Embed Size (px)
Citation preview

COMBINED MOVEMENTS OF THE LUMBAR SPINE:EXAMINATION AND CLINICAL SIGNIFICANCE
BRIAN C. EDWARDSPrivate Practitioner, West Perth
The aim of this paper is to describe a method of examining the lumbar spine, incorporating theprinciple of combining movements and relating this to selection of technique. Almost all of the passivemovement procedures used in the treatment of the lumbar spine are, in [act, procedures which involvecombining or coupling different movements. The importance of examining the lumbar spine usingthe principles of combining movements is emphasised and it is suggested that this should be a centralpart of any planned examination. The importance of relating these movements to range and distribution of pain is considered in detail and the application of techniques, rotation in particular isdescribed using positions which involve the combining of different movements.
The movements of the vertebral columnare complex and there has been a considerableamount of material published on this subject.Most of the studies seem to have been relatedto the movements of flexion and extension,presumably as this is the easiest movement todescribe, perform and control. Results vary butit would seem that most ranges of movementlie between 60° to 75° (Begg and Falconer,1949; Clayson, Newman, Debevec, Anger,Skowland and Kottke, 1962; Davis, Troup andBurnard, 1965; Loebl, 1967; Troup, Hood andChapman, 1967; Wiles, 1935). Allbrook (1957)found in his study, which was conducted onindividuals not complaining of lumbar pain,that movement between L4 and LS was greatestand gradually lessened as one moved to the upperlumbar spine. Farfan (1975) showed that thespine elongated as it flexed revealing that thereis about 25% enlongation at the level of thefacet capsules at 60° of spinal flexion. Notquite as much has been published relating tothe movement of lateral flexion. Tanz (1953)concluded that lateral flexion was about 2/3of the range of flexion and extension for thewhole of the lumbar spine except L5 and Sl.Hasner, Schalimizek, and Snorrason (1952)described the spines of each vertebral bodycombining to form an arcuate line in lateralflexion, and the vertebral bodies angled inrelationship to one another. The results of Moll,Liyanage and Wright (1972) indicated thatthere was about 10°-45° of lateral angular
BRIAN C. EDWARDS is in private practice as well asholding a half time appointment as lecturer in theGraduate Diploma in Manipulative Therapy offeredby the Department of Physiotherapy at the WesternAustralian Institute of Technology. He has been involved in teaching graduate physiotherapists in jointmanipulation and mobilisation since 1968. In 1975he completed an extensive study tour of Europe,United States of America and throughout Australia:he is currently emolled in a Masters programme inAnatomy at the University of Western Australia.
Aust. J. Physiother. 25,4, August,1979
bending and 2.6-7.8 cm of linear movement ofthe trunk laterally.
There have been relatively few studies ofrotation of the lumbar spine. Tanz (1953)reported a range of rotation in the lumbarspine but was not able to measure it. Gregersonand Lucas (1967) compared ranges of rotationduring sitting, standing and walking: theirresults indicated that more rotation occurredin standing, particularly at the lumbosacraljoint. Lumsden and Morris (1968) showed thatthere was an average of 6° of rotation at thelumbosacral joint during maximum rotation ofthe trunk and that rotation of the joint wasalways combined with some flexion. Loebl(1973) showed a mean regional rotation of thelumbar spine of 25°.
The combination of movements, namelyflexion, extension, lateral flexion and rotationor coupling, as it has been called, has been investigated by a number of authors (Farfan,1975; Loebl, 1973; Rolander, 1966; Troupet al., 1967). Gregerson and Lucas (1 967)found that axial rotation was to the left whenthe Sil bject bent to the left and to the rightwhen bending to the right. They did find thatin one subject the reverse was the case. Lovell(1903) stated that when the spine was fixed atits lower end and bent forward and to the left,it twisted to the right. Stoddard (1959) reported the opposite. Schultz, Belytschko,Andriacchi and Galante (1973) showed thatcounter-clockwise axial rotation towards theconcavity of the curve was evident, but wasvery small. Arkin (1950) showed that in adultsrotation to the convexity of the curve appeared when the spine was in lateral flexion,whether it was in flexion, extension or neutraLRoaf (1958), using the spines of still-bornbabies and normal children, showed thatlateral flexion and rotation normally occurredindependently. Kapandji (1974) stated thatcontralateral rotation occurs in conjunctionwith lateral flexion.
Considerable work has been done on the
147

THE LUMBAR SPINE
effect of movements on the disc. Rolander(1966) and Farfan, Cossette, Robertson, Wellsand Kraus (1970) discuss the effect of rotationon the disc and point out the possibility ofdamage from forceful rotatory movements.Many authors consider that one of the mainfunctions of the facet joint is to prevent rotation. However, MacConnaill (1965) suggeststhat this is only the case when the spine is notlaterally flexed as in this position some conjunct rotation is possible.
The biornechanical principles of the lumbarspine are complex. Cossette, Farfan, Robertsonand Wells (1971) and Farfan et aI. (1970)found that the instantaneous centre of axialrotation of the L3-4 disc was anterior to thefacet joint in the region of the posterior part ofthe nucleus, but this centre moved towards theside to which the rotation was forced. Farfan'sdetermination of the centre of rotation (Farfanet al., 1970; Farfan, 1973) appears to beaccurate but where there was obvious asymmetry of facet joints the centre of rotationappeared to be at the intersection of the facetplanes.
Edwards (1978) has observed the use of theso called "physiological movements" (Stoddard,1959) in relation to mobilising techniques butthese have not been done with sufficient assessment relative to range and/or pain: neitherhave they been done in the standing positionnor used in relation to the selection of techniques and positioning. Maitland (1977) refersto "quadrant" positions in relation to upperand lower cervical spine and lumbar spine butthese involve only the movements of extension,lateral flexion and rotation.
From the above, it is obvious that there isstill some controversy regarding just what doeshappen when one bends forward, backwards,rotates, or laterally flexes. This particularproblem is compounded when one considersthat anatomical variations, namely size, effectof ligaments, positioning of nerve roots andpathological changes may alter the mechanicalprinciples. What then has the clinician left onwhich to base a treatment regime? The oneaspect that we can be sure of is, of course, thesigns and symptoms. These are there for us tosee and to examine and cannot be disputed. Itis also obvious that the coupling, or combination of movements has been demonstratedquite clearly to occur to some degree even ifthe details remain a little obscure. We mustalso realise that nearly all of the passive move~
ment procedures we use are, in effect, combining or coupling certain movements. If this isthe case then we should endeavour to examinethe lum bar spine using the concept of com~
bined or coupled movements.
148
EXAMINATION OF LUMBARMOVEMENTS
In the standard examination of the lum barspine we examine flexion, extension, lateralflexion and rotation by asking the patient tobend in the appropriate direction and to stopwhen pain is reproduced. We accordingly takenote of the range, distribution of pain and howthe movement is restricted if at all. For example,consider the situation where a patient has lowback pain with pain radiating in an unbrokenline from the level of L4 down the posterioraspect of the buttock into the calf; underthese circumstances we are concerned withhow the distribution of pain reacts or changesas we perform a particular movement. We mayhave the situation where, as patient A bendsforward, pain is reproduced in the buttock andas further flexion is performed there is an increase in the calf pain. With patient B however,although pain is reproduced in the buttock atthe same range of flexion) further flexion increases only the buttock pain and not the calfpain. Each of these patients, therefore, presentsa different clinical picture, and may be treatedquite differently. However, if one is to use aprocedure in treatment which is sometimes incorrectly referred to as a unilateral procedure(e.g. rotation) then such a procedure by its verynature immediately involves the coupling ofvarious movements (i.e~ some degree of flexion,lateral flexion and rotation or extension, lateralflexion and rotation). If this is the case thenone should endeavour to examine with thesemovements in mind, namely flexion combinedwith lateral flexion and rotation or extensioncombined with lateral flexion and rotation.
COMBINED MOVEMENTSWhen examining the movement of flexion
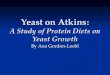
one will ask the patient to bend forward andthen ask them to bend actively to the left orright. During this procedure the therapist mustguide the movement to ensure accuracy. It isthen necessary to ask the patient to twist tothe left and then to the right while maintainingthe same degree of lateral flexion an d forwardflexion. (See Figures 1, 2 and 3).
When performing the above it is essentialthat the therapist stands on the side to whichthe patient is laterally flexed and stabilizes thepatient's pelvis by firmly holding betweenabdomen and hand. The therapist's other handis then free to guide the movement of lateralflexion and rotation. The same method is usedwhen combining the movement in extension,although the position of the therapist isdifferent in so far as both hands are placed onthe patient's shoulders when guiding the movements. This is a similar movement to the"quadrant'~ procedure as described by Maitland (1977, pp. 28-29). These procedures can
AU8t. J. Physiother. 25,4, August,1979

EDWARDS
Figure 1: Flexion combines with left lateralflexion.
Figures 2 & 3: Flexion combined with leftlateral flexion and left and right rotation.
Aust. J. Physiother. 25,4, Augus!,1979
be done in sitting, however the reproduction ofsymptoms does not appear to be as precise.
CLINICAL APPLICATION OF COMBINEDMOVEMENTS
For descriptive purposes, flexion and extension will be termed primary movements andlateral flexion and rotation, secondary movements.
This particular concept is easiest to applywhen one is dealing with referred pain fromthe lower lum bar joints into the lower lim bs.On most occasions, forward flexion is the bestprimary movement to choose, although exactlythe same principles are used if extension ischosen as the primary movement. Followingthe subjective examination, an assessment ismade to determine, amongst other things,(a) irritability, and(b) whether one will treat pain, resistance or
spasm or, in fact, a combination of these.Although the subjective assessment may changeduring the objective examination it is essentialto constantly refer to this while using thecombined movements.
Consider firstly the patient who is complaining of low back pain and pain radiatingfrom the level of L4 down the posterior aspectof the left buttock and thigh to the left calf.From the subjective examination the therapisthas decided to treat the pain rather than therestriction of movement. Under these circumstances one would ask the patient to bendforwards to the pOSItion where pain begins. Ifthis pain is reproduced in the buttock and anycontinuation of forward flexion increases thedistal distribution of the pain, then the positionof flexion where the pain is first felt is chosenas the primary position. From this primaryposition the patient is then asked to performthe secondary movement of lateral flexion tothe left and right, and left and right rotationwhile in each position of lateral flexion. Noteis taken of reduction or increase in pain. Thepatient would then be placed in the positionwhich most relieves the distal pain, and mobilisation would be done in this position. (Figure 4).
It is not unusual to find that in the neutralposition, left lateral flexion reproduces leftdistal pain whereas on bending forwards bothright and left lateral flexion are painless. It isimportant under these circumstances to useleft lateral flexion as a secondary movement.In any situation where the combined movements reproduce different signs and symptomsthan those done in the neutral position it isthe combined movements that provide theguidelines for positioning. Exactly the sameprinciples can be used when using extension asthe primary movement.
There is one set of signs and symptoms that
149

THE LUMBAR SPINE
Figure 4' PosItioning of patient for mobilIzation.
requires special mention where left lateralflexion in the neutral position reproduces rightbuttock pain and when one does this in flexionthe same amount of buttock pain is reproduced,but this is relieved when rotation is combinedwith it. Here it is important to use a combinedmovement of the lateral flexion which producesthe opposite side pain and the rotation whicheases it. This procedure does not apply whenlateral flexion reproduces pain on the samesIde; under these Circumstances it is better toplace the patient in the position of lateralflexion which reduces the pain and similarlyrotate in the painless direction. The reason forthis is not clear, however it is most likelyrelated to the stretching of structures in onecase and compression in the other' the latteris more often helped by reducing the pressure,the fonner by, in fact, stretching the structures.
Using the same principles, if stiffness is themain problem the moverrlents are coupled toshow which is the most restricted. Wherebilateral paiD is present, using combined movements will elicIt qUIte Inarked unilateral signsin the majority of cases. Lateral flexion to theleft, in the neutral positIon, may produce theleft sided pain the patient is complaining of,but when the patient is bent forward to wherethe pain begins, left lateral flexion in thisposition may be full range and painless whereasfIght lateral fle~xion may be painfully restricted.Under these circumstances, one has a choice ofrna bilising eIther the least paInfully restrictedmovement or the most painfully restrictedmovement and the choice will depend on theassessment of the total clinical picture. In manycases extension can be used in the same way; ifthe important signs cannot be obtained withflexion then the mobilisation can be done inextension.
Lengthy de bates as to which side to lie thepatient on, either painful sIde up or down, cannow be seen to be irrelevant. One will choosea position which either reduces or produces therelevant signs and symptoms: if we choose touse a technique of rotation, and this by itsnature involves coupling procedures, then we
150
should endeavour to position the patient keeping this in mind. Stoddard (1959) described socalled "locking procedures" for localisedmanipulation and Maigne (1 965) has mentioned theconcept of Dlanipulating in the painless direction. The important aspect, I suggest, is wherethe pain is reproduced when doing combinedmovements and at what range the pain is reproduced. Under some circumstances one maychoose to use the position which is restricted orin fact, reproduces more pain (usually, however, this would be more local than referredpain) and in this case one is endeavouring tostretch or move the joint in its most restricteddirection to obtain the maximum mobilisingeffect.
Extension can be used in a similar mannerwith the same governing guidelines, namelycoupling the movements and relating them tothe distribution of pain and range of move~
ment. I do not think it is entirely correct toconsider mobilising in flexion for the lowerlum bar spine and extension for the upperlum bar joints. If one tests the passive physiological intervertebral movement of rotation inthe lum bar spine, one can feel a rotatory movement occurring at the lower lumbar jointseven when they are placed in hyper-extension.It is logical, therefore, to use this positioncoupled with the appropriate lateral flexionwhen treating the lumbar spine, providing therelevant signs and symptoms are produced inthis position. Similarly, I do not think it isentirely correct to refer to the moving of say,L4, to the right as being the same as moving LSto the left. Clinically there is certainly adifference and those who refer to the above asbeing the same might be criticised as being too"mechanical" in their approach to technique.Although the precise reason for this differenceis not yet clear, part of the answer may lie inthe fact that the vertebral column may actsomething like a cork screw and move up ordown depending on which end is fixed andwhich end is rotated. This in turn may have adifferent effect on the nerve root and duramater.
When one is positioning a patient, a numberof points need to be closely watched.1. It is important that the position adopted
resem bles, as closely as possible, the positionused when examining.
2. Particular care must be taken when rotatingthe patient to the position that lateralflexion in the reverse direction is not inadvertantly performed (see Figures 5 and 6).
3. Although mechanically it is probably true tosay that moving the trunk to the left is thesame as moving the pelvis to the right interms of its effect on, say, the L5 level, asmentioned previously, it is not always true
Aust. J. Physiother 25,4, August, 1979

EDWARDS
Figures 5 & 6: Lateral flexion decreases whenpatient is positioned in full rotation.
clinically. In practice it often happens thatmore lateral flexion is performed whenusing the pelvis than when using the trunk.This may be related to the greater ease ofapplying force when the pelvis is used asthe lever. Whatever the case this particularaspect needs to be considered.The reasons for the change in signs and
symptoms when movements are coupled is notclear. There are a number of simple observations one can make. Firstly, the position of thenerve root when lateral flexion is performed inthe neutral position is slightly altered when thesame movement is done in some degree offlexion or extension. Obviously the positionof the facet joint is very different when lateralflexion is done in forward flexion, neutral, orthe extended position. One can observe clearlyon the anatomical model or the unpreservedspecimen that the shape of the foramen altersin flexion and extension combined with lateralflexion. As we have seen, axis and instantaneouscentres of rotation would alter in these differentpositions. If one then considers the soft tissue(e.g. dura mater, ligamentum flava, capsule offacet joint and disc) further altered effects canbe observed when movements are coupled.Finally, pathological changes of disc, facet orsoft tissue origin may affect the movementsand symptoms when there is a coupling pro-
Aust. J. Physiother. 25,4, August, 1979
cedure carried out.
CONCLUSIONBy its very nature our work tends to be
empirical. The above is a method of examination and treatment which should help us toelicit and observe signs and symptoms whichpreviously have been masked. Becoming moreaware of the effects of coupling movementswill, I think, take us a little further towardsour ultimate goal, i.e., making manipulativetherapy a more precise science.
REFERENCESALLBROOK, D.A. (1957): HMovernents of the Lumbar
Spinal Column". Journal of Bone and Joint Surgery, 39B; 2: 339-345.
ARKIN, A.M. (1950): "The Mechanism of Rotationin Combination with Lateral Deviation in theNormal Spine". Journal of Bone and Joint Surgery,32A: 180-188.
BEGG, A.G. and FALCONER, M. (1949): ~'Plain
Radiographs in Intraspinal Protrusion of LumbarI-V Discs: A Correlation with Operative Findings".British Journal ofSurgery, 36: 225-239.
CLAYSON, S.l., NEWMAN, I.M.'1 DEBEVEC, D.P.,ANGER, R.W., SKOWLUND, H.V. and KOTTKE,F.J. (1962): "Evaluation of Mobility of Hips andLumbar Vertebrae of Normal Young WomenH
•
Archives of Physical Medicine and Rehabilitation,43: 1-8.
COSSETTE, l.W., FARFAN, H.F., ROBERTSON,G.H. and WELLS, R.V. (1971): '4The Instantaneous Centre of Rotation of the Third LumbarIntervertebral Joint". Journal of Biomechanics, 4:149...153.
DAVIS, P.R., TROUP, J.D. and BURNARD, D.(1965): ~'Movements of the Thoracic and LumbarSpine when Lifting: A Chrono-cyclophotographicStudy". Journal ofAnatomy, 99; 1: 13-26.
EDWARDS, B.C. (1978): "Study Leave 1975".Western Australian Institute of Technology Publication.
FARFAN, H.P., COSSETTE, l.W., ROBERTSON,C.H., WELLS, R.V. and KRAUS, H. (1970):"The Effects of Torsion on the Lumbar Intervertebral Joints: The Role of Torsion in theProduction of Disc Degeneration". Journal ofBone and Joint Surgery, 52A; 3: 468-497.
F ARPAN, H.F. (1973): "Mechanical Disorders of theLow Back". Lea and Ferbiger, Philadelphia.
FARFAN, H.P. (1975): "Muscular Mechanism of theLumbar Spine and the Position of Power andEfficiency': Orthopaedic Clinics ofNorth America,6; 1: 135-144.
GREGERSON, G.C. and LUCAS, D.B. (1967): "AnIn-Vivo Study of the Axial Rotation of the HumanThoraco-Lumbar Spine". Journal of Bone andJoint Surgery, 49A; 2: 247-262.
HASNER, E., SHALIMIZEK, M. and SNORRASON,E. (1952): "Roentgenological Examination ofthe Function of the Lumbar Spine~'. Acta Radiologica, 37: 141-149.
151

THE LUMBAR SPINE
KAPANDJI, LA. (1974): '~Trunk and VertebralColumn". The Physiology of the JOll'itS (Vol. 3)(2nd ed.). Churchill-Livingstone, London.
LOEBL, W. Y. (1967): "Measurement of SpinalPosture and Range of Spinal Movement". Annalsof Physical Medicine, 9; 3: 103-110.
LOEBL, W. Y. (1973): ~4Regional Rotation of theSpine". Rheumatology and Rehabilitation, 12: 223.
LOVETT, R.W. (1902-3): '4A Contribution to theStudy of the Mechanics of the Spine". AmericanJournal ofAnatomy, 2: 457-462.
LUMSDEN, R.M. and MORRIS, J.M. (1968): "AnIn-Vivo Study of Axial Rotation and Immobilization at the Lumbosacral Joint". Journal of Boneand Joint Surgery, 50A' 1591-1602.
MacCONAILL, M.A. (1965): "Mechanical Anatomyof Motion and Posture". In S. Licht (ed.), Therapeutic Exerclse (2nd ed.). Waverley Press Inc.,Baltimore, Maryland.
MAIGNE, R. (1965). "Concept of PaInlessness andOpposite Motions in Spinal Manipulation".Alnerican Journal of Physical Medicine, 44:55-69.
MAITLAND, G.D. (1977): Vertebral Manipulation.4th ed. Butterworths, London.
MOLL, J.M.H., LIYANAGE, S.P. and WRIGHT, V.(1972): "An Objective Clinical Method to MeasureLateral Spinal Flexion". Rheun1atology and
152
Physical Medicine, 11: 293-312.ROAF, R. (1958): "Rotation Movements of the
Spine with Special Reference to Scoliosis".Journal ofBone and Joint Surgery, 40B: 312-332.
ROLANDER, S.D. (1966): '4Motion of the LumbarSpine with Special Reference to the StabilizingEffect of Posterior Fusion". Acta OrthopaedicaScandinavica, Supp. No.90.
SCHULTZ, A.B., BELYTSCHKO, T.B., ANDRIACCHI,J.P. and GALANTE, J.L. (1973): "Analog. Studiesof Forces in the Human Spine: Mechanical Propertiesand Motion Segment Behaviour". Journal of Biomechanics, 6; 4: 373-383.
STODDARD, A. (1959): Manual of OsteopathicTechnique. Hutchinson, London.
TANZ, 5.S. (1953): "Motion of the Lumbar Spine.A Roentgenologic Study". American Journal ofRoentgenologYJ Radium Therapy and NuclearMedicine, 69; 3: 399-412.
TROUP, J.D.G., HOOD, C.A. and CHAPMAN, A.E.(1968): HMeasurements of the Sagittal Mobility ofthe Lumbar Spine and Hips". Annals of PhysicalMedicine, 9; 8: 308-21.
WILES, P. (1935): "Movements of the LumbarVertebrae During Flexion and Extension". Proceedings of the Royal Society of Medicine, 28:647-651.
Aust. J. Physiother. 25,4, August, 1979