Embed Size (px)
Citation preview

PHASE II STUDIES
Combination of docetaxel and TSU-68, an oral antiangiogenicagent, in patients with metastatic breast cancer previously treatedwith anthracycline: Randomized phase II multicenter trial
Sung-Bae Kim & Changhoon Yoo & Jungsil Ro & Seock-Ah Im & Young-Hyuck Im &
Jee Hyun Kim & Jin-Hee Ahn & Kyung Hae Jung & Hong Suk Song &
Seok Yun Kang & Hee Sook Park & Hyun-Cheol Chung
Received: 20 January 2014 /Accepted: 18 March 2014# Springer Science+Business Media New York 2014
Summary The novel oral antiangiogenic agent TSU-68 wasinvestigated in patients with metastatic breast cancer. Patientswith anthracycline-pretreated metastatic breast cancer were ran-domly assigned to receive either TSU-68 400 mg twice daily ondays 1–21 plus docetaxel 60 mg/m2 on day 1 every 3 weeks, ordocetaxel 60 mg/m2 on day 1 every 3 weeks. The primaryendpoint was progression-free survival. Between November2006 and December 2007, 81 patients were included in thisstudy (41 for TSU-68 plus docetaxel and 40 for docetaxel alone).Median progression-free survival was 6.8 months (95 % confi-dence interval [CI]=5.4–12.5 months) in the TSU-68 plus doce-taxel group and 8.1 months (95 % CI=4.0–13.7 months) in thedocetaxel-alone group (hazard ratio [HR]=1.0; 95 % CI=0.6–1.8; p=0.95). There were no significant differences in the overallresponse rates and overall survival between groups (p=0.29 and
p=0.42, respectively). In subgroup analysis, TSU-68 plus doce-taxel was associated with better overall survival than docetaxelalone in anthracycline-resistant patients (HR=0.3; 95%CI=0.1–0.8; p=0.02). Themost frequent adverse eventswere neutropeniaand anorexia in both arms. Although both regimens were welltolerated, grade 3/4 non-hematologic toxicity wasmore frequent-ly observed in the TSU-68 plus docetaxel group. Combination ofTSU-68 and docetaxel is well tolerated but failed to demonstratesuperior efficacy over docetaxel alone in anthracycline-pretreatedbreast cancer patients. As TSU-68 was associated with bettersurvival in the anthracycline-resistant subgroup, it should befurther explored in this subgroup.
Keywords TSU-68 . Breast cancer . Angiogenesis .
Docetaxel
S.-B. Kim and C. Yoo contributed equally to this work and should beconsidered as first co-authors.
S.<B. Kim :C. Yoo : J.<H. Ahn :K. H. JungDepartment of Oncology, Asan Medical Center, University of UlsanCollege of Medicine, Seoul, South Korea
J. RoCenter for Breast Cancer, National Cancer Center, Goyang, SouthKorea
S.<A. ImDepartment of Internal Medicine, Seoul National UniversityHospital, Seoul, South Korea
Y.<H. ImDivision of Hematology-Oncology, Samsung Medical Center,Sungkyunkwan University School of Medicine, Seoul, South Korea
J. H. KimDepartment of Internal Medicine, Seoul National UniversityBundang Hospital, Gyeonggi-do, South Korea
H. S. SongDivision of Hematology/Oncology, Department of Medicine,Keimyung University Dongsan Hospital, Daegu, South Korea
S. Y. KangDepartment of Hematology and Oncology, Ajou University Schoolof Medicine, Suwon, South Korea
H. S. ParkDepartment of Internal Medicine, Soonchunhyang UniversityHospital, Soonchunhyang University College of Medicine, Seoul,South Korea
H.<C. Chung (*)Department of Medical Oncology, Yonsei Cancer Center, YonseiUniversity College of Medicine, Seoul, South Koreae-mail: [email protected]
Invest New DrugsDOI 10.1007/s10637-014-0093-6

Introduction
Even though the survival of patients with metastatic orrecurrent breast cancer improves following the intro-duction of novel chemotherapy and targeted therapy,these patients still have unmet medical needs [1].Docetaxel is one of key drugs involved in the manage-ment of advanced breast cancer as a single agent or incombination with other drugs. Single-agent docetaxelon a dosing schedule of 60–100 mg/m2 every 3 weeksdemonstrates proven efficacy as a second-line breastcancer therapy [2]. In a previous phase III trial, timeto progression tended to improve following the admin-istration of higher doses of docetaxel (12.7 weeks for60 mg/m2 vs 15.0 weeks for 75 mg/m2 vs 16.6 weeksfor 100 mg/m2), though this finding was not statisti-cally significant according to the intention-to-treat anal-ysis and increased toxicity was noted [2].
Angiogenesis is a fundamental event in breast cancergrowth and metastasis [3–5]. According to supporting preclin-ical data, inhibition of angiogenesis has been a major target indevelopment of new breast cancer agents. A number of typesof antiangiogenic agents have been investigated in phase IIItrials on patients with advanced breast cancer. Bevacizumab, amonoclonal antibody that binds to vascular endothelialgrowth factor (VEGF), has been evaluated in combinationwith chemotherapy in six randomized phase III trials [6],and all except one trial reported improved progression-freesurvival (PFS) in bevacizumab-treated patients. None of thesetrials, however, proved improved overall survival (OS). Thesefindings led to the withdrawal of bevacizumab approval forbreast cancer treatment by the US Food and DrugAdministration. On the other hand, oral small moleculemultikinase inhibitors, which demonstrate a wide range oftargets, including VEGF receptor (VEGFR) and platelet-derived growth factor receptor (PDGFR), have also beeninvestigated to determine the role of antiangiogenesis in themanagement of patients with advanced breast cancer. Despitethe efficacy of sunitinib has not been proven in previous trials,sorafenib is now under investigation in a randomized phase IIItrial based on promising results of a previous phase II trial [6].
TSU-68 (orantinib) is a novel oral antiangiogenicmultikinase agent that selectively inhibits VEGFR-2,PDGFR, and fibroblast growth factor receptor (FGFR) [7].TSU-68 inhibits tumor growth in a number of human xeno-graft models, including breast, colon, stomach, prostate, andpancreas tumors [7–9]. Preclinical studies reported synergismbetween taxanes and TSU-68 in human breast cancer xeno-grafts without increased overall toxicity in comparison withTSU-68 or taxane alone [10]. Based on the results of threephase I trials conducted in Japan, the recommended dose ofTSU-68 for further development was determined to be400 mg/m2 twice daily [11].
TSU-68 was previously investigated in two single-armphase II trials, either as a single agent or in combination withdocetaxel [12, 13]. TSU-68 plus docetaxel demonstratedpromising anticancer activity in anthracycline-resistant breastcancer patients with response rates of 21 %, median time toprogression of 4.9 months, and OS of 19.3 months [13]. Thisstudy also reported no pharmacokinetic interactions betweenTSU-68 and docetaxel. Based on the results of these studies,we here conducted a randomized phase II study comparing theefficacy and safety of TSU-68 plus docetaxel and docetaxelalone in patients with metastatic breast cancer who had pre-viously been treated with anthracycline.
Methods
This was an open-label, randomized, multicenter phase IIstudy that compared TSU-68 plus docetaxel with docetaxelalone in patients with metastatic breast cancer who had re-ceived prior therapy with an anthracycline-containing regi-men. Nine referral hospitals in Korea participated in this study.This study was approved by the institutional review boards ofeach participating institution, and conducted in accordancewith the Declaration of Helsinki and Good Clinical Practiceguidelines. All participants provided written informed consentbefore enrollment.
Study population
Women with histologically or cytologically confirmed meta-static breast cancer were eligible for this study if they metfollowing inclusion criteria: age between 18 and 75 years;Eastern Cooperative Oncology Group (ECOG) performancestatus ≤2; ≥1 measurable lesion according to ResponseEvaluation Criteria In Solid Tumor (RECIST) version 1.0[14]; life expectancy ≥3 months; prior treatment with ananthracycline-containing regimen as neoadjuvant, adjuvanttherapy, or treatment for metastatic disease; no chemotherapyand radiotherapy for ≥4 weeks (6 weeks if mitomycin wasused); no hormone therapy for ≥2 weeks; complete recoveryfrom all relevant toxicities associated with prior anticancertreatment except alopecia; and adequate hematologic, hepatic,renal, and cardiac function. Neoadjuvant or adjuvant taxaneswere permitted if patients were disease-free for >12 months.Patients were excluded if they had following conditions:pregnant; currently breast feeding; symptomatic brain metas-tasis; inflammatory breast cancer, prior high-dose chemother-apy followed by hematopoietic stem cell support; concurrentmalignancies except adequately treated basal cell carcinomaof the skin or in situ carcinoma of the cervix; or any seriousmedical conditions. Prior therapy with taxanes for metastaticbreast cancer was not permitted.
Invest New Drugs

Study treatment
Eligible patients were randomized at a 1:1 ratio toreceive either docetaxel 60 mg/m2 on day 1 plus TSU-68 400 mg/m2 on days 1–21 every 3 weeks, or doce-taxel 60 mg/m2 alone on day 1 every 3 weeks.Randomization was accomplished using an interactivevoice response system. Prior use of taxanes (priortaxane vs no prior taxane use) and anthracycline sensi-tivity (resistant vs sensitive) were used as stratificationfactors. Anthracycline resistance was defined as recur-rence or progression <12 months after the completion ofanthracycline-containing neoadjuvant or adjuvant thera-py, or progression <6 months after the last dose ofchemotherapy for metastatic breast cancer. Otherwise,patients were considered to have anthracycline-sensitivedisease.
Study treatment was discontinued if patients developeddisease progression or unacceptable toxicity, or withdrewconsent. Doses were modified according to the worst gradeof toxicity allowed by the protocol: TSU-68 dose was reducedto 200 mg/m2 twice daily, and docetaxel was reduced to50mg/m2 and subsequently 40mg/m2. If patients experiencedunacceptable adverse events to only docetaxel, the continuousadministration of TSU-68 as monotherapy was allowed untildocumented disease progression or unacceptable TSU-68toxicity.
Efficacy and safety assessment
Pretreatment evaluation included medical history, physicalexamination, complete blood counts with differential counts,and renal and liver function tests. Baseline radiological tumorevaluations, including computed tomography (CT), magneticresonance imaging (MRI), and ultrasonography, were per-formed 4 weeks before enrollment. Response was evaluatedevery two cycles of treatment using the same imaging modal-ities, which were performed at baseline. Additional imagingwas performed if disease progression was clinically indicated,and objective response was confirmed by repeated assessment<4 weeks after the response criteria were first met. All imageswere evaluated by a Central Imaging Review Committee, andtumor response was determined according to RECIST version1.0. At each cycle, patients underwent adverse events (AEs)assessment, physical examination, and laboratory tests. AEswere graded according to the National Cancer InstituteCommon Terminology Criteria for Adverse Events version3.0. Any ongoing AEs were followed for 30 days after the lastdose of study treatment or until recovery or the start ofalternative anticancer therapy. Following the discontinuationof study treatment, patients underwent follow-up evaluationsevery 3 months to collect survival data.
Biomarker assays
Blood samples were collected at baseline and prior to the startof each cycle in order to evaluate potential TSU-68 bio-markers. Plasma levels of angiogenesis-related factors(VEGF, platelet-derived growth factor [PDGF]-AA, PDGF-AB, PDGF-BB, and fibroblast growth factor [FGF]), apopto-sis markers (soluble cytokeratin 18 [M65] and caspase-cleaved fragment of cytokeratin 18 [M30]) and inflammatorymarkers (C-reactive protein [CRP] and interleukin [IL]-6)were measured using enzyme-linked immunosorbent assays(ELISA). Baseline values and changes following study treat-ment were analyzed to determine the relationship with prog-nosis and TSU-68 efficacy. The results of these biomarkeranalyses will be presented elsewhere.
Statistical analysis
The primary end point was progression-free survival (PFS).The secondary endpoints included response rate, overall sur-vival (OS), and safety profile. PFS was defined as time be-tween randomization and disease progression or death fromany cause, whichever occurred first. OS was calculated as thetime from the date of randomization to the date of death fromany cause. Patients were censored if they were progression-free or alive at the last follow-up. Objective response rateswere calculated as the proportion of patients who demonstrat-ed complete response (CR) or partial response (PR), andclinical benefit rates were estimated as the proportion ofpatients who achieved CR, PR, or stable disease (SD) for≥6 months.
Based on the results of a phase III study on docetaxel [2],PFS of the docetaxel-alone group was estimated as 3 months.The median PFS of the TSU-68 plus docetaxel group wasassumed to be 5.5 months. According to Freedman’s formula,38 patients in each arm and a total of 72 events (progression ordeath) were needed to demonstrate superior PFS in the TSU-68 plus docetaxel group (1-sided alpha <5 % and 80 %power). Assuming a dropout rate of 5 %, a total of 80 patients(40 patients in each group) were required for this study.
The data cut-off point corresponded to 1 year after the lastpatient was randomized or the time of the 72nd event (pro-gression or death), whichever occurred earlier. The chi-squareor Fisher exact tests were used to analyze categorical vari-ables. The probability of survival was estimated using theKaplan-Meier method and compared using the log-rank test.Cox regression modeling was used to estimate hazard ratios(HRs), compare efficacy between the two arms of the primaryanalysis, and analyze prespecified subgroups. The efficacyand safety analyses was based on the full analysis set (FAS),which included all randomized patients who met eligibilitycriteria and received at least 1 dose of the study treatment. Thesafety analysis set included all patients who received ≥1 dose
Invest New Drugs

of the study medication. All statistical analyses were per-formed using SAS version 8.2 (SAS Institute, Cary, NC).
Results
Patients
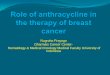
Between November 4, 2006 and December 13, 2007, a total of81 patients were enrolled and randomized to receive eitherTSU-68 plus docetaxel (n=41) or docetaxel alone (n=40).Two patients in the TSU-68 plus docetaxel arm and a patientin the docetaxel-alone arm did not receive study treatment,and a patient in the TSU-68 plus docetaxel arm did not meeteligibility criteria. Thus, the remaining 77 patients (38 in theTSU-68 plus docetaxel arm and 39 in the docetaxel-alonearm) were included in the FAS for efficacy analyses (Fig. 1).Thirty-nine patients were included in each group of the safetyanalysis set. Patient baseline characteristics are presented inTable 1. The majority of patients (78 %) were <60 years, andabout 30 % of patients were premenopausal. Prior to studyentry, 21 % and 62 % of patients had received taxanes andhormonal therapy, respectively. Estrogen receptor and HER2were positive in 46 (60 %) and 11 (14 %) patients, respective-ly. According to the prespecified definition, 52 (67 %) and 25(33 %) patients were classified with anthracycline-sensitive
and -resistant disease, respectively. There were no notabledifferences in the baseline characteristics between groups. Atthe time of analysis, 26 (68 %) and 26 (67 %) patients showeddisease progression, and 19 (51 %) and 21 (58 %) patientsdied in the TSU-68 plus docetaxel and docetaxel-alonegroups, respectively.
Efficacy
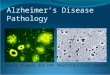
The median PFS determined by independent review—the pri-mary endpoint of this study—was 6.8 months (95 % confidenceinterval [CI]: 5.4–12.5 months) in the TSU-68 plus docetaxelarm and 8.1 months (95 % CI: 4.0–13.7 months) in thedocetaxel-alone arm (Fig. 2). There was no significant differenceof PFS between groups (HR=1.0, 95 % CI: 0.6–1.8; stratified 1-sided p=0.90). This was consistent with investigator-assessedPFS (TSU-68 plus docetaxel: median 7.0 months [95%CI: 5.4–9.8months]; docetaxel-alone: median 9.3months [95%CI: 5.6–15.5 months]; HR=1.2, 95 % CI: 0.7–2.1; p=0.50). Median OSwas 29.0 months (95 % CI: 23.8–33.3 months) in the TSU-58plus docetaxel arm and 26.0 months (95 % CI: 13.9 months–notassessable) in the docetaxel-alone arm (HR=0.8; 95 % CI:0.5–1.6; p=0.42).
Response assessment was available in 37 patients in theTSU-68 plus docetaxel arm and 36 patients in the docetaxel-alone arm (Table 2). CR was achieved in 1 patient in the TSU-
Fig. 1 CONSORT diagram
Invest New Drugs

68 plus docetaxel arm, and PRwas confirmed in 18 patients inthe TSU-68 plus docetaxel arm and 16 patients in the
docetaxel-alone arm, indicating objective response rates of50.0 % (95 % CI: 33.4–66.6 %) in the TSU-68 plus docetaxelarm and 41.0% (95%CI: 25.6–57.9%) in the docetaxel alonearm (p=0.29). Clinical benefit rates were 60.5 % (95 % CI:43.4–76.0 %) in the TSU-68 plus docetaxel arm and 51.3 %(95 % CI: 34.8–67.6 %) in the docetaxel-alone arm (p=0.28).The patient who achieved CR in the TSU-68 plus docetaxelarm was diagnosed with anthracycline-sensitive, estrogenreceptor-positive, and HER2-negative breast cancer and hadbeen previously treated with taxane.
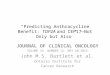
Subgroup analyses were performed on prespecifiedpatient subgroups (anthracycline-sensitive/resistant, priortaxanes/non-prior taxane, estrogen receptor-positive/neg-ative, progesterone receptor-positive/negative, HER2-positive/negative, triple-negative). Although PFS did notdiffer across all subgroups between arms, the TSU-68plus docetaxel arm was significantly associated withbetter OS in comparison with the docetaxel-alone arm(median OS=29.0 months [95 % CI: 27.5–33.3 months]vs 13.2 months [95 % CI: 10.0–19.5 months]; HR=0.3,95 % CI : 0 .1–0 .8 ; p = 0 .02) in pa t i en t s wi thanthracycline-resistant breast cancer (Fig. 3), whereas
Fig. 2 Progression-free survival(a) and overall survival (b). Thedotted lines indicate 95 %confidence interval
Table 2 Response according to RECIST version 1.0
TSU-68 plus docetaxel(n=38), n (%)
Docetaxel (n=39),n (%)
CR 1 (3 %) 0
PR 18 (47 %) 16 (41 %)
SD 12 (32 %) 11 (28 %)
SD ≥24 weeks 4 (11 %) 4 (10 %)
PD 6 (16 %) 9 (23 %)
Not assessed 1 (3 %) 3 (8 %)
CR complete response; PR partial response, SD stable disease; PDprogressive disease
Table 1 Baseline characteristics
TSU-68 plus docetaxel(n=38)
Docetaxel(n=39)
Age (y), median (range) 52 (25–68) 50 (30–73)
ECOG performance status
0 21 (55 %) 19 (49 %)
1 15 (40 %) 15 (38 %)
2 2 (5 %) 5 (13 %)
Menopausal status
Premenopausal 11 (29 %) 16 (41 %)
Postmenopausal 27 (71 %) 23 (59 %)
Anthracycline sensitivity
Resistant 13 (34 %) 12 (31 %)
Sensitive 25 (66 %) 27 (69 %)
HER2 status (IHC or FISH)
Positive 6 (16 %) 5 (13 %)
Negative 27 (71 %) 34 (87 %)
Estrogen receptor status
Positive 26 (70 %) 20 (51 %)
Negative 11 (30 %) 19 (49 %)
Progesterone receptor status
Positive 20 (54 %) 17 (44 %)
Negative 17 (46 %) 22 (56 %)
Previous therapy
Surgery 34 (90 %) 38 (97 %)
Hormonal therapy 25 (66 %) 23 (59 %)
Radiotherapy 21 (55 %) 26 (67 %)
Chemotherapy
Anthracycline 38 (100 %) 39 (100 %)
Taxanes 8 (21 %) 8 (21 %)
ECOG Eastern Cooperative Oncology Group, IHC immunohistochemis-try, FISH fluorescence in situ hybridization
Invest New Drugs

there were no differences in anthracycline-sensitive pa-tients (HR=1.3, 95 % CI: 0.6–2.9; p=0.52).
Safety
The AEs occurred in more than 10 % of patients are summa-rized in Table 3. All patients in both arms experienced AEs.The most frequent AEs in both arms were neutropenia andanorexia. Edema, anorexia, hand-foot syndrome, and periph-eral sensory neuropathy were more common in the TSU-68plus docetaxel arm. Change in urine color was only observedin patients who received TSU-68 plus docetaxel. However,these AEs were generally mild in severity as grade 1 or 2 andmanageable with supportive care. Grade 3 or higher AEs weremore common in the TSU-68 plus docetaxel arm. The mostfrequent grade 3 or higher AEs were neutropenia (90 % vs92 %), followed by anorexia (15 % vs 8 %), myalgia (8 % vs8 %), peripheral sensory neuropathy (8 % vs 5 %), andpneumonia (8 % vs 3 %). Although there were no treatment-related deaths in the docetaxel-alone arm, 1 patient in theTSU-68 plus docetaxel arm died due to febrile neutropeniathat was complicated by pneumonia and sepsis.
The total number of treatment cycles per patient (mean±standard deviation) was 12.0±10.37 cycles in the TSU-68plus docetaxel group and 10.6±10.20 cycles in thedocetaxel-alone group. Doses were interrupted and modifieddue to the AEs in 10 (26 %) and 5 (13 %) patients, respec-tively, in the TSU-68 plus docetaxel group, and 5 (13 %) and10 (26 %) patients, respectively, in the docetaxel-alone group.The most common AEs that led to dose modification werefebrile neutropenia in both arms (3 patients each in the TSU-
68 plus docetaxel and docetaxel-alone arms). Study treatmentwas discontinued in 14 (36 %) and 5 (13 %) patients in theTSU-68 plus docetaxel and docetaxel-alone arms, respective-ly. In the TSU-68 plus docetaxel group, study treatments werediscontinued most frequently due to fatigue (n=4; 10 %) andperipheral edema (n=4; 10 %).
Discussion
This randomized phase II trial shows that the combination ofdocetaxel and TSU-68—a novel tyrosine kinase inhibitor thattargets VEGFR-2 and PDGFR—is feasible in patients withmetastatic breast cancer. Although this study was conductedbased on the strong rationale provided by preclinical studies,TSU-68 plus docetaxel failed to meet the primary endpoint,superiority to docetaxel alone in terms of PFS (median6.8 months for TSU-68 plus docetaxel vs 8.1 months fordocetaxel alone). Moreover, there were no significant differ-ences in terms of response rates (50.0 % vs 41.0 %), clinicalbenefit rates (60.5 % vs 51.3%), and OS (median 29.0monthsvs 26.0 months). According to the preplanned subgroup anal-yses, no subgroup benefited from combination therapy interms of PFS. However, TSU-68 plus docetaxel resulted insignificant improvement in OS among patients withanthracycline-resistant breast cancer (median 29.0 months vs13.2 months; HR=0.3). Although this trial was not statistical-ly designed for this comparison, our findings suggest thepotential benefits of TSU-68 in anthracycline-resistant breastcancer and warrant further investigation of TSU-68 in thispatient group.
The results of our study are in line with previous studies onsunitinib, another multi-targeted tyrosine kinase inhibitor withantiangiogenic activities. In a number of phase III trials,sunitinib was tested in combination with various chemother-apeutic agents, such as capecitabine, paclitaxel, and docetaxel.In all of these trials, however, sunitinib failed to demonstratesurvival benefits or even showed worse survival outcomescompared with the active comparator with excessive toxicity[15–18]. Considering that the addition of bevacizumab tochemotherapy has at least consistently demonstrated im-proved PFS despite the lack of benefits to OS, this discrepancyin the outcomes between monoclonal antibody andmultikinase inhibitor could be attributed to the different clas-ses of these agents. On the other hand, a recent randomizedphase IIb trial on patients with HER2-negative advancedbreast cancer demonstrated that sorafenib-capecitabine com-bination resulted in significant improvement in PFS in com-parison with placebo-capecitabine (median 6.4 months vs4.1 months; HR=0.58) [19]. A modest but statistically signif-icant improvement in PFS with the addition of sorafenib wasalso reported in another phase IIb trial, which comparedsorafenib with placebo in combination with gemcitabine or
Fig. 3 Overall survival in patients with anthracycline-resistant breastcancer. The dotted lines indicate 95 % confidence interval
Invest New Drugs

capecitabine (median 3.4 months vs 2.7 months; HR=0.65)[20]. Although the addition of sorafenib did not improve OSin these trials, a randomized phase III trial defining the role ofsorafenib in HER2-negative advanced breast cancer is ongo-ing (RESILIENCE study). The results of this phase III studymay give the clues whether differences in the target profiles ofantiangiogenic multikinase inhibitors have a significant im-pact on outcomes in patients with advanced breast cancer.
There are several possible explanations for the limitedefficacy of TSU-68 plus docetaxel in advanced breast cancer.Although the TSU-68 dose and schedule were based on theresults of three phase I trials [11, 21, 22], current TSU-68dosing might be insufficient to have clinically significantantiangiogenic activities. In our pharmacodynamic analysis,which measured changes in candidate biomarkers in order toassess the activity of the VEGF and PDGF pathways, wecould not find significant differences between the two groupsduring study treatment, except PDGF-BB (data not shown).The different target profile of TSU-68, which strongly inhibitsPDGFR [7], may impact activity against advanced breastcancer, especially considering that other antiangiogenic agentspredominantly target the VEGF pathway. One of other con-sideration is the backbone or partner chemotherapy. Since
monotherapy with antiangiogenic agents demonstrates onlylimited efficacy, many of them have been investigated incombined with cytotoxic agents [4]. However, optimal che-motherapy agents, dose, and schedule in combination withantiangiogenic agents have not yet been defined. The mixedresults of previous trials on the same antiangiogenic agentswhen different partner agents were used suggest that optimiz-ing the partner chemotherapy regimen may be critical to thesuccess of clinical trials investigating antiangiogenic agents[19, 23–26]. Because docetaxel is a standard second-linetherapy following anthracycline failure in breast cancer pa-tients, a number of antiangiogenic agents have been tested incombination with docetaxel. However, most of these havefailed [16, 27, 28], and bevacizumab only showed modestPFS benefit when combined with docetaxel, in comparisonwith weekly paclitaxel [23, 26]. These findings suggest thatdocetaxel might not be the optimal partner for combinationwith antiangiogenic agents.
The addition of TSU-68 to docetaxel was tolerable, al-though toxicities generally increased as expected. Most toxic-ities were mild and manageable in both regimens. The fre-quency of dose interruption and modification in the TSU-68plus docetaxel arm was comparable to docetaxel alone. The
Table 3 Adverse events reportedby ≥10 % of patients
HFS hand-foot syndrome
Toxicity grade by treatment arm
TSU-68 plus docetaxel (n=39) Docetaxel (n=39)
All grade Grade ≥3 All grades Grade ≥3
Hematologic
Neutropenia 35 (90 %) 35 (90 %) 36 (92 %) 36 (92 %)
Febrile neutropenia 5 (13 %) 5 (13 %) 5 (13 %) 5 (13 %)
Anemia 6 (15 %) 2 (5 %) 4 (10 %) 1 (3 %)
Non-hematologic
Abdominal pain 15 (38 %) 0 13 (33 %) 2 (5 %)
Constipation 8 (21 %) 0 13 (33 %) 1 (3 %)
Diarrhea 21 (54 %) 1 (3 %) 19 (58 %) 1 (3 %)
Nausea 20 (51 %) 2 (5 %) 19 (58 %) 0
Vomiting 14 (36 %) 2 (5 %) 11 (28 %) 0
Asthenia 7 (18 %) 3 (8 %) 6 (15 %) 0
Facial edema 27 (69 %) 0 13 (33 %) 0
Stomatitis 5 (13 %) 1 (3 %) 4 (10 %) 0
Anorexia 31 (79 %) 6 (15 %) 24 (62 %) 3 (8 %)
Arthralgia 7 (18 %) 1 (3 %) 10 (26 %) 0
Myalgia 26 (67 %) 3 (8 %) 27 (69 %) 3 (8 %)
HFS 11 (28 %) 0 6 (15 %) 2 (5 %)
Chromaturia 7 (18 %) 0 0 0
Peripheral motor neuropathy 7 (18 %) 2 (5 %) 5 (13 %) 2 (5 %)
Peripheral sensory neuropathy 21 (54 %) 3 (8 %) 15 (38 %) 2 (5 %)
Nail change 18 (46 %) 1 (3 %) 11 (28 %) 1 (3 %)
Invest New Drugs

most common grade 3 or higher AEs were neutropenia, an-orexia, myalgia, peripheral sensory neuropathy, and pneumo-nia. Although these severe AEs were manageable by doseinterruption and supportive care, there was 1 treatment-related death in the TSU-68 plus docetaxel arm due to com-plicated febrile neutropenia.
In conclusion, although the combination of TSU-68 anddocetaxel was feasible, there were no differences in efficacy incomparison with docetaxel monotherapy in anthracycline-pretreated patients with advanced breast cancer. As potentialactivity of TSU-68 in patients with anthracycline-resistantbreast cancer has been shown in present study, further inves-tigations are warranted to demonstrate the efficacy of TSU-68in this subgroup.
Disclosure The authors have nothing to disclose.
References
1. Chia SK, Speers CH, D’yachkova Y, Kang A, Malfair-Taylor S,Barnett J, Coldman A, Gelmon KA, O’reilly SE, Olivotto IA(2007) The impact of new chemotherapeutic and hormone agentson survival in a population-based cohort of women with metastaticbreast cancer. Cancer 110(5):973–979. doi:10.1002/cncr.22867
2. Harvey V, Mouridsen H, Semiglazov V, Jakobsen E, Voznyi E,Robinson BA, Groult V, Murawsky M, Cold S (2006) Phase III trialcomparing three doses of docetaxel for second-line treatment ofadvanced breast cancer. J Clin Oncol 24(31):4963–4970
3. Hicklin DJ, Ellis LM (2005) Role of the vascular endothelial growthfactor pathway in tumor growth and angiogenesis. J Clin Oncol23(5):1011–1027
4. Gasparini G, Longo R, Fanelli M, Teicher BA (2005) Combination ofantiangiogenic therapy with other anticancer therapies: results, chal-lenges, and open questions. J Clin Oncol 23(6):1295–1311
5. Dvorak HF, Brown LF, Detmar M, Dvorak AM (1995) Vascularpermeability factor/vascular endothelial growth factor, microvascularhyperpermeability, and angiogenesis. Am J Pathol 146(5):1029–1039
6. Reddy S, Raffin M, Kaklamani V (2012) Targeting angiogenesis inmetastatic breast cancer. Oncologist 17(8):1014–1026
7. Laird AD, Vajkoczy P, Shawver LK, Thurnher A, Liang C,Mohammadi M, Schlessinger J, Ullrich A, Hubbard SR, Blake RA,Fong TA, Strawn LM, Sun L, Tang C, Hawtin R, Tang F, Shenoy N,Hirth KP, McMahon G, Cherrington (2000) SU6668 is a potentantiangiogenic and antitumor agent that induces regression ofestablished tumors. Cancer Res 60(15):4152–4160
8. Machida S, SagaY, Takei Y,Mizuno I, Takayama T, Kohno T, KonnoR, Ohwada M, Suzuki M (2005) Inhibition of peritoneal dissemina-tion of ovarian cancer by tyrosine kinase receptor inhibitor SU6668(TSU-68). Int J Cancer 114(2):224–229. doi:10.1002/ijc.20751
9. Naumova E, Ubezio P, Garofalo A, Borsotti P, Cassis L, Riccardi E,Scanziani E, Eccles SA, Bani MR, Giavazzi R (2006) The vasculartargeting property of paclitaxel is enhanced by SU6668, a receptortyrosine kinase inhibitor, causing apoptosis of endothelial cells andinhibition of angiogenesis. Clin Cancer Res 12(6):1839–1849
10. Yonekura K, Basaki Y, Fujita H, Chikahisa L, Hashimoto A,Cherrington J, Shavwer L, Yamada Y, Kitazata K (2001) Inhibitionof VEGF/KDR signaling by TSU-68 (SU6668), an oral anti-
angiogenic agent, can synergistically enhance the anti-tumor activityof taxol; a new paradigm for breast cancer chemotherapy. BreastCancer Res Treat 69:216, abstr 29
11. Murakami H, Ueda Y, Shimoyama T, Yamamoto N, Yamada Y,Arioka H, Tamura T (2011) Phase I, pharmacokinetic, and biologicalstudies of TSU-68, a novel multiple receptor tyrosine kinase inhibi-tor, administered after meals with solid tumors. Cancer ChemotherPharmacol 67(5):1119–1128. doi:10.1007/s00280-010-1405-y
12. Suzuki Y, Saeki T, Aogi K, Toi M, Fujii H, Inoue K, Watanabe T,Fujiwara Y, Ito Y, Takatsuka Y, Iwata H, Arioka H, Tokuda Y (2013)A multicenter phase II study of TSU-68, a novel oral multipletyrosine kinase inhibitor, in patients with metastatic breast cancerprogressing despite prior treatment with an anthracycline-containingregimen and taxane. Int J Clin Oncol 18(4):590–597. doi:10.1007/s10147-012-0421-9
13. Toi M, Saeki T, Iwata H, Inoue K, Tokuda Y, Sato Y, Ito Y, Aogi K,Takatsuka Y, Arioka H (2012) A multicenter phase II study of TSU-68, an oral multiple tyrosine kinase inhibitor, in combination withdocetaxel in metastatic breast cancer patients with anthracyclineresistance. Breast Cancer. doi:10.1007/s12282-012-0344-3
14. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS,Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT,Christian MC, Gwyther SG (2000) New guidelines to evaluate theresponse to treatment in solid tumors. European Organization forResearch and Treatment of Cancer, National Cancer Institute of theUnited States, National Cancer Institute of Canada. J Natl Cancer Inst92(3):205–216
15. Barrios CH, Liu MC, Lee SC, Vanlemmens L, Ferrero JM, Tabei T,Pivot X, Iwata H, Aogi K, Lugo-Quintana R, Harbeck N, BrickmanMJ, Zhang K, Kern KA, Martin M (2010) Phase III randomized trialof sunitinib versus capecitabine in patients with previously treatedHER2-negative advanced breast cancer. Breast Cancer Res Treat121(1):121–131. doi:10.1007/s10549-010-0788-0
16. Bergh J, Bondarenko IM, Lichinitser MR, Liljegren A, Greil R,Voytko NL, Makhson AN, Cortes J, Lortholary A, Bischoff J, ChanA, Delaloge S, Huang X, Kern KA, Giorgetti C (2012) First-linetreatment of advanced breast cancer with sunitinib in combinationwith docetaxel versus docetaxel alone: results of a prospective,randomized phase III study. J Clin Oncol 30(9):921–929
17. Robert NJ, Saleh MN, Paul D, Generali D, Gressot L, Copur MS,Brufsky AM, Minton SE, Giguere JK, Smith JW, Richards PD,Gernhardt D, Huang X, Liau KF, Kern KA, Davis J (2011)Sunitinib plus paclitaxel versus bevacizumab plus paclitaxel forfirst-line treatment of patients with advanced breast cancer: a phaseIII, randomized, open-label trial. Clin Breast Cancer 11(2):82–92
18. Crown J, Dieras V, Staroslawska E, YardleyD, DavidsonN, BachelotT, Tassell V, Huang X, Kern K, Romieu G (2010) Phase III trial ofsunitinib (SU) in combination with capecitabine (C) versus C inpreviously treated advanced breast cancer (ABC). J Clin Oncol28(18 suppl), abstr LBA1011
19. Baselga J, Segalla JG, Roche H, Del Giglio A, Pinczowski H,Ciruelos EM, Filho SC, Gomez P, Van Eyll B, Bermejo B,Llombart A, Garicochea B, Duran MA, Hoff PM, Espie M, deMoraes AA, Ribeiro RA, Mathias C, Gil Gil M, Ojeda B, MoralesJ, Kwon Ro S, Li S, Costa F (2012) Sorafenib in combination withcapecitabine: an oral regimen for patients with HER2-negative local-ly advanced or metastatic breast cancer. J Clin Oncol 30(13):1484–1491
20. Hudis C, Tauer K, Hermann R, Makari-Judson G, Isaacs C, Beck J(2011) Sorafenib (SOR) plus chemotherapy (CRx) for patients (pts)with advanced (adv) breast cancer (BC) previously treated withbevacizumab (BEV). J Clin Oncol 29:1009
21. Ueda Y, Shimoyama T, Murakami H, Yamamoto N, Yamada Y,Arioka H, Tamura T (2011) Phase I and pharmacokinetic study ofTSU-68, a novel multiple receptor tyrosine kinase inhibitor, by twicedaily oral administration between meals in patients with advanced
Invest New Drugs

solid tumors. Cancer Chemother Pharmacol 67(5):1101–1109. doi:10.1007/s00280-010-1404-z
22. Kanai F, Yoshida H, Tateishi R, Sato S, Kawabe T, Obi S, Kondo Y,Taniguchi M, Tagawa K, Ikeda M, Morizane C, Okusaka T, AriokaH, Shiina S, Omata M (2011) A phase I/II trial of the oralantiangiogenic agent TSU-68 in patients with advanced hepatocellu-lar carcinoma. Cancer Chemother Pharmacol 67(2):315–324. doi:10.1007/s00280-010-1320-2
23. Miller K, Wang M, Gralow J, Dickler M, Cobleigh M, Perez EA,Shenkier T, Cella D, Davidson NE (2007) Paclitaxel plusbevacizumab versus paclitaxel alone for metastatic breast cancer. NEngl J Med 357(26):2666–2676
24. Robert NJ, Dieras V, Glaspy J, Brufsky AM, Bondarenko I, LipatovON, Perez EA, Yardley DA, Chan SY, Zhou X, Phan SC,O’Shaughnessy J (2011) RIBBON-1: randomized, double-blind,placebo-controlled, phase III trial of chemotherapy with or withoutbevacizumab for first-line treatment of human epidermal growthfactor receptor 2-negative, locally recurrent or metastatic breast can-cer. J Clin Oncol 29(10):1252–1260
25. Bondarde S, Kaklamani V, Sahoo TP, Lokanatha D, Raina V, Jain M,Schwartzberg L, GradisharWJ (2010) Sorafenib in combination withpaclitaxel as a first-line therapy in patients with locally recurrent or
metastatic breast cancer: overall survival results from a double-blind,randomized, placebo-controlled, phase 2b trial. Cancer Res 70(24suppl), abstr P2-16-03
26. Miles DW, Chan A, Dirix LY, Cortes J, Pivot X, Tomczak P, DelozierT, Sohn JH, Provencher L, Puglisi F, Harbeck N, Steger GG,Schneeweiss A, Wardley AM, Chlistalla A, Romieu G (2010)Phase III study of bevacizumab plus docetaxel compared with place-bo plus docetaxel for the first-line treatment of human epidermalgrowth factor receptor 2-negative metastatic breast cancer. J ClinOncol 28(20):3239–3247
27. Mariani G, Burdaeva O, Roman L, Staroslawska E, Udovitsa D,Driol P, Goisis G, Zamagni C, Semiglazov V, Gianni L (2011) Adouble-blind, randomized phase lib study evaluating the efficacy andsafety of sorafenib (SOR) compared to placebo (PL) when adminis-tered in combination with docetaxel and/or letrozole in patients withmetastatic breast cancer (MBC): FM-B07-01 Trial. Eur J Cancer 47:10
28. Rugo HS, Stopeck AT, Joy AA, Chan S, Verma S, Lluch A, Liau KF,Kim S, Bycott P, Rosbrook B, Bair AH, Soulieres D (2011)Randomized, placebo-controlled, double-blind, phase II study ofaxitinib plus docetaxel versus docetaxel plus placebo in patients withmetastatic breast cancer. J Clin Oncol 29(18):2459–2465
Invest New Drugs