Embed Size (px)
Citation preview
Colorectal Caner
Sun Yang, BsPharm, BCPPS, APh.Department of Pharmacy PracticeChapman University School of Pharmacy

Objectives
• Discuss the etiology, clinical presentation, and risk factors associated with colon cancer
• Discuss and understand the preventive strategy in screening and early detection of colon cancer
• Discuss and understand the treatment options for various stages of colon cancer (neoadjuvant, adjuvant, and metastatic setting)
• Discuss chemotherapy, dosages, side effects and monitoring parameters commonly associated with treatment of colon cancer
Colorectal carcinomas
• Colorectal cancer A group of cancers that start in the colon or the rectum.
• More than 95 percent of colorectal cancers are adenocarcinomas that arise in cells forming glands that make mucus to lubricate the inside of the colon and rectum.
• Before a colorectal cancer develops, a growth of tissue or tumor usually begins as a noncancerous polyp on the inner lining of the colon or rectum.
• Most polyps can be found—for example, through colonoscopy—and removed before they turn into cancer.
• Rare colon and rectal cancers• May both arise from carcinoid, lymphoma, neuroendocrine, and gastrointestinal stromal
tumors.
https://www.youtube.com/watch?v=fW4Y_poPPxg

Epidemiology: FACTS IN U.S.
• 3rd most common cancer in both men and women.• 135,430 new cases estimated in year of 2017
• 95,520 colon cancer• 39,910 rectal cancer
• 50,260 deaths estimated in the year of 2017
• 5-year survival rate• The 5- and 10-year relative survival rates for colorectal cancer are 65% and 58%
respectively.• 5-year relative survival
• Localized stage: 90%• Regional stage: 71%• Distant stage: 14%
Birth to 49 50-59 60-69 70 and older Birth to death
Male 0.3 (1 in 294) 0.7 (1 in 149) 1.2 (1 in 84) 3.5 (1 in 28) 4.6 (1 in 22)
Female 0.3 (1 in 318) 0.5 (1 in 198) 0.8 (1 in 120) 3.2 (1 in 31) 4.6 (1 in 24)

Colon and Rectum
26%
26%27%
13%
6%
Overall colorectal cancer mortality has decreased slightly over the last 30 years• Improve screening and better
treatment modalities• Occurs equally in men and
women• African-Americans have the
highest colorectal cancer rates and mortality• Diet?• Genes?
Etiology-Patient case
• Neil Colon, a 35-year-old male, recently learned that his 68-year-old father was diagnosed with colon cancer. N.C. is obese and smokes a pack of cigarette per day. He loves eating out and spends most of his evening watching TV and playing video games at home. N.C would like to know the risk factors for colorectal cancer.
Risk Factors
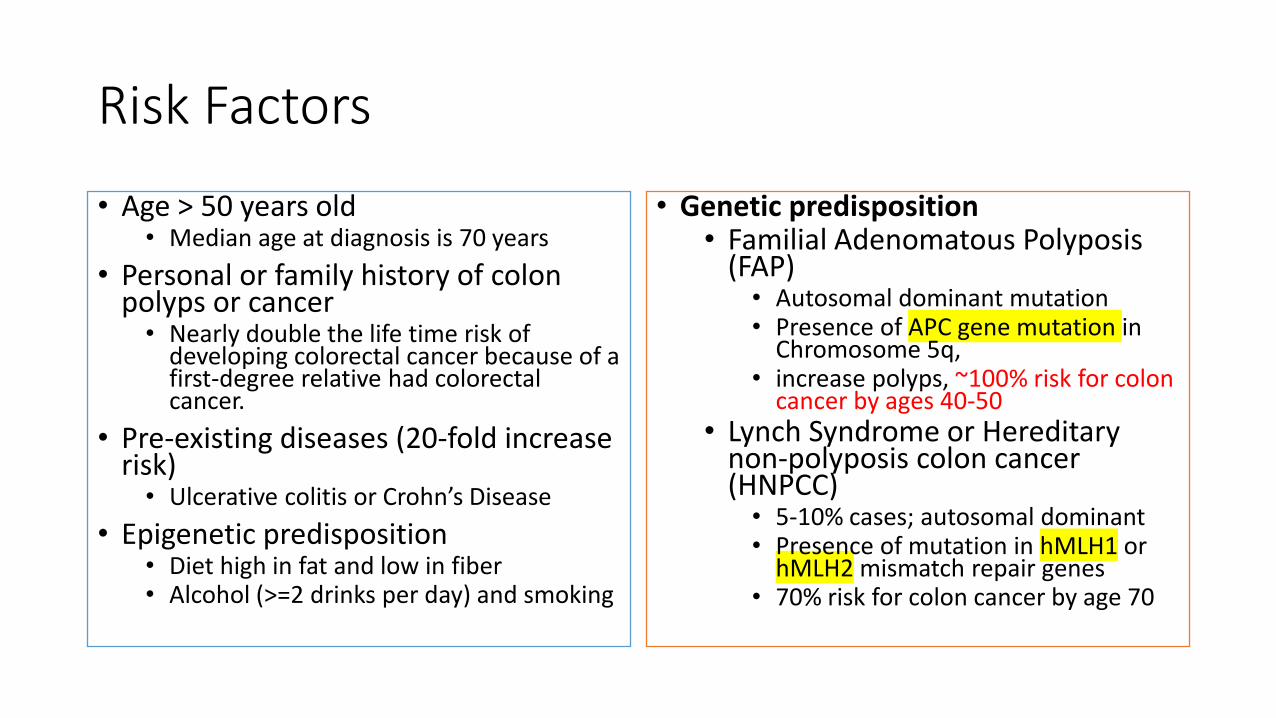
• Age > 50 years old• Median age at diagnosis is 70 years
• Personal or family history of colon polyps or cancer
• Nearly double the life time risk of developing colorectal cancer because of a first-degree relative had colorectal cancer.
• Pre-existing diseases (20-fold increase risk)
• Ulcerative colitis or Crohn’s Disease• Epigenetic predisposition
• Diet high in fat and low in fiber• Alcohol (>=2 drinks per day) and smoking
• Genetic predisposition• Familial Adenomatous Polyposis
(FAP)• Autosomal dominant mutation• Presence of APC gene mutation in
Chromosome 5q, • increase polyps, ~100% risk for colon
cancer by ages 40-50• Lynch Syndrome or Hereditary
non-polyposis colon cancer (HNPCC)
• 5-10% cases; autosomal dominant• Presence of mutation in hMLH1 or
hMLH2 mismatch repair genes• 70% risk for colon cancer by age 70
Patient case
• Neil Colon, a 35-year-old male, recently learned that his 68-year-old father was diagnosed with colon cancer. N.C. is obese and smokes a pack of cigarette per day. He loves eating out and spends most of his evening watching TV and playing games at home.
• He would like to know whether there is anything he can do to reduce his risk of developing colorectal cancer in the future.
Reducing colon cancer risk
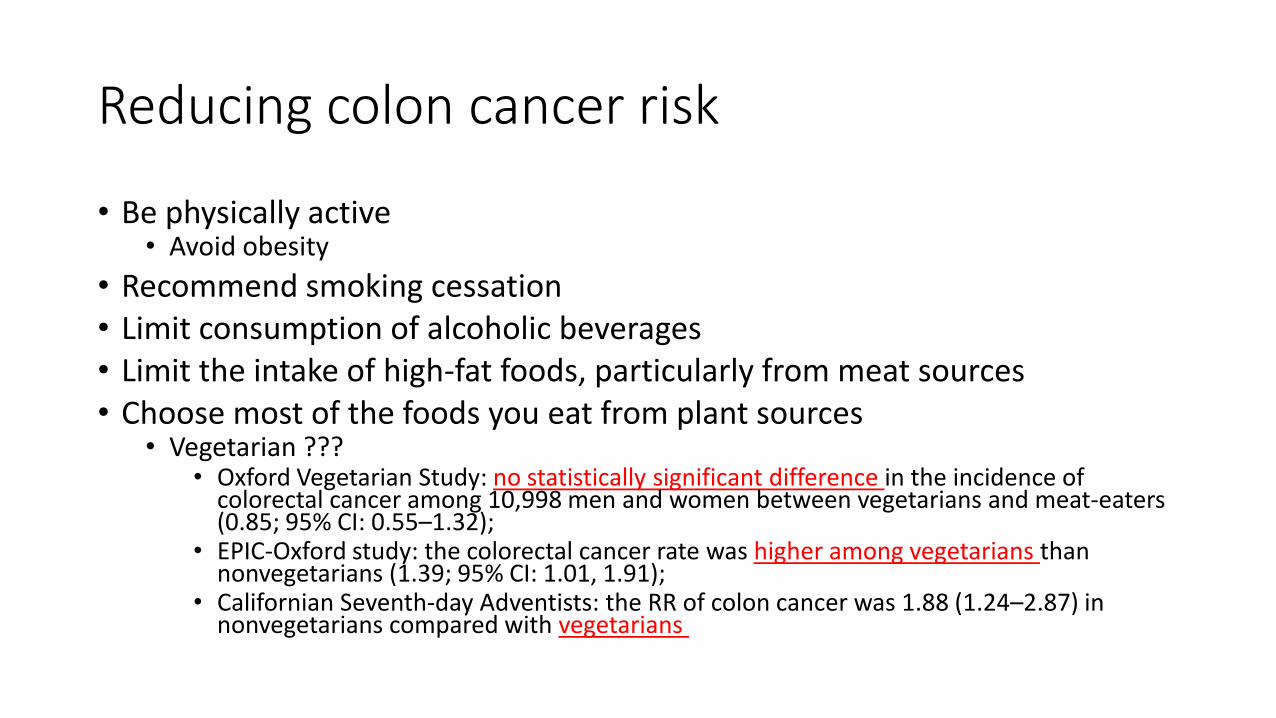
• Be physically active• Avoid obesity
• Recommend smoking cessation• Limit consumption of alcoholic beverages• Limit the intake of high-fat foods, particularly from meat sources• Choose most of the foods you eat from plant sources
• Vegetarian ???• Oxford Vegetarian Study: no statistically significant difference in the incidence of
colorectal cancer among 10,998 men and women between vegetarians and meat-eaters (0.85; 95% CI: 0.55–1.32);
• EPIC-Oxford study: the colorectal cancer rate was higher among vegetarians than nonvegetarians (1.39; 95% CI: 1.01, 1.91);
• Californian Seventh-day Adventists: the RR of colon cancer was 1.88 (1.24–2.87) in nonvegetarians compared with vegetarians
Prevention for colon cancer
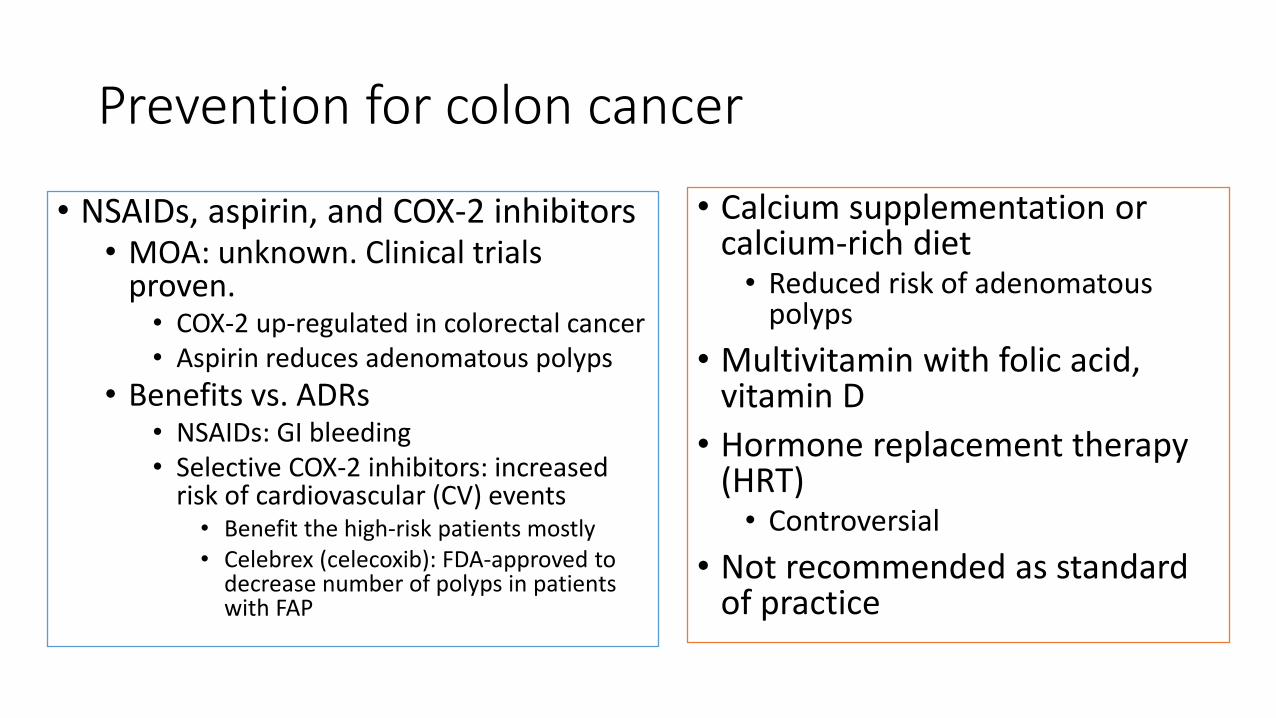
• NSAIDs, aspirin, and COX-2 inhibitors• MOA: unknown. Clinical trials
proven.• COX-2 up-regulated in colorectal cancer• Aspirin reduces adenomatous polyps
• Benefits vs. ADRs• NSAIDs: GI bleeding• Selective COX-2 inhibitors: increased
risk of cardiovascular (CV) events• Benefit the high-risk patients mostly• Celebrex (celecoxib): FDA-approved to
decrease number of polyps in patients with FAP
• Calcium supplementation or calcium-rich diet
• Reduced risk of adenomatous polyps
• Multivitamin with folic acid, vitamin D
• Hormone replacement therapy (HRT)
• Controversial• Not recommended as standard
of practice
Signs and symptoms of colorectal cancer
• A change in bowel habits: diarrhea, constipation, or narrowing of the stool, that lasts for more than a few days
• Tenesmus-sensation of the urgent need to defecate that is not relieved by doing so
• Rectal bleeding, dark stools, or blood in the stool (often, though, the stool will look normal)
• Cramping or abdominal pain• Weakness and fatigue, anemia• Unintended weight loss
• Roll out of any other causes: IBD, UTI, hemorrhoids

Screening-patient case• Neil would like to know whether there is a way to screen for
colorectal cancer. If there is, does this method detect cancer early?
• The importance of screening• Colon and rectal cancers can be prevented by removal of
precancerous tissue• Formation of colorectal cancermultistep process• Early detection reduce mortality
• Asymptomatic

Colorectal Cancer Screening
• NCCN Average Risk Screening Criteria• Age>=50 years• No history of adenomas or colorectal cancer• No history of inflammatory bowel disease• Negative family history
• Screening schedule is dependent on method used
Screening test
• Fecal screening test• To detect occult blood in the stool
• Fully rely on fecal screening test is not recommended.
• Fecal Occult Blood Test (FOBT)• Inexpensive and noninvasive; at home• Reduce mortality by 33%
• Fecal immunochemical test (FIT)• Higher sensitivity for detecting colorectal
cancer• Using antibody to detect Hgb or other
blood components; • No interaction with drug or foods• Expensive
• Digital rectal examination• Barium enema with radiography
• Late-stage cancers; miss pre-cancer lesions
• Endoscopic screening• Flexible sigmoidoscopy:
• Sigmoid colon and rectum ONLY; • does not need sedation;• Reduce incidence and mortality caused by
distal colorectal cancer by 60-80%• Colonoscopy
• Entire colon• Can remove polyps and obtain biopsy
samples during the procedure
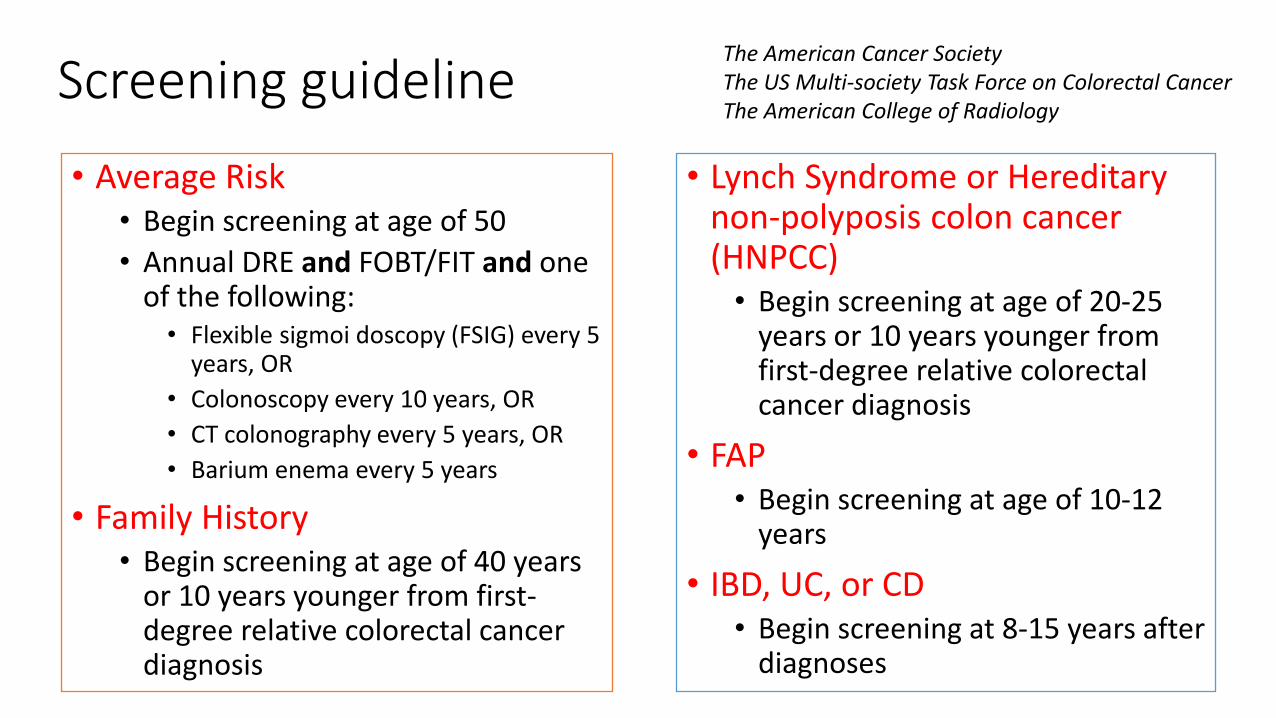
Screening guideline
• Average Risk• Begin screening at age of 50• Annual DRE and FOBT/FIT and one
of the following:• Flexible sigmoi doscopy (FSIG) every 5
years, OR• Colonoscopy every 10 years, OR• CT colonography every 5 years, OR• Barium enema every 5 years
• Family History• Begin screening at age of 40 years
or 10 years younger from first-degree relative colorectal cancer diagnosis
The American Cancer SocietyThe US Multi-society Task Force on Colorectal CancerThe American College of Radiology
• Lynch Syndrome or Hereditary non-polyposis colon cancer (HNPCC)
• Begin screening at age of 20-25 years or 10 years younger from first-degree relative colorectal cancer diagnosis
• FAP• Begin screening at age of 10-12
years
• IBD, UC, or CD• Begin screening at 8-15 years after
diagnoses

Colorectal carcinoma prevalence/distribution by Stage at Diagnosis
Stage at Diagnosis Stage distribution (%)
Localized (primary site) 39
Regional (spread to regionallymph nodes)
37
Distant (metastasized) 19
Unknown 5

Diagnosis
• CBC: complete blood count• CEA: carcinoembryonic antigen• FOBT: fecal occult blood test• Colonoscopy
• Entire bowel

Carcinoembryonic Antigen (CEA)
• Oncofetal protein expressed during embryonic development
• 1st tumor marker identified in 1965 from human colon caner tissue
• Glycoprotein; MW=180kDa• Increased in many gastrointestinal
tumors• Also increased in non-malignant
disease states such as pancreatitis, hepatitis, renal failure, and smoking and therefore limits CEA screening potential
• Normal range: 0-5 ng/ml• Should NOT be used as screening
tool• Uses include:
• Detection of recurrence following surgery
• Tumor response to chemotherapy and/or radiation therapy
• Disease progression if elevated initially

Poor prognostic factors
• Pathologic stage• Late stage at diagnosis poor prognosis
• Histologic grade• Poorly differentiated tumor
• Bowel obstruction or perforation• Preoperative elevation of CEA titer >5 ng/ml• High thymidylate synthase (TS) tumor expression
• Target enzyme by 5’-FU metabolite, FdUMP• Increased expression observed as mechanism of resistance to 5’-FU.
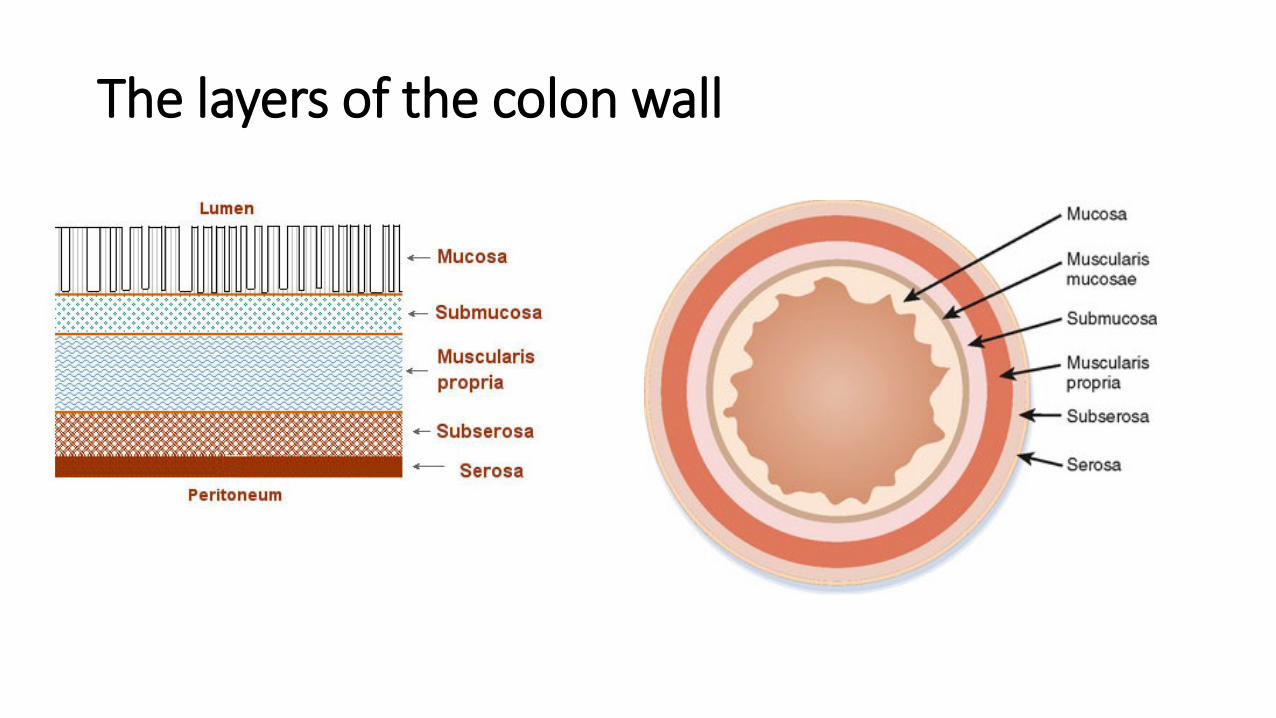
The layers of the colon wall

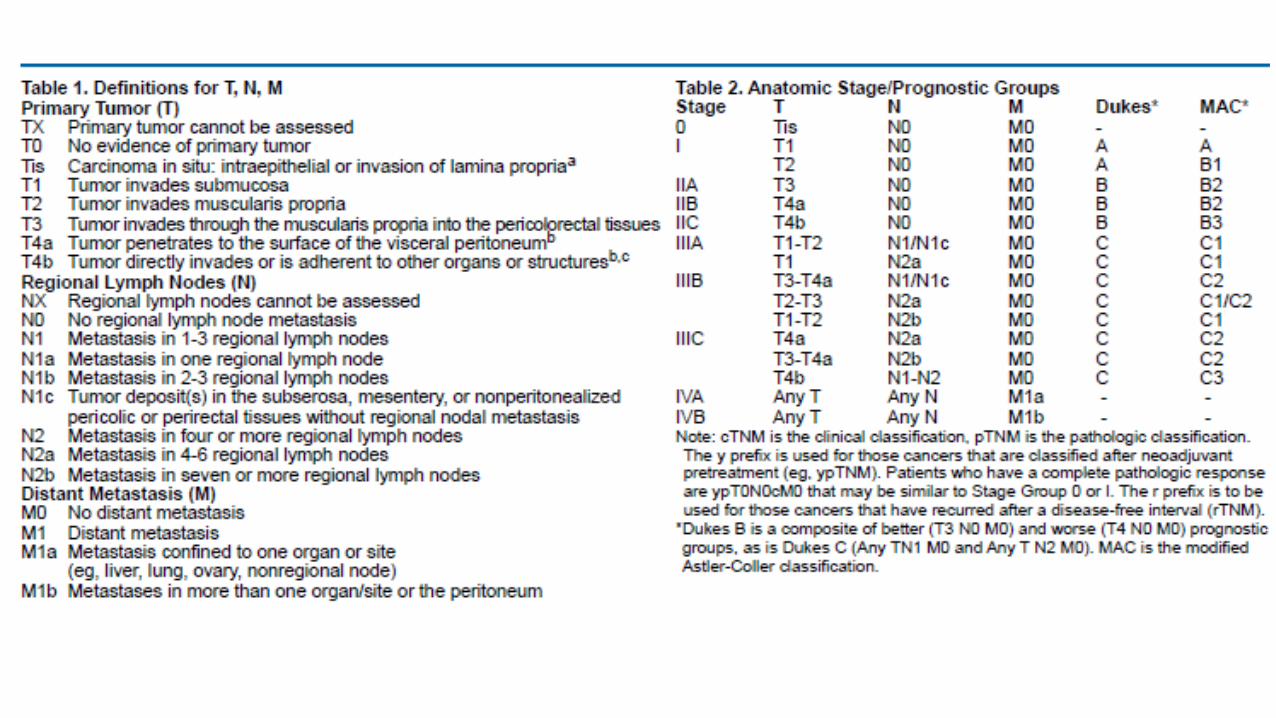
Stage of Colon Cancer
• Determination for treatment options, survival and recurrence of disease
• Uses both clinical (Dukes system) and pathological (TNM system)
• TNM system• T: Depth of tumor invasion into and
through the intestinal wall• N: number of regional lymph nodes
involved• M: Presence or absence of distant
metastases
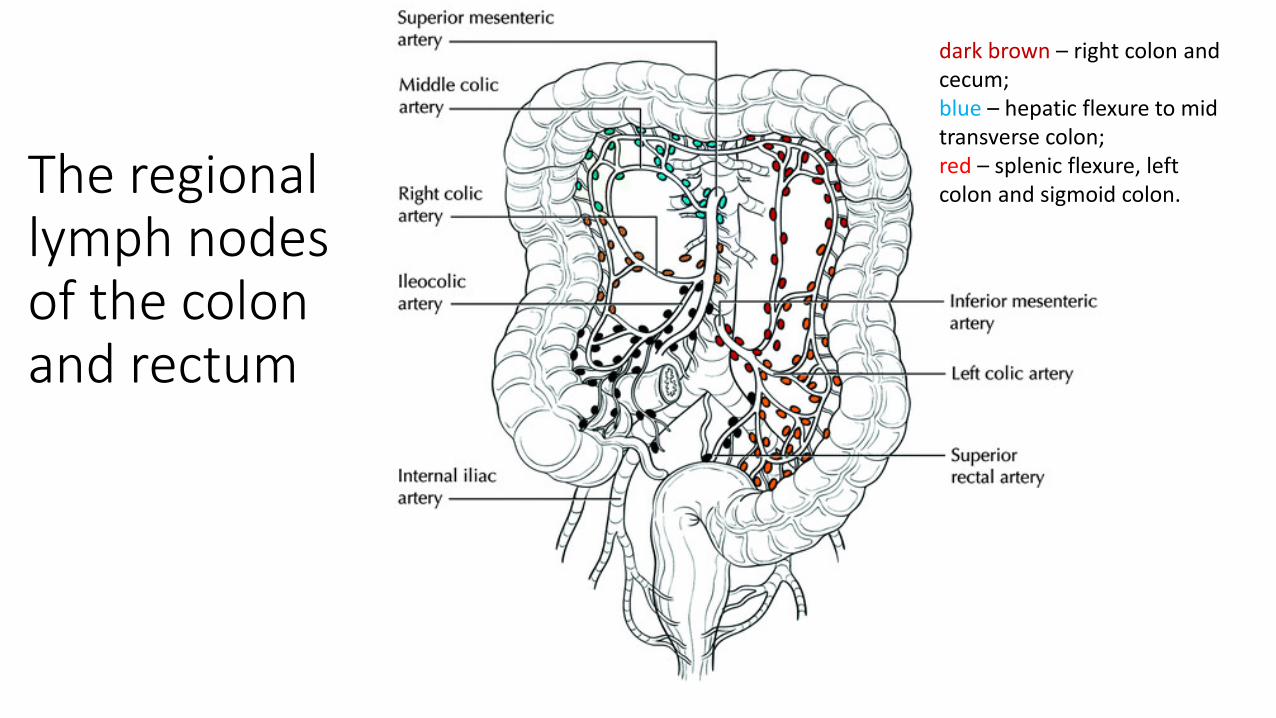
The regional lymph nodes of the colon and rectum
dark brown – right colon and cecum; blue – hepatic flexure to mid transverse colon; red – splenic flexure, left colon and sigmoid colon.

Patient Neil
CBC=slight anemiaFOBT (+)CEA=220ng/ml (normal non-smoker: <2.5 ng/ml; smoker: < 5ng/ml)
Colonoscopy showed a tumor in the descending colon.
The biopsy of the tumor confirmed with adenocarcinoma.
Patient Neil is scheduled for a surgical consult to discuss his surgical options and a oncology consult subsequent therapy.

Treatment Options for Colorectal Cancer• Surgery
• Curative for Stage I, II colon cancer• Curative for Stage I rectal cancer• Mainstay therapy for Stage I to III colorectal cancer
• Radiation• Palliative for un-resectable colon cancer• Pain control• Adjuvant therapy for Stage II, III rectal cancer
• Chemotherapy• Standard adjuvant for Stage III colon cancer and Stage IV metastatic colon cancer• 5-FU-based regimens• Capecitabine –pro-drug of 5-FU, PO
Rationale for chemotherapy treatment
• 40-50% of all colorectal cancer patients initially cured by surgery will eventually develop and subsequently die from metastatic disease
• 30% of all patients have advanced disease, either have local recurrence or distant metastases at presentation.
• Multiple regimens• NCCN• NCI Clinical Trial
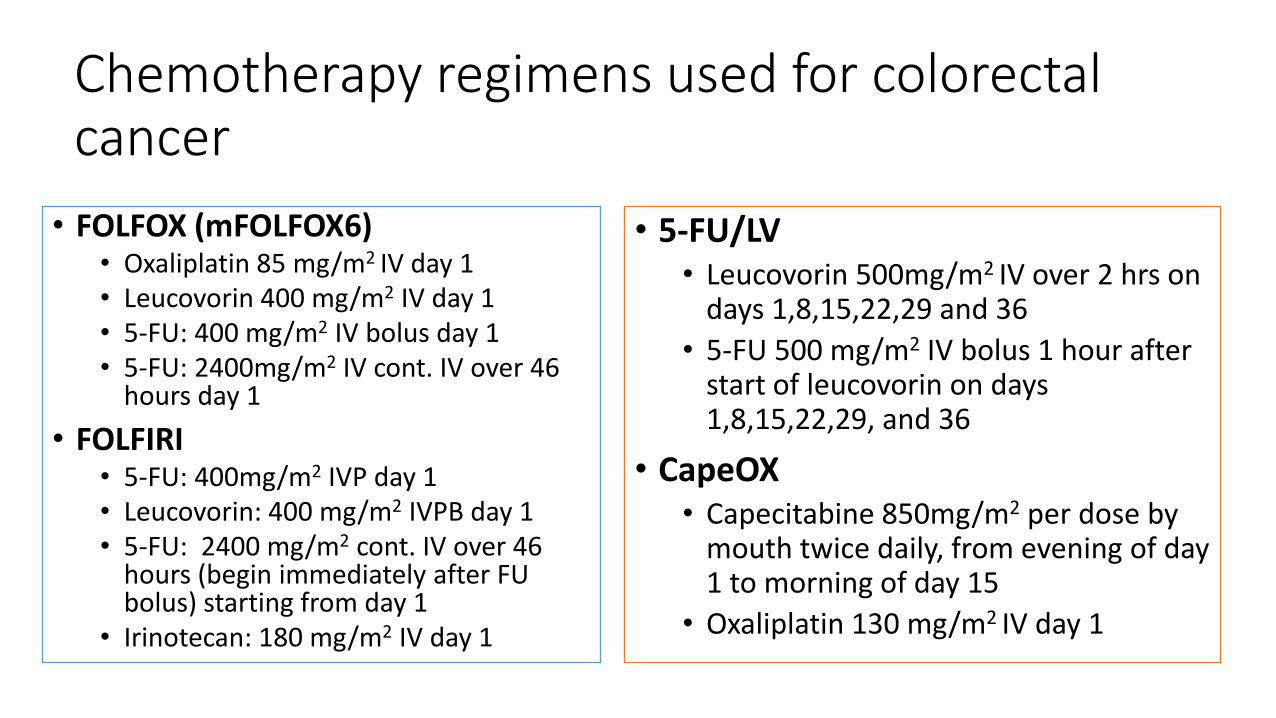
Chemotherapy regimens used for colorectal cancer
• FOLFOX (mFOLFOX6)• Oxaliplatin 85 mg/m2 IV day 1• Leucovorin 400 mg/m2 IV day 1• 5-FU: 400 mg/m2 IV bolus day 1• 5-FU: 2400mg/m2 IV cont. IV over 46
hours day 1• FOLFIRI
• 5-FU: 400mg/m2 IVP day 1• Leucovorin: 400 mg/m2 IVPB day 1• 5-FU: 2400 mg/m2 cont. IV over 46
hours (begin immediately after FU bolus) starting from day 1
• Irinotecan: 180 mg/m2 IV day 1
• 5-FU/LV• Leucovorin 500mg/m2 IV over 2 hrs on
days 1,8,15,22,29 and 36• 5-FU 500 mg/m2 IV bolus 1 hour after
start of leucovorin on days 1,8,15,22,29, and 36
• CapeOX• Capecitabine 850mg/m2 per dose by
mouth twice daily, from evening of day 1 to morning of day 15
• Oxaliplatin 130 mg/m2 IV day 1
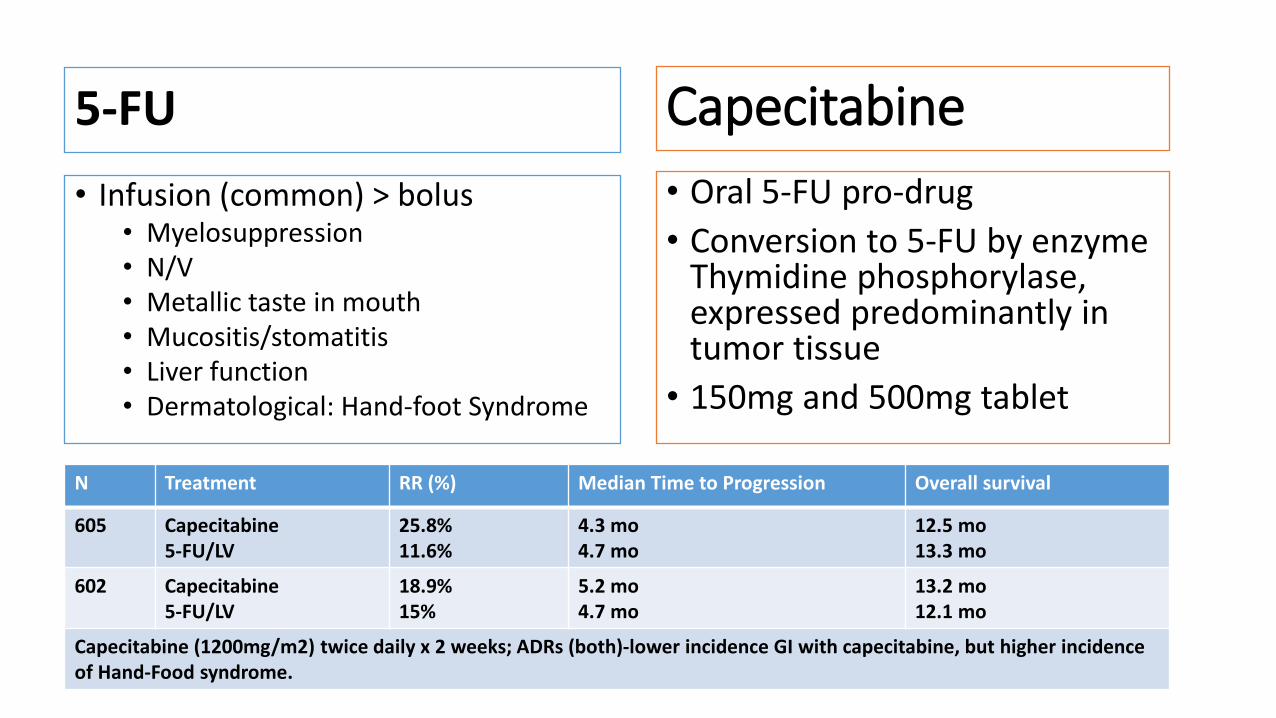
5-FU• Infusion (common) > bolus
• Myelosuppression• N/V• Metallic taste in mouth• Mucositis/stomatitis• Liver function• Dermatological: Hand-foot Syndrome
• Oral 5-FU pro-drug• Conversion to 5-FU by enzyme
Thymidine phosphorylase, expressed predominantly in tumor tissue
• 150mg and 500mg tablet
N Treatment RR (%) Median Time to Progression Overall survival
605 Capecitabine5-FU/LV
25.8%11.6%
4.3 mo4.7 mo
12.5 mo13.3 mo
602 Capecitabine5-FU/LV
18.9%15%
5.2 mo4.7 mo
13.2 mo12.1 mo
Capecitabine (1200mg/m2) twice daily x 2 weeks; ADRs (both)-lower incidence GI with capecitabine, but higher incidence of Hand-Food syndrome.
Capecitabine


Leucovorin
• MOA• Reduced form of folic acid
• Leucovorin has almost no side effects/anti-cancer activities of its own.• When used in combination with fluorouracil, it can increase the
severity of side effects of 5-FU, as well as 5-FU’s anti-cancer activity.• Stabilizes the binding of 5-dUMP and thymidylate synthase, enhancing the
activity of fluorouracil. • Fluorouracil given in combination with Leucovorin enhance the binding of
fluorouracil to thymidylate synthase inside of the cancer cells fluorouracil stay in the cancer cell longer and exert its anti-cancer effect on the cells.

Colorectal Cancer Stage I: Treatment
• Surgery• Wide surgical resection and
anastomosis via open colectomy with enbloc removal of at least 12 regional lymph nodes
• Laparoscopic-assisted colectomy may be performed if surgeon is certified in LAC and locally advanced disease, adhesions and rectal involvement have been ruled out.

Colon cancer Stage II: Treatment
• Risk Assessment for Stage II Disease• NCCN guideline
• Number of lymph nodes analyzed after surgery (<12)• Poor prognosis features (poorly differentiated histology; lymphatic/vascular invasion, bowel
obstruction, localized perforation, positive margins etc.)• Assessment of other comorbidities and anticipated life expectancy
• Adjuvant chemotherapy• Adjuvant chemotherapy does not improve survival more than 5%• NCCN guideline
• FOLFOX:• Good for high-risk Stage II patients• NOT indicated for good- or average-risk patients with Stage II Colon cancer.
• Targeted therapy should NOT be used in the adjuvant setting for patients with stage II or III colon cancer outside the setting of a clinical trial.
• Bevacizumab, cetuximab, panitumumab, irinotecan, amucirumab

Colon cancer Stage III: Treatment
• Surgery:• Wide surgical resection and anastomosis via open colectomy with sampling of
at least 12 regional lymph nodes and removal of all involved nodes.
• Chemotherapy• Adjuvant chemotherapy with mFOLFOX6 as the preferred regimen
• NCCN Category 1 recommendation• Other options:
• CapeOX• 5-FU-Leucovorin
• Single agent: Capecitabine as an equivalent alternative
• No role for irinotecan, bevacizumab, penitumumab, or cetuximab in Stage II or III disease outside of clinical trials.

Metastatic Sites
• Liver-most common• ~60% patients• Surgery: resect the isolated lesion
• Lung-most common• Higher incidence of isolated
pulmonary metastases in rectal vas colon cancer patients
• Surgery: resect the isolated lesion• Less common
• Bone• Brain
• Treatment options• Surgical resection of tumor
(reduce tumor load if possible)• Radiation therapy (palliation of
symptoms only)• Chemotherapy (recurrence and
metastatic disease)

Chemotherapy for advanced or metastatic Disease• NCCN guideline
• ChemoTx as initial treatment in a patient that is appropriate for intensive therapy (performance of status, goal of therapy, age etc.)
• According to results recently presented at the American Society of Clinical Oncology (ASCO)
• The chemotherapy regimen consisting of oxaliplatin, 5-FU and leucovorin improves survival compared to other standard chemotherapy combinations for the treatment of advanced colorectal cancer.
• Other regimens +/- targeted agents• FOLFIRI/CapeOX/FOLFOXIRI/Infusional 5-FU/LV• Targeted therapy
• Bevacizumab (VEGF)• Cetuximab (in KRAS wild type patients)

Pharmacogenomics application in oncology
• 5-FU and dihydropyrimidine dehydrogenase (DPD)• Irinotecan and UGT1A1

Fluoropyrimidines and DPD
• 5-Fluorouracil (5-FU)• Capecitabine
• Pro-drug of 5-FU
• 5-FU dihydrofluorouracil (DHFU) by dihydropyrimidine dehydrogenase (DPD).
• Decreased DPYD activity is associated with high risk of severe or fatal toxicity from standard doses of 5-FU
Thorn Caroline F, Marsh Sharon, Carrillo Michelle Whirl, McLeod Howard L, Klein Teri E, Altman Russ B . "PharmGKB summary: fluoropyrimidine pathways" Pharmacogenetics and genomics (2010).
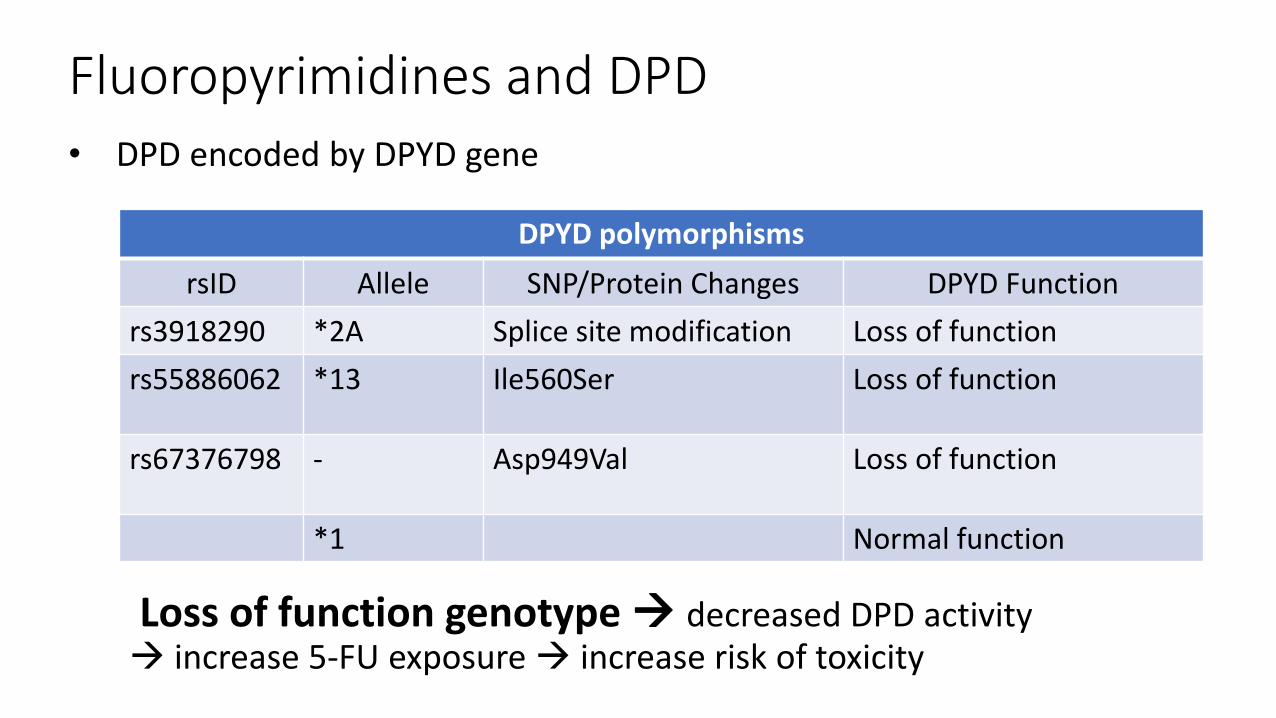
Fluoropyrimidines and DPD• DPD encoded by DPYD gene
DPYD polymorphismsrsID Allele SNP/Protein Changes DPYD Function
rs3918290 *2A Splice site modification Loss of functionrs55886062 *13 Ile560Ser Loss of function
rs67376798 - Asp949Val Loss of function
*1 Normal function
Loss of function genotype decreased DPD activity increase 5-FU exposure increase risk of toxicity
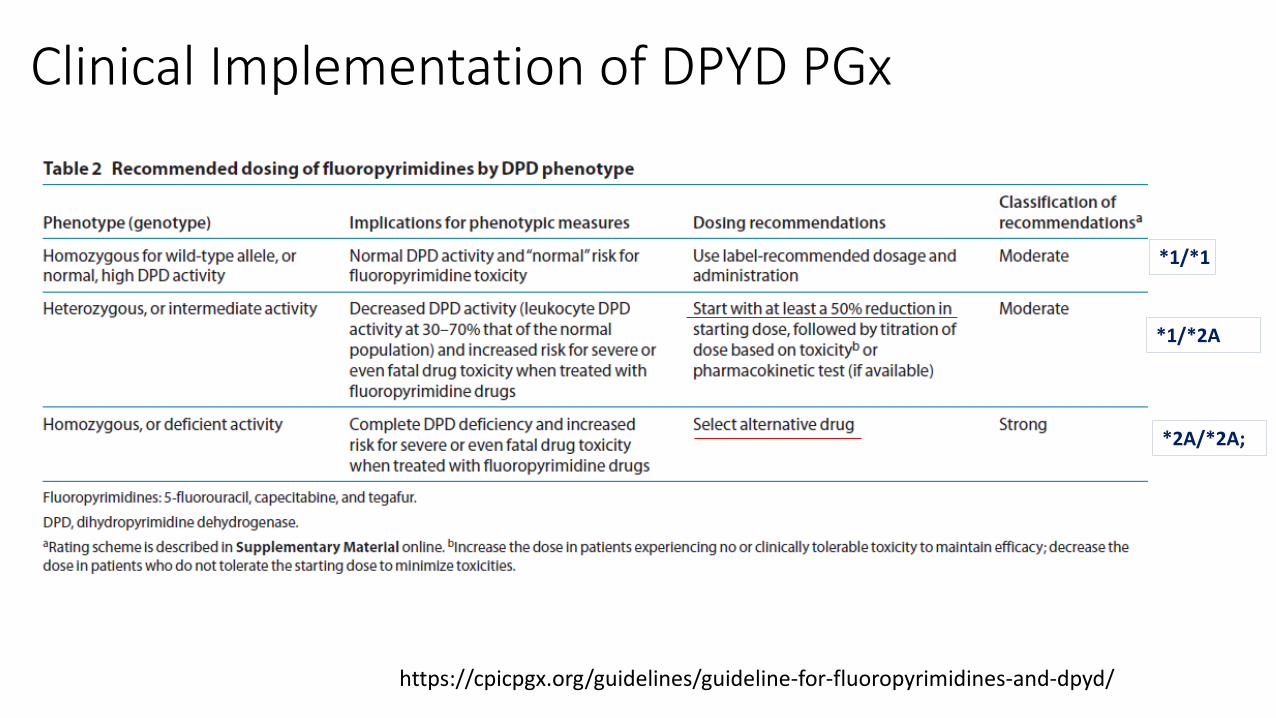
*1/*1
*1/*2A
*2A/*2A;
https://cpicpgx.org/guidelines/guideline-for-fluoropyrimidines-and-dpyd/
Clinical Implementation of DPYD PGx

Irinotecan and UGT1A1• Irinotecan is a prodrug
requiring bioactivation to SN-38
• Damage DNA • Causing toxicities
• Diarrhea and myelosuppression
• Uridine diphosphate-glucuronosyltransferase 1A1 (UGT1A1)
• Detoxification of SN-38 by glucuronidation.
M. Whirl-Carrillo, E.M. McDonagh, J. M. Hebert, L. Gong, K. Sangkuhl, C.F. Thorn, R.B. Altman and T.E. Klein. "Pharmacogenomics Knowledge for Personalized Medicine" Clinical Pharmacology & Therapeutics (2012) 92(4): 414-417.
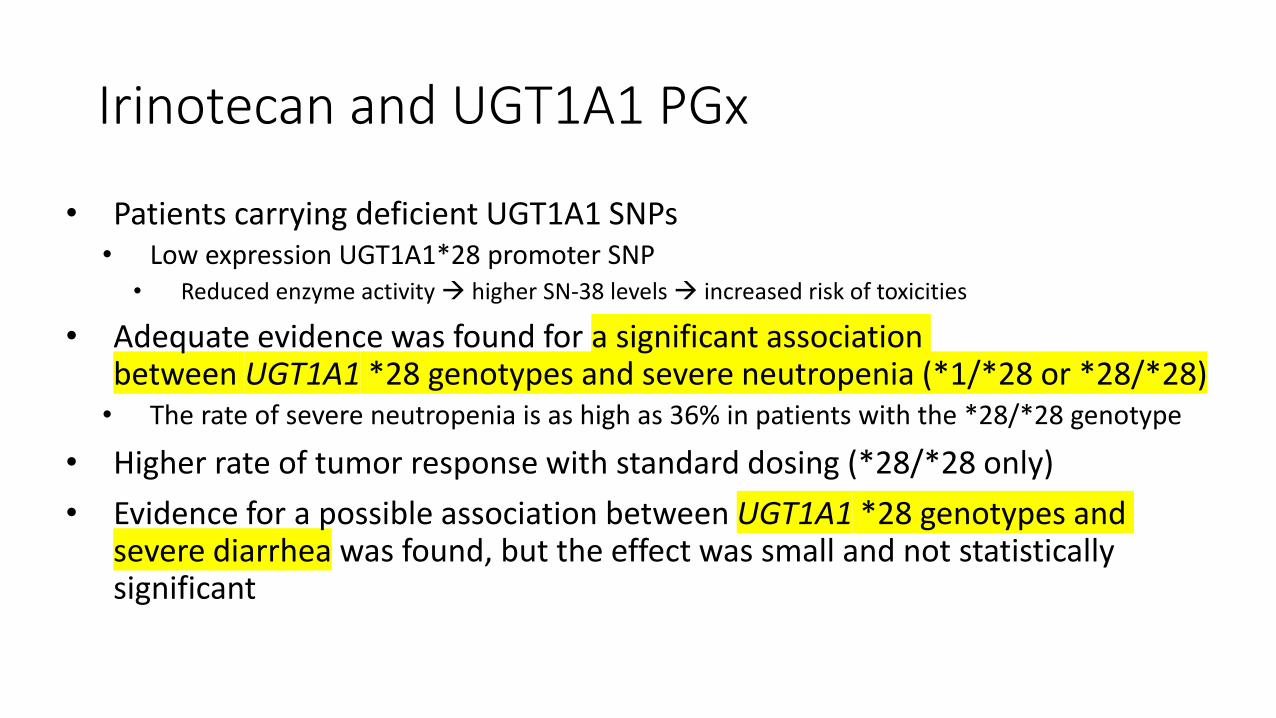
• Patients carrying deficient UGT1A1 SNPs• Low expression UGT1A1*28 promoter SNP
• Reduced enzyme activity higher SN-38 levels increased risk of toxicities
• Adequate evidence was found for a significant association between UGT1A1 *28 genotypes and severe neutropenia (*1/*28 or *28/*28)
• The rate of severe neutropenia is as high as 36% in patients with the *28/*28 genotype
• Higher rate of tumor response with standard dosing (*28/*28 only)• Evidence for a possible association between UGT1A1 *28 genotypes and
severe diarrhea was found, but the effect was small and not statistically significant
Irinotecan and UGT1A1 PGx
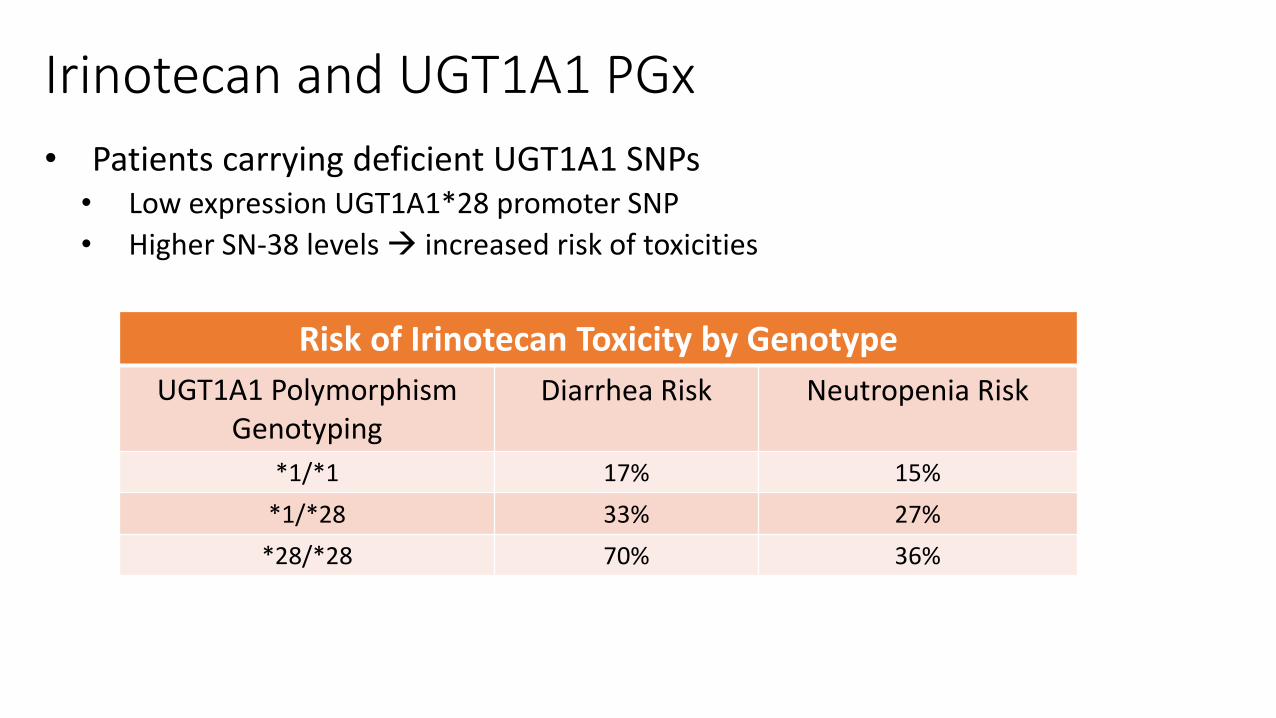
Irinotecan and UGT1A1 PGx• Patients carrying deficient UGT1A1 SNPs
• Low expression UGT1A1*28 promoter SNP• Higher SN-38 levels increased risk of toxicities
Risk of Irinotecan Toxicity by GenotypeUGT1A1 Polymorphism
GenotypingDiarrhea Risk Neutropenia Risk
*1/*1 17% 15%*1/*28 33% 27%
*28/*28 70% 36%

Irinotecan and UGT1A1 PGx• Dose intensification with starting dose ≥ 240mg/m2 (FOLFIRI-HIGH)
• UGT1A1 genotyping strongly recommended
Heterozygous*1/*28
Homozygous*28/*28
HomozygousWild type *1/*1
Toxicity risk not increasedToxicity risk significantly increased
https://www.pharmgkb.org/chemical/PA450085Annotation of PRO Guideline for irinotecan and UGT1A1

Phenotype (Genotype)
Therapeutic Dose Recommendation Level of Evidence Clinical Relevance
*1/*28 None.
Published controlled studies of moderate quality* relating to phenotyped and/or genotyped patients or healthy volunteers, and having relevant pharmacokinetic or clinical endpoints..
Clinical effect (S): death; arrhythmia; unanticipated myelosuppression.
*28/*28
Dose >250mg/m2: reduce initial dose by 30%. Increase dose in response to neutrophil count. Dose <=250mg/m2: no dose adjustment.
Published controlled studies of moderate quality* relating to phenotyped and/or genotyped patients or healthy volunteers, and having relevant pharmacokinetic or clinical endpoints.
Clinical effect (S): Failure of lifesaving therapy e.g. anticipated myelosuppression; arrhythmia; neutropenia < 0.5x109/l; leucopenia < 1.0x109/l; thrombocytopenia < 25x109/l; life-threatening complications from diarrhea.
https://www.pharmgkb.org/chemical/PA450085Annotation of PRO Guideline for irinotecan and UGT1A1

Study guide• Understand that family history, patient-specific factors, and environmental
factors are identified as risk factors for colorectal cancer.• Environmental factors could be modified to reduce the risk of colorectal cancer
• Early detection of colorectal cancer through screening reduces cancer-related mortality. Most patients at low risk of colorectal cancer are recommended to begin screening at the age of 50 every 10 years using colonoscopy.
• Patients may be asymptomatic at diagnosis or have nonspecific symptoms. Carcinoembryonic antigen (CEA) may be elevated in patients with colorectal cancer, but it can not be used alone for diagnosis.
• Adjuvant combination chemotherapy with 5’-fluorouracil (5’-FU) and oxaliplatin is currently considered the standard of care for patients with stage III colorectal cancer after surgery with curative intent.
• All patients diagnosed with localized colorectal cancer should undergo routine surveillance visits with their oncologist for a period of 5 years after completion of their definitive therapy.
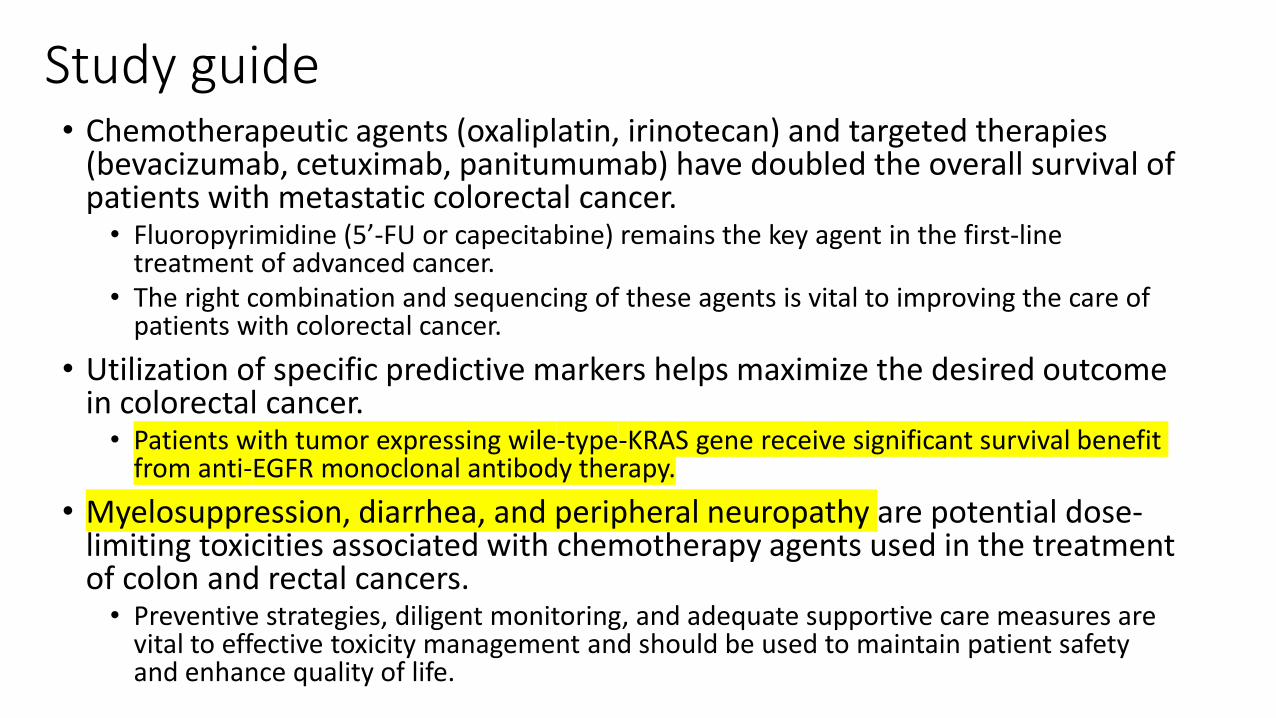
Study guide• Chemotherapeutic agents (oxaliplatin, irinotecan) and targeted therapies
(bevacizumab, cetuximab, panitumumab) have doubled the overall survival of patients with metastatic colorectal cancer.
• Fluoropyrimidine (5’-FU or capecitabine) remains the key agent in the first-line treatment of advanced cancer.
• The right combination and sequencing of these agents is vital to improving the care of patients with colorectal cancer.
• Utilization of specific predictive markers helps maximize the desired outcome in colorectal cancer.
• Patients with tumor expressing wile-type-KRAS gene receive significant survival benefit from anti-EGFR monoclonal antibody therapy.
• Myelosuppression, diarrhea, and peripheral neuropathy are potential dose-limiting toxicities associated with chemotherapy agents used in the treatment of colon and rectal cancers.
• Preventive strategies, diligent monitoring, and adequate supportive care measures are vital to effective toxicity management and should be used to maintain patient safety and enhance quality of life.
Study guide
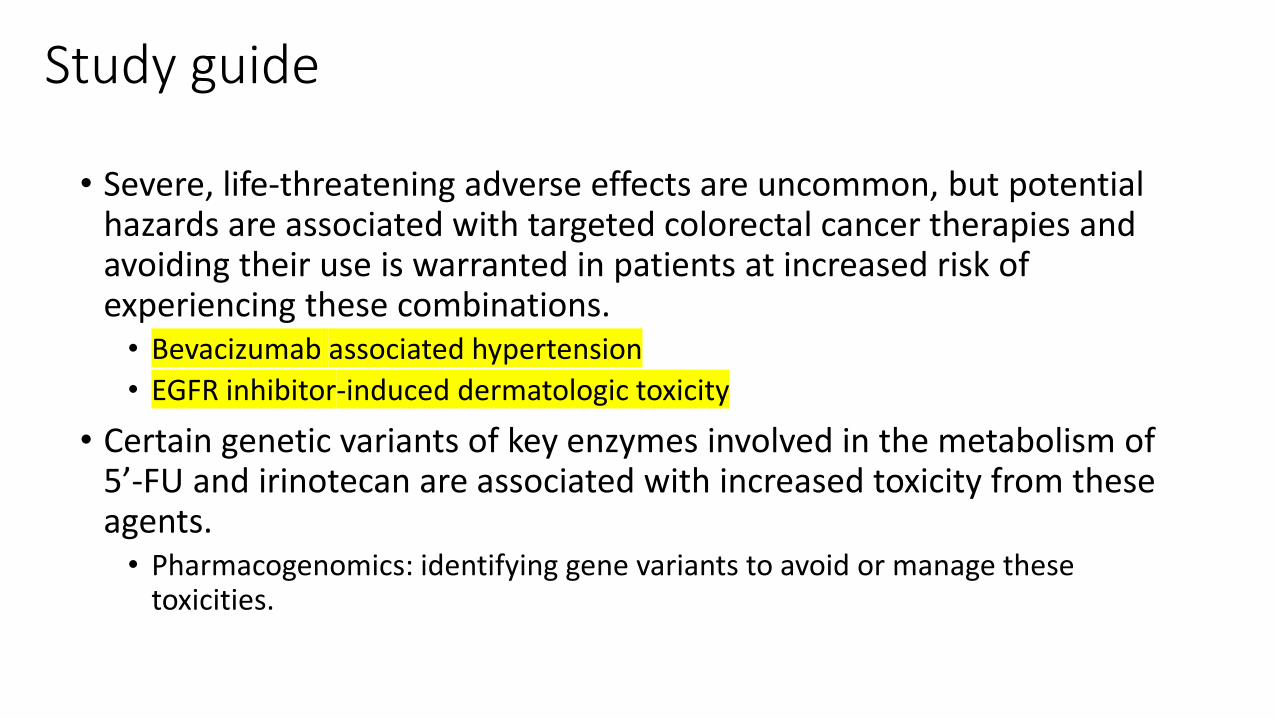
• Severe, life-threatening adverse effects are uncommon, but potential hazards are associated with targeted colorectal cancer therapies and avoiding their use is warranted in patients at increased risk of experiencing these combinations.
• Bevacizumab associated hypertension• EGFR inhibitor-induced dermatologic toxicity
• Certain genetic variants of key enzymes involved in the metabolism of 5’-FU and irinotecan are associated with increased toxicity from these agents.
• Pharmacogenomics: identifying gene variants to avoid or manage these toxicities.























![Esophageal caner ahmed md [compatibility mode]](https://img.pdfslide.net/doc/110x75/54804a65b4af9fea158b5bdf/esophageal-caner-ahmed-md-compatibility-mode.jpg)




