Embed Size (px)
Citation preview

COI Disclosure for Dr. Montalescot: Research Grants to the Institution or Consulting/Lecture Fees from Abbott Vascular, Astra-Zeneca, Bayer, Biotronik, Boehringer-Ingelheim, Boston Scientific, Cleveland Clinic Foundation, Cardiovascular Research Foundation, Cordis, Daiichi-Sankyo, Duke institute, Eli-Lilly, Europa, Fédération Française de Cardiologie, Fondation de France, GSK, ICM, INSERM, Medtronic, Menarini, Nanospheres, Novartis, Pfizer, Sanofi-Aventis Group, Servier, Société Française de Cardiologie, The Medicines Company, TIMI group.
Aldosterone Lethal effects Blockade in Acute myocardial infarction Treated with or
without Reperfusion to improve Outcome and Survival at Six months follow-up
F. Beygui, G. Cayla, V. Roule, F. Roubille, N. Delarche, J. Silvain, E. Van Belle, L. Belle, M. Galinier, P. Motreff, L. Cornillet, JP Collet, A. Furber, P.
Goldstein, P. Ecollan, D. Legallois, A. Lebon, H. Rousseau, J. Machecourt, F. Zannad, E. Vicaut, G. Montalescot
on behalf of the ALBATROSS investigators

Years
Tertile 3Tertile 3
Tertile 1Tertile 1
Death according to tertiles of aldosterone in MI
Log rank P = 0.005
Cu
mu
lati
ve S
urv
ival
Rat
e, %
Beygui F, et al. Circulation. 2006;114:2604-2610.
70
75
80
85
90
95
100
1 11 21 31 41 51 61 71 81 91 101 111 121 131 141 151 161 171 181
Days
Quartile 1Quartile 2Quartile 3Quartile 4
Log rank P = 0.005
Cu
mu
lati
ve S
urv
ival
Rat
e, %
Beygui F, et al. Circulation. 2006;114:2604-2610.
70
75
80
85
90
95
100
1 11 21 31 41 51 61 71 81 91 101 111 121 131 141 151 161 171 181
Days
Quartile 1Quartile 2Quartile 3Quartile 4
Death according to quartiles of aldosterone in STEMI
Palmer B, et al. Eur Heart J. 2008; 29:2489-96Beygui F, et al. Circulation 2006; 114:2604-10
Aldosterone levels and death in AMI
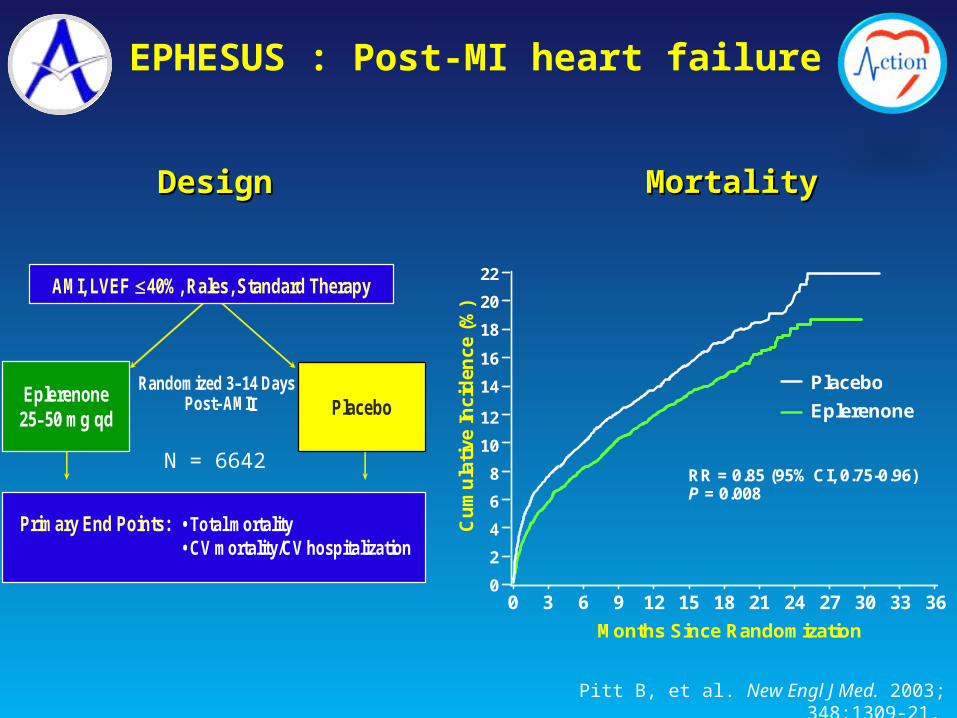
EPHESUS : Post-MI heart failure
Months Since Randomization
Cu
mu
lati
ve I
nci
den
ce (
%)
22
0
2
20
16
18
14
12
10
8
6
4
RR = 0.85 (95% CI, 0.75-0.96) P = 0.008
Placebo
Eplerenone
3633302724211815129630
MortalityMortalityDesignDesign
Primary End Points: • Total mortality• CV mortality/CV hospitalization
PlaceboRandomized 3–14 Days
Post–AMIEplerenone 25–50 mg qd
AMI, LVEF 40%, Rales, Standard Therapy
I
Pitt B, et al. New Engl J Med. 2003; 348:1309-21.
N = 6642

ALBATROSS study designALBATROSS study design
1° End Point: death, resuscitated cardiac death, VF/VT, indication for defibrillator, heart failure
up to 6-month FU
controlRandomizedOpen label
N=1600
AMI (ST+ or ST-) in the first 72hrs
clinicaltrials.gov registration number NCT 01059136 ALBATROSS study protocol - Beygui et al. Am Heart J 2010
iv K+ canrenoate* then
spironolactone**
* Soludactone 200mg
** Aldactone 25mg od
Aldosterone blockade

Standard treatment(N=801)
MRA regimen(N=802)
Age (median) 58 58
Current smoking (%) 52 47
Diabetes (%) 16 16
Hypertension (%) 44 42
Dyslipidemia (%) 46 47
Prior MI (%) 9 8
Prior HF (%) 1 1
STEMI (n) 617 612
NSTEMI (n) 183 186
Killip I (%) 91 93
PCI (%) 81 82
LV ejection fraction (median in %) 50 50
Baseline characteristics

HR = 0,97 [0,73-1,28]p= 0. 81
Pri
mary
end p
oin
t
N at risks
Standard Therapy 801 687 669 645 273
MRA Regimen 802 705 683 660 183
Follow-up (days)
In CYP2C19 Extensive &
Standard TherapyMRA regimen
HR = 0,97 [0,73-1,28]p= 0. 81
Pri
mary
end p
oin
t
N at risks
Standard Therapy 801 687 669 645 273
MRA Regimen 802 705 683 660 183
Follow-up (days)
In CYP2C19 Extensive &
Standard TherapyMRA regimen
Primary End PointDeath, resuscitated death, VF/VT, indication for ICD or heart failure
MRA: Mineralocorticoid Receptor Antagonist; VF: Ventricular Fibrillation; VT: Ventricular Tachycardia; ICD: Implantable Cardioverter Defibrillator

Standard therapy(n=801)
MRA regimen (n=802)
P value
Significant ventricular arrhythmia (%) 6 5.6 0.75
New or worsening heart failure (%) 5.6 5.9 0.85
Recurrent myocardial infarction (%) 1 0.6 0.39
Death or resuscitated cardiac arrest (%) 2.4 1.6 0.28
Secondary End Points
Hyperkalemia > 5.5mmol.L-1 (%) 0.2 3 <0.0001

Death in pre-specified subgroups

HR = 0,20 [0,06-0,69]p= 0. 0044
Death
N at risks
Standard Therapy 617 587 579 556 236
MRA Regimen 612 595 587 571 162
Follow-up (days)
In e &
Standard TherapyMRA regimen
Death in STEMI patients (n=1229)

1. Despite a strong pre-clinical rationale and favorable clinical data from registries and small randomized studies, the he ALBATROSS trial failed to show a benefit of aldosterone ALBATROSS trial failed to show a benefit of aldosterone blockade initiated early in MI, when heart failure is in blockade initiated early in MI, when heart failure is in general general notnot present present
2. The ALBATROSS study highlights the relative safety of the aldosterone blockade aldosterone blockade used in the study
3.3. Our finding of a mortality reduction associated with early Our finding of a mortality reduction associated with early aldosterone blockade in aldosterone blockade in STEMISTEMI patients needs confirmation patients needs confirmation in future studies specifically dedicated to these patientsin future studies specifically dedicated to these patients
4.4. Meanwhile, the results of the ALBATROSS study do not Meanwhile, the results of the ALBATROSS study do not warrant the extension of aldosterone blockade to MI warrant the extension of aldosterone blockade to MI patients without heart failure.patients without heart failure.





























