Embed Size (px)
Citation preview

Colony-stimulating factors for prevention and treatment of
infectious complications in patients with acute myelogenous
leukemia (Review)
Gurion R, Belnik-Plitman Y, Gafter-Gvili A, Paul M, Vidal L, Ben-Bassat I, Shpilberg O,
Raanani P
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2012, Issue 6
http://www.thecochranelibrary.com
Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
6BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
17ADDITIONAL SUMMARY OF FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . .
26DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
58DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 All-cause mortality, Outcome 1 All-cause mortality at 30 days. . . . . . . . . . 60
Analysis 1.2. Comparison 1 All-cause mortality, Outcome 2 All-cause mortality at the end of follow up. . . . . . 61
Analysis 1.3. Comparison 1 All-cause mortality, Outcome 3 All-cause mortality subgroup analysis age > 60. . . . 62
Analysis 1.4. Comparison 1 All-cause mortality, Outcome 4 All-cause mortality subgroup analysis age < 60. . . . 63
Analysis 1.5. Comparison 1 All-cause mortality, Outcome 5 All-cause mortality sensitivity analysis for allocation
concealment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Analysis 1.6. Comparison 1 All-cause mortality, Outcome 6 All-cause mortality sensitivity analysis using random effects
model. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Analysis 2.1. Comparison 2 Overall survival, Outcome 1 Overall survival. . . . . . . . . . . . . . . . 66
Analysis 3.1. Comparison 3 Complete remission, Outcome 1 Complete response. . . . . . . . . . . . . 67
Analysis 4.1. Comparison 4 Disease-free survival, Outcome 1 Disease-free survival. . . . . . . . . . . . . 68
Analysis 5.1. Comparison 5 Relapse rate, Outcome 1 Relapse rate. . . . . . . . . . . . . . . . . . . 69
Analysis 6.1. Comparison 6 Bacteremias, Outcome 1 Bacteremias. . . . . . . . . . . . . . . . . . . 70
Analysis 7.1. Comparison 7 Invasive fungal infections, Outcome 1 Invasive fungal infections. . . . . . . . . 71
Analysis 8.1. Comparison 8 Episodes of febrile neutropenia, Outcome 1 Episodes of febrile neutropenia. . . . . 72
Analysis 9.1. Comparison 9 Adverse events requiring discontinuation of CSFs, Outcome 1 Adverse events requiring
discontinuation of CSFs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
73APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
79FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
81WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
81HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
81CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
81DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
82SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
82INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iColony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Colony-stimulating factors for prevention and treatment ofinfectious complications in patients with acute myelogenousleukemia
Ronit Gurion1, Yulia Belnik-Plitman1, Anat Gafter-Gvili2, Mical Paul3, Liat Vidal2, Isaac Ben-Bassat4 , Ofer Shpilberg1, Pia Raanani1
1Institute of Hematology, Davidoff Center, Beilinson Hospital, Rabin Medical Center, Petah Tikva, Israel. 2Department of Medicine
E, Beilinson Hospital, Rabin Medical Center, Petah Tikva, Israel. 3Infectious Diseases Unit, Sackler Faculty of Medicine, Tel Aviv,
Israel. 4Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel
Contact address: Pia Raanani, Institute of Hematology, Davidoff Center, Beilinson Hospital, Rabin Medical Center, 39 Jabotinski
Street, Petah Tikva, 49100, Israel. [email protected].
Editorial group: Cochrane Haematological Malignancies Group.
Publication status and date: Edited (conclusions changed), comment added to review, published in Issue 6, 2012.
Review content assessed as up-to-date: 24 January 2011.
Citation: Gurion R, Belnik-Plitman Y, Gafter-Gvili A, Paul M, Vidal L, Ben-Bassat I, Shpilberg O, Raanani P. Colony-stimulating
factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia. Cochrane Database of
Systematic Reviews 2012, Issue 6. Art. No.: CD008238. DOI: 10.1002/14651858.CD008238.pub3.
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Acute myelogenous leukemia (AML) is a fatal bone marrow cancer. Colony-stimulating factors (CSFs) are frequently administered
during and after chemotherapy to reduce complications. However, their safety with regard to disease-related outcomes and survival in
AML is unclear. Therefore, we performed a systematic review and meta-analysis to evaluate the impact of CSFs on patient outcomes,
including survival.
Objectives
To assess the safety/efficacy of CSFs with regard to disease-related outcomes and survival in patients with AML.
Search methods
We conducted a comprehensive search strategy. We identified relevant randomized clinical trials by searching the Cochrane Central
Register of Controlled Trials (The Cochrane Library 2010, Issue 7), MEDLINE (January 1966 to July 2010), LILACS (up to December
2009), databases of ongoing trials and relevant conference proceedings.
Selection criteria
Randomized controlled trials that compared the addition of CSFs during and following chemotherapy to chemotherapy alone in
patients with AML. We excluded trials evaluating the role of CSFs administered for the purpose of stem cell collection and/or priming
(e.g. before and/or only for the duration of chemotherapy).
Data collection and analysis
Two review authors appraised the quality of trials and extracted data. For each trial, we expressed results as relative risk (RR) with 95%
confidence intervals (CI) for dichotomous data. We analyzed time-to-event outcomes as hazard ratios (HRs).
1Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
The search yielded 19 trials including 5256 patients. The addition of CSFs to chemotherapy yielded no difference in all-cause mortality
at 30 days and at the end of follow up (RR 0.97; 95% CI 0.80 to 1.18 and RR 1.01; 95% CI 0.98 to 1.05, respectively) or in overall
survival (HR 1.00; 95% 0.93 to 1.08). There was no difference in complete remission rates (RR 1.03; 95% CI 0.99 to 1.07), relapse
rates (RR 0.97; 95% CI 0.89 to 1.05) and disease-free survival (HR 1.00; 95% CI 0.90 to 1.13). CSFs did not decrease the occurrence
of bacteremias (RR 0.96; 95% CI 0.82 to 1.12), nor the occurrence of invasive fungal infections (RR 1.40; 95% CI 0.90 to 2.19).
CSFs marginally increased adverse events requiring discontinuation of CSFs as compared to the control arm (RR 1.33; 95% CI 1.00
to 1.56).
Authors’ conclusions
In summary, colony-stimulating factors should not be given routinely to acute myelogenous leukemia patients post-chemotherapy since
they do not affect overall survival or infectious parameters including the rate of bacteremias and invasive fungal infections.
P L A I N L A N G U A G E S U M M A R Y
The use of colony-stimulating factors in the supportive care of patients with acute myelogenous leukemia (AML)
Acute myelogenous leukemia (AML) is an aggressive, rare type of blood cancer manifested by infections, bleeding and a high rate
of mortality. It requires immediate treatment with intensive chemotherapy and sometimes also with bone marrow transplantation.
Infections are a major cause of mortality in AML patients since intensive chemotherapy lowers the white blood cell (WBC) count and
disrupts the immune system. Colony-stimulating factors (CSFs) are agents administered in order to increase the WBC count, in the
hope that this will decrease the rate of infections. However, it has not been established whether their administration might adversely
affect other outcomes related to the disease, such as the achievement of remission or the relapse rate. Most importantly, it is unknown
whether their administration affects the survival of AML patients. Therefore, we conducted a systematic review assessing the influence
of CSFs on disease and infection-related outcomes. Our review showed that the addition of CSFs to chemotherapy in AML patients
affected neither overall survival, nor the achievement of disease remission or the rate of relapse. Importantly, they did not affect the rate
of infections in this population. We concluded that CSFs post-chemotherapy should not be given routinely in AML patients. However,
their administration could be considered on an individual basis.
2Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
All cause mortality for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings: inpatients
Intervention: All cause mortality
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control All cause mortality
All cause mortality - 30
days
Follow-up: 30 days
Study population RR 0.97
(0.8 to 1.18)
3319
(11 studies)
⊕⊕©©
low1,2
109 per 1000 105 per 1000
(87 to 128)
Moderate
95 per 1000 92 per 1000
(76 to 112)
All cause mortality - End
of follow up
Follow-up: 3-7 years
Study population RR 1.01
(0.98 to 1.05)
4029
(14 studies)
⊕⊕©©
low1,3
729 per 1000 736 per 1000
(715 to 766)
Moderate
758 per 1000 766 per 1000
(743 to 796)
All cause mortality sub-
group analysis age>60
Follow-up: 3-7 years
Study population RR 1.01
(0.97 to 1.06)
2035
(7 studies)
⊕⊕©©
low1,2
3C
olo
ny-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

775 per 1000 782 per 1000
(751 to 821)
Moderate
852 per 1000 861 per 1000
(826 to 903)
All-cause mortality sub-
group analysis age<60
Follow-up: 3-7 years
Study population RR 1.08
(0.97 to 1.2)
1079
(5 studies)
⊕⊕©©
low1,2
533 per 1000 576 per 1000
(517 to 640)
Moderate
493 per 1000 532 per 1000
(478 to 592)
All-cause mortality -
sensitivity analysis
Follow-up: 3-7 years
Study population RR 1.03
(0.99 to 1.07)
3405
(10 studies)
⊕⊕⊕⊕
high
710 per 1000 731 per 1000
(703 to 760)
Moderate
680 per 1000 700 per 1000
(673 to 728)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
4C
olo
ny-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

1 Some of the trials were not allocation concealed. Most studies were unblinded2 The CI is very wide up to 20%3 Range of follow-up is wide
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
5C
olo
ny-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Description of the condition
Acute myeloid leukemia (AML) is a group of neoplastic disorders
characterized by the proliferation and accumulation of immature
hematopoietic cells in the bone marrow and blood. These ma-
lignant cells gradually replace and inhibit the growth and matu-
ration of normal erythroid, myeloid and megakaryocytic precur-
sors (Hoffman 2008). Acute myelogenous leukemia results from
sporadic acquired somatic mutations in hematopoietic progeni-
tors that confer a proliferative and/or survival advantage, impair
hematopoietic differentiation and confer properties of limitless
self-renewal. Approximately 8000 new cases of AML in the USA
occur per year and the incidence has remained stable over the last
decade. AML is a disease of adults with a median age at diagno-
sis of 65 years. AML represents approximately 90% of all acute
leukemias in adults. The age-specific incidence is 3.5:100,000, 15:
100,000 and 22:100,000 in individuals 50, 70 and 80 years, re-
spectively (Hoffman 2008).
The classification and diagnosis of AML has evolved from the
primarily morphologic and cytochemical system proposed by the
French American British (FAB) Co-operative Group in 1976
(Bennet 1976) to the current World Health Organization (WHO)
2008 classification (Vardiman 2009), which includes clinical in-
formation, cytogenetics and molecular abnormalities. The FAB
co-operative group classified the acute leukemias according to the
resemblance of the predominant leukemic cell type to a normal
differentiating hematopoietic precursor cell. The FAB group di-
vided the myeloid leukemias into eight broad categories based on
morphology, cytochemical staining and immunologic phenotype
of the predominant cell type, based on Wright-Giemsa stained
blood and marrow smears or biopsies. The WHO classification
defines unique clinical and biologically important subgroups. A
change introduced by the WHO classification reduces the defin-
ing blast threshold for the diagnosis of AML from 30% blasts to
20% blasts. The WHO classification has now replaced the FAB
classification of AML (Hoffman 2008).
Infiltration of the bone marrow by leukemic blasts is a major cause
of morbidity and mortality in AML patients due to neutropenia,
anemia and thrombocytopenia. Chemotherapy used for the treat-
ment of AML is highly suppressive and thus worsens myelosup-
pression. Moreover, it is more frequently associated with infec-
tious complications than regimens used to treat solid tumors. Al-
most all AML patients suffer from prolonged grade 4 neutrope-
nia during induction and intensive consolidation chemotherapy
and the incidence of neutropenic fever ranges between 50% and
90%, depending on the phase of the disease and the intensity of
chemotherapy (Ottmann 2007). Bacterial and fungal infections
are the major causes of morbidity and mortality in AML patients.
Overall, there are about 10% infectious deaths during induction
chemotherapy, with an even higher rate in patients older than 60
years of age (Bennett 1999; Bennett 2001). Allogeneic hematopoi-
etic stem cell transplantation is the treatment of choice for many
patients with AML. The major complications of allogeneic HSCT
are infections, the need for red blood cell and platelet transfu-
sions, organ damage, graft versus host disease (GVHD) and graft
rejection (Bernstein 1998; Blume 2004; Goker 2001; Lee 2003;
Nichols 2003; Smith 2006).
Given the uncertainty in the literature, several systematic re-
views and meta-analyses have previously assessed the efficacy of
hematopoietic CSFs among cancer patients. These reviews can be
divided into two groups: those looking at CSFs for the prevention
of febrile neutropenia and those looking at CSFs for the treatment
of febrile neutropenia. Both groups concentrated on infection-re-
lated outcomes. Patients with AML were included in these reviews,
although not always separately. For example, Dekker 2006 con-
ducted a meta-analysis including 34 trials to estimate the efficacy
of CSFs in stem cell transplantation. The results of this meta-anal-
ysis showed that CSFs reduced the risk of documented infections
and duration of parenteral antibiotics but did not reduce infection-
related or treatment-related mortality. Of note, this meta-analysis
included only AML patients undergoing hematopoietic stem cell
transplantation (HSCT) and not AML patients receiving induc-
tion or consolidation treatment. Furthermore, the study popula-
tion included all patients undergoing HSCT for any indication
and not only for AML. Sung 2004 published a meta-analysis on
the role of prophylactic CSFs in the reduction of the rate of febrile
neutropenia, hospitalization duration, documented infection rate,
parenteral antibiotic duration, amphotericin B use, or infection-
related mortality in children with cancer. They showed that CSFs
were associated with a 20% reduction in febrile neutropenia and
a shorter duration of hospitalization but did not reduce infection-
related mortality. Unlike the present meta-analysis, Sung 2004 in-
cluded only children and the patients included in this meta-anal-
ysis had all types of cancer and not only AML. Only one trial
included in the meta-analysis conducted by Sung included AML
patients (Channa 2002).
Our review addresses AML patients only, compiling trials that as-
sessed the use of growth factors during and after chemotherapy,
regardless of the indication. Thus, our review offers the opportu-
nity to assess endpoints related to the primary disease and overall
survival and concentrate on safety issues.
Description of the intervention
Hematopoietic CSFs are a class of cytokines that regulate pro-
liferation, differentiation and functions of hematopoietic cells.
More than 20 different molecules of CSFs have been identi-
fied. Among them, granulocyte colony-stimulating factor (G-
CSF) and the granulocyte macrophage colony-stimulating factor
(GM-CSF) have been studied in cancer patients. G-CSF regulates
the production of neutrophil lineage. The administration of G-
CSF to humans results in a dose-dependent increase in circulat-
6Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ing neutrophils. GM-CSF stimulates the growth of granulocyte,
macrophage and eosinophil colonies. Administration of GM-CSF
to humans results in a dose-dependent increase in blood neu-
trophils, eosinophils, macrophages and sometimes lymphocytes.
Different types of G-CSF and GM-CSF have been tested in clin-
ical trials (De Vita 2001).
CSFs may be administered in the context of AML in three
scenarios:
1. Before and/or during chemotherapy in a priming strategy,
in order to recruit leukemic cells into the cell-cycle and enhance
cell susceptibility to the cytotoxic effects of chemotherapy,
especially by cell-cycle specific agents like cytarabine.
2. After chemotherapy and/or allogeneic HSCT in order to
accelerate myeloid regeneration and decrease the incidence and
severity of neutropenia-associated infectious complications.
3. During febrile neutropenia with or without documented
infections in order to enhance recovery and resolution of
infection.
In the present systematic review and meta-analysis we included
only those trials reporting on patients treated with CSFs started
with or after chemotherapy (induction therapy, consolidation ther-
apy, salvage treatment or conditioning for HSCT) and continued
for more than 24 hours, in order to accelerate myeloid regenera-
tion and decrease the incidence and severity of neutropenia-asso-
ciated infectious complications. We excluded trials assessing the
role of CSFs for priming.
How the intervention might work
In most studies, shortening of neutropenia duration has been ac-
companied by reduced duration of fever, less use of antibiotics
and antifungal drugs and a shorter duration of hospitalization.
However, the incidence and severity of infections remained largely
unchanged and mortality was unchanged. In a systematic re-
view and meta-analysis, which included 1518 patients with febrile
neutropenia from 13 trials assessing all types of cancer, patients
randomized to receive CSFs experienced a shorter time to neu-
trophil recovery (hazard ratio (HR) 0.32; 95% CI 0.23 to 0.46),
a shorter length of hospitalization (HR 0.63; 95% CI 0.49 to
0.62), marginally less infection-related mortality (HR 0.56; 95%
CI 0.26 to 1.0) and no significant difference in overall mortality
(HR 0.68; 95% CI 0.43 to 1.08) (Clark 2000).
The effect of myeloid growth factors on other outcomes, such as
complete remission (CR) rate and disease-free survival (DFS) or
overall survival (OS) in AML patients, is not clear. AML cells,
like their normal cellular counterparts, express functional growth
factor receptors on their cell surface. The effect of having CSF
receptors on leukemic cells has been evaluated in multiple clinical
trials. Diverging results were reported (Griffin 1986; Inoue 1990;
Lemoli 1991; Lowenberg 1988; Ohno 1990; Ohno 1993; Ohno
1994; Park 1989; Souza 1986; Vellenga 1987; Witz 1998; Zittoun
1996).
CSFs stimulate clonogenic leukemic colony-forming units in vitro,
therefore their clinical application in leukemia has been contro-
versial. In vitro laboratory investigations have provided ample ev-
idence to show that the effect of chemotherapy on leukemic cells
can be amplified when they are simultaneously activated by CSFs
stimulation. While this effect is positive, caution must be taken
due to the risk that CSFs can cause leukemic cells to multiply
(Griffin 1986; Inoue 1990; Lemoli 1991; Lowenberg 1988; Park
1989; Souza 1986; Vellenga 1987; Witz 1998 ; Zittoun 1996).
According to the American Society of Clinical Oncology (ASCO)
recommendations, the use of CSFs following induction therapy
is reasonable, although there has been no favorable impact on
remission rate, remission duration or survival (Smith 2006).
According to the ASCO guidelines, when the risk of febrile neu-
tropenia is approximately 20%, reduction in febrile neutropenia
is an important clinical outcome that justifies the use of CSFs,
regardless of the impact on other factors (Smith 2006). The use
of CSFs following allogeneic blood HSCT has been shown to de-
crease the duration of absolute neutropenia but did not lead to
shortened hospitalizations, cost savings or reduced antibiotic use
(Smith 2006). The potential risks of CSFs in the management of
AML remain inconclusive.
Why it is important to do this review
A systematic review and meta-analysis assembling the current data
might provide more conclusive evidence regarding the role and
safety of CSFs in the management of patients with AML and might
help in establishing the policy of treatment for patients with AML
after induction, consolidation or salvage therapy and after HSCT.
In the present systematic review and meta-analysis we evaluate the
safety of CSFs administered after these treatment phases.
O B J E C T I V E S
• To evaluate the safety and efficacy of CSFs administered
after induction, consolidation or salvage treatment and after
HSCT in patients with AML.
• To evaluate the safety of CSFs in young versus elderly
patients as defined per study (usually older than 55 to 60 years).
M E T H O D S
Criteria for considering studies for this review
Types of studies
7Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Randomized controlled trials.
Types of participants
Patients with AML of all six main WHO 2008 classification
categories (AML with recurrent genetic abnormalities, AML
with myelodysplasia-related changes, therapy-related myeloid neo-
plasms, AML not otherwise specified, myeloid sarcoma, myeloid
proliferations related to Down syndrome) (Vardiman 2009)) at all
stages of treatment after the administration of chemotherapy (in-
duction, consolidation, salvage treatment and those undergoing
HSCT). AML patients were included irrespective of age.
We included studies that assessed patients with AML as part of a
cohort with other cancer patients or those undergoing HSCT and
we tried to extract outcomes separately from the publications or
through correspondence with the primary investigators. If separate
data were unavailable, we excluded the study if the AML patients
constituted less than 75% of the study cohort.
Types of interventions
Intervention
CSFs, including G-CSF or GM-CSF, administered either intra-
venously or subcutaneously, started with or after chemotherapy
(induction, consolidation, salvage or conditioning for HSCT) and
continued for more than 24 hours, compared with placebo or no
treatment. We included both patients with and without neutrope-
nia (absolute blood neutrophil count less than 0.5 x 103/ml) and/
or fever on admission. Fever was defined per study according to the
definitions of neutropenic fever (usually, body temperature higher
than 38.3 °C or 38.5 ºC on one occasion or higher than 38 °C on
two or more occasions).
We excluded CSFs administered for the purpose of stem cell col-
lection and/or priming, namely: CSFs administered before and/
or only for the duration of chemotherapy.
Types of outcome measures
Primary outcomes
• All-cause mortality at the end of study follow up (number
of deaths out of number evaluated).
• Overall survival (hazard ratio (HR); 95% confidence
interval (CI)).
Although both outcomes express the same meaning, the way of
reporting is different and each outcome includes different RCTs.
Secondary outcomes
• All-cause mortality at 30 days (number of deaths/number
evaluated) (mortality at 30 days usually parallels mortality related
to AML induction treatment).
• Number of patients achieving complete remission (CR)
defined according to the International Working Group at the
time point as defined per study (Cheson 1990).
• Disease-free survival (DFS) (HR; 95% CI) and number of
patients with relapse.
• Neutropenia duration from randomization (mean or
median).
• Episodes of febrile neutropenia per patient and per patient-
day (number of patients and number of episodes).
• Episodes of invasive fungal infections (IFI), defined as
probable or proven IFI according to acceptable guidelines
(Ascioglu 2002; De Pauw 2008).
• Number of bacteremias per patient.
• Duration of hospital stay (mean or median) (only inpatients
were included for the evaluation of hospitalization duration).
• Any adverse events.
• Adverse events requiring discontinuation of CSFs
including: bone pain, allergic reaction (rash, urticaria, facial
edema, respiratory (wheezing, dyspnea), and cardiovascular
(hypotension, tachycardia), splenic rupture, acute respiratory
distress syndrome (ARDS).
• Secondary leukemia according to new chromosomal
aberrations or a different type of leukemia.
Search methods for identification of studies
Electronic searches
We conducted a comprehensive search strategy to identify both
published and unpublished trials, with no restriction on language
or study years. We identified relevant randomized clinical trials by
searching the Cochrane Review Group (CRG), Cochrane Central
Register of Controlled Trials (The Cochrane Library 2010, Issue 7)
(Appendix 1), MEDLINE (January 1966 to July 2010) (Appendix
2), LILACS (up to December 2009), and references of all included
studies and major reviews. In addition, we searched the following
conference proceedings (2002 to June 2010):
• European Group for Bone and Marrow Transplantation
(available at: http://www.ebmt.org/);
• Annual Meeting of the European Hematology Association
(available at: http://www.ebmt.org/);
• Annual Meeting of the Society for Hematology and Stem
Cells (available at: http://www.exphem.org/); and
• The Center for International Blood and Marrow Transplant
Research (CIBMTR) (http://www.cibmtr.org/).
8Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Searching other resources
We inspected all identified studies for references to further trials.
Data collection and analysis
Selection of studies
YB and RG independently inspected each reference identified by
the search and applied the inclusion criteria. For possibly relevant
articles, or in cases of disagreement between the two review au-
thors, we obtained the full article and the two review authors in-
spected it independently.
Data extraction and management
Two review authors independently extracted the data from the
included trials. In case of any disagreement, a third review author
extracted the data. We discussed the data extraction, documented
our decisions and, where necessary, contacted the study authors
for clarification.
Trials were identified by the name of the first author and year in
which the trial was first published and ordered chronologically.
We extracted the following data from the included studies:
Characteristics of trials
• Date (defined as recruitment initiation year); location
(country); centre (single centre or multi-centre); setting of trial
(inpatients or outpatients)(if inpatients - isolation single room,
laminar air flow room, positive pressure room).
• Publication status: published; published as abstract;
unpublished.
• Design of trial: sources of bias: sequence generation and
allocation concealment; blinding; incomplete outcome data;
selective reporting.
• Sponsor of trial (specified, known, unknown).
• Duration of follow up: duration of planned CSFs
administration; duration of follow up after the intervention and
actual duration of follow up in the study.
• Case definitions used (inclusion and exclusion criteria
defined by each trial).
• Inclusion criteria as defined by study: age; type of AML
(morphology criteria according to the FAB classification);
leukemia type (de novo AML, secondary AML, refractory AML,
relapsed AML); white blood cell count; platelet count; treatment
stage (induction, consolidation, relapse).
Characteristics of participants
• Number of participants in each group.
• FAB subtype (M0 to M7, not assessed).
• Disease stage (newly diagnosed AML, primarily refractory
AML, relapsed AML, relapsed and refractory AML).
• Type of treatment (induction, consolidation, salvage). We
recorded specifically for each treatment the chemotherapy
protocol administered including the type of chemotherapy, dose
intensity and schedule.
• Age.
• Gender.
• Eastern Co-operative Oncology Group (ECOG) status.
• Cytogenetics (favorable, normal, unfavorable, not assessed).
• Infection at diagnosis (number of patients) (none, FUO
(fever of unknown origin, i.e.>38.3°C on several occasions,
duration of >3 weeks and failure to reach diagnosis despite 1
week of inpatient investigation, documented infection, severe
infection at diagnosis).
• White cell count at diagnosis (number of patients).
• Mean marrow blast infiltration (in %).
• Fever at diagnosis.
• Prophylactic antibiotics.
Characteristics of interventions
• Type of CSF.
• Dose of CSF.
• Schedule of administration.
• Total duration of intervention.
Characteristics of outcome measures as defined
above
We extracted outcomes preferably by intention-to-treat, including
all individuals randomized in the outcome assessment.
Assessment of risk of bias in included studies
Two review authors assessed the trials fulfilling the review inclu-
sion criteria for methodological quality. We extracted information
about randomization and allocation concealment, blinding, sam-
ple size, exclusions after randomization, and different lengths of
follow up. We used the criteria described in the Cochrane Handbook
for Systematic Reviews of Interventions (Higgins 2009) and ‘Risk of
bias’ tables. The standard ‘Risk of bias’ table includes assessments
for sequence generation, allocation sequence concealment, blind-
ing, incomplete outcome data, selective outcome reporting and
‘other issues’. For each item, the table provides a description of
what was reported to have happened in the study and a subjective
judgment regarding protection from bias (low risk of bias, high
risk of bias or unclear risk of bias).
Measures of treatment effect
We analyzed dichotomous data by calculating the risk ratio (RR)
for each trial with the uncertainty in each result being expressed
9Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

using 95% confidence intervals (CI). We pooled trial results ac-
cording to the duration of follow up at the time at which outcomes
were assessed.
Dealing with missing data
The four general recommendations for dealing with missing data
in Cochrane Reviews were followed (Higgins 2009).
• Whenever possible we contacted the original investigators
to request missing data.
• We clearly stated the assumptions of any methods used to
cope with missing data.
• We performed sensitivity analyses to assess how sensitive
results are to reasonable changes in the assumptions that are
made.
• We addressed the potential impact of missing data on the
findings of the review in the Discussion section.
Assessment of heterogeneity
We assessed heterogeneity (degree of difference between the results
of different trials) in the results of the trials using a Chi2 test of
heterogeneity and the I2 statistic measure of inconsistency.
The Chi2 test assesses whether observed differences in results are
compatible with chance alone. A low P value (or a large Chi2
statistic relative to its degree of freedom) provides evidence of het-
erogeneity of intervention effects (variation in effect estimates be-
yond chance). A useful statistic for quantifying inconsistency is
the I2 (measure of inconsistency). A rough guide to interpretation
of the I2 statistic is as follows: 0% to 40%: might not be impor-
tant; 30% to 60%: may represent moderate heterogeneity; 50%
to 90%: may represent substantial heterogeneity; 75% to 100%:
considerable heterogeneity (Higgins 2009).
We also investigated heterogeneity through subgroup and sensi-
tivity analyses as defined below (Higgins 2002; Higgins 2003).
Assessment of reporting biases
Reporting biases arise when the dissemination of research find-
ings is influenced by the nature and direction of results. There
are several types of reporting bias: publication bias, time-lag bias,
multiple (duplicate) publication bias, location bias, citation bias,
language bias and outcome reporting bias .
To avoid reporting bias we searched comprehensively for studies
that met the eligibility criteria for a Cochrane Review. We searched
multiple sources but study reports may selectively present results,
reference lists may selectively cite sources and duplicate publication
of results can be difficult to spot. Furthermore, the availability of
study information may be subject to time-lag bias, particularly in
fast-moving research areas. In order to reduce reporting biases we
included unpublished studies and trial registries. Prospective trial
registration has the potential to substantially reduce the effects of
publication bias.
Small study effects are one of the possible causes of publication
bias, i.e. a tendency for estimates of the intervention effect to be
more beneficial in smaller studies. Funnel plots allow for a visual
assessment of whether small study effects are present in the meta-
analysis. Funnel plots are valid for continuous outcomes but less
so for dichotomous outcomes. When there was evidence of small
study effects we attempted a funnel plot to understand the source
of the small study effects and considered their implications in
sensitivity analyses (Higgins 2009).
Data synthesis
We used the Mantel-Haenszel method (Review Manager
(RevMan) RevMan 2011) to estimate risk ratios (RR) and 95%
confidence intervals (CI) for dichotomous data. We used a fixed-
effect model and performed a sensitivity analysis by repeating the
above analysis using a random-effects model (DerSimonian and
Laird method) (DerSimonian 1986). We analyzed time-to-event
outcomes as hazard ratios (HR) and estimated their variances as
described by Parmar et al (Parmar 1998). We pooled time-to-event
variables using the inverse of variance. We analyzed continuous
data using the mean and standard deviation (SD) of each trial and
calculating the effect size (average mean difference) and the 95%
CI.
Subgroup analysis and investigation of heterogeneity
We performed subgroup analyses in order to assess the impact of
these possible sources of heterogeneity on mortality at the end of
follow up and on complete remission (CR).
• Age > 60 versus age < 60 including children (or otherwise
defined for elderly AML).
• Type of treatment: induction versus consolidation.
• Type of CSF: G-CSF versus GM-CSF.
• Patients undergoing chemotherapy only versus those
undergoing allogeneic HSCT.
Sensitivity analysis
We performed sensitivity analyses in order to assess the robust-
ness of the findings to different aspects of the trials’ methodology:
allocation concealment (adequate or unclear), allocation genera-
tion (adequate or unclear), blinding (double-blinded or unblinded
studies) and intention-to-treat analysis (ITT).
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
10Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The computerized search strategy identified 1421 potentially rele-
vant publications, of which we considered 89 publications for fur-
ther investigation. Of them, we excluded 46 publications, report-
ing on 40 trials, as described below. We included 43 publications
reporting on 19 trials.
Included studies
Nineteen trials (43 publications) performed between the years
1990 and 2003 and including a total of 5256 patients (range 53
to 803 patients per trial) fulfilled the inclusion criteria (Amadori
2005; Beksac 2010; Bernasconi 1998; Bradstock 2001; Dombret
1995; Estey 1999; Godwin 1998; Harousseau 2000; Heil 1997;
Lehrnbecher 2007; Lowenberg 1997; Milligan 2006; Nakajima
1995; Rowe 1995; Stone 1995; Usuki 2002; Wheatley 2009; Witz
1998; Zittoun 1996).
Type of patients
Patients with AML were defined according to the WHO 2008
classification. In four studies the age of the patients ranged from
15 to 60 years (Bradstock 2001; Harousseau 2000; Lowenberg
1997; Zittoun 1996), in six studies the age of the patients was
above 55 years (Amadori 2005; Dombret 1995; Godwin 1998;
Rowe 1995; Stone 1995; Witz 1998), in one study patients’ ages
were lower than 18 years (Lehrnbecher 2007) and in the remaining
studies, patients’ ages were higher than 15 years with no upper
limit (Beksac 2010; Heil 1997; Usuki 2002).
Chemotherapy regimens
Seventeen trials included patients undergoing induction che-
motherapy (Amadori 2005; Beksac 2010; Bernasconi 1998;
Bradstock 2001; Dombret 1995; Estey 1999; Godwin 1998;
Heil 1997; Lehrnbecher 2007; Lowenberg 1997; Nakajima 1995;
Rowe 1995; Stone 1995; Usuki 2002; Wheatley 2009; Witz 1998;
Zittoun 1996), one trial included patients undergoing consolida-
tion chemotherapy (Harousseau 2000) and one trial included pa-
tients undergoing salvage chemotherapy (Milligan 2006).
The chemotherapy protocols used in the trials were heteroge-
neous. They consisted of different combinations of anthracyclines
(daunorubicin, idarubicin or mitoxantrone) and cytarabine with
or without etoposide. In seven trials the chemotherapy regimen in-
cluded intravenous (IV) daunorubicin 45 to 60 mg/m2 for three to
four days and intravenous cytarabine 100 to 200 mg/m2 for seven
days with etoposide (Heil 1997) or without it ( Dombret 1995;
Godwin 1998; Lowenberg 1997; Rowe 1995; Stone 1995; Zittoun
1996). In five trials the regimen included intravenous idarubicin 8
to 12 mg/m2 and intravenous cytarabine 100 mg/m2 with etopo-
side (Bernasconi 1998; Bradstock 2001; Witz 1998) or without
it (Beksac 2010; Lehrnbecher 2007). One trial also combined
idarubicin with fludarabine (Estey 1999). Two trials consisted of
mitoxantrone-containing regimens with cytarabine and etoposide
(Amadori 2005; Harousseau 2000). Three trials included several
chemotherapy regimens depending on physicians’ choice and the
population’s age (Milligan 2006; Usuki 2002; Wheatley 2009). In
one trial the chemotherapy regimen was not reported (Nakajima
1995).
Intervention
Type of CSF
The CSF used in five trials was GM-CSF (Lowenberg 1997;
Rowe 1995; Stone 1995; Witz 1998; Zittoun 1996), while in 14
trials G-CSF was used (Amadori 2005; Beksac 2010; Bernasconi
1998; Bradstock 2001; Dombret 1995; Estey 1999; Godwin 1998;
Harousseau 2000; Heil 1997; Lehrnbecher 2007; Milligan 2006;
Nakajima 1995; Usuki 2002; Wheatley 2009).
Schedule
CSF administration started concurrent with chemotherapy in
three trials (Estey 1999; Milligan 2006; Witz 1998), during the
48-hour period post-chemotherapy in 10 trials (Amadori 2005;
Bernasconi 1998; Bradstock 2001; Dombret 1995; Harousseau
2000; Heil 1997; Lowenberg 1997; Stone 1995; Usuki 2002;
Zittoun 1996) and 48 hours after chemotherapy completion in
five trials (Beksac 2010; Godwin 1998; Lehrnbecher 2007; Rowe
1995; Wheatley 2009).
Excluded studies
We excluded 40 trials (46 publications). Reasons for exclusion
were the following:
• Non-randomized studies: 15 trials (Bernell 1994; Braess
2006; Buchner 2004; Chen 1998; Estey 1990; Freud 1995;
Godwin 1995; Kalaycio 2001; Kern 1998; Maslak 1996;
Montillo 1998; Moore 1997; Schriber 1994; Takeshita 1995;
Takeshita 2000).
• Studies which did not randomize CSF: four trials (Hanel
2001; Ossenkopple 2004; Stone 2001; Thomas 2007b).
• Studies which randomized different schedules of CSF: four
trials (Ohtake 2006; Sierra 2005; Takeyama 1995; von Lilienfeld
Toal 2007).
• Randomized studies of CSF with a low number of AML
patients included: two trials (Bishop 2000; Ojeda 1999).
• Randomized study with use of monocyte colony-
stimulating factor which was not in the included characteristics
(Ohno 1997).
• Studies evaluating the role of CSFs for the purpose of
priming (e.g. before and/or only for the duration of
chemotherapy): nine trials (Buchner 1993; Frenette 1995; Hast
2003; Heil 1995; Lowenberg 1997; Lowenberg 2003; Ohno
1994; Rowe 2004; Thomas 2007a).
11Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• Studies which evaluated CSFs for the purpose of stem cell
collection: two trials (Morton 2001;Schmitz 1998).
• Double publication: two trials (Creutzig 2006;Goldstone
2001).
Risk of bias in included studies
See Characteristics of included studies, ’Risk of bias’ tables.
We assessed generation of randomization sequence as adequate in
four studies (classified as low risk of bias). In the other 15 studies
the method of randomization was not specified (classified as high
risk of bias).
Allocation
Allocation concealment was adequate in 12 studies (classified as
low risk of bias). In the remaining seven studies the method of
allocation concealment was not clear (classified as high risk of
bias).
Blinding
Four studies were conducted in a double-blinded manner
(placebo-controlled), however it was not mentioned which per-
sons were blinded. All the remaining trials were open or blinding
was not reported.
Incomplete outcome data
In all trials the numbers and reasons for dropout were reported in
the original articles.
Selective reporting
All the included trials were published in full text.
Effects of interventions
See: Summary of findings for the main comparison All cause
mortality for prevention and treatment of infectious complications
in patients with acute myelogenous leukemia; Summary of
findings 2 Overall survival for prevention and treatment of
infectious complications in patients with acute myelogenous
leukemia; Summary of findings 3 Complete remission for
prevention and treatment of infectious complications in patients
with acute myelogenous leukemia; Summary of findings 4
Disease free survival for prevention and treatment of infectious
complications in patients with acute myelogenous leukemia;
Summary of findings 5 Relapse rate for prevention and treatment
of infectious complications in patients with acute myelogenous
leukemia; Summary of findings 6 Bacteremias for prevention
and treatment of infectious complications in patients with
acute myelogenous leukemia; Summary of findings 7 Invasive
fungal infections for prevention and treatment of infectious
complications in patients with acute myelogenous leukemia;
Summary of findings 8 Episodes of febrile neutropenia for
prevention and treatment of infectious complications in patients
with acute myelogenous leukemia; Summary of findings 9
Adverse events requiring discontinuation of CSFs for prevention
and treatment of infectious complications in patients with acute
myelogenous leukemia
Primary outcomes
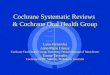
1. All-cause mortality at the end of study follow up
Fourteen trials including 4119 patients reported all-cause mortal-
ity. The end of study follow up ranged between three and seven
years. The addition of colony-stimulating factors (CSFs) to che-
motherapy yielded no difference in all-cause mortality between
patients treated with chemotherapy and CSFs and those treated
with chemotherapy alone, with a risk ratio (RR) of 1.01 (95%
confidence interval (CI) 0.98 to 1.05) (Figure 1). The results did
not change when we performed a sensitivity analysis using a ran-
dom-effects model (Figure 2).
12Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Forest plot of comparison: All-cause mortality at the end of follow up
When tested, the quality of allocation concealment (adequate
or unclear) had no statistically significant impact on the results.
Pooled RR of trials with adequate allocation concealment was 1.03
(95% CI 0.99 to 1.07, 10 trials) at the end of follow up.
Subgroup analysis of the primary outcome
Results were not influenced by age of patients or type of CSFs.
In subgroup of patients older than 60 years versus younger than
60 years, CSFs did not reduce all-cause mortality, with a RR of
1.01 (95% CI 0.97 to 1.05, eight trials) and 1.08 (95% CI 0.97
to 1.20, five trials) respectively (Figure 3; Figure 4).
Type of CSF had no effect on outcomes. Mortality of patients
treated with G-CSF (RR 1.00; 95% CI 0.97 to 1.05, nine trials)
and GM-CSF (RR 1.05; 95% CI 0.96 to 1.14, four trials) was
similar.
We did not conduct a subgroup analysis by type of chemotherapy
since only one trial included patients who received consolidation
chemotherapy while most trials included patients who received
induction chemotherapy.
Also, we did not conduct a subgroup analysis by conventional
chemotherapy versus allogeneic transplantation since no trial in-
cluded patients undergoing allogeneic transplantation.
2. Overall survival
Eleven trials including 3335 patients reported on overall survival.
The addition of CSFs to chemotherapy yielded no difference in
overall survival between patients treated with chemotherapy and
CSFs and those treated with chemotherapy alone, with a hazard
ratio (HR) of 1.00 (95% CI 0.93 to 1.08, 11 trials) (Figure 2).
13Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Forest plot of comparison: 2 Overall survival, outcome: 2.1 Overall survival.
Secondary outcomes
All-cause mortality at 30 days
Eleven trials including 3319 patients reported all-cause mortality
at 30 days. The addition of CSFs to chemotherapy yielded no dif-
ference in all-cause mortality between patients treated with che-
motherapy and CSFs and those treated with chemotherapy alone,
with a RR of 0.97 (95% CI.0.80 to 1.18) (Figure 3).
Figure 3. Forest plot of comparison: 1 All-cause mortality, outcome: 1.1 All-cause mortality at 30 days.
14Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Complete remission (CR)
Seventeen trials including 4774 patients reported CR rate.
The addition of CSF to chemotherapy compared to placebo or no
intervention did not alter the rate of CR, with a RRof 1.03 (95%
CI 0.99 to 1.07) (Figure 4).
Figure 4. Forest plot of comparison: 3 Complete remission, outcome: 3.1 Complete response.
Disease-free survival (DFS)
Seven trials including 1639 patients reported on DFS. There was
no difference in DFS between patients receiving or not receiving
CSFs(HR 1.00; 95% CI 0.90 to 1.13) (Figure 5).
Figure 5. Forest plot of comparison: 4 Disease-free survival, outcome: 4.1 Disease-free survival.
15Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Relapse rate
Ten trials including 2189 patients reported on relapse rate. The
addition of CSFs to chemotherapy yielded no difference in relapse
rate between the two groups(RR 0.97; 95% CI 0.89 to 1.05)
(Figure 6).
Figure 6. Forest plot of comparison: 5 Relapse rate, outcome: 5.1 Relapse rate.
Episodes of febrile neutropenia per patient
Ten trials including 2140 patients reported on episodes of febrile
neutropenia. The use of CSFs did not decrease the occurrence of
these events(RR 0.98; 95% CI 0.94 to 1.03) (Figure 10).
Bacteremias
Seven trials including 1638 patients reported on bacteremias. The
administration of CSFs did not decrease the occurrence of bac-
teremias(RR 0.96; 95% CI 0.82 to 1.12) (Figure 11).
Invasive fungal infections
Four trials including 929 patients reported invasive fungal infec-
tions. The addition of CSFs did not decrease the occurrence of
invasive fungal infections(RR 1.40; 95% CI 0.90 to 2.19) (Figure
12).
Duration of neutropenia
Seventeen studies reported on neutropenia duration. In studies
where neutropenia was defined as less than 0.5 x 109 /L neutrophils
(nine trials) the median duration of neutropenia ranged between
12 and 24 days in the CSFs arm and between 17 and 29 days
in the control arm (Amadori 2005; Bradstock 2001; Godwin
1995; Harousseau 2000 ; Heil 1997; Lehrnbecher 2007; Stone
1995; Witz 1998; Zittoun 1996). In studies where neutropenia
was defined as less than 1.0 x 109/L neutrophils (four trials) the
median duration of neutropenia ranged between 7 and 26 days
in the CSF arm and between 16 and 30 days in the control arm
(Bernasconi 1998; Dombret 1995; Estey 1999; Milligan 2006).
CSFs significantly shortened the duration of neutropenia in all
studies except for one (Zittoun 1996). We could not conduct a
meta-analysis on this outcome since it is a non-normally dispersed
variable and outcomes were reported as medians in most trials with
different dispersion measures, and were non-normally dispersed.
Hospital stay duration
16Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Twelve trials reported on the duration of hospitalization. The me-
dian duration of hospitalization ranged between 23 and 36 days in
the CSF arm and between 27 and 38 days in the control arm. Sev-
eral studies reported on a significant shortening of hospitalization
duration with CSF administration (Amadori 2005; Harousseau
2000; Heil 1997; Milligan 2006 ; Wheatley 2009), while others
showed no significant difference (Beksac 2010; Bradstock 2001;
Godwin 1995; Lowenberg 1997; Stone 1995; Witz 1998). Due
to the variability in data reporting we could not conduct a meta-
analysis on this outcome.
Any adverse events
Only two studies reported on the total number of adverse events,
therefore we could not conduct a meta-analysis. One study re-
ported on 11 cases with adverse events in the CSF arm while no
adverse events were reported in the control arm (Usuki 2002).
Another study reported on 25 cases in the CSF arm compared to
nine cases in the control arm (Zittoun 1996).
Adverse events requiring discontinuation of CSFs
Four studies, including 770 patients, reported on adverse events
requiring discontinuation of CSFs (Rowe 1995; Stone 1995; Witz
1998; Zittoun 1996). There were marginally statistically more
adverse events requiring discontinuation of CSFs in the CSF arm
compared to the control arm(RR 1.33; 95% CI 1.00 to 1.76)
(Figure 13).
In addition, three studies reported on adverse events of grade three
to four and in all of them there was no statistical difference between
the CSF arm and the control (Amadori 2005; Bradstock 2001;
Godwin 1995).
Secondary leukemia
There was no report of secondary leukemia in any of the included
studies, except for Lehrnbecher 2007 who described three events
of secondary malignancies in the control arm compared to one
event in the CSF arm.
17Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A D D I T I O N A L S U M M A R Y O F F I N D I N G S [Explanation]
Overall survival for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patientswith acute myelogenous leukemia
Settings:inpatients
Intervention: Overall survival
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Overall survival
Overall survival
Follow-up: 3-5 years
722 per 1000 722 per 1000
(696 to 749)
HR 1
(0.93 to 1.08)
3335
(11 studies)
⊕⊕©©
low1,2
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; HR: Hazard ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Some of RCTs are lack of allocation concealment. Only four RCTs are double blinded.2 The CI is wide regarding OS - There is 7% chance that CSFs can improved survival and also there is 8% that CSFs cannot improved
survival.
18
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Complete remission for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings:inpatients
Intervention: Complete remission
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Complete remission
complete response Study population RR 1.03
(0.99 to 1.07)
4774
(17 studies)
⊕⊕⊕©
moderate1
642 per 1000 661 per 1000
(635 to 687)
Moderate
612 per 1000 630 per 1000
(606 to 655)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Some of the studies lack allocation concealement
19
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Disease free survival for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings:inpatients
Intervention: Disease free survival
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Disease free survival
Disease free survival Study population OR 1
(0.9 to 1.13)
1639
(7 studies)
⊕⊕©©
low1,2
728 per 1000 728 per 1000
(706 to 751)
Moderate
722 per 1000 722 per 1000
(700 to 746)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; OR: Odds ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Part of the studies were not blinded and allocation was not concealed2 The CI was wide
20
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Relapse rate for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings:
Intervention: Relapse rate
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Relapse rate
Relapse rate Study population RR 0.97
(0.89 to 1.05)
2189
(10 studies)
⊕⊕©©
low1,2
513 per 1000 498 per 1000
(456 to 539)
Moderate
547 per 1000 531 per 1000
(487 to 574)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Not in all studies was allocation concealed2 CI interval is not narrow
21
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Bacteremias for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patientswith acute myelogenous leukemia
Settings:inpatients
Intervention: Bacteremias
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Bacteremias
Bacteremia Study population RR 0.96
(0.82 to 1.12)
1638
(7 studies)
⊕⊕⊕©
moderate1
267 per 1000 256 per 1000
(219 to 299)
Moderate
272 per 1000 261 per 1000
(223 to 305)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Very wide CI
22
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Invasive fungal infections for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patientswith acute myelogenous leukemia
Settings:
Intervention: Invasive fungal infections
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Invasive fungal infec-
tions
Invasive fungal infection Study population RR 1.4
(0.9 to 2.19)
929
(4 studies)
⊕⊕©©
low1,2
62 per 1000 87 per 1000
(56 to 136)
Moderate
53 per 1000 74 per 1000
(48 to 116)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Most studies were not allocation concealed or blinded2 Very wide CI
23
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Episodes of febrile neutropenia for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: patients with prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings:inpatients
Intervention: Episodes of febrile neutropenia
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Episodes of febrile neu-
tropenia
Episodes of febrile neu-
tropenia
Study population RR 0.98
(0.94 to 1.03)
2140
(9 studies)
⊕⊕⊕©
moderate1
710 per 1000 696 per 1000
(667 to 731)
Moderate
731 per 1000 716 per 1000
(687 to 753)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 In half of the studies allocation was not concealed and were not blinded
24
Co
lon
y-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Adverse events requiring discontinuation of CSFs for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Patient or population: Prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Settings:inpatients
Intervention: Adverse events requiring discontinuation of CSFs
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Control Adverse events requir-
ing discontinuation of
CSFs
Adverse events requir-
ing discontinuation of
CSFs
Study population RR 1.33
(1 to 1.76)
770
(4 studies)
⊕©©©
very low1,2
156 per 1000 207 per 1000
(156 to 274)
Moderate
21 per 1000 28 per 1000
(21 to 37)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Very wide CI2 Allocation of most studies was not concealed and generally studies were not blinded2
5C
olo
ny-stim
ula
ting
facto
rsfo
rp
reven
tion
an
dtre
atm
en
to
fin
fectio
us
co
mp
licatio
ns
inp
atie
nts
with
acu
tem
yelo
gen
ou
sle
ukem
ia
(Revie
w)
Co
pyrig
ht
©2012
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

D I S C U S S I O N
Summary of main results
Our aim was to assess the influence of colony-stimulating factors
(CSFs) on the prevention and treatment of infectious complica-
tions in acute myelogenous leukemia (AML) patients. The addi-
tion of CSFs did not alter all-cause mortality in the short and long
term. The administration of CSFs did not affect the occurrence
of episodes of neutropenic fever, bacteremias or invasive fungal
infections. There was also no effect on hematological outcomes,
including complete remission, relapse rate or disease-free survival.
Potential biases in the review process
We carried out a subgroup analysis according to age (above 60
years) which did not show any advantage for the addition of CSFs
to chemotherapy in elderly patients. Nevertheless, this analysis
included only eight trials. Furthermore, we could not perform a
subgroup analysis by type of treatment (induction versus consoli-
dation) or by leukemia prognostic factors such as cytogenetic anal-
ysis, due to lack of data.
A meta-analysis of secondary outcomes such as neutropenia and
hospitalization duration could not be carried out since these vari-
ables were not given as mean numbers but mostly as medians
which are parameters that are not distributed normally and thus
cannot be pooled in a meta-analysis. We therefore conducted a
descriptive analysis of these outcomes.
Agreements and disagreements with otherstudies or reviews
The American Society of Clinical Oncology (ASCO) recommen-
dations state that it is reasonable to use CSFs after induction che-
motherapy in AML patients despite lack of evidence to prove this
(Smith 2006), whereas the British Society of Haematology guide-
lines are more straightforward in not recommending the routine
use of CSFs for the post-induction period (Milligan 2006). Both
the ASCO and the British Society of Haematology guidelines
state that CSFs can be recommended after the completion of the
consolidation phase on the basis of two randomized controlled
trials showing a significant decrease in duration of neutropenia
(Harousseau 2000; Heil 1997; Milligan 2006; Smith 2006).
A recent meta-analysis which focused on AML patients was pub-
lished by Wang et al. The authors compared the use of granulo-
cyte colony-stimulating factor (G-CSF) in AML patients receiv-
ing chemotherapy to placebo or no treatment. It concentrated on
overall survival and remission rate and showed that the addition of
G-CSF did not alter overall survival (Wang 2009a), yet it showed
an improved complete remission in the G-CSF arm compared to
the control arm (Wang 2009b). These conclusions regarding over-
all survival were based only on seven randomized controlled trials
(RCTs). Conversely, the present systematic review summarizes all
the evidence currently available, including 19 RCTs which used
G-CSF as well as GM-CSF, and thus is more powerful in its capac-
ity to support or challenge these results. Regarding the outcome
of complete remission Wang’s meta-analysis included five RCTs;
one of them was published with partial results (Goldstone 2001).
In our meta-analysis, however, the conclusions are based on 17
RCTs; 12 of them used G-CSF.
Another systematic review and meta-analysis has recently been
published by Heuser et al. The authors evaluated the use of CSFs
in adult AML patients receiving chemotherapy in two separate
meta-analyses: primary prophylaxis and priming. The first meta-
analysis, focusing on primary prophylaxis, included 14 RCTs with
4069 participants. It showed that CSFs decreased time to neu-
trophil recovery and hospitalization stay, yet it did not influence
other important outcomes(i.e. complete remission rate, event/dis-
ease-free survival or overall survival. The second meta-analysis, fo-
cusing on the use of CSFs for priming, also consisted of 14 studies
with 4518 participants. There was no difference in complete re-
mission rate, event/disease-free survival or overall survival (Heuser
2010). Our meta-analysis focused on primary prophylaxis only,
yet it included RCTs irrespective of age. Therefore, it included
more RCTs on this subject (19 RCTs versus 14 RCTs in Heuser
et al). The results of both meta-analyses were similar.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
In summary, colony-stimulating factors should not be given rou-
tinely to acute myelogenous leukemia patients post-chemotherapy
since they do not improve overall survival, or infectious parameters
including the rate of bacteremias and invasive fungal infections.
Yet, our results show that, on the other hand, they do not adversely
affect hematological outcomes such as complete remission, relapse
rate and disease-free survival.
Implications for research
Further randomized controlled trials should be encouraged in or-
der to examine the role of colony-stimulating factors in specific
acute myelogenous leukemia patient subgroups, such as elderly
patients, those at different treatment stages and those with various
genetic abnormalities.
A C K N O W L E D G E M E N T S
We thank Prof. Lowenberg and Prof. Beksac for providing com-
plementary data from their trials.
26Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Amadori 2005 {published data only}
Amadori S, Suciu S, Jehn U, Stasi R, Thomas X, Marie JP,
et al.Use of glycosylated recombinant human G-CSF during
and/or after induction chemotherapy in elderly patients
with acute myeloid leukemia: final results of AML-13, a
randomized phase III study of the EORTC and GIMEMA
Leukemia Groups. Blood 2003;102:177a.∗ Amadori S, Suciu S, Jehn U, Stasi R, Thomas X, Marie
JP, et al.EORTC/GIMEMA Leukemia Group. Use of
glycosylated recombinant human G-CSF (lenograstim)
during and/or after induction chemotherapy in patients 61
years of age and older with acute myeloid leukemia: final
results of AML-13, a randomized phase-3 study. Blood
2005;106(1):27–34.
Amadori SA, Suciu S, Jehn U, Thomas X, Marie JP, Muus P,
et al.Lenograstim combined with induction chemotherapy
in elderly patients with AML: results of a randomized phase
III trial (AML-13) of the EORTC Leukemia Group and
the GIMEMA Cooperative Group. European Hematology
Association Website (http://www.ehaweb.org) 2003.
Beksac 2010 {published data only}
Beksac M, Ali R, Ozcelik T, Ozcan M, Ozcebe O, Bayik M,
et al.Short and long term effects of granulocyte colony-
stimulating factor during induction therapy in acute
myeloid leukemia patients younger than 65: results of a
randomized multicenter phase III trial. Leukemia Research
2011;35(3):340–5.
Bernasconi 1998 {published data only}
Bernasconi C, Alessandrino EP, Bernasconi P, Bonfichi M,
Lazarino M, Canevari A, et al.Randomized clinical study
comparing aggressive chemotherapy with or without G-
CSF support for high risk myelodysplastic syndromes or
secondary acute myeloid leukemia evolving from MDS.
British Journal of Haematology 1998;102:678–83.
Bradstock 2001 {published data only}∗ Bradstock. Effects of glycosylated recombinant human
granulocyte colony-stimulating factor after high-dose
cytarabine based chemotherapy for adult acute myeloid
leukemia. Leukemia 2001;15:1331–8.
Bradstock KF, Matthews JP, Young GAR, Lowentahl RM.
Effects of lenograstim (glycosylated huG-CSF) after high
dose cytarabine based induction chemotherapy for adult
acute myeloid leukemia (AML) [abstract]. Blood 1999;94
(10 Suppl 1):299a.
Dombret 1995 {published data only}∗ Dombret H, Chastang C, Fenaux P, Reiffers J, Bordessoule
D, Bouabdallah R, et al.A controlled study of recombinant
human G-CSF in elderly patients after treatment for AML.
New England Journal of Medicine 1995;332(25):1678–83.
Dombret H, Yver A, Chastang C, Degos L. Increased
frequency of complete remission by lenograstim
recombinant human granulocyte colony-stimulating
factor (rhG-CSF) administration after intensive induction
chemotherapy in elderly patients with de novo acute
myeloid leukemia (AML): final results of a randomized
multi-centre double-blind controlled study. Blood 1994;84
(10 Suppl 1):231a.
Dombret H, Yver A, Chastang C, Fenaux P, Bordessoule
D, Reiffers J. European multicentre phase III randomized
placebo-controlled study of lenograstim recombinant
glycosylated human granulocyte colony stimulating factor
(rhG-CSF) in elderly patients with de novo acute myeloid
leukemia (AML). British Journal of Haematology 1994;87
(Suppl 1):154.
Estey 1999 {published data only}∗ Estey E, Thall P, Pierce S, Cortes J, Beran M, Kantarjian
H, et al.Randomized phase II study of fludarabine +
cytosine arabinoside + idarubicin +/- all-trans retinoic
acid +/- granulocyte colony-stimulating factor in poor
prognosis newly diagnosed acute myeloid leukemia and
myelodysplastic syndrome. Blood 1999;93(8):2478–84.
Godwin 1998 {published data only}
Godwin JE, Kopecky KJ, Head DR, Hynes HE, Balcerzak
SP, Appelbaum FR. A double-blind placebo controlled trial
of G-CSF in elderly patients with previously untreated acute
myeloid leukemia: a South West Oncology Group study.
Blood 1995;86(10 Suppl 1):434a.∗ Godwin JE, Kopecky KJ, Head DR, Willman CL, Leith
CP, Hynes HE, et al.A double-blind placebo-controlled
trial of granulocyte colony-stimulating factor in elderly
patients with previously untreated acute myeloid leukemia:
a Southwest oncology group study (9031). Blood 1998;91
(10):3607–15.
Harousseau 2000 {published data only}∗ Harousseau. G-CSF after intensive consolidation
chemotherapy in acute myeloid leukemia: results of a
randomized trial of the GOELAM. Journal of Clinical
Oncology 2000;18(4):780–7.
Harousseau JL, Witz F, Desablens B, Leprise PY, Francois
S, Delain M, et al.G-CSF after intensive consolidation
chemotherapy in acute myeloid leukemia. Blood 1997;90
(10 Suppl 1):504a.
Harousseau JL, Witz F, Desablens B, Leprise PY, Francois
S, Delain M, et al.G-CSF after intensive consolidation
chemotherapy in acute myeloid leukemia (AML). Blood
1997;90(10 Suppl 1 (Pt 1)):504–5a.
Heil 1997 {published data only}∗ Heil G, Hoelzer D, Sanz MA, Lechner K, Liu Yin JA, Papa
G, et al.A randomized, double-blind, placebo-controlled,
phase III study of filgrastim in remission induction and
consolidation therapy for adults with de novo acute myeloid
leukemia. The International Acute Myeloid Leukemia
Study Group. Blood 1997;90(12):4710–8.
Heil G, Hoelzer D, Sanz MA, Lechner K, Liu YJ, Papa
G, et al.Results of a randomized, double-blind, placebo-
controlled phase III study of filgrastim in remission
induction and early consolidation therapy for adults with
27Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

de-novo acute myeloid leukemia. Blood 1995;86(10 Suppl
1):267a.
Heil G, Hoelzer D, Sanz MA, Lechner K, Noens L, Szer
J, et al.Long-term survival data from a phase 3 study of
Filgrastim as an adjunct to chemotherapy in adults with de
novo acute myeloid leukemia. Leukemia 2006;20(3):404–9.
Heil G, Hoelzer D, Sanz MA, Lechner K, Yin JA, Noens L,
et al.Long-term survival from a phase 3 study of filgrastim
in remission induction and consolidation therapy for adults
with de novo acute myeloid leukemia. Blood 2002;100(11
Pt 2).
Heil G, Sanz M, Lechner K, Yin J, Noens L, Papa G, et
al.Results of a randomized double-blind placebo controlled
phase III study of filgrastim in remission induction and
early consolidation therapy for adults with de-novo acute
myeloid leukemia. Annals of Hematology 1997;74 Suppl 1:
A4.
Heil G, Sanz MA, Lechner K, Lju YJ, Noens L, Papa G, et
al.Results of a randomized, double-blind placebo controlled
phase III study of filgrastim in remission induction and
early consolidation therapy for adults with de-novo acute
myeloid leukemia. Annals of Hematology 1996;73(Suppl 2):
A90.
Lehrnbecher 2007 {published data only}
Lehrnbecher T, Zimmermann M, Reinhardt D, Dworzak
M, Stary J, Creutzig U. Impact of granulocyte colony-
stimulating factor during induction therapy in children with
acute myelogenous leukemia: results from the prospective
and randomized trial AML-BFM 98. Blood 2004;104(11):
796a.∗ Lehrnbecher T, Zimmermann M, Reinhardt D, Dworzak
M, Stary J, Creutzig U. Prophylactic human granulocyte
colony-stimulating factor after induction therapy in
pediatric acute myeloid leukemia. Blood 2007;109(3):
936–43.
Lowenberg 1997 {published data only}
Lowenberg B. Value of different modalities of granulocyte-
macrophage colony-stimulating factor applied during or
after induction therapy of AML. Journal of Clinical Oncology
1997;15(12):3496–506.
Milligan 2006 {published data only}
Milligan DW, Wheatley K, Craig JI, Littlewood TJ, Burnett
AK. Randomised comparison of FLA versus ADE, with
or without G-CSF and with or without ATRA, for high-
risk AML: results of the MRC AML-HR trial. Hematology
Journal 2004;5(Suppl 2):202.∗ Milligan DW, Wheatley K, Littlewood T, Craig JI,
Burnett AK, NCRI Haematological Oncology Clinical
Studies Group. Fludarabine and cytosine are less effective
than standard ADE chemotherapy in high-risk acute
myeloid leukemia, and addition of G-CSF and ATRA are
not beneficial: results of the MRC AML-HR randomized
trial. Blood 2006;107(12):4614–22.
Nakajima 1995 {published data only}
Nakajima H, Ikeda Y, Hirashima K, Toyama K, Okuma M,
Saito H, et al.A randomized controlled study of r.GCSF in
patients with neutropenia after induction therapy for acute
myelogenous leukemia (G.CSF Clinical Study Group).
Rinsho Ketsueki 1995;36(6):597–605.
Rowe 1995 {published data only}
Rowe JM, Andersen JW, Mazza JJ, Bennett JM, Paietta E,
Hayes FA, et al.A randomized placebo-controlled phase
III study of granulocyte-macrophage colony-stimulating
factor in adult patients (> 55 to 70 years of age) with acute
myelogenous leukemia: a study of the Eastern Cooperative
Oncology Group (E1490). Blood 1995;86(2):457–62.
Stone 1995 {published data only}
Stone R, George S, Berg D, Paciucci P, Schiffer C. GM-CSF
’v’ placebo during remission induction for patients greater
than or equal to 60 years old with de novo acute myeloid
leukemia: CALGB study 8923. Proceedings of the American
Society of Clinical Oncology 1994;130:304.∗ Stone RM, Berg DT, George SL, Dodge RK, Paciucci PA,
Schulman P, et al.GM-CSF after initial chemotherapy for
elderly patients with primary AML. New England Journal of
Medicine 1995;332(25):1671–7.
Usuki 2002 {published data only}
Usuki K, Urabe A, Masaoka T, Ohno R, Mizoguchi H,
Hamajima N, et al.Gran AML Study Group. Efficacy of
granulocyte colony-stimulating factor in the treatment of
acute myelogenous leukaemia: a multicentre randomized
study. British Journal of Haematology 2002;116(1):103–12.
Wheatley 2009 {published data only}
Goldstone AH, Burnett AK, Milligan DW, Prentice AG,
Wheatley K. Lack of benefit of G-CSF on complete
remission and possible increased relapse risk in AML: an
MRC study of 800 patients. Blood 1997;90(10 Suppl 1 (Pt
1)):583a.∗ Wheatley K, Goldstone AH, Littlewood T, Hunter
A, Burnett AK. Randomized placebo-controlled trial of
granulocyte colony stimulating factor (G-CSF) as supportive
care after induction chemotherapy in adults patients with
acute myeloid leukemia: a study of the United Kingdom
Medical Research Council Adult Leukaemia Working Party.
British Journal Haematology 2009;146(1):54–63.
Witz 1998 {published data only}
Witz F, Harousseau JL, Cahn JY, Abgrail JF, Briere J,
Sadoun A. GM-CSF during and after remission induction
treatment for elderly patients with acute myeloid leukemia
(AML). Blood 1994;84:231a.
Witz F, Harousseau JL, Cahn JY, Abgrall JF, Briere J, Sadoun
A, et al.GM-CSF during and after remission induction
treatment for elderly patients with acute myeloid leukemia
(AML). Annals of Hematology 1995;70 Suppl 1:A135.
Witz F, Harousseau JL, Sadoun A, Guyotat D, Berthou C,
Cah JY. GM-CSF during and after remission induction
treatment for elderly patients with acute myeloid leukemia
(AML). British Journal of Haematology 1996;93(Suppl 2):
134.
Witz F, Harousseau JL, Sadoun A, Guyotat D, Berthou
C, Cahn JY, et al.GM-CSF during and after remission
28Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

induction treatment for elderly patients with acute myeloid
leukemia (AML). Blood 1995;86(10 Suppl 1):512a.∗ Witz F, Sadoun A, Perrin MC, Berthou C, Brière J, Cahn
JY. A Placebo controlled study of recombinant human GM-
CSF administered during and after induction treatment for
de novo AML in elderly patients. Blood 1998;8:2722–30.
Zittoun 1996 {published data only}
Zittoun R, Mandelli F, de WT, Willemze R, Thaler J, Hayat
M. Recombinant human granulocyte-macrophage colony-
stimulating factor (GM-CSF) during induction treatment
of acute myelogenous leukemia (AML). A randomized trial
from EORTC-GIMEMA leukemia cooperative groups.
Blood 1994;84:231a.∗ Zittoun R, Suciu S, Mandelli F, de Witte T, Thaler
J, Stryckmans P, et al.Granulocyte-macrophage colony-
stimulating factor associated with induction treatment of
acute myelogenous leukemia: a randomized trial by the
European Organization for Research and Treatment of
Cancer Leukemia Cooperative Group. Journal of Clinical
Oncology 1996;14(7):2150–9.
References to studies excluded from this review
Bernell 1994 {published data only}
Bernell P, Kimby E, Hast R. Recombinant human
granulocyte-macrophage colony-stimulating factor in
combination with standard induction chemotherapy in
acute myeloid leukemia evolving from myelodysplastic
syndromes: a pilot study. Leukemia 1994;8(10):1631.
Bishop 2000 {published data only}
Bishop MR, Tarantolo SR, Geller RB, Lynch JC, Bierman
PJ, Pavletic ZS, et al.A randomized double blind trial of
filgrastim (granulocyte colony stimulating factor) vs placebo
following allogeneic blood stem cell transplantation. Blood
2000;96(1):80.
Braess 2006 {published data only}
Braess J, Fiegl M, Reichle A, Wormann B, Oruzio D, Staib
P, et al.A randomized phase II trial for primary induction
therapy in AML using sequential high dose cytarabine
arabinoside and mitoxantrone and pegylated G-CSF
for shortening therapy induced neutropenia. Annals of
Hematology 2006;85(Suppl 1):28.
Buchner 1993 {published data only}
Buchner T, Hiddemann W, Rottmann R, Zuhlsdorf M,
Wortmann B, Maschmeyer G, et al.Granulocyte colony-
stimulating factor in acute myeloid leukemia. Annals of
Hematology 1994;Suppl 1:9a.∗ Buchner T, Hiddemann W, Wormann B, Maschmeyer G,
Ludwig W, Sauerland MC. Granulocyte colony-stimulating
factor in acute myeloid leukemia. Annals of Hematology
1993;66(6):116a.
Buchner 2004 {published data only}
Buchner T, Berdel WE, Hiddemann W. Priming with
granulocyte colony-stimulating factor - relation to high dose
cytarabine in acute myeloid leukemia. New England Journal
of Medicine 2004;350(21):2215.
Chen 1998 {published data only}
Chen SH, Liang DC, Liu HC. High-dose cytarabine
containing chemotherapy with or without granulocyte
colony-stimulating factor for children with acute leukemia.
American Journal of Hematology 1998;58(1):20.
Creutzig 2006 {published data only}
Creutzig U, Reinhardt D, Lehrnbecher T, Ziimmermann
M. G-CSF during induction, increased dose intensity
during consolidation and intensified therapy for standard
risk patients in the pediatric trial AML-BFM 98. Annals of
Hematology 2006;85(Suppl 1):63.
Creutzig U, Zimmermann M, Lehrnbecher T, Graf N,
Hermann J, Niemeyer CM, et al.Less toxicity by optimizing
chemotherapy, but not by addition of granulocyte colony-
stimulating factor in children and adolescents with acute
myeloid leukemia: results of AML-BFM 98. Journal of
Clinical Oncology 2006;24(27):4499.
Estey 1990 {published data only}
Estey EH, Dixon D, Kantarjian HM, Keating MJ,
McCredie K, Bodey GP, et al.Treatment of poor-prognosis,
newly diagnosed acute myeloid leukemia with ara-c and
recombinant human granulocyte-macrophage colony-
stimulating factor. Blood 1990;75(9):1766.
Frenette 1995 {published data only}
Frenette PS, Desforges JF, Schenkein DP, Rabson A,
Slapack CA, Miller KB. Granulocyte-macrophage colony
stimulating factor (GM-CSF) priming in the treatment of
elderly patient with acute myelogenous leukemia. American
Journal of Hematology 1995;49(1):48.
Freud 1995 {published data only}
Freud DA, Dittus RS. Double-blind, placebo-controlled
trial of daunorubicin and cytarabine with and without
recombinant human granulocyte colony-stimulating factor
in elderly patients with acute myeloid leukemia: economic
evaluation with attention to inpatient and outpatient
resource utilization. Journal of National Cancer Institute
Monograph 1995;19:37.
Godwin 1995 {published data only}
Godwin J. Design and conduct of double-blind, placebo-
controlled trial of daunorubicin and cytarabine with or
without granulocyte colony stimulating factor in elderly
patients with acuta myeloid leukemia: a Southwest
Oncology Group study. Journal National Cancer Institute
Monograph 1995;19:31–5.
Goldstone 2001 {published data only}
Goldstone AH, Burnett AK, Wheatley K, Smith AG,
Hutchinson RM, Clarck RE. Attempts to improve outcomes
in AML in older patients: results of UK MRC AML11.
Blood 2001;98:1302.
Hanel 2001 {published data only}
Hanel M, Friedrichsen K, Hanel A, Herbst R, Morgner A,
Neser S, et al.Mito-flag as salvage therapy for relapsed and
refractory AML. Onkologie 2001;24(4):356.
Hast 2003 {published data only}
Hast R, Hellstrom-Lindberg E, Ohm L, Bjorkholm L,
Celsing F, Dahl IM, et al.No benefit from adding GM-CSF
29Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to induction chemotherapy in transforming myelodysplastic
syndromes: better outcome in patients with less proliferative
disease. Leukemia 2003;17:1827.
Heil 1995 {published data only}
Heil G, Chadid L, Hoelzer D, Seipelt G, Mitrou P, Huber
C, et al.GM-CSF in a double-blind randomized placebo
controlled trial in therapy of adult patients with de-novo
acute myeloid leukemia (AML). Annals of Hematology 1993;
66(6):A117.∗ Heil G, Chadid L, Hoelzer D, Seipelt G, Mitrou P, Huber
C, et al.GM-CSF in a double-blind randomized, placebo
controlled trial in therapy of adult patients with de novo
acute myeloid leukemia. Leukemia 1995;9(1):3.
Heil G, Chadid L, Hoelzer D, Seipelt G, Mitrou P, Huber
C, et al.GM-CSF in the therapy of de-novo AML patients:
an update of a double-blind randomized, placebo controlled
trial. Annals of Hematology 1994;68 Suppl 1:A34.
Heil G, Chadid L, Seipelt G, Mitrou P, Hoelzer D, Kolbe
K, et al.GM-CSF in a double-blind randomized, placebo
controlled trial in therapy of adult patients with de-novo
acute myeloid leukemia (AML). Annals of Hematology 1992;
65(Suppl):A67.
Kalaycio 2001 {published data only}
Kalaycio M, Pohlman B, Elson P, Lichtin A, Hussein
A, Tripp B, et al.Chemotherapy for acute myelogenous
leukemia in the elderly with cytarabine, mitoxantrone,
and granulocyte-macrophage colony stimulating factor.
American Journal of Clinical Oncology 2001;24(1):58.
Kern 1998 {published data only}
Kern W, Aul C, Maschmeyer G, Schonrock-Nabulsi R,
Ludwig WD, Bartholomaus A, et al.Granulocyte colony-
stimulating factor shortens duration of critical neutropenia
and prolongs disease-free survival after sequential high dose
cytosine arabinoside and mitoxantrone (S-HAM ) salvage
therapy for refractory and relapsed acute myeloid leukemia.
Annals of Hematology 1998;77:115.
Lofgren 2004 {published data only}
Lofgren C, Paul C, Astrom M, Hast R, Hedenius M,
Lerner R, et al.Granulocyte-macrophage colony-stimulating
factor to increase efficacy of mitoxantrone, etoposide and
cytarabine in previously untreated elderly patients with acute
myeloid leukaemia: a Swedish multicentre randomized trial.
British Journal of Haematology 2004;124(4):474.
Lowenberg 1997b {published data only}∗ Lowenberg B, Suciu C, Archimbaud E, Ossenkoppele G,
Verhoef GE, Vellenga E, et al.Use of recombinant GMCSF
during and after remission induction chemotherapy in
patients aged 61 years and older with AML: final report
of AML-11, a phase III randomized study of leukemia
cooperative group of EORTC-LCG and HOVON. Blood
1997;90(8):2952.
Lowenberg B, Suciu S, Zittoun R, Ossenkoppele G,
Boogaerts MA, Wijermans P, et al.GM-CSF during as well
as after induction chemotherapy (CT) in elderly patients
with acute myeloid leukemia (AML). The EORTC-
HOVON Phase III trial (AML 11). Blood 1995;86(10
Suppl 1):433a.
Lowenberg 2003 {published data only}
Lowenberg B, Van Putten W, Theobald M, Gmur J,
Verdonck L, Sonneveld P, et al.Effect of priming with
granulocyte colony-stimulating factor on the outcome of
chemotherapy for AML. New England Journal of Medicine
2003;349:743.
Maslak 1996 {published data only}
Maslak PG, Weiss MA, Berman E, Yao TJ, Tyson D, Golde
DW, et al.Granulocyte colony-stimulating factor following
chemotherapy in elderly patients with newly diagnosed
acute myelogenous leukemia. Leukemia 1996;10(1):32.
Montillo 1998 {published data only}
Montillo M, Mirto S, Petti MC, Latagliata R, Magrin S,
Pinto A, et al.Fludarabine, cytarabine, and G-CSF (FLAG)
for the treatment of poor risk acute myeloid leukemia.
American Journal of Hematology 1998;58(2):105.
Moore 1997 {published data only}
Moore JO, Dodge RK, Amrein PC, Kolitz J, Lee EJ,
Powell B, et al.Granulocyte-colony stimulating factor (
filgrastim) accelerates granulocyte recovery after intensive
postremission chemotherapy for acute myeloid leukemia
with aziridinyl benzoquinone and mitoxantrone: Cancer
and Leukemia Group B study 9022. Blood 1997;89(3):780.
Morton 2001 {published data only}
Morton J, Hutchins C, Durrrant S. Granulocyte-colony
stimulating factor (G-CSF)-primed allogeneic bone marrow:
significantly less graft-versus-host disease and comparable
engraftment to G-CSF-mobilized peripheral blood stem
cells. Blood 2001;98:3186.
Ohno 1994 {published data only}
Ohno R, Naoe T, Kanamaru A, Yoshida M, Hiraoka A,
Kobayashi T, et al.A double blind controlled study of G-
CSF started two days before induction therapy in refractory
AML. Blood 1994;83(8):2086.
Ohno 1997 {published data only}
Ohno R, Miyawaki S, Hatake K, Kuriyama K, Saito K,
Kanamaru A, et al.Human urinary macrophage colony-
stimulating factor reduces the incidence and duration of
febrile neutropenia and shortens the period required to
finish three courses of intensive consolidation therapy in
acute myeloid leukemia: a double-blind controlled study.
Journal of Clinical Oncology 1997;15(8):2954.
Ohtake 2006 {published data only}
Ohtake S, Yagasaki F, Miyawaki S, Matsuda M, Taguchi H,
Matsushima T, Toba K, Yoshida M, Naoe T, Ueda R, Ohno
R. A multicenter prospective randomized study of G-CSF
in consolidation chemotherapy for elderly patients with
AML. Haematologica abstract book 2006;91(Suppl 1).
Ojeda 1999 {published data only}
Ojeda E, Garcia-Bustos J, Aguado M, Arrieta R, Quevedo
E, Yuste VJ, et al.A prospective randomized trial of G-CSF
after autologous blood stem cells transplantation. Bone
Marrow Transplant. 1999;24(6):601.
30Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Ossenkopple 2004 {published data only}
Ossenkopple GJ, Graveland WJ, Sonneveld P, Daenen SM,
Biesma DH, Verdonck LF, et al.The value of fludarabine in
addition to ARA-C and G-CSF in the treatment of patients
with high-risk myelodysplastic syndromes and AML in
elderly patients. Blood 2004;103:2908.
Rowe 2004 {published data only}
Rowe JM, Neuberg D, Freidenberg W, Bennet JM, Paietta
E, Makary AZ, et al.A phase III study of 3 induction
regimens and of priming with GM-CSF in older adults with
AML: a trial by ECOG. Blood 2004;103(2):479.
Schmitz 1998 {published data only}
Schmitz N, Bacigalupo A, Hasenclever D, Nagler A,
Gluckman E, Clark P, et al.Allogeneic bone marrow
transplantation vs filgrastim - mobilised peripheral blood
progenitor cell transplantation in patients with early
leukemia: first results of a randomised multicentre
trial of the European Group for Blood and Marrow
Transplantation. Bone Marrow Transplantation 1998;21
(10):995.
Schriber 1994 {published data only}
Schriber JR, Chao NJ, Long GD, Negrin RS, Tierney DK,
Kusnierz-Glaz C, et al.Granulocyte colony-stimulating
factor after allogeneic bone marrow transplantation. Blood
1994;84(5):1680.
Sierra 2005 {published data only}
Sierra J, Bosi A, Szer J, Kassis J, Yang BB, Kido A, et
al.A single dose of pegfilgrastim successfully supports
recovery from prolonged neutropenia following induction
chemotherapy for AML. Haematologica abstract book 2005;
90(Suppl 2):176.
Stone 2001 {published data only}
Stone RM, Berg DT, George SL, Dodge RK, Paciucci PA,
Schulman PP, et al.Postremission therapy in older patients
with de novo acute myeloid leukemia: a randomized trial
comparing mitoxantrona and intermediate dose cytarabine
and standard dose cytarabine. Blood 2001;98(3):548.
Takeshita 1995 {published data only}
Takeshita A, Ohno R, Hirashima K, Toyama K, Okuma M,
Saito H, et al.A randomized double-blind controlled study
of recombinant human granulocyte colony-stimulating
factor in patient with neutropenia induced by consolidation
chemotherapy for acute myeloid leukemia (G-CSF clinical
study group). Rinsho Ketsueki 1995;36(6):606–14.
Takeshita 2000 {published data only}
Takenshita A, Saito H, Toyama K, Horiuchi A, Kuriya
S, Furusawa S, et al.Efficacy of a new formulation of
lenograstim (recombinant glycosylated human granulocyte
colony stimulating factor) containing gelatin for the
treatment of neutropenia after consolidation chemotherapy
in patients with AML. Internal Journal of Hematology 2000;
71(2):136–43.
Takeyama 1995 {published data only}
Takeyama H, Yamada H, Eml N, Saito H, Takeshita
A, Ohno R, et al.Efficacy of early administration of G-
CSF after intensive chemotherapy in acute leukemia: a
randomized controlled trial. Tokai Infection Study Group
on Hematological Disorders. Rinsho Ketsueki 1995;36(11):
1257.
Thomas 1999 {published data only}
Thomas X, Fenaux P, Dombret H, Delair S, Dreyfus F,
Tilly H, et al.Granulocyte-macrophage colony-stimulating
factor (GM-CSF) to increase efficacy of intensive sequential
chemotherapy with etoposide, mitoxantrone and cytarabine
(EMA) in previously treated acute myeloid leukemia: a
multicenter randomized placebo-controlled trial (EMA91
Trial). Leukemia 1999;13(8):1214–20.
Thomas 2007a {published data only}
Thomas X, Raffoux E, Botton S, Pautas C, Arnaud P,
de Revel T, et al.Effect of priming with granulocyte-
macrophage colony-stimulating factor in younger adults
with newly diagnosed acute myeloid leukemia: a trial by
the Acute Leukemia French Association (ALFA) Group.
Leukemia 2007;21(3):453.
Thomas 2007b {published data only}
Thomas X, Suciu S, Rio B, Leone G, Broccia G, Fillet G,
et al.Autologous stem cell transplantation after complete
remission and first consolidation in acute myeloid leukemia
patients aged 61-70 years: results of prospective EORTC
GIMEMA AML-13 trial. Haematologica 2007;92(3):389.
von Lilienfeld Toal 2007 {published data only}
von Lilienfeld Toal, Hahn Ast C, Kirchner H, Flieger
D, Dolken G, Glasmacher A. A randomized comparison
of immediate versus delayed application of G-CSF in
induction therapy for patients with acute myeloid leukemia
unfit for intensive chemotherapy. Haematologica 2007;92
(12):1719.
Additional references
Ascioglu 2002
Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J,
Crokaert F, et al.Defining opportunistic invasive fungal
infections in immunocompromised patients with cancer
and hematopoietic stem cell transplants: an international
consensus. Clinical Infectious Disease 2002;34:7–14.
Bennet 1976
Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton
DA, Gralnick HR, Sultan C. Proposals for the classification
of the acute leukaemias.. British Journal of Haematology
1976;33(4):451–8.
Bennett 2001
Bennett CL, Hynes D, Godwin J, Stinson TJ, Golub RM,
Appelbaum FR. Economic analysis of granulocyte colony
stimulating factor as adjunct therapy for older patients
with acute myelogenous leukemia (AML): estimated
from a Southwest Oncology Group clinical trial. Cancer
Investigation 2001;19(6):603–10.
Bernstein 1998
Bernstein SH, Nademanee AP, Vose JM. A multicenter
study of platelet recovery and utilization in patients
after myeloablative therapy and hematopoietic stem cell
transplantation. Blood 1998;91:3509.
31Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Channa 2002
Channa J, Hashmi KZ. Role of recombinant granulocyte-
macrophage colony-stimulating factors in reducing the
duration of neutropenia. Journal of the College of Physicians
and Surgeons - Pakistan 2002;12:53841.
Cheson 1990
Cheson BD, Cassileth PA, Head DR, Schiffer CA, Bennett
JM, Bloomfield CD, et al.Report of the National Cancer
Institute-sponsored workshop on definitions of diagnosis
and response in acute myeloid leukemia. Journal of Clinical
Oncology 1990;8:813–9.
Clark 2000
Clark OA, Lyman G, Castro AA, Clark LG, Djulbegovic
B. Colony stimulating factors for chemotherapy induced
febrile neutropenia. Cochrane Database of Systematic Reviews
2000, Issue 4. [DOI: 10.1002/14651858.CD003039]
De Vita 2001
Griffin JD. Hematopoietic growth factors. In: DeVita VT
Jr, Hellman S, Rosenberg SA editor(s). Cancer: Principles
and Practice of Oncology. 6th Edition. Lippincott Williams
& Wilkins, 2001.
Dekker 2006
Dekker A, Bulley S, Beyene J, Dupuis LL, Doyle JJ,
Sung L. Meta-analysis of randomized controlled trials of
prophylactic granulocyte colony-stimulating factor and
granulocyte-macrophage colony-stimulating factor after
autologous and allogeneic stem cell transplantation. Journal
of Clinical Oncology 2006;24(33):5207–15.
DerSimonian 1986
DerSimonian R, Laird N. Meta-analysis in clinical trials.
Controlled Clinical Trials 1986;7:177–88.
Goker 2001
Goker H, Haznedaroglu IC, Chao NJ. Acute graft vs host
disease: pathobiology and management. Experimental
Hematology 2001;29(3):259–77.
Griffin 1986
Griffin JD, Lowenberg B. Clonogenic cells in acute
myeloblastic leukemia. Blood 1986;68:1185.
Heuser 2010
Heuser M, Zapf A, Morgan M, Krauter J, Ganser A.
Myeloid growth factors in acute myeloid leukemia:
systematic review of randomized controlled trials. Annals of
Hematology 2011;90(3):273–81.
Higgins 2002
Higgins JPT, Thompson SG. Quantifying heterogeneity in
a meta-analysis. Statistics in Medicine 2002;21:1539–58.
Higgins 2003
Higgins JPT, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. BMJ 2003;327:
557–60.
Higgins 2009
Higgins JPT, Green S, editors. Cochrane Handbook
for Systematic Reviews of Interventions 5.0.2 [updated
September 2009]. The Cochrane Collaboration, 2009.
Available from www.cochrane-handbook.org.
Hoffman 2008
Miller KB, Pihan G. Clinical manifestations of acute
myeloid leukemia. In: Hoffman R, Furie B, Benz Jr. EJ,
McGlave P, Silberstein LE, Shattil SJ editor(s). Hematology:
Basic Principles and Practice. 5th Edition. Churchill
Livingstone, 2008.
Inoue 1990
Inoue C, Murate T, Hotta T, Satio H. Response of leukemic
cells to the sequential combination of GM-CSF and G-CSF.
International Journal of Cell Cloning 1990;8(1):54–62.
Lee 2003
Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-
host disease. Biology of Blood and Marrow Transplantation
2003;9(4):215–33.
Lemoli 1991
Lemoli RM, Gulati SC, Strife A, Lambek C, Perez A,
Clarkson BD. Proliferative response of human acute myeloid
leukemia cells and normal marrow enriched progenitor cells
to human recombinant growth factors IL-3, GM-CSF and
G-CSF alone and in combination. Leukemia 1991;5(5):
386–91.
Lowenberg 1988
Lowenberg B, Salem M, Delwel R. Effect of recombinant
multi-CSF, GM-CSF,G-CSF and M-CSF on the
proliferation and maturation of human AML in vitro. Blood
Cells 1988;14(2-3):539–49.
Nichols 2003
Nichols WG. Management of infectious complications in
the hematopoietic stem cell transplant recipient. Journal of
Intensive Care Medicine 2003;18:295.
Ohno 1990
Ohno R, Tomonaga M, Kobayashi T, Kanamaru A,
Shirakawa S, Masaoka T, et al.Effect of granulocyte colony
stimulating factor after intensive induction therapy in
relapsed or refractory acute leukemia. New England Journal
of Medicine 1990;323(13):871–7.
Ohno 1993
Ohno R, Hiraoka A, Tanimoto M, Asou N, Kuriyama K,
Kobayashi T, et al.No increase of leukemia who received
granulocyte colony stimulating factor for life threatening
infection during remission induction and consolidation
therapy. Blood 1993:197.
Ottmann 2007
Ottmann OG, Bug G, Krauter J. Current status of growth
factors in the treatment of acute myeloid and lymphoblastic
leukemia. Seminars in Hematology 2007;44:183–92.
Park 1989
Park LS, Waldron PE, Friend D, Sassenfeld HM, Price V,
Anderson D, et al.Interleukin-3, GM-CSF, and G-CSF
receptor expression on cell lines and primary leukemia cells:
receptor heterogeneity and relationship to growth factor
responsiveness. Blood 1989;74(1):56–65.
Parmar 1998
Parmar MK, Torri V, Stewart L. Extracting summary
statistics to perform meta-analyses of the published
32Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

literature for survival endpoints. Statistics in Medicine 1998;
17:2815–34.
RevMan 2011
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 5.1. Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2011.
Smith 2006
Smith TJ, Khatcheressian J, Lyman GH, Ozer H, Armitage
JO, Balducci L, et al.2006 update of recommendations for
the use of white blood cell growth factors: an evidence-
based clinical practice guideline. Journal of Clinical Oncology
2006;24(19):3187–205.
Souza 1986
Souza LM, Boone TC, Gabrilove JL, Lai PH, Zsebo KM,
Murdock DC, et al.Recombinant human granulocyte
colony-stimulating factor: effects on normal and leukemic
myeloid cells.. Science 1986;232(4746):61–5.
Sung 2004
Sung L, Nathan PC, Lange B, Beyene J, Buchanan GR.
Prophylactic granulocyte colony-stimulating factor and
granulocyte-macrophage colony-stimulating factor decrease
febrile neutropenia after chemotherapy in children with
cancer: a meta-analysis of randomized controlled trials.
Journal of Clinical Oncology 2004;22(16):3350–6.
Vardiman 2009
Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz
MJ, Porwit A, et al.The 2008 revision of the World Health
Organization (WHO) classification of myeloid neoplasms
and acute leukemia: rationale and important changes. Blood
2009;114(5):937–51.
Vellenga 1987
Vellenga E, Young DC, Wagner K, Wiper D, Ostapovicz
D, Griffin JD. The effect of GM-CSF and G-CSF in
promoting growth of clonogenic cells in acute myeloblastic
leukemia. Blood 1987;69:1771.
Wang 2009a
Wang J, An L, Chen S, Ouyang J, Zhou R, Chen B, et
al.Prophylactic use of granulocyte colony-stimulating factor
after chemotherapy does not affect survival rate in acute
myeloid leukemia: a meta-analysis. Acta Haematologica
2009;121(4):223–6.
Wang 2009b
Wang J, Zhan P, Ouyang J, Chen B, Zhou R. Prophylactic
use of granulocyte colony-stimulating factor after induction
chemotherapy in patients with newly diagnosed acute
myeloid leukemia may increase the complete remission
rate: a meta-analysis of five randomised controlled trials.
Leukemia Lymphoma 2009;50(3):457–9.∗ Indicates the major publication for the study
33Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Amadori 2005
Methods Randomized, open-label, controlled trial
Median follow up: 4.7 years
Participants 722 patients
Median age: 54 years
Male: 53%
Newly diagnosed AML patients receiving induction chemotherapy
Europe, multi-center
Interventions Induction chemotherapy: MICE (IV mitoxantrone 7 mg/m2 on days 1, 3, 5; IV cytara-
bine 100 mg/m2 on days 1 to 7; IV etoposide 100 mg/m2 on days 1 to 3)
IV G-CSF 150 µg/m2/d starting with or after chemotherapy (depending on trial’s arm)
and discontinued if blast cells increased > 2-fold during chemotherapy course or blast
cells persisted at significant levels (> 1 x 109 /L) for 3 days after chemotherapy completion,
or if blasts at significant level (> 1 x 109/L) reappeared after chemotherapy completion,
or until WBC > 10 x 109/L, or when serious toxicity attributed to G-CSF occurred
The trial included 4 arms: G-CSF during and after chemotherapy (A) versus G-CSF
after chemotherapy (B) versus G-CSF during chemotherapy (C-arm excluded) versus
control (D)
Outcomes All-cause mortality at 30 days and at the end of follow up
Number of patients achieving complete remission (CR)
Number of patients with relapse
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “randomization was performed
centrally”
Blinding (performance bias and detection
bias)
All outcomes
High risk Quote: “open-label”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “A total of 35 patients were consid-
ered ineligible: 5 in group A, 10 in group
B, 10 in group C, and 10 in group D. Rea-
sons for ineligibility included insufficient
34Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Amadori 2005 (Continued)
data in 13, concomitant malignant diseases
in 11, prior chemotherapy in 4, inadequate
performance status in 3, leukemia super-
vening after a myeloproliferative disorder
in 2, and other causes in 2. Ineligible pa-
tients were also included in the intention-
to-treat analysis.”
Selective reporting (reporting bias) Low risk All the outcomes which were described in
the Methods section were reported in the
Results section
Other bias Low risk The day of randomization is the first day
of chemotherapy
Beksac 2010
Methods Randomized, controlled, open trial
Median follow up: 3 years
Participants 260 patients
Median age: 38.5 years, range 16 to 60 years
Male: 56.9%
Newly diagnosed AML patients who had received induction chemotherapy
Turkey, multicenter
Interventions Induction chemotherapy: IV cytarabine 100 mg/m2/d for 10 days + IV idarubicin 12
mg/m2/d for 3 days
IV G-CSF 5 µg/d starting on day 8 until neutrophil count > 0.5 x 109/L for 2 days
The trial included 2 arms: G-CSF after chemotherapy versus control
Outcomes All-cause mortality at the end of follow up
Number of patients achieving complete remission (CR)
Number of patients with relapse
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Adequate, shuffling
Allocation concealment (selection bias) Low risk Adequate, sealed and opaque envelopes
35Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Beksac 2010 (Continued)
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not reported
Selective reporting (reporting bias) High risk Although one of the outcomes in the Meth-
ods section was disease-free survival, it was
not described in the Results section
Other bias High risk Randomization was done on day 8 after
chemotherapy and only if marrow blasts
were less than 20%, so some of the patients
were excluded (died or medically declined)
Bernasconi 1998
Methods Randomized controlled trial
Maximal range follow up: 25 months
Participants 105 patients
Median age: 58 years in the G-CSF arm and 57 years in the control arm
Male: 28% in the G-CSF arm and 29% in the control arm
De novo myelodysplastic syndrome (RAEB, RAEB-T) and AML patients who had re-
ceived induction chemotherapy
Italy, multicenter
Interventions Induction chemotherapy: idarubicin 12 mg/m2 on days 1, 2 + etoposide 60 mg/m2/
12hr for 5 days + cytarabine 120 mg/m2/12 hr for 5 days
SC G-CSF 5 µg/kg/d starting 48 hrs after the end of chemotherapy until neutrophil
count > 10 x 109/L or until day 21
The trial included 2 arms: G-CSF versus control
Outcomes All-cause mortality at 30 days
Number of patients achieving complete remission (CR)
Number of patients with relapse
Number of bacteremias
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
36Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bernasconi 1998 (Continued)
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk No withdrawals and protocol violations af-
ter randomization reported. Not reported
if the analysis was performed on an ITT
basis
Selective reporting (reporting bias) Unclear risk Not all the outcomes described in the
Methods section were reported in the Re-
sults section
Other bias Unclear risk Day of randomization was not reported
Bradstock 2001
Methods Randomized controlled trial
Median follow up: 3.6 years
Participants 114 patients
Median age: 43 years (range 15 to 60)
Male: 67% in the control arm, 48% in the G-CSF arm
Newly diagnosed AML patients who had received induction chemotherapy
Australia, multicenter
Interventions Induction chemotherapy: ICE (cytarabine 3 gr/m2 every 12 hrs on days 1, 3, 5, 7 +
etoposide 75 mg/m2 on days 1 to 7 + idarubicin 12 mg/m2 on days 1 to 3 , later dose
was reduced to 9 mg/m2 d/t toxicity)
SC G-CSF 5 µg/kg/d starting on day 8 after chemotherapy until recovery of neutrophils
> 2 x 109/L for 3d or > 5 x 109/L for 1 day or evidence of residual leukemia in day 28
bone marrow biopsy
The trial included 2 arms: G-CSF versus control
Outcomes All-cause mortality at 1 year and at the end of follow up
Overall survival
Infection-related mortality
Number of patients achieving complete remission (CR)
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
37Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bradstock 2001 (Continued)
Random sequence generation (selection
bias)
Low risk Quote: “The method of randomisation was
based on a biased coin design.”
Allocation concealment (selection bias) Low risk Quote: “Patients were randomised by tele-
phoning the ALSG trial centre.”
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “A total of 114 eligible patients had
been enrolled at that time; 54 had been ran-
domised to receive lenograstim and 60 to
no cytokine. Two patients, both on the no
cytokine arm, were inevaluable with respect
to the primary endpoint: one was with-
drawn from the trial before commencing
induction therapy due to pneumonia and
one died from non-protocol-related causes
2 days after commencing induction. These
patients are included in the response and
survival comparisons. The remaining 112
randomised patients provided the basis of
the toxicity comparisons.”
Selective reporting (reporting bias) Low risk All the outcomes which were described in
the Methods section, were reported in the
Results section
Other bias Low risk The randomization was performed before
initiation of chemotherapy
Dombret 1995
Methods Randomized controlled trial
Follow up: 3.5 years
Participants 173 patients
Median age: 70 years (range: 64 to 83)
Male: 54% in the G-CSF arm and 56% in the control arm
Newly diagnosed AML patients who had received induction chemotherapy
Europe, multicenter
Interventions Induction chemotherapy: IV daunorubicin 45 mg/m2 for 4 days + IV continuous cy-
tarabine 200 mg/m2 for 7 days
SC G-CSF 5 µg/kg/d starting on day 9 after chemotherapy until neutrophil recovery >
1 x 109/L for 3 days or maximum 28 days
The trial included 2 arms: G-CSF versus control
38Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dombret 1995 (Continued)
Outcomes All-cause mortality at 30 days, 1 year and at the end of follow up
Overall survival
Number of patients achieving complete remission (CR)
Number of bacteremias
Number of invasive fungal infections
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “one patient was lost to follow-up
in each treatment group.”
Selective reporting (reporting bias) Low risk All the outcomes which were described in
the Methods section, were reported in the
Results section
Other bias High risk Randomization was done on day 8 of the
induction chemotherapy. Therefore, pa-
tients who were unsuitable for chemother-
apy or declined during chemotherapy were
not randomized
Estey 1999
Methods Randomized controlled trial
Median follow up: 35 weeks
Participants 216 patients
Median age: 65
With AML or RAEB/RAEB-T who received induction chemotherapy
USA
Interventions Induction chemotherapy: FAI (fludarabine 30 mg/m2/d on days 1 to 4 + cytarabine 2
gr/m2/d on days 1 to 4 + idarubicin 12 mg/m2/d on days 2 to 4); ATRA 45 mg/m2/d
in divided doses
G-CSF 200 µg/m2/d: in patients with WBC count<10 x 109/L start on day 1; in patients
39Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Estey 1999 (Continued)
with WBC count 10 x 109-50 x 109/L start on day 1 (simultaneously with chemotherapy)
; in patients with WBC count > 50 x 109/L start on day 2 until neutrophil recovery > 1
x 109/L
The trial included 4 arms: G-CSF versus ATRA and G-CSF versus ATRA versus control
Outcomes All-cause mortality at 30 days, 1 year and at the end of follow up
Overall survival
Number of patients achieving complete remission (CR)
Number of bacteremias
Number of invasive fungal infections
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Quote: “All but four of the 215 were eligi-
ble, and we include all 215 in this report.”
Selective reporting (reporting bias) Unclear risk All the outcomes which were described in
the Methods section were reported in the
Results section
Other bias Unclear risk Day of randomization was not reported
Godwin 1998
Methods Double-blind, placebo-controlled study
Median follow up: 33 months
Participants 234 patients
Median age: 68 years (range: 56 to 88)
Male: 58%
Patients with AML FAB M0 to M7 who had received induction chemotherapy
USA, multicenter
Interventions Induction chemotherapy: IV cytarabine 200 mg/m2/d 1-7d + IV daunorubicin 45 mg/
m2/d 1-3d and 2 consolidations - IV daunorubicin 30 mg/m2 1-2d + cytarabine 200
40Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Godwin 1998 (Continued)
mg/m2/d 1-7d
IV G-CSF 400 µg/m2/d starting on day 11 of induction or on day 8 of consolidation
until neutrophil recovery > 1 x 109/L
The trial included 2 arms: G-CSF versus placebo
Outcomes All-cause mortality at 1 year and at the end of follow up
Overall survival
Infection-related mortality
Number of patients achieving complete remission (CR)
Disease-free survival
Notes Funding: academic
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double-blinding (not specified who was
blinded)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “The analyses are based on intent to
treat and include the 211 patients with cen-
trally confirmed diagnoses of AML. Nine
of these 211 cases failed to meet other eli-
gibility criteria.”
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias High risk The randomization was performed on day
11 of induction.
Harousseau 2000
Methods Randomized, open, controlled trial
Median follow up: 26 months
Participants 194 patients
Median age: 47.5 years in the G-CSF arm and 45 years in the control arm
Male: 49% in the G-CSF arm and 50% in the control arm
Patients with de novo AML who received consolidation chemotherapy
France, multicenter
41Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Harousseau 2000 (Continued)
Interventions Consolidation chemotherapy: ICC1 (cytarabine 3 g/m2 every 12 hrs for days 1 to 4 +
mitoxantrone 12 mg/m2 on days 5 to 6) + ICC2 (amsacrine 150 mg/m2 for 5 days +
etoposide 100 mg/m2 for 5 days)
SC G-CSF 5 µg/kg/d starting on day 8 of consolidation until recovery of neutrophil
count > 1 x 109/L or > 0.5 x 109/L for 3 days
The trial included 2 arms: G-CSF versus placebo
Outcomes All-cause mortality at 30 days
Overall survival
Relapse rate
Number of bacteremias
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “Central randomization”
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Of the 194 patients, 29 (15%) could not
proceed to ICC2 (16 in the G-CSF arm
and 13 in the control arm)
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias Low risk Randomization was done before the initia-
tion of chemotherapy
Heil 1997
Methods Randomized, double-blind, controlled trial
Median follow up: 24 months
Participants 521 patients
Median age: 54 years (range: 16 to 89)
Male: 54%
Patients with AML who had received induction chemotherapy
Europe, multicenter
42Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Heil 1997 (Continued)
Interventions Induction chemotherapy: IV daunorubicin 45 mg/m2 for 3 days + IV continuous cy-
tarabine 200 mg/m2 for 7 days + IV etoposide 100 mg/m2 for 5 days
SC G-CSF 5 µg/kg/d starting 24 hours after the last dose of chemotherapy until recovery
of neutrophil count > 1 x 109/L or > 0.5 x 109/L for 3 days
The trial included 2 arms: G-CSF versus placebo
Outcomes All-cause mortality at 30 days and at the end of follow up
Overall survival
Infection-related mortality
Number of patients achieving complete remission (CR)
Disease-free survival
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “Patients were centrally random-
ized after 6 days of chemotherapy”
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double-blinding: blinded study drug
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “All analyses, with the exception of
disease-free survival and analysis of courses
subsequent to induction course 1, were per-
formed in an intent-to-treat manner, i.e.
, including all randomized patients in the
treatment groups assigned at randomiza-
tion. The analysis of disease-free survival
only included patients who achieved a CR.
”
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias High risk Randomization was done on the sixth day
of chemotherapy
43Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lehrnbecher 2007
Methods Randomized controlled trial
Median follow up: 4.1 years
Participants 429 patients
Age: < 16 years
Male: 59.6% in the G-CSF arm and 46.2% in the control arm
Patients with AML who had received induction chemotherapy
Europe, multicenter
Interventions Induction chemotherapy: AIE 1st induction (cytarabine at dose of 100 mg/m2/d con-
tinuous on days 1 to 2 and infusion every 12 hours on 3-8d; idarubicin 12 mg/m2 on 3-
5d; etoposide 150 mg/m2 on 6-8d; IT cytarabine on days 0, 8) + HAM 2nd induction
IV/SC G-CSF 5 µg/kg/d starting on day 15 after the start of chemotherapy until the
neutrophil count was > 0.5 x 109/L for 3 consecutive days
The trial included 2 arms: G-CSF versus placebo
Outcomes All-cause mortality at 30 days and at the end of follow up
Overall survival
Infection-related mortality
Number of patients achieving complete remission (CR)
Disease-free survival
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “Randomization was centrally per-
formed using the permuted block method.
”
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “All efficacy analyses were per-
formed according to the intent-to-treat
principle.”
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias High risk Quote: “randomization regarding G-CSF
performed on day 15.”
44Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lowenberg 1997
Methods Randomized controlled trial
Median follow up: 5 years
Participants 274 patients
Mean age: 42 years (+/- 12)
Male: 56%
Patients with previously untreated newly diagnosed AML according to FAB who had
received induction chemotherapy
Europe, multicenter
Interventions Induction chemotherapy: first course: IV daunorubicin 45 mg/m2 on days 1, 2, 3 &
cytarabine 200 mg/m2 on days 1 to 7. 2nd course: IV amsacrine 120 mg/m2 on days 4,
5, 6 and cytarabine 1 gr/m2 every 12 hr on days 1 to 6
IV/SC GM-CSF 5 µg/kg/d starting at the end of chemotherapy (course 1- day 8, course
2 - day 7) until the neutrophil count was > 0.5 x 109/L for 3 consecutive days or until
28 days
The trial included 4 arms: GM-CSF during and after chemotherapy (arm excluded) ver-
sus GM-CSF after chemotherapy versus GM-CSF during chemotherapy (arm excluded)
versus control
Outcomes All-cause mortality at the end of follow up
Number of patients achieving complete remission (CR)
Relapse rate
Number of bacteremias
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Central randomization
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Not reported
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “A total of 274 patients were ran-
domized. Twenty-one patients were not as-
sessable and excluded from the analysis for
the following reasons: treatment had been
started before randomization (n = 3), no
diagnosis of AML (n = 6), age greater than
60 years (n = 1), no treatment (n = 3), no
data available (n = 1), and the possibility of
placebo treatment instead of GM-CSF (n
45Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lowenberg 1997 (Continued)
= 6).”
Selective reporting (reporting bias) Unclear risk All the outcomes described in the Methods
section were reported in the Results section
Other bias Unclear risk Day of randomization was not reported
Milligan 2006
Methods Randomized controlled trial
Median follow up: 4 years
Participants 356 patients
Age: 15 years and older (no median/mean reported)
Male - 96% in the G-CSF arm and 87% in the control arm
Patients with relapsed/refractory AML or AML with adverse cytogenetics in CR after
chemotherapy who had received re-induction chemotherapy
Britain, Ireland and New Zealand
Interventions Reinduction chemotherapy: ADE (ara-c, daunorubicin, etoposide)/FLA (fludarabine,
ara-c)
IV/SC G-CSF 5 µg/kg/d starting on day 1 of chemotherapy until the neutrophil count
was > 0.5 x 109/L for 2 consecutive days or until 28 days
The trial included 2 arms: G-CSF versus control
Outcomes All-cause mortality at 30 days, 1 year and at the end of follow up
Overall survival
Number of patients achieving complete remission (CR)
Disease-free survival
Relapse rate
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Quote: “allocation was computer gener-
ated”
Allocation concealment (selection bias) Low risk Quote: “randomization was performed by
telephone call to the central trial office”
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
46Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Milligan 2006 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Quote: “all analyses are performed on the
“intention to treat” principle with all pa-
tients analyzed in their allocated arms, ir-
respective of whether they actually received
their allocated treatment ”
Selective reporting (reporting bias) Unclear risk All the outcomes described in the Methods
section were reported in the Results section
Other bias Unclear risk Day of randomization was not reported
Nakajima 1995
Methods Randomized controlled trial
Participants 95 patients
Age: < 16 years
Patients with AML who had received induction chemotherapy
Japan, multicenter
Interventions Induction chemotherapy - unknown
IV G-CSF 5 µg/kg/d
The trial included 2 arms: G-CSF versus placebo
Outcomes All-cause mortality at 30 days
Infection-related mortality
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not reported
Selective reporting (reporting bias) Unclear risk Not reported
47Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rowe 1995
Methods Double-blind, randomized study
Median follow up: 13.1 months
Participants 124 patients
Median age: 64 years
Male: not reported
Patients with AML who had received induction chemotherapy
USA, multicenter
Interventions Induction chemotherapy: induction - daunorubicin 60 mg/m2/d on days 1 to 3 and
cytarabine 25 mg/m2 IV push on day 1 followed by 100 mg/m2 /d by continuous infusion
on days 1 to 7; consolidation - for patients that entered CR, 1 course of cytarabine 1.5
g/m2 every 12 hr over 1 hr for 12 doses
IV GM-CSF 250 µg/m2/d starting on day 11 after the start of chemotherapy until the
neutrophil count was > 1.5 x 109or until a maximum of 42 days
The trial included 2 arms: GM-CSF versus placebo
Outcomes All-cause mortality at 1 year
Overall survival
Number of patients achieving complete remission (CR)
Notes Funding: academic
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double-blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quotes: “Of these patients, 117 were eligi-
ble and evaluable: 60 on the GM-CSF arm
and 57 on the placebo arm. Reasons for
exclusion were prior chemotherapy (1 pa-
tient), no follow-up (2 patients), and wrong
pathology (4 patients).”
“All eligible and evaluable patients to be
included in an intent-to-treat analysis.”
Selective reporting (reporting bias) Unclear risk All the outcomes described in the Methods
section were reported in the Results section
48Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rowe 1995 (Continued)
Other bias Unclear risk The day of randomization was not reported
Stone 1995
Methods Randomized, double-blind trial
Median follow up: not mentioned
Participants 388 patients
Median age: 69 years
Male: 56%
Patients with primary AML as defined by FAB who had received induction chemotherapy
USA, multicenter
Interventions Induction chemotherapy: IV daunorubicin 45 mg/m2 for 3 days + IV continuous cy-
tarabine 200 mg/m2 for 7 days
IV GM-CSF 5 µg/kg/d starting one day after the cytarabine infusion was completed
until life-threatening toxicity due to study drug or neutrophil recovery > 1 x 109/L or
peripheral myeloblast count > 1 x 109/L
The trial included 2 arms: GM-CSF versus placebo
Outcomes All-cause mortality at the end of follow up
Overall survival
Number of patients achieving complete remission (CR),
Number of bacteremias
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Quote: “The computer program control-
ling the randomization was a general pro-
gram used for randomized studies of the
CALGB.”
Allocation concealment (selection bias) Low risk Quote: “randomly assigned to one of the
two treatment groups by means of a tele-
phone call to the CALGB Statistical Cen-
ter.”
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double-blinding. Not reported who was
blinded.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quotes: “Since all enrolled patients were
randomized, no patients were excluded
from the primary analyses.”
49Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Stone 1995 (Continued)
“The primary analyses in this study fol-
lowed the intention-to-treat principle”
Selective reporting (reporting bias) Unclear risk Disease-free survival was one of the out-
comes in the Methods section, but it was
not described in the Results section
Other bias Low risk The first day of chemotherapy was the day
of randomization
Usuki 2002
Methods Randomized controlled trial
Median follow up: 20 months
Participants 270 patients
Mean age: 49.5 +/- 16.5, range: 15 to 87 years
Male: 65%
Patients with newly diagnosed de novo AML as defined by FAB who had received
induction chemotherapy
Japan, multicenter
Interventions Various induction regimens: BHAC-DM; BHAC-DMP; BHAC-EDM, depending on
each hospital
IV G-CSF 200 mg/m2/d starting 48 hours after the completion of chemotherapy until
neutrophil count > 1.5 x 109/L
The trial included 2 arms: G-CSF versus control
Outcomes All-cause mortality at 30 days and at the end of follow up
Infection-related mortality
Overall survival
Number of patients achieving complete remission (CR)
Disease free survival
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Central
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
50Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Usuki 2002 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “All analyses were performed in
an intent-to-treat manner, i.e. including all
patients assigned to each group at the time
of randomization.”
Quote: “A total of 270 patients were ran-
domized from October 1993 to Septem-
ber 1996. Sixteen patients had their di-
agnosis amended to another disease (15
had myelodysplastic syndrome and one
had acute lymphoblastic leukaemia), two
patients had severe heart or liver failure,
five patients concomitantly received G-
CSF during induction chemotherapy, and
two patients were treated with all-trans
retinoic acid. These 25 patients were with-
drawn from the study and the remaining
245 patients were included in the analyses.
”
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the results section
Other bias High risk The randomization day was the first day
after completion of chemotherapy
Wheatley 2009
Methods Randomized, placebo-controlled trial
Median follow up: 5 years
Participants 803 patients
Median age of patients: 49 years (range: 15 to 77)
Male: 53%
Patients with de novo AML or secondary AML defined by FAB received induction
chemotherapy
Britain, multicenter
Interventions Induction chemotherapy: AML12 (ADE 10 + 3 + 5 or MAE 3 + 10 + 5) or AML11
(ADE, DAT or MAC)
IV G-CSF 263 µg/d starting on day 8 from the end of chemotherapy (18 days after
the start of ADE, MAE or DAT and 13 days after the start of MAC) until recovery of
neutrophil count > 0.5 x 109/L for 2 days or for 10 days maximum
The trial included 2 arms: G-CSF versus control
Outcomes All-cause mortality at 30 days, at 1 year and at the end of follow up
Overall survival
Number of patients achieving complete remission (CR)
Disease-free survival
51Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Wheatley 2009 (Continued)
Relapse rate
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “Randomizations were performed
by telephone call to a central randomiza-
tion office”
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Not reported
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Quotes: “The principal analyses were ‘in-
tention-to-treat’ on all randomized pa-
tients, with a subsidiary analysis of the ma-
jor clinical endpoints performed excluding
patients who did not commence G-CSF or
placebo.”
“599 (75%) were known to have com-
menced either the G-CSF or placebo”
Reasons not to receive G-CSF or placebo
include: patients either died before, or were
too ill, or refused, or were not given by mis-
take and other
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias Unclear risk The day of randomization is unclear
Witz 1998
Methods Randomized controlled trial
Median follow up: 3 years
Participants 244 patients
Median age: 65 years
Male: 56.5%
Patients with previously untreated de novo AML as defined by FAB who received induc-
tion chemotherapy
France, multicenter
52Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Witz 1998 (Continued)
Interventions Induction chemotherapy: IV idarubicin 8 mg/m2/d for 5 days + cytarabine 100 mg/m2/d for 7 days
IV GM-CSF 5 µg/kg/d starting on day 1 (12 hr after chemotherapy was started) until
recovery of neutrophil count > 0.5 x 109/L for 3 days or for 28 days maximum
The trial included 2 arms: GM-CSF versus control
Outcomes All-cause mortality at 30 days and at the end of follow up
Overall survival
Number of patients achieving complete remission (CR)
Disease-free survival
Relapse rate
Number of bacteremias
Number of invasive fungal infections
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Unclear risk Not reported
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quotes: “All eligible patients who received
the randomly assigned treatment were in-
cluded in the analysis for comparison be-
tween the two treatment groups whether
the planned program was completed or the
study drug prematurely discontinued.”
“Among 240 eligible patients included in
the study, eight (four in each treatment
group) were judged nonassessable for in-
duction treatment: one because of death
before the first administration of the study
medication and seven because of major
protocol violation (one never received the
medication because of a supply problem,
three did not receive the assigned medica-
tion, one received the medication only dur-
ing induction treatment, one received the
medication only after induction treatment,
and one received chemotherapy with high-
53Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Witz 1998 (Continued)
dose Ara-C).”
Selective reporting (reporting bias) Low risk All the outcomes described in the Methods
section were reported in the Results section
Other bias Unclear risk The day of randomization was not reported
Zittoun 1996
Methods Randomized controlled trial
Median follow up: 34 months
Participants 102 patients
Median age: 42 years (range: 17 to 59) in the G-CSF arm and 45 years (range: 26 to 59)
in the control arm
Patients with previously untreated AML who received induction chemotherapy
Europe, multicenter
Interventions Induction chemotherapy: IV daunorubicin 45 mg/m2/d in days 1 to 3 + IV cytarabine
200 mg/m2/d in days 1 to 7
IV GM-CSF 5 µg/kg/d starting on day 8 until recovery of neutrophil count or till 28
days
The trial included 4 arms: GM-CSF during and after chemotherapy (arm excluded) ver-
sus GM-CSF after chemotherapy versus GM-CSF during chemotherapy (arm excluded)
versus control
Outcomes All-cause mortality at 30 days and at the end of follow up
Number of patients achieving complete remission (CR)
Relapse rate
Notes Funding: industry
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not reported
Allocation concealment (selection bias) Low risk Quote: “Randomization was centrally per-
formed at the EORTC Data Center in
Brussels using the minimization tech-
nique”
Blinding (performance bias and detection
bias)
All outcomes
High risk No blinding
54Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Zittoun 1996 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Quote: “In all analyses, the intention-to-
treat principle was used, i.e., all patients
were kept in the treatment arm allocated by
randomization.”
Selective reporting (reporting bias) Low risk All the outcomes which were described in
the methods section were reported in the
results section
Other bias Unclear risk Day of randomization was not reported
AML: acute myelogenous leukemia; CR: complete remission; d: day; EORTC: European Organization; for Research and Treatment
of Cancer; G-CSF: granulocyte colony-stimulating factor; GM-CSF: granulocyte macrophage colony-stimulating factor; hr: hour;
ITT: intention-to-treat; IV: intravenous; WBC: white blood cell
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Bernell 1994 G-CSF was started 48 hours prior to chemotherapy
Not a RCT
Bishop 2000 Most patients were not AML (only 6 out of 55 had AML)
Braess 2006 There was no randomization to G-CSF or control/placebo
Buchner 1993 GM-CSF was started 48 hours prior to chemotherapy
Buchner 2004 Not a RCT
Chen 1998 Not a RCT
Creutzig 2006 Double publication with Lehrnbecher 2007
Estey 1990 Historical control
Not a RCT
Frenette 1995 GM-CSF was started prior to chemotherapy
Freud 1995 Cost-effectiveness study of a RCT in elderly patients with AML with or without G-CSF
Godwin 1995 Not a RCT
55Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Goldstone 2001 Double publication with Wheatley 2009. Goldstone’s paper presents the results of AML11 trial, while
Wheatley’s presents the results of AML11 AND ANL12
Hanel 2001 There was no randomization to G-CSF or control/placebo
Hast 2003 GM-CSF was started 48 hours prior to chemotherapy in patients with WBC < 50000
Heil 1995 GM-CSF was started 48 hours prior to chemotherapy
Kalaycio 2001 Not a RCT
Kern 1998 Historical control
Not a RCT
Lofgren 2004 Aim of the study was priming (1 day before chemotherapy)
Lowenberg 1997b GM-CSF started 1 day before chemotherapy
Lowenberg 2003 G-CSF was given concurrently with chemotherapy only
Maslak 1996 Historical control and not a RCT
Montillo 1998 Not a RCT
Moore 1997 Not a RCT - a study comparing tandem groups
Morton 2001 Patients were randomized to receive growth factor-induced bone marrow or growth factor-induced pe-
ripheral blood stem cells for allogeneic stem cell transplantation
Ohno 1994 Aim of the study was priming (2 days before chemotherapy)
Ohno 1997 Used monocyte-colony stimulating factor and not granulocyte-colony-stimulating factor or granulocyte-
monocyte-stimulating factor
Ohtake 2006 Comparison of 2 schedules of G-CSF (prophylactic versus therapeutic) and not randomized between G-
CSF and control
Ojeda 1999 Included patients with carcinoma of breast and lymphoma. Only a minority were AML patients
Ossenkopple 2004 RCT that randomized to G-CSF, cytarabine and fludarabine or G-CSF and cytarabine
Rowe 2004 Aim of the study was priming (2 days before chemotherapy)
Schmitz 1998 RCT that randomized to bone marrow-derived stem cell transplantation or filgrastim-mobilized peripheral
blood stem cell transplantation
Schriber 1994 Not a RCT
56Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Sierra 2005 Comparison of 2 schedules of G-CSF (pegfilgrastim versus filgrastim)
Stone 2001 Comparison of postremission therapy - mitoxantrone and intermediate-dose cytarabine compared to
standard-dose cytarabine
Takeshita 1995 Not a RCT
Takeshita 2000 Retrospective study
Takeyama 1995 Randomization was between routine addition of G-CSF after chemotherapy and addition of G-CSF in
case of neutropenic fever
Thomas 1999 GM-CSF was given during chemotherapy only
Thomas 2007a Aim of the study was priming (G-CSF during chemotherapy only)
Thomas 2007b Randomization to autologous stem cell transplantation or not
von Lilienfeld Toal 2007 Randomization between 2 schedules of G-CSF (immediate versus delayed G-CSF) in induction therapy
for patients with AML
AML: acute myelogenous leukemia; G-CSF: granulocyte colony-stimulating factor; GM-CSF: granulocyte macrophage colony-stim-
ulating factor; RCT: randomized controlled trial
57Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. All-cause mortality
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 All-cause mortality at 30 days 11 3319 Risk Ratio (M-H, Fixed, 95% CI) 0.97 [0.80, 1.18]
1.1 30 days 11 3319 Risk Ratio (M-H, Fixed, 95% CI) 0.97 [0.80, 1.18]
2 All-cause mortality at the end of
follow up
14 4119 Risk Ratio (M-H, Fixed, 95% CI) 1.01 [0.98, 1.05]
2.1 End of follow up 14 4119 Risk Ratio (M-H, Fixed, 95% CI) 1.01 [0.98, 1.05]
3 All-cause mortality subgroup
analysis age > 60
8 2125 Risk Ratio (M-H, Fixed, 95% CI) 1.01 [0.97, 1.05]
4 All-cause mortality subgroup
analysis age < 60
5 1079 Risk Ratio (M-H, Fixed, 95% CI) 1.08 [0.97, 1.20]
5 All-cause mortality sensitivity
analysis for allocation
concealment
10 3405 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.99, 1.07]
6 All-cause mortality sensitivity
analysis using random effects
model
14 4119 Risk Ratio (M-H, Random, 95% CI) 1.00 [0.96, 1.04]
6.1 End of follow up 14 4119 Risk Ratio (M-H, Random, 95% CI) 1.00 [0.96, 1.04]
Comparison 2. Overall survival
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Overall survival 11 3335 Hazard Ratio (95% CI) 1.00 [0.93, 1.08]
Comparison 3. Complete remission
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Complete response 17 4774 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.99, 1.07]
58Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 4. Disease-free survival
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Disease-free survival 7 1639 Hazard Ratio (95% CI) 1.00 [0.90, 1.13]
Comparison 5. Relapse rate
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Relapse rate 10 2189 Risk Ratio (M-H, Fixed, 95% CI) 0.97 [0.89, 1.05]
Comparison 6. Bacteremias
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Bacteremias 7 1638 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.82, 1.12]
Comparison 7. Invasive fungal infections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Invasive fungal infections 4 929 Risk Ratio (M-H, Fixed, 95% CI) 1.40 [0.90, 2.19]
Comparison 8. Episodes of febrile neutropenia
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Episodes of febrile neutropenia 9 2140 Risk Ratio (M-H, Fixed, 95% CI) 0.98 [0.94, 1.03]
59Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 9. Adverse events requiring discontinuation of CSFs
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Adverse events requiring
discontinuation of CSFs
4 770 Risk Ratio (M-H, Fixed, 95% CI) 1.33 [1.00, 1.76]
Analysis 1.1. Comparison 1 All-cause mortality, Outcome 1 All-cause mortality at 30 days.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 1 All-cause mortality at 30 days
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 30 days
Amadori 2005 53/360 25/182 18.6 % 1.07 [ 0.69, 1.67 ]
Bernasconi 1998 3/53 8/52 4.5 % 0.37 [ 0.10, 1.31 ]
Dombret 1995 13/88 17/85 9.7 % 0.74 [ 0.38, 1.43 ]
Harousseau 2000 2/100 2/94 1.2 % 0.94 [ 0.14, 6.54 ]
Heil 1997 21/259 25/262 13.9 % 0.85 [ 0.49, 1.48 ]
Milligan 2006 14/178 16/178 9.0 % 0.88 [ 0.44, 1.74 ]
Nakajima 1995 7/47 4/48 2.2 % 1.79 [ 0.56, 5.71 ]
Usuki 2002 7/120 5/125 2.7 % 1.46 [ 0.48, 4.47 ]
Wheatley 2009 48/401 48/402 26.9 % 1.00 [ 0.69, 1.46 ]
Witz 1998 20/110 19/122 10.1 % 1.17 [ 0.66, 2.07 ]
Zittoun 1996 1/27 2/26 1.1 % 0.48 [ 0.05, 4.99 ]
Total (95% CI) 1743 1576 100.0 % 0.97 [ 0.80, 1.18 ]
Total events: 189 (CSF), 171 (placebo/no treatment)
Heterogeneity: Chi2 = 5.75, df = 10 (P = 0.84); I2 =0.0%
Test for overall effect: Z = 0.32 (P = 0.75)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours CSFs Favours control
60Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 All-cause mortality, Outcome 2 All-cause mortality at the end of follow up.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 2 All-cause mortality at the end of follow up
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 End of follow up
Amadori 2005 307/360 155/182 13.7 % 1.00 [ 0.93, 1.08 ]
Beksac 2010 59/123 59/137 3.7 % 1.11 [ 0.85, 1.45 ]
Bradstock 2001 29/54 35/60 2.2 % 0.92 [ 0.66, 1.28 ]
Dombret 1995 75/88 73/85 5.0 % 0.99 [ 0.88, 1.12 ]
Godwin 1998 90/106 90/105 6.0 % 0.99 [ 0.89, 1.11 ]
Heil 1997 205/259 212/262 14.1 % 0.98 [ 0.90, 1.07 ]
Lowenberg 1997 36/60 34/63 2.2 % 1.11 [ 0.82, 1.51 ]
Milligan 2006 135/178 135/178 9.0 % 1.00 [ 0.89, 1.12 ]
Rowe 1995 39/44 44/46 2.9 % 0.93 [ 0.82, 1.05 ]
Stone 1995 162/193 150/195 9.9 % 1.09 [ 0.99, 1.20 ]
Usuki 2002 69/120 81/125 5.3 % 0.89 [ 0.73, 1.08 ]
Wheatley 2009 302/401 286/402 19.0 % 1.06 [ 0.97, 1.15 ]
Witz 1998 78/114 99/126 6.3 % 0.87 [ 0.75, 1.02 ]
Zittoun 1996 19/27 10/26 0.7 % 1.83 [ 1.06, 3.15 ]
Total (95% CI) 2127 1992 100.0 % 1.01 [ 0.98, 1.05 ]
Total events: 1605 (CSF), 1463 (placebo/no treatment)
Heterogeneity: Chi2 = 17.23, df = 13 (P = 0.19); I2 =25%
Test for overall effect: Z = 0.60 (P = 0.55)
Test for subgroup differences: Not applicable
0.02 0.1 1 10 50
Favours CSF Favours placebo/no tx
61Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 All-cause mortality, Outcome 3 All-cause mortality subgroup analysis age > 60.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 3 All-cause mortality subgroup analysis age > 60
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Amadori 2005 307/360 155/182 25.3 % 1.00 [ 0.93, 1.08 ]
Beksac 2010 59/123 59/137 6.8 % 1.11 [ 0.85, 1.45 ]
Dombret 1995 75/88 73/85 9.1 % 0.99 [ 0.88, 1.12 ]
Godwin 1998 90/106 90/105 11.1 % 0.99 [ 0.89, 1.11 ]
Rowe 1995 39/44 44/46 5.3 % 0.93 [ 0.82, 1.05 ]
Stone 1995 162/193 150/195 18.3 % 1.09 [ 0.99, 1.20 ]
Wheatley 2009 104/110 103/111 12.6 % 1.02 [ 0.95, 1.09 ]
Witz 1998 78/114 99/126 11.5 % 0.87 [ 0.75, 1.02 ]
Total (95% CI) 1138 987 100.0 % 1.01 [ 0.97, 1.05 ]
Total events: 914 (CSF), 773 (placebo/no treatment)
Heterogeneity: Chi2 = 8.53, df = 7 (P = 0.29); I2 =18%
Test for overall effect: Z = 0.31 (P = 0.75)
Test for subgroup differences: Not applicable
0.2 0.5 1 2 5
Favours CSF Favours pkacebo/no tx
62Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 All-cause mortality, Outcome 4 All-cause mortality subgroup analysis age < 60.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 4 All-cause mortality subgroup analysis age < 60
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bradstock 2001 29/54 30/60 9.9 % 1.07 [ 0.75, 1.53 ]
Harousseau 2000 27/100 31/94 11.1 % 0.82 [ 0.53, 1.26 ]
Lowenberg 1997 36/67 34/69 11.7 % 1.09 [ 0.79, 1.51 ]
Wheatley 2009 198/291 183/291 63.7 % 1.08 [ 0.96, 1.22 ]
Zittoun 1996 19/27 10/26 3.5 % 1.83 [ 1.06, 3.15 ]
Total (95% CI) 539 540 100.0 % 1.08 [ 0.97, 1.20 ]
Total events: 309 (CSF), 288 (placebo/no treatment)
Heterogeneity: Chi2 = 5.19, df = 4 (P = 0.27); I2 =23%
Test for overall effect: Z = 1.44 (P = 0.15)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours experimental Favours control
63Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 All-cause mortality, Outcome 5 All-cause mortality sensitivity analysis for
allocation concealment.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 5 All-cause mortality sensitivity analysis for allocation concealment
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Amadori 2005 307/360 155/182 17.2 % 1.00 [ 0.93, 1.08 ]
Beksac 2010 59/123 59/137 4.7 % 1.11 [ 0.85, 1.45 ]
Bradstock 2001 29/54 35/60 2.8 % 0.92 [ 0.66, 1.28 ]
Heil 1997 205/259 212/262 17.6 % 0.98 [ 0.90, 1.07 ]
Lowenberg 1997 36/60 34/63 2.8 % 1.11 [ 0.82, 1.51 ]
Milligan 2006 135/178 135/178 11.3 % 1.00 [ 0.89, 1.12 ]
Stone 1995 162/193 150/195 12.5 % 1.09 [ 0.99, 1.20 ]
Usuki 2002 69/120 81/125 6.6 % 0.89 [ 0.73, 1.08 ]
Wheatley 2009 302/401 286/402 23.8 % 1.06 [ 0.97, 1.15 ]
Zittoun 1996 19/27 10/26 0.9 % 1.83 [ 1.06, 3.15 ]
Total (95% CI) 1775 1630 100.0 % 1.03 [ 0.99, 1.07 ]
Total events: 1323 (CSF), 1157 (placebo/no treatment)
Heterogeneity: Chi2 = 11.25, df = 9 (P = 0.26); I2 =20%
Test for overall effect: Z = 1.32 (P = 0.19)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours CSF Favours placebo/no tx
64Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 All-cause mortality, Outcome 6 All-cause mortality sensitivity analysis using
random effects model.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 1 All-cause mortality
Outcome: 6 All-cause mortality sensitivity analysis using random effects model
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 End of follow up
Amadori 2005 307/360 155/182 15.1 % 1.00 [ 0.93, 1.08 ]
Beksac 2010 59/123 59/137 2.1 % 1.11 [ 0.85, 1.45 ]
Bradstock 2001 29/54 35/60 1.4 % 0.92 [ 0.66, 1.28 ]
Dombret 1995 75/88 73/85 7.9 % 0.99 [ 0.88, 1.12 ]
Godwin 1998 90/106 90/105 9.1 % 0.99 [ 0.89, 1.11 ]
Heil 1997 205/259 212/262 12.8 % 0.98 [ 0.90, 1.07 ]
Lowenberg 1997 36/60 34/63 1.6 % 1.11 [ 0.82, 1.51 ]
Milligan 2006 135/178 135/178 8.5 % 1.00 [ 0.89, 1.12 ]
Rowe 1995 39/44 44/46 7.9 % 0.93 [ 0.82, 1.05 ]
Stone 1995 162/193 150/195 10.8 % 1.09 [ 0.99, 1.20 ]
Usuki 2002 69/120 81/125 3.5 % 0.89 [ 0.73, 1.08 ]
Wheatley 2009 302/401 286/402 13.2 % 1.06 [ 0.97, 1.15 ]
Witz 1998 78/114 99/126 5.5 % 0.87 [ 0.75, 1.02 ]
Zittoun 1996 19/27 10/26 0.5 % 1.83 [ 1.06, 3.15 ]
Total (95% CI) 2127 1992 100.0 % 1.00 [ 0.96, 1.04 ]
Total events: 1605 (CSF), 1463 (placebo/no treatment)
Heterogeneity: Tau2 = 0.00; Chi2 = 17.23, df = 13 (P = 0.19); I2 =25%
Test for overall effect: Z = 0.05 (P = 0.96)
Test for subgroup differences: Not applicable
0.02 0.1 1 10 50
Favours CSF Favours placebo/no tx
65Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 Overall survival, Outcome 1 Overall survival.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 2 Overall survival
Outcome: 1 Overall survival
Study or subgroup CSFplacebo/notreatment Hazard Ratio Weight Hazard Ratio
n/N n/N
Exp[(O-E)/V],Fixed,95%
CI
Exp[(O-E)/V],Fixed,95%
CI
Bradstock 2001 29/54 35/60 2.6 % 0.84 [ 0.51, 1.37 ]
Dombret 1995 75/88 73/85 6.1 % 0.95 [ 0.69, 1.31 ]
Godwin 1998 90/106 90/105 7.3 % 0.95 [ 0.71, 1.27 ]
Harousseau 2000 27/100 31/94 2.3 % 0.73 [ 0.44, 1.23 ]
Heil 1997 205/259 212/262 17.5 % 1.00 [ 0.83, 1.21 ]
Milligan 2006 135/178 135/178 10.8 % 1.03 [ 0.81, 1.31 ]
Rowe 1995 39/44 44/46 3.4 % 0.65 [ 0.42, 1.00 ]
Stone 1995 162/193 150/195 12.6 % 1.20 [ 0.96, 1.50 ]
Usuki 2002 69/120 81/125 6.0 % 0.90 [ 0.65, 1.24 ]
Wheatley 2009 302/401 262/402 24.3 % 1.15 [ 0.98, 1.35 ]
Witz 1998 78/114 99/126 7.1 % 0.77 [ 0.57, 1.03 ]
Total (95% CI) 100.0 % 1.00 [ 0.93, 1.08 ]
Heterogeneity: Chi2 = 15.15, df = 10 (P = 0.13); I2 =34%
Test for overall effect: Z = 0.05 (P = 0.96)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
66Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Complete remission, Outcome 1 Complete response.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 3 Complete remission
Outcome: 1 Complete response
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Amadori 2005 203/360 89/182 7.9 % 1.15 [ 0.97, 1.37 ]
Beksac 2010 77/123 89/137 5.6 % 0.96 [ 0.80, 1.16 ]
Bernasconi 1998 23/53 17/52 1.1 % 1.33 [ 0.81, 2.18 ]
Bradstock 2001 44/54 44/59 2.8 % 1.09 [ 0.90, 1.33 ]
Dombret 1995 62/88 40/85 2.7 % 1.50 [ 1.15, 1.95 ]
Estey 1999 61/107 49/108 3.2 % 1.26 [ 0.96, 1.64 ]
Godwin 1998 43/106 52/105 3.5 % 0.82 [ 0.61, 1.11 ]
Heil 1997 178/259 177/262 11.7 % 1.02 [ 0.90, 1.14 ]
Lehrnbecher 2007 154/161 149/156 10.1 % 1.00 [ 0.96, 1.05 ]
Lowenberg 1997 46/60 47/63 3.1 % 1.03 [ 0.84, 1.26 ]
Milligan 2006 103/178 109/178 7.3 % 0.94 [ 0.80, 1.12 ]
Rowe 1995 36/60 25/57 1.7 % 1.37 [ 0.96, 1.96 ]
Stone 1995 99/193 106/195 7.0 % 0.94 [ 0.78, 1.14 ]
Usuki 2002 97/120 96/125 6.3 % 1.05 [ 0.92, 1.20 ]
Wheatley 2009 292/401 302/402 20.1 % 0.97 [ 0.89, 1.05 ]
Witz 1998 69/110 74/122 4.7 % 1.03 [ 0.84, 1.27 ]
Zittoun 1996 13/27 20/26 1.4 % 0.63 [ 0.40, 0.98 ]
Total (95% CI) 2460 2314 100.0 % 1.03 [ 0.99, 1.07 ]
Total events: 1600 (CSF), 1485 (placebo/no treatment)
Heterogeneity: Chi2 = 27.92, df = 16 (P = 0.03); I2 =43%
Test for overall effect: Z = 1.27 (P = 0.20)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
67Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Disease-free survival, Outcome 1 Disease-free survival.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 4 Disease-free survival
Outcome: 1 Disease-free survival
Study or subgroup CSFplacebo/notreatment Hazard Ratio Weight Hazard Ratio
n/N n/N
Exp[(O-E)/V],Fixed,95%
CI
Exp[(O-E)/V],Fixed,95%
CI
Godwin 1998 36/43 46/52 6.9 % 0.82 [ 0.53, 1.27 ]
Heil 1997 142/178 140/177 23.9 % 1.00 [ 0.79, 1.26 ]
Milligan 2006 71/103 78/108 13.2 % 0.89 [ 0.65, 1.22 ]
Rowe 1995 18/27 13/21 2.6 % 0.98 [ 0.48, 2.00 ]
Usuki 2002 64/97 64/96 10.9 % 0.99 [ 0.70, 1.40 ]
Wheatley 2009 203/292 206/302 34.6 % 1.11 [ 0.91, 1.35 ]
Witz 1998 40/69 57/74 8.0 % 1.00 [ 0.67, 1.50 ]
Total (95% CI) 100.0 % 1.00 [ 0.90, 1.13 ]
Heterogeneity: Chi2 = 2.38, df = 6 (P = 0.88); I2 =0.0%
Test for overall effect: Z = 0.08 (P = 0.94)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
68Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.1. Comparison 5 Relapse rate, Outcome 1 Relapse rate.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 5 Relapse rate
Outcome: 1 Relapse rate
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Amadori 2005 145/203 64/89 16.0 % 0.99 [ 0.85, 1.16 ]
Beksac 2010 37/123 50/137 8.5 % 0.82 [ 0.58, 1.17 ]
Bernasconi 1998 20/39 15/27 3.2 % 0.92 [ 0.59, 1.46 ]
Harousseau 2000 36/100 43/94 8.0 % 0.79 [ 0.56, 1.11 ]
Lehrnbecher 2007 49/154 43/149 7.9 % 1.10 [ 0.78, 1.55 ]
Lowenberg 1997 25/46 26/47 4.6 % 0.98 [ 0.68, 1.42 ]
Milligan 2006 60/103 71/108 12.5 % 0.89 [ 0.72, 1.10 ]
Wheatley 2009 172/292 163/302 28.8 % 1.09 [ 0.95, 1.26 ]
Witz 1998 40/69 57/74 9.9 % 0.75 [ 0.59, 0.95 ]
Zittoun 1996 7/13 5/20 0.7 % 2.15 [ 0.87, 5.35 ]
Total (95% CI) 1142 1047 100.0 % 0.97 [ 0.89, 1.05 ]
Total events: 591 (CSF), 537 (placebo/no treatment)
Heterogeneity: Chi2 = 13.68, df = 9 (P = 0.13); I2 =34%
Test for overall effect: Z = 0.81 (P = 0.42)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
69Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.1. Comparison 6 Bacteremias, Outcome 1 Bacteremias.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 6 Bacteremias
Outcome: 1 Bacteremias
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Dombret 1995 14/88 13/85 6.0 % 1.04 [ 0.52, 2.08 ]
Godwin 1998 50/106 45/105 20.6 % 1.10 [ 0.82, 1.48 ]
Harousseau 2000 40/100 45/94 21.2 % 0.84 [ 0.61, 1.15 ]
Lehrnbecher 2007 25/161 23/156 10.7 % 1.05 [ 0.63, 1.77 ]
Lowenberg 1997 10/60 6/63 2.7 % 1.75 [ 0.68, 4.52 ]
Stone 1995 47/193 53/195 24.1 % 0.90 [ 0.64, 1.26 ]
Witz 1998 24/110 34/122 14.7 % 0.78 [ 0.50, 1.23 ]
Total (95% CI) 818 820 100.0 % 0.96 [ 0.82, 1.12 ]
Total events: 210 (CSF), 219 (placebo/no treatment)
Heterogeneity: Chi2 = 4.17, df = 6 (P = 0.65); I2 =0.0%
Test for overall effect: Z = 0.55 (P = 0.58)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
70Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.1. Comparison 7 Invasive fungal infections, Outcome 1 Invasive fungal infections.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 7 Invasive fungal infections
Outcome: 1 Invasive fungal infections
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Dombret 1995 4/88 0/85 1.7 % 8.70 [ 0.48, 159.11 ]
Godwin 1998 21/104 16/103 54.6 % 1.30 [ 0.72, 2.35 ]
Lehrnbecher 2007 4/161 0/156 1.7 % 8.72 [ 0.47, 160.67 ]
Witz 1998 11/110 13/122 41.9 % 0.94 [ 0.44, 2.01 ]
Total (95% CI) 463 466 100.0 % 1.40 [ 0.90, 2.19 ]
Total events: 40 (CSF), 29 (placebo/no treatment)
Heterogeneity: Chi2 = 4.17, df = 3 (P = 0.24); I2 =28%
Test for overall effect: Z = 1.51 (P = 0.13)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours CSF Favours placebo/no tx
71Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 8.1. Comparison 8 Episodes of febrile neutropenia, Outcome 1 Episodes of febrile neutropenia.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 8 Episodes of febrile neutropenia
Outcome: 1 Episodes of febrile neutropenia
Study or subgroup CSFplacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bradstock 2001 11/54 13/60 1.6 % 0.94 [ 0.46, 1.92 ]
Dombret 1995 42/88 41/85 5.5 % 0.99 [ 0.73, 1.35 ]
Heil 1997 236/259 241/261 31.7 % 0.99 [ 0.94, 1.04 ]
Lehrnbecher 2007 78/161 72/156 9.7 % 1.05 [ 0.83, 1.32 ]
Lowenberg 1997 51/60 48/63 6.2 % 1.12 [ 0.94, 1.33 ]
Stone 1995 112/179 118/184 15.4 % 0.98 [ 0.83, 1.14 ]
Usuki 2002 92/120 95/125 12.3 % 1.01 [ 0.88, 1.16 ]
Witz 1998 93/110 121/122 15.1 % 0.85 [ 0.79, 0.92 ]
Zittoun 1996 22/27 19/26 2.6 % 1.12 [ 0.83, 1.50 ]
Total (95% CI) 1058 1082 100.0 % 0.98 [ 0.94, 1.03 ]
Total events: 737 (CSF), 768 (placebo/no treatment)
Heterogeneity: Chi2 = 15.07, df = 8 (P = 0.06); I2 =47%
Test for overall effect: Z = 0.64 (P = 0.53)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours CSF Favours placebo/no tx
72Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 9.1. Comparison 9 Adverse events requiring discontinuation of CSFs, Outcome 1 Adverse events
requiring discontinuation of CSFs.
Review: Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
Comparison: 9 Adverse events requiring discontinuation of CSFs
Outcome: 1 Adverse events requiring discontinuation of CSFs
Study or subgroup CSFs Control Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Rowe 1995 0/62 0/62 0.0 [ 0.0, 0.0 ]
Stone 1995 60/179 56/182 1.09 [ 0.81, 1.47 ]
Witz 1998 15/110 5/122 3.33 [ 1.25, 8.85 ]
Zittoun 1996 4/27 0/26 8.68 [ 0.49, 153.60 ]
Total (95% CI) 378 392 1.33 [ 1.00, 1.76 ]
Total events: 79 (CSFs), 61 (Control)
Heterogeneity: Chi2 = 6.69, df = 2 (P = 0.04); I2 =70%
Test for overall effect: Z = 1.96 (P = 0.050)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours experimental Favours control
A P P E N D I C E S
Appendix 1. CENTRAL search strategy
Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2009, Issue 3)
ID Search
#1 MeSH descriptor Hematopoietic Cell Growth Factors explode all trees
#2 (pegylated granulocyte colony-stimulating factor, human)
#3 “granulocyte colony-stimulating factor, Tyr(1)-Tyr(3)-”
#4 MeSH descriptor Colony-Stimulating Factors explode all trees
73Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
#5 MeSH descriptor Colony-Stimulating Factors, Recombinant explode all trees
#6 MeSH descriptor Granulocyte Colony Stimulating Factor, Recombinant explode all trees
#7 MeSH descriptor Granulocyte Colony-Stimulating Factor explode all trees
#8 MeSH descriptor Granulocyte-Macrophage Colony-Stimulating Factor explode all trees
#9 MeSH descriptor Macrophage Colony-Stimulating Factor explode all trees
#10 (RHG*CSF* or RH-G*CSF* or RHGM*CSF* or RH-GM*CSF*)
#11 (RMETHUG* or RHMETHUG* or R-METHUG* or RH-METHUG*)
#12 (RHUG* or RHUGM*)
#13 (GCSF* or G-CSF*)
#14 (GM-CSF* or GMCSF*)
#15 (GRANULO*YT* NEAR/3 FA*TOR*)
#16 (MA*ROPHAG* NEAR/5 FA*TOR*)
#17 (FILGRASTIM*)
#18 (neupogen*)
#19 (religrast*)
#20 (nugraf*)
#21 (LENOGRASTIM*)
#22 (Granocyte*)
#23 (Euprotin*)
#24 (PEG*FILGRASTIM*)
#25 (Neulasta*)
#26 (LEUKINE*)
#27 (sagramostim*)
#28 (MOLGRAMOSTIN*)
74Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
#29 (macrogen*)
#30 (Mielogen*)
#31 (Leucomax*)
#32 (nartograstim*)
#33 (pegnartograstim*)
#34 (ecogramostim*)
#35 (regramostim*)
#36 (leridistim*)
#37 (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15
OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR
#29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36)
#38 MeSH descriptor Leukemia, Myeloid, Acute explode all trees
#39 MeSH descriptor Leukemia, Myeloid explode all trees
#40 MeSH descriptor Acute Disease explode all trees
#41 (#39 AND #40)
#42 (acut* or akut* or agud* or aigu*) and (myelo* or nonlympho* or granulocytic* or monocyt* or megakaryoblast* or
promyelocyt* or erythroblast*) and (leuk*em* or leuc*)
#43 (myelo* and naegel* ) and (leuk*em* or leuc*)
#44 (erythroleuk*em*)
#45 (di guglielmo*)
#46 (erythremic* NEAR myelos*)
#47 MeSH descriptor Leukemia, Monocytic, Acute explode all trees
#48 MeSH descriptor Leukemia, Megakaryoblastic, Acute explode all trees
#49 MeSH descriptor Leukemia, Myelomonocytic, Acute explode all trees
#50 MeSH descriptor Leukemia, Promyelocytic, Acute explode all trees
75Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
#51 MeSH descriptor Leukemia, Erythroblastic, Acute explode all trees
#52 (aml)
#53 (#38 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 OR #49 OR #50 OR #51 OR #52)
#54 (#37 AND #53)
Appendix 2. MEDLINE search strategy
1 Hematopoietic Cell Growth Factors/
2 pegylated granulocyte colony-stimulating factor, human.nm.
3 “granulocyte colony-stimulating factor, Tyr(1)-Tyr(3)-”.nm.
4 COLONY-STIMULATING FACTORS/
5 exp COLONY-STIMULATING FACTORS, RECOMBINANT/
6 exp GRANULOCYTE COLONY STIMULATING FACTOR, RECOMBINANT/
7 exp GRANULOCYTE COLONY-STIMULATING FACTOR/
8 exp GRANULOCYTE-MACROPHAGE COLONY-STIMULATING FACTOR/
9 MACROPHAGE COLONY-STIMULATING FACTOR/
10 (RHG?CSF$ or RH-G?CSF$ or RHGM?CSF$ or RH-GM?CSF$).tw.
11 (RMETHUG$ or RHMETHUG$ or R-METHUG$ or RH-METHUG$).tw.
12 (RHUG$ or RHUGM$).tw.
13 (GCSF$ or G-CSF$).tw.
14 (GM-CSF$ or GMCSF$).tw.
15 (GRANULO?YT$ adj3 FA#TOR$).tw.
16 (MA#ROPHAG$ adj5 FA#TOR$).tw.
17 FILGRASTIM$.tw,hw,nm,kf.
76Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
18 neupogen$.tw,hw,nm,kf.
19 religrast$.tw,kf,nm,kf.
20 nugraf$.tw,kf,nm,kf.
21 LENOGRASTIM$.tw,hw,nm,kf.
22 Granocyte.tw,hw,nm,kf.
23 Euprotin.tw,hw,nm,kf.
24 PEG?FILGRASTIM$.tw,hw,nm,kf.
25 Neulasta.tw,hw,nm,kf.
26 LEUKINE.tw,hw,nm,kf.
27 sagramostim$.tw,kf,nm,ot.
28 MOLGRAMOSTIN$.tw,hw,nm,kf.
29 macrogen$.tw,kf,nm,ot.
30 Mielogen$.tw,kf,nm,ot.
31 Leucomax$.tw,hw,nm,kf.
32 nartograstim$.tw,kf,nm,ot.
33 pegnartograstim$.tw,kf,nm,ot.
34 ecogramostim$.tw,kf,nm,ot.
35 regramostim$.tw,kf,nm,ot.
36 leridistim$.tw,kf,ot.
37 or/1-36
38 exp LEUKEMIA, MYELOID, ACUTE/
39 LEUKEMIA, MYELOID/
40 ACUTE DISEASE/
41 39 and 40
77Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
42 (acut$ or akut$ or agud$ or aigu$).tw,kf,ot.
43 ((myelo$ or nonlympho$ or granulocytic$ or monocyt$ or megakaryoblast$ or promyelocyt$ or erythroblast$) and (leuk?em$
or leuc$)).tw,kf,ot
44 42 and 43
45 (myelo$ and naegel$ and (leuk?em$ or leuc$)).tw,kf,ot.
46 erythroleuk?em$.tw,kf,ot.
47 di guglielmo$.tw,kf,ot.
48 (erythremic$ adj myelos$).tw,kf,ot.
49 LEUKEMIA, MONOCYTIC, ACUTE/
50 LEUKEMIA, MEGAKARYOBLASTIC, ACUTE/
51 LEUKEMIA, MYELOMONOCYTIC, ACUTE/
52 LEUKEMIA, PROMYELOCYTIC, ACUTE/
53 LEUKEMIA, ERYTHROBLASTIC, ACUTE/
54 aml.tw,kf,ot.
55 or/44-54
56 38 or 41 or 55
57 randomized controlled trial.pt.
58 controlled clinical trial.pt.
59 randomized.ab.
60 placebo.ab.
61 drug therapy.fs.
62 randomly.ab.
63 trial.ab.
64 groups.ab.
65 or/57-64
78Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
66 humans.sh.
67 65 and 66
68 37 and 56
69 67 and 68
Lines 1 to 37:
Search part for CSF. The search consists of subject heading and text word search
In, for example, search line 5 the MeSH-term was exploded (exp). This search command lets you retrieve results that contain
the subject heading in combination with all of its narrower terms
It is necessary to use a text word search. The search term ran in the fields tw (text word), kf (keyword), ot (original title), nm
(name of substance) and hw (subject heading word)
Lines 40 to 56:
Search part for the disease AML.
Line 57 to 68:
Cochrane RCT search filter for MEDLINE/OVID.
Line 69:
Result of the search.
F E E D B A C K
Inappropriate conclusions, 4 October 2011
Summary
The review has the title: “Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute
myelogenous leukemia.” This makes it clear what the review is about, namely the possibility of preventing or treating infections by
using colony-stimulating factors (CSFs). This could be life-saving. Acute myelogenous leukaemia has a high mortality rate and the
patients may die from infections acquired during chemotherapy-induced neutropenia. Accordingly, the primary outcomes in the review
are mortality outcomes. The review did not find an effect on any major outcome. The abstract tells us that the relative risk or hazard
ratio was 1 for all-cause mortality, overall survival, complete remission rates, relapse rates, disease-free survival and bacteremias. For
invasive fungal infections, there was a non-significant tendency towards more infections when CSF was used (RR 1.40; 95% CI 0.90
to 2.19).
1. “Authors’ conclusions” in the abstract do not reflect these unequivocally negative findings: “The addition of CSFs to chemotherapy
does not adversely influence all-cause mortality, complete remission or relapse rates in patients with AML. Although the benefit of
CSFs is limited to reduction of neutropenic and febrile days, they can be administered safely when necessary.”
This conclusion is inappropriate. When the relative risk and hazard ratio for all the most important outcomes are 1, with narrow
confidence intervals, as the total sample size was very large (19 trials including 5256 patients), it is inappropriate to say that CSFs “does
not adversely influence all-cause mortality, complete remission or relapse rates.” The hope was that CSF would work, i.e. reduce these
outcomes, which it did not, and the authors should say so, rather than concluding that CSFs reduce neutropenic and febrile days and
can be administered safely when necessary.
2. Furthermore, it is not appropriate to give a result in the conclusions that was not given under Results in the abstract.
79Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

3. These drugs are highly expensive. When exactly do the authors imagine they should be used when they have no effect on the outcomes
that matter? One should not use expensive drugs that were supposed to reduce infections and deaths for reducing days with fever. That
can be obtained with very cheap drugs.
4. The conclusions are not in accordance with the findings and the title of the review and should be changed; neutropenic and febrile
days should not appear in the abstract at all.
5. I find it likely that the “Authors’ conclusions” either reflect the biases of the authors, or the editors, or the peer reviewers.
• Did the editors ask the authors to change their conclusions into something more positive than they had intended?
• Did the editors (or peer reviewers) have conflicts of interest related to companies marketing colony-stimulating factors?
Submitter agrees with default conflict of interest statement: I certify that I have no affiliations with or involvement in any organization
or entity with a financial interest in the subject matter of my feedback..
Reply
Reply to point 1:
The goal of this review as stated in the objectives paragraph was:
“- To evaluate the safety and efficacy of CSFs administered after induction, consolidation or salvage treatment and after HSCT in
patients with AML.
- To evaluate the safety of CSFs in young versus elderly patients as defined per study (usually older than 55 to 60 years).”
We agree that we could not show a beneficial effect in terms of efficacy. Nevertheless, as the main concern with the administration of
growth factors in AML patients is their safety, the “raison d’être” of our review was to establish their safe use in AML. This indeed was
shown in our results for all AML patients as well as for the subgroup of elderly patients, as manifested by the fact that, as stated by the
critic himself, the relative risks and hazard ratios for all the most important outcomes were 1, with narrow confidence intervals.
Nevertheless, in view of the feedback we revised:
1. Authors’ conclusions in the abstract:
“In summary, colony-stimulating factors should not be given routinely to acute myelogenous leukemia patients post-chemotherapy
since they do not affect overall survival or infectious parameters including the rate of bacteremias and invasive fungal infections.”
2. The authors’ conclusions in the main text / Implications for practice:
“In summary, colony-stimulating factors should not be given routinely to acute myelogenous leukemia patients post-chemotherapy
since they do not improve overall survival, or infectious parameters including the rate of bacteremias and invasive fungal infections.
Yet, our results show that, on the other hand, they do not adversely affect hematological outcomes such as complete remission, relapse
rate and disease-free survival.”
Reply to point 2:
We agree that it is not appropriate to give a result in the conclusions that was not given under results. We therefore changed our
conclusions in the abstract and the conclusions in the main text / Implications for practice as stated in “Reply to point 1”.
Reply to point 3:
We accepted the feedback and changed our conclusions in the abstract and the conclusions in the main text/implications for practice
as stated in “Reply to point 1”.
Reply to point 4:
We accepted the feedback and changed our conclusions in the abstract and conclusions / Implications for practice as stated in “Reply
to point 1”. We deleted neutropenic and febrile days from the authors’ conclusions in the abstract.
Reply to point 5 (from the Editorial Base):
All the authors of the review filled out the conflict of interest statement and declared that they had no conflict of interest. During the
time the editors have commented on the present review, the Editorial Base had not yet asked the editors for the disclosure of potential
conflicts of interest. After reviewing the e-mail exchange on this review the Editorial Base and the Feedback Editor were not able to
identify any indications for conflicts of interest on the side of the editors. The editorial discussion was mainly about methodological/
statistical issues. None of the editors questioned the initial conclusions of the authors.
In the meantime the CHMG adapted the group’s policy: Since November 2011 the Editorial Base asks all editors to disclose their
potential conflicts of interest with respect to each review they comment on. The conflict of interest statement can be requested at the
Editorial Base.
Contributors
80Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Gurion R, Belnik-Plitman Y, Gafter-Gvili A, Paul M, Vidal L, Ben-Bassat I, Shpilberg O, Raanani P: author and co-authors of the
review
Trelle S, Kluge S, Skoetz N: Feedback Editor, Managing Editor, Co-ordinating Editor of the Cochrane Haematological Malignancies
Group
W H A T ’ S N E W
Last assessed as up-to-date: 24 January 2011.
Date Event Description
11 May 2012 New citation required and conclusions have changed Changes made in full text and abstract
11 May 2012 Feedback has been incorporated Amended review according to valid feedback
H I S T O R Y
Protocol first published: Issue 1, 2010
Review first published: Issue 9, 2011
C O N T R I B U T I O N S O F A U T H O R S
Ronit Gurion - conception and design, provision of study material, protocol development, search for trials, data extraction, analysis
and data interpretation, writing of the review and final approval
Yulia Belnik-Plitman- conception and design, provision of study material, protocol development, search for trials, data extraction, final
approval of the review.
Anat Gafter-Gvili - conception and design, provision of study material, protocol development, data extraction, final approval of the
review, methodological advice.
Mical Paul - conception and design, protocol development, provision of study material, data extraction, analysis and data interpretation,
writing of the review and final approval, clinical and scientific advice.
Liat Vidal - provision of study material, protocol development, data extraction, analysis and data interpretation, final approval of the
review, methodological advice.
Isaac Ben-Bassat - conception and design, protocol development, final approval of the review, clinical and scientific advice.
Ofer Shpilberg - conception and design, protocol development, final approval of the review, clinical and scientific advice.
Pia Raanani - conception and design, provision of study material, protocol development, analysis and data interpretation, writing of
the review and final approval, clinical and scientific advice.
81Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
Internal sources
• Young Investigator’s Grant, Rabin Medical Center, Beilinson Hospital, Israel.
A 30,000 NIS grant donated to young investigator - Dr. Ronit Gurion
External sources
• No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Antineoplastic Combined Chemotherapy Protocols [∗therapeutic use]; Granulocyte Colony-Stimulating Factor [∗therapeutic use];
Granulocyte-Macrophage Colony-Stimulating Factor [∗therapeutic use]; Induction Chemotherapy [methods]; Infection [∗drug ther-
apy; etiology]; Leukemia, Myeloid, Acute [complications; ∗drug therapy; mortality]
MeSH check words
Humans
82Colony-stimulating factors for prevention and treatment of infectious complications in patients with acute myelogenous leukemia
(Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.