Embed Size (px)
Citation preview

5/18/2015
1
Learning Objectives
• The Participant will understand the requirements for a successful program of injury prevention in a healthcare organization.
• The participant will be able to reference industry standards and legal requirements for healthcare organizations regarding general injury prevention, Safe Patient Handling and Healthcare Ergonomics.
• The participant will formulate a perspective of the broad spectrum between research and practical application and how the two are integrated.
Swedish Medical Center
First Hill Cherry Hill Ballard
Issaquah ACC’s: Mill Creek & Redmond Edmonds

5/18/2015
2
Alaska•Prov. Alaska Med. Center Anchorage
Montana•Prov. St. Patrick’s Medical Center Missoula•Prov. St. Joseph’s Medical Center PolsonProv. Alaska Med. Center Anchorage
•Prov. Kodiak Medical Center•Pro. Valdez Medical Center•Providence Seward Medical Center Oregon
•Prov. Portland Medical Center Portland•Prov. St. Vincent’s Portland•Prov. Seaside Hospital•Prov. Willamette Med. Center•Prov. Milwaukie Hospital•Prov. Medford Med. Center•Prov. Willamette Falls Med. Center•Prov. Hood River Memorial Hospital
•Washington•Prov. Regional Med. Center Everett•Prov. St. Peters Olympia•Prov. St. Mary’s Walla Walla•Prov. Sacred Heart Spokane•Prov. Holy Family Spokane•Prov. Centralia•Prov. Mt. Carmel•Prov. St. Joseph’s ChewelaSwedish Medical Center – 5 hospitalsKadlec Medical Center – RichlandPac‐Med
California•Prov. Tarzana Medical Center•Prov. Holy Cross Medical Center•Prov. Little Company of Mary Torrance•Prov. Little Company of Mary San Pedro•Prov. St. Joseph’s Med. Center Burbank•Prov. St. John’sFacey Medical Group
34 hospitals76,000 employees
Team Structure
HR : Operations ‐ Benefits
Employee Health & Injury Prevention
Alaska
Injury Management (Work Comp) Wellness Compliance Health & Welfare
Plans
Western WA
EWA/MT
Oregon
Calif.
Building a Team
• Limited Team Size – 9.5 FTE’s = 1:8000
• Team Background:– 2 Physical Therapists
– 1 Occupational Therapist1 Occupational Therapist
– 2 RN’s
– 2 Exercise Physiologists
– 1 PhD (Engineering / Research / Ergo)
– 1 MBA
– 1 ED Tech.

5/18/2015
3
Key Componentsfor Success
• Top Management Support and Involvement
• Worker Motivation / Participation
• Risk Identification and Assessment
• Risk Control
• Education and Training
• Program Evaluation / Process Improvement
Year One
• Transformation into “One System”
• Policy formation for
– Safe Patient Handling
– Ergonomics
– Blood and body fluid exposure
– TB Surveillance
– Respiratory Protection
Workers’ Compensation Board of B.C. Handle with Care

5/18/2015
4
Legal Duties
• Joint Commission for Accreditation on Healthcare Facilities
• Safe Patient Handling Legislation in 2 of the 5 regionsregions.
• Facilities Guideline Institute (FGI)
• Americans with Disabilities Act (ADA)
• OSHA General Duty Clause
Joint Commission Report ‐ 2012
•High Reliability Organization•“Culture of Safety”
•Calls out the relationship between worker and patient f tsafety.
•Values the input of Human Factors and Ergonomics in reducing error.
•Use of Safety Coaches, Champions and Unit Peer Leaders.
•Integration of Safety in Design.
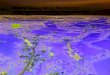
Prevalence* of Self‐Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2013

5/18/2015
5
State Policy Committee Hazard Assess Procedure Training RTR Yr. Assess Design Monetary
Texas (2005) X X X X X X X
Ohio (2005) X
Hawaii (2006)
Washington (2006) X X X X X X X X X
Rhode Island(2006) X X X X X X
State Law Comparison Chart-10 Laws / 2 other (12 total)
13
New Jersey (2007) X X X X X X X
Maryland (2008) X X X X X X
Minnesota (2011) X X X X X X
Illinois (2011) X X X X X X X
Missouri (2011) X X X X X X X
California (2011) X X X X X
New York (2014) X X X X X X X X
http://www.nursingworld.org/MainMenuCategories/Policy‐Advocacy/State/Legislative‐Agenda‐Reports/State‐SafePatientHandling
FGI Guidelines 2010 / 2014
• 2010 included Safe Patient Handling
– Patient Handling and Movement Assessment (PHAMA) Inadequate(PHAMA)
– Bariatric Considerations
Inadequate Equipment
Lack of Empathy
Avoid Patient
Fear of Injury
2010 ‐ PHAMA
1. An interdisciplinary approach to identify patient handling and movement equipment for each service area.
2. Definition of space requirements and structural and other architectural design considerations to accommodate incorporation of patient handling and movement equipment. (2010: 1.2‐5/A1.2‐5)

5/18/2015
6
2014 FGI guidelines
Major Revisions:
• The PHAMA is incorporated into the guidelines to address the patient handling and movement needs. (1.2‐3.3.1.1)patient handling and movement needs. (1.2 3.3.1.1)
• Safety Risk Assessment: Multidisciplinary (1.2‐3.3.2)
• Bariatric ‐ Specific Design Considerations(1.2‐5.4)
• Accommodations to encourage patient mobility (A2.1‐2.1)
• Design Criteria for Acoustic Surfaces (A1.2‐5.1.3)
Safety Risk Assessment (1.2‐3.3.2)‐2014
• All health care facility projects shall be designed and constructed to facilitate the safe delivery of care.
• To support this goal, an interdisciplinary team shall develop a safety risk assessment.
• Identify hazards and potential risks.
• Evaluate hazards and risks.
• SRA Report– Patient and caregiver safety hazards and risks identified by the safety
risk assessment. Design features that contribute to the identified hazards and risks
– Design strategies to reduce, mitigate, or eliminate identified hazards and risks

5/18/2015
7
Americans with Disabilities Act
Requires everyone to have equalaccess to medical care:
• Medical Clinics• Dental Offices• Dental Offices• Access to exam tables and other equipment
Free On‐lineADA Standards for Accessible Design –ADA – Access to Medical Care for Individuals with Mobility Disabilities –
WA. Ergo Rule / OSHA General Duty Clause
• Washington State Ergonomics Rule
– Implemented May 26, 2000
– Repealed November 2003
• Each Employer shall furnish to each of his employees employment and a place of employment which is free from recognized hazards that are causing or likely to cause death or serious physical harm to his employees.
Risk Identification

5/18/2015
8
Linen
Ergonomics
Housekeeping
Purchasing SeniorLeadership
Physicians/Surgeons
All staff/ unitswho handle patients
Mangers Workman’sCompensation/Return to Work
SPHCommittees
Leadership /
Linen
Ergonomics
Workman’sCompensation/
Leadership /Managers
Physicians/Surgeons
BiomedLearningCenter
EMR / IS
ProjectManagers
Facilities /Carpentry
InjuryInvestigation
InjuryInvestigation
Purchasing
Housekeeping
All staff/ unitswho handle patients
p /Managers
p /Return to Work
Linen / Co‐op Laundry
EMR / IS
Safety /Fire
Remodel/Construction
gProjectManagers
NEO
Clinical Education
Fall / SkinPrevention
Linen
Ergonomics
Workman’sCompensation/
SeniorLeadership
Physicians/Surgeons
BiomedLearningCenter
EMR / IS
ProjectManagers
Facilities /Carpentry
Nursing/TherapySchools
InjuryInvestigation
InjuryInvestigation
Purchasing
Housekeeping
EMT’s
DepartmentOf
Health
StateLabor Code
VendorsNursing /Therapy/
SurgeonRecruits
Other Hospitals
OSHA, L & I,ADA, FGI
Magnet Status
All staff/ unitswho handle patients
Mangersp /
Return to Work
Linen / Co‐op Laundry
EMR / IS
Safety /Fire
Remodel/Construction
gProjectManagers
NEO
Clinical Education
Fall / SkinPrevention

5/18/2015
9
Linen
Ergonomics
Workman’sCompensation/
SeniorLeadership
Physicians/Surgeons
BiomedLearningCenter
EMR / IS
ProjectManagers
Facilities /Carpentry
Nursing/TherapySchools
InjuryInvestigation
InjuryInvestigation
Purchasing
Housekeeping
EMT’s
DepartmentOf
Health
StateLabor Codes
VendorsNursing /Therapy/
SurgeonRecruits
Other Hospitals
OSHA, L & I, ADA, FGI
Magnet Status
All staff/ unitswho handle patients
Mangersp /
Return to Work
Linen / Co‐op Laundry
EMR / IS
Safety /Fire
Remodel/Construction
gProjectManagers
NEO
ClinicalEducation
Fall / SkinPrevention
HAPUReduction
Fall reduction
Poor patienthandling experience Poor
staff satisfaction
Injuriesreduction
Risk Assessments
• Center for Health Design:https://www.healthdesign.org/chd/learning_tools_and_resources/safety_risk_assess
ment_toolkit
Infection Control
Patient Handling
Falls
Medication Safety
Behavioral Health
Security
Education and Training
• Three hours of New Employee Education for Safe Patient Handling.
• Two hours of yearly training for annual refresher.
• Unit Safety Champions: combination of Safety Coaches, Safe Patient Handling Champions and
Wellness Advocates.

5/18/2015
10
Program Evaluation
• Employee involvement!
– Safety and Safe Patient Handling Committees.
R t l i f i j• Root cause analysis of injury.
• Good data trending.
– Challenges with data.
Ram Maikala, PhD
My Transition
Hopkinton, MA(12.9 years)
Everett, WA(since Sept 29’2014)

5/18/2015
11
Liberty Mutual’s Contribution
• Knowledge Transfer and Exchange (from Research to Reality) has been a Liberty Mutual differentiator since 1954.
• Nothing proprietary; all research published in the lit topen literature.
• Many examples over the years in Vehicle Safety, Machine safety (safe distance openings), Ergonomics, and Slips, Trips and Falls.
• As safety practitioners we rely on evidence based research to help sell our interventions!
Thanks to Wayne Maynard, Liberty Mutual
Knowledge Transfer & Exchange
Liberty Mutual Research Institute for
Liberty Mutual Research Institute for SafetySafety
Risk Control ServicesClaims & Case Management
Risk Control ServicesClaims & Case Management
Thanks to Wayne Maynard, Liberty Mutual
Examples of Research
Thanks to Wayne Maynard, Liberty Mutual

5/18/2015
12
Manual Materials Handling• Snook & Ciriello 1991, Ciriello,
Ciriello et al., 1999, 2001, 2005, 2007, 2008, 2009
Research??
….Research got to know its limitations!
Researchers say…… Practitioners say……
Research Vs. Reality (Practice)
I need more time I need the answer yesterday
I need more money I need the answer yesterday
Modified from text of Dr Patrick Dempsey, CDC-NIOSH, Pittsburgh, PA
You don’t understand the implications of my findings!
“Give me something I can use” (Wayne Maynard, LM)
More research is needed! Do your findings have any implications??
I published a Journal article on that!
Yeah, whatever!! “Give me something I can use”

5/18/2015
13
My Transition
Everett, WA(since Sept 29’2014)
Epidemiologic Trend in Health
86% 65%37%
(hypertension, heart disease, diabetes, cancer)
5/18/2015 38Global Health and Aging, WHO (2011)
• A shift in the leading causes of death and illness from infectious and parasitic diseases to noncommunicable diseases and chronic conditions!
• Aged above 60 years ‐ noncommunicable dieases account for more than 87% of the burden in low, middle and high‐income countries!
• Obesity is associated with increased risk of hypertension, heart disease, diabetes!
National Trend of Caregivers
• AGING - One-third of Nursing workforce is older than 50 (National Center for Health Workforce Analysis 2013)!
• OBESITY - Almost 54% Nurses are overweight or obese (Miller et al. 2008).
The biggest problem: Aging and Obese Workforce Vs Caring for Aging and Obese Patients

5/18/2015
14
Patient Handling
• Total Transfers
• Repositioning
• Limb Holding
• Lateral
• Falls on same level
• Fall from elevation
• Manipulating Needle in Patient
• Disposal‐Related Causes
• Handling /Passing • Cleanup
Exposures Falls
• Lateral Transfer
• Fall –Prevention
• Push‐Pull
• Assaults?
• Trip but no fall
• Slip but no fall
p• Improper Disposal • IV Line‐Related Causes • Collision with
Caregiver or Sharps • Recapping• Handling/ Transferring
Specimens
Injury* Definition
• Any unintentional (e.g., accidents) OR intentional(e.g., violence or assaults) damage to the body resulting from acute exposure to thermal, mechanical, electrical or chemical energy OR , gyfrom the absence of such essentials as heat or oxygen!
*CDC, National Center for Injury Prevention and Control, Department of Health and Human Services
Haddon Matrix*
Host Vector Environment
Pre-eventPre event
Event
Post-event
*Dr William Haddon, First Director of NHTSA

5/18/2015
15
Haddon Matrix*Factors contributing to injury process
Phases at which
HOST AGENT/VEHICLE ENVIRONMENT
• Person at risk for an injury
• Energy that is transmitted to the host through a vehicle (inanimate object) OR vector (person or animal)
• Characteristics of the setting in which the injury event takes place (e.g., roadway, playground)
• Social and legalCHANGE would have its effect
Pre‐Event
Event
Post‐Event
animal)• That is causing energy
transfer
• Social and legal norms and practices (e.g., policies)
Haddon MatrixFactors contributing to injury process
Phases at which CHANGE would have its effect
HOST AGENT/VEHICLE ENVIRONMENTPhysical and/or Social
Pre‐Event( i f
PRIMARYIntervention
• Conditions necessary for the transfer of energy• What leads to an injury?(time frame –
Seconds to Years)
Event(time frame –Fraction of Second to Minutes)
Post‐Event(time frame –Seconds to Years)
Intervention
SECONDARY Intervention
TERTIARY Intervention (to lessen long‐term adverse effects)
• What leads to an injury?• Time before the event occurs OR the period before release of
injury‐causing energy• (What are) Events that influence likelihood of an injury
• Given the Event occurrence, what leads to an injury• Release of uncontrolled energy• Events affect transmission of energy
• Period after injury
Exploring Strategies for Injury Prevention*
Hierarchy of Controls
(from Most Effective to Least Effective)
*The Hierarchy of Hazard Controls (http://creativesafetypublishing.com/the‐hierarchy‐of‐hazard‐controls/ )

5/18/2015
16
SUMMARY
• Injuries are predictable and preventable.
• Specific injuries have similar characteristics of: person, place, and time.
d di i j ( h i )• By understanding an injury (mechanism), interventions can be developed and implemented to prevent or limit the extent of a given injury!
Thank You!
Leslie pickett@providence [email protected]

5/18/2015
17
NPR Report on ADA Clinic Access
http://www.npr.org/templates/story/story.php?storyId=14362338