Embed Size (px)
Citation preview

COMA 2003, Version 1
Christopher C. Luzzio, MD

Consciousness
• An active process with multiple components.• Wakefulness or alertness is a precondition.• Self-awareness of one’s own cognition and mental
processes.• Processing of internal and external stimuli.• Working memory and attention.• Spatial and temporal ordering of long-term memory.• Decision making.• Deductive reasoning, planning, or synthesis of above.

“Cogito, ergo sum”
(I think, therefore, I am.)
Rene Descartes

Altered Consciousness
• Delirium or acute confusional state.mostly awake to easily aroused
level of consciousness fluctuates
• Stuporous.difficult to arouse
medical emergency
• Coma (unresponsive).
no speech, no eye opening, no motor response

Encephalopathy
• Delirium– Acute onset– Inattention– Disorganized thinking– Altered alertness– Fluctuating course– Metabolic or structural– MMS test not useful
• Dementia– Chronic– Attentive (early)– Progressive loss of
cognitive abilities– Little fluctuation– Structural– MMS test useful
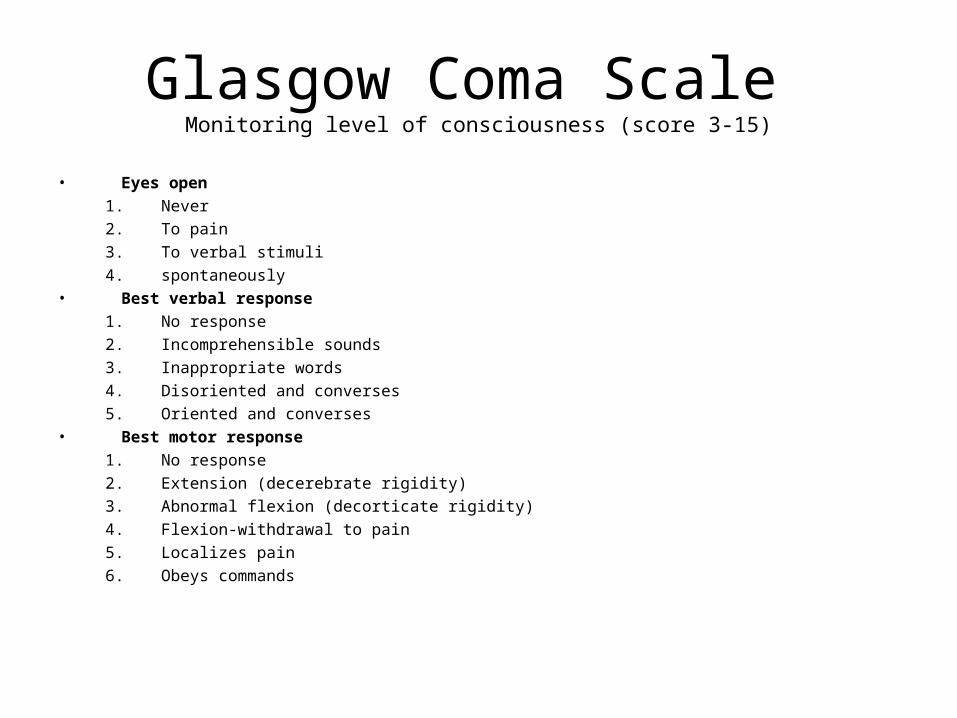
Glasgow Coma Scale Monitoring level of consciousness (score 3-15)
• Eyes open
1. Never
2. To pain
3. To verbal stimuli
4. spontaneously• Best verbal response
1. No response
2. Incomprehensible sounds
3. Inappropriate words
4. Disoriented and converses
5. Oriented and converses• Best motor response
1. No response
2. Extension (decerebrate rigidity)
3. Abnormal flexion (decorticate rigidity)
4. Flexion-withdrawal to pain
5. Localizes pain
6. Obeys commands

E.R. Pitfall #1
• Acute Parietal lobe infarcts:– Aphasia– Visual Sensory Neglect – Often treated as metabolic delirium– Thrombolytic window missed– CT scan often does not show acute CVA

Physiology of Coma and Acute Delirium
• Pathologic processes that impair:– Globally cortical neurons or– Bilateral thalamic nuclei or– Brainstem
• Ascending reticular activating system
The Coma Exam
• Rapidly determine level of injury.– Diffuse (metabolic)– Focal
• Supratentorial (hemispheres)• Infratentorial (brainstem)• Likely more serious
Resuscitation FirstNeurological ABCs
• Avoid worsening neck injuries• Airway• Breathing• Circulation• Diabetes-check blood sugar• Drugs-nalaxone for opiate overdose• Epilepsy-control seizures (bitten tongue)• Fever-meningitis-antibiotics• Glasgow Coma Scale• Herniation syndromes

Herniation Syndromes
• Uncal Herniation– Unilateral mass forces the
ipsilateral temporal lobe through the tentorium.
• Contralateral upper motor neuron signs.
– Ipsilateral third nerve compression.
• Dilated pupil
– Contralateral upper brainstem.• Ipsilateral hemiplegia
– CSF flow interrupted– Abnormal respirations
• Cheyne-Stokes
• Erratic

Herniation Syndromes
• Central Herniation– Supratentorial lesion forces the
diencephalon centrally through the tentorium.
– Compresses upper midbrain, later pons and medulla.
– Early• Erratic respirations
• Small reactive pupils
• Increased limb tone
• Babinsky sign
• Decorticate rigidity
• Decerebrate posturing (later)
• Fixed and dilated pupils

Herniation Syndromes
• Bad prognosis
• Avoid if possible– Recognize possibility (strokes)– Treat edema (masses)– Evacuate blood– Hyperventilate– Raise head of bed– Osmotic agents (Mannitol)
• Neurosurgical emergency
• Craniotomy
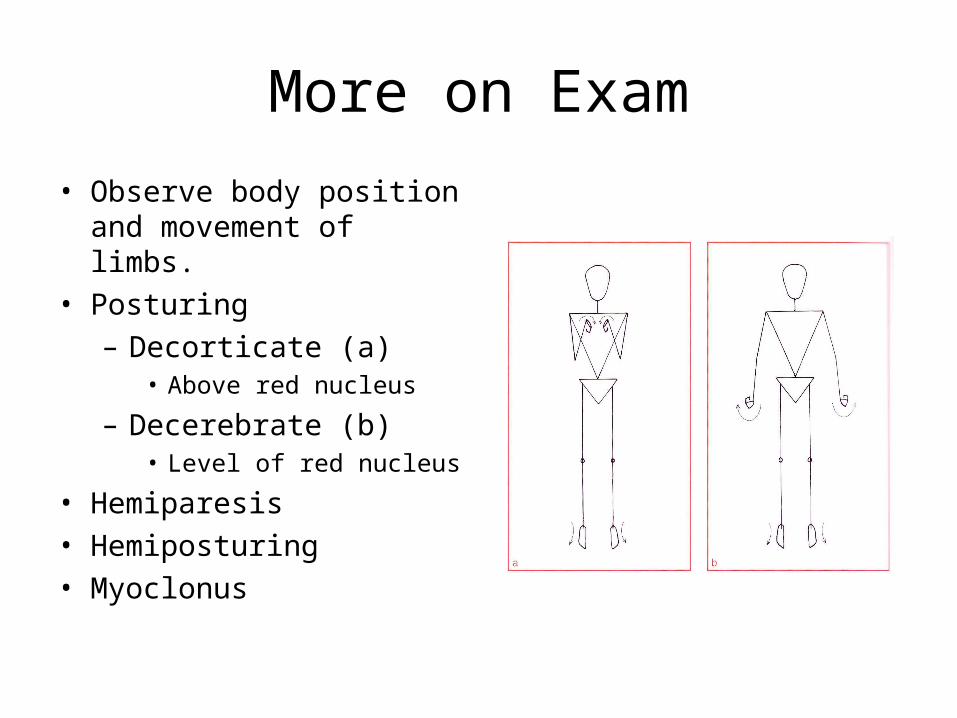
More on Exam
• Observe body position and movement of limbs.
• Posturing– Decorticate (a)
• Above red nucleus
– Decerebrate (b)• Level of red nucleus
• Hemiparesis• Hemiposturing• Myoclonus
More on Exam
• Best verbal response– Don’t miss aphasia
• Head and neck– Fractures– Stiffness– Otitis media
• Eyelids– Ptosis– Facial weakness

More on Exam
• Pupils equal– Pinpoint…………………opiates or pontine lesion– Small and reactive…….metabolic encephalopathy– Mid-sized fixed…………midbrain lesion– Mid-sized reactive……..metabolic lesion
• Pupils unequal– Dilated and unreactive...3rd nerve palsy– Small and reactive……..Horner syndrome

More on Exam
• Examine the fundi, eye position and eye movements.
• Papilloedema:– Absence does not exclude raised
ICP– Hypertension– Masses– Hydrocephalus– CVT– Meningitis– Hemorrhage
More on Exam
• Doll’s eye maneuver (oculocephalic testing)– Not to done unless cervical injury is excluded.– Both eyes move (normal).– One eye moves (unilateral lesion).– Eyes fail to move any direction (bilateral brainstem lesions).
• Caloric testing• Corneal reflex• Gag reflex
More on Exam
• Motor system– Tone– Movements– Symmetry
• Tendon Reflexes
• Plantar response
• Response to painful stimuli
More on Exam
• Vitals– BP, respirations, temperature, pulse– Cushing’s response
• hypertension, bradycardia, irregular respirations
• General exam
Causes of Coma and Delirium

Investigations

Other Conditions
• Locked-in state
• Persistent vegetative
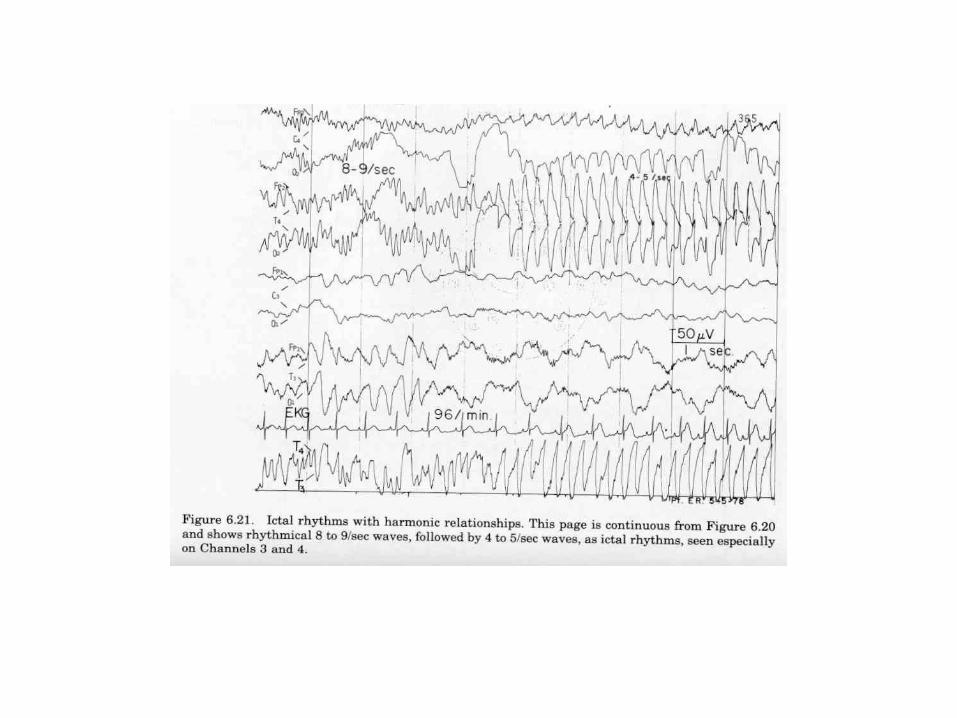
• Brain death– EEG