Embed Size (px)
Citation preview

COEXISTENCE OF LEUKEMIC RETICULOENDOTHELIOSIS AND HISTIOCYTIC LYMPHOMA
A Case Report
SOLOMON S. ADLER, MD,* J A Y A R A M A SHETTY, M D , t A N D HARVEY M. GOLOMB, MD$
A 65-year-old woman had pancytopenia, splenomegaly, and an inaspirable bone marrow. Diagnostic evaluation demonstrated that she had both leukemic reticuloendotheliosis (LRE), or hairy cell leukemia, and an additional lympho-reticular neoplasm, most likely a “histiocytic” lymphoma. The diagnosis of LRE was based on the histopathology of spleen tissue and of a bone marrow biopsy specimen. The diagnosis of diffuse “histiocytic” lymphoma was based on the histopathology of a splenic hilar and a mesenteric lymph node, tumor nodules in the kidney and spleen, and tissue from a mass obstructing a ureter. This is the first well-documented association of a second lympho-reticular neoplasm with LRE. Even relatively gentle treatment of the “histiocytic” lymphoma resulted in fatal pancytopenia, illustrating the restrictions on therapy imposed by the marrow impairment due to the LRE.
Cancer 43:1872-1880, 1979.
HE TERM “leukemic reticuloendotheliosis” T (LRE) was coined in 1923,y but the recognition of this disease as a distinct clinical
From the Departments of Medicine and Pathology, Rush-Presbyterian-St. Luke’s Medical Center, Chicago. Illinois, and the Department of Medicine, University of Chicago Hospitals and Clinics, Chicago. Illinois.
* Assistant Professor of Medicine, Rush-Presbyterian- St. Luke’s Medical Center.
t Resident, Department ot‘ Pathology, Rush-Presby- terian-St. Luke’s Medical Center; currently at St. Luke’s Episcopal Hospital, Houston. Texas.
t Assistant Professor of Medicine, University of Chicago Hospitals and Clinics.
Supported in part by grants from the Leukemia Rc- search Foundation. Chicago, Illinois, and in part by the Julius Frankel Endowment Fund, Hetnatology Research Foundation, Otho S. A. Sprague Memorial Institute. and the Thomas Moore Fund.
The authors thank S. A. Xydakis, MI), SC:, Chicago, IL, for referi-ing the patient to us; E. V. Pellettiere. MD. Rush-Presbyterian-St. 1.uke’s Medical Center, Chicago. IL, for his collaboration, encouragement. and advice in preparing the manuscript; 1. Vardiiixin. MD, and D. Variakqjis, MD. University of Chicago Hospitals and Clinics, Chicago, IL. and H. Rappaport, MD, and 6. Nathwani. MD. City of Hope National Medical Center, Duane. CA, for their aid in reviewing the pathology and for special cytological studies; and Deborah Simon, Eileen Leatherman, and Craig Rosner for technical as- sistance.
Address for reprints: Solomon S. Atller. MD, Section of Hematology, Rush-Presb~terian-St. Luke’s Medical Center, 17.53 West Congress Parkway, Chicago, I L 60612.
Accepted for publication June 9, 1978.
entity was established only two decades ago with a report by Bouroncle et aL3 Since that time, much speculation on the nature of the cell involved has appeared in the medical liter- ature, and the issue is not yet resolved.’ De- spite the large number of patients with LRE who have been followed closely, there are only passing references in the l i t e r a t ~ r e ~ “ ~ * * ~ to second malignancies in this group of patients, and no instance has been reported in which LRE transformed into another disorder. Here w e report on a patient with coexistent LRE and a lymphoid neoplasm, probably a “histio- cytic” lymphoma.
CASE REPORT
A 65-year-old Caucasian woman with a six year history of insulin-dependent diabetes mellitus and with a two-month history of weakness and malaise was referred LO one of us (S.A.) in June 1977. She had been found to have splenomegaly, pancyto- penia, and a “myelofibrotic” marrow. Therapy with prednisone, 40 mg/day, for the “myelo- fibrosis” had been started about one monih prior t o her referral.
On physical examination, she was found to be in no obvious distress. She was 5’4” tall and weighed 149 Ibs; her tadial pulse was 80/minute, respira- tory rate 20/minute, and blood pressure 180/90 nim Hg. T h e liver was not enlarged, and there was no palpable lymphadenopathy. T h e follow- ing pertinent abnormalities were observed: the
0008-543X/79/0500/1872 $0.95 0 American Cancer Society
1872

No. 5 LRE AND HISTIOCYTIC LYMPHOMA * Adler et al. 1873
spleen edge was felt about 7 cm below the left costal margin on inspiration; there was a firm, nonpulsatile mass, about 4 cm in diameter, in the upper abdomen just to the right of the midline; and there was pitting edema of both lower extremities.
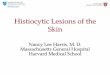
The hemogram included: a hemoglobin value of 1 1.7 g/dl and hematocrit of 34.6% with MCV of 90 cu microns, a MCH of 30.4 pg, and a MCHC of 33.8%; a relative reticulocyte count of 4.1%; a white blood cell count of 1,900/mm3 with 22% polymorphonuclear leukocytes, 4% bands, 1 % metamyelocytes, 7 1 % lymphocytes, 1 % monocytes and 1% basophils; and a platelet count of 86,000/ mm3. Three to 4% of the lymphocytes had cyto- plasmic projections giving them the appearance of hairy cells (Fig. 1). The results of the SMA-18 were normal except for the following: glucose 233 mg/dl, LDH 255 IU, SGPT 39 IU. The serum folk acid level was 4 ng/dl, and the vitamin B- 12 level was 320 pg/ml. The direct and indirect Coombs’ tests were negative and protein elec- trophoresis, immunoelectrophoresis, and quan- titative analysis of the immunoglobulins were un- remarkable. A bone marrow aspirate from the posterior iliac crest did not yield any spicules; the diagnosis of LRE was made on the basis of the findings of a core biopsy (Fig. 2).
The patient’s steroid therapy was discontinued on 6/9/77 because there appeared to be no in- dication for it. While being cared for as an out- patient, she developed pain in the upper abdomen just to the right of the mid-line; she was, therefore, admitted to Rush-Presbyterian-St. Luke’s Medical Cedter. At this time, she was somewhat more anemic and leukopenic than previously. By lymphangiography, the patient was found to have abnormal abdominal lymph nodes. and by intra- venous pyelography and cystoureteroscopy, hy- dronephrosis on the right side related to ob- struction of the right ureter was detected. The patient did not respond to skin tests for SKSD and PPD even at second strengths or for Candida, tricophyton, and staphylococcus lysate.
The patient had intermittent fever, but no in- fection was found. On 7/26/77, the following sur- gical procedures were performed: excision of the enlarged primary spleen and of a small accessory spleen; wedge biopsies of the right and left lobes of the liver; excision of an omental node; and right nephrectomy with partial ureterectomy. A por- tion of the abdominal aorta was encased in tumor which was not biopsied. Histologic evaluation of the various specimens led to the diagnosis of LRE and “histiocytic” lymphoma (for details of patho- logic findings, see Results).
After surgery, the patient’s hemogram improved substantially. A tomographic gallium scan con- firmed the presence of tumor in the area of the abdominal aorta and revealed a small lesion in the right upper chest cage, probably in a rib.
FIG. 1 . Hairy cell in peripheral blood (H & E, X 1000).
The patient was discharged, and outpatient treatment of the “histiocytic” lymphoma was planned. In the first week after discharge, how- ever, she developed increasing edema of the lower extremities, with severe pain radiating from the left groin to the thigh.
She was readmitted on 8/22/77; this was her second and final admission. Her left leg was markedly edematous. The admitting physician diagnosed severe lymphatic obstruction and therefore initiated radiation therapy to the abdominal area. A venogram, performed during the course of radiotherapy, demonstrated ex- tensive bilateral thromboses of the deep veins, and heparin therapy was instituted. After the patient had received 1500 rads, her white blood cell count fell to 200/mm3 and her platelet count to 2,000/ mm3; radiotherapy was discontinued. Recovery of the blood counts was extremely slow; over 3-4 months the white cell count reached 5,000/mm3 and the platelet count increased to only 50,000/ mm3. During a period of marked thrombocyto- penia, heparin was omitted briefly. The patient developed phlegmasia cerulea dolens which re-

1874 CANCER May 1979 Vol. 43
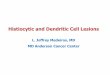
FIG. 2. Photomicrograph of typical area of the prc- splenectomy bone marrow biopsy specimen. Lytiiphoicl elements with vesicular nuclei have infiltrated the marrow, and there is a prominent increase of stroinal fibers; this picture is characteristic of leukemic reticuloendotheliosis (Reticulin stain, ~ 3 6 0 ) .
solved over the next 2-3 months with conserva- tive management.
The abdominal tumor was not visible on a gallium scan performed after the abdominal ir- radiation, but several new bone lesions as well as a probable pulmonary lesion were evident. A bone scan indicated the presence of numerous meta- static lesions. T h e bone marrow was still in- aspirable three months after surgery, but a marrow biopsy showed substantial improvement. There were no diffuse areas of infiltration by lymphoid elements such as were seen in the speci- men taken prior to splenectorny; instead, there was good representation of all myeloid and erythroid precursors. Scattered abnormal lymphoid elements were still seen, in addition to significant fibrosis.
During most of this hospital stay, the patient had considerable anorexia and lost about 50 pounds. After improvement of the phlegmasia cerulea dolens and the radiation-induced cyto-
penias, w e instituted the following therapy for the “histiocytic” lymphoma: cyclophosphamide, 750 mg. i v on day 1; vincristine, 2 mg iv on day 1; bleomycin, 15 mg/dose on days 1 and 5; and prednisone, 100 mg PO in a single daily dose on days 1-5. About 10 days after completion of this therapy, the granulocyte count decreased from about 3,000/mm3 to 500/mm3; the nadir of the platelet count was about 40.000/mm3. By 2-2% weeks after this course of therapy, the blood counts had improved substantially; the leukocyte count was above 5,000/mm3 with 80% granulocytes, and the platelet count was lZ0,000/n1m3-ZO0,000/ mmY. A second course of therapy, similar to the first was administered, but with the addition of a single dose of hvdroxyldaunomycin, 50 mg iv on day 1. Shortly after the conclusion of this kherapy, the patient’s total leukocyte count declined to less than 50/mm3, and her platelet count to Z,000/mm3. She was treated with platelet transfusions, with multiple antibiotics and granulocyte transfusions for spiking fevers and with dopamine and fluids for hypotension. Staphylococcus aureus (coagulase- positive) was cultured from the blood. In spite of appropriate antibiotic therapy and maintenance of a fair blood pressure and good urine output, the patient died. Permission for autopsy was not graii ted.
MATERIALS AND METHODS
Morphologic Studies
Corivvri t ion a/ M icroscoppic S t tidias: Peripheral blood smears were stained with Wright’s stain and for acid phosphatase and tartrate-resis- tant acid phosphatase reactivity, a technique modified from that of Yam et ( ~ 1 . ~ ’ was used. (The latter was kindly performed in the laboratory of Drs. J. Vardiman and D. Variako- jis, University of Chicago Hospitals and Clinics, Chicago, Illinois.) T h e bone marrow biopsy speciniens were stained with hema- toxylin and eosin, Masson’s trichrome stain for collagen, and Gridley’s silver impregna- tion reaction for reticulin fibers. Bone marrow biopsy imprints were inadequate for evalua- tion. All other tissues were stained with hetnatoxylin and eosin and sections of spleen tissue were also stained with the Periodic Acid Schiff (PAS) reaction. In addition, tissues from the lymph nodes and from the nodule in the kidney were stained with PAS, methyl green pyronine, and naphtol AS-D chloracetate esterase reactions, and with Gridley’s silver stain. Imprints of the spleeh were stained for acid phosphatase and tartrate-resistant acid phosphatase reactivity, and with peroxidase, PAS, a-naphthyl acetate with NaF, and a-

No. 5 LRE A N D HISTIOCYTIC LYMPHOMA Adlet- et nl. 1875
FIG. 3. Photomicrograph of subcapsular area of the spleen, showing I) mphoid elements consistent with infiltration of hairy cells in the cords and sinuses (PAS, X440).
naphthyl butyrate reactions. Microscopic examination of all tissues was performed by hematopathologists at three separate institu- tions: by Dr. E. V. Pellettiere, Rush-Pres- byterian-St. Luke's Medical Center, Chicago, IL; Drs. J. Vardinian and D. Variakojis, Uni- versity of Chicago Hospitals and Clinics, Chicago, IL; and Drs. H. Rappaport and B. Nathwani, City of Hope National Medical Center, Duarte, CA. A suspension of fresh spleen cells was examined by one of us (H.G.) by phase contrast microscopy, and an im- munoperoxidase stain for intracellular im- munoglobulin by means of a peroxidase- antiperoxidase reaction" was kindly per- formed in the laboratory of Dr. H. Rappaport.
FliLore~ce,iccJ-,MicI.oJc.opic Studies: Suspensions of spleen cells were stained with fluorescein- conjugated polyvalent or monovalent (anti- IgG, IgA, IgM, Ig kappa and Ig) goat anti- human antisera (Meloy Laboratories, Spring- field, VA). Each antiserum was filtered through a 0.22 nm filter immediately before use for removal of aggregates.
Electron-MicroJcopzc~icro~copic Studies: Tissue frag-
ments from the spleen and lymph nodes were fixed in a solution of 45% paraformaldehyde o r 4% glutaraldehyde, washed in S-Colledine buffer, dehydrated in solutions of increasing concentrations of ethanol, and then ern- bedded in Epon. One micron thick sections used for orientation were stained Lvith tolu- idine blue, and selected areas were examined with a Philips 300 or a Philips 200 electron microscope. Ultrastructural studies were performed by Dr. E. V. Pellettiere and one of us (H.G.).
Studies of Hairy Cell Function Attempts were made to study the capacity
of the hairy cells to synthesize immuno- globulins; after 48 hours in culture, how- ever, the number of viable cells was insufficient for the studies. We also attempted LO study the capacity of the hairy cells to ingest latex, staphylococcus, pseudomonas, and zymosan; only the zymosan study was evaluable. In addition, the capacity of spleen cells to in- duce rosette formation of sheep erythrocytes (E-rosettes) was evaluated. These studies of

1876 CANCER May 1979 Vol. 43
FIG. 4. Electromicrograph of an area in the spleen containing t w o cells with long cytoplasmic projections (arrows); the cells have the appearance of hairy cells ( X 10.300).
hairy-cell function were performed by pre- viously reported methods.”
RESULTS
Peripheral Blood
Only a few cells had the morphologic char- acteristics of hairy cells (Fig. I ) , and rare cells reacted strongly in the acid phosphatase and acid phosphatase with tartrate reaction.
Bone Marrow
The appearance of the presplenectomy bone marrow specimen was characteristic of LRE (Fig. 2). The bone marrow specimen ob- tained four months after splenectomy con- tained no areas characteristic of LRE, but revealed scattered abnormal lymphoid ele- ments similar to those found in the first specimen.
Spleen
The prirnary spleen was firm, appeared congested, and weighed 1,325 g; its cut sur- faces were uniform except for a single 1 cm nodule; the white pulp was inconspicuous. When studied by conventional microscopy, clusters of lymphoid elements similar to those in the marrow were seen within cords and sinuses (Fig. 3) in the subcapsular areas, but there was no diffuse infiltration by hairy cells. The cells comprising the tumor nodule, how- ever, appeared to be malignant “histiocytes” and were similar to the cells comprising the patient’s lytnph nodes (Fig. 6). When examined by phase contrast microscopy, about one- third of the cells in a suspension prepared from fresh spleen tissue were found to have cytoplasmic projections.
By electron microscopy, hairy cells were identified in sections of spleen tissue (Fig. 4)

No. 5 LRE A N D HISTIOCYTIC LYMPHOMA * Adler et al. 1877
and were shown to contain ribosome lamella complexes (Fig. 5).
Cytocheinical reactivities of cells on spleen imprints on a scale of 0 (nonstaining) to + + + (intensely staining) were as follows: PAS, 0- +; peroxidase, no reactive cells were detected; (Y naphthyl butyrate, 84/100 cells were k and 16/100 were 0; (Y naphthyl acetate esterase with NaF, 38/100 cells were 4 and 62/100 were 0; naphthol AS-D chloracetate esterase, no reactive cells were detected; acid phosphatase, 67/100 cells were ++++ and 33/100 cells were 0; and acid phosphatase with tartrate, 16/100 cells were ? to + and 84/100 were 0. The hairy cells did not react with the irnmunoperoxidase stain for intra- cellular immunoglobulin.
The hairy cells from the spleen reacted
FIG. 6. Photomicrograph of a typical area in a lymph node which is infiltrated with histiocytic lymphorna cells ( H & E, x360).
with fluorescein-conjugated antisera as fol- lows (no. of positive staining cells/total no. of cells studied): Polyvalent, 10/10; IgG, 13/14; IgA, 12/12; IgM, 12/12; IgD, 12/12; lambda, 11/12; and kappa 13/13. The reactions were weak with anti-IgA and anti-IgD antisera, were strong with anti-IgM antiserum and were equal with anti-kappa and anti-A anti- sera. The following proportions of nonhairy lymphoid elements from the spleen reacted positively with the antisera: polyvalent, 2/15; IgC, 1/16; IgA, 0/15; IgD, 1/12; lambda, 1/13; and kappa, 1/14. Twenty-eight of 83 (34%) spleen cells evaluated formed E-rosettes. About one-eighth of the hairy cells from the spleen phagorytosed zymosan particles; thus, the hairy cells il l this case were of the inter-
FIG. 5. Electronmicrograph of a hairy cell in the sdeen. Two ribosomelamella comdexes (arrows) are shown ( X 17,500). mediate phagocytic type."

1878 CANCER May 1979 VOl. 43
FIG. 7 . Photomicrograph of a typical area in the liver infiltrated with lymphoid elements similar to those seen in the bone marrow and subcapsular areas of the spleen ( H & E. x360).
Lymph Nodes T h e architecture of the lymph nodes from
the greater omentum and splenic hiluin was totally effaced. T h e nodes were diffusely in- filtrated by large, oval, pleomorphic cells which had vesicular and often clefted nuclei (Fig. 6); the latter contained prominent eosinophilic nucleoli. The cytoplasmic borders of the cells were indistinct. Mitotic figures were nu- merous, and a sparse network of reticulin fibers surrounded small group of cells. T h e cells were moderately pyroninophilic with the methyl green pyronine stain, but did not react with PAS, naphthol AS-D chloracetate, or im- mu noperoxidase stains.
Liver T h e sinusoids were diffusely infiltrated by
mononuclear cells similar to those seen in the bone marrow (Fig. 7).
Right Kidney and Ureter
A solitary nodule in the right kidney was identified. There was mild hydronephrosis caused by tumor which obstructed the distal portion of the ureter. T h e histological ap- pearance of the tumor nodule in the kidney and of the tumor obstructing the ureter was similar to that of the lymphoma in the lymph nodes.
DISCUSSION
We report here on the first well-docu- mented association of a second lymphoid malignancy, most likely a ”histiocytic” lym- phoma, with LRE. A case mentioned in- cidentally by Mitus et d . 1 8 may have been the first in which such an association was recog- nized. Our case differs from the earlier one in that the two disorders were diagnosed at the same time in ours. Also, it is not known whether the patient reported by Mitus P& a/. had previously received chemotherapy or radiation therapy; our patient had not.
We cannot make any definitive statement about the relationship between the t w o neoplasms because of practical problems which prevented us from performing studies critical to the typingof the hairy cells. Further- more, we recognized that two separate malig- nancies were present when it was too late to perform special studies on the tissues con- taining the presumed “histiocytic” lymphoma which might have permitted an unequivocal diagnosis as to the type of cell involved. Nevertheless, the association of “histiocytic” lymphoma and LRE provides abundant material for speculation.
T h e sequence of events in this patient may be viewed as that of a variant of chronic lymphocytic leukemia, i . ~ . , LRE, which gave rise to a “histiocytic” lymphoma. Many studies have shown that hairy cells have char- acteristics of B lymphocytes,8~t0~13~15~zo~z4~z8~30 and the majority of histiocytic lymphomas whose cells have identifiable cell-markers seem to be B-lymphocyte neoplasms as In 1928, Richterz3 reported on a patient with apparent progression of chronic lymphocytic leukemia to a reticulum cell sarcoma. Han- son12 reported a number of such cases, but none are well documented. More recently, “histiocytic” lymphoma was found in pa- tients who had various antecedent B-cell lymphoproliferative disorders, including chronic lytnphocytic leukemia, multiple mye-

No. 5 LRE A N D HISTIOCYTIC LYMPHOMA . Adlrr d (11. 1879
l ~ m a ; ~ or Waldenstrom’s macroglobuline- mia.I6 Thus, there is substantial evidence that “histiocytic” lymphomas are, on occasion, related to prior B-cell neoplasms. It may be, as Salmon and Seligman have suggested, that a single malignant B lymphocyte transforms into a less differentiated cell resulting in a second m a l i g n a n ~ y . ~ ~
If transformation from one malignancy to another took place in our patient, w e feel that transformation of the “histiocytic” lymphoma from LRE is more likely than the reverse, for the following reasons: 1) “histiocytic” lyrn- phomas seldom have a leukemic phase and only rarely, if ever, transform to a leukemia of another cell type;’ 2) the cells of “his- tiocytic” lymphomas are probably more primi- tive than hairy cells; and 3) this patient’s “histiocytic” lymphoma progressed rapidly, even while the bone marrow invasion by LRE was improving after splenectomy.
Another possibility is that the presence of the two malignancies in this patient is merely a case of unrelated multiple primary malig- nant n e o p l a ~ m s ’ ~ * ’ ~ which occurred by chance o r was due to a defective immunosurveillance
T h e patient was anergic; we do not
know, however, whether this state antidated her malignancies. T h e fact that no well- documented case of ;I second lymphoid neo- plasm coexisting with LRE has been reported previously although hundreds of patients with this disorder are being followed closely, supports a fortuitous association o f these two malignancies. Bouroncle2 recently indicated that none of her original 26 patients, first reported t w o decades ago, had developed a second malignancy, and that there was no ap- parent transformation of L,KE t o a different disorder. Sebahoun rl d.27 also did not find a second neoplasm in 1 3 1 patients with LRE.
From the clinical standpoint. the associa- tion of these t w o disorders was catastrophic for the patient, as the leukemic disorder markedly impaired tolerance for the cytore- ductive therapy mandated by the presence of the aggressive “hist iocytic” neoplas 111. This was dramatically demonstrated by the severe and prolonged cytopenias which followed even a small dose of radiation, and by the severe granulocytopenia and throtnbocyto- penia which occurred even after a short period o f low-dose in yelosuppressive chemo- therapy.
REFEREN(:ES
1. Bloomfield. C. B.. and Brunning, R. D.: Acute leukemia as a terminal event in nonleukemic henia- topoietic disorders. S p n r n . O n r o l . 3:297-3 17, 1976.
2. Bouroncle. B. A,: Leukemic reticuloendotheliosis (“Hairy cell leukemia”) A clinical pathologic study of 82 patients and indications for splenectoniy. B h J d (Suppl.) 50: 184, 1977 (Abstract),
3. Bouroncle, B. A,, Wiseman, B. K., and Doan, C. A.: Leukemic reticuloendotheliosis. B/ood 13:609-630, 1958.
4. Brouet, J. C., Preud’Homme, J . L., Flandrin. G.. Chelloul. N., and Seligman, M.: Brief communication: Membrane markers in “histiocytic” lymphoma (reticulum cell sarcomas).,/. Nnll. Crinctr /mf. 56:63 1-633, 1976.
5. Burke, J. S., Byrne. G. E., Jr. , and Rappaport, H.: Hairy cell leukemia (leukemic reticuloendotheliosis) I . A clinical pathologic study of 21 patients. Cnnrrr 33:
6. Burnet, M.: Cancer-A biological approach. Br. Med. J. 1:779-841, 1957.
7. Catovsky. D.: Hairy Cell Leukaeinia and Pro- lymphocytic Leukaeniia. (.‘/in. Hnrnntcrl. 6:245-268. 1977.
8. Deegan, M. J., Cossinan. ,I., Chosney, B. T., and Schnitzer, B.: Hairy cell leukemia. An immunologic and ulrrastructural study. Catrrer 38: 1952- 1961, 1976.
9. Ewald. 0.: Die Leukamische Reticuloendotheliose. Deutsch. Arch. Klin. M p d . 142:222-228, 1923.
10. Golde, D. W., Saxon, A., and Stevens, R. H.: Macroglobulinemia and hairy cell leukemia. N. EngI.
11. Golomb. H. M.: Hairy cell leukemia: An unusual
1399-1410. 1974.
J. M d . 296~92-93, 1977.
lyinphoproliferative disease. A s t u d y of 24 pitielits. Cancer 42:946-956, 1978.
12. Hatisen, bl . ht.: (:hronic I)inphcicytic- 1eukcnii;i: Clinical studies based n i l 1851 G ~ S K S I’ollowed for a long time. Sroird. ,/. Hiirwnfof. (Su,?$,pl. 18) $):?Mi. I073.
, ,Jorlrs, K. A., and Wiiificld, . I . B.: a with nionoclonal IgA gammopithy.
B h d (Sufij?d.) 50: 193, I!l77 (Abstract). 14. Karchmer. R. K., Mellman, J . A,, Caldwell, C . G.,
and Chin, ‘1’. 1). I,.: Previous and simult;iiieous cancers in patients with 1eukenii;i. /. C/IJ-IJI/. Djs. 27:5- 13, 1974.
15. Leech. J., Roy. K. % I . Flexner. J. M.. (;lick. A. l)., Waltlron, J. A., slid Giillings. K. D.: Evidence for syii- thesis ol surlace ininiiinoglot)ulit~ in leukeinic rciic- uloendotheliosis. B h d ( . $ / i / @ ) 30: 109. I977 (Abst ract).
16. 1.ukes. R. J., ant1 (:iiIlins, R. I),: I in~i iunol~~gic characterization of human malignant lymphomas. Cancer 34: 1488- 1503. 1974.
17. I.ukes. R. ,I., .I‘aylor. c:. R., Parker. . I . W., 1,incoln. T. l.., Patiengale, 1’. K.. ant1 ’l~indlr, R. H.: A ntwpho- logic and immunologic surface market. s tudy of 2%) rases of non-Hodgkin I > mphonias ;ind related Iru- keniia,. ,4m. J . Pftlhol. 90:46l-486. 1978.
18. Mitus. W. , I . , hlrtlnicotf, I . B., \Vittels. B.. ;uitl Dameshek. W.: Neoplastic lymphoid rericuluiri cells i n the pel-ipheral I h o t l : A histochemical s ~ u t l y . H l ~ d 17:
19. hfoei-tel, (:. (;.: Multiple priniary inalignant iieo- plasms. (,’uirwr 40: 1786- I 792. 1977.
20. Naeiin, F.. Gatti. K. A.. and Walf’ortl. R. I . . : “H;iiry” cell leukemia with B o r 7. cell characteristics. B h i d (Suppl.) 50:201, 1977 (Absrr-acr).
206-215. 1961.

1880 C A N C E R 1979 VOl. 43
21. Pangalis, C . A,, and Rappaport. H.: Common clonal origin o f lymphoplasmacytic proliferarion and imniunoblastic Iymphonia in intestinal alpha-chain dis- ease. Lunwi 2:80. 1977 (Letter).
22. Penn, I . : Occurrence of cancer in iinmune de- ficiencies. C u w r r 34:858-866, 1974.
23. Richter, M. N.: Generalized reticular cell sar- coma of Ivniph nodes associated with lymphatic leu- kemia. Ant. /. Poihol. 4:285-292. 1928.
24. Rubin. A. D., Dnuglas. S. D., Chessin, L. N., Glatlc. P. R., and Dameshek, W.: Chronic reticulol!:inphocvtic leukemia. ‘4n1, J. , M F ~ . 47: 149- 162, 1969.
25. Salmon, S. E., antl Seligman. M.: B-cell neoplasia in man. Lmirri 2: 1230- 1253. 1974.
26. Schnitzer, B., and Kass, I..: Hairy-cell leukemia: A clinicopathologic and ultrastructui-;tl study. ,4w. ,/. c ; / i ~ . Pdhol . 61:176-187, 1974.
27. Sebahoun. G., Bouffette. P.. ;md Flandrin. G.: Hair): cell leukemia: Prognosis of a series of 131 cases. Leukrmia Rrs. 2: 187-195. 1978.
28. Sinkovics, J. G . , Wang, C. H., and Gyorkey, F.: Hairy cell5 in culture. L n ~ r i 1:749-750, 1975 (Letter).
29. .I’a):lor, C. R.: T h e nature of Reed-Sternberg cells antl other malignant “reticulum” cells. Lnrirri
90. Utsinger, P. D., Yount, W. J., Fuller, C. R.. Logue. M . J.. and Orringel, E. P.: Hairy cell leuketnia: B-lymphocyte a n d phagocytic properties. Blood 49: 19- 27. 1977.
3 1. Yam. I.. T.. I.i, <:. Y.. ;iiitl Lain. K. W.: Tartrate- resistant acid phosphatase isoenzyrne in the reticulum cells ( i f Ieukrmic reticiiloendorheliosis. A’. Engl. J . M o d 284:357-360, 1971.
2:802-807. 3974.


























![Title [原著]An Autopsy Case of Histiocytic Medullary ...okinawa-repo.lib.u-ryukyu.ac.jp/bitstream/20.500.12001/...The findings of this case were those of histiocytic medullary reticulosis,](https://img.pdfslide.net/doc/110x75/610486836382170066209593/title-ean-autopsy-case-of-histiocytic-medullary-okinawa-repolibu-.jpg)