Embed Size (px)
Citation preview
COMMON ARRHYTHMIAS Diagnosis and Therapy
Zachary D. Goldberger, MD, FACC, FHRS Assistant Professor of Medicine
Division of Cardiology UW School of Medicine
Harborview Medical Center

FINANCIAL OR OTHER RELATIONSHIP DISCLOSURE:
None

KEY POINT
Regular or irregular
Irregular
Regular

Sinus tachycardia: sinus rhythm with a HR >100 bpm
Short differential diagnosis: • Physiologic (e.g., exercise, excitement, pregnancy) • Pain /anxiety • Drugs (e.g., alpha/beta-agonists, stimulants, withdrawal) • Hypovolemia (e.g., bleeding, vomiting, diarrhea) • Heart failure (CO=HR x SV) • Pulmonary embolism • Acute MI • Endocrine (e.g., hyperthyroidism, pheochromocytoma)
Sinus Tachycardia


Are there P waves?

Atrial Fibrillation with Rapid Ventricular Response
• Most common pathologic arrhythmia • Hallmarks: irregularly irregular, no P waves • AVERAGE rate >100 bpm (count QRS’s, multiply by 6) • Narrow complex (when ventricles activated normally) • May be acute, paroxysmal, or chronic • Always try to account for etiology

Atrial fibrillation with a rapid ventricular response: irregularly irregular, no P waves, >100 bpm
Some associated causes/conditions: • Aging • Hyperthyroidism • Hypertension • Post-operative (esp post cardiac surgery) • Valvular disease (esp mitral stenosis) • Sepsis/infection (esp endocarditis) • Coronary artery disease (including ischemia/ACS) • Pulmonary disease (COPD, PE)

Multiple Wavelets Synchronized Activation
Mechanism of Atrial Fibrillation

KEY POINT When you see an irregularly
irregular rhythm, suspect atrial fibrillation (and confirm by absence
of P waves)

Atrial Flutter
• Common pathologic arrhythmia • Hallmarks: “saw tooth” flutter waves, may be regular or irregular • Rate depends on degree of conducted flutter waves (usually 75-150) • Narrow complex • May be acute, paroxysmal, chronic

• Atrial flutter can be regular or irregular
• Conduction may be variable (e.g., 3:1, 4:1)
• Caution! Irregularity may mimic atrial fibrillation, but irregularity not random
• 300/min, so rates approximate 150 (2:1), 100 (3:1), 75 (4:1), etc
Atrial Flutter

• Atrial flutter with 2:1 conduction (150 bpm). The saw-tooth appearance is not always easily apparent with 2:1 conduction.

KEY POINT When you see a narrow complex tachycardia at ~150 bpm, suspect atrial flutter with 2:1 conduction

A 27 year-old woman comes to the ED with palpitations which began 2 hours ago. She says she was watching television when she suddenly began to feel as though her “shirt was fluttering” and had a sensation of someone “pounding” on her neck. She has had similar episodes occurring twice yearly for approximately 5 years, but now they are increasing--she has had 5 episodes during the past 6 months. Her previous episodes have always started and resolved suddenly, never lasting longer than 10 minutes; she has noticed that they occasionally resolve with coughing. Her medical history otherwise is unremarkable, and she takes no medications. Her family history is significant for the death of her father from a myocardial infarction at age 55 years. The patient's vital signs reveal a HR of 180/min and her BP is 124/75 mmHg. She appears mildly anxious, but alert and oriented. Physical examination reveals prominent jugular venous pulsations and tachycardia. She has no carotid bruits, and the remainder of her exam is normal. An ECG is performed:
CASE 1


Which of the following is the most appropriate next step in management?
A. Administration of intravenous adenosine B. Carotid sinus massage C. Direct current cardioversion D. Observation only E. Oral metoprolol therapy

A. Flecainide therapy B. Metoprolol therapy C. Reassurance only D. Refer for radiofrequency ablation E. Refer for an implantable cardioverter-defibrillator
Carotid sinus massage is performed. Her pulse remains 180/min and blood pressure is now 100/60 mmHg. The patient remains alert and oriented but appears increasingly anxious. Intravenous adenosine is administered, after which normal sinus rhythm is restored with a pulse of 85/min.
CASE 1, cont’d

AV Nodal Reentrant Tachycardia
Paroxysmal SVT (PSVT)
• Clinical syndrome
• Subset of all SVTs, but often simply called “SVT”
• Narrow complex
• Regular, rapid, abrupt onset and termination
• P waves, if seen, are not of sinus origin
• Defined as: AV nodal reentrant tachycardia (AVNRT) AV reentrant tachycardia (AVRT) (Ectopic) atrial tachycardia (AT)

Paroxysmal SVT (PSVT)
KEY POINT: Mechanism is either: Automatic (ectopic atrial tachycardia) Reentrant
(AVNRT, AVRT)
Note: atrial flutter is also a reentrant rhythm, and may be paroxysmal, but not typically classified as “PSVT”
AV nodal reentry
AV reentry
(Ectopic) atrial tachycardia

Which is not a common symptom of a supraventricular tachycardia?
A.Chest pain (if underlying heart disease)
B.Dyspnea
C.Light-headedness
D.Palpitations
E.Syncope

AV Nodal Reentrant Tachycardia (AVNRT)
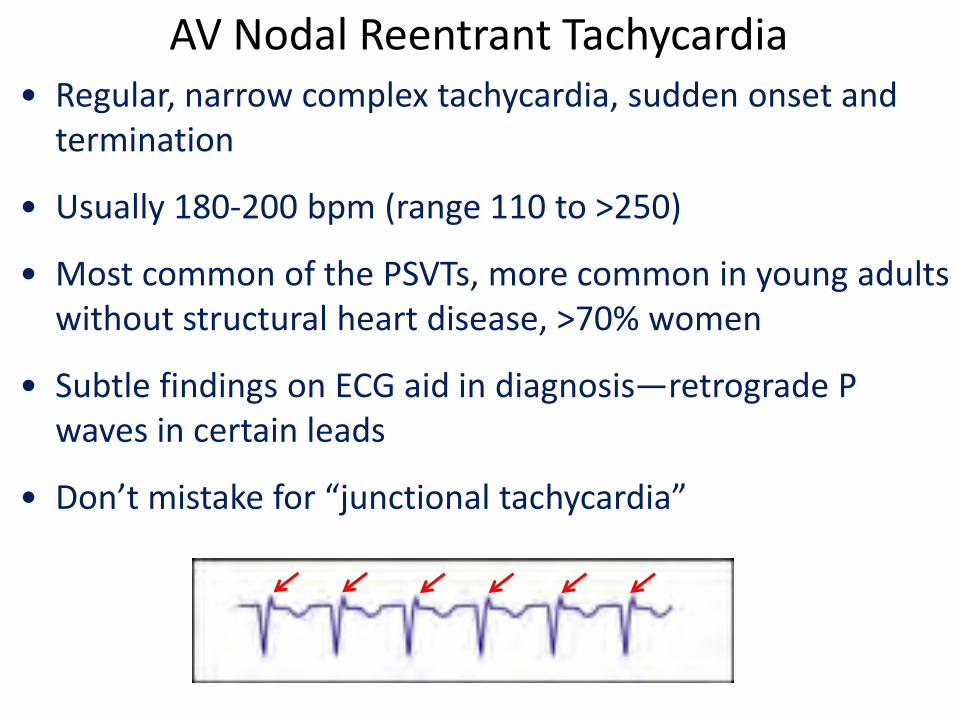
AV Nodal Reentrant Tachycardia • Regular, narrow complex tachycardia, sudden onset and
termination
• Usually 180-200 bpm (range 110 to >250)
• Most common of the PSVTs, more common in young adults without structural heart disease, >70% women
• Subtle findings on ECG aid in diagnosis—retrograde P waves in certain leads
• Don’t mistake for “junctional tachycardia”

Acute Termination: AVNRT
• Vagal maneuvers—always try first (carotid sinus massage, Valsalva maneuver)
• If ineffective, or possibility of carotid plaque (i.e., elderly, bruit present), administer adenosine (6 mg IV, may increase to 12 mg, 2-3 times)
Long-Term Therapy: AVNRT
3 strategies to treat/prevent AVNRT: Reassurance Pharmacologic therapy Invasive therapy

Long-Term Therapy: AVNRT
• Pharmacologic therapy: flecainide/propafenone during symptomatic episodes (pill-in-the-pocket)
• Antiarrhythmics carry proarrhythmic risk, careful selection of appropriate patients
• AV nodal blockers
• Radiofrequency ablation: ~99% curative procedure, low complication rate
• (Low) risk of AV node injury/ablation, and risk of invasive EP study itself

A 35 y/o man was playing basketball when he experienced the acute onset of palpitations. They lasted approximately 3 minutes, and subsided when he kneeled down. His teammates encouraged him to present to his internist the next day. He has experienced palpitations for nearly 20 years. He was referred to a cardiologist during college who did not feel further cardiac testing was needed. He takes no medications, and his examination is unremarkable. His ECG is shown below:
CASE 2


A. “Surgery will offer the most effective therapy for this condition.”
B. “Your palpitations are likely due to anxiety.”
C. “This problem may worsen as you get older.”
D. “Antiarrhythmics are less effective than a catheter ablation.”
E. “You have a high risk of sudden death.”
What do you tell the patient?
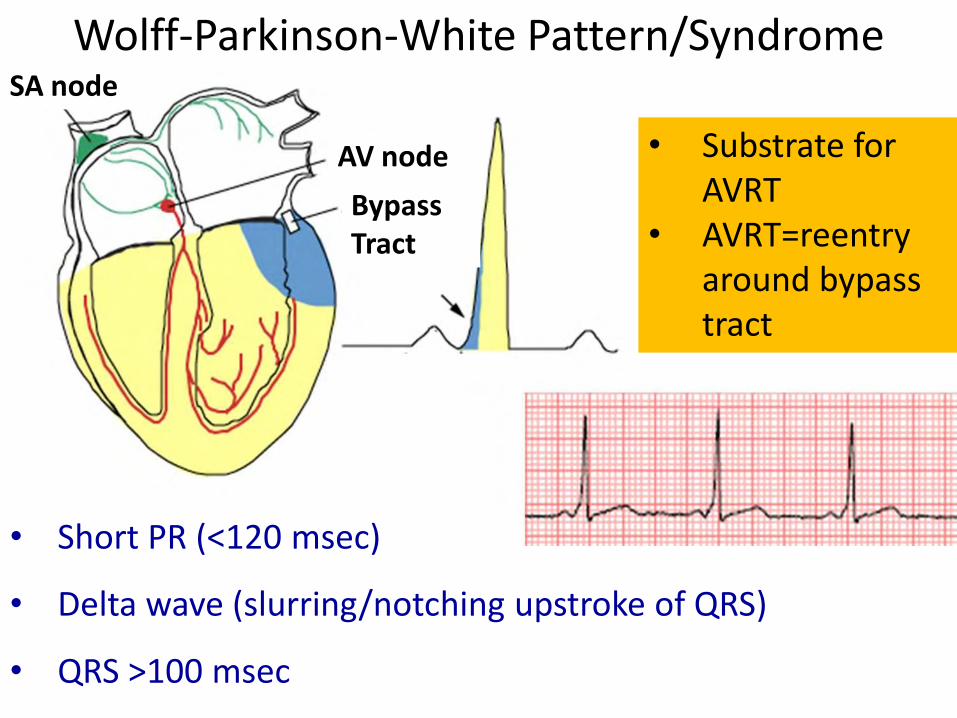
Wolff-Parkinson-White Pattern/Syndrome
• Short PR (<120 msec)
• Delta wave (slurring/notching upstroke of QRS)
• QRS >100 msec
Bypass Tract
AV node
SA node
• Substrate for AVRT
• AVRT=reentry around bypass tract
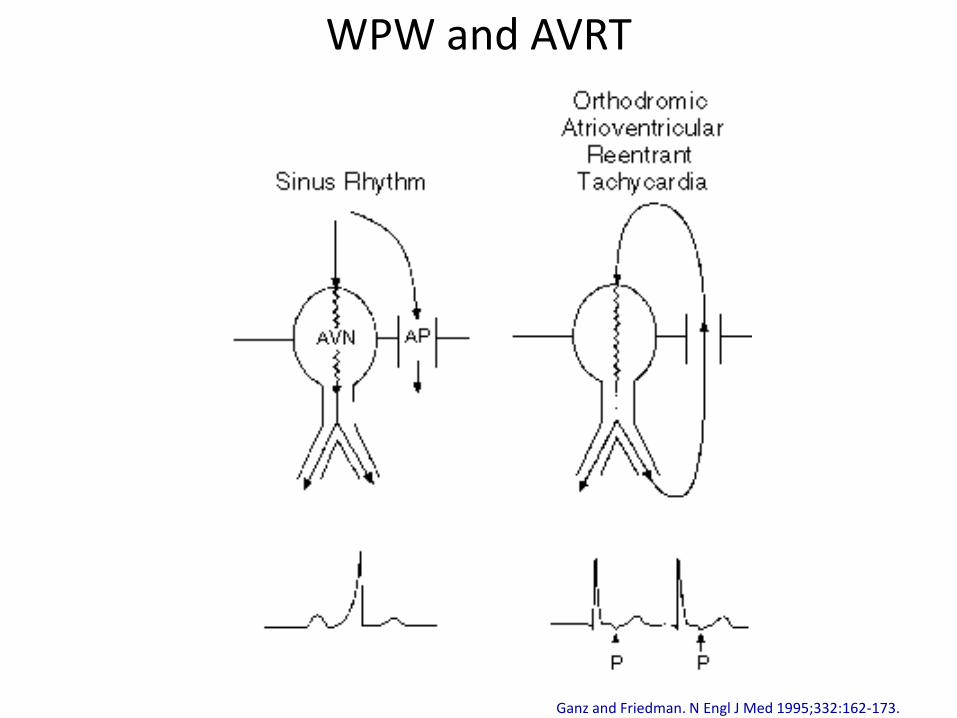
Ganz and Friedman. N Engl J Med 1995;332:162-173.
WPW and AVRT

Asymptomatic Preexcitation (WPW Pattern)
Short PR (<120 ms)
Delta wave (slurring/notching upstroke of QRS)
QRS >100 ms

Long-Term Therapy: AVRT
• Radiofrequency ablation: ~90-95% curative, low complication rate
• Treating asymptomatic WPW pattern is controversial
• Not every bypass tract capable of rapid conduction and risk of pre-excited a-fib is generally low, and risk-stratification requires careful evaluation
• Patients with high-risk occupations (e.g., bus driver, pilot) often receive mandatory ablation

AVRT (before) and WPW (after)

KEY POINT Suspect AVRT when the ECG in
sinus rhythm shows a WPW pattern (i.e., pre-excitation)

Ferguson J, DiMarco J. Circulation 2003;107:1096-1099
PSVT: Summary Slide

KEY POINT Adenosine is a safe, effective therapy for narrow-complex
tachycardias suspected to be PSVT (i.e., diagnostic, potentially
therapeutic)

A 65 y/o man presents with chest pain. The first ECG is taken on admission. He undergoes a procedure. The second ECG is performed 3 hours later.

What is the most appropriate step in management (after seeing the 2nd ECG)?
A. Activate the cardiac catheterization laboratory
B. Administer IV amiodarone C. Administer IV lidocaine D. Direct current cardioversion E. Observation only

Acute inferolateral MI (ST elevations in II, III, aVF, V5, V6)

• Acute MI is resolving, likely treated with PCI or thrombolytics
• Beats 6-11: accelerated idioventricular rhythm (AIVR)
• AIVR common with acute MI, associated with reperfusion after thrombolytic agents or PCI, occurring spontaneously
• This arrhythmia is generally short-lived (minutes or less), and usually requires no specific therapy. Not a new BBB. No need for BBs, amiodarone, lidocaine, cath lab reactivation, troponins, etc

An 85 y/o man with severe emphysema is admitted to the medical intensive care unit due to acute shortness of breath and tachycardia. His pulse is irregular; you perform an ECG:
What is the most appropriate step in management?
A. DC cardioversion B. IV amiodarone C. IV beta-blockers and initiate
anticoagulation once stable D. Oral theophylline E. Oxygen and nebulizers
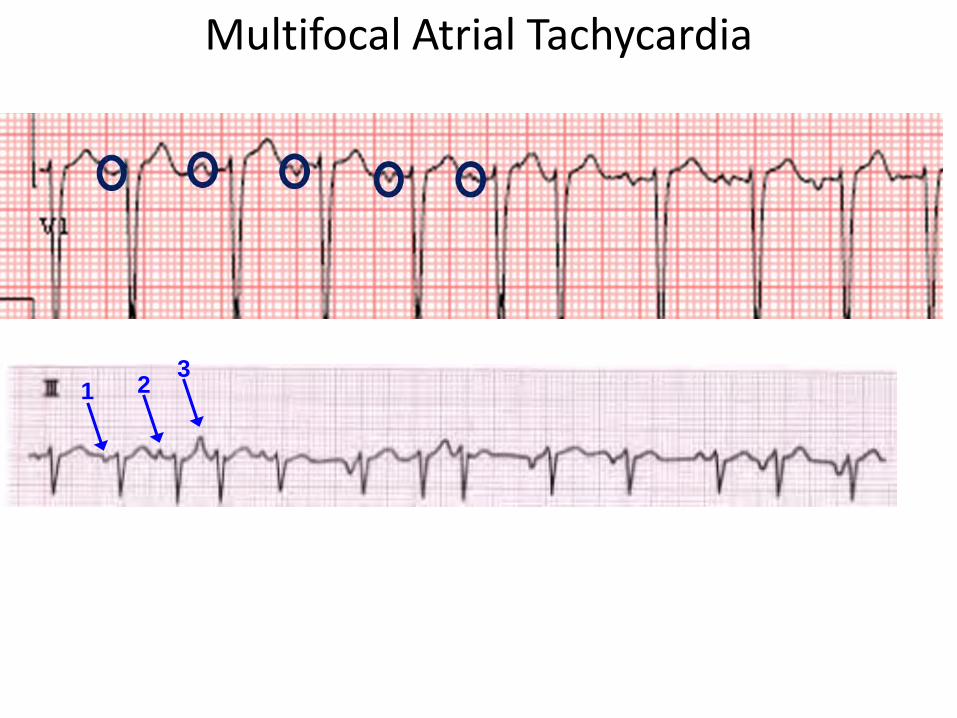
Multifocal Atrial Tachycardia
1 2 3

Multifocal Atrial Tachycardia • ≥3 consecutive, different (non-sinus) P waves at rapid
rate, varying PR interval
• Suspect with irregularly irregular rate, especially with COPD, pulmonary hypertension, coronary/valvular heart disease, hypomagnesemia, theophylline therapy
• First-line treatment: management of the underlying condition. IV magnesium may also be helpful even with normal magnesium levels; rate control with BBs, CCBs
• Antiarrhythmic medications in general are not helpful in suppression of multifocal AT
• Do NOT cardiovert (can provoke VT)

CAUTION! A-fib mimic! Need to look for p-waves!

KEY POINT When you see an irregularly
irregular rhythm, suspect atrial fibrillation (but confirm by absence
of P waves)

AV Block • Delay between atrial and ventricular activation allows
ventricle time to fill
• Excessive slowing or interruption = AV block

• AV conduction disorders: 2nd major cause of bradyarrhythmias (after SA node dysfunction)
• Key clinical decision: “Does this patient need a pacemaker?”
• Decision (usually) relies on three factors:
Symptoms
Site of block
Degree of block
AV block

• What is the degree of block?
1st, 2nd, 3rd degree (complete)
• What is the most likely level of block / delay?
Key Questions
Nodal (narrow QRS)—often benign Infranodal (wide QRS)—potentially lethal

• Autonomic factors (↑ vagal tone) • RCA ischemia / infarct (AV nodal artery in 85%) • Mediations (β-blockers, Ca++-channel, digitalis) • Electrolyte (e.g., hyperkalemia) • Inflammatory (rheumatic fever, SLE,
myocarditis) • Infectious (Lyme, toxoplasmosis, Chagas,
endocarditis ) • Congenital
• Anterior MI • Infiltrative dz (e.g., amyloid, sarcoid, lymphoma) • Degeneration / fibrosis of conduction tissue • Neuromuscular dz (e.g., myotonic dystrophy,
Kearns-Sayre, Erb’s dystrophy) • Iatrogenic (e.g., surgery, post-ablation)
Causes

Prolonged PR interval (First-degree AV block)

Prolonged PR interval (First-degree AV block)
• Not block, per se—delay
• P waves (usually sinus) followed by QRS with uniformly prolonged PR (>200 ms)
• Usually 210-240 ms, but can be longer
• All impulses transmitted from atrialventricles

2nd Degree AV Block
• Characterized by intermittently dropped QRS complexes
Mobitz type I (AV Wenckebach)
Mobitz type II
• Wenckebach AV block = nodal
• Mobitz type II AV block = infranodal
Karel Wenckebach (1864-1940)

2nd Degree, Mobitz I AV Block

AV Wenckebach
• Each stimulus from atria has PROGRESSIVE difficulty traversing the AV node to ventricles (i.e., node increasingly refractory)
• Atrial impulse ultimately not conducted (“dropped QRS”)
• Cycle followed by relative recovery, and starts all over

Mobitz II
• Abruptly dropped QRS:
without PR prolongation
without the shortening of PR after dropped QRS
• Type II AVB is infranodal (wide QRS present)

Complete (3rd Degree) AV Block

Complete (3rd Degree) AV Block
• NO stimuli are transmitted from the atria to the ventricles
• Each paced independently
• SA node usually the pacemaker
• Ventricles paced by nodal or infranodal escape pacemaker, located below point of block
• Rate usually 30-60 bpm

• Atrial rate faster than ventricular rate • Ventricular rate slow, usually regular
• Regularity is key—remember, 2nd degree block irregular (group beating)
• No consistent P-QRS relationship (AV dissociation)


Recipe for 3rd degree (complete) heart block:
1)Bradycardia, REGULAR (usually <50 bpm)
2)Atrial rate > Ventricular rate
3)AV dissociation

Summary: Atrioventricular Conduction Disturbances Prolonged PR/first degree (nodal delay)
2nd degree Mobitz I (intranodal)
2nd degree Mobitz II (infranodal)
Complete/3rd degree (intra or infranodal)

KEY POINTS 3rd degree block is slow and regular,
without “dropped QRS’s”
Mobitz I and II are irregular (pauses due to dropped QRS’s)

Permanent Pacemakers
Key indications to know for ABIM exam:
• Symptomatic sinus bradycardia (including required drug therapy for medical conditions [i.e., beta-blockers for HF])
• Symptomatic AV block
• Mobitz II AV block usually requires a pacemaker
• Do NOT implant for reversible causes (i.e., Lyme carditis with AV block)
Note: 2nd/3rd degree AV block that occurs after STEMI:
Anterior: does not usually improve (necrosis)
Inferior: can improve (vagally mediated)

Key indications to know for ABIM exam:
• Survivors of VT/VF arrest (with nonreversible cause)
• Ischemic/nonischemic cardiomyopathy, LVEF ≤35%, NYHA Class II or III
• Need to be >40 days post-MI
• Optimize medical therapy for at least 3 months prior to ICD (i.e., increase ACE, BB)
• Consider biventricular ICD for symptomatic HF patient with LVEF ≤35%, and wide QRS complex (e.g., LBBB)
Implantable Cardioverter-Defibrillators

A 79 y/o woman is brought into the ED by EMS. Her neighbor found her in the hallway of their apartment building, obtunded. No records are available.

What is the most appropriate next step in management?
A. Activate the cath lab B. Administer naloxone C. Emergent hemodialysis D. Insert a transvenous pacemaker E. Order a brain MRI

Hyperkalemia
Moderate-Severe Severe Mild-Moderate

You can now…. • Identify and treat paroxysmal SVT
• Distinguish atrial fibrillation and MAT
• Recognize a reperfusion arrhythmia
• Recognize and differentiate AV block
• Identify who may need a pacemaker or ICD
• Recognize the ECG signature of a life threatening electrolyte abnormality

AVNRT AVRT
Narrow-complex Narrow or wide complex
Reentry: fast and slow AV pathways Reentry: AV node and bypass tract
Young, generally female (32±18 y/o) Younger (23±14 y/o)
No risk of sudden death Low risk of sudden death (pre-excited atrial fibrillation)
Baseline ECG: normal Baseline ECG: WPW
Tachycardia may show no P waves, (don’t confuse with junctional tachycardia) or P waves just after QRS complex
Tachycardia may show P waves more distinct from QRS complex