ctxguidelines.pdf (accessed on 14 August 2009).
II. GLOBAL MANUALS RELATED TO CO-TRIMOXAZOLE PROPHYLAXIS AND PAEDIATRIC HIV/AIDS
Abrams EJ, Fayorsey R, Gonzalez LF. Diagnosis of HIV infection in infants: a comprehensive implementation and clinical manual. New York, Columbia University, Mailman School of Public Health, International Center for AIDS Care and Treatment Programs, 2007.
African Network for the Care of Children Affected by AIDS (ANECCA). Handbook on paediatric AIDS in Africa. Revised edition. Kampala, Uganda, ANECCA, July 2006. http://www.anecca.org/modules/PDdownloads/ (Also available in French)
Baylor International Pediatric AIDS Initiative (BIPAI). HIV curriculum for the health professional. Third edition. Houston, TX, BIPAI, 2007. http://www.bayloraids.org/curriculum/ (Also available in multiple languages)
Expanded Inter-Agency Task Team (IATT) on Prevention of HIV infection in Pregnant Women, Mothers and their Children. A report card on prevention of mother-to-child transmission of HIV and paediatric HIV care and treatment in low- and middle-income countries: scaling up progress from 2004 to 2005. New York, IATT, February 2007.
Hope R, Israel E. The essentials of antiretroviral therapy for health care and program managers. Watertown, Massachusetts, Pathfinder International, 2007 (Technical Guidance Series Number 5).
International Center for AIDS Care and Treatment Programs (ICAP). Care of the HIV-exposed infant. New York, Columbia University, Mailman School of Public Health. http://www.columbia-icap.org/resources/peds/trainingresources/care_hiv_infant.pdf (accessed on 27 July 2009).
WHO/UNICEF. Scale up of HIV-related diagnosis, care, support and treatment of infants and children: a programming framework. Geneva, WHO/UNICEF, 2008. http://www.who.int/hiv/paediatric/Paeds_programming_framework2008.pdf (accessed on 27 July 2009).
WHO. Antiretroviral therapy of HIV infection in infants and children in resource-limited settings: toward universal access. Recommendations for a public health approach. Geneva, WHO, 2006. http://www.who.int/hiv/pub/guidelines/art/en/index.html (accessed 13 August 2009).
WHO/UNICEF. Management of HIV infection and antiretroviral therapy in infants and children: a clinical manual. New Delhi, WHO SEARO, 2006.
WHO/UNICEF. Guidance on the global scale-up of the prevention of mother-to-child transmission of HIV: towards universal access for women, infants and young children and eliminating HIV and AIDS among children. Geneva, WHO, 2007.

40
APPENDICES
REFERENCES
1 Joint United Nations Programme on HIV/AIDS. 2008 Report on the global AIDS epidemic. Geneva, UNAIDS, 2008.
2 World Health Organization. Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants:
towards universal access: recommendations for a public health approach. Geneva, WHO, 2006:5. http://www.who.int/
hiv/pub/mtct/arv_guidelines_mtct.pdf (accessed on 09 August 2009).
3 United Nations Children’s Fund/Joint United Nations Programme on HIV/AIDS/World Health Organization. Children and
AIDS: second stocktaking report. New York, UNICEF/UNAIDS/WHO, 2008.
4 Joint United Nations Programme on HIV/AIDS/World Health Organization/ United Nations Children’s Fund. Towards
universal access: scaling up priority HIV/AIDS interventions in the health sector. Progress report 2009. Geneva, UNAIDS,
WHO, UNICEF, 2009.
5 Violari A et al for the CHER Study Group. Early antiretroviral therapy and mortality among HIV-infected infants. New
England Journal of Medicine, 2008, 359:2233–2244.
6 World Health Organization. Early detection of HIV infection in infants and children: guidance note on the selection of
technology for the early diagnosis of HIV in infants and children. Geneva, WHO, 2007. http://www.who.int/hiv/paediatric/
EarlydiagnostictestingforHIVVer_Final_May07.pdf (accessed on 29 July 2009).
7 Expanded Inter-Agency Task Team (IATT) on Prevention of HIV infection in Pregnant Women, Mothers and their Children.
A report card on prevention of mother-to-child transmission of HIV and paediatric HIV care and treatment in low- and
middle-income countries: scaling up progress from 2004 to 2005. New York, IATT, February 2007.
8 World Health Organization. Guidelines on co-trimoxazole prophylaxis for HIV-related infections among children,
adolescents and adults. Recommendations for a public health approach. Geneva, WHO, 2006 . http://www.who.int/hiv/
pub/guidelines/ctxguidelines.pdf (accessed 14 August 2009).
9 Chintu C et al. Cotrimoxazole as prophylaxis against opportunistic infections in HIV-infected Zambian children (CHAP): a
double-blind randomised placebo-controlled trial. The Lancet, 2004, 364:1865–1871.
10 Marinda E et al. Child mortality according to maternal and infant HIV status in Zimbabwe. Pediatric Infectious Diseases
Journal, 2007, 26:519–526.
11 Mulenga V et al. Effect of cotrimoxazole on causes of death, hospital admissions and antibiotic use in HIV-infected
children. AIDS, 2007, 21:77–84.
12 Thera MA et al. Impact of trimethorpim–sulfamethoxazole prophylaxis on falciparum malaria and disease. Journal of
Infectious Diseases, 2005, 192:1823–1829.
13 Nunn AJ et al. for the UNZA-UCLMS Project LUCOT Collaboration. Role of co-trimoxazole prophylaxis in reducing
mortality in HIV infected adults being treated for tuberculosis: randomised clinical trial. British Medical Journal, 2008,
337:a257 (doi: 10.1136/bmj.a257).
14 Zachariah R et al. Scaling-up co-trimoxazole prophylaxis in HIV-exposed and HIV-infected children in high HIV-prevalence
countries. Lancet Infectious Diseases, 2007, 7:686–693.
15 World Health Organization. Taking stock: HIV in children. The state of affairs. Geneva, WHO, 2006. http://www.who.int/
hiv/toronto2006/takingstockchildren.pdf (accessed on 29 July 2009).
16 Ginsburg AS et al. Provision of care following prevention of mother-to-child HIV transmission services in resource-limited
settings. AIDS, 2007, 21:2529–2532.
17 World Health Organization. Priority interventions: HIV/AIDS prevention, treatment and care in the health sector. Version
1.1. Geneva, WHO, 2008. http://www.who.int/hiv/pub/priority_interventions_web_c1.pdf (accessed on 29 July 2009).
18 World Health Organization. Guidance on provider-initiated HIV testing and counselling in health facilities. Geneva, WHO,
2007. http://www.who.int/hiv/pub/guidelines/pitc2007/en/index.html (accessed on 29 July 2009).
19 World Health Organization. Antiretroviral therapy of HIV infection in infants and children: towards universal access.
Recommendations for a public health approach. Geneva, WHO, 2007. http://www.who.int/hiv/pub/guidelines/art/en/
index.html (accessed 13 August 2009).

41
APPENDICES
20 World Health Organization. HIV and infant feeding. Geneva, WHO, 2008. http://www.who.int/child_adolescent_health/
documents/9789241595964/en/index.html (accessed 13 August 2009).
21 Tuberculosis Coalition for Technical Assistance. International standards for tuberculosis care. The Hague, TBCTA, 2006.
http://www.who.int/tb/publications/2006/istc_report.pdf (accessed on 29 July 2009).
22 World Health Organization. Pregnant women and infants. Geneva, WHO Global Malaria Programme, http://apps.who.int/
malaria/malariainpregnancy.html, and http://apps.who.int/malaria/malariaininfants.html (accessed on 10 August 2009).
23 World Health Organization. Guidelines for the treatment of malaria. Geneva, WHO, 2006. http://www.who.int/malaria/
pregnantwomenandinfants.html (accessed on 10 August 2009).
24 World Health Organization. Integrated Management of Childhood Illness. Geneva, WHO, 2008. http://whqlibdoc.who.int/
publications/2008/9789241597289_eng.pdf (accessed on 10 August 2009).
25 World Health Organization/United Nations Children’s Fund. Integrated Management of Childhood Illness for high HIV
settings: chart booklet. Geneva, WHO Department of Child and Adolescent Health, 2008:20–21.
26 Mazia G et al. Integrating quality postnatal care into PMTCT in Swaziland. Global Public Health Journal, 2009 (in press).
27 HIV Unit, Department of Clinical Services, Ministry of Health; National TB Control Program; Lighthouse Trust, Lilongwe;
and the United States Centers for Disease Control and Prevention, Malawi. Report of a country-wide survey of HIV/AIDS
services in Malawi for the year 2006. Lilongwe, HIV Unit, Department of Clinical Services, Ministry of Health, 2006.
28 Management Sciences for Health/World Health Organization. International drug price indicator guide. Arlington, VA, MSH,
2007. http://erc.msh.org/mainpage.cfm?file=1.0.htm&module=DMP&language=English (accessed on 13 August 2009)
29 World Health Organization. Transaction prices for antiretroviral medicines and HIV diagnostics from 2004 to September
2008. Geneva, WHO Global Price Reporting Mechanism, 2008. http://www.who.int/hiv/amds/gprm/en/index.html, and
http://www.who.int/hiv/amds/GPRMsummaryReportOct2008.pdf (accessed on 29 July 2009).
30 WHO. Monitoring and evaluating the prevention of mother-to-child transmission of HIV: a guide for national programmes.
Geneva, WHO, September 2009.
31 International Center for AIDS Care and Treatment Programs (ICAP). Care of the HIV-exposed infant. New York, Columbia
University, Mailman School of Public Health, June 2006.
32 Abrams EJ, Fayorsey R, Gonzalez LF. Diagnosis of HIV infection in infants: a comprehensive implementation and clinical
manual. New York, Columbia University, Mailman School of Public Health, International Center for AIDS Care and
Treatment Programs, 2007.

42
NOTES
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................

43
NOTES
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................
................................................................................................................................................................................................................................................................................................................



This document was written on behalf of the Expanded Inter-Agency Task Team (IATT) on Prevention of HIV Infection in Pregnant Women, Mothers and their Children and with the collaboration of multiple organizations working to improve pediatric HIV prevention, care and treatment.
For more information, please contact any of the organizations which supported the development of this document.
ISBN 978 92 4 159863 7