Embed Size (px)
Citation preview

“Cold Case – a Hot Topic”
Dr. Bridget Freyne Infectious Disease Fellow
Royal Children’s Hospital Melbourne
Melbourne Infectious Disease Group Meeting 28/04/2015

Case
20 month old boy
Presentation 3 week history of limp Left knee pain Worse in the mornings Some response to paracetamol and ibuprofen Unwitnessed trauma reported by 4-year old brother Intermittent fevers - 5/6 episodes
Birth history NVD at term
Past Medical History Mild seborrheic dermatitis

Case Immunisations
In line with schedule up to 18 months
Hep A and BCG at 14 months of age for travel to India
Family history No unwell contacts
No history of rheumatological disorders, immune deficiency
Social history Parents from Punjab, non-consanguineous
1 older brother
Suburban Melbourne
No pets
Case Examination
General Height and weight 30th centile
Well nourished
Developmentally appropriate
Well healed BCG scar
Normal tonsillar tissue
No cervical or peripheral adenopathy
No hepatosplenomegaly
Chest clear
Musculoskeletal Mobilising but limping
Tender and swollen over left proximal tibial tuberosity
Investigations Hb 121, Plts 321
WCC 10.8 (N 4.32, L 6.05)
U&E / LFTs -> Normal
CRP < 5 ESR 18
BC no growth

Case Differential diagnosis
Sub-acute bacterial osteomyelitis
TB osteomyelitis
(Septic arthritis)
Plan Imaging +/- surgical washout
Start Flucloxacillin 50 mg/kg iv 6H post op
QFT-IT
TST (Mantoux)
Requested ZN stain, mycobacterial culture and TB PCR on operative samples

There is an aggressive looking lesion involving the proximal metaphysis and epiphysis of the tibia. It is predominantly lucent with internal trabeculations noted in the epiphyseal component. The metaphyseal component is poorly defined with a wide zone of transition.

There is laminar periosteal reaction extending down the tibia. The features of this lesion are more consistent with infection, however malignancy cannot be excluded. MRI is recommended.
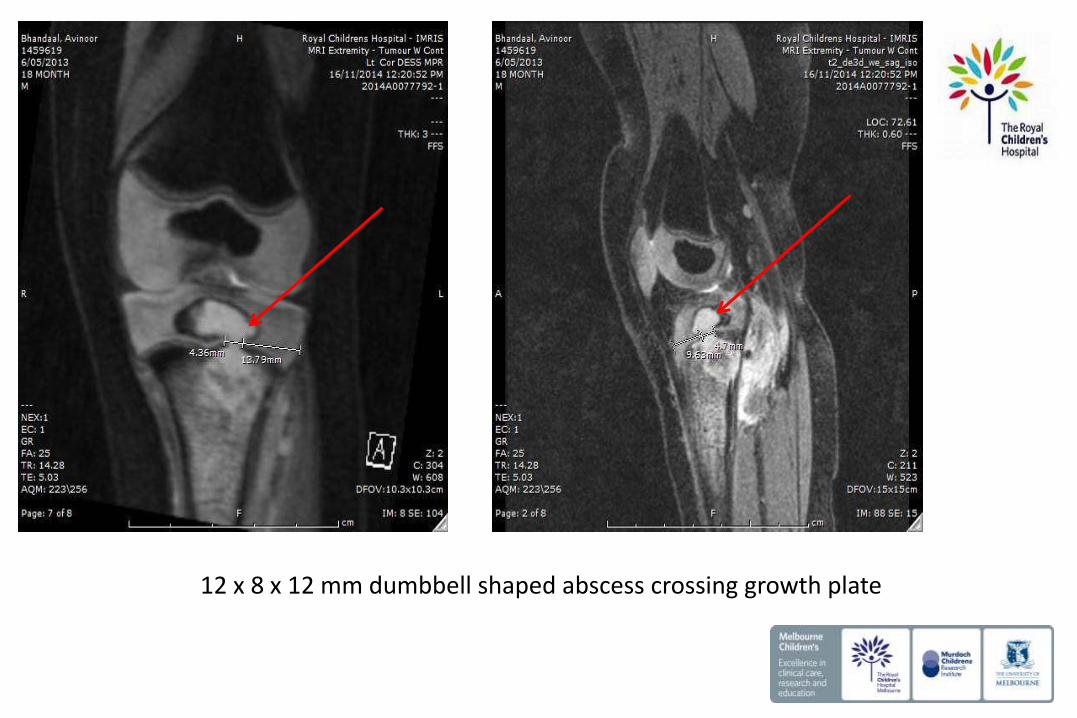
12 x 8 x 12 mm dumbbell shaped abscess crossing growth plate

Breach of posterior cortex and non-enhancing area in popliteal fossa ? Extruded sequestrum

Popliteal lymph nodes

Case
Intraoperative findings Osteotomy to anterior tibia
No pus under pressure
Extensive curettage of pale bony fragments
No need for prolonged drainage
Do these imaging & intraoperative findings suggest anything in particular?

Cold abscess pathology and imaging
Cold abscess -> purulent collection with no associated heat or erythema
• Formed by collection of products of liquefaction and reactive exudation
• Migrates in multiple directions along path of least resistance
Tuberculosis Actinomycosis Sporotrichosis Blastomycosis Coccidomycoses Chromomycoses Trichophyton rubrum Protothecosis Bacterial abscess in 1ry immunodeficiency

Case
QFT-IT
TB specific antigens (ESAT-6, FCP10 & TB7.7) 0.01 IU/mL
Mitogen control (PHA) 1.91 IU/mL
Nil control 0.02 IU/mL

Case
QFT-IT
TB specific antigens (ESAT-6, FCP10 & TB7.7) 0.01 IU/mL
Mitogen control (PHA) 1.91 IU/mL
Nil control 0.02 IU/mL
(Mantoux TST cancelled)
Histopathology
Necrotising and suppurative granulomatous osteomyelitis
AFB not seen on Ziehl-Neelsen stain
Gene-Xpert TB PCR positive

Case
Commenced therapy 3 drugs
Isoniazid 10 mg/kg od Rifampicin 15 mg/kg od Pyrazinamide 35 mg/kg od
Major problems with adherence
Personal telephone support hotline Close OPD follow up Admitted for DOTS Play therapy for patient Psychology referral for mother

Case
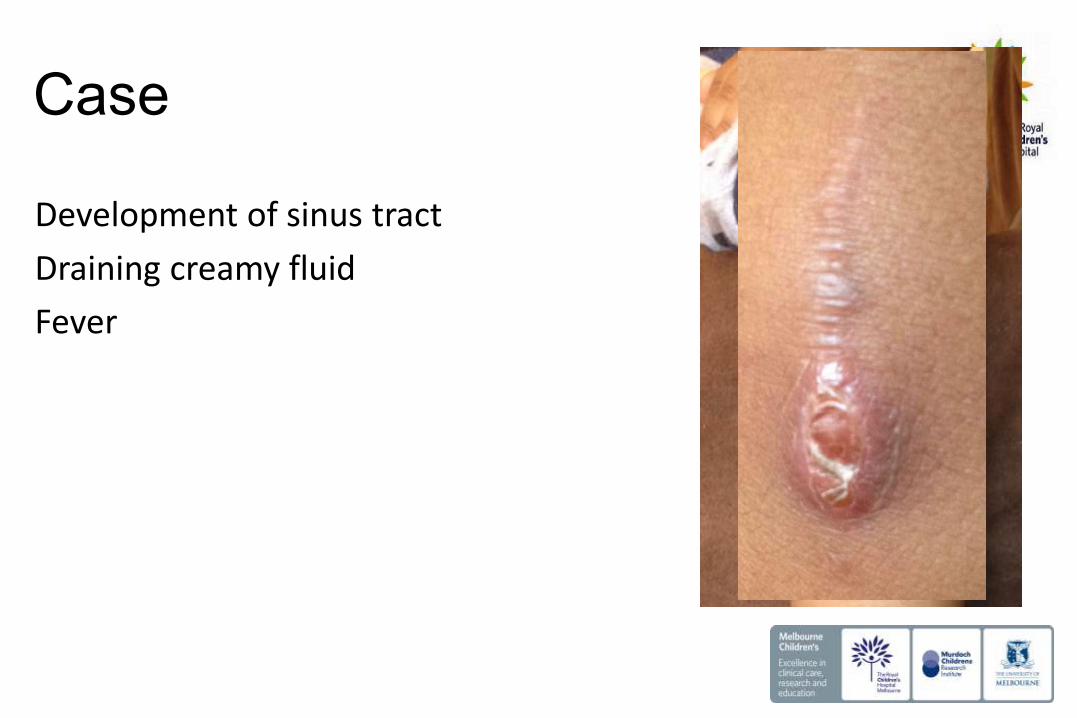
Development of sinus tract
Draining creamy fluid
Fever
Case
Development of sinus tract
Draining creamy fluid
Fever

Case
Development of sinus tract
Draining creamy fluid
Fever

Discussion
1. Molecular diagnosis of TB in children
2. BCG vaccination in Australia
3. BCG osteomyelitis & osteitis
4. BCG-itis and immuodeficiency

TB PCR diagnostics – the MTB complex
• Distinguish by fixed deletions and SNPs • Distribution of deletions provides
insights into evolution of MTB • Primarily animal adapted species
identified by deletion of RD9 • Primary hosts vs Maintenance hosts
vs Spillover hosts
Smith et al. Nature Reviews Immunology 2009 “Myths and Misconceptions on the evolution of MTB”
8 species of mycobacterium 99.95% sequence similarity at nucleotide level
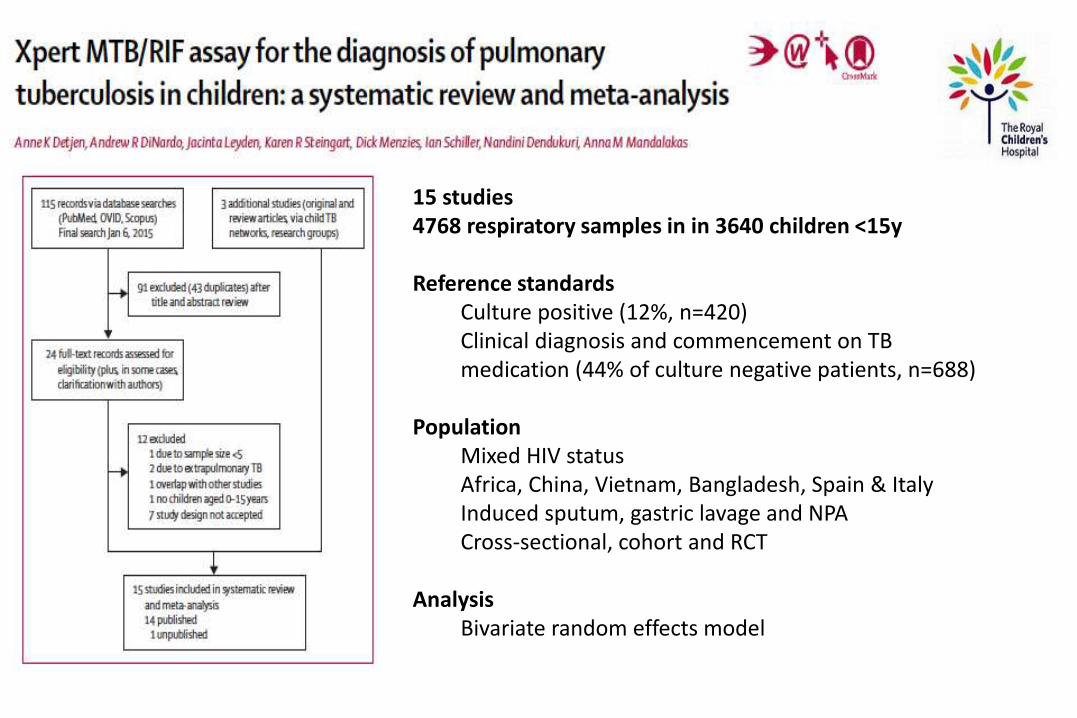
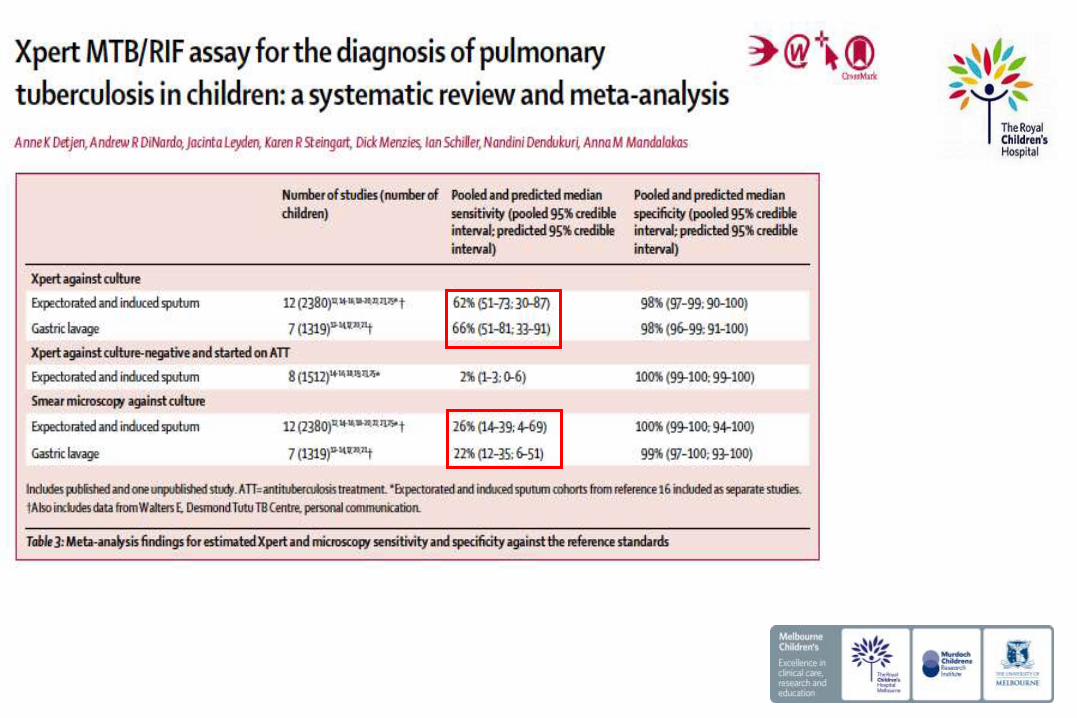
15 studies 4768 respiratory samples in in 3640 children <15y Reference standards
Culture positive (12%, n=420) Clinical diagnosis and commencement on TB medication (44% of culture negative patients, n=688)
Population
Mixed HIV status Africa, China, Vietnam, Bangladesh, Spain & Italy Induced sputum, gastric lavage and NPA Cross-sectional, cohort and RCT
Analysis
Bivariate random effects model

Compared to culture Variety in sensitivities by specimen type
Induced Sputum
Specificity 93-100% Sensitivity 25-100%

Compared to culture Variety in sensitivities by specimen type
Gastric fluid
Specificity 93-100% Sensitivity 40-100%

Compared to culture Variety in sensitivities by specimen type
Nasopharyngeal aspirate
Specificity 99-100% Sensitivity 33-40%


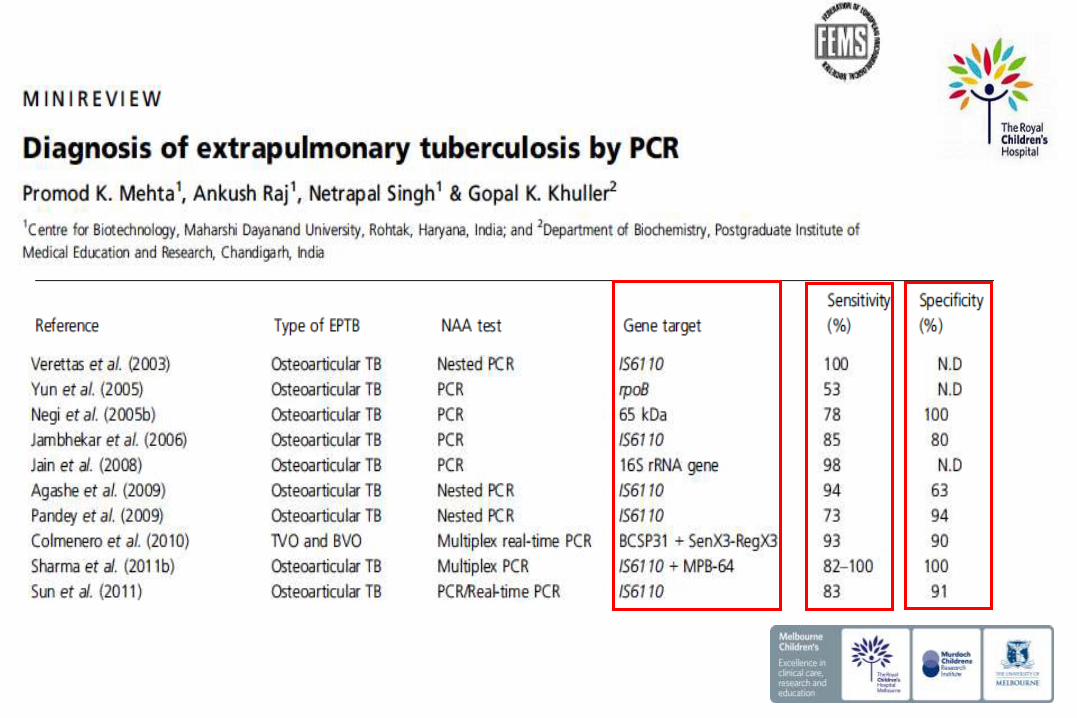
DNA PCR (Nested or Multiplex)
Reverse Transcriptase PCR
RT-PCR
mRNA Viable bacteria
Quantification Automation
Non-viable bacteria
Proposed gold standards • Culture on solid and liquid media • BACTEC • Histopathology • Response to TB therapy

Gene Target
IS6110 MTBC, M. smegmatis
65kDa (Rv0440) MTBC
MPB-64/MBT-64 (Rv1980c) MTBC
38kDa (Rv0934) MTBC, M. leprae
Conserved repetitive element (TRC4) MTBC
Guanine-cytosine rich repetitive sequence (GCRS) MTBC, MAC
devR (Rv3133c) MTBC, M. leprae, M. canetti
HupB (Rv2986c) Candidate for differentiation

Gene Target
IS6110 MTBC, M. smegmatis
65kDa (Rv0440) MTBC
MPB-64/MBT-64 (Rv1980c) MTBC
38kDa (Rv0934) MTBC, M. leprae
Conserved repetitive element (TRC4) MTBC
Guanine-cytosine rich repetitive sequence (GCRS) MTBC, MAC
devR (Rv3133c) MTBC, M. leprae, M. canetti
HupB (Rv2986c) Candidate for differentiation
Commercially available
Roche Amplicor (16srRNA) Genprobe MTB direct (16srRNA)
Roche COBAS Taqman (RT-PCR IS6110/MB64) Gene/Xpert (Nested PCR for rpoB gene)



Discussion
1. Molecular diagnosis of TB in children
2. BCG vaccination in Australia
3. BCG osteomyelitis & osteitis
4. BCG-itis and immuodeficiency

BCG Down Under
BCG vaccine is only recommended for:
• all ATSI born in parts of QLD/NT
• parents have TB or leprosy (or who have been treated for leprosy in the past)
• <5 yr old travellers to countries where TB is common
• <16 yr old who live with, or are exposed to, someone with TB, or from a country where TB is present
• healthcare workers who may come into contact with people with TB


172/195 (88%)

Proposed causes of variable efficacy Host genetic factors
Environmental factors Age and route of administration
Vaccine strain
Prior BCG vaccination does not out rule diagnosis of TB

Calmette & Guerin passaged BCG for 13 years on potato slices imbibed with glycerol On loss of virulence -> dissemination -> individual laboratory passages -> 1960s “seed lots” Comparative genomics of vaccine strains Regions of difference (RDs) SNPs Tandem duplications (DU I-IV) in response to selective pressure -> enzymes of glycerol metabolism

BCG Denmark (10 million) BCG Japan (20 million) BCG Russia (85 million)


Effectiveness Clinical Culture BCG-Japan 69% 92% BCG-Serbia 43% 82% BCG-Russia 22% 51% No BCG

Osteitis & osteomyelitis
Rare but most frequent in Scandinavia & Eastern Europe Typically associated with changes to BCG strain
1998 Czechoslovakia switch from Prague -> Russia (35/1,000,000) 1971 Sweden switch from Pasteur -> Gothenburg (1/3,000) Decline after change to Denmark 1331 2012 WHO report “Infrequent” (1/3,333 – 1/108)
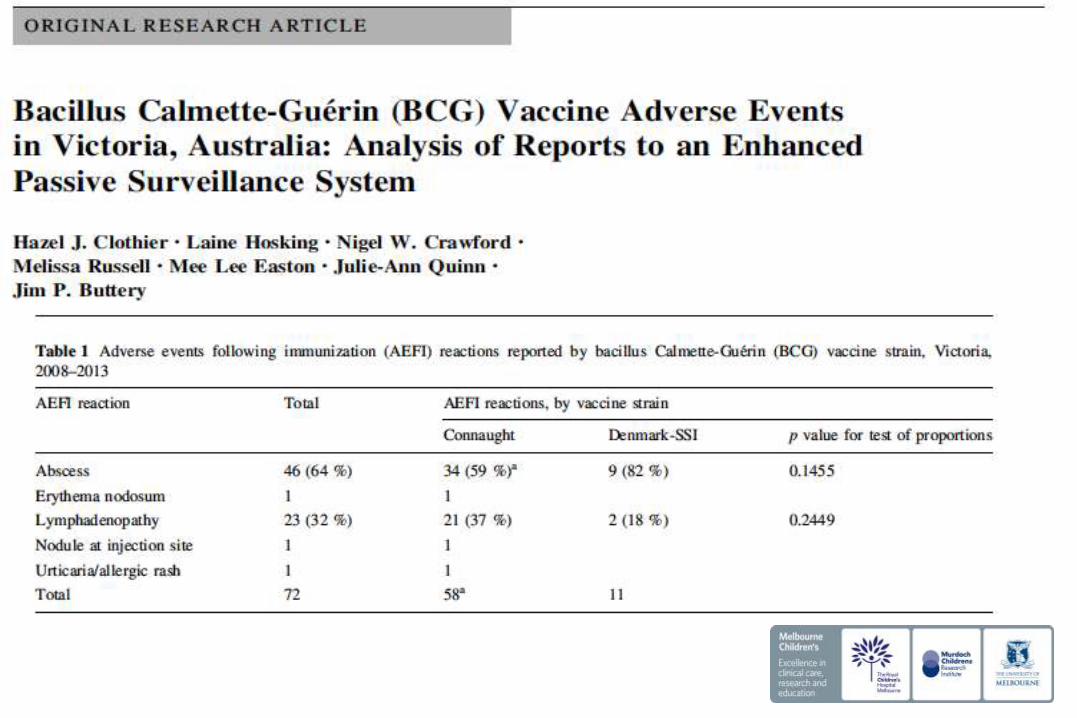
General coplication from Jim’s paper
Discussion
1. Molecular diagnosis of TB in children
2. BCG vaccination in Australia
3. BCG osteomyelitis & osteitis
4. BCG-itis and immuodeficiency
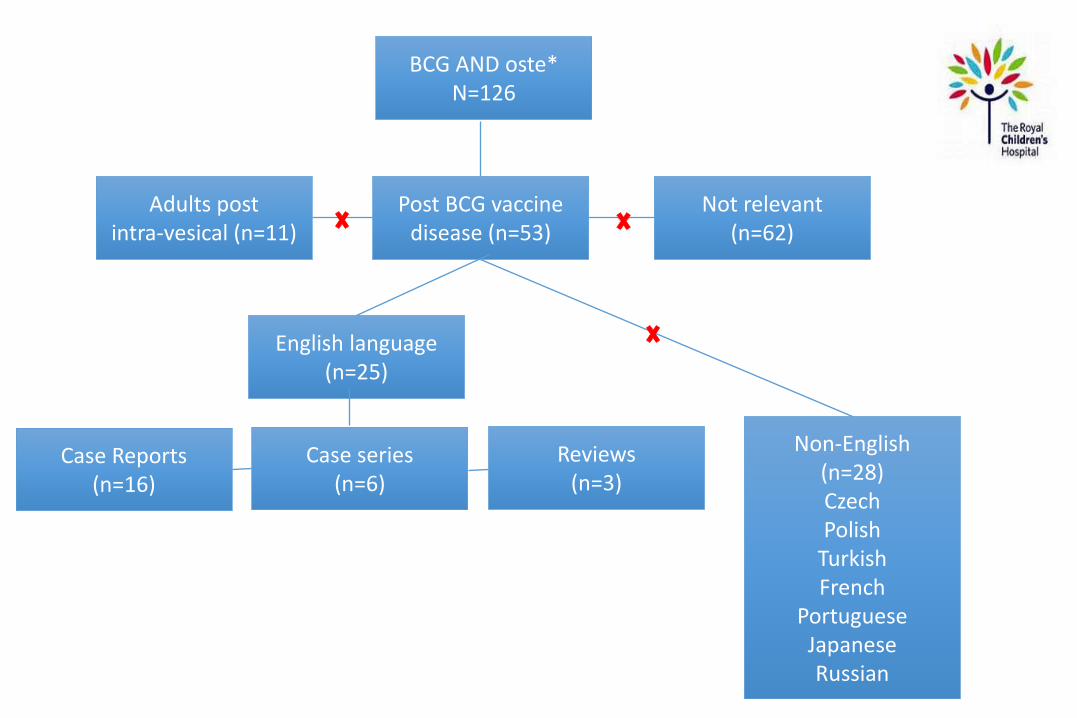
Not relevant (n=62)
Post BCG vaccine disease (n=53)
Adults post intra-vesical (n=11)
English language (n=25)
Reviews (n=3)
Case series (n=6)
Case Reports (n=16)
Non-English (n=28) Czech Polish
Turkish French
Portuguese Japanese Russian
BCG AND oste* N=126

Onset 3 months – 5 years post vaccine (average 18 months)
Location Long bone metaphysis Femur 27%, Tibia 19% Humerus 11% Sternum 15% Ribs 11% Case reports: skull, foot and clavicle
Minimal systemic symptoms
Diagnostic Criteria 1971: Foucard & Hjelmsted
BCG vaccination in the neonatal period
Radiology consistent with osteitis No known TB contact
At least 1 of compatible histopathology, ZN stain pos or culture

QFT-IT negative and PPD positive (89%)
ESR (mean 34)
Histopathology Granulomatous inflammation with epitheiloid cells
Caseous necrosis (92%)
AFB positive (45%)
Culture positive (56%)

Management Issues with medical treatment
Pyrazinamide resistance (PTNA deletion)
Variable isoniazid resistance (0.1 ug/L vs 0.4 ug/L)
Role of surgery
Duration
Underlying immune deficiency
Clinical and Radiological resoultion
Report (cases) Regimen Duration Outcome
Finland (222) 1960-1988
Streptomycin 1/12 + INH + Ethionamide Streptomycin 1/12 + INH + Rifampicin INH + Ethionamide + Rifampicin
12 months 97% resolution 4 cases growth disturbance
Denmark (18) 1961-74
Streptomycin 1/12 + INH + Rifampicin
6 months Full resolution


Phone a friend Ethambutol Moxifloxacin Isoniazid Rifampicin Isoniazid Rifampicin
2 months
10 months

Discussion
1. Molecular diagnosis of TB in children
2. BCG vaccination in Australia
3. BCG osteomyelitis & osteitis
4. BCG-itis and immuodeficiency

Conditions increasing susceptibility to BCG infection
Mendelian susceptibility to mycobacterial sisease Primary immune deficiency Acquired
HIV Post BMT
SCID CGD
EDA-ID XR CD40L deficiency AR STAT1 deficiency AR IRF8 deficiency AR TYK2 deficiency
IFN-gR deficiencies AD STAT1 deficiency
XR gp91 phox deficiency AD IRF8 deficiency
XR Nemo deficiency IL-12 & IL12R deficiencies
AR IS GI5 deficiency

Non – infectious phenotype Ectodermal dysplasia (EDA-ID) Family history Consanguinity Infectious phenotype Disseminated NTM disease Systemic features History of past infections Mucocutaneous candidiasis FBE characteristics Total lymphocyte counts Blood dyscrasias Baseline immunological investigations HIV 1/2 antibody Immune globulins T cell subsets Oxidative burst test CD62L (L-selectin shedding)

Conditions increasing susceptibility to BCG infection
Mendelian susceptibility to mycobacterial sisease Primary immune deficiency Acquired
HIV Post BMT
SCID CGD
EDA-ID XR CD40L deficiency AR STAT1 deficiency AR IRF8 deficiency AR TYK2 deficiency
IFN-gR deficiencies AD STAT1 deficiency
XR gp91 phox deficiency AD IRF8 deficiency
XR Nemo deficiency IL-12 & IL12R deficiencies
AR IS GI5 deficiency
Following history, examination, FBE and baseline immunology
tests

Conditions increasing susceptibility to BCG infection
Mendelian Susceptibility to Mycobacterial Disease Primary Immune deficiency Acquired
HIV Post BMT
SCID CGD
EDA-ID XR CD40L deficiency AR STAT1 deficiency AR IRF8 deficiency AR TYK2 deficiency
IFN-gR deficiencies AD STAT1 deficiency
XR gp91 phox deficiency AD IRF8 deficiency
XR Nemo deificiency IL-12 & IL12R deficiencies
AR IS GI5 deficiency
Following history, examination, FBE and baseline immunology
tests

Conditions increasing susceptibility to BCG infection
Mendelian Susceptibility to Mycobacterial Disease Primary Immune deficiency Acquired
HIV Post BMT
SCID CGD
EDA-ID XR CD40L deficiency AR STAT1 deficiency AR IRF8 deficiency AR TYK2 deficiency
IFN-gR deficiencies AD STAT1 deficiency
XR gp91 phox deficiency AD IRF8 deficiency
XR Nemo deificiency IL-12 & IL12R deficiencies
AR IS GI5 deficiency
Following history, examination, FBE and baseline immunology
tests

MSMD First reported in Maltese kindred 1996
Genetic defects in the interferon gamma (IFN-γ) - (IL-12) pathway
AD / AR / XR
Clinical presentation can be non-specific -> life-threatening
Unifocal NTM OM
IFNgR deficiencies
AD STAT1 deficiency
IL12 & IL12R deficiencies

Evaluation of IFN-gamma – IL12 pathway (RCH)
Royal Children’s Hospital Melbourne
Whole blood & PBMC
Set up on a Tuesday with blood from a healthy control
Method Incubate with PHA +/- IL-12 and the level measure IFN-gamma (Day 3)
Incubate with LPS +/- IFN-gamma and measure TNF-alpha & IL-12p70 (Day 1)
Westmead Immunology Laboratory
Flow cytometry IFN-gamma receptor, IL-12 receptor, Phospho-Stat 1 and Phospho-Stat 4
Gene sequencing for confirmation of suspected defects
Slides and information adapted from Sheree Poulton and Rashelle Farah, RCH Immunology Scientists

Conditions increasing susceptibility to BCG infection
Mendelian susceptibility to mycobacterial disease Primary immune deficiency Acquired
HIV Post BMT
SCID CGD
EDA-ID XR CD40L deficiency AR STAT1 deficiency AR IRF8 deficiency AR TYK2 deficiency
IFN-gR deficiencies AD STAT1 deficiency
XR gp91 phox deficiency AD IRF8 deficiency
XR Nemo deificiency IL-12 & IL12R deficiencies
AR IS GI5 deficiency
Following IFN-gamma / IL12 pathway assay

TB PCR results need to be interpreted as MTB Complex positivity
Variable sensitivity depending on age, disease location and smear
BCG vaccine is safe and effective
Complication of osteomyelitis/osteitis is rare
Epiphyseal disease associated with worse outcome and warrants conservative approach to treatment duration
Evaluate for HIV, Primary immunodeficiency and MSMD
Conclusions





























