Embed Size (px)
Citation preview
Combating Second Victim Trauma in Healthcare Providers
Bernadette Johnson, DNAP, CRNA
2021 Psych Retreat - Virtual
Acknowledgement and Thank You
• The University of Missouri Healthcare System and Dr. Sue Scott graciously provided permission to use any and all content and material as provided in the Train-The-Trainer Workshop.
• Their tireless efforts and pursuit on The Second Victim Phenomenon is acknowledged and appreciated.
OBJECTIVES
Define Second Victim Phenomenon.
Identify the 6 stages one goes through following a traumatic event.
Provide effective ways to help individuals through the recovery process.
Do you have a “story”? Research supports over 90% of us do.
Today’s Health Care: The Facts44,000-98,000 deaths/year in U.S. due to preventable adverse events (Kohn et. al, 2000).
Revised estimates at least 210,000 (and possibly more like 400,000) die in U.S due to preventable harm (James, 2013).
With revised estimates: At least 4 clinicians/patient = 840,000 to 1.6 million clinicians impacted
Could this represent a crisis for our caregivers?
Kohn, LT, Corrigan, JM, & Donaldson, MS. (2000). To err is human: building a safer health system. Washington, D.C.:National Academy of Sciences Press. James, J.T. (2013). A new, evidence-based estimate of patient harms associated with hospital care. Journal of Patient Safety, 9(3), 122-128.
Chantler, C., Lancet 1999; 353:1178-91
“Medicine used to be simple, ineffective and relatively safe..... now it is complex, effective, and potentially dangerous"
Sir Cyril Chantler
Albert Wu, MD
Review of the Literature
“Virtually every practitioner knows the sickening realization of making a bad mistake. You feel singled out and exposed…..You agonize about what to do…… Later, the event replays itself over and over in your mind”
Wu, A. (2000). Medical error: the second victim. The doctor who makes the mistake needs help too. British Medical Journal, 320, 726-727.

Who are second victims?
• Health care providers involved in:
• Unanticipated adverse patient event
• Medical error• Patient related injury
• Provider is traumatized by the event; a victim
• Scott et al., 2010
Who are second victims?
• Feel personally responsible
• Failure towards patients• Second guess clinical skills• Question knowledge base
• Scott et al., 2010
This event shook me
to my core.”
Commonly Heard Phrases
“This has been a turning point in my career.”
“It just keeps replaying over and
over in my mind.”
“I’ll never be the same.”
I’m going to check out my options as a
Walmart greeter. I can’t mess that up.”

High Risk ScenariosPatient ‘connects’ staff member to familyPediatric casesMedical errorsFailure to rescue casesFirst death experienceUnexpected patient demise
Recent Observations = Exposure to Workplace Violence EventsCOVID-19 pandemic

At least 50% of health care workers will
experience this phenomenon
Clark & Scott, 2015

The emotional distress associated with an unanticipated clinical event is one that no
one wants to experience, yet…
Most clinicians have already witnessed colleagues suffering as ‘second victims’.Most clinicians will have this response 3-4 times (or more) during their clinical years of practice.When it happens, most clinicians are unsure of what they are experiencing.Most do not know how to respond or assist others who are suffering.
The Facts…..More than 2/3 of providers involved in adverse event suffer from troubling memories, anxiety, anger, remorse & distress.Nearly 80% of doctors have experienced a distressing patient event in the last year.
Busch, IM, Moretti, F, Purgato, M, Barbui, C., Wu, A. & Rimondini, M. (2019). Journal of Patient Safety. Psychological and psychosomatic symptoms of second victims of adverse events: a systematic review and meta-analysis. Doi: 10.1097/PTS.0000000000000589.
Hu, YY et al. 2012. Physicians’ needs in coping with emotional stressors: The case for peer support. Arch Surg. 147(3):212-217. Paturel, A. (2019) When physicians are traumatized. Association of American Medical Colleges AAMC News. August 13, 2019. https://news aamc org/medical-education/article/when-physicians-are-traumatized

Second Victim Recovery Trajectory
Chaos & Accident Response
Intrusive Reflections
Restoring Personal Integrity
Enduring the
Inquisition
Obtaining Emotional First Aid
Moving On
Surviving
Impact Realization
Chaos and Accident Response
“Right after the code, I was having trouble concentrating.
It was nice to have people take over….that I trusted. I
was in so much shock I don’t think I was useful.”
Characteristics:- Error realized/event recognized- Tell someone/ get help!- Stabilize/treat patient- May not be able to continue care of
patient- Clinician commonly distracted

Intrusive Reflections
Characteristics:- Re-evaluate scenario- Self-isolate- Haunted re-enactments of event- Feelings of internal inadequacy
“I started to doubt myself... There were some things that I thought maybe if I’d have done it this way it wouldn’t have
happened…but everything was more clear looking at things in retrospect. I lost my
confidence for some time.”
Restoring Personal Integrity
Characteristics:- Acceptance among work/social
structure- Managing gossip/grapevine- Fear is prevalent
“I thought every single day for months I’d walk in and think
everyone knows what happened… I thought these
people are never going to trust me again.”
Enduring the Inquisition
Characteristics:- Realization of level of seriousness- Reiterate case scenario- Respond to multiple “why’s” about the event- Interact with many different even responders- Understanding even disclosure to patient/family- Physical and psychosocial symptoms
“I didn’t know what to do or who to talk to professionally or legally.”
---------------------------------------“Clearly, I know we needed to keep that quiet - it might have been helpful to be
able to talk to someone else but I couldn’t do that.”
Obtaining Emotional First Aid
Characteristics:- Identify who is safe to confide in- Hoping someone will reach out- Getting personal/professional
support- Litigation concerns emerge
“There was nobody I could tell, not even my husband. All I could say is I’ve had a
really horrible day.”
Moving On….Thriving
Characteristics:- Does not base practice/ work on one event- Minimal adverse effect from event- Advocates for patient safety initiatives- Tries to make a difference for the next
patient/clinician
“I was questioning myself over and over again…but then I thought … I’ve just had this experience in my life where I had to encounter this tragedy but it made me a better person. It really did, and it gave
me insight.”
Moving On….Surviving
Characteristics:- Coping with what happened- Persistent sadness prevails- Trying to learn from the event- Never quite the same……
“I figured out how to cope and how to say yes, I made a mistake. And that mistake caused a bad patient outcome but I haven’t figured out how to forgive myself for that or
forget it. It’s impossible to let it go.”
Moving On….Dropping Out
Characteristics:- Feelings of inadequacy/failure- Leave current role by transferring to
different facility/unit- Consider quitting profession altogether
“A fresh start was good for me.” --------------------------------
“I actually ended up moving to a different floor. My new supervisor who oriented me expressed confidence and belief in me and
helped me re-grow my own sense of confidence and self belief.”
The Drop OUT……….Defined as ‘a career transition as a direct result of a single unexpected patient event’.
Kim Hiatt, RN

Insights Into Dropping-Out
Vast majority in-patient care (77%)70% related to permanent harm/death of patient50% were direct care providers~58% assumed roles with less or equal risk to similar exposure
Rodriquez, J. & Scott, S.D. (2017). Dropping out and starting over: The impact of adverse events on clinicians. Joint Commission Journal on Quality and Patient Safety. 44:137-145. DOI: 10.1016/j.jcjq.2017.08.008.

Insights Into Dropping-Out (continued)
1/3 of participants reported significant decrease in joy and meaning of work post event. Major influencers to change role: 1) Inadequate social support and 2) Effects of emotional labor
Rodriquez, J. & Scott, S.D. (2017). Dropping out and starting over: The impact of adverse events on clinicians. Joint Commission Journal on Quality and Patient Safety. 44:137-145. DOI: 10.1016/j.jcjq.2017.08.008.
Further insight into dropping out……Cross sectional survey to 1,163 nurses from acute care public hospital in Singapore:
31.8% turnover intentions9.3% absenteeism
Nurses younger and less experienced more likely to experience greater second victim response.
Mok, W. Chin, G., Yap, S. & Wang, W. (2019). A cross-sectional survey on nurses’ second victim experience and quality of support resources in Singapore. J Nurs Manag, 2019; 001-8.

Unanticipated ClinicalEvent
Second Victim ReactionPsychosocial
Physical
Thriving
Surviving
Dropping OutInstitutional
ResponseClinician Support
Clinician Recovery
Tier 1
Tier 2
Tier 3
Comprehensive Tiered Support Interventions
Thriving
Surviving
Dropping Out
Second VictimIntervention Model
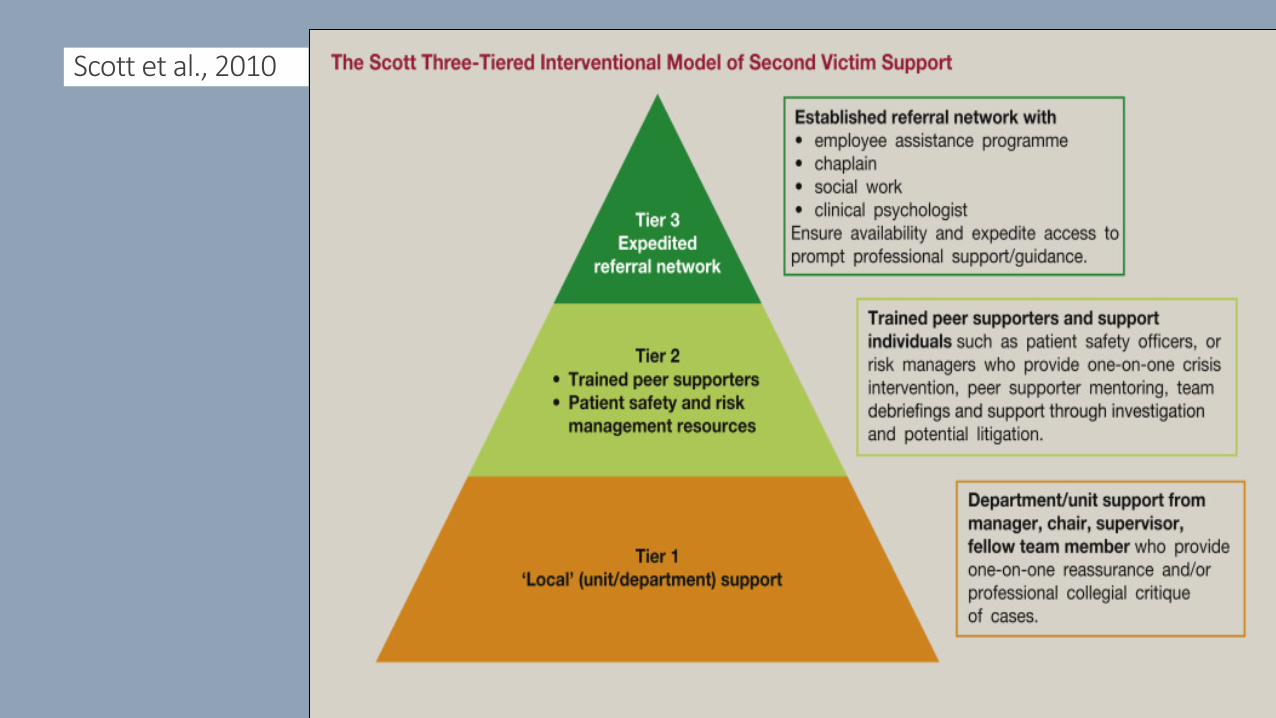
Scott et al., 2010
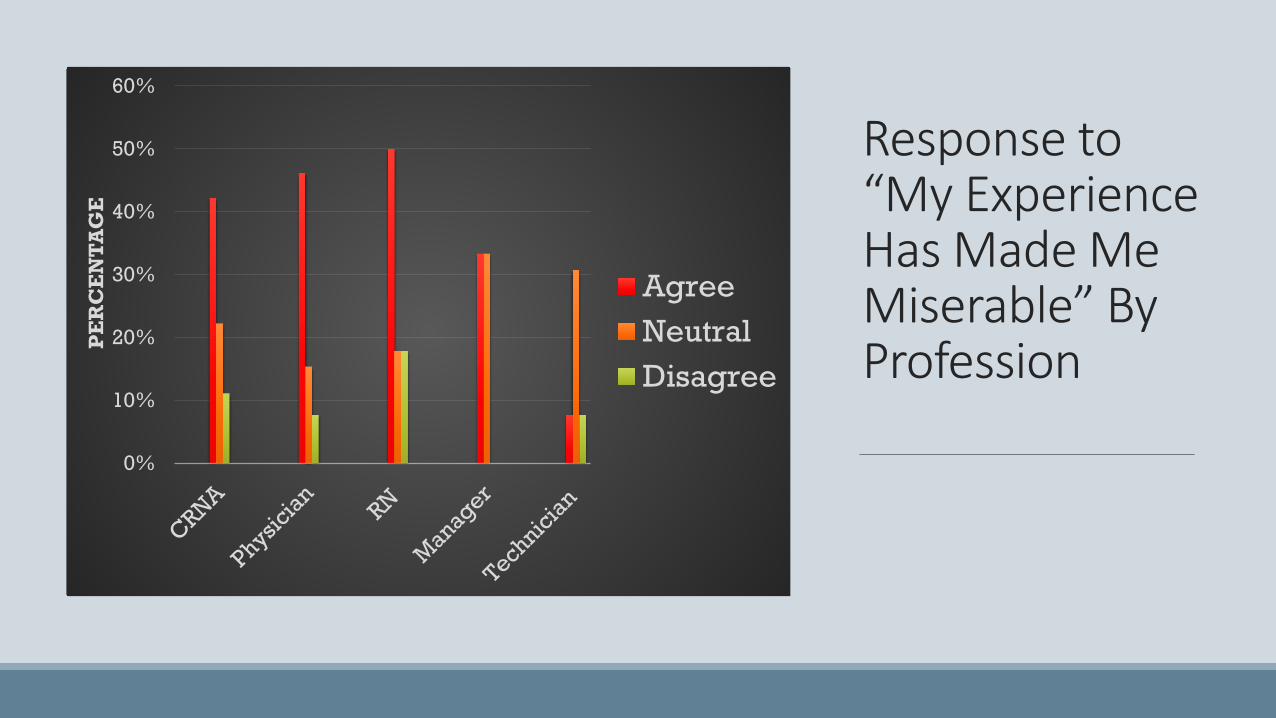
Response to “My Experience Has Made Me Miserable” By Profession
0%
10%
20%
30%
40%
50%
60%P
ER
CE
NT
AG
E
AgreeNeutralDisagree
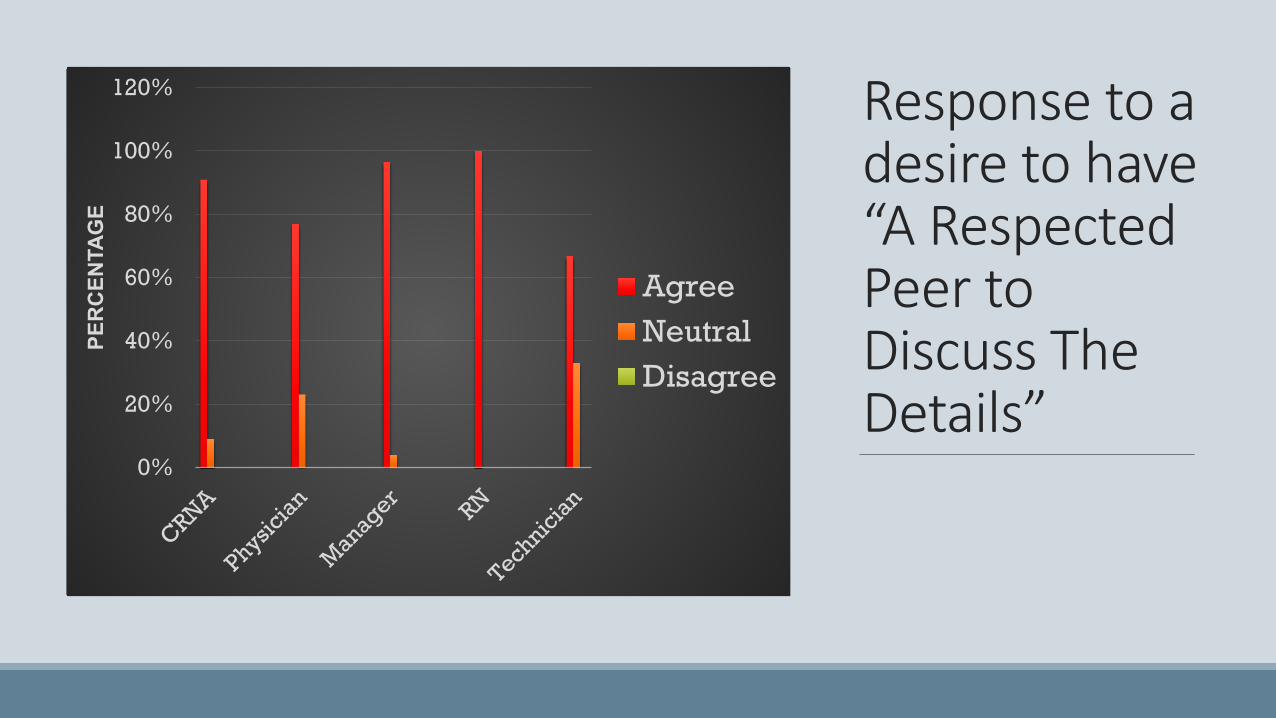
Response to a desire to have “A Respected Peer to Discuss The Details”
0%
20%
40%
60%
80%
100%
120%PE
RC
ENTA
GE
AgreeNeutralDisagree
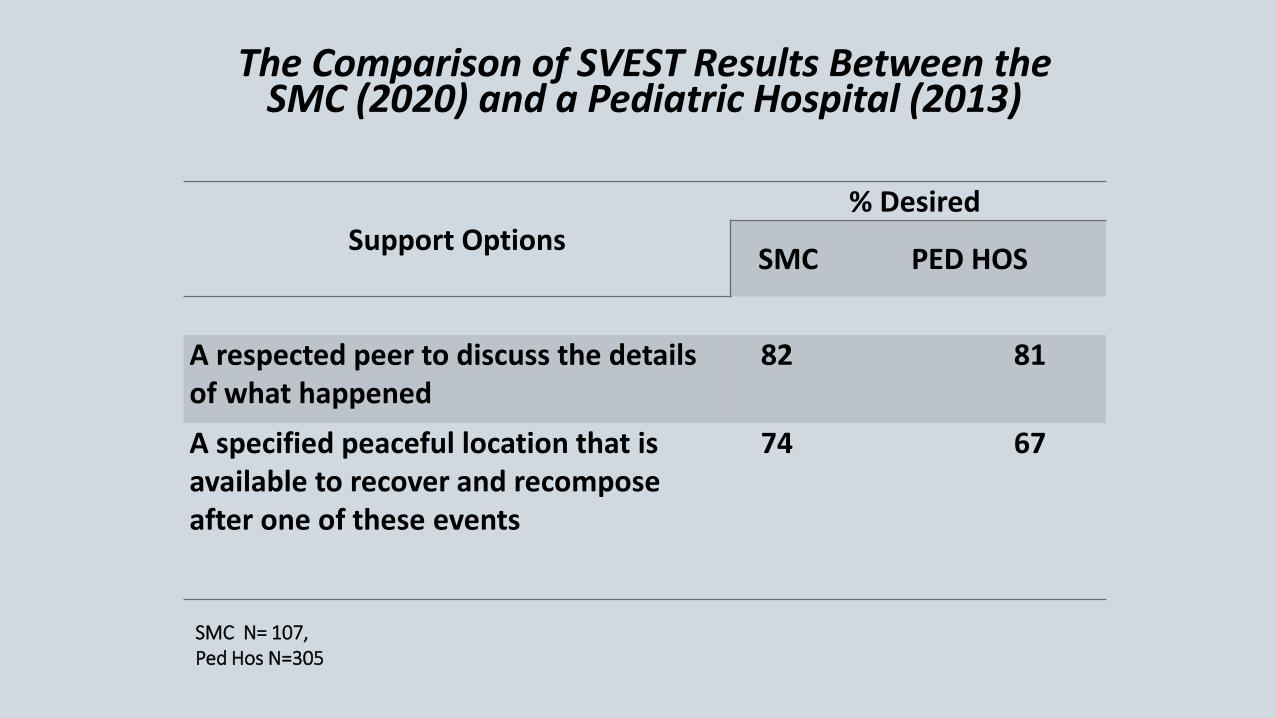
The Comparison of SVEST Results Between the SMC (2020) and a Pediatric Hospital (2013)
Support Options% Desired
SMC PED HOS
A respected peer to discuss the details of what happened
82 81
A specified peaceful location that is available to recover and recompose after one of these events
74 67
SMC N= 107, Ped Hos N=305

An Occupational Hazard: The Cost of Caring…•Burnout•Vicarious Trauma•Compassion Fatigue•Moral Distress•Second Victim Response
• Potential for ongoing psychological trauma, personally and professionally
• Safety and quality in care• Can ultimately lead to the loss of
providers/employees to the profession.
• Financial cost to the organization (lost wages, absenteeism., etc)
This Photo by Unknown Author is licensed under CC BY-NC-ND

Benefits of a Peer Support Network
Teammates have a way to get their needs metafter going through a traumatic event
Helps reduce the harmful effects of stress
Provides some normalization and helps the teammate get back to their routine after a traumatic event
Promotes the continuation of productive careers while building healthy stress management behaviors

WHY IS THIS IMPORTANT?
The teammate can return to their duties without lingering effects and their pre-event function in a normal capacity.
This Photo by Unknown Author is licensed under CC BY-NC-ND

LD.04.04.05 – EP 9
The leaders make support systems available for staff who have been involved in an adverse or sentinel event.
http://www.jointcommission.org/improving_Patient_Worker_Safety/
Guidelines - Regulatory
National Quality Forum – Safe Practice 8: Care for the Caregiver
GUIDELINES FOR CLINICIAN CARE (CONTINUED)
Provide care to the caregivers (clinical providers, staff, and administrators) involved in serious preventable harm to patients, through systems that also foster transparency and performance improvement that may reduce future harmful events.

Teammate engagement + satisfaction and well-being = improved patient satisfaction
and outcomes
This Photo by Unknown Author is licensed under CC BY-SA


AVAILABLE RESOURCES
• SHAREPOINT SITE• REDCAP METRIC TOOLS• 24/7 CONFIDENTIAL EMAIL TO REQUEST PEER SUPPORT
• EMBEDDED PEER SUPPORTERS WITHIN (2) ATRIUM’S PERIOPERATIVE FACILITIES
• ATRIUM HEALTH CABARRUS –7 PEER SUPPORTERS• ATRIUM HEALTH PINEVILLE – 10 PEER SUPPORTERS

Questions……
“ I’ve seen this frequently during my 30 plus years of clinical work. How come I didn’t truly ‘see’ it until today?” Pediatric Oncologist, 2017

This Photo by Unknown Author is licensed under CC BY-SA