Embed Size (px)
Citation preview

1
Colorectal Cancer
Sal Bottiglieri, PharmD, BCOPClinical Oncology Pharmacist, GI & Head & Neck Clinics
Moffitt Cancer Center, Tampa, FL
Disclosures
• Dr. Bottiglieri has no relevant financial disclosures.

2
Learning Objectives
• Describe the epidemiology, risk factors, and pathology of colorectal cancer.
• Discuss the screening, diagnosis, and staging for colorectal cancer.
• Outline typical treatment regimens for adjuvant and metastatic colorectal cancers.
• Describe the side effects and monitoring parameters associated with with oral chemotherapy and targeted treatments in colorectal cancer.
• Discuss counseling strategies to maximize compliance and adherence.
Colorectal Cancer (CRC) Epidemiology• Third most common cause of cancer
– Incidence 2016: 70,820 Men & 63, 670 Women
• Third most common cause of cancer related deaths– Mortality 2016: 26,020 Men & 23,170 Women
– 5 year survival: 65.1%• Localized: 90.1%
• Metastatic: 13.5%
• Stage at presentation– Localized: 39%
– Regional: 35%
– Metastatic: 21%
Siegel RL, et al. CA Cancer J Clin 2016; 66: 7‐30.National Cancer Institute: SEER Database. Available at: https://seer.cancer.gov/statfacts/html/colorect.html. Accessed: 2/5/2017.
3
Risk Factors
• Obesity & Physical Inactivity• Diet• Smoking• Heavy Alcohol Use• Age > 50 years old• History of colorectal polyps• Inflammatory bowel disease• African American race and Ashkenazi Jews• Family history of CRC• Genetic risk factors
– Familial adenomatous polyposis (FAP)– Lynch syndrome– Rare disorders
Colorectal Cancer Risk Factors; American Cancer Society. Available at: https://www.cancer.org/cancer/colon‐rectal‐cancer/causes‐risks‐prevention/risk‐factors.html. Accessed on: 2/5/17.
Colorectal Cancer Screening
• Average Risk: Age ≥ 50 years old– Colonoscopy every 10 years
• If adenoma or sessile polyp rescreen every 3‐5 years
– Flexible sigmoidoscopy every 5‐10 years• +/‐ Guaiac‐based or immunochemical‐base testing at 3 year intervals
– CT Colonography every 5 years
– Stool Testing• Guaiac (FOBT) or immunochemical‐based testing (FIT) annually
• DNA‐based testing every 3 years
NCCN. Colorectal Cancer Screening. V.2.2016. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colorectal_screening.pdf. Accessed on: February 11, 2017.

4
Colorectal Cancer Screening
• Inflammatory bowel disease (IBD)
– 8‐10 years after IBD diagnosis colonoscopy
• Family History
– First degree relative diagnosed <60 years old or two first degree relatives diagnosed at any age
• Colonoscopy every 5 years at age 40 or 10 years before relatives age of diagnosis
• High Risk Syndromes
NCCN. Colorectal Cancer Screening. V.2.2016. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colorectal_screening.pdf. Accessed on: February 11, 2017.
Multitarget Stool DNA Testing
• Stool DNA Test:– Methylated BMP3 & NDRG4– Mutated KRAS– Beta‐actin
• Asymptomatic persons between 50‐84 with average risk (N=9989)• Stool sample and colonoscopy within 90 days
– No dietary or medication restrictions– FIT and DNA tests on stool samples in blinded fashion
• 65 (0.7%) had colon cancer on colonoscopy• 757 (7.6%) had precancerous lesions on colonoscopy• Sensitivity Analysis
– Sensitivity Colon Cancer: 92.3% vs. 73.8% (DNA vs. FIT p=0.002)– Sensitivity precancerous: 42.4% vs. 23.8% (DNA vs. FIT p<0.001)
• Specificity Analysis– 86.6% vs. 94.9% (p<0.001)
Imperiale TF, et al. N Engl J Med 2014; 370(14): 1287‐97.

5
Symptoms
Blood in the stool
Narrow stools
Change in bowel habits
Unexplained stomach discomfort
Frequent gas pains
Unexplained weight loss
Rectal Cancer: Straining
during bowel movements
Libutti SK, et al. Colon Cancer. In Cancer: Principle & Practice of Oncology, edited by DeVita VT Jr., et al., 1232‐1285. Philadelphia: Lippincott Williams & Wilkins, 2008.
Diagnosis
• Physical exam and history• Digital rectal exam• Stool Testing• FOBT or FIT or DNA Colonoscopy if positive• Colonoscopy or Sigmoidoscopy with biopsy• Pathology
– Adenocarcinoma– Signet ring carcinoma– Mucinous carcinoma– High grade neuroendocrine– Medullary carcinoma
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.Libutti SK, et al. Colon Cancer. In Cancer: Principle & Practice of Oncology, edited by DeVita VT Jr., et al., 1232‐1285. Philadelphia: Lippincott Williams & Wilkins, 2008.
6
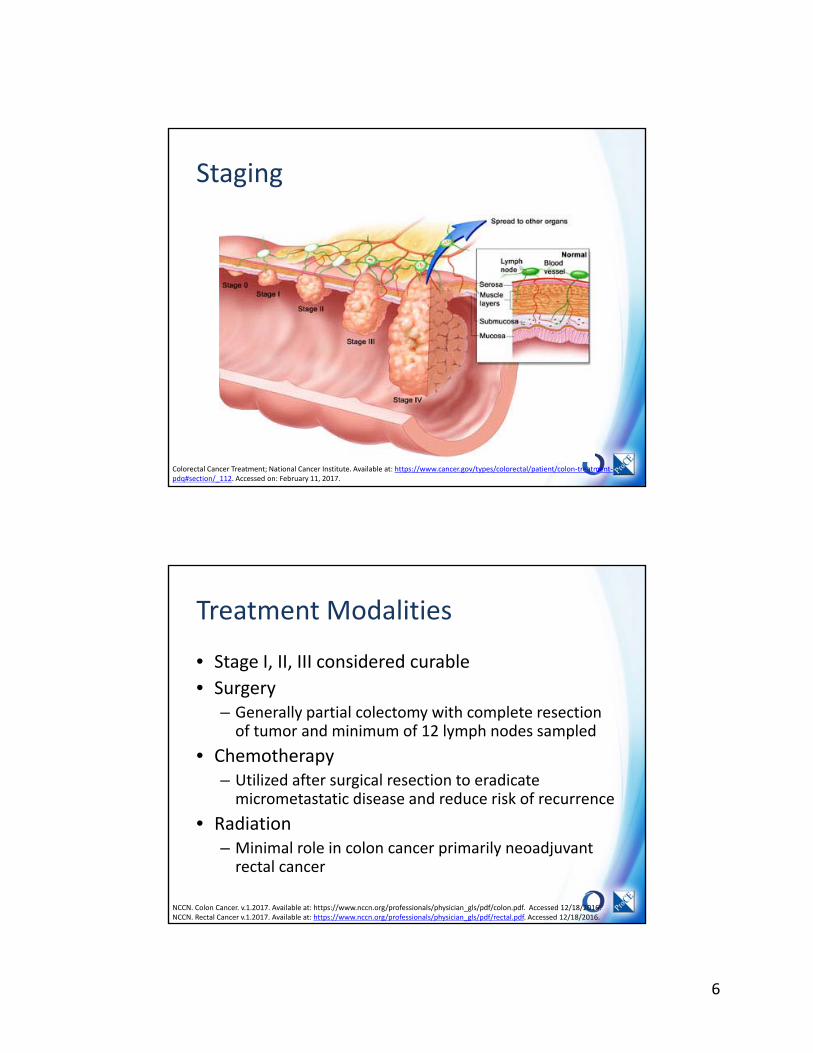
Staging
Colorectal Cancer Treatment; National Cancer Institute. Available at: https://www.cancer.gov/types/colorectal/patient/colon‐treatment‐pdq#section/_112. Accessed on: February 11, 2017.
Treatment Modalities
• Stage I, II, III considered curable
• Surgery– Generally partial colectomy with complete resection of tumor and minimum of 12 lymph nodes sampled
• Chemotherapy– Utilized after surgical resection to eradicate micrometastatic disease and reduce risk of recurrence
• Radiation– Minimal role in colon cancer primarily neoadjuvantrectal cancer
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
7
Surgery
• Curative
– Partial or total colectomy
– Primary and regional lymph node removal
– Isolated liver/lung metastatic resection
• Palliative
– Decrease bleeding
– Relieve obstruction
– Increase QOL
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
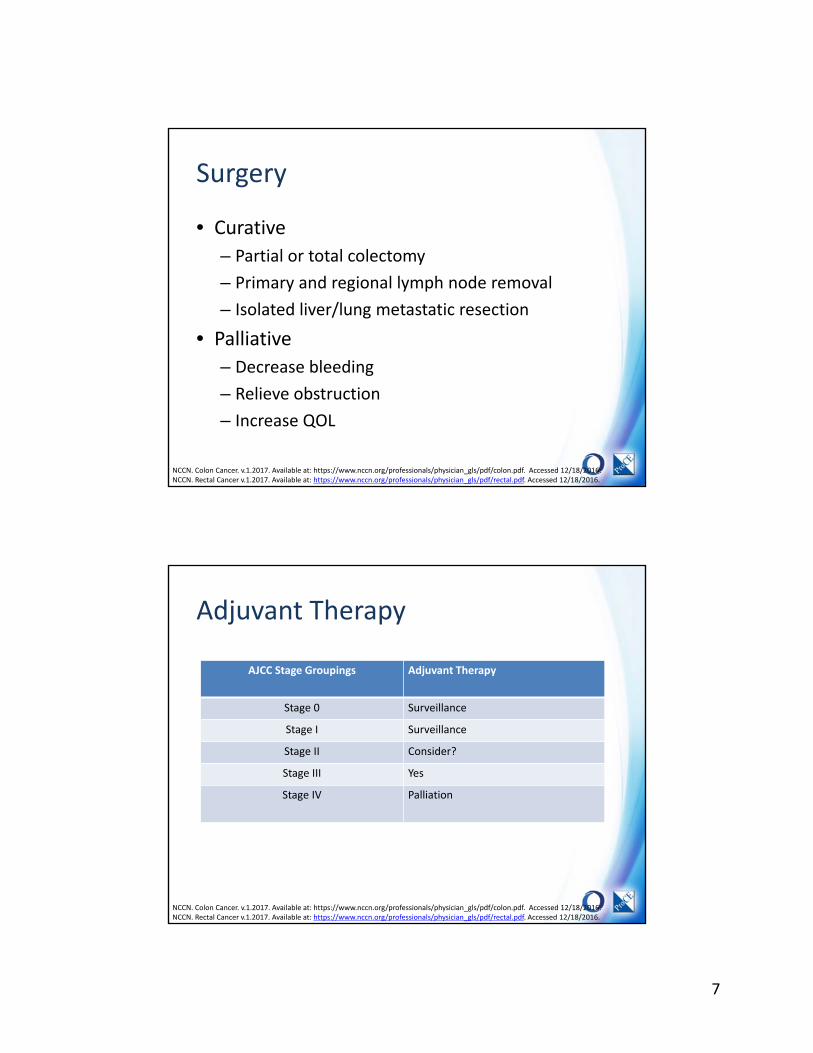
Adjuvant Therapy
AJCC Stage Groupings Adjuvant Therapy
Stage 0 Surveillance
Stage I Surveillance
Stage II Consider?
Stage III Yes
Stage IV Palliation
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
8
Adjuvant Therapy Summary
• Initiate 4‐8 weeks after surgery• Colon
– Stage II• Fluorouracil/Leucovorin (Roswell Park or Simplified)• Modified FOLFOX6 (Fluorouracil/Leucovorin/Oxaliplatin)• CAPEOX (Capecitabine/Oxaliplatin)
– Stage III (6 months)• Modified FOLFOX6*• CAPEOX* • FLOX (Bolus Fluorouracil/Leucovorin/Oxaliplatin)
• Rectal (6 months perioperative chemotherapy)– Chemoradiation: Fluorouracil or Capecitabine– Chemotherapy: Follow colon
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
Mosaic Trial: Role of Adjuvant Therapy
• 3‐Year Outcomes– Disease‐free Survival (DFS) Stage II and III
• 78.2% versus 72.9% (FOLFOX versus Fluorouracil/Leucovorin, p=0.002)
– Stage II: FOLFOX and Simplified 5FU/LV has no difference in risk of recurrence (HR:0.8; 95% CI, 0.56‐1.15)
– Stage III: FOLFOX confers 23% risk reduction versus Fluorouracil/Leucovorin alone (HR: 0.77, p=0.002)
– Risk of recurrence similar for stage II and III with FOLFOX adjuvant therapy (p=0.77)
• 6‐Year Outcomes– DFS 73.3% versus 67.4% Stage II and III, HR: 0.8; 95% CI, 0.68‐0.93
(FOLFOX vs 5FU/LV)– Overall Survival Stage III: 72.9% vs 68.7%, HR: 0.8; 95% CI, 0.65‐0.97
(FOLFOX vs 5FU/LV)– No difference in DFS and OS for stage II disease
Andre T, et al. N Engl J Med 2004; 350: 2343‐51.Andre T, et al. J Clin Oncol 2009; 27(19): 3109‐3116.

9
Adjuvant Chemotherapy: Stage II Colon Cancer• Clinical Controversy• Consider in the following patients
– Less than 12 lymph nodes analyzed– Poorly differentiated histology– Lymphatic/vascular or perineural invasion– Bowel obstruction or perforation on presentation– Close, intermediate, or positive margins
• Microsatellite Instability High do not benefit from adjuvant therapy
• Minimal improvement in survival ≤ 5%
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
Adjuvant Therapy: 5 Year Survival Data
Stratification Group Chemotherapy No Chemotherapy
Hazard Ratio
Stage IINo Poor Prognosis: 69%
70% 69.5% HR: 1.02; 95% CI, 0.84‐1.25
Stage IIPoor Prognosis: 57%
56.7% 56.1% HR: 1.03; 95% CI, 0.94‐1.13
Stage III: 44% 48.9% 35.2% HR: 0.64; 95% CI, 0.6‐0.67
O’Connor ES, et al. J Clin Oncol 2011; 29: 3381‐3388.
10
Mismatch Repair
• Defective mismatch repair (dMMR) in 15% of CRC– Microsatellite Instability (MSI)
– Loss of protein products for genes involved in DNA mismatch repair (MMR)
• MLH1, MSH2, MSH6, & PMS2
• Tumor features– Proximal colon predominance, poor differentiation, mucinous histology, lymphocytic infiltration, diploid DNA content
• Improved stage independent survival
Ionov Y, et al. Nature 1993; 363: 558‐61.Thibodeau SN, et al. Science 1993; 260: 816‐19.
Adjuvant Regimens
• Roswell Park– Fluorouracil (5FU) 500mg/m2 & Leucovorin (LCV) 500mg/m2 IV weekly X 6 weeks
• Cycled every 8 weeks X 3 cycles
• CapeOx– Oxaliplatin 130mg/m2 IV over 2 hours day 1, Capecitabine 1000mg/m2 PO twice daily
days 1‐14 every 3 weeks X 8 cycles
• Capecitabine 1250mg/m2 PO twice daily days 1‐14 every 3 weeks X 8 cycles• FLOX
– Fluorouracil 500mg/m2 IV bolus, LCV 500mg/m2 IV weekly X 6weeks– Oxaliplatin 85mg/m2 IV weeks 1, 3, and 5– Cycled every 8 weeks X 3 cycles
• FOLFOX – Oxaliplatin 85mg/m2 & LCV 400mg/m2 over 2 hours, 5FU 400mg/m2 IV bolus Day 1– 5FU 2400mg/m2 IV over 46 hours– Cycled every 14 days X 12 cycles
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
11
Adjuvant Therapy Counseling
Fluorouracil
• Diarrhea– Loperamide– Oral fluids– Bland foods
• Mucositis– Oral fluids– Soft foods– Mouth rinse
• Hand Foot Syndrome– Oral fluids– Urea based creams
• Photosensitivity
Oxaliplatin
• Neutropenia & Thrombocytopenia
• Neuropathy
• Cold sensitivity
– Avoid cold objects or food/drink
Monitoring:•CBC and CMP prior to treatment•Skin/Mouth examination•Neurotoxicity examination
Metastatic Colorectal Cancer: Initial Therapy
Intensive Therapy Options
• FOLFOX +/‐ Bevacizumab• CAPEOX +/‐ Bevacizumab• FOLFOX + Cetuximab or
Panitumumab– KRAS Wild Type & Left Sided Tumors
• Fluorouracil/Leucovorin/Irinotecan (FOLFIRI) +/‐ Bevacizumab
• FOLFIRI + Cetuximab or Panitumumab
– KRAS Wild Type & Left Sided Tumors
• Fluorouracil/Leucovorin/Oxaliplatin/Irinotecan (FOLFOXIRI) +/‐Bevacizumab
• Fluorouracil/Leucovorin +/‐Bevacizumab
• Capecitabine +/‐ Bevacizumab
Non‐intensive Therapy Options
• Fluorouracil/Leucovorin +/‐ Bevacizumab
• Capecitabine +/‐Bevacizumab
• Cetuximab or Panitumumab– KRAS Wild Type & Left Sided Tumors
• Nivolumab or Pembrolizumab– dMMR or MSI‐H
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
12
Bevacizumab
• Anti‐ vascular endothelial growth factor (VEGF) antibody that inhibits tumor angiogenesis
• Approved: first or second line with 5FU chemotherapy
• 5mg/kg every 2 weeks or 7.5mg/kg every 3 weeks
• In combination with FOLFOX or XELOX– Improved progression free survival (PFS)
• In combination with FOLFIRI– Improved PFS & Overall Survival (OS)
• Toxicities– Hypertension, Bleeding, Venous Thromboembolism, Wound healing impairment, Proteinuria
Drugs 2008. 68 (4):487‐506
Cetuximab• Binds to and blocks epidermal growth factor receptor (EGFR)• Approval:
– KRAS wild‐type metastatic colorectal cancer (mCRC)– In combination with FOLFIRI in first line therapy– In combination with irinotecan in refractory disease– Single in refractory disease
• 400mg/m2 IV infusion once over 120 minutes, then 250mg/m2 IV over 60 minutes weekly
• In combination with irinotecan– PFS=4.1 months, RR=22.9%
• Monotherapy in patients who have progressed on irinotecan– OS=6.1 months– One‐year survival=21%
• Toxicities:– Infusion reactions, Acneiform rash, Hypomagnesemia, Fatigue,
Abdominal Pain, & Diarrhea
Anti‐Cancer Drugs 2008. 19(2):99‐113Erbitux ® (package insert). Indianapolis, IN: Eli Lilly; 2016.

13
Panitumumab• Fully human antibody• Approved for mCRC with FOLFOX chemotherapy in first line or as monotherapy in refractory disease
• 6mg/kg IV over one hour every 14 days• Multi‐center trial vs. best supportive care
– PFS=96 v 60 days– 75% pts in BSC crossed over– No difference in OS, RR or symptoms
• Toxicities– Infusion reactions, Acneiform rash, Hypomagnesemia, Fatigue, Abdominal pain, & Diarrhea
Clin Cancer Res 2008; 14(5):1296‐1302.Vectibix ® (package insert). Thousand Oaks, CA: Amgen; 2016
EGFR Monitoring & Management
• Acneiform Rash– Grade 1: Continue EGFR agent
• Topical 1‐2.5% hydrocortisone cream or clindamycin 1% gel
– Grade 2: Continue EGFR agent• Topical 2.5% hydrocortisone cream or clindamycin 1% gel or pimecrolimus 1% cream
• Doxycycline 100mg PO BID or Minocycline 100mg PO BID
– Grade 3 or 4: Hold EGFR agent• As above plus methylprednisolone dose pack
• Diarrhea Management• Electrolytes periodically• Infusion reactions
Hirsch V. Curr Oncol. 2011; 18(3): 126‐138.
14
Second Line Therapy of Colorectal Cancers
Previous Oxaliplatin Therapy
• FOLFIRI OR Irinotecan +/‐– Bevacizumab OR– Ziv‐aflibercept OR– Ramucirumab
• KRAS WT: FOLFIRI OR Irinotecan +– Cetuximab OR– Panitumumab
• MSI‐H: Nivolumab or Pembrolizumab
Previous Irinotecan Therapy
• FOLFOX OR CAPEOX +/‐ Bevacizumab
• KRAS WT: Irinotecan +– Cetuximab OR
– Panitumumab
• MSI‐H: Nivolumab or Pembrolizumab
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.
Ziv‐Aflibercept• Recombinant fusion protein• Approval: Second line mCRC in combination
with FOLFIRI following progression on first line FOLFOX
– Median OS: 13.5 vs. 12.06 months (FOLFIRI + ziv‐aflibercept vs. FOLFIRI + Placebo) p=0.0032
• Decoy receptor:– Vascular endothelial growth factor‐A (VEGF‐A),
VEGF‐B and Placental Growth Factor (PlGF)
• Administer via IV infusion over one hour• Boxed warnings
– Hemorrhage– GI perforation– Compromised wound healing
• Hold 4 weeks prior and post surgery
• Warnings and precautions:– Fistula, hypertension, thromboembolic events,
proteinuria, neutropenia, diarrhea, reversible posterior leukoencephalopathy syndrome
Abraham J, et al. Commun Oncol. 2012; 9: 120‐1.

15
Ramucirumab
• Fully human IgG‐1 monoclonal antibody– Binds to VEGF receptor 2 (VEGFR‐2)
• Indications/dosage:– Single agent or combination with paclitaxel for gastric or gastro‐esophageal adenocarcinoma
(8mg/kg IV every two weeks)– Combination with docetaxel in non‐small cell lung cancer (10mg/kg IV every three weeks)– Combination with FOLFIRI in mCRC (8mg/kg IV every two weeks)
• Median OS: 13.3 vs. 11.7 months (FOLFIRI + Ramucirumab vs. FOLFIRI + Placebo)
• Administration:– Pre‐medicate with IV anti‐histamine
• If Grade 1 or 2 infusion reaction add acetaminophen and dexamethasone and decrease rate by 50%
– Administer dose in normal saline with final volume of 250ml over one hour
• Boxed warnings:– Hemorrhage– Gastrointestinal perforation– Impaired wound healing
• Warnings and precautions:– Arterial thromboembolic events, hypertension, infusion reactions, RPLS, proteinuria, thyroid
dysfunction, cirrhosis
Cyramza ® (package insert). Indianapolis, IN: Eli Lilly; 2016.
mCRC: Refractory Treatment Options• Regorafenib
• Trifluridine + Tipiracil
• Nivolumab or Pembrolizumab (MSI‐H)
• Clinical trial
• Best supportive care (BSC)
NCCN. Colon Cancer. v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf. Accessed 12/18/2016.NCCN. Rectal Cancer v.1.2017. Available at: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed 12/18/2016.

16
Regorafenib• Multikinase inhibitor
– Inhibits VEGFR, RET, KIT, PDGFR, BRAF tyrosine kinases– Fluorinated phenyl ring added to sorafenib
• Indications– mCRC post progression of chemotherapy & targeted therapies– Gastrointestinal stromal tumor (GIST) post progression with imatinib and sunitinib
• Dose: 160mg PO daily days 1‐21 every 28 day cycle– Take with a low fat breakfast (<30% fat)
• Boxed Warnings– Severe and fatal hepatotoxicity
• Warnings/Precautions– Hemorrhage, dermatologic toxicity, hypertension, cardiac ischemia, reversible posterior
leukoencephalopathy syndrome (RPLS), GI perforation, and wound healing impairment– Avoid use in Child Pugh C
• Drug Interactions– Regorafenib inhibits: CYP2B6, 2C8, 2C9, 2C19, and 3A4– M2 metabolite inhibits: 2C8, 2C9, 2D6, and 3A4– Avoid CYP3A4 inhibitors and inducers
Stivarga ® (package insert). Whippany, NJ: Bayer HealthCare Pharmaceuticals; 2016.
CORRECT Phase III TrialMCRC adenocarcinoma
Received locally and currently approved standard therapies
Known KRAS status
(N=760)
MCRC adenocarcinoma
Received locally and currently approved standard therapies
Known KRAS status
(N=760)
Regorafenib + BSC
(N=505)
Regorafenib + BSC
(N=505)
Placebo + BSC
(N=255)
Placebo + BSC
(N=255)
End Point Regorafenib Placebo Hazard Ratio P Value
Median OS (Months) 6.4 5 0.77; 95% CI, 0.64‐0.94
0.0052
Median PFS (Months) 1.9 1.7 0.49; 95% CI, 0.42‐0.58
<0.0001
CR+PR=ORR (%) 1 0.4 0.19
Disease control= PR+SD (%)
41 15 <0.0001
Patients required exposure if available in each site: fluoropyrimidine, oxaliplatin, irinotecan, bevacizumab, and cetuximab or panitumumab (KRAS WT)Randomization: 2:1 ratio (Regorafenib: placebo)Stratification:•Previous anti‐VEGF therapy•Time from diagnosis of metastatic disease•Geographical regionKRAS MT:•51% vs. 51% (Regorafenib vs. Placebo)•BRAF MT 4% vs 2%Number of previous therapies:•1‐2: 27% vs. 15%•3: 25% vs. 28%•≥ 4: 49% vs. 47%
Grothey A, et al. Lancet. 2013; 381: 303‐12.

17
Regorafenib ToxicityAdverse Event Regorafenib + BSC
All (%) Grade 3 (%) Grade 4 (%)Placebo + BSCAll (%) Grade 3 (%) Grade 4 (%)
Any 93 51 3 61 12 2
Fatigue 47 9 <1 28 5 <1
Hand‐foot syndrome (HFS)
47 17 0 8 <1 0
Diarrhea 34 7 <1 8 1 0
Anorexia 30 3 0 15 3 0
Voice changes 29 <1 0 6 0 0
Hypertension 28 7 0 6 1 0
Mucositis 27 3 0 4 0 0
Rash 26 6 0 4 0 0
Taste alteration 7 0 0 2 0 0
Thrombocytopenia 13 3 <1 2 <1 0
Hyperbilirubinemia 9 2 0 2 1 0
Proteinuria 7 1 0 2 <1 0
Anemia 7 2 <1 2 0 0
Hypophosphatemia 5 4 0 <1 <1 0
• Death related to adverse events (N=8)
• One fatality due to drug induced liver injury
• Grade 1‐5 hemorrhage: 21%
• Fatal hemorrhage: 0.6% (CORRECT & GRID)
• GI perforation: 0.6%• Hypertensive crisis: 0.25%
Grothey A, et al. Lancet. 2013; 381: 303‐12.Crona DJ, et al. Ann Oncol. 2013; 47(12): 1685‐96.
Regorafenib Dose ModificationsToxicity Dose Modification
Hepatotoxicity•Grade 3 AST and or ALT elevation•AST or ALT > 20 X ULN•AST or ALT > 3 X ULN and bilirubin > 2 X ULN•Reoccurrence of AST or ALT > 5 X ULN despite dose reduction to 120mg
•Withhold dose until recovered, resume at 120mg dose*•Permanently discontinue•Permanently discontinue•Permanently discontinue*If recurrence of AST or ALT > 5 X ULN permanently discontinue
Dermatological Toxicity•Grade 2 HFS•Grade 3 HFS
•120mg daily for first occurrence•Interrupt therapy X 7 days then reduce to 120mg daily•If recurrence of grade 2‐3 HFS may reduce to 80mg daily
Grade 2 hypertension Interrupt therapy
Additional grade 3 or 4 events Interrupt therapy, on recovery reduce to 120mg daily
GI perforation or fistulaSevere or life threatening hemorrhageWound dehiscence
Permanently discontinue
RPLS Permanently discontinue
Failure to tolerate 80mg dose Permanently discontinue
Stivarga ® (package insert). Whippany, NJ: Bayer HealthCare Pharmaceuticals; 2016.

18
Regorafenib MonitoringToxicity Monitoring Parameter Outcome and Frequency
Hepatotoxicity Liver function tests (LFT) Baseline then every 2 weeks X 2 months then monthly
Hemorrhage Signs and symptoms of bleeding or bruising
Permanently discontinue in patients with severe or life threatening hemorrhage
Dermatologic Signs and symptoms of rash, erythema, pain, blisters or swelling on palms of hands or soles of feet
Modify dose or permanently discontinue depending on severity
Hypertension Blood pressure Weekly X 6 weeks then monthly, temporarily or permanently withhold for severe or uncontrolled hypertension
Cardiac Ischemia Physical Exam/Patient Report Withhold in patient who develop new or acute onset cardiac ischemia
RPLS RPLS evaluation Perform in any patient presenting with seizures, headache, visual disturbances, confusion or altered mental status. Permanently discontinue
GI perforation or fistula
Physical examination Permanently discontinue
Wound Healing Examination prior to surgery Stop treatment two weeks prior to surgery, reinitiate after surgery based on adequate healing
Crona DJ, et al. Ann Oncol. 2013; 47(12): 1685‐96.
Toxicity Management• Fatigue
– Conduct Brief Fatigue Inventory– Check thyroid function– Consider dosing at night
• HFS– Full skin exam prior to initiation– Keratolytic agents
• Urea 10% cream• Salicylic acid 3% cream• Ammonium lactate 12% cream
– Topical steroids• Clobetasol 0.05% ointment• Betamethasone ointment
– Topical analgesics (lidocaine cream)
• Mucositis: Oral care• Diarrhea
– Loperamide, Atropine/Diphenoxylate, Tincture of opium– IV fluids– Octreotide
• Hypertension– Consider angiotensin‐converting enzyme inhibitors or beta blockers
Hofheinz R‐D, et al. Oncol Res Treat. 2015; 38: 300‐308.

19
Regorafenib Counseling
• Take every morning with low fat breakfast– 2 slices of white toast, 1 tablespoon of low‐fat margarine, 1 tablespoon of jelly and 8 ounces
of skim milk– Do not take two doses in one day if a dose is missed– Swallow whole, do not crush or chew– Open one bottle at a time
• Liver function monitoring and risk of liver damage• Blood pressure monitoring at home
– Signs of hypertension: headache & lightheadedness
• Diarrhea– Loperamide for initial symptoms, oral fluid intake, avoid exacerbating foods
• HFS– Symptoms: Redness, pain, blisters, and/or bleeding and swelling on their palmar and plantar
surfaces– Wear comfortable shoes, avoid stress to hands and feet, keep skin moisturized, avoid exposure
to hot water, and vigorous exercise
• Seek attention for severe bleeding, chest pain, or dyspnea• Inform provider of any recent or pending surgery• Inform their pharmacist of any new medications• Appropriate contraception (pregnancy category D)
Crona DJ, et al. Ann Oncol. 2013; 47(12): 1685‐96.
Trifluridine + Tipracil (TAS‐102)
• Oral combination thymidine nucleic acid analogue (Trifluridine) and thymidine phosphorylase inhibitor (Tipracil)
• 35mg/m2 PO twice daily days 1‐5 and 8‐12 every 28 day cycle after meals– Do no initiate a cycle if ANC< 1500, Platelets <75,000 or Grade 3 or 4 non‐
hematologic toxicity– Hold within a cycle if ANC<500, febrile neutropenia (FN), platelets <50,000, or
Grade 3 or 4 non‐hematologic toxicity
• Supplied as 15mg and 20mg tablets• Warnings/Precautions:
– Myelosuppression– Embryo‐Fetal Toxicity
• Monitoring– CBC with Differential Day 1 and 15 X 2 cycles then monthly– CMP monthly– Physical exam monthly
• Consider monitoring patient with CrCl 30‐59 ml/min closer
Mayer RJ, et al. N Engl J Med 2015; 372: 1909‐19.Lonsurf ® (package insert) . Princeton, NJ: Taiho Oncology; 2016.

20
RECOURSE Phase III TrialMCRC adenocarcinoma
At least two previous standard therapies
Known KRAS status
(N=800)
MCRC adenocarcinoma
At least two previous standard therapies
Known KRAS status
(N=800)
TAS‐102 + BSC
(N=534)
TAS‐102 + BSC
(N=534)
Placebo + BSC
(N=266)
Placebo + BSC
(N=266)
End Point TAS‐102 Placebo Hazard Ratio P Value
Median OS (Months) 7.1 5.3 0.68; 95% CI, 0.58‐0.81
<0.001
Median PFS (Months) 2 1.7 0.48; 95% CI, 0.41‐0.57
<0.001
CR+PR=ORR (%) 1.6 0.4 0.29
Disease control= PR+SD (%)
44 16 <0.001
Mayer RJ, et al. N Engl J Med 2015; 372: 1909‐19.
Patients required exposure: fluoropyrimidine, oxaliplatin, irinotecan, bevacizumab, and cetuximab or panitumumab (KRAS WT)Randomization: 2:1 ratio (TAS‐102: placebo)Stratification:•KRAS status•Time from diagnosis of metastatic disease•Geographical regionKRAS MT:•51% vs. 51% (TAS‐102 vs. Placebo)Previous therapies:•All patients received previous fluoropyrimidine, oxaliplatin, and irinotecan•Bevacizumab: 100% vs. >99%•Anti‐EGFR: 52% vs. 54%•Regorafenib: 17% vs. 20%
TAS‐102 Toxicity DataAdverse Event TAS‐102 + BSC
All (%) Grade ≥3 (%) Placebo + BSCAll (%) Grade ≥3 (%)
Any 98 69 93 52
Nausea 48 2 24 1
Vomiting 28 2 14 <1
Decreased Appetite 39 4 29 5
Fatigue 35 4 23 6
Diarrhea 32 3 12 <1
Asthenia 18 3 11 3
Febrile Neutropenia 4 4 0 0
Stomatitis 8 <1 6 0
HFS 2 0 2 0
Neutropenia 67 38 <1 0
Leukopenia 77 21 5 0
Anemia 77 18 33 3
Thrombocytopenia 42 2 27 <1
Mayer RJ, et al. N Engl J Med 2015; 372: 1909‐19.
21
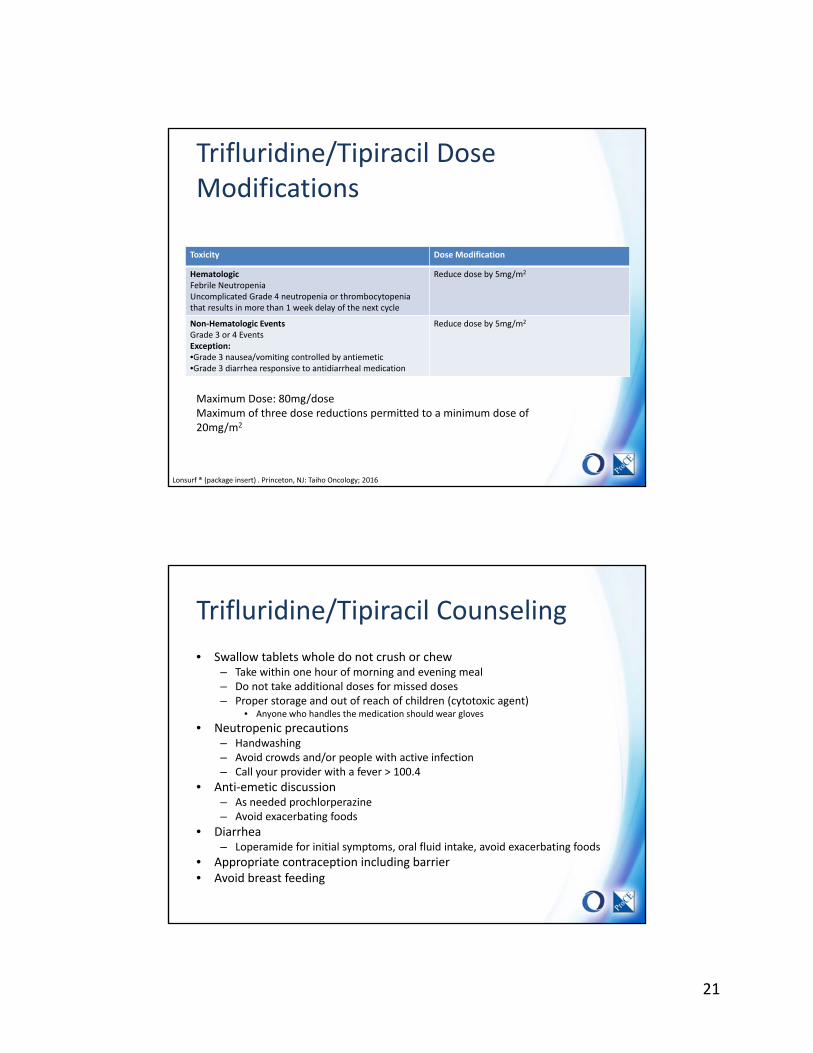
Trifluridine/Tipiracil Dose Modifications
Toxicity Dose Modification
HematologicFebrile NeutropeniaUncomplicated Grade 4 neutropenia or thrombocytopenia that results in more than 1 week delay of the next cycle
Reduce dose by 5mg/m2
Non‐Hematologic EventsGrade 3 or 4 EventsException:•Grade 3 nausea/vomiting controlled by antiemetic•Grade 3 diarrhea responsive to antidiarrheal medication
Reduce dose by 5mg/m2
Lonsurf ® (package insert) . Princeton, NJ: Taiho Oncology; 2016
Maximum Dose: 80mg/doseMaximum of three dose reductions permitted to a minimum dose of 20mg/m2
Trifluridine/Tipiracil Counseling
• Swallow tablets whole do not crush or chew– Take within one hour of morning and evening meal– Do not take additional doses for missed doses– Proper storage and out of reach of children (cytotoxic agent)
• Anyone who handles the medication should wear gloves
• Neutropenic precautions– Handwashing– Avoid crowds and/or people with active infection– Call your provider with a fever > 100.4
• Anti‐emetic discussion– As needed prochlorperazine– Avoid exacerbating foods
• Diarrhea– Loperamide for initial symptoms, oral fluid intake, avoid exacerbating foods
• Appropriate contraception including barrier• Avoid breast feeding
22
PD1 Data and MSI‐H CRC
• Pembrolizumab– KEYNOTE‐177 (Phase III)
• First line vs investigators choice
– KEYNOTE‐164 (Phase II)• Previously treated all standard therapies• 200mg IV Q3 weeks
• Nivolumab– Checkmate‐142 (Phase II)
• Previously treated or intolerance ≥ 1 therapy• Nivolumab 3mg/kg Q 2 weeks (N3)or Nivolumab 3mg/kg + Ipilimumab 1mg/kg Q 3 weeks X 4 does then Nivolumab 3mg/kg Q 2 weeks (N3 +I1)
• ORR: N3 (27%) N3+I1 (15%)
Leal AD, et al. ASCO Meeting Abstracts 2017.Le DT, et al. ASCO Meeting Abstracts 2016; 34: TPS787.Overman MJ, et al. ASCO Meeting Abstracts 2016; 34: 3501.
Conclusions
• Although the incidence and mortality of CRC is declining the disease continues to affect many Americans each year
• Optimization adjuvant therapy has improved tolerability and efficacy outcomes
• Targeted therapies have increased survival and treatment options in the metastatic setting
• The tolerability and adherence to oral therapies in mCRC can be challenging– Clinical pharmacists can be at the forefront to manage these patients
23
Colorectal Cancer
Sal Bottiglieri, PharmD, BCOPClinical Oncology Pharmacist, GI & Head & Neck Clinics
Moffitt Cancer Center, Tampa, FL