-
Joe Avelino RN, BSN, MHSA, CPHQChief Executive OfficerCollege
Medical Center
-
We, the unwilling, led
by the unknowing, are
doing the impossible
for the ungrateful. We
have done so much,
for so long, with so
little, we are now
qualified to do
anything with nothing.
(Mother Teresa)
-
Objectives
1) Structure & Design
2) Initiating ED Psychiatry Overflow Unit
3) Building a Discharge Waiting Area
4) Key Success Factors for an Access Department
5) Reviewing Your Staffing & Recruitment
6) ED Physician Collaboration with the Hospital
7) Managing the Homeless Population
8) Collaborating an Alliance with Your Local Police
Department
9) Managing the Care of the Med.- Psych Patient
Population
Strategies
-
Strategy #1
Structure and Design
-
Strategy #2
ED Psychiatry Overflow Unit
-
ED Psychiatry Overflow Unit Policy
-
ED Overflow Unit Form
COLLEGE MEDICAL CENTER
BEHAVIORAL HEALTH UNIT OVERFLOW REPORT
DATE: October 16, 2014
LICENSE BEDS BHU CENSUS OVERFLOW Unit C
157 73 8
NOTE: * This is on a interim basis, staffing is appropriate,
nurses assigned are Competent in taking care of the patients and
supplies needed are in place.
-
Strategy #3
Discharge Waiting Area
-
Discharge Waiting Area
-
COLLEGE MEDICAL CENTER
MANUAL: Behavioral Health POLICY #: BHU-00-177
SUBJECT: Discharge Waiting Area EFFECTIVE: Draft
APPROVALS: Chief of Psychiatry REVISED:
REVIEWED:
I. Purpose:
To define guidelines for use of the Discharge Waiting Area
(DWA).The Discharge Waiting Area (DWA) is intended to provide a
safe, private, relaxing environment for patients leaving the
hospital that are waiting for transportation to go to their
community setting, discharge designation. The DWA was designed to
accommodate prompt patient discharge from the acute behavioral
health unit once they have been cleared for discharge and to open
up bed availability for patients requiring an acute behavioral
admission. The DWA is only for patients that will be discharged to
the community.
II. Policy
Discharged behavioral health adult patients who have been
cleared and processed for discharge and are awaiting rides, will
wait in the designated Discharge Waiting Area until their
transportation arrives.
Description of the Discharge Waiting Area
Physical Set-up
• Located adjacent to the behavioral health unit • Staffed with
a licensed nurse(s) and experienced behavioral health worker(s)
o Staffing ratio 6 patients to 1 nurse and 1 BH worker •
Security will perform rounds every 30 minutes • The location is
manned with phone access and security cameras
Comfort
• Recliners • Bathroom • Televisions • Meals • Beverages •
Reading materials
Discharge Waiting Area P&P
-
Pt. Last Name, First
DWA
Arrival
Time
D/C Staff
Name
D/C
Staff
Phone
Ext.
Pt.
Pick-
up
Time
Trans
Type car
taxi
ambulance
other
Trans.
Contact
Name
Trans.
Contact
#
Patient
Pick-up
Time
Pt. given
meds &
Belonging
Discharge Waiting Area Log
-
Giving Back
I've come to believe that
each of us has a personal
calling that is as unique as a
fingerprint—and the best
way to succeed is to
discover your passion and
then find a way to serve
others.
(Oprah Winfrey)
Strategy #4
Access Services
-
Scope of Service
Access Services The Access Services Department is open 24 hours
a day, seven days a week. It is located on 1725 Pacific Avenue;
Long Beach, CA 90806 (South Campus). The department consists of 12
work stations, ambulance dispatch area, employee break area, Access
Director Office, and Access Coordinator Office. Access Services
averages approximately 1,000 calls a month with over 300 inpatient
admissions a month along with over 200 declined admissions (i.e.,
no bed availability). The most common diagnoses include
schizophrenia, psychosis, and bipolar disorders. The Access
Department is staffed with Intake Specialists, who are supportive
staff, with a minimum of three years’ experience in Patient Access
or Access Services. The skill mix and competency of the Intake
Specialist includes, but not limited to, insurance verification,
financial counselor, and patient access representative. Access
Services provides services for inpatient adult and geriatric
patients from eighteen and above.
The Scopes of Services offered include:
• Coordinate admissions for Behavioral Health Services from
other hospitals, nursing homes,
emergency departments, and acute care services;
• Facilitates transportation of patients for admission from
other facilities and our Emergency
Department;
• Dispatches Psychiatric Evaluation Team (PET Team) to assess
psychiatric medical necessity for
admission;
• Verifies financial clearance (i.e., authorization and
notification);
• Notifies Orange County ETS (Emergency Treatment Services) of
all OC residents into our facility ;
• Collaborates with law enforcement to ensure bed placement;
• Transfers adolescent patients to a facility that provides
adolescent inpatient services;
• Informs Department of Mental Health (DMH) of all admissions
for LA County residents into our
facility.
-
College Medical Center of Long Beach
Referral Check off List
Face sheet
Insurance Eligibility
H&P
Labs including pregnancy test
Assessment to include Psych history
Hold if applicable
Medical History
Your Contact Information if our nurse has any questions
Please provide us all the necessary documents on this list at
once in order to
avoid delays in the review process by our clinical team.
Fax# (562) 256-8493
Access/Intake (855) 844-8898
Access
Services
Referral
Check-Off
List
-
Bed
Assignment
Form
-
Date: Time: From: Ext: To: Ext:
Attending Physician: Code Status: Full unless otherwise
stated
DNR or Modified Name:
Gender: F or M Age: Diet:
Allergies:
Isolation: Standard Contact Airborne Droplet
Risks: Fall Seizure Suicide Aspiration Assault
Transfer to unit verified: Y N
Medication Reconciliation Done: Y N
Chief Complaint: __________________________
Patient Diagnosis: __________________________
Past Medical Hx: __________________________
______________________________________________
____________________________
Misc. Amb, Wheelchair, Weakness (L,R Bil)
PERTINENT MEDICATIONS
Given: ___________________________________
Pending: _________________________________
Drips/Current Infusion: _____________________
Last Pain Med: ____________________________
IMAGING
ORDERED DONE
___ CT___________ ___
___ MRI__________ ___
___ XRAY_________ ___
___ Other__________ ___
Labs Sent: ________________________________
Pertinent Lab Results: _______________________
Last Vitals: ____________ IV Access: _________
HR: __________________ SpO2: _____________
BP:___________________ RR: ______________
Temp: ________________ Glucose:___________
Pregnancy Test : Pos, Neg, N/A
NEURO: Alert Oriented: x_________
___ PERRLA MAE
Deficits: _________________________
RENAL: VOIDS Foley DOI:______ Anuric DTV
___ Dialysis Cath Site/Type: ______________
Dialysis Sched: M W F or T TH
Last:____
CARDIO: SR SB ST AFIB/AFLUTTER
OTHER
__ Pulse Present
SKIN: Warm/Dry Intact Diaphoretic
___ Skin Alterations: _________________
Photo: DONE
___Cloth removed and change in hospital gown
PULM: RA NC VENTIMASK NRB
BIPAP
Liters O2: _____________________________
Vent Settings: __________________________
ETT/Trach Size/Position_________________
SAFETY: Belonging Searched/ Secured: Y N
___ Valuable in security: Y N
Home meds in pharmacy or with patient
MISC: Restraints: ____ Chemical/
Physical/Med
___ Sitter: Y N
________Date/Time 5150 GD DTO DTS VOL
GI: Abd: Soft Nontender Tender
Distended
___ NPO PO BM: __________________
NGT/OGT Drainage: _____________
Surgical Patient: _____Per-op Surgical check list
____NPO at least 6 hours
____Consent obtained
____Anesthesia consent obtained
PROCEED WITH TRANSFER WHEN ALL OF THE FOLLOWING HAVE BEEN
COMPLETED…
___ Report faxed
___ Receiving RN has confirmed receipt of SBAR report
Signature of transferring RN: ______________________ Print
Name__________________________
Date:_______ Time:_____
ER Transfer SBAR Form ICU FAX # 562 4261503 Med Surg Fax # 2N
562 997 2493// 2 W 562-490-9668
Unit B 562 997 2284 Perinatal 562 997 2455BHU: 1 W# 562 997 2519
1 S# 562 997 9859 SC # 5622568445
SBAR
Documentation
Form
-
Strategy #5
Staffing and Recruitment
-
Strategy #6
ED Physician Collaboration with the
Hospital
From the
Physician Leadership Institute
We need physicians to lead the
healthcare transformation and not just
be spectators. Physician leadership is
not limited to a specific role, title or
position…it is about physicians
embodying the attitudes, behaviors,
perspectives, professional identity
and competencies of a leader.
By Mo Kasti
-
CONFIDEN
TIAL
PA
GE
25INSERT HOSPITAL LOGO
2016 Emergency Department Efficiencies: Length of Stay
Psychiatric avg LOS is under 6 hrs while LA County is reported
to be 10.5 hrs
-
CONFIDEN
TIAL
PA
GE
26INSERT HOSPITAL LOGO
2016 Emergency Department Efficiencies: Door to Doctor Times
Avg door to doctor times are under BMK of 30 minutes
-
CONFIDEN
TIAL
PA
GE
27INSERT HOSPITAL LOGO
Best Practices for Psychiatric Emergencies
• Triage and rapid medical evaluation
• High psychiatric acuity with a low rate of restraints utilized
at
-
Strategy #7
Managing the Behavioral Health
Homeless Population
-
FIRST ADDENDUM TO
MEDICAL TRANSPORTATION AGREEMENT
BETWEEN
COLLEGE HOSPITAL LONG BEACH
AND
FIRSTMED AMBULANCE SERVICES, INC.
The Medical Transportation Agreement between CHLB, LLC dba
College Medical
Center/College Hospital Long Beach (“Hospital”) and FirstMed
Ambulance Services, Inc.
(“Provider”) effective ____, shall be amended as follows:
1.5 Ambulance Assignment. Provider shall assign two (2) 2013
Ford E-350
ambulances to service Hospital. The said ambulances shall, at
Hospital’s discretion, be
customized with the Hospital’s insignia to promote and identify
the Hospital and its services.
Hospital retains the right to have its insignia removed from the
ambulances at any time, with or
without cause. To the extent Hospital desires to have its
insignia removed from the ambulances,
Hospital will provide written notice to Provider requesting that
the insignia be removed. Within
seven (7) days from receipt of the written notice, Provider
shall have Hospital’s insignia
removed from all ambulances and Provider shall provide Hospital
with confirmation of the same.
1.5(a) Transports to “Patient Safety Zone” The Patient Safety
Zone is an area in Los
Angeles that is generally known as “Skid Row” and is more
specifically described as the
geographic area encompassed by the Central and Newton Divisions
of the Los Angeles Police
Departments, bounded by the Pasadena freeway and the Los Angeles
River to the North; by the
Harbor freeway to the West; by the Los Angeles River to the
East; and by Florence Avenue to
the South. A map of the Patient Safety Zone is attached hereto
and incorporated herein.
It is the practice of the Hospital to not transport patients to
the “Patient Safety Zone”
unless certain exceptions exist, such as the patient having a
fixed permanent residence in the
Patient Safety Zone; the patient is being discharged to a family
member with a fixed permanent
residence in the Patient Safety Zone; or the patient is being
transferred to another health care
facility that is located in the Patient Safety Zone.
By executing this Addendum, Provider agrees to abide by and
comply with Hospital’s
Best Practices on Psychiatric Homeless Patient Discharge
Planning, a copy of which is attached
and incorporated herein. Unless an exception applies, Provider
agrees to not transport any of the
Hospital’s patients to the Patient Safety Zone. If Provider is
requested to transport a Hospital
patient to the Patient Safety Zone pursuant to one of the
exceptions identified above, Provider
agrees to first consult with the Hospital’s Chief Executive
Officer and Director of Corporate Risk
Management prior to making the transport.
Provider further agrees to keep all ambulances that contain
Hospital’s insignia away from
the Patient Safety Zone unless there is an emergency medical
need for the ambulances to be
present in the Patient Safety Zone or Provider is making a
permitted transport to the Patient
Safety Zone pursuant to the provisions above.
-
College Medical Center of Long Beach
HOMELESS PATIENT INFORMED CONSENT DISCHARGE FORM /
PLACEMENT OPTIONS
Patient’s Name: ___________________________ Patient’s ID #:
__________________________
PLEASE READ THIS DOCUMENT CAREFULLY. IF YOU CANNOT READ OR DO
NOT
UNDERSTAND THIS FORM, PLEASE ASK FOR HELP. YOUR SIGNATURE IS
REQUIRED WHETHER YOU ACCEPT OR REFUSE THE DISCHARGE
RECOMMENDATIONS. YOU WILL BE GIVEN A FULLY COMPLETED AND
SIGNED
COPY OF THIS CONSENT FORM.
Patient’s Rights: You, as a patient, have numerous rights
guaranteed by law which include the
right to compassionate and respectful care, the right to
participate in your care and to ask for and to
be provided with all the information you need to make an
informed decision about your care, the
right to request or to refuse appropriate and medically
necessary treatment, service or medication as
well as the right to leave the hospital against the advice of
members of the medical staff except in
certain situations involving an emergency or legal detention. A
disclosure of your rights is attached.
Recommended post-hospital care:
The attached Discharge Plan recommends that you:
Offered Rejected
by staff by patient
□ □ be referred to __________________________ □ Sober Living
□ Shelter
□ □ be transferred to _______________________ □ Skilled Nsg
□ Board & Care
□ Retirement/ Asst. Living
□ □ be transported to ________________________ □ Other
Reasons for Recommendations:
Homeless
Patient
Informed
Consent
Discharge
Form
-
Shelter Contact Checklist
Document Instructions: Complete this form At the time of
discharge, if patient requires
shelter- (1) Provide patient with a copy; (2) Maintain a copy in
the medical record; (3)
Send another copy to the Behavioral Health Director.
1.
Patient’s Address/
Location of Preference:
2
Accepting Shelter:
Shelter Name:
Shelter Address:
Shelter Phone #:
Shelter Contact Person:
Date of Contact:
Time of Contact:
3.
Requirements of
Accepting Shelter (i.e.,
waiting in line, specific
time format):
Special Instructions:
4a.
4b.
Patient Agrees to
Shelter:
Patient Declines Shelter:
Patient Signature: Date: _ _
Patient Name (printed):
Patient Signature: Date: _ _
Patient Name (printed):
5.
Responsible Party Approval:
I attest that:
The medical record documents that the patient is cognitively
intact and able to negotiate the community.
Responsible Party’s Signature: Date: Print
Name: Comments:
Patient Sticker
Homeless
Patient
Shelter
Contact
Checklist
-
Strategy #8
Build an
Alliance with
Your Local
Police
Department
-
Mental Evaluation Team (MET) and
Mobile Response Team (MRT)
-
The Three
Seasons of Timing
When they heard enough
that they have to;
When they learn enough
that they want to; and
When they receive enough
that they are able to.
By John C. Maxwell
Strategy #9
Care of the Med.- Psych
Patient Population
-
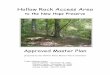
Medical Psych Patient Transfer ProcessRevised January 11,
2017
House Supervisor notifies
Referring Facility.
Physicians must have a phone conversation for official
acceptance.
Supervisor to continue to process as a direct admit by
getting orders from admitting physician and contacting
admitting.Email Gina, Joe, Ava, Access,
Tammy Jo, Mirna, and
Mike Hartman the disposition of
patient.
To determine need for acute medical or surgical care,
Nursing Supervisor will request a faxed copy of the
prospective patient’s clinicals.
(562)989-4850
Please make sure transferring facility is
aware that if they need to reach the
Nursing Office, and use the Office
extension, to please leave a very
detailed message if they are unable to
reach the Nursing Supervisor directly.
Transferring facility will contact Nursing Office House
Supervisor to indicate that they have a patient with acute
medical or surgical care, and behavioral health needs
Supervisor Direct Line: (562)997-2418
Office Phone: (562)997-2275
Email Gina, Joe, Ava, Jay Ann,
Tammy Jo, Mirna, and Mike
Hartman the information on why
the patient does not need acute
medical care.
If it is during the day, you may also
call Access
855-844-8898
562-256-8350
Does the Physician Accept the patient? No
Access continues to evaluate for potential psych admission since
they
are not a medical patient.
Supervisor determines type of Physician needed, (ex:
ortho, surgery) and calls Physician from call panel to
present case regarding need for acute medical care.
Yes
Does the patient appear to need Acute Care?
(Please contact Case Management if you feel there is a
need for InterQual assessment; this may delay the
transfer process)
No
Yes
PET team will be notified to travel to transferring facility
to assess need for placement of a hold.
-
Transferring Medical/Psych Patients to
College Medical Center
Please contact our House Supervisor at (562)997-2418 or
(562)997-2275
If you do not reach them directly, and instead reach the
voicemail, please leave
a detailed message which includes:
✓ Your Name
✓ Your Number (where they can reach you directly at your
facility)
✓ The patient’s medical diagnosis
After speaking with our House Supervisor, please fax the
following to
(562)989-4850:
☐ Face Sheet ☐ EKGs
☐ History and Physical ☐ X-Rays
☐ Last 24 Hour Vital Signs ☐ Physician Consultations
☐ Last 24 Hour Medication Sheet ☐ Physician Progress Notes
☐ Last 24 Hour Nurses’ Notes ☐ All Lab Work, Including
UA/UDS
☐ Any Legal Hold Paperwork (5150, 5250, etc.)
☐ Emergency Department Records
Upon receipt and review of these records, and if there is a bed
available, our
House Supervisor will contact you with the name and number of
the on-call
physician.
In order to complete this transfer, the College Medical Center
(CMC) physician
must accept the patient from your physician.
If the patient is not on a hold, and once they are accepted by
CMC, the PET
team will be sent to your facility prior to transfer. Results of
PET will not
change acceptance.
-
Strategy #10
Other Points of Consideration in
Behavioral Health Services
-
Resolution
of Patient
Grievances
-
College Medical Center
Complaint Documentation Form
Grievance # 2013-
Name of Complainant:
Ph:
Address:
MR#:
Date Submitted:
____________________________________________________________
Department(s):
Complaint Issues:
Call Log: (3 call attempts to complainant)
Investigation Details: (include details on what specific actions
were taken. If
staff was counseled include names and dates)
Action/Resolution:
Complaint
Documentation
Form
-
Trade Name Product Desc # Doses QuantityCost per
Box Total0 $0.00
Latuda lurasidone 80 mg Tab #100 UD 168 1.68 1,808.23
$3,037.83
Abilify ARIPiprazole 20 mg Tab #100 UD 65 0.65 3,498.65
$2,274.12
Restoril TEMAZepam 30 mg Cap #100 UD 467 15.6 138.00
$2,152.80
Abilify ARIPiprazole 10 mg Tab #100 UD 61 0.61 2,473.92
$1,509.09
Latuda lurasidone 120 mg Tab #30 45 1.5 809.69 $1,214.54
Risperdal Consta risperiDONE 25 mg/2 weeks IM Inj, ER (ea) 4 4
290.50 $1,162.00
Abilify ARIPiprazole 5 mg Tab # 100 45 0.45 2,473.92
$1,113.26
Zyprexa OLANZapine 10 mg IM Inj (ea) 31 31 25.20 $781.20
Seroquel ER QUEtiapine 300 mg oral ER Tab #100 44 0.44 1,735.60
$763.66
Abilify ARIPiprazole 2 mg Tab #30 29 0.97 742.23 $719.96
Latuda lurasidone 40 mg Tab #100 28 0.28 1,808.23 $506.30
Geodon ziprasidone 80 mg Cap #40 92 2.3 183.63 $422.35
Abilify ARIPiprazole 30 mg Tab #100 UD 7 0.07 3,498.65
$244.91
Risperdal risperiDONE 2 mg Tab #100 UD 535.5 5.355 34.14
$182.82
Top Ten Drugs (By Month)
In Behavioral Health Services
-
SERVICE CHIEF/CLINICAL DIRECTOR AGREEMENT
UTILIZATION REVIEW
THIS SERVICE CHIEF/CLINICAL DIRECTOR AGREEMENT is entered into
as of this
1st day of April, 2014, by and between College Hospital, Inc., a
California corporation doing
business as College Hospital ("Hospital"), and _________________
("Service Chief/Clinical
Director/Clinical Director"), with reference to the following
facts:
RECITALS
A. Hospital is the operator of an acute psychiatric hospital at
Cerritos, California, and
desires to establish and operate a program to provide
psychiatric services to patients in need of
acute and/or sub-acute services.
B. Service Chief/Clinical Director is an expert in general
psychiatry and wishes to
provide services in his area of expertise to Hospital.
C. The parties desire to enter into this Agreement whereby
Service Chief/Clinical
Director shall provide the services described herein to
Hospital.
NOW THEREFORE, it is agreed as follows:
I. DUTIES OF SERVICE CHIEF/CLINICAL DIRECTOR
Service Chief/Clinical Director shall:
1.01 Provide clinical supervision and direction of the
Utilization Review department on
difficult cases.
1.02 Interact with and give advice to physicians, after
reviewing the patient’s chart when
potential for a denial is eminent. Such signs of denial include
but are not limited to the
following:
1.02.01 A geriatric patient whose length of stay (LOS) is beyond
7 days.
1.02.02 When Utilization Review informs Service Chief/Clinical
Director about specific patients who have reached a baseline for at
least 24 to 48 hours
or whose documentation is not descriptive supported by evidence
of a
UR Medical
Director to
Address
Denials
-
PSYCHIATRIC EVALUATION SERVICES AGREEMENT
This Psychiatric Evaluation Services and Transfer Agreement (the
“Agreement”) is made and entered into as of October 1, 2013 (the
“Effective Date”) by and between College Hospital Long Beach, LLC,,
a California corporation, d/b/a College Medical Center
(“Facility”), and Little Company of Mary Hospital (“Hospital”).
R E C I T A L S:
A. Hospital operates an acute care hospital located at 4101
Torrance Blvd. in Torrance, California and is in need of
psychiatric evaluation services for patients presenting with
behavioral health problems (“Hospital Patients”).
B. Facility employs and/or contracts with qualified physicians
and registered and/or
certified staff duly licensed in the State of California
(“State”) with expertise and experience in providing psychiatric
evaluation services for patients with behavioral health
problems.
C. Hospital and Facility desire to enter into an agreement under
which Facility shall
provide psychiatric evaluation services for all appropriate
patients of Hospital and care for those patients who require a
psychiatric facility.
NOW THEREFORE, in consideration of the promises and mutual
covenants herein set forth, it is agreed as follows:
1. RESPONSIBILITIES OF FACILITY
1.1 Services
1.1.1 Evaluation Services. Facility shall provide psychiatric
evaluation and related services for Hospital Patients as described
in, and in accordance with, Exhibit A as requested by Hospital
pursuant to the order of patient’s attending physician. 1.1.2
Placement of Indigent Patients. For patients who require inpatient
psychiatric hospitalization but lack the ability to pay for such
services (“Indigent Patient”), Hospital may authorize Facility to
arrange, at Hospital’s sole cost, inpatient placement for such
Indigent Patients at Facility. Such Indigent Patients must meet the
admission criteria as set forth in Exhibit D (“Medical Guidelines
for Psychiatric Inpatient Admissions”). Prior to admission of an
Indigent Patient pursuant to this Section 1.1.2, Facility and
Hospital shall complete an authorization form (“Authorization
Form”), a copy of which is attached as Exhibit C.
1.2 Hours of Service. Facility shall be available to provide
psychiatric
evaluation and placement services twenty-four (24) hours a day,
seven (7) days a week. Facility shall respond to requests to
perform emergency psychiatric evaluations with a call back to
Hospital within thirty (30) minutes of receiving such a request as
in accordance with Exhibit A.
Transfer
Agreement
Form
With
Hospital
-
Summary
1) Review of ED Patient Flow from an Acute Care vs. Behavioral
Health from a Patient Perspective.
2) Review Design Structure to avoid a BH patient from harming
self and elopement avoidance
3) Create a ED Psychiatry Overflow Unit
4) Create a Discharge Waiting Area
5) Access Services: Check Off List, Bed Assignment Form,
SBAR
6) Reducing Registry and Travel Contracted Staff
7) Creating a Reporting Structure to create a culture of ED
Physician Collaboration
8) Homeless Patient: Patient Safety Zone, Informed Consent,
Shelter Contact Checklist.
9) Collaborate with Your Local Police Department
10) Evaluate Your Process of Admitting Med.-Psych. Patients
11) Patient Grievances
12) Top 10 Behavioral Health Medications
13) UR Medical Director
14) Transfer Agreement Form With Hospitals
Action Items
-
Questions?