Embed Size (px)
Citation preview
CoagulopathyCoagulopathy
Bundarika Suwanawiboon M.D. Yingyong Chinthammitr M.D.Theera Ruchutrakool M.D.
Division of HematologyDepartment of Medicine Faculty of medicineSiriraj HospitalBangkok Thailand 10700
CoagulopathyCoagulopathy
Bundarika Suwanawiboon M.D.
Yingyong Chinthammitr M.D.
Theera Ruchutrakool M.D.

CoagulopathyCoagulopathyOutline
Basic of Normal Hemostasis (35 minutes) Theera
Clinical and Laboratory Approach to
Bleeding Patients (35 minutes)
Bundarika
Management of Bleeding Patients
(35 minutes)
Yingyong
Question and answer (15minutes) All

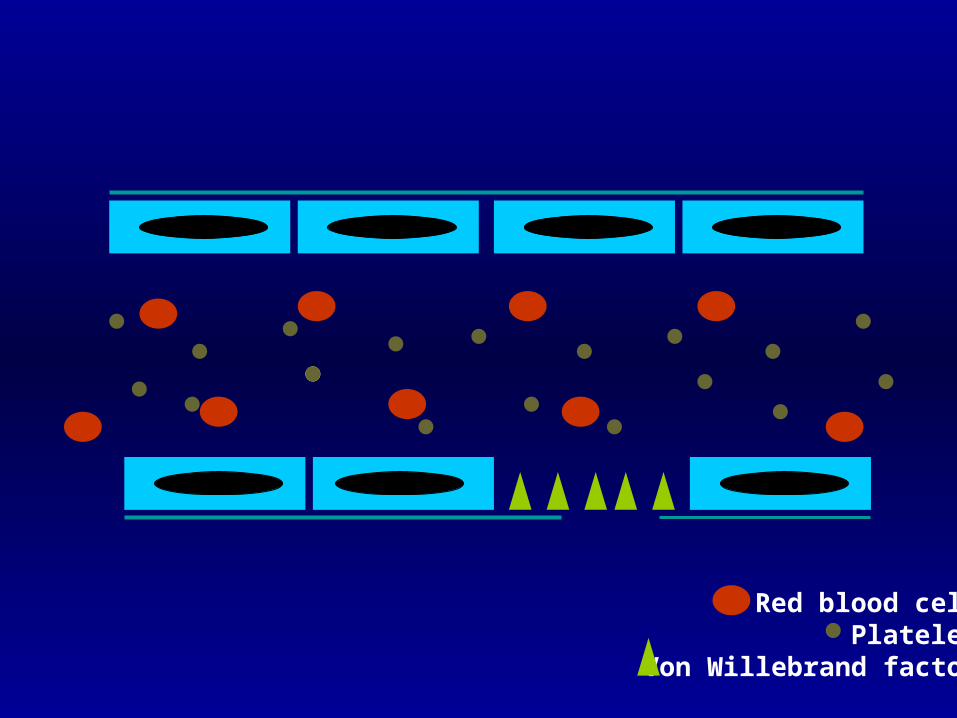
Normal HemostasisNormal Hemostasis
Normal hemostasis Blood vessel Platelet Coagulation factors Fibrinolytic system Natural anticoagulants

Red blood cellPlatelet
Red blood cellPlatelet

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor
Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factor

Red blood cellPlatelet
Von Willebrand factorFibrin polymer
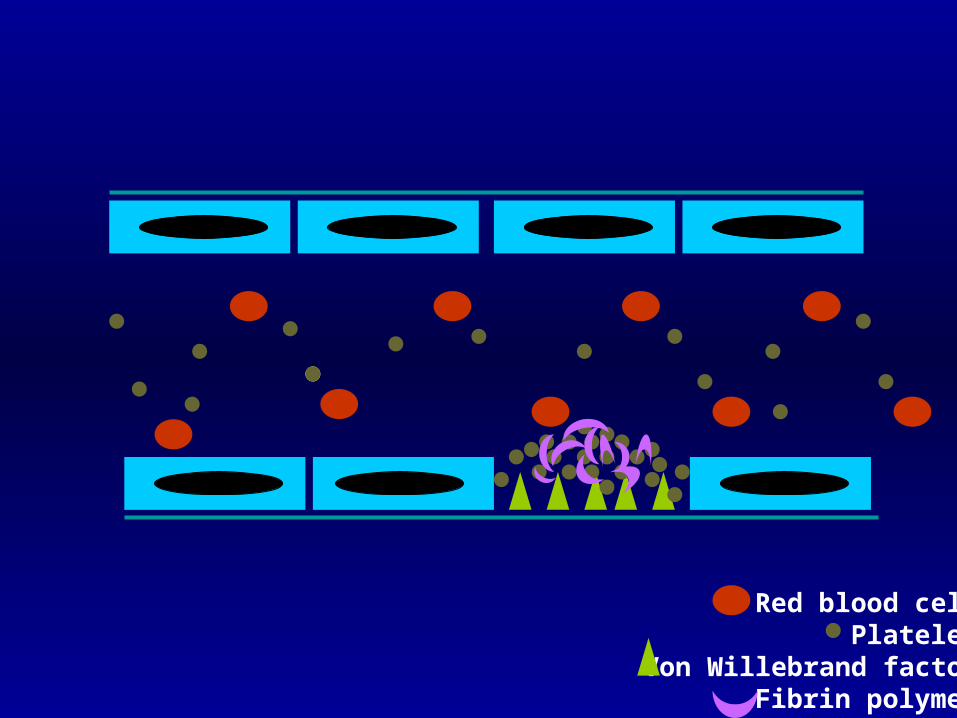
Red blood cellPlatelet
Von Willebrand factorFibrin polymer

Red blood cellPlatelet
Von Willebrand factorFibrin polymer

Normal HemostasisNormal Hemostasis
Normal hemostasis Blood vessel Platelet Coagulation factors Fibrinolytic system Natural anticoagulants

Blood vesselBlood vessel Endothelium Connective tissue or collagen
Normal HemostasisNormal Hemostasis

Blood vesselBlood vessel Endothelium
Normal HemostasisNormal Hemostasis
Antithrombotic Effect
Thrombomodulin Platelet derived relaxing
factor (PDRF) Prostacyclin (PGI2) Tissue plasminogen
activator
Thrombogenesis
von Willebrand factor Tissue thromboplastin Endothelin

Blood vesselBlood vessel Endothelium Connective tissue or collagen
Normal HemostasisNormal Hemostasis

Blood vesselBlood vessel Endothelium Connective tissue or collagen
Normal HemostasisNormal Hemostasis
Collagen direct bind and activate platelet Release von Willebrand factor to bind platelet

Normal HemostasisNormal Hemostasis
PlateletPlatelet Adhesion
via glycoprotein (GP) Shape change
from disc to ameboid form Release
ADP, thromboxane A2, vWF Aggregation
via glycoprotein (GP)

Normal HemostasisNormal Hemostasis
PlateletPlatelet
ligand receptor
adhesion vWF GP Ib/IX/V
collagen GP Ia/IIa
aggregation fibrinogen GP IIb/IIIa

Normal HemostasisNormal Hemostasis
PlateletPlatelet
Platelet plug formation and vasoconstriction
Primary hemostatic plug formation which is enough to stop bleeding from
small and shallow wound

Factor XII HMWK/PK
Factor XI Factor XIa
Factor IX Factor IXa Factor VIIaFactor VIIIa Tissue factor
Factor X Factor Xa Factor XFactor Va
Prothrombin Thrombin
Fibrinogen Fibrin
Normal HemostasisNormal HemostasisCoagulation pathwayCoagulation pathway

Factor XII HMWK/PK
Factor XI Factor XIa
Factor IX Factor IXa Factor VIIaFactor VIIIa Tissue factor
Factor X Factor Xa Factor XFactor Va
Prothrombin Thrombin
Fibrinogen Fibrin
Normal HemostasisNormal Hemostasis
Common pathway
Intrinsic pathway
Extrinsic pathway

Factor XII HMWK/PK
Factor XI Factor XIa
Factor IX Factor IXa Factor VIIaFactor VIIIa Tissue factor
Factor X Factor Xa Factor XFactor Va
Prothrombin Thrombin
Fibrinogen Fibrin
Normal HemostasisNormal HemostasisCoagulation pathwayCoagulation pathway

Normal HemostasisNormal Hemostasis Factor XII HMWK/PK
Factor XI Factor XIa
Factor IX Factor IXa Factor VIIaFactor VIIIa Tissue factor
Factor X Factor Xa Factor XFactor Va
Prothrombin Thrombin
Fibrinogen Fibrin
heparin
Activated proteinC
ProteinC
Protein S
antithrombin
Natural anticoagulantNatural anticoagulant

High Molecular Weight Kininogen (HMWK)Prekallekrein (PK)F.XII
Tissue plasminogen activator (t-PA)Urokinase
Plasminogen PlasminFibrin polymer
Fibrin degradation products (FDP)
Normal HemostasisNormal HemostasisFibrinolytic systemFibrinolytic system
Streptokinase
Normal HemostasisNormal Hemostasis
““New concept !”New concept !”
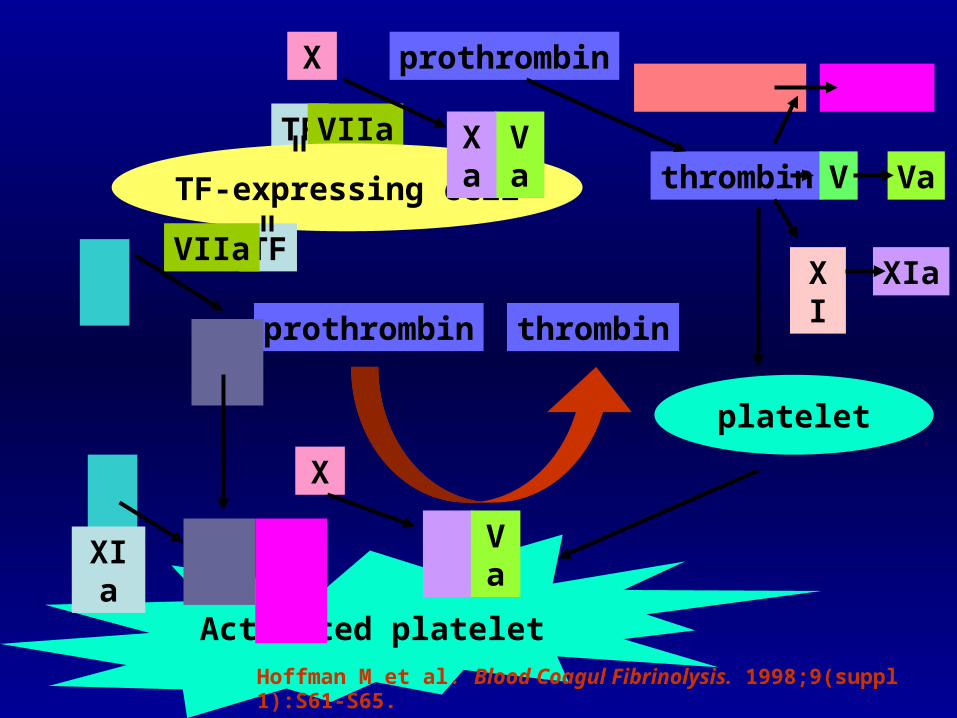
Cell-based model of coagulation

1. Initiation
3. Propagation
IIa
IIa
2. Amplificatio
n
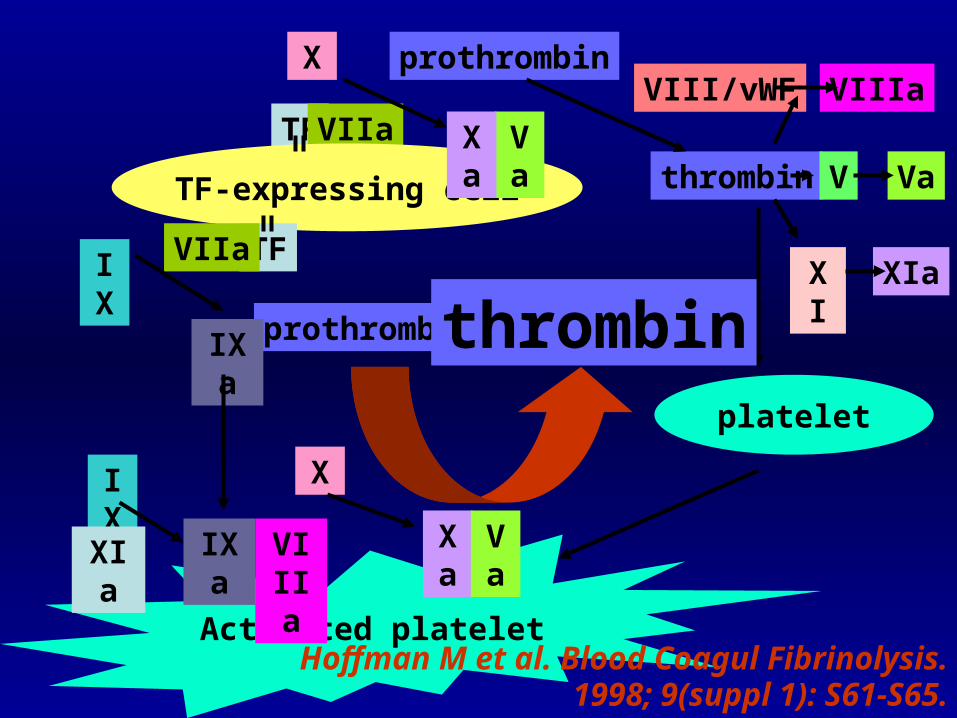
Hemostasis occurs on two surfaces:TF- bearing cells and platelet
Normal HemostasisNormal Hemostasis
TF
VIIa
TF-expressing cell
TF
VIIa
Activated platelet
platelet
X
Va
Xa
prothrombin
thrombin
VIII/vWF VIIIa
V
XI XIa
Va
prothrombinthrombin
X
Xa
Va
IX
IXa
IXa
VIIIa
IXXIa
Hoffman M et al. Blood Coagul Fibrinolysis. 1998; 9(suppl 1): S61-S65.
TF
VIIa
TF-expressing cell
TF
VIIa
Activated platelet
platelet
X
Va
Xa
prothrombin
thrombin
VIII/vWF VIIIa
V
XI XIa
Va
prothrombin thrombin
X
Xa
Va
IX
IXa
IXa
VIIIa
IXXIa
Hoffman M et al. Blood Coagul Fibrinolysis. 1998;9(suppl 1):S61-S65.

Cell-based model “Three overlapping phases”
Initiation phase “TF-bearing cell to generate F.Xa,
F.IXa and (little amount of) thrombin”
Amplification phase“Gererate cofactor F.V and F.VIII by
little amount of thrombin from initiation phase”
Propagation phase“Large amount of thrombin production
(burst of thrombin) on activated platelet”

Approach to Hemostatic Disorders:
Clinical and Laboratory Approach
Bundarika Suwanawiboon, M.D.
Division of Hematology
Department of Medicine

What is the diagnosis?What is the diagnosis?

Clinical Evaluation of Bleeding PatientsClinical Evaluation of Bleeding Patients
“80% of correct diagnosis can be made by history taking and physical examination.”
History TakingHistory Taking
Identify if the bleeding problem is due toLocal vs. systemic defect
Location: single vs. multiple sitesSeverity: Spontaneous? Appropriate to trauma?
Hereditary vs. acquired disorderOnsetFamily historyUnderlying diseaseMedication
Primary vs. secondary hemostatic disoder

Deep Deep ecchymosis,
hematoma
Rare
Retroperitoneal hematoma, hemarthrosis
Superficial Petechiae, superficial
ecchymosis
Common
Rare
Sites Skin
Mucosal
Others
DelayedImmediateOnset
Secondary HemostasisPrimary Hemostasis
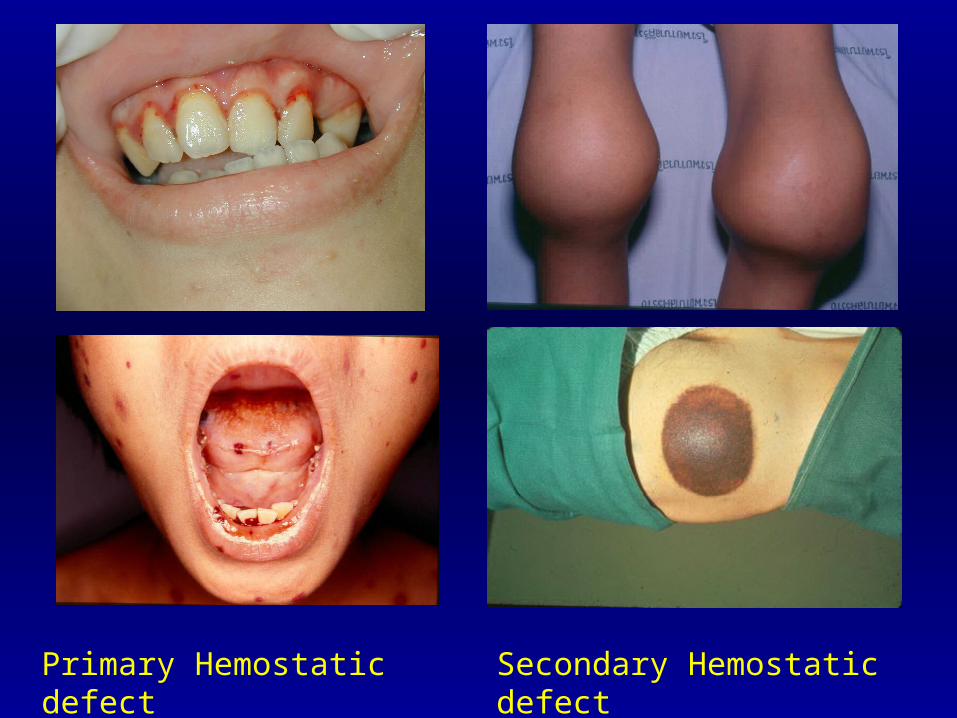
Primary Hemostatic defect Secondary Hemostatic defect
Laboratory Investigation of Laboratory Investigation of Hemostatic DisordersHemostatic Disorders

Assessment of Primary HemostasisAssessment of Primary Hemostasis
PlateletComplete blood count (CBC)Bleeding time/ PFA-100Platelet aggregation study
Blood vesselBleeding time
von Willebrand factor (vWF)Bleeding timevWF Antigen, vWF: RCO, vWF multimer, FVIII
Complete Blood Count (CBC)Complete Blood Count (CBC)
Platelet number Normal platelet count: 150,000 –400,000/uL
> 100,000/uL Bleeding unlikely
< 20,000/uL ↑ risk for spontaneous
bleeding
Must exclude pseudothrombocytopenia
Assess for platelet morphology

Bernard-Soulier Syndrome
Giant platelet
Thrombocytopenia
Pseudothrombocytopenia
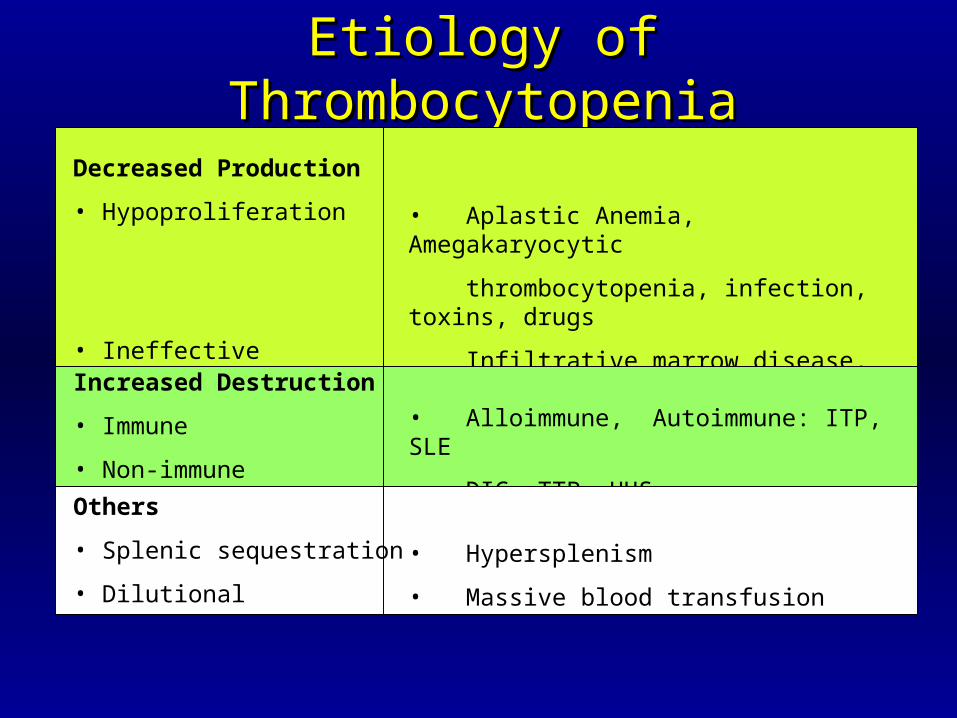
Etiology of ThrombocytopeniaEtiology of Thrombocytopenia
Decreased Production
• Hypoproliferation
• Ineffective Thrombopoiesis
• Aplastic Anemia, Amegakaryocytic
thrombocytopenia, infection, toxins, drugs
Infiltrative marrow disease, TAR
• Megaloblastic anemia
Increased Destruction
• Immune
• Non-immune
• Alloimmune, Autoimmune: ITP, SLE
• DIC, TTP, HUS
Others
• Splenic sequestration
• Dilutional
• Hypersplenism
• Massive blood transfusion

Bleeding TimeBleeding Time

Bleeding Time: InterpretationBleeding Time: Interpretation
Normal value* : 1-9 minProlonged bleeding time:
Thrombocytopenia/ anemia (Hct < 20%)Hereditary platelet dysfunctionvon Willebrand diseaseSevere hypofibrinogenemiaBlood vessels disordersUremiaMyeloproliferative disordersMedication: Aspirin, NSAIDs,other antiplatelet drugs

Platelet Aggregation StudyPlatelet Aggregation Study

Normal Platelet ResponseNormal Platelet Response
Arterioscler Thromb Vasc Biol 2000 20:285

Epinephrine ADP Collagen Ristocetin Arachidonic
acid
Normal +++ +++ +++ +++ +++
Glanzmann’s - - - +++ -
Thrombasthenia
Bernard-Soulier +++ +++ +++ - +++
Syndrome
Storage Pool + +* +* +++ ++
Disease (no secondary wave)
Aspirin + ++ + ++ -
Effect

von Willebrand Factorvon Willebrand Factor
Synthesized in endothelial cells and megakaryocytes
Two important functions:Carrier protein for plasma FVIII
Ligand binding to platelet GPIb receptor to initiate platelet adhesion
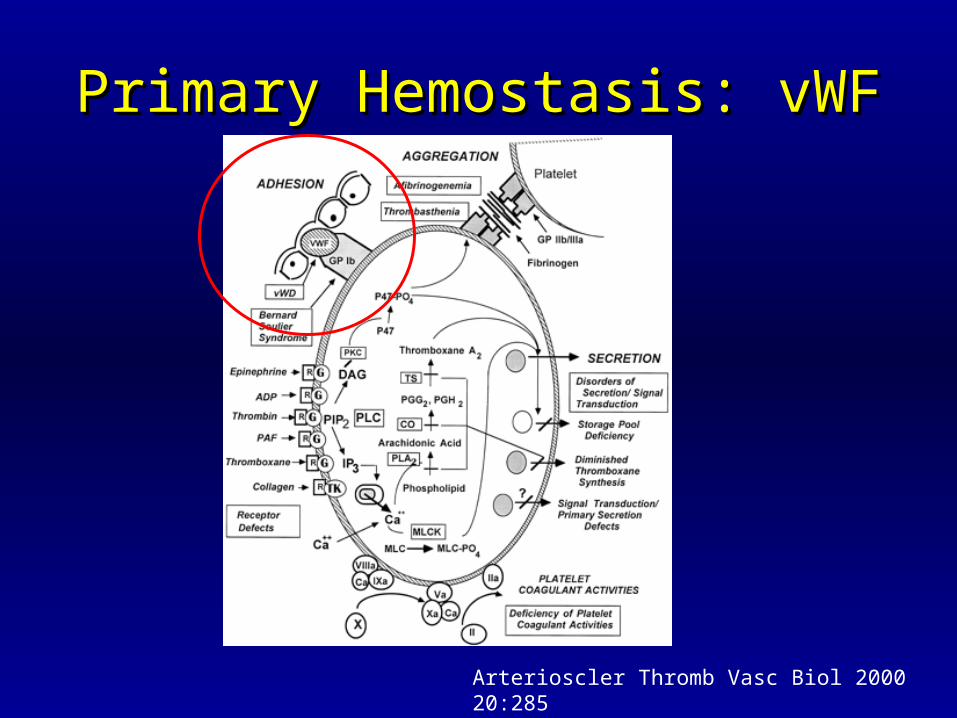
Primary Hemostasis: vWFPrimary Hemostasis: vWF
Arterioscler Thromb Vasc Biol 2000 20:285

von Willebrand Factor Panelvon Willebrand Factor Panel
vWF antigen
vWF ristocetin cofactor activity
vWF multimer analysis
FVIII level

vWD Laboratory DiagnosisvWD Laboratory Diagnosis
Test/Type 1 2A 2B 2M 2N 3
BT N or ↑ ↑ ↑ N or ↑ ↑ ↑ N ↑↑↑↑
vWF:Ag ↓ ↓ ↓ ↓ or N ↓ or N ↓↓↓↓
vWFR:Co ↓ ↓↓↓ ↓↓ ↓ ↓ or N ↓↓↓↓
LD-RIPA - - ↑ - - -
FVIII N or ↓ N or ↓ N or ↓ N ↓↓↓ ↓↓↓
Multimer N but ↓ abnormal abnormal N but ↓ N but ↓ absent
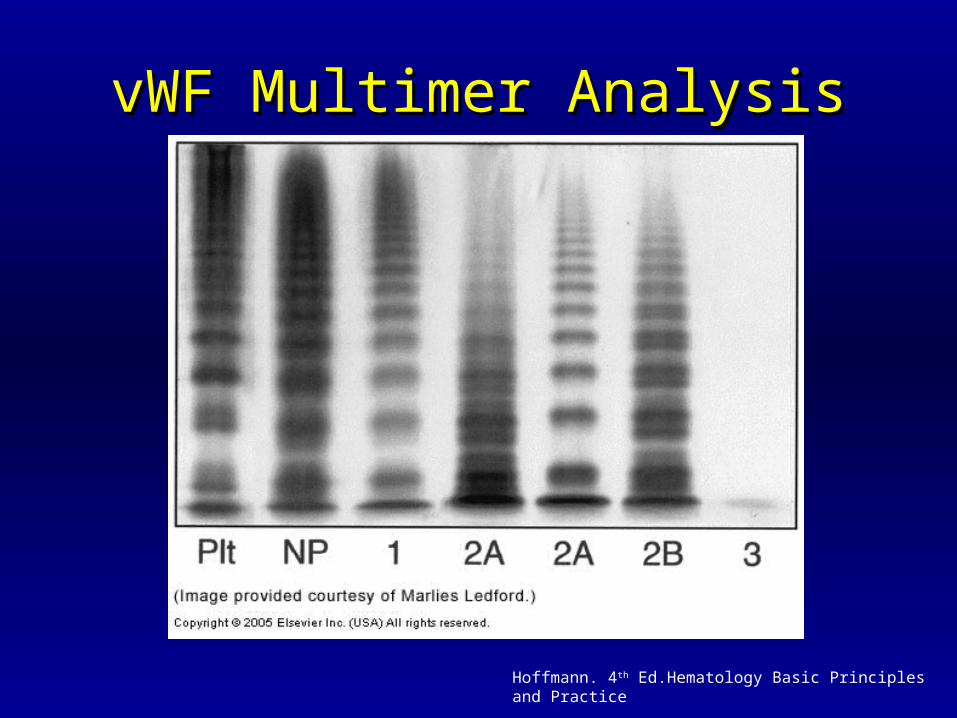
vWF Multimer AnalysisvWF Multimer Analysis
Hoffmann. 4th Ed.Hematology Basic Principles and Practice

Assessment of Secondary HemostasisAssessment of Secondary Hemostasis
Screening tests:PT
aPTT
Mixing study
Additional TestsFibrinogen
Thrombin Time
Reptilase time
Coagulation factor assays
D-dimer
Fibrin Degradation Product
Euglobulin lysis time

Accurate Sample Collection is the KeyAccurate Sample Collection is the Key
Always use 3.2% sodium citrate tube and sent to the lab immediately.
Fill tube to the proper level.
(anticoagulant to plasma ratio = 1:9)
Modification may be required based on Hct Sodium citrate (ml) = (100 – Hct pt) x 0.5 / 55*
* normal plasma vol.

XII XIIa
XI XIaHMWK
IXaIXVIIIa/PL
Tenase
Ca++X Xa
II IIaVa/PL
Ca++
Fibrinogen Fibrin
X-linkedFibrin
XIIIa
Intrinsic Pathway Extrinsic Pathway
Common Pathway
XII XIIa
XIHK/PK
IXa/IX
VIIIaVIIa/TF
VIIVIIa
TF
Ca++X Xa
II IIaVa/PL
Ca++
Fibrinogen Fibrin
XIa

Prothrombin Time (PT)Prothrombin Time (PT)
PT : test extrinsic and common pathway

Activated Partial Thromboplastin Time Activated Partial Thromboplastin Time (aPTT)(aPTT)
aPTT : test intrinsic and common pathway

Mixing StudyMixing Study
+
0% 100%
50%
<35%
Correctable
Normal coagulation
time
Uncorrectable
prolonged coagulation
time
Deficiency
Inhibitor
Prolonged PT or aPTT occurs when coagulation factor < 35-40%
Interpretation of Abnormal Interpretation of Abnormal CoagulogramCoagulogram
Isolated prolonged PT
Isolated prolonaged aPTT
Prolonged PT and aPTT

Isolated prolonged PT
Mixing study
Correctable Uncorrectable Deficiency Inhibitor
Hereditary: FVII FVII (rare) Lupus anticoagulant Acquired: Early liver impairment
Vitamin K antagonist Vitamin K deficiency

Isolated prolonged aPTT
Bleeding No bleeding
Mixing study Mixing study
Correctable Uncorrectable Correctable Uncorrectable
Deficiency Inhibitor Deficiency Inhibitor
Factor VIII /vWD Factor VIII Factor XII Factor XIIFactor IX Factor IX HMWK HMWKFactor XI Factor XI Prekallekrein Prekallekrein Heparin Lupus anticoagulant

Acquired FVIII inhibitor
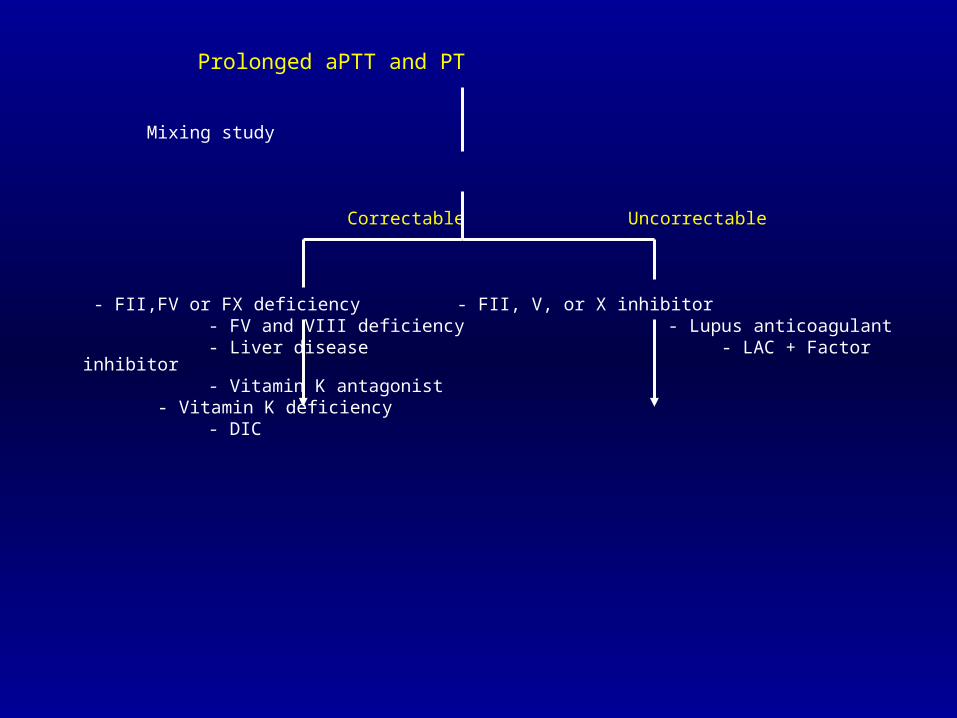
Prolonged aPTT and PT
Mixing study
Correctable Uncorrectable
- FII,FV or FX deficiency - FII, V, or X inhibitor - FV and VIII deficiency - Lupus anticoagulant - Liver disease - LAC + Factor inhibitor - Vitamin K antagonist - Vitamin K deficiency - DIC

Bleeding Disorders with Bleeding Disorders with Normal PT and aPTTNormal PT and aPTT
Factor XIII deficiency
Dysfibrinogenemia
Mild isolated factor deficiency
-antiplasmin deficiency
Elevated fibrin degradation products
Platelet disorders
Vascular disorders

Further Diagnostic TestsFurther Diagnostic Tests
Specific coagulation factor assay
Coagulation factor inhibitor assay
Lupus anticoagulant panel

Other Tests for Secondary HemostasisOther Tests for Secondary Hemostasis
Fibrinogen
D-dimer
Fibrin(ogen) degradtion product
Thrombin time
Reptilase time
Euglobulin lysis time
FibrinogenFibrinogen
Functional level (200-400 mg/dl)↓ Fibrinogen (esp. < 100 )
DICFibrinolytic therapyPrimary fibrinolytic stateCongenital afibrinogenemiaAcquired/congenital dysfibrinogenemia
↑ FibrinogenInflammatory states/acute illnessMay associated with shortened PT/aPTT

D-Dimer
Measured cross-linked fibrin degradation product by plasmin
More sensitive and specific for fibrinolysis than Fibrin(ogen) Degradatioin Product (FDP)
↑ D-dimer:DIC
Acute thromboembolic episodes
Post-trauma or surgery
Malignancy

Fibrin(ogen) Degradation Product
↑ levels inPrimary fibrinolytic syndromes
DIC
After lytic therapy
Acute thromboembolic episodes
After injury/surgery
Thrombin TimeThrombin Time
Thrombin Time (TT)Assess the ability to convert fibrinogen fibrin by adding thrombin to plasma
Prolonged TT:Inhibitor of thrombin: heparin, anti-thrombin antibody
Hypofibrinogenemia or dysfibrinogenemia
Inhibitor of fibrin polymerization: fibrin degradation product, paraprotein
Euglobulin Lysis TimeEuglobulin Lysis Time
Euglobulin fraction of plasma is precipitated by acetic acid and thrombin added.
Lysis of clot is observed.
Normal : > 120 min
Shortened ELT:DIC
Liver disease
Primary fibrinogenolysis: malignancy, e.g. prostate carcinoma


Management of Bleeding Patients
Yingyong Chinthammitr27 June 2007

Objectives
• Efficient practice of replacement therapy
• Management of common bleeding problems

Goal of replacement Rx
• Treatment of bleeding
• Prevention of bleeding before procedure
• Not treat only lab. esp. in irreversible causes of coagulopathy

WB
PRC PRP
FFP PC
CRP Cryo
WB = Whole blood
PRC = Pack Red CellPRP = Platelet-rich plasma
FFP = Fresh frozen plasmaPC = Platelet concentrates(other: apheresis PLT = 4-6 u)
CRP = Cryo-removed plasma,FFP with cryo.-removed
Cryo. = Cryoprecipitate(F VIII 100 u, vWF, Fibrinogen, F XIII)
1 unit

Other products
• Factor concentrates : VIII, IX• Prothrombin complex concentrates (PCC)• Activated PCC (APCC)• DDAVP• Vitamin K injection• Recombinant F VIIa (novoseven)• Tranexamic acid – antifibrinolysis• Fibrin glue – two bottles: Fibrinogen & Thrombin

Recombinant Factor VIIa (NovosevenR)
EFFECTIVE+SAFE but VERY EXPENSIVE
- Hemophilia with inhibitor (alloantibody)- Factor VIII inhibitor (autoantibody)
- Uncontrolled bleeding from coagulopathy (liver failure)- Uncontrolled bleeding from thrombocytopenia- Uncontrolled bleeding from platelet dysfunction (uremia , congenital defect)- Severe surgical and traumatic hemorrhage

VIIa
TFPI
Activated Platelet
TF
Va
XI a XaIXa
X II
IIa
IX
IX
Activated platelet
VaVIIIa
IIa
VIII/vWF
XI
XIaPlatelet
Va
V
VIIIa + free vWF
V
TF
Tissue factor--bearing cell
TFTF
VIIaVIIaXaXa
TF TFTF
TF
Va
II
X

TFPI
Activated Platelet
TF
Va
Xa
X II
IIaActivated platelet
Va
IIa
VIII/vWF
XI
XIaPlatelet
Va
V
VIIIa + free vWF
V
TF
Tissue factor--bearing cell
TFTF
VIIaVIIaXaXa
TF TFTF
TF
Va
II
X
VIIa
Fibrin Glue- มี� 2 ขวด คือ
1. Thrombin2. Fibrinogen, F XIII (cryoprecipitate)
Thrombin XIIIaFibrinogen ------------->Fibrin ------> Cross-linked
Fibrin
เติ มี Calcium ใน Thrombin
อาจเติ มี Tranexamic acid ใน Fibrinogen
ใช้� อ�ปกรณ์� two syringes with one air-line

Tranexamic acid
- anti-fibrinolysis- adjunctive Rx in areas with high fibrinolysis (Oral cavity, GI tract, GU tract)- Contraindication : DIC, Thrombosis, Renal bleeding (obstructive uropathy)- IV : 10 mg/kg/dose q 8 h- Oral : 25 mg/kg/dose q 8 hr- Oral wash in dental bleeding

Bleeding
• Thrombocytopenia
• Coagulopathy
• Combined

Platelet level & Bleeding
• > 100,000/mm3 No bleeding tendency• < 100,000/mm3 Bleeding time prolongation• < 50,000/mm3 Bleeding after trauma , surgery• < 10,000/mm3 Spontaneous bleeding• < 5,000/mm3High risk for spontaneous CNS bleeding

• Platelet level
• Platelet function
• Anemia
• Local problem
• Coexisting coagulopathy
Thrombocytopenia & Bleeding

Platelet transfusion
• Symptomatic Rx , not Rx cause• Dose: 1 unit per 10 kg BW• Indication
– Bleeding associated with thrombocytopenia– Prophylaxis, before invasive procedure/surgery
• Contra-indication– TTP (Thrombotic thrombocytopenic
purpura) /HUS (Hemolytic uremic syndrome), HIT (Heparin-induced thrombocytopenia)

Prophylaxis in thrombocytopenia
Condition Threshold
Chronic stable thrombocytopenia (underproduction e.g. aplastic anemia)
<5,000 or No
Post-chemo stable patient <10,000
Unstable (fever or infection or coagulopathy or platelet dysfunction)
<20,000
Invasive procedures, surgery <50,000
Neurosurgery, ocular Sx <100,000

Plasma derivatives: FFP, Cryo.
• No medications added• Return to blood bank if not use within 30 min• Most adverse transfusion reactions occur in the
first 15 min.• Time of transfusion – not exceed 4 hr• Rate in adult (good cardiac
condition) : 200 - 300 mL/hr• NOT for: volume expansion, protein (alb, glob)
nutrient
Cirrhosis• FFP 10-15 ml/kg• Vitamin K 10 mg IV • Pitfalls
– Uncorrected localized bleeding problem e.g. varice, mucosal lesion
– Overdependence on PT – Goal: to correct or prevent bleeding, NotNot to achieve a
normal PT– Timing of FFP therapy before an invasive procedure

- Vitamin K : fat-soluble vitamin- Vitamin K-dependent factors : II,VII,IX,X ; Protein C,S,Z- Vit.K : K1(green vegetables), K2(gut flora), K3(synthetic water-soluble)
Vitamin K deficiency

* Neonatal : hemorrhagic disease of the newborn* Children & Adult : - low intake- absorption defect - cholestasis, fat malabsorption syndrome- broad-spectrum antibiotics (+low intake)
Vitamin K deficiency

Vitamin K deficiency
• Vit. K 10 mg IV slowly, sc
• FFP
• Prothrombin complex concentrate (PCC)

HEMARTHROSIS AND HEMOPHILIC ARTHROPATHY
Hemophilia A• Cryoprecipitate• Factor VIII concentrates• FFP• DDAVP
Hemophilia B
• FFP• Cryo. Removed Plasma• F IX concentrates
vWD• DDAVP• Cryoprecipitate• F VIII concentrates • FFP

Rx of Bleeding episodes in Hemophilia
Site Level (%) Rx Length
Joint 30-40 1 dose
Muscle 30-40 1-3 doses
Hematuria 30-40 1 dose
Retroperitoneal 50 5-7 d
GI 50 5-7 d
Neck 100 7-10 d
Intracranial 100 10-14 d

Hemophilia A with hemarthrosis
• 60 kg.
• Raise F VIII to 30 %
• 1 u/kg raise 2%
• F VIII half life = 12 hr– Raise 30% -> 15 u/kg = 15x60 = 900 u– Cryo. 9 bags ( cont. ~5 bags q 12 hr)
Hemophilia B with hemarthrosis
• 60 kg.
• Raise F IX to 30 %
• 1 u/kg raise 1%
• F IX half life = 24 hr– Raise 30% -> 30 u/kg = 30x60 = 1800 u– FFP 1800 ml. ( cont. 900 ml. q 24 hr)
Warfarin-associated coagulopathy & bleeding
• Life-threatening Bleeding– withhold warfarin, FFP/PCCs, vit. K 5-10 mg.
i.v., provide medical support (e.g. PRC)
• Major, non-life-threatening Bleeding– withhold warfarin, FFP/PCCs, vit. K 1-10 mg.
i.v., provide medical support (e.g. PRC)
J Thromb Haemost 2006;4:1853-63

Warfarin-associated coagulopathy & NoNo bleeding
– Withhold warfarin– Vit. K 1 mg.– Reintroduce at a
lower dose on the following day
– Recheck INR in < 72 hr
Beware of re-thrombosis from overcorrection
– Withhold warfarin– Vit. K 1 mg. i.v.– Recheck INR in 24
hr
– Withhold warfarin
– Recheck INR in 24-48 hr
INR 4.5-10INR 4.5-10
Identify and correct the cause of elevated INR
INR >10INR >10
J Thromb Haemost 2006;4:1853-63

Heparin
• Unfractionated heparin (prolonged APTT)– Bleeding: hold heparin, protamine (1 mg/100
u heparin)– No bleeding: hold heparin (Hf. life 1 hr)
• LMWH (normal APTT)– Bleeding: protamine (neutralize all anti-IIa but
75% of anti-Xa)

DIC
• Rx cause
• Bleeding– FFP , PLT concentrate– Cryoprecipitate raise fibrinogen > 100 mg/dL
:1 bag/5 kg BW raise fibrinogen 100 mg/dL
Treatment of DIC
* Treat associated disease* Bleeding - Replacement therapy* Thrombosis - heparin : purpura fulminans, acral/dermal ischemia, retained dead fetus syndrome, giant hemangioma, aortic aneurysm without rupture, solid tumor* AT concentrate, APC

Massive blood transfusion
• > Total blood volume in 24 hour
• Dilution and/or consumption of PLT, Coag. Factors
• LAB: platelet, coagulogram, fibrinogen
• PLT > 50,000, PT <1.5 times the midpoint of normal range, Fibrinogen >100 mg/dL : generally adequate for hemostasis

Platelet dysfunction
• Stop Antiplatelet agents before surgery– Aspirin : 7 days (irreversible inhibition)– NSAID : 1-4 days (reversible inhibition)– Clopidogrel : 10 days

Uremic bleedingTreatment Regimen Onset Duration
*PRC /LPB Hct ~30% 1 h While Hct at this level
*EPO 50-100 U/kg Hct 30% Same
(~6 wk)
*Cryoppt. 10 units 1 h 24–36 h[Effective ~ 50%]
*DDAVP 0.3-0.4 mcg/kg 1 h 4 – 8 h IV or SC 2-3 mcg/kg intranasal
*Conjugated 0.6 mkd IV 6 h 14 d (IV)
estrogen 50 mkd po 2 d 5 d (PO)
x 5 days
*Dialysis

Thank you for your attentionThank you for your attention
Question…