Embed Size (px)
Citation preview
Collaboration & Quality Improvement “It Takes A Village”
South East Michigan Quality Forum
Health Trends Conference
January 24, 2003John E. Billi, M.D.
Associate Dean, Clinical Affairs
Associate Vice President, Medical Affairs
University of Michigan
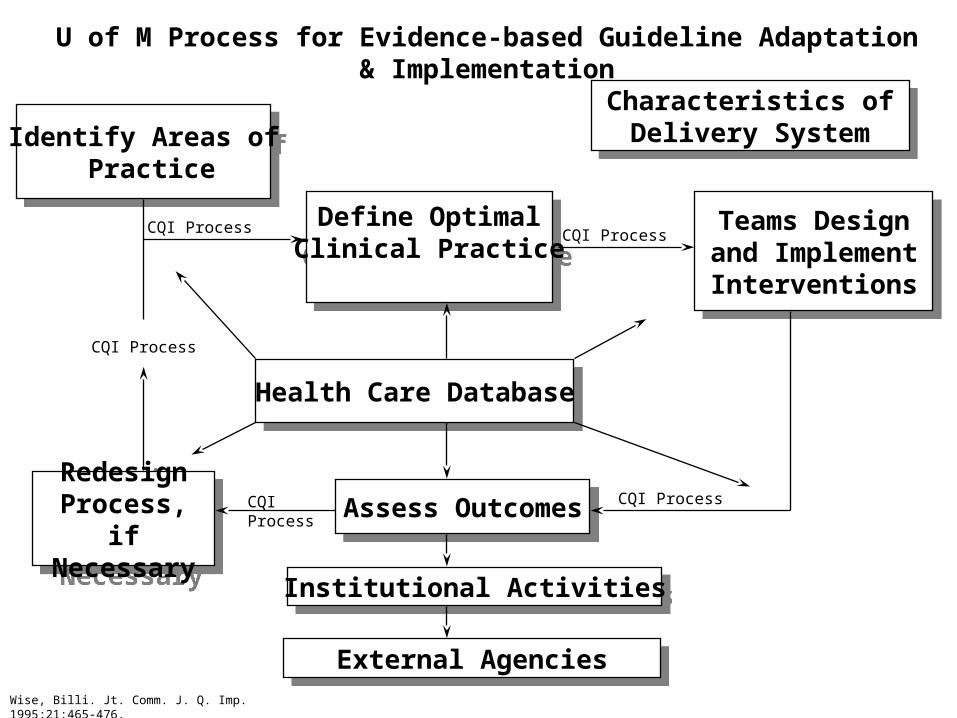
Identify Areas of Practice
Identify Areas of Practice
U of M Process for Evidence-based Guideline Adaptation & Implementation
Define OptimalClinical Practice
Define OptimalClinical Practice
Teams Design and Implement
Interventions
Teams Design and Implement
Interventions
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal AgenciesWise, Billi. Jt. Comm. J. Q. Imp. 1995;21:465-476.
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Southeast Michigan Health Care Quality Forum
• Mission: To improve the quality of health care services provided to SEM residents, with primary emphasis upon promoting the scientific practice of medicine.
• Operated under the auspices of GDAHC• Established to bring together physician leaders, health
systems, health plans, business, labor to work collaboratively on quality improvement.
• Overall approach: – Start with existing, evidence-based, widely accepted,
credible practice guidelines. – Focus upon collaborative, value-added strategies to
increase use of guidelines at the point of care.
SEM Quality Forum
• Roles– Serve as locus of coordination, collaboration for QI
projects/activities within SEM.– Conduct community-wide QI initiatives.– Support efforts of other entities to promote use of
guidelines, evidence-based medicine.– Promote sharing of quality improvement strategies and
experiences.– Serve as a liaison between SEM QI activity and state,
national-level QI efforts.
SEM Quality Forum
• Membership
– 6 SEM health systems and physician leaders
– 3 auto companies
– UAW
– BCBSM
– MPRO
• Other organizations can join!
Southeast Michigan Quality Forum- Specifics• Who
– GM, Ford, Daimler-Chrysler, UAW, GDAHC, MPRO– UM, St John, Oakwood, Trinity, Henry Ford, DMC
• What – Coordinated, community-wide quality improvement
efforts• Pharmacy (antibiotics, generics, dose optimization)• Coronary disease (GAP)• Diabetes (coordinated physician interventions)
• Coordinate implementation of MQIC Guidelineshttp://www.gdahc.org/deliv.htm
ACC AMI GAP Projects: Southeast MI(Guidelines Applied in Practice)
• National pilot project, including 10 SEM hospitals; followed by SEM expansion project, with 18 additional SEM hospitals.
• Hypothesis: quality of inpatient AMI care can be improved through a performance improvement initiative that uses QI tools, emphasizes key targets of care and focuses on improving key processes of care.
• Partnership among American College of Cardiology, MPRO, GDAHC/Quality Forum and participating hospitals/physicians.
• Use of well-defined performance measures – ASA; beta blockers; cholesterol management, tobacco cessation…
ACC AMI GAP Project• Methods – a variety of interventions:
– the partnership– opinion leaders and physician champions– ACC AMI tool kit (order sets, posters…)– rapid cycle timeline measurement and analysis– collaborative model w/ learning sessions
• Both projects were 12 months duration• Results
– Performance on “early-in-stay” indicators shows substantial improvement when AMI/ACC standing order sets are used
– Performance on “at discharge” indicators shows substantial improvement when AMI discharge tool is used.
Drucker’s Three Questions and the Forum• Who are our customers?
– Patients, employers, physicians, health systems, health plans
• What do our customers find of value?– Improved quality, cost, access– Reduced administrative hassle and conflicting initiatives
• What are we uniquely qualified to provide that our customers find of value?– Coordination of quality improvement activities– Sharing of what works and what doesn’t– Elimination of barriers – dueling guidelines, measurements,
profiles, interventions
Benefits of Cooperation for the Physician and Health System
• Avoid the “Disease of the Month” problem• Eliminate
– conflicting guidelines (differences are not evidence based)– conflicting measures (A1C: 2x or 4x a year?)– conflicting measurement method (chart or claims?)– conflicting measurement process (If this is Tuesday, you
must be from HAP)– conflicting profiles (I’m a good BCN doctor, but a poor
MCARE doctor) – conflicting interventions (MPRO, MCARE, MHA, MAHP,
U of M)
Benefits of Cooperation for the Health Plans
• Gain synergy of their participating physicians receiving a consistent QI message from multiple sources
– Demonstrates respect for physician’s perspective, time and challenges
• Eventually reduce or eliminate costs, work and noise – Investment in development/maintenance of guidelines
– Cost of measuring each physician (doctors are multi-plan)
– Variability due to small numbers of members per doctor
– Better chance for external funding
Benefits of Cooperation for the Employers and Government Payers
• Higher probability of improving quality, cost and value
• Eventually reduce administrative costs
– Improved health plan efficiency lowers costs
• Allows a forum for redesigning the organization and financing of care across employers, payers, and providers
– New incentive alignment models – fee for benefit – performance-based contracting – need all at the table.
Barriers to Cooperation• Stuck in the half-way point to integration• Health Plans compete – invested $$ in guidelines, QI• Health Plans worried about HEDIS rules and NCQA credit• Lack of office systems in many doctors’ offices• Lack of a community health info system (CHIN)• Lack of a trusted intermediary to house data• HIPAA- confidentiality – physician, patient, plan• Lack of sources of funding or staff help for reengineering care process at the point
of care, in the doctor’s office – “no business case for quality”• “Measure to judge” - provider skeptical of use/release• Issues of risk adjustment• ACCME resists giving CME credit for QI!!!• Patient expectations, direct-to-consumer ads• Impatience
University of Michigan Efforts
• SE Michigan Quality Forum• Michigan Quality Improvement Consortium• Michigan Patient Safety Coalition• Patient Safety Conference, Toolkit, Workshops• MSMS Medical Economics and Quality• Medicare Carrier Advisory Committee• Evidence-based guidelines on the web
There’s plenty to do…but there’s plenty of help!
END
Traditional Care Episodic, uncoordinatedEpisodic, uncoordinated Focused on the acutely illFocused on the acutely ill Patient initiatedPatient initiated Patient education is sporadicPatient education is sporadic Communication among clinicians is sporadicCommunication among clinicians is sporadic
- Information scattered on paperInformation scattered on paper Process of care is variable Clinicians’ Clinicians’ opinionsopinions drive decisions drive decisions ExpensiveExpensive
Next Model of Health Care• Coordinated care• Integrated delivery systems• Population-based
– Outreach initiated by plan/physicians– Incorporates prevention and patient education
• Communication among providers & patients– Facilitated by information technology
• Standardized, evidence-based process– Guidelines, pathways, disease management
• Performance-based contracting– Clinical outcomes– Cost
“Crossing the Quality Chasm”
Health care should be: Safe Effective Patient-centered Timely Efficient Equitable - not vary due to gender, ethnicity,
geography, socioeconomic status
Source: Crossing the Quality Chasm: A New Health System for the 21st Century, Institute of Medicine, National Academy of Sciences, 2000.
The Coming Train Wreck...• Aging, growing population
• Dramatic advances in clinical capabilities
• Information technology requirements
• 40 million uninsured
• Unbounded patient demands vs. Taxpayer, employer, individual
willingness to pay
MQIC Intervention Strategies
• Public Education– Tools: public service announcements, pamphlets
• Physician Education– Tools: tool kit for physicians, patient handouts, MPRO
• Data Collection and Feedback– Tools: data collected by health plans, physician groups
Professional Values - Enduring• Altruism
– patients’ interests come first
• Commitment to self-improvement– master and incorporate new knowledge– contribute to the knowledge base of the
discipline
• Peer review– collective sense of responsibility and
accountability among medical professionals for the conduct of colleagues
Source: D Blumenthal, Health Affairs, Spring (I) 1994
Integrated Delivery Systems
• Organized system of care• Integrates:
– Providers (doctors, nurses, …)– Facilities (tertiary and community hospitals, nursing homes,…) – (Health plan)
• Full spectrum of services• Geographic coverage• Economically viable scale (contracting clout)• Ultimate goals: improve quality, lower cost
– Harder to do in reality than the “paper merger”
Source: Adapted from R Lichtenstein
Accountability for Cost and Quality
Integrated Health Systems should:• Promote clinical effectiveness research• Only use effective procedures, therapies, tests
(Evidence-based Medicine)• Develop and use clinical guidelines, clinical
pathways• Follow principles of Continuous Quality
Improvement (CQI)• Document fastidiously
Trends 2003 Trends 2003 Shifting Accountability DownwardShifting Accountability Downward
Performance-based contractingPerformance-based contracting Report cards: outcomes, costsReport cards: outcomes, costs Defined contribution health plansDefined contribution health plans Individualized Medical Savings Individualized Medical Savings
Accounts, with provider report cardsAccounts, with provider report cards Differential copays for high cost Differential copays for high cost
hospitals/groupshospitals/groups
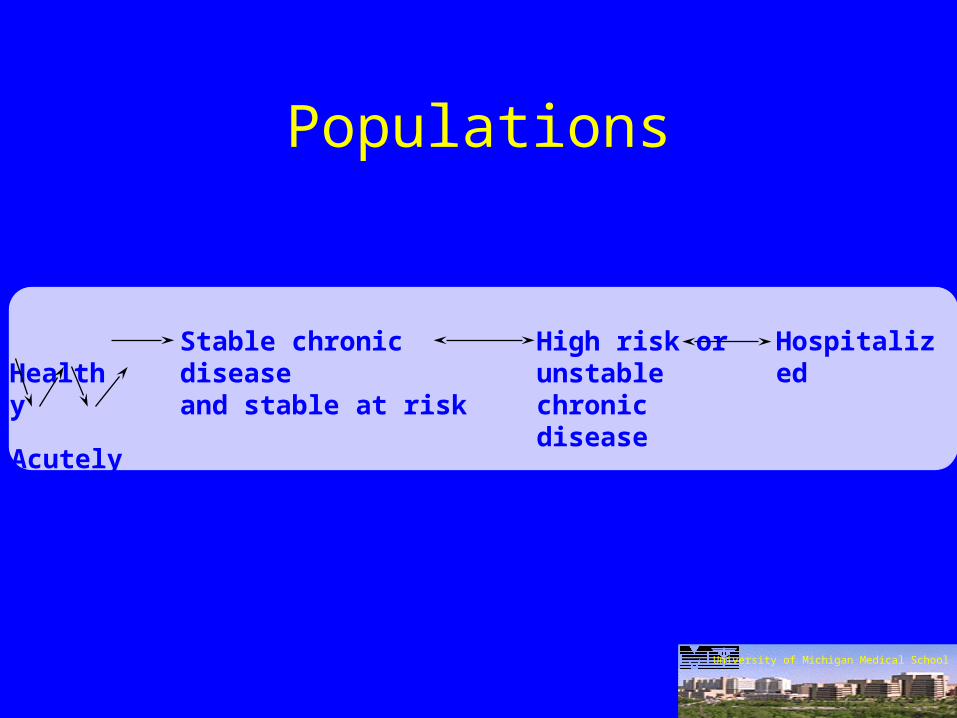
Populations
Healthy Stable chronic disease
and stable at riskHigh risk orunstablechronic disease
Hospitalized
Acutely ill
University of Michigan Medical School
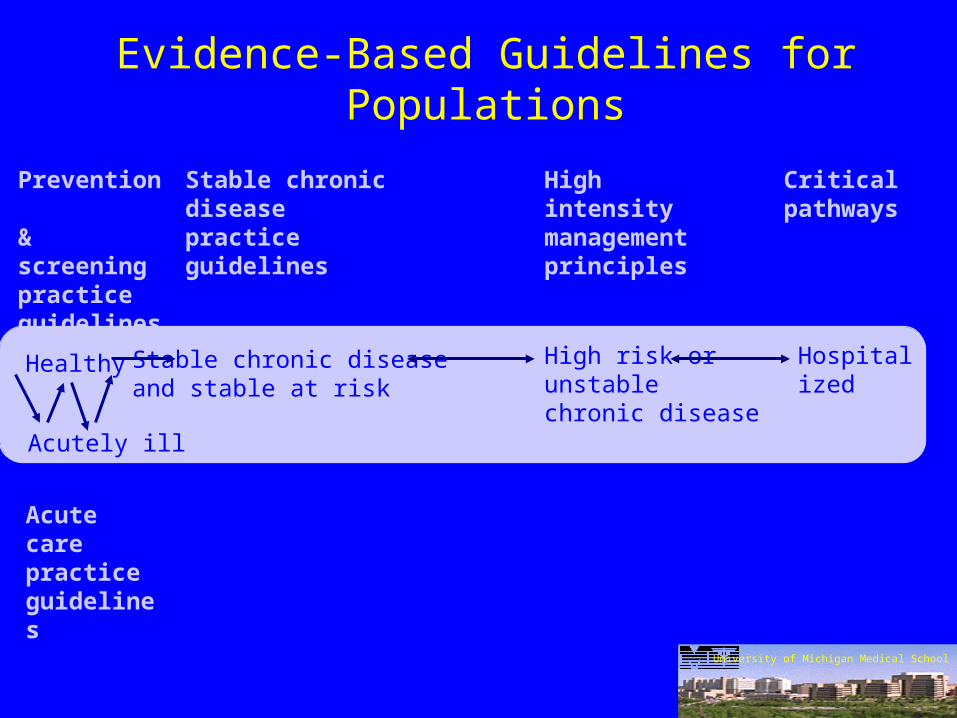
Evidence-Based Guidelines for Populations
Prevention & screeningpracticeguidelines
Stable chronic diseasepractice guidelines
High intensitymanagement principles
Criticalpathways
Acute carepracticeguidelines
University of Michigan Medical School
Healthy
Acutely ill
HospitalizedStable chronic diseaseand stable at risk
High risk orunstablechronic disease
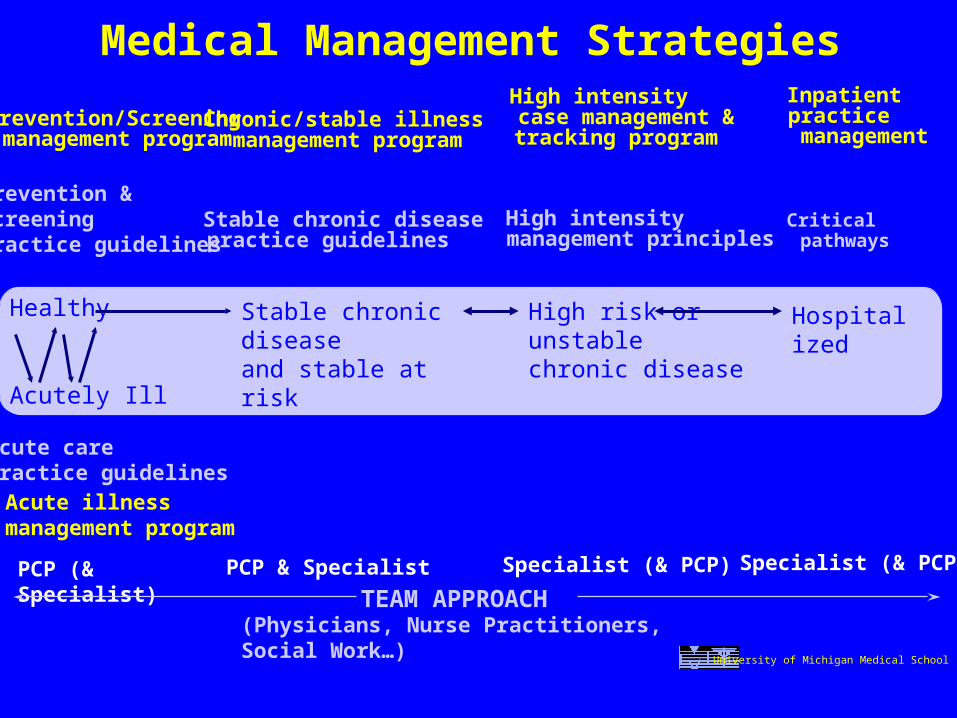
Specialist (& PCP)
Prevention &screeningpractice guidelines
Acute care practice guidelines
Stable chronic diseasepractice guidelines
High intensity management principles
Critical pathways
Prevention/Screeningmanagement program
Acute illnessmanagement program
Chronic/stable illnessmanagement program
High intensitycase management &tracking program
Inpatient practice management
PCP (& Specialist)
PCP & Specialist Specialist (& PCP)
Medical Management Strategies
TEAM APPROACH(Physicians, Nurse Practitioners, Social Work…)
University of Michigan Medical School
Healthy
Acutely Ill
Stable chronic diseaseand stable at risk
High risk or unstable chronic disease
Hospitalized
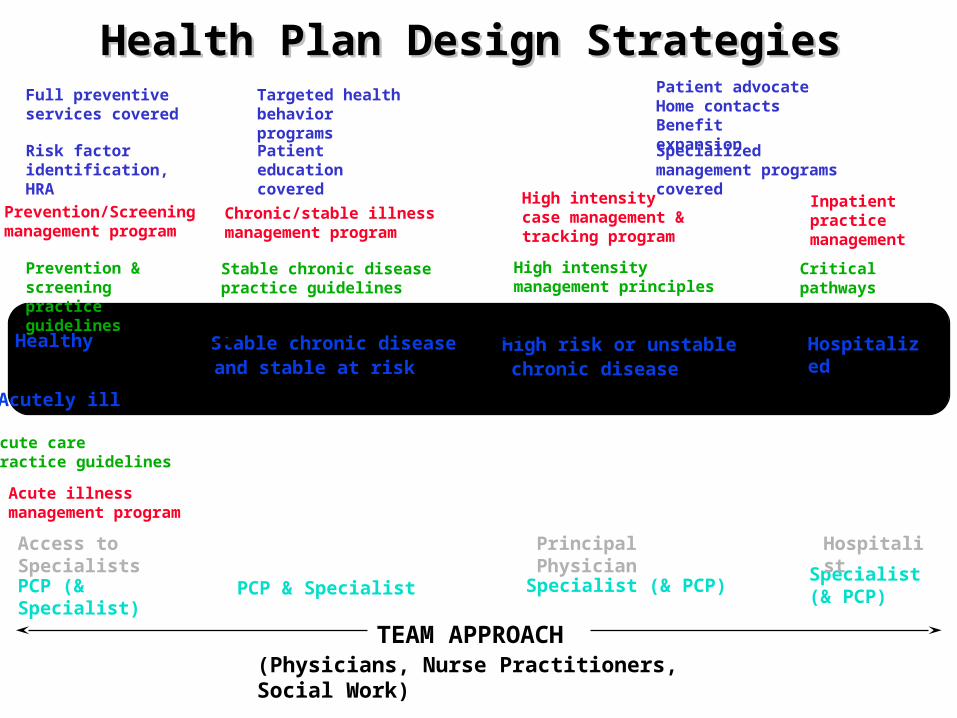
Specialist(& PCP)
Hospitalized
Healthy Stable chronic diseaseand stable at risk
High risk or unstablechronic disease
Acutely ill
Prevention & screeningpractice guidelines
Acute carepractice guidelines
Stable chronic diseasepractice guidelines
High intensity management principles
Critical pathways
Prevention/Screeningmanagement program
Acute illnessmanagement program
Chronic/stable illnessmanagement program
High intensitycase management &tracking program
Inpatientpracticemanagement
PCP (& Specialist)
PCP & Specialist Specialist (& PCP)
Health Plan Design StrategiesHealth Plan Design Strategies
Principal Physician
Hospitalist
TEAM APPROACH(Physicians, Nurse Practitioners, Social Work)
Access to Specialists
Risk factoridentification, HRA
Patient educationcovered
Specialized management programs covered
Full preventiveservices covered
Targeted health behaviorprograms
Patient advocateHome contactsBenefit expansion
Continuous Quality Improvement
The Approach to Better Healthcare
A process for continuous improvement:- evidence based- consensus building - data driven
Can be used to address:- overuse- underuse- misuse
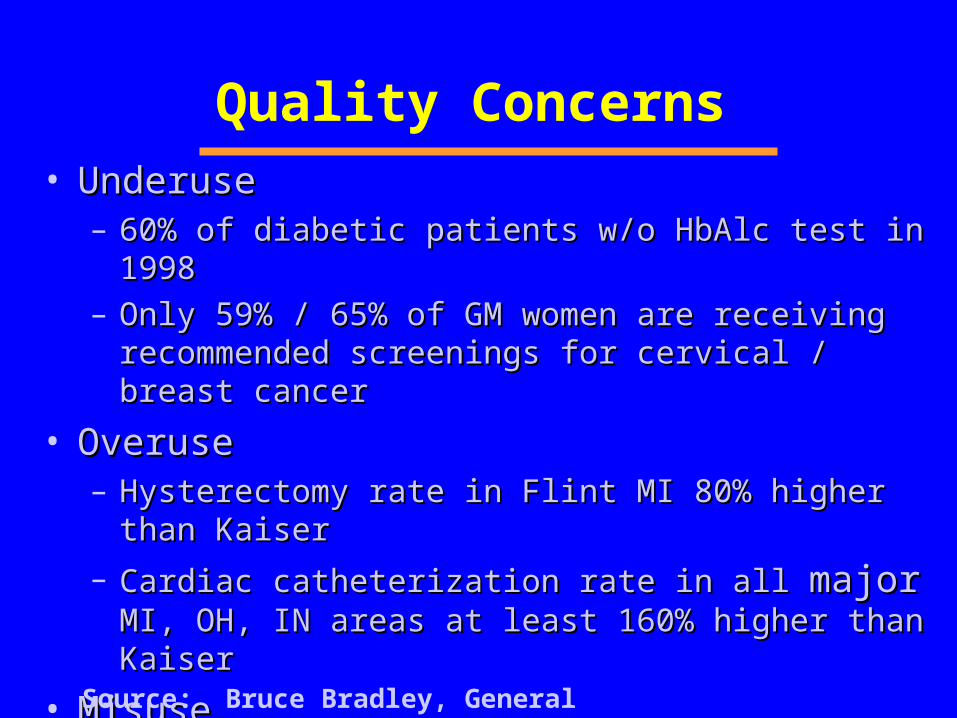
Quality Concerns• UnderuseUnderuse
– 60% of diabetic patients w/o HbAlc test in 199860% of diabetic patients w/o HbAlc test in 1998– Only 59% / 65% of GM women are receiving Only 59% / 65% of GM women are receiving
recommended screenings for cervical / breast cancerrecommended screenings for cervical / breast cancer
• OveruseOveruse– Hysterectomy rate in Flint MI 80% higher than KaiserHysterectomy rate in Flint MI 80% higher than Kaiser
– Cardiac catheterization rate in all Cardiac catheterization rate in all majormajor MI, OH, IN MI, OH, IN areas at least 160% higher than Kaiserareas at least 160% higher than Kaiser
• MisuseMisuse– 60% of cold / URI / bronchitis patients receive antibiotics60% of cold / URI / bronchitis patients receive antibiotics
Source: Bruce Bradley, General Motors
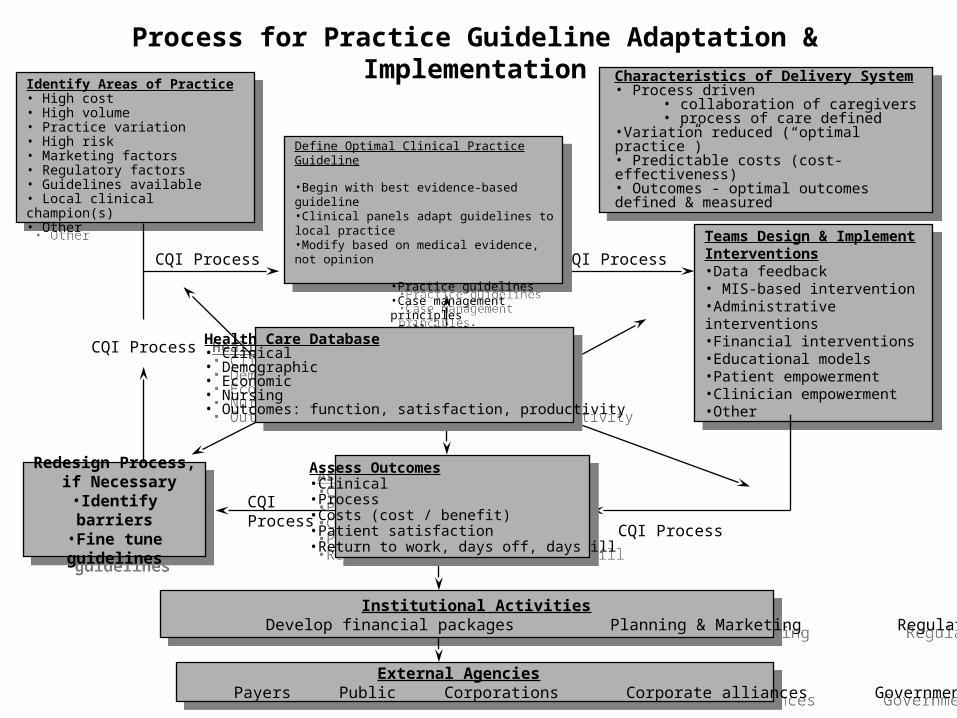
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Define Optimal Clinical Practice & Systems Processes
* Clinical panels adapt guidelines to local practice
* Collaborative critical pathways * Case management
Define Optimal Clinical Practice & Systems Processes
* Clinical panels adapt guidelines to local practice
* Collaborative critical pathways * Case management
Teams Design and Implement
Interventions
Teams Design and Implement
Interventions
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal Agencies
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
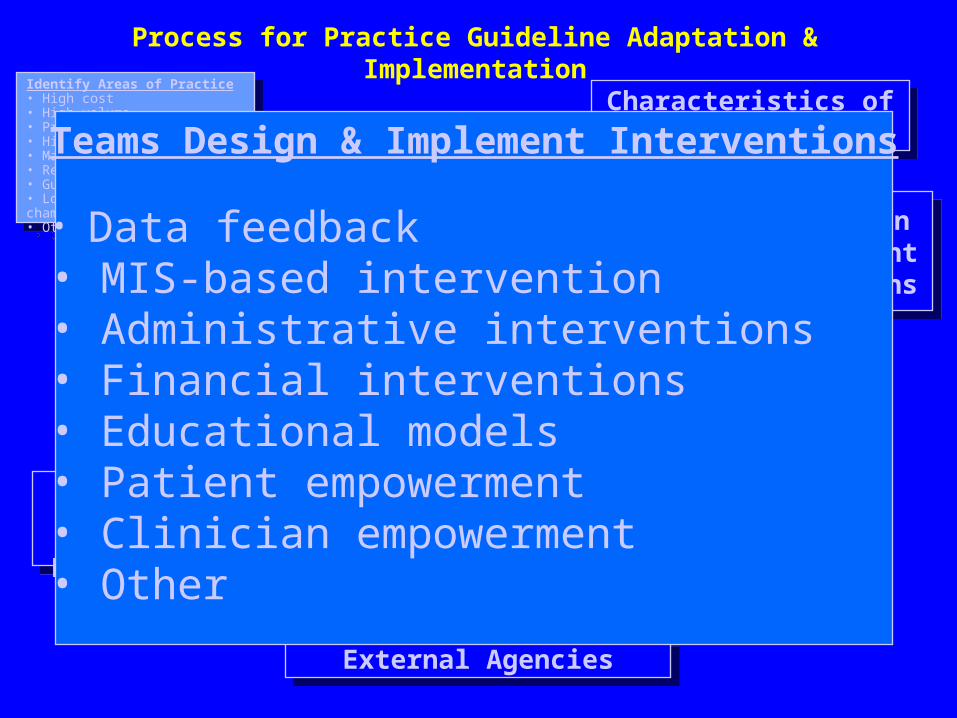
Teams Design & Implement Interventions
• Data feedback• MIS-based intervention• Administrative interventions• Financial interventions• Educational models• Patient empowerment• Clinician empowerment• Other
Process for Practice Guideline Adaptation & Implementation
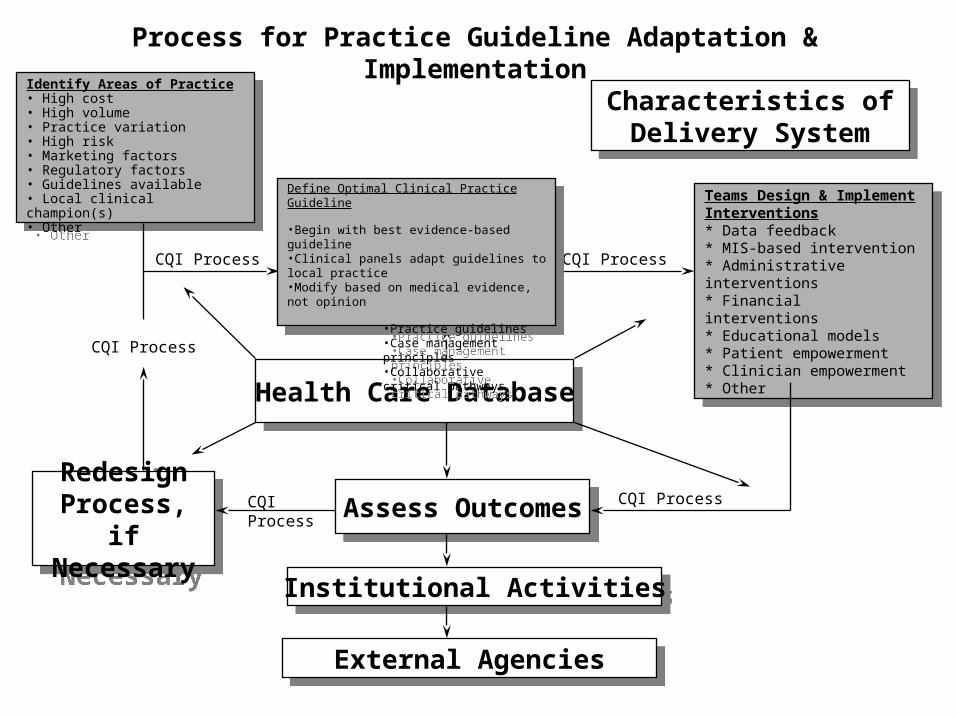
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Teams Design & Implement Interventions* Data feedback* MIS-based intervention* Administrative interventions* Financial interventions* Educational models* Patient empowerment* Clinician empowerment* Other
Teams Design & Implement Interventions* Data feedback* MIS-based intervention* Administrative interventions* Financial interventions* Educational models* Patient empowerment* Clinician empowerment* Other
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal Agencies
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Process for Practice Guideline Adaptation & Implementation
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Process for Practice Guideline Adaptation & Implementation
Teams Design & Implement Interventions•Data feedback • MIS-based intervention•Administrative interventions•Financial interventions•Educational models•Patient empowerment•Clinician empowerment•Other
Teams Design & Implement Interventions•Data feedback • MIS-based intervention•Administrative interventions•Financial interventions•Educational models•Patient empowerment•Clinician empowerment•Other
Institutional Activities Develop financial packages Planning & Marketing Regulatory reporting
Institutional Activities Develop financial packages Planning & Marketing Regulatory reporting
External Agencies Payers Public Corporations Corporate alliances Government agencies
External Agencies Payers Public Corporations Corporate alliances Government agencies
Characteristics of Delivery System• Process driven
• collaboration of caregivers• process of care defined
•Variation reduced (“optimal practice”)• Predictable costs (cost-effectiveness)• Outcomes - optimal outcomes defined & measured
Characteristics of Delivery System• Process driven
• collaboration of caregivers• process of care defined
•Variation reduced (“optimal practice”)• Predictable costs (cost-effectiveness)• Outcomes - optimal outcomes defined & measured
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Redesign Process, if Necessary
•Identify barriers•Fine tune guidelines
Redesign Process, if Necessary
•Identify barriers•Fine tune guidelines
Assess Outcomes•Clinical•Process•Costs (cost / benefit)•Patient satisfaction•Return to work, days off, days ill
Assess Outcomes•Clinical•Process•Costs (cost / benefit)•Patient satisfaction•Return to work, days off, days ill
Health Care Database• Clinical• Demographic• Economic• Nursing• Outcomes: function, satisfaction, productivity
Health Care Database• Clinical• Demographic• Economic• Nursing• Outcomes: function, satisfaction, productivity
Evidence-Based Medicine• Systematic process to encourage all practitioners
to apply the appropriate scientific evidence to individual clinical decisions.
• Evidence is not:– An expert’s or healthcare consultant’s opinion – A black box– The “Brand Name” clinical guideline book
• Evidence is:– scientific studies and meta-analyses– published in peer-reviewed journals– with appropriate methods and populations– showing significant outcomes
Practice Guidelines“I can’t keep all that evidence in my head…”
PG = A distillation of scientific evidence into a practical guide to assist a clinician in the management of a problem.
A prospective agreement among clinicians to use in the care of similar cases.
To reduce variation -- toward optimal
While permitting a doctor to vary -- with a reason!
Practice Guidelines
• Prospective agreement among clinicians for the management of typical cases
• Synthesis of knowledge of diagnoses & therapy
• Tool to improve appropriateness and efficiency
• Documentation of excellent process of care
• Evidence-based
8 Characteristics of Good Practice Guidelines
• Open development process (who developed it, why?)
• Focused on improving important, targeted health outcomes.
• Specify the most important question• Systematic use of the peer-reviewed
medical literature to support key steps.
8 Characteristics of Good Practice Guidelines
• Full disclosure of the level of evidence for each step in the guideline.
• “Expert opinion” minimized and labeled.• Include a care algorithm and key points.• Make available: supporting materials, text
rationales, literature reviews, evidence tables, patient education materials and bibliography.
UMHS Guidelines: http://cme.med.umich.edu/iCME
12 Characteristics of Good Uses of Practice Guidelines
• Start with good guidelines, including the source(s).
• Use the guidelines nested in a constructive, educationally-oriented quality improvement model.
• In the local endorsement process, involve true representatives of the clinicians whose practice the guideline covers.
• Allow local adaptation, with justification and documentation. Focus on aspects which may not be feasible.
12 Characteristics of Good Uses of Practice Guidelines
• Carefully design implementation programs to encourage education, dialogue and constructive use of data.
• The guidelines and supporting materials, literature reviews and evidence tables must be broadly available.
• Help clinicians measure their performance with a “measure to improve” rather than a “measure to judge” philosophy.
• Measure only key steps supported by high grade scientific evidence. Don’t sweat the small stuff!
12 Characteristics of Good Uses of Practice Guidelines
• Assess barriers to successful practice improvement. Make changes to overcome them.
• Activate allies to help with the changes: staff, patients, payers, employers, other physicians.
• Plan to modify the guidelines based on their use, as experience grows.
• Plan to update guidelines formally and regularly.




























![Billi Kay Khuwab Main Chechrey [Urdu]](https://img.pdfslide.net/doc/110x75/577ca59a1a28abea748b99dd/billi-kay-khuwab-main-chechrey-urdu.jpg)
