Embed Size (px)
Citation preview

ColloColloïïdesdes--CristalloCristalloïïdesdes::le point en 2005le point en 2005
FrFrééddéérique rique SchortgenSchortgenrrééanimation manimation méédicaledicale
hôpital Henri hôpital Henri MondorMondor--CrCrééteilteil

Colloids withCrystalloids
n=312 (65% )
Colloidsn=173 (18%)
Crystalloidsn=92 (17%)

Justifications of plasma expander choice:Justifications of plasma expander choice:The most frequently cited arguments
Colloid users n=4771) The rapidity to reverse intravascular volume loss 96%2) The choice of volume expander is strongly
dependent on the clinical situation 81%3) The long lasting volume-expansion effect 66%4) The reduced risk of pulmonary oedema 49%
Colloid nonusers n=991) The low risk of adverse events 92%2) Crystalloids are as effective as colloids
if the volume administered is sufficient 90%3) The low cost 86%

Pourquoi utiliser un colloPourquoi utiliser un colloïïde? de?
EfficacitEfficacitéé pour un moindre volumepour un moindre volume

Haemorrhagic shock
Amount of fluid required5% albumin 18.6 ± 2.3 mL25% albumin 7.6 ± 1.4 mLRL group 63.5 ± 6.0 mL
Endotoxic shock
Amount of fluid required5% albumin 11.6 ± 0.7 mL25% albumin 5.1 ± 0.3 mL RL group 50.2 ± 2.7 mL
Zhang et al. Crit. Care Med. 2003

1 : 3 RLPentastarch
Increase in Blood Volume: 500 ml
SurgeryUeyama1999
1 : 1.6RLHES 10%
PAPO 16-18Critically ill patientsHankeln1989
1 : 2.9RLDextran 60
PAOP maintenanceVascular surgeryDawidson1991
1 : 1.7RLAlb 5%
PAOP and CI maintenance
Vascular surgeryVirgilio1979
1 : 1.9RLPlasma
PAOP maintenance Vascular surgeryShires1982
1 : 1RLAlb 5%
PAM>80 mmHgTrauma+chocMoss1981
1 : 1.4 to 2NSHetastarch5% alb
250 ml/15min until PAOP 10-15 mmHg
Hypovolemic shockHaupt1982
1 : 1.8 to 2.4NS Hetastarch5% alb
250 ml/15 mins until PAOP 15 mmHg
Septic shockRackow1983
Colloids :Crystalloids
FluidsobjectiveIndication

30 hypovolemic septic shock (ITBVI<850 ml/m2)
250 ml bolus4% Gelatine 35 kDa
250 ml bolus6% HES 200 kDa/0.62
ITBVI>900 ml/m2 ITBVI>900 ml/m2
750+274 ml 714+254 ml
ITBVI=798+37 ml/m2 ITBVI=791+52 ml/m2

Pourquoi utiliser un colloPourquoi utiliser un colloïïde? de? Pour prPour préévenir lvenir l’’oedoedèème pulmonaireme pulmonaire
AA
πmvPmv
Ppmv πpmv Qf
Qf = Kf [(Pmv-Ppmv) - σ(πmv-πpmv)]

EffectsEffects of of albuminalbumin supplementationsupplementationon on microvascularmicrovascular permeabilitypermeability in in septicseptic patientspatients
Michael P. Michael P. MargarsonMargarson andand Neil C. Neil C. SoniSoni Vol. 92, Issue 5, 2139Vol. 92, Issue 5, 2139--2145, May 20022145, May 2002
ALB 20%200 ml (90sec)

AlbuminAlbumin andand furosemidefurosemide therapytherapy in in hypoproteinemichypoproteinemic patients patients withwith acute acute lunglung injuryinjury
GS Martin GS Martin CriticalCritical Care Care MedicineMedicine 2002; 30(10):21752002; 30(10):2175--21822182
- 930 €

30 hypovolemic septic shock (ITBVI<850 ml/m2)
250 ml bolus4% Gelatine 35 kDa
250 ml bolus6% HES 200 kDa/0.62
ITBVI>900 ml/m2 ITBVI>900 ml/m2
750+274 ml 714+254 ml
ITBVI=798+37 ml/m2 ITBVI=791+52 ml/m2

0
200
400
600
800
1000
1200
BL End 30 min 60 min0
2
4
6
8
10
12
14
16
18
20
ITBVI-HESITBVI-GelEVLW-HESEVLW-Gel
ITBVI, ml/m2 EVLW, ml/kg
Molnar et al. Intensive Care Med 2004

Effects of albumin and Ringer's lactate on production of lung cytokines and hydrogen peroxide after resuscitated hemorrhage and endotoxemia in rats Haibo Zhang, MD, PhD; Stefanos Voglis, BSc; Chang-Ho Kim, MD; Arthur S. Slutsky, MD 2003; 31(5):1515-1522
Cytokines pulmonaires

Twenty-five percent albumin prevents lung injury following shock/resuscitation
Kinga A. Powers 2003; 31(9):2355-2363
Sham
ALB 25%
RL
ALB 5%

EffectsEffects of of albuminalbumin supplementationsupplementationon on microvascularmicrovascular permeabilitypermeability in in septicseptic patientspatients
Michael P. Michael P. MargarsonMargarson andand Neil C. Neil C. SoniSoni Vol. 92, Issue 5, 2139Vol. 92, Issue 5, 2139--2145, May 20022145, May 2002
Comparison before and after 40-g albumin infusion
Preinfusion Postinfusion Pvalue
Albumin, g/l 9.9 ± 3.9 18.3 ± 4.1 (at 30 min) <0.001
CVP, mmHg 11.2 ± 3.3 13.2 ± 3.6 (at 30 min) <0.001
TER, %/h 6.6 ± 1.5 6.1 ± 2.2 0.406
t1/2 of 125I-albumin min 571 (Median) (95% CI 545-752) 672 (Median) (95% CI 575-918) 0.511

Restrictive
Libre ImprovedImproved outcomeoutcome basedbased on on fluidfluidmanagement in management in criticallycritically illillpatients patients requiringrequiring pulmonarypulmonary
arteryartery catheterizationcatheterization
Mitchell et al. ARRD 1992

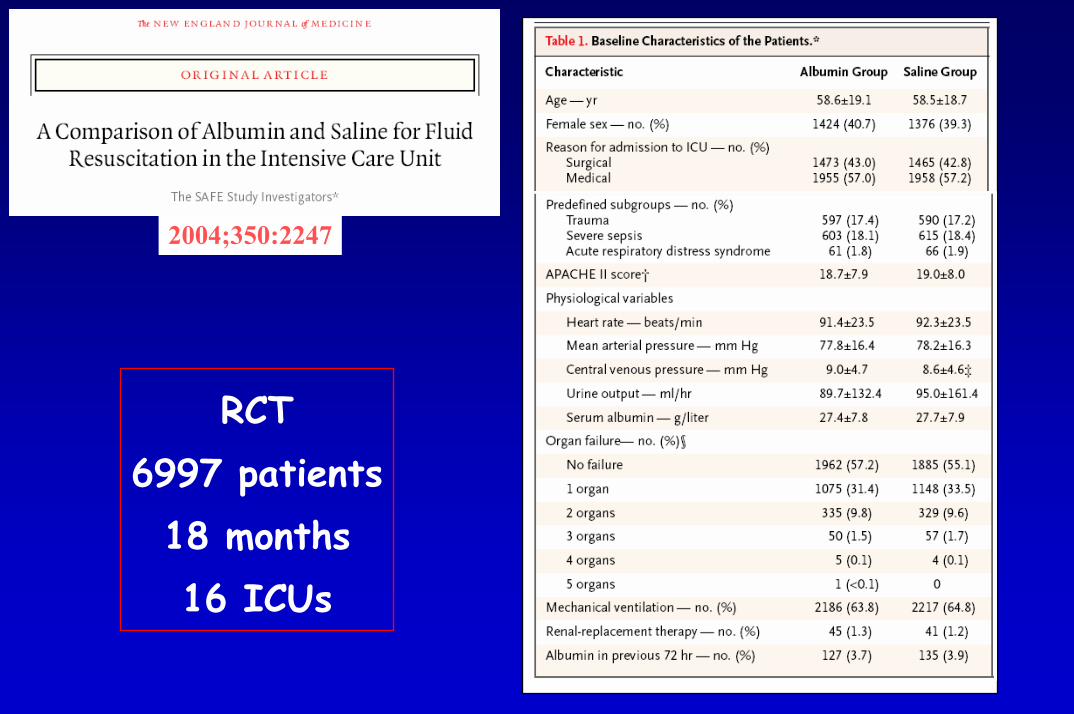
2004;350:2247
RCT6997 patients
18 months16 ICUs
2004;350:2247
RCT6997 patients
18 months16 ICUs


N Engl J Med 2004; 350: 2247

Patients with trauma andan associated brain injury
0
5
10
15
20
25
30
Saline Albumin
Mortality (%)P=0.009

CrystalloidsCrystalloids vs. vs. colloidscolloids in in fluidfluid resuscitationresuscitation: : a a systematicsystematic reviewreview..
All StudiesAll Studies
1515
Studies in traumaStudies in trauma
55
nn
732732
302302
0.86 (0.630.86 (0.63--1.17)1.17)
0.39 (0.170.39 (0.17--0.69)0.69)
11 22 55 1010 2020 5050 100100.5.5.2.2.1.1.05.05.02.02.01.01
Favors ColloidsFavors ColloidsFavors CrystalloidsFavors Crystalloids
Choi PT et al. CCM 1999Choi PT et al. CCM 1999

0
200
400
600
800
1000
1200
1400
1600
Day 1 Day 2 Day 3 Day 4
AlbuminCrystalloids
Liters
1:1.4
SAFE N. Engl. J. Med. 2004; 350: 2247

Impact of fluid choice on the outcomeof critically ill patients with shock
F. Schortgen, S Bastuji-Garin, N. Deye, L. BrochardMedical ICU and Public health
Henri Mondor HospitalCréteil-France

Methods
• Prospective cohort study
• Consecutive adult patients admitted in 115 ICUs (30 countries) during a 4 weeks period and needing fluid resuscitation for shock in the intensive care unit

736 patients with shock
611 receiving colloids 125 receiving crystalloids
% of patients
100Type(s) of colloids administered
80
60
40
20
0Starches Gelatins Plasma Albumin Dextrans
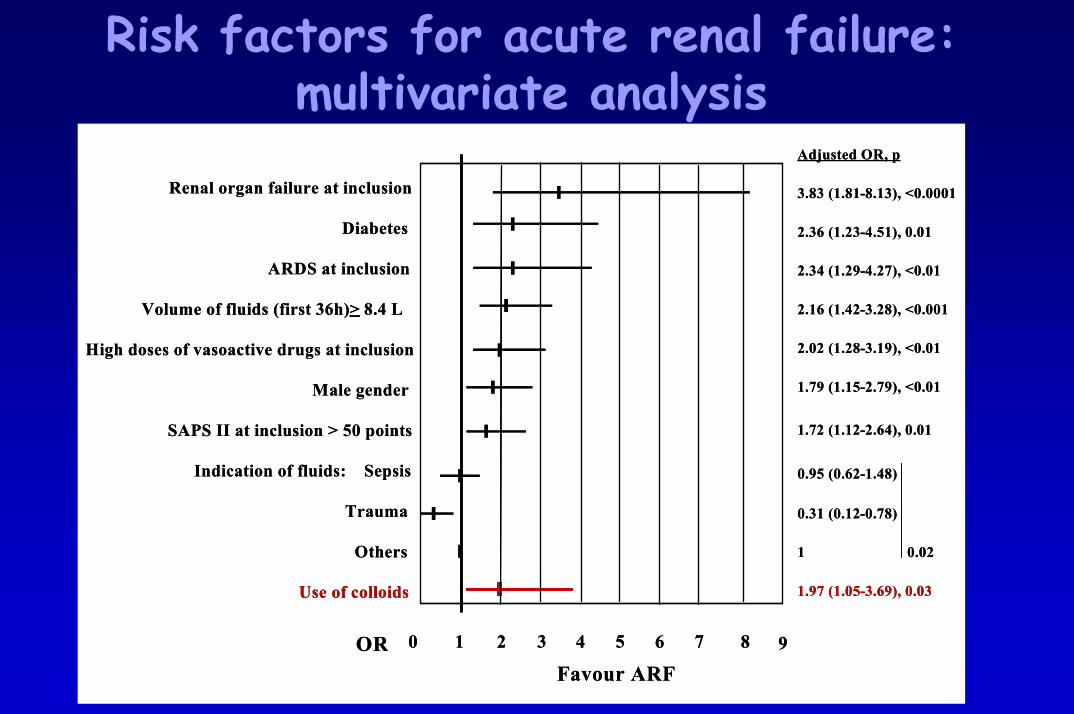
Risk factors for acute renal failure:multivariate analysis
Renal organ failure at inclusion
Diabetes
ARDS at inclusion
Volume of fluids (first 36h) > 8.4 L
High doses of vasoactive drugs at inclusion
Male gender
SAPS II at inclusion > 50 points
Indication of fluids: Sepsis
Trauma
Others
Use of colloids
ORFavour ARF
Adjusted OR, p
3.83 (1.81-8.13), <0.0001
2.36 (1.23-4.51), 0.01
2.34 (1.29-4.27), <0.01
2.16 (1.42-3.28), <0.001
2.02 (1.28-3.19), <0.01
1.79 (1.15-2.79), <0.01
1.72 (1.12-2.64), 0.01
0.95 (0.62-1.48)
0.31 (0.12-0.78)
1 0.02
1.97 (1.05-3.69), 0.03
1 2 4 6 80 3 5 7 9
Renal organ failure at inclusion
Diabetes
ARDS at inclusion
Volume of fluids (first 36h) > 8.4 L
High doses of vasoactive drugs at inclusion
Male gender
SAPS II at inclusion > 50 points
Indication of fluids: Sepsis
Trauma
Others
Use of colloids
ORFavour ARF
Adjusted OR, p
3.83 (1.81-8.13), <0.0001
2.36 (1.23-4.51), 0.01
2.34 (1.29-4.27), <0.01
2.16 (1.42-3.28), <0.001
2.02 (1.28-3.19), <0.01
1.79 (1.15-2.79), <0.01
1.72 (1.12-2.64), 0.01
0.95 (0.62-1.48)
0.31 (0.12-0.78)
1 0.02
1.97 (1.05-3.69), 0.03
1 2 4 6 80 3 5 7 9

Risk factors for acute renal failure:multivariate analysis
Renal organ dysfunction at inclusion
Diabetes
ARDS at inclusion
Volume of fluids (first 36h) > 8.4 L
High doses of vasoactive drugs at inclusion
Male gender
SAPS II at inclusion > 50 points
Indication of fluids: Sepsis
Trauma
Others
Use of starches
Use of plasma
Use of albumin
ORFavor ARF
Adjusted OR, p
3.73 (1.75-7.97), <0.0001
2.12 (1.10-4.10), 0.03
2.29 (1.25-4.20), <0.01
1.88 (1.22-2.91), <0.01
1.97 (1.24-3.14), <0.01
1.81 (1.15-2.85), <0.01
1.79 (1.16-2.76), <0.01
1.05 (0.67-1.64)
0.33 (0.13-0.85)
1 0.02
1.57 (1.03-2.39), 0.04
1.66 (1.06-2.61), 0.03
1.76 (1.02-3.04), 0.04
1 2 4 6 80 3 5 7 9
Renal organ dysfunction at inclusion
Diabetes
ARDS at inclusion
Volume of fluids (first 36h) > 8.4 L
High doses of vasoactive drugs at inclusion
Male gender
SAPS II at inclusion > 50 points
Indication of fluids: Sepsis
Trauma
Others
Use of starches
Use of plasma
Use of albumin
ORFavor ARF
Adjusted OR, p
3.73 (1.75-7.97), <0.0001
2.12 (1.10-4.10), 0.03
2.29 (1.25-4.20), <0.01
1.88 (1.22-2.91), <0.01
1.97 (1.24-3.14), <0.01
1.81 (1.15-2.85), <0.01
1.79 (1.16-2.76), <0.01
1.05 (0.67-1.64)
0.33 (0.13-0.85)
1 0.02
1.57 (1.03-2.39), 0.04
1.66 (1.06-2.61), 0.03
1.76 (1.02-3.04), 0.04
1 2 4 6 80 3 5 7 9

RiskRisk factorsfactors for ARDS: for ARDS: multivariatemultivariate analysisanalysis
Volume of expander > 1.3 L/d
X ray score > 2
Sepsis as indication of fluids
SAPS II > 50 points
Use of colloids
Age > 63 years
Adjusted OR, p
9.03 (4.30-18.90), <0.0001
4.36 (2.42-7.84), <0.0001
1.49 (0.84-2.65), 0.17
1.25 (0.70-2.25), 0.45
1.19 (0.51-2.78), 0.68
0.51 (0.28-0.93), 0.03
OR
Favour ARDS
1 2 4 60 8 10 12

Risk factors for mortality:multivariate analysis
SAPS II at inclusion > 50 points
Fatal underlying disease
High doses of vasoactive drugs at inclusion
Medical admission
Volume of expander (first 36h) > 3.7L
ARDS at inclusion
Use of colloids
Adjusted OR, p
4.89 (3.40-7.03), <0.0001
2.09 (1.45-3.00), <0.0001
1.81 (1.20-2.75), < 0.001
1.74 (1.16-2.62), <0.01
1.53 (1.06-2.21), 0.02
1.73 (0.98-3.06), 0.06
1.57 (0.97-2.55), 0.07
ORFavor mortality
1 2 4 60 3 5 7
SAPS II at inclusion > 50 points
Fatal underlying disease
High doses of vasoactive drugs at inclusion
Medical admission
Volume of expander (first 36h) > 3.7L
ARDS at inclusion
Use of colloids
Adjusted OR, p
4.89 (3.40-7.03), <0.0001
2.09 (1.45-3.00), <0.0001
1.81 (1.20-2.75), < 0.001
1.74 (1.16-2.62), <0.01
1.53 (1.06-2.21), 0.02
1.73 (0.98-3.06), 0.06
1.57 (0.97-2.55), 0.07
ORFavor mortality
1 2 4 60 3 5 7ORFavor mortality
1 2 4 60 3 5 7
Experts recommendations
SCCM 2004SCCM 2004Isotonic crystalloids or iso-oncotic colloidsare equally effective when titrated to thesame hemodynamic end points.
SurvivingSurviving SepsisSepsis CampaignCampaignUse crystalloids or colloids.
ATSconsensus statement

For a same pric€ in 2005...
79 L
9 L4 L
0.5 L
ALB 4% Starches Gelatin Saline















![MEMOIRE - Tlemcendspace.univ-tlemcen.dz/bitstream/112/15396/1/Modelisation-des... · Table Des Figures Figure 1 : Spectre donnant les dimensions des colloïdes [9]. 3 Figure (1.1)](https://img.pdfslide.net/doc/110x75/5fae4f446cd5ab65fb77f3b4/memoire-table-des-figures-figure-1-spectre-donnant-les-dimensions-des-collodes.jpg)













![La spectrométrie à écho de spins neutrons€¦ · composés magnétiques désordonnés [3] ou encore la physico-chimie (colloïdes, microémulsions.. .) [4]. Mais le SES peut également](https://img.pdfslide.net/doc/110x75/605ff5a1453fdc615d66e63e/la-spectromtrie-cho-de-spins-neutrons-composs-magntiques-dsordonns.jpg)