Embed Size (px)
Citation preview
Common Connective tissueCommon Connective tissue Diseases
Siriporn Juthong, M.D.
Division of Rheumatology
Songklanagarind HospitalSongklanagarind Hospital
23/11/58
Wh t th di i ti ti• What are the diseases in connective tissue disorder ?
• Sign and symptoms of CTD ?
Nonspecific organ manifestations of CTDNonspecific organ manifestations of CTD
Fatigue/tiredness/malaise
CTD Chronic infection
Fever
Weight lossMalignancy (esp.hemato)
g
Enlarged lymph nodes
differential diagnosis to be
consider23/11/58
consider
Specific organ/system manifestation of CTDSpecific organ/system manifestation of CTD
Polyarthritis / Polyarthralgia
Raynaud phenomenon
Skin/mucosal lesionsSkin/mucosal lesions
Serositis/myositis/vasculitis
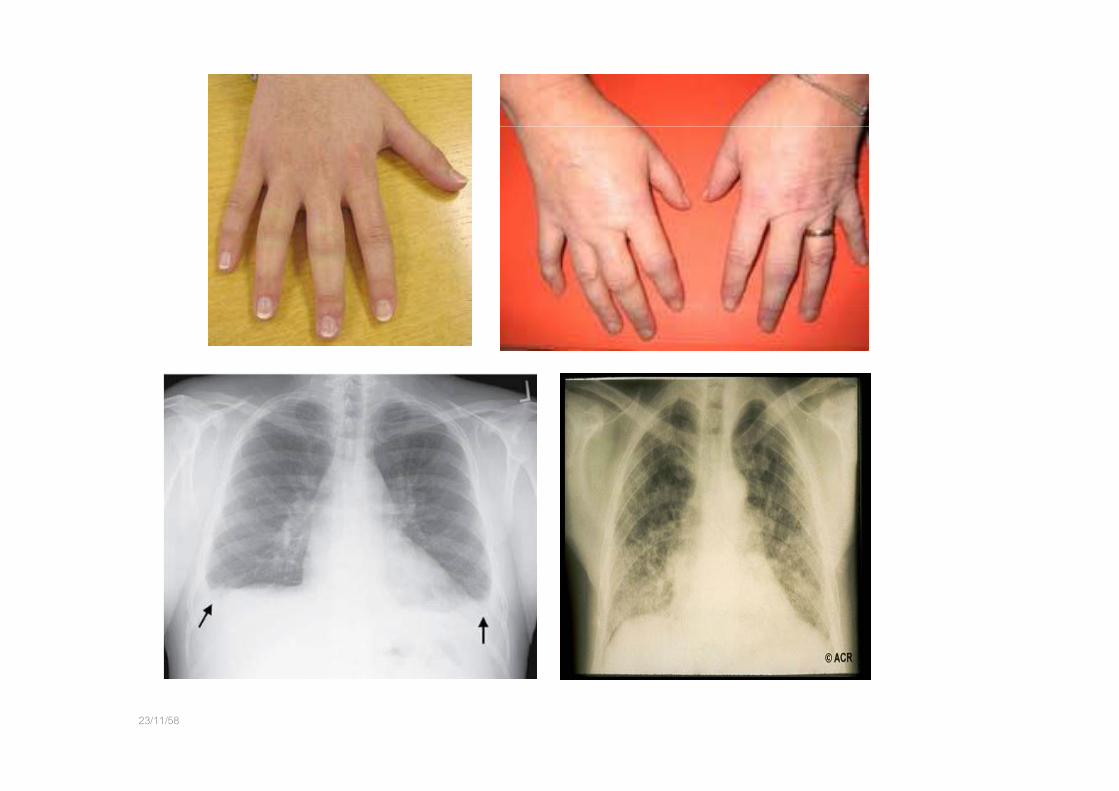
Interstitial lung disease
Multi‐organ systems involvement
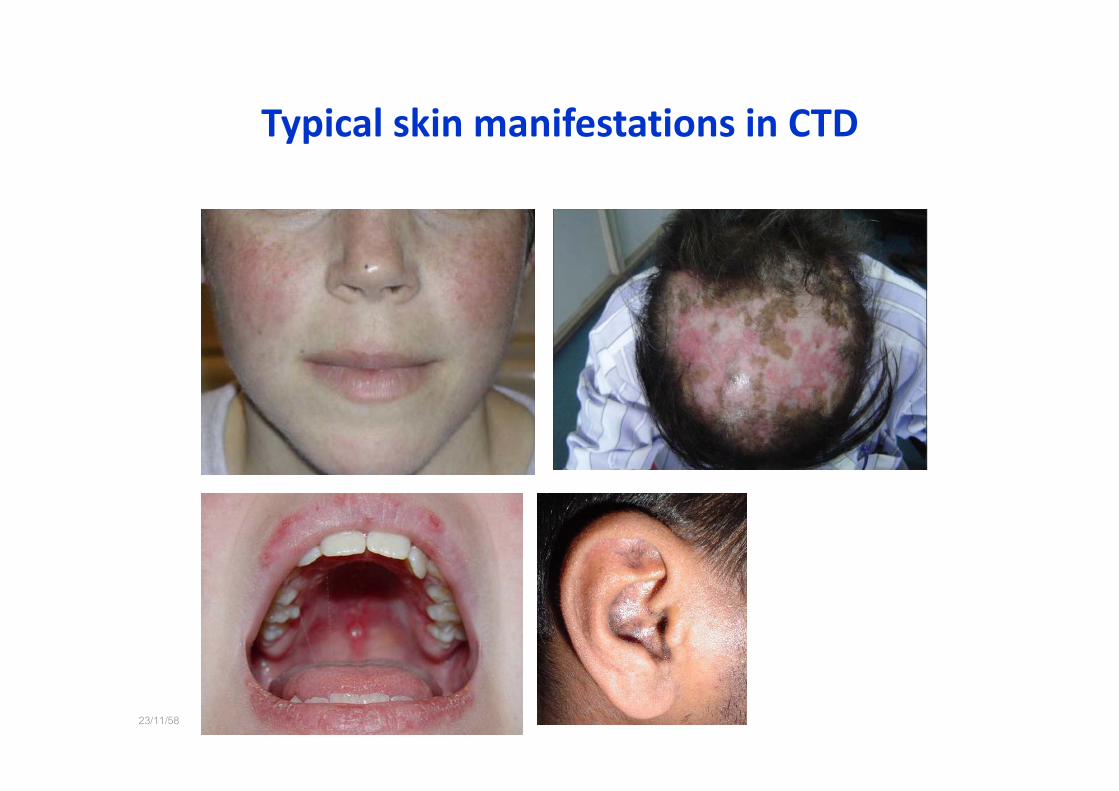
Typical skin manifestations in CTDTypical skin manifestations in CTD
23/11/58
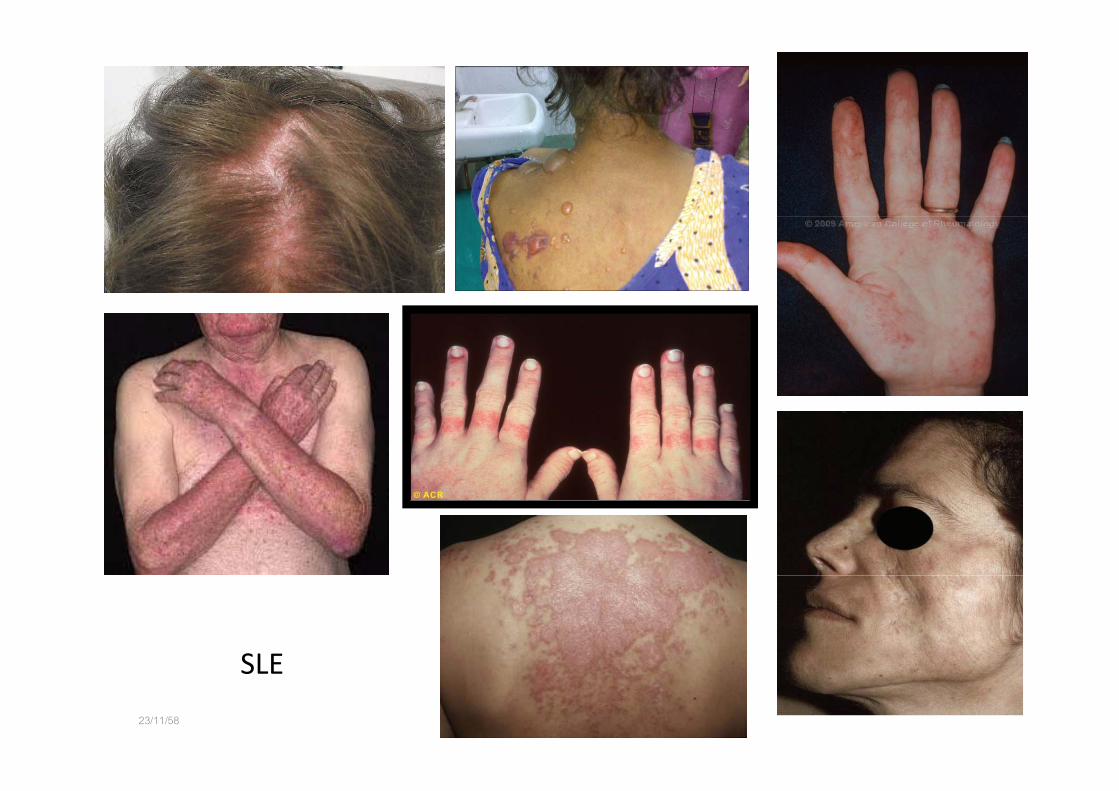
SLE
23/11/58
SLE

Systemic sclerosis
23/11/58

23/11/58 Abnormal nail fold capillaroscopy

23/11/58 Inflammatory myositis : Dermatomyositis

V liti h23/11/58
Vasculitic rash
23/11/58
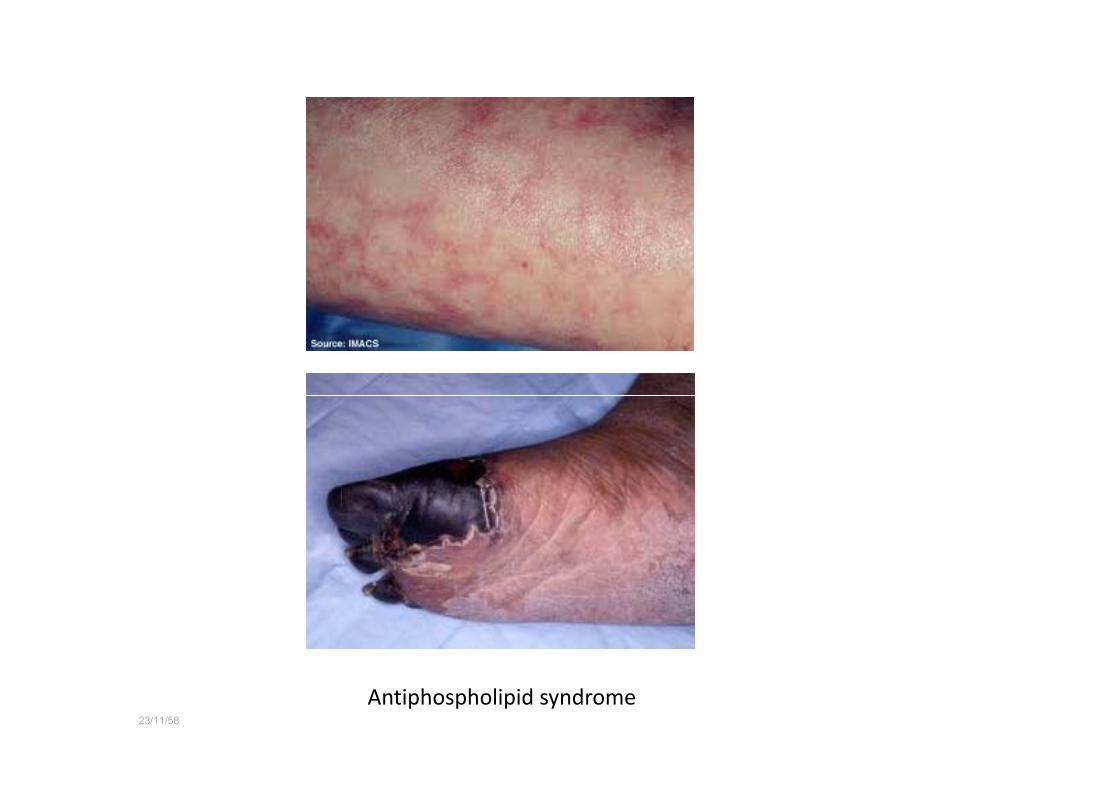
Antiphospholipid syndrome

Sicca symptom : “ Sjogren syndrome”
23/11/58
23/11/58
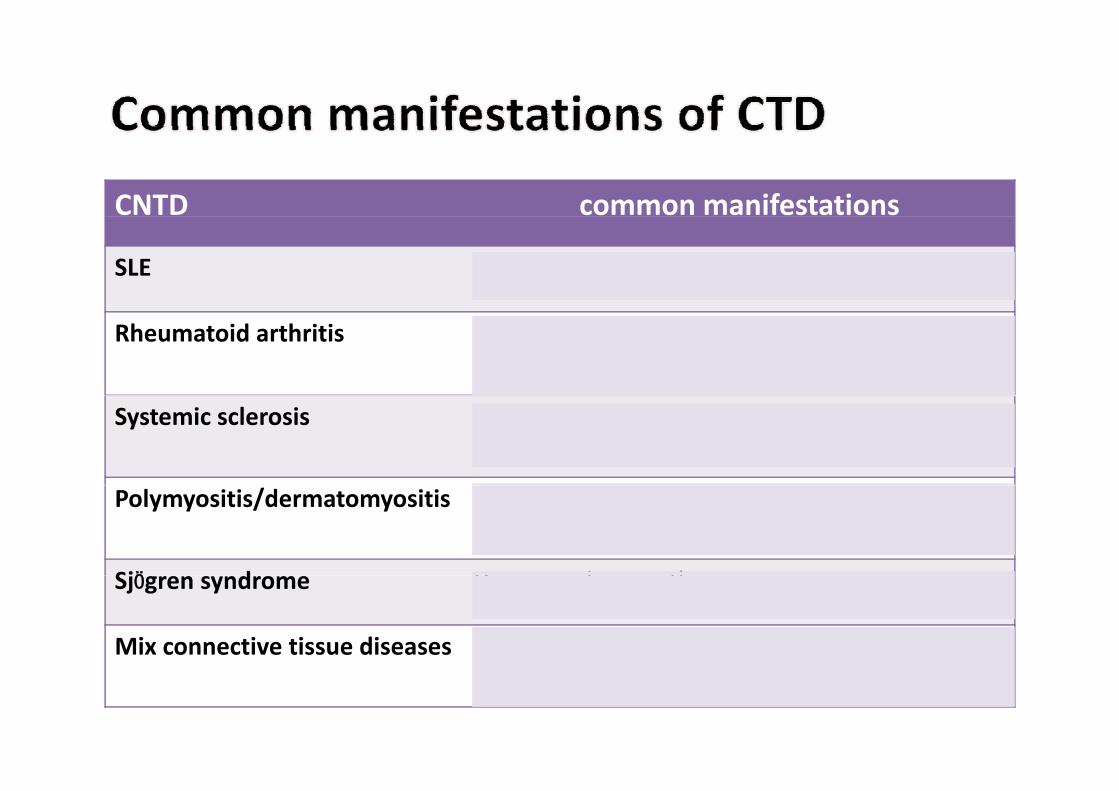
CNTD common manifestations
SLE malar rash, discoid rash, arthritis, oral ulcer
Rheumatoid arthritis Chronic symmetrical polyarthritis of hands joints, erosion +, ± deformities
Systemic sclerosis Cutaneous sclerosis, sclerodactyly, digital pitting scar
Polymyositis/dermatomyositis Proximal muscle weakness, CPK↑, heliotrope, gottron papules
SjӦ d D d thSjӦgren syndrome Dry eyes, dry mouth
Mix connective tissue diseases Mixed pattern of CNTD manifestations and positive U1RNP
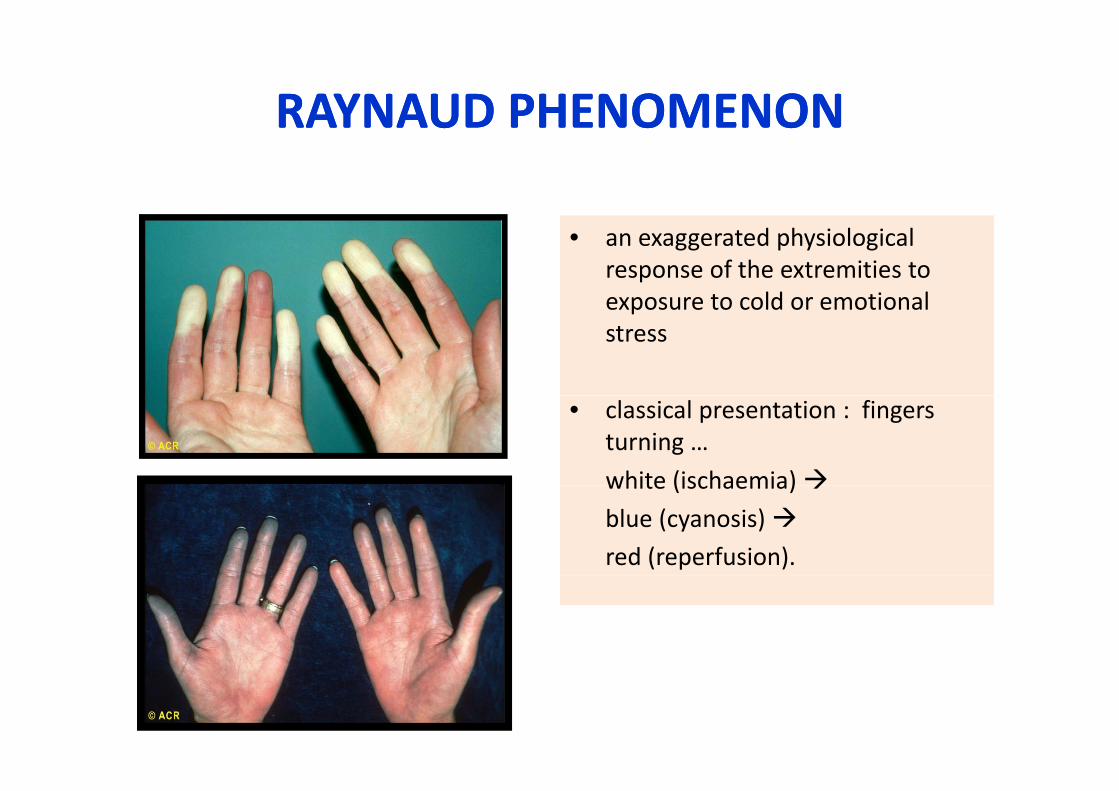
RAYNAUD PHENOMENONRAYNAUD PHENOMENONRAYNAUD PHENOMENONRAYNAUD PHENOMENON
• an exaggerated physiological response of the extremities to exposure to cold or emotionalexposure to cold or emotional stress
• classical presentation : fingers turning …
white (ischaemia)white (ischaemia)
blue (cyanosis) red (reperfusion).
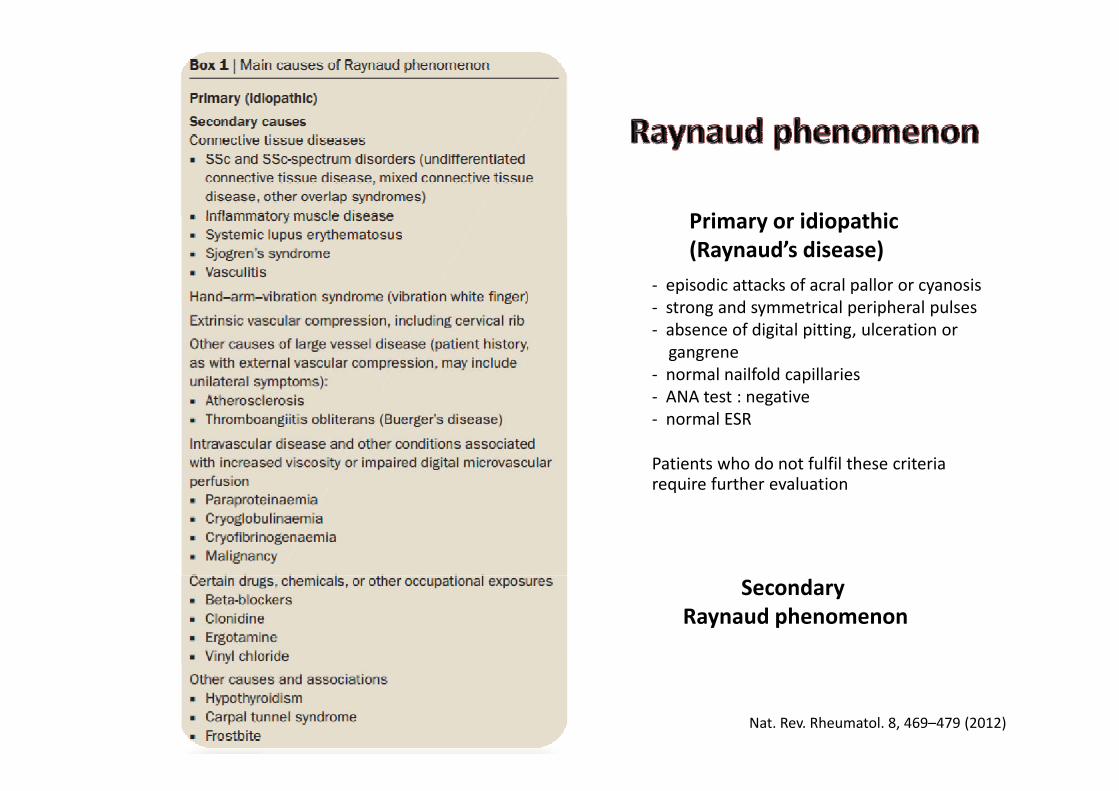
P i idi thiPrimary or idiopathic(Raynaud’s disease)
‐ episodic attacks of acral pallor or cyanosisstrong and symmetrical peripheral pulses‐ strong and symmetrical peripheral pulses
‐ absence of digital pitting, ulceration or gangrene
‐ normal nailfold capillariesANA test : negative‐ ANA test : negative
‐ normal ESR
Patients who do not fulfil these criteria require further evaluationrequire further evaluation
Secondary Raynaud phenomenon
Nat. Rev. Rheumatol. 8, 469–479 (2012)
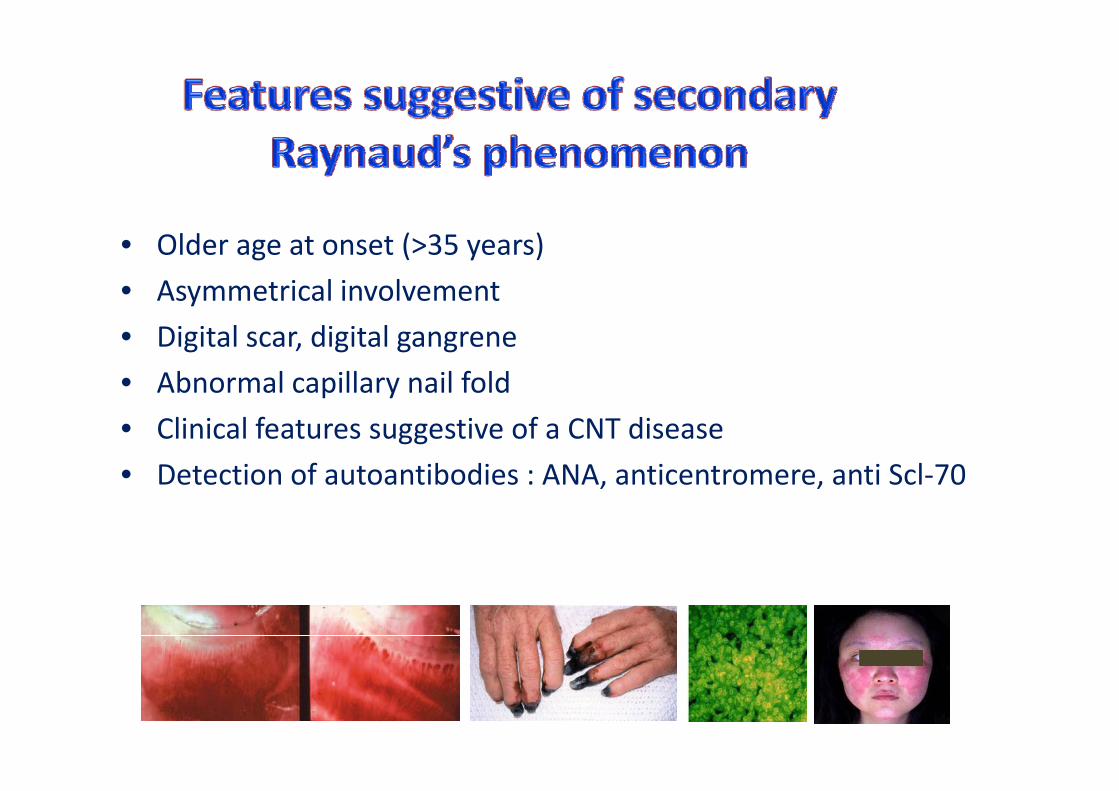
• Older age at onset (>35 years)
• Asymmetrical involvementy
• Digital scar, digital gangrene
• Abnormal capillary nail fold p y
• Clinical features suggestive of a CNT disease
• Detection of autoantibodies : ANA, anticentromere, anti Scl‐70, ,

23/11/58
A 23 year old woman presents to her general practitioner withy p g pa three month history of malaise, fatigue, and arthralgia whichshe attributes to a viral illness. She had also attended theemergency department with pleuritic chest pain at the start ofsymptoms. She has had two miscarriages in the past, but hasth i b h lth O i ti th llotherwise been healthy. On examination, there are small,
non‐tender lymph nodes in her neck and mildly swollen,tender proximal interphalangeal joints in her handstender, proximal interphalangeal joints in her hands.
What are the next investigations?g
BMJ 2013;347:f5060 doi: 10.1136/bmj.f5060
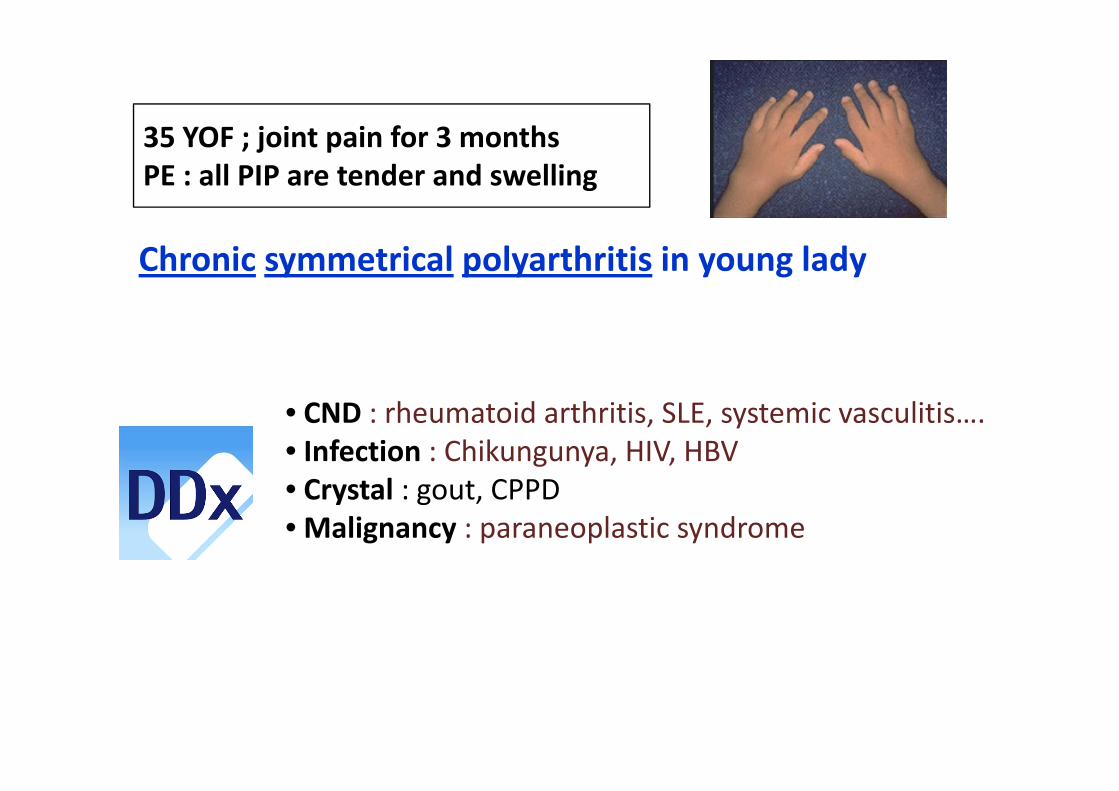
j i i f h35 YOF ; joint pain for 3 monthsPE : all PIP are tender and swelling
Chronic symmetrical polyarthritis in young lady
• CND : rheumatoid arthritis, SLE, systemic vasculitis….• Infection : Chikungunya, HIV, HBV• Crystal : gout CPPD• Crystal : gout, CPPD• Malignancy : paraneoplastic syndrome
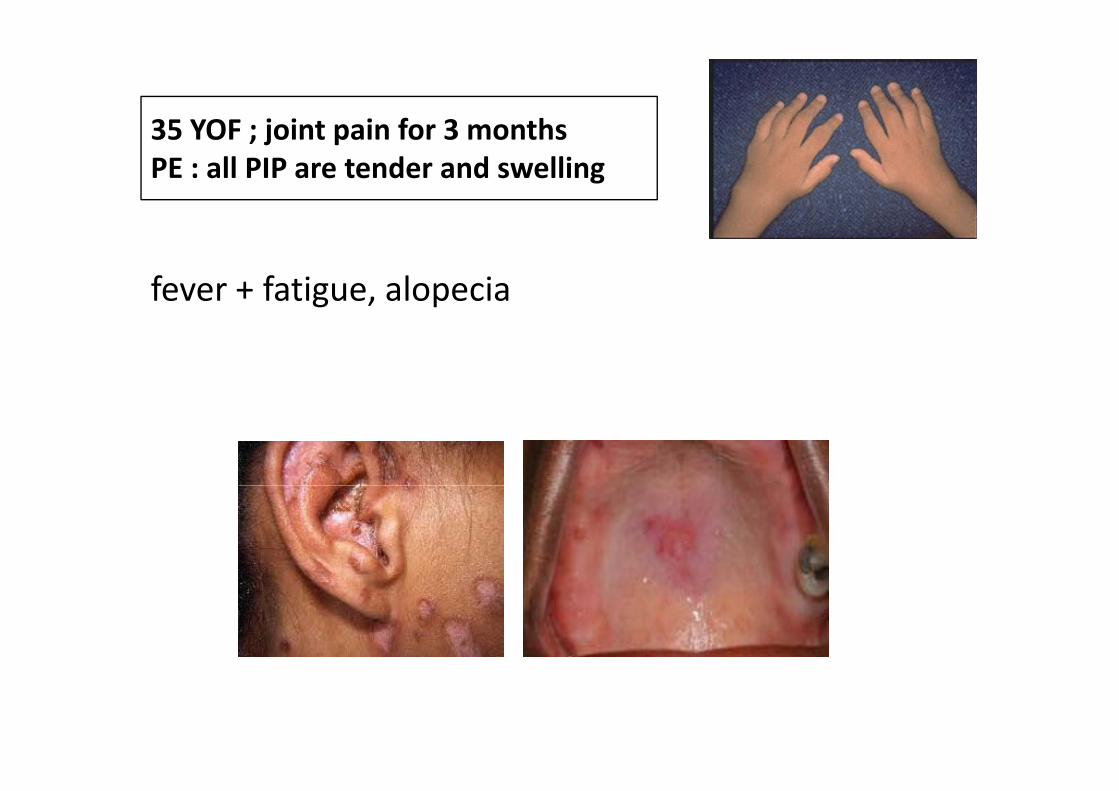
35 YOF ; joint pain for 3 months35 YOF ; joint pain for 3 monthsPE : all PIP are tender and swelling
fever + fatigue, alopecia g , p
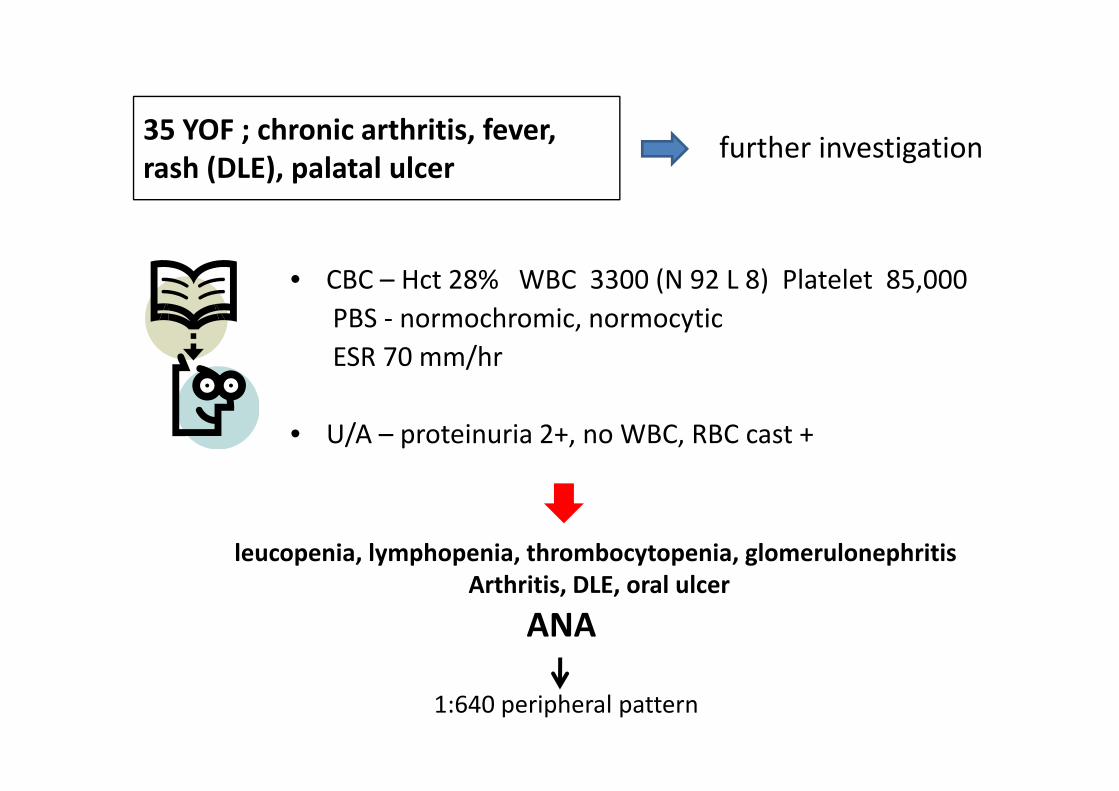
35 YOF ; chronic arthritis fever35 YOF ; chronic arthritis, fever, rash (DLE), palatal ulcer
further investigation
• CBC – Hct 28% WBC 3300 (N 92 L 8) Platelet 85,000 PBS ‐ normochromic, normocyticESR 70 mm/hr
• U/A – proteinuria 2+, no WBC, RBC cast +
leucopenia, lymphopenia, thrombocytopenia, glomerulonephritish l l
ANA Arthritis, DLE, oral ulcer
1:640 peripheral pattern
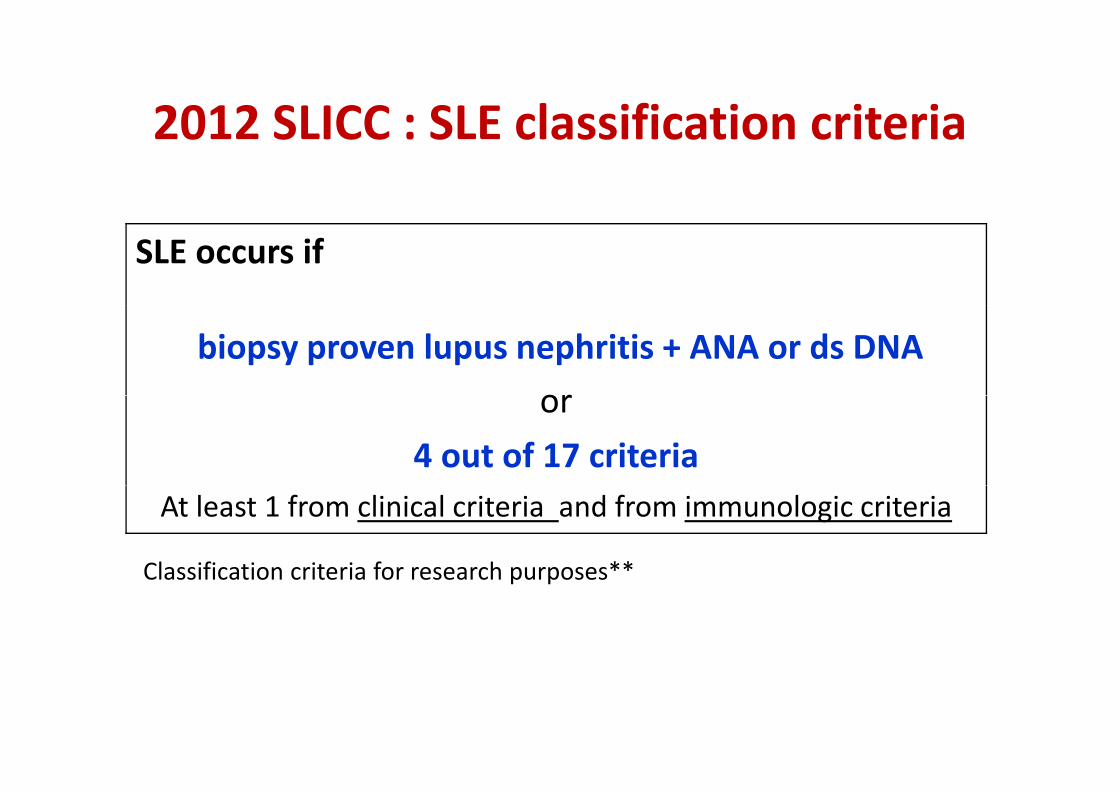
2012 SLICC : SLE classification criteria2012 SLICC : SLE classification criteria
SLE occurs if
biopsy proven lupus nephritis + ANA or ds DNA
oror
4 out of 17 criteria At least 1 from clinical criteria and from immunologic criteria
Classification criteria for research purposes**Classification criteria for research purposes
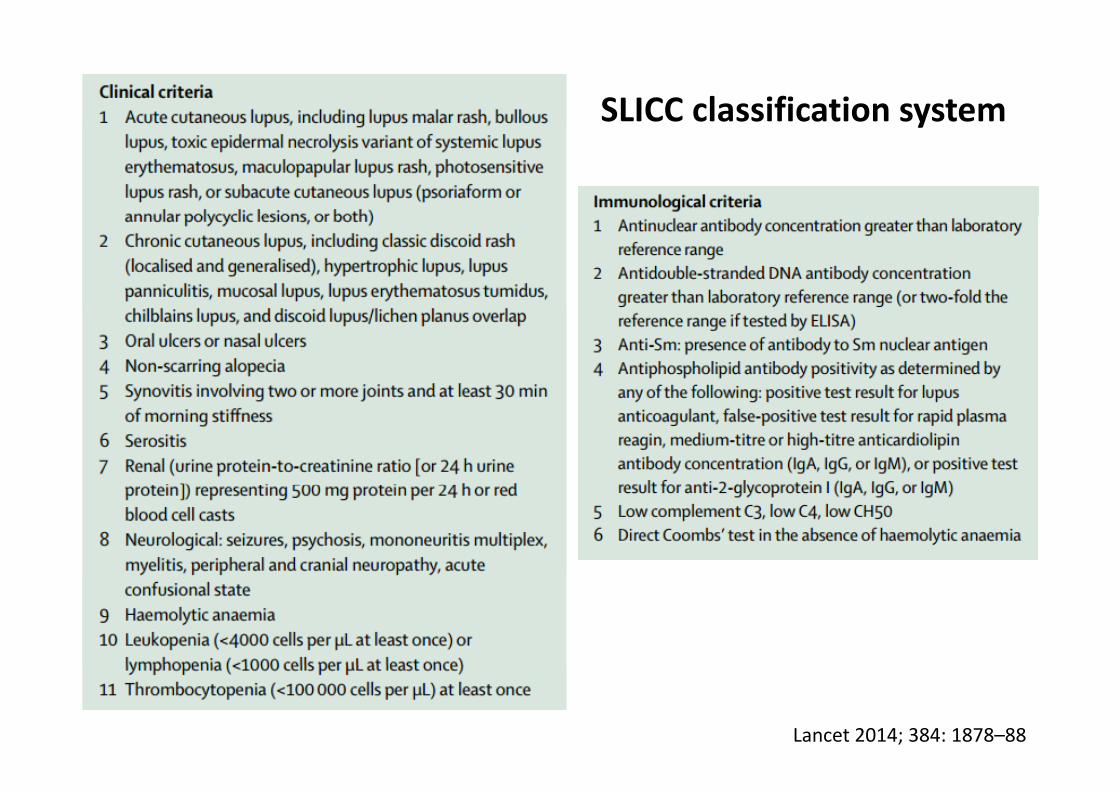
SLICC classification systemy
Lancet 2014; 384: 1878–88
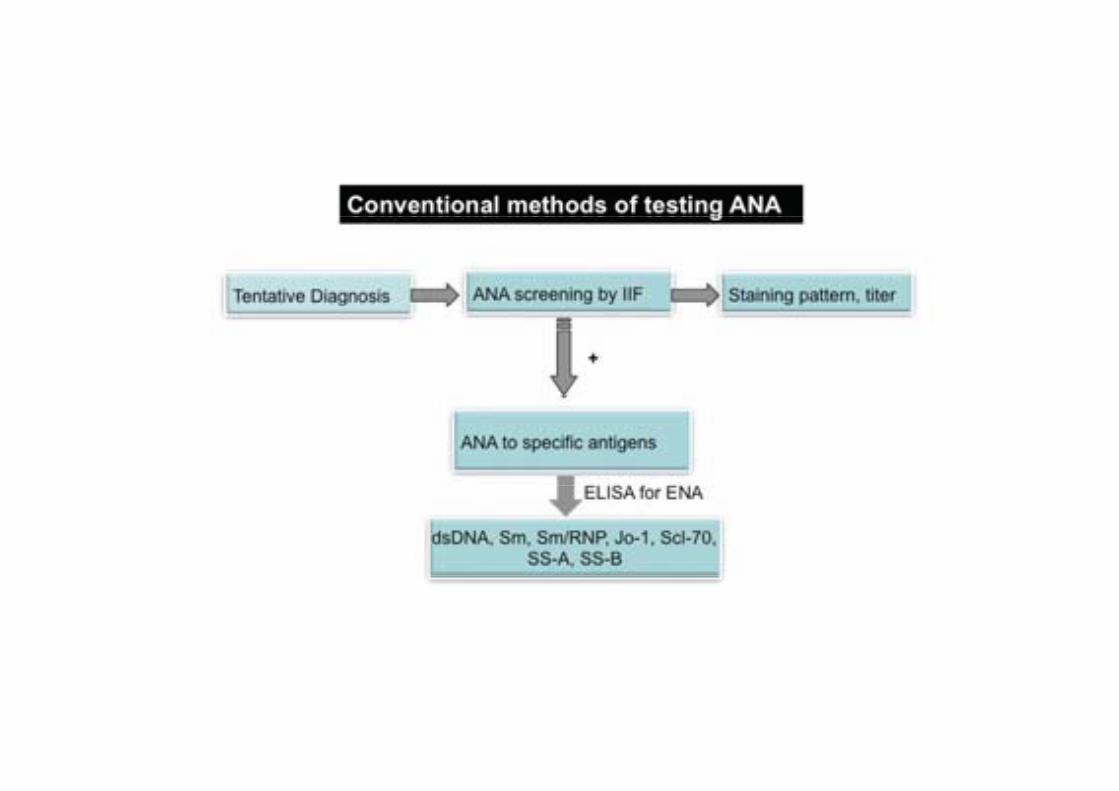
Antinuclear antibodiesAntinuclear antibodies
• A group of autoAb specificities targeting antigens in nucleus, also in cytoplasm.
Highly sensitive, but non‐specific and not diagnostic Serum titer of ANA does not correlate with disease severity and activity
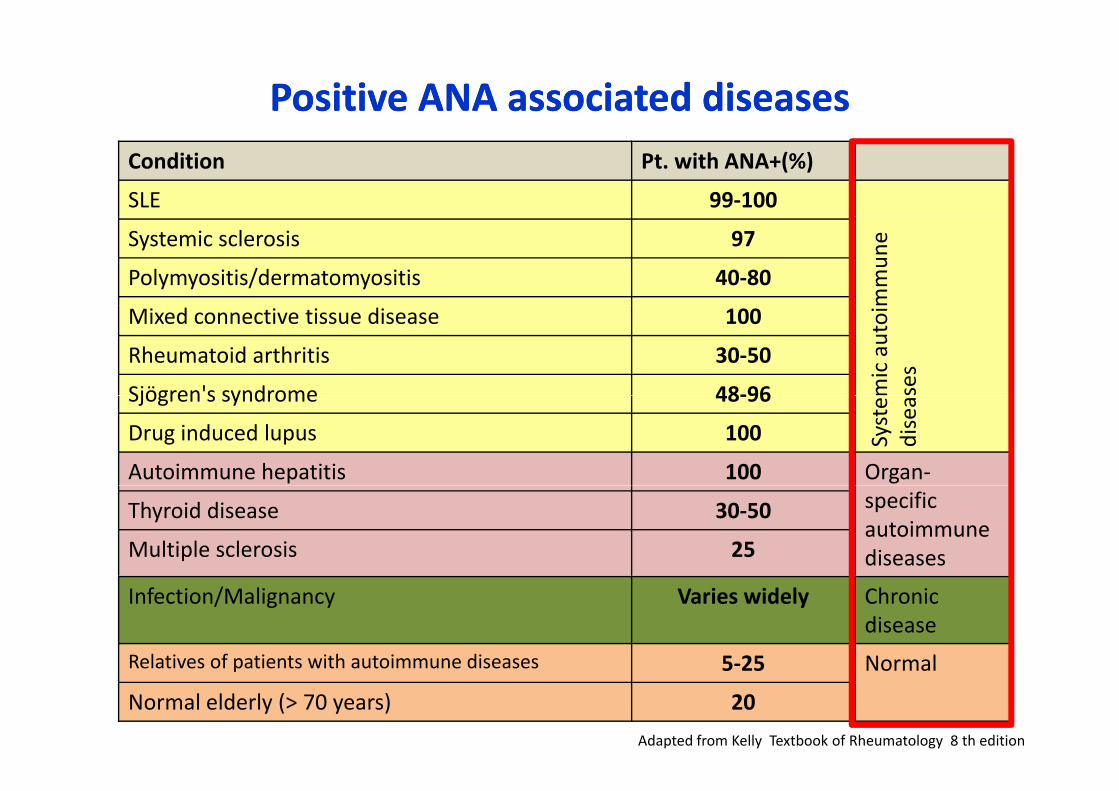
Positive ANA associated diseasesPositive ANA associated diseasesCondition Pt. with ANA+(%)
SLE 99‐100
mmun
e Systemic sclerosis 97
Polymyositis/dermatomyositis 40‐80
mic autoi
ses
Mixed connective tissue disease 100
Rheumatoid arthritis 30‐50
Sjögren's syndrome 48‐96
Syste
diseaSjögren s syndrome 48‐96
Drug induced lupus 100
Autoimmune hepatitis 100 Organ‐specificautoimmunediseases
Thyroid disease 30‐50
Multiple sclerosis 25
Infection/Malignancy Varies widely Chronicdisease
Relatives of patients with autoimmune diseases 5‐25 NormalRelatives of patients with autoimmune diseases 5‐25 Normal
Normal elderly (> 70 years) 20
Adapted from Kelly Textbook of Rheumatology 8 th edition
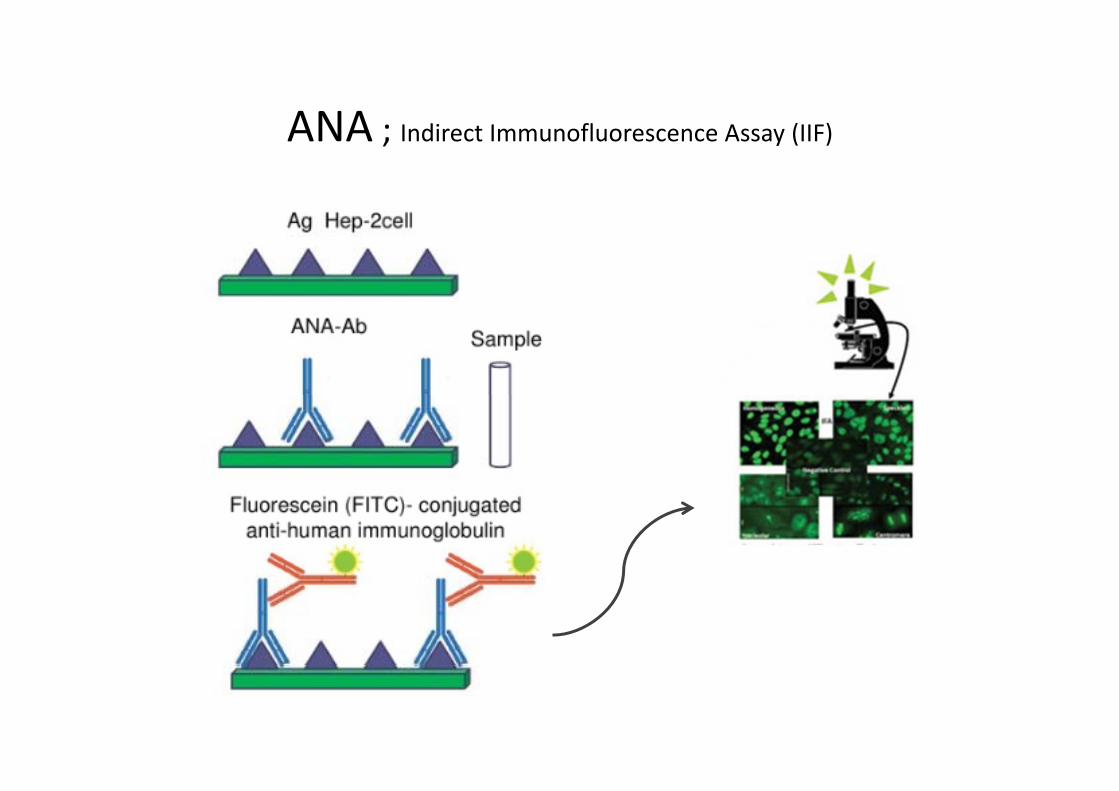
ANA ; I di t I fl A (IIF)ANA ; Indirect Immunofluorescence Assay (IIF)
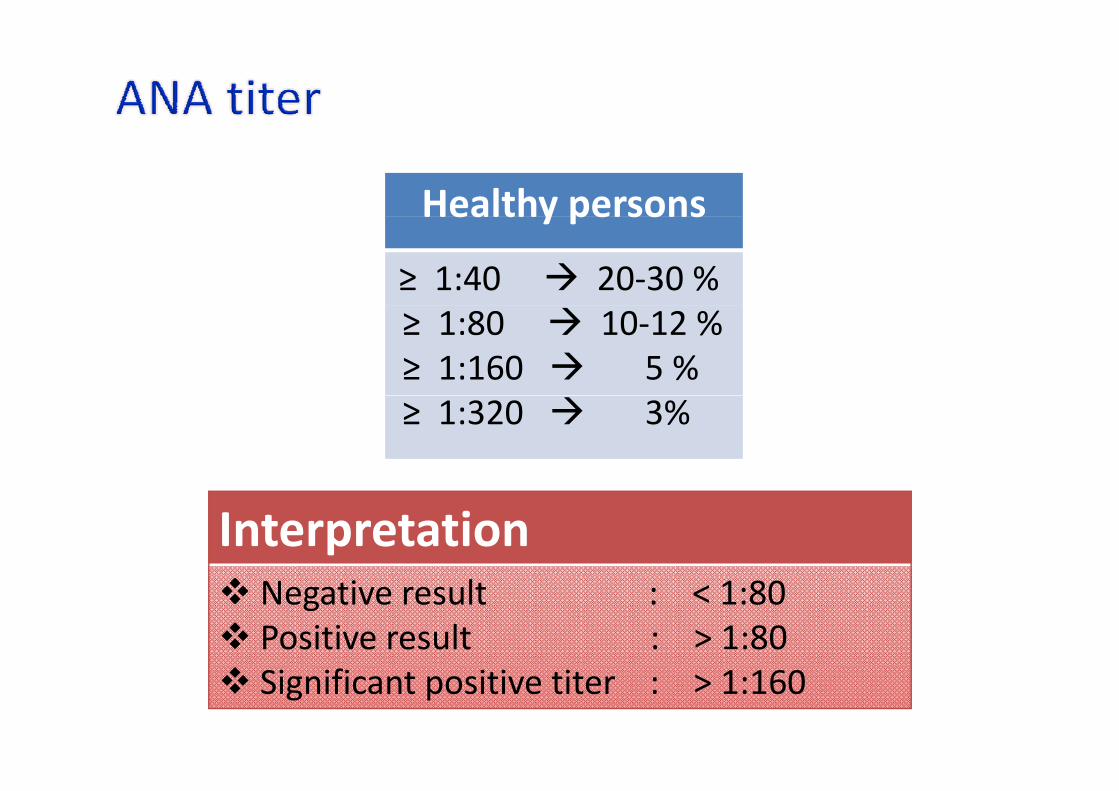
Healthy personsHealthy persons
≥ 1:40 20‐30 %≥ 1:80 10‐12 %≥ 1:160 5 %≥ 1:320 3%
InterpretationNegative result : < 1:80Positive result : > 1:80Significant positive titer : > 1:160
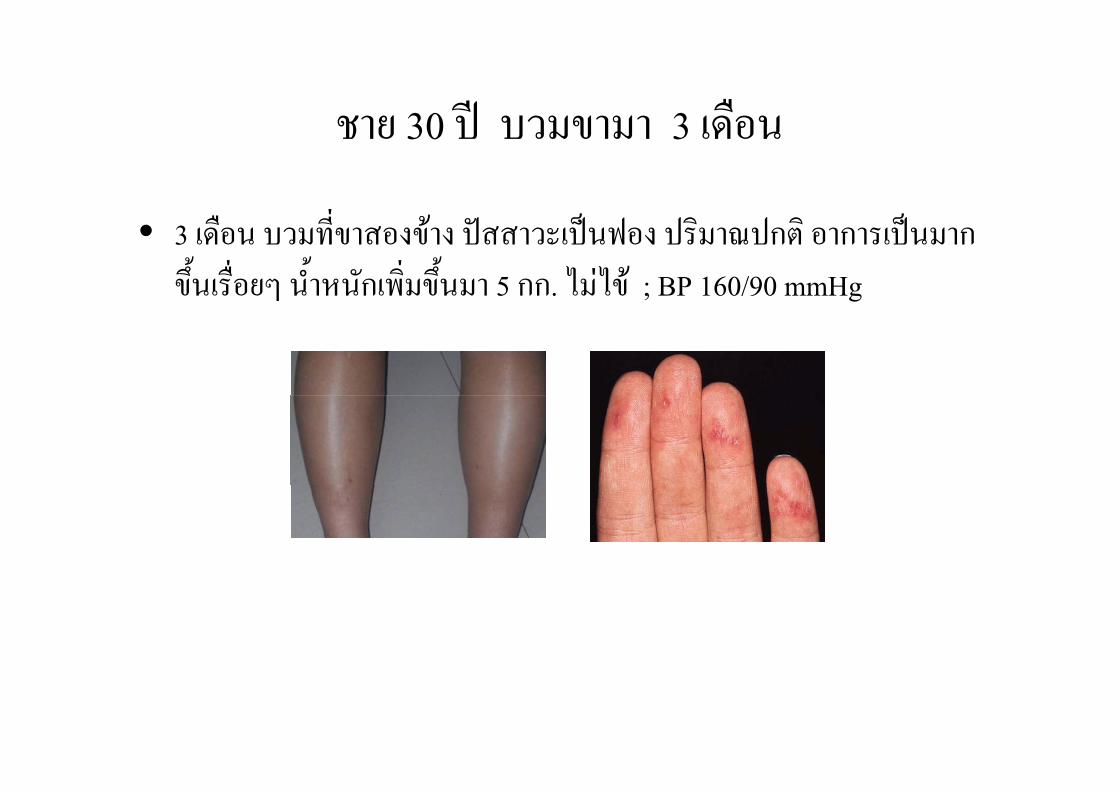
ชาย 30 ป บวมขามา 3 เดือน ชาย 30 ป บวมขามา 3 เดอน
ื ่ • 3 เดือน บวมทีขาสองขาง ปสสาวะเปนฟอง ปริมาณปกติ อาการเปนมาก
ขึ้นเรื่อยๆ น้ําหนักเพิ่มขึ้นมา 5 กก. ไมไข ; BP 160/90 mmHg
ชาย 30 ป บวมขามา 3 เดอืน
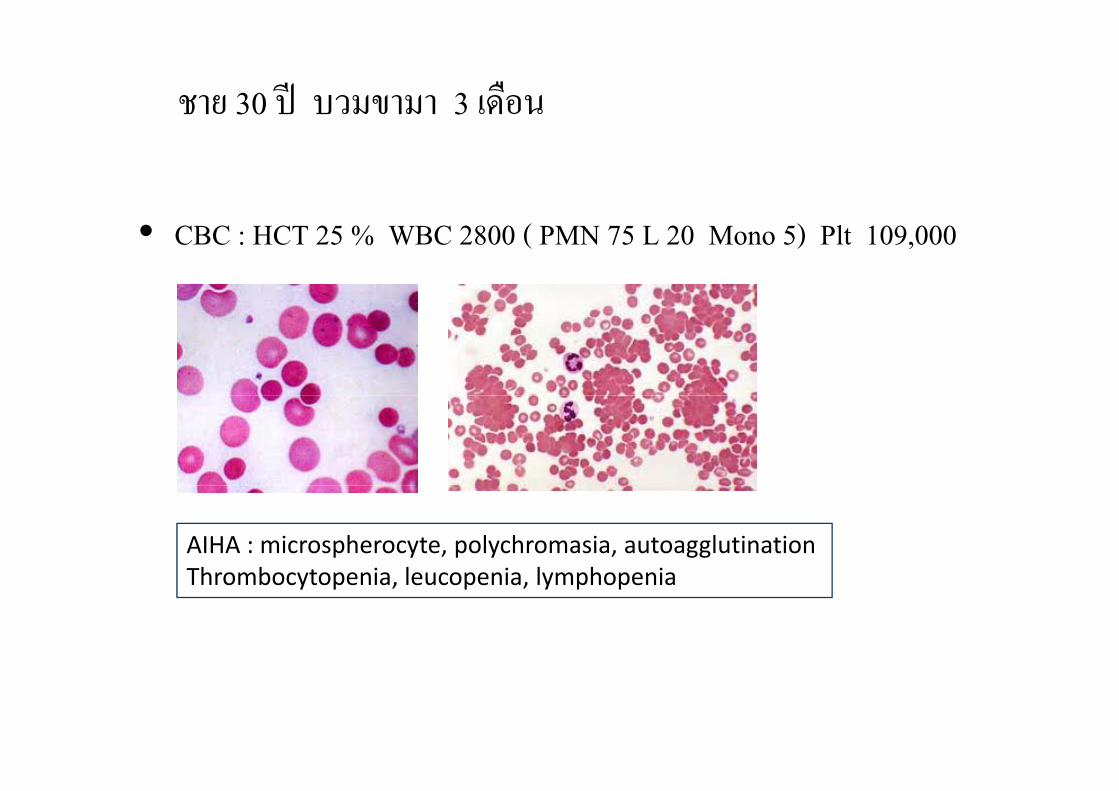
• CBC : HCT 25 % WBC 2800 ( PMN 75 L 20 Mono 5) Plt 109,000
AIHA : microspherocyte, polychromasia, autoagglutinationThrombocytopenia leucopenia lymphopeniaThrombocytopenia, leucopenia, lymphopenia
ชาย 30 ป บวมขามา 3 เดอืน
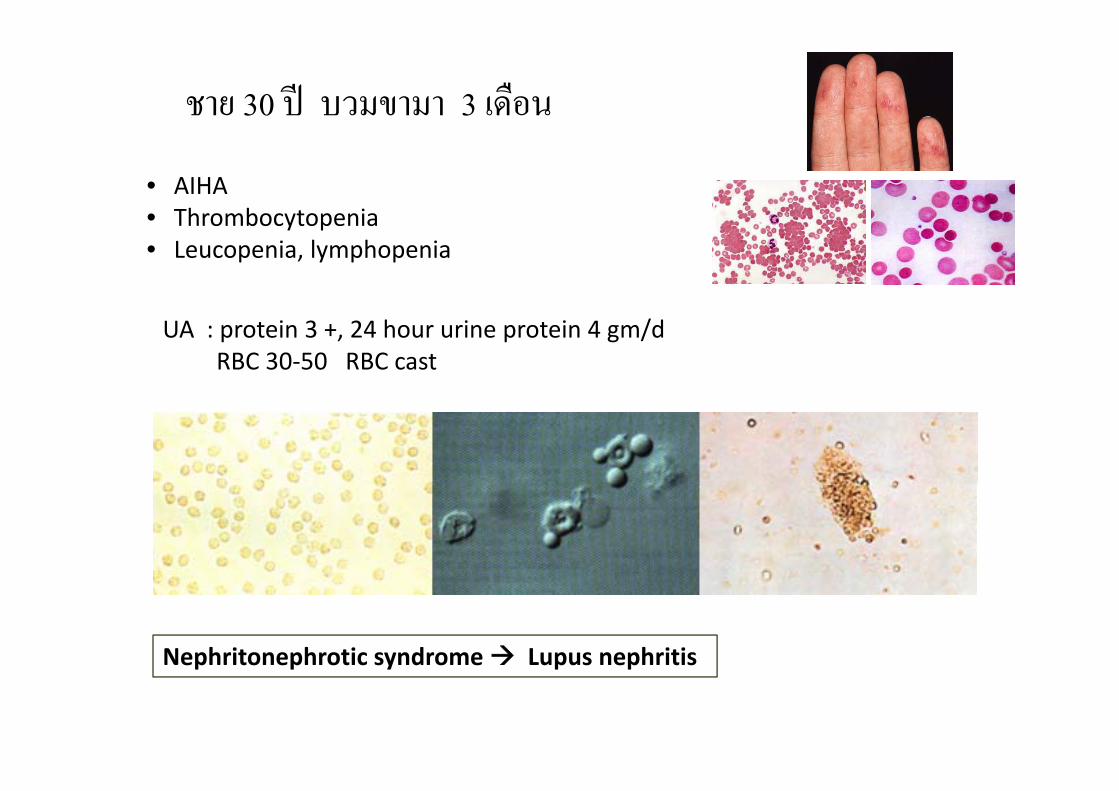
• AIHA• Thrombocytopenia• Thrombocytopenia• Leucopenia, lymphopenia
UA : protein 3 +, 24 hour urine protein 4 gm/dRBC 30‐50 RBC cast
Nephritonephrotic syndrome Lupus nephritisNephritonephrotic syndrome upus nephritis
ชาย 30 ป บวมขามา 3 เดอืน
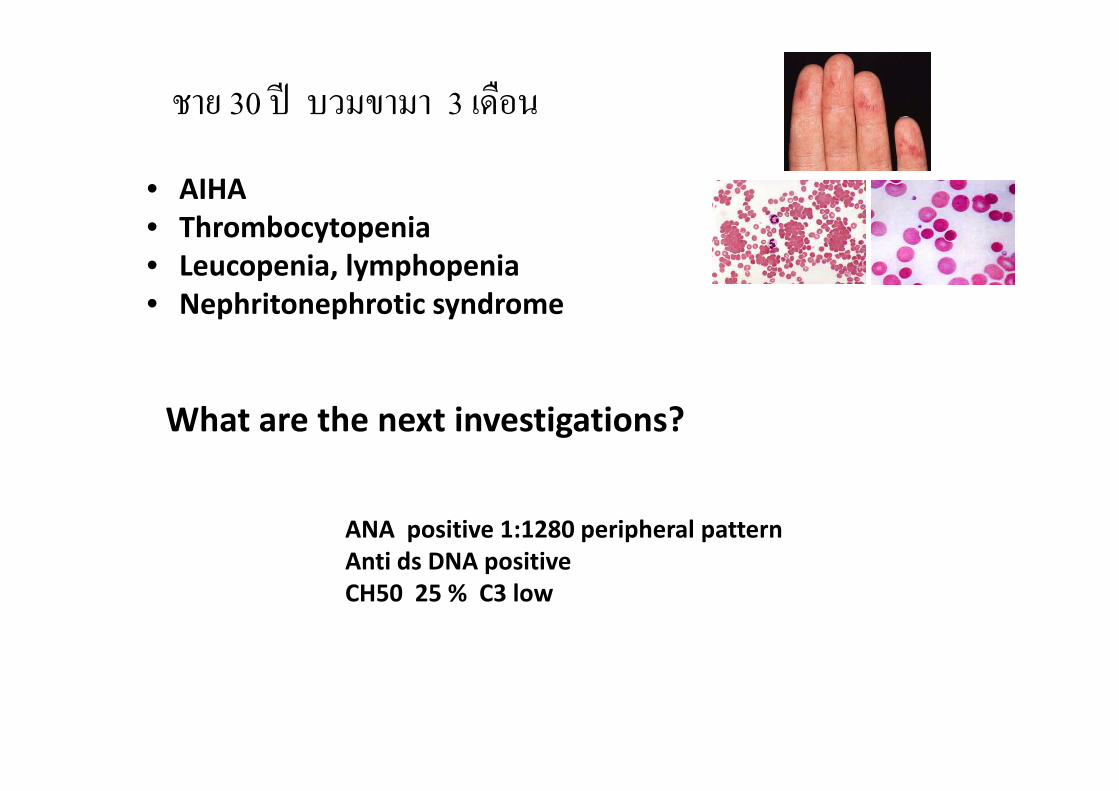
• AIHAh b i• Thrombocytopenia
• Leucopenia, lymphopenia• Nephritonephrotic syndrome• Nephritonephrotic syndrome
What are the next investigations?
ANA positive 1:1280 peripheral patternAnti ds DNA positiveCH50 25 % C3 low
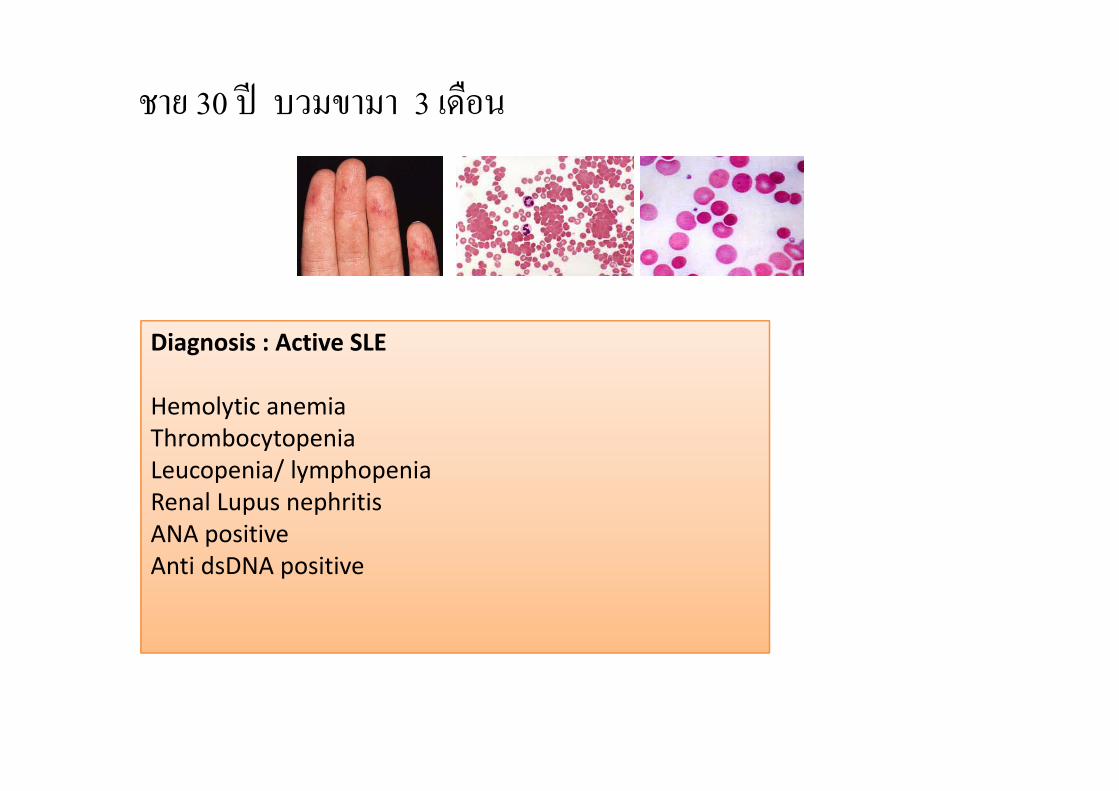
ชาย 30 ป บวมขามา 3 เดอืน
Diagnosis : Active SLE
Hemolytic anemiaThrombocytopeniaLeucopenia/ lymphopeniaRenal Lupus nephritisANA positive Anti dsDNA positivep
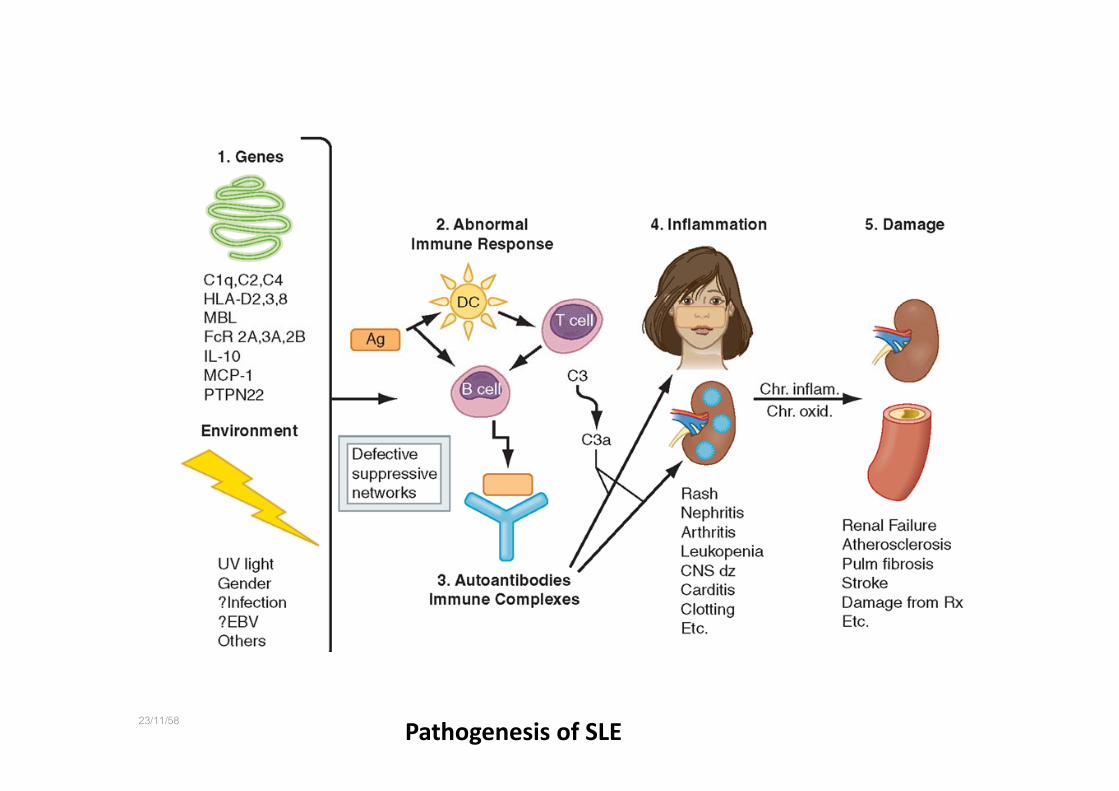
23/11/58Pathogenesis of SLE
23/11/58
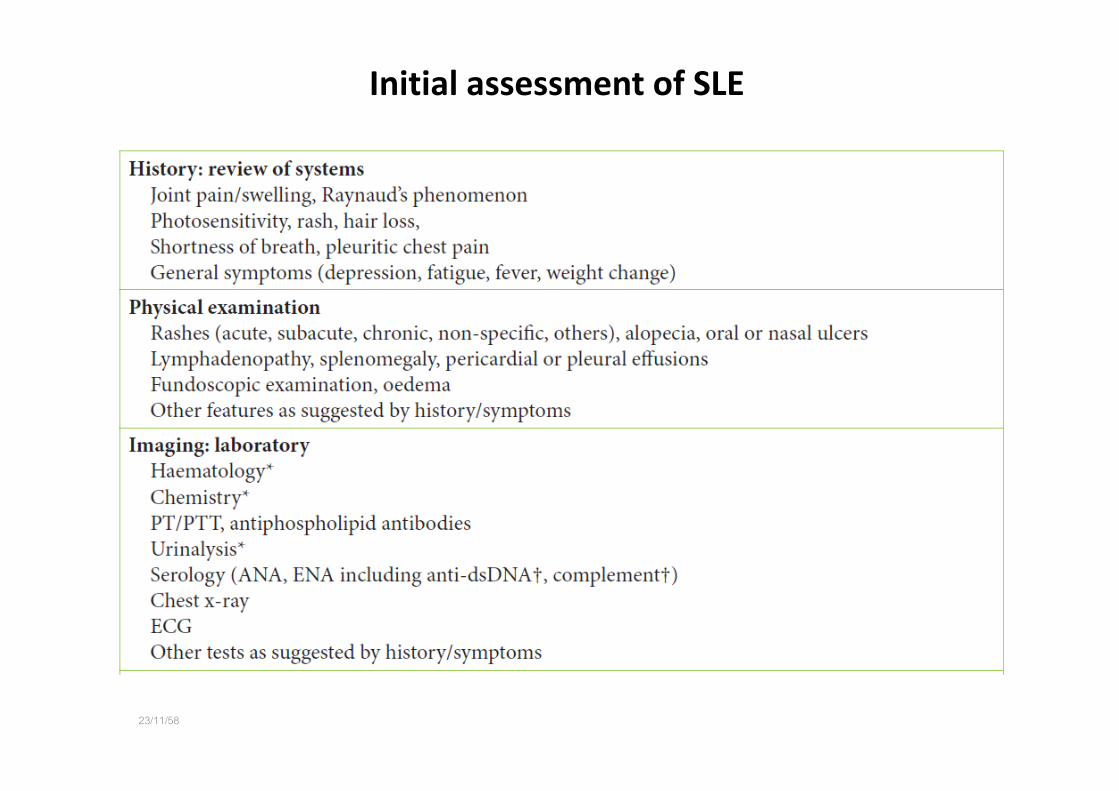
Initial assessment of SLE
23/11/58

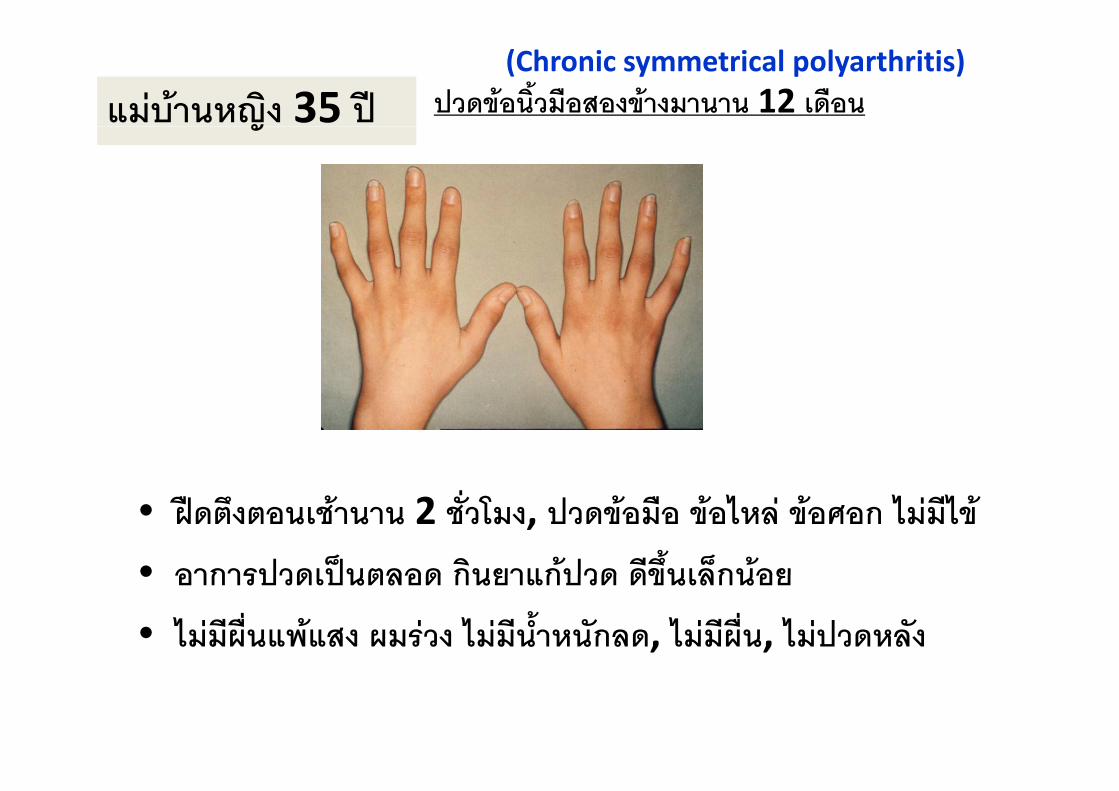
แมบานหญิง 35 ป(Chronic symmetrical polyarthritis)
ปวดขอนิ้วมือสองขางมานาน 12 เดือนญ
• ฝดตึงตอนเชานาน 2 ชั่วโมง, ปวดขอมือ ขอไหล ขอศอก ไมมีไข
• อาการปวดเปนตลอด กินยาแกปวด ดีขึ้นเล็กนอย• อาการปวดเปนตลอด กนยาแกปวด ดขนเลกนอย
• ไมมีผื่นแพแสง ผมรวง ไมมีน้ําหนักลด, ไมมีผื่น, ไมปวดหลัง
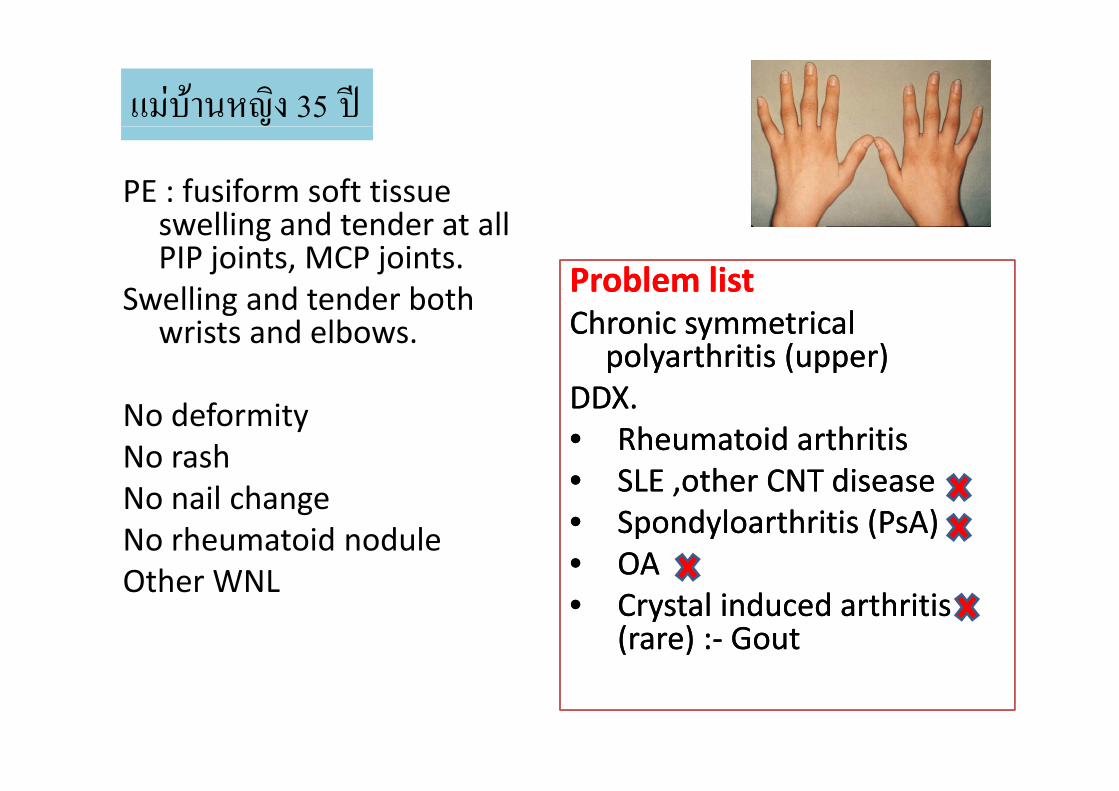
แมบานหญิง 35 ป
PE : fusiform soft tissue lli d t d t llswelling and tender at all
PIP joints, MCP joints.Swelling and tender both Problem listProblem listSwelling and tender both
wrists and elbows. Chronic symmetrical polyarthritis (upper)
DDX
Chronic symmetrical polyarthritis (upper)
DDXNo deformityNo rash
DDX.• Rheumatoid arthritis• SLE other CNT disease
DDX.• Rheumatoid arthritis• SLE other CNT diseaseNo nail change
No rheumatoid noduleOth WNL
SLE ,other CNT disease• Spondyloarthritis (PsA)• OA
SLE ,other CNT disease• Spondyloarthritis (PsA)• OAOther WNL• Crystal induced arthritis
(rare) :‐ Gout• Crystal induced arthritis
(rare) :‐ Gout
แมบานหญิง 35 ป
• CBC, ESR, Film both hands ( AP, Oblique), RF
• Cr, AST, ALT, CXR
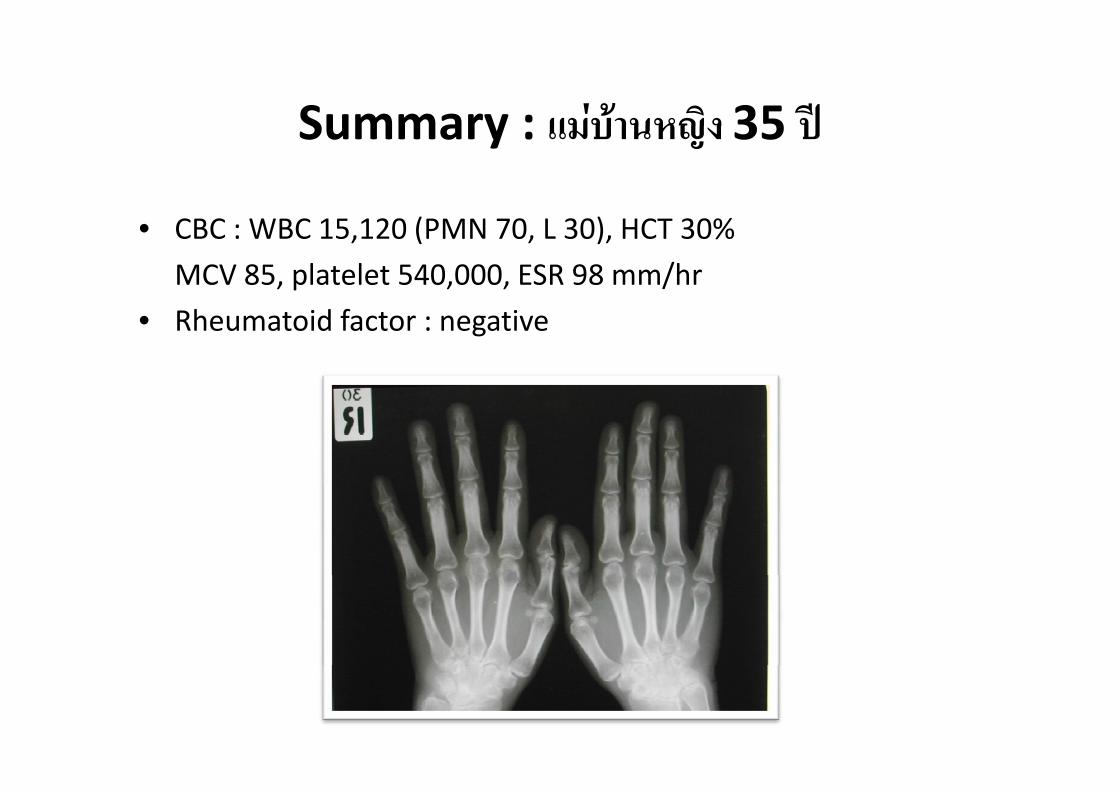
Summary : แมบานหญิง 35 ปSummary : แมบานหญง 35 ป
• CBC : WBC 15,120 (PMN 70, L 30), HCT 30%
MCV 85, platelet 540,000, ESR 98 mm/hr
• Rheumatoid factor : negative
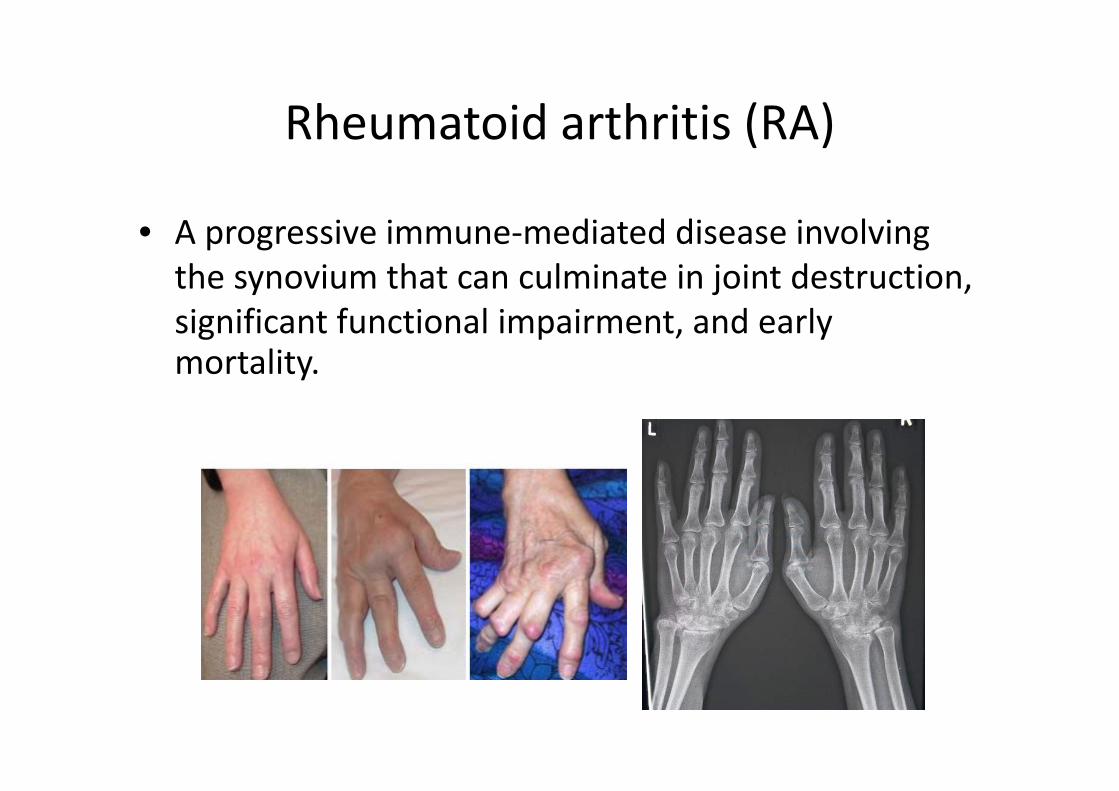
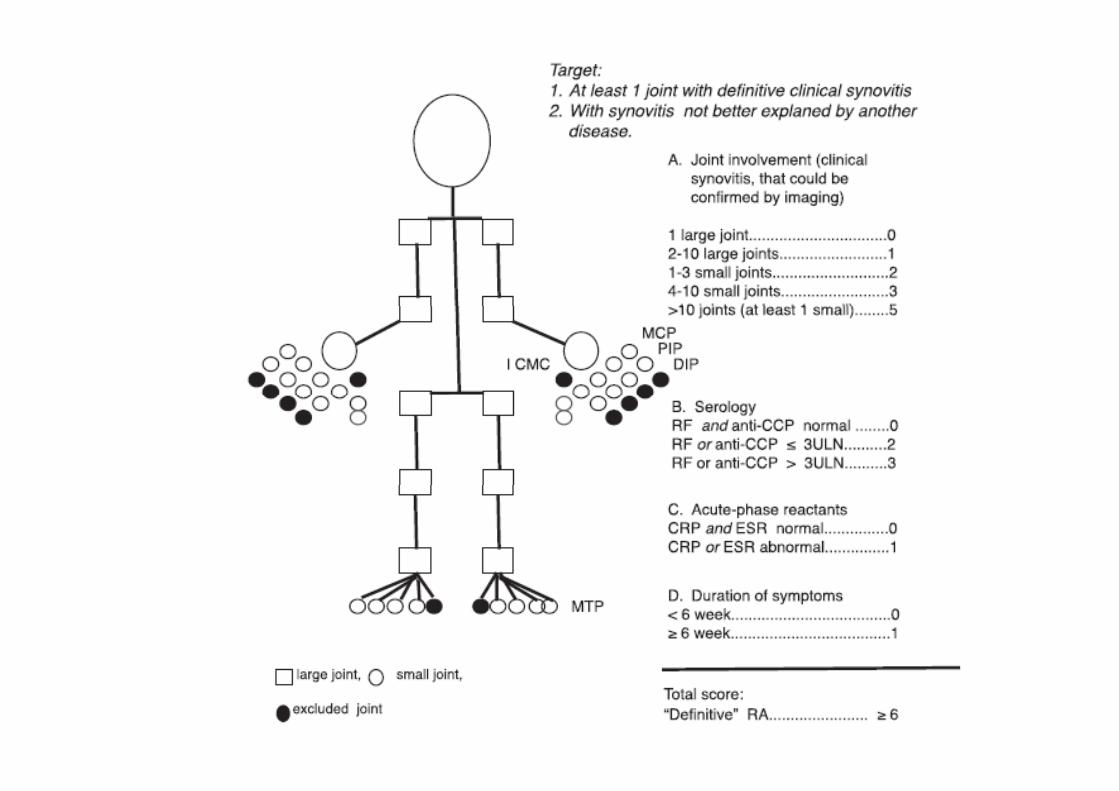
Rheumatoid arthritis (RA)Rheumatoid arthritis (RA)
• A progressive immune‐mediated disease involving the synovium that can culminate in joint destruction, significant functional impairment, and early mortality.
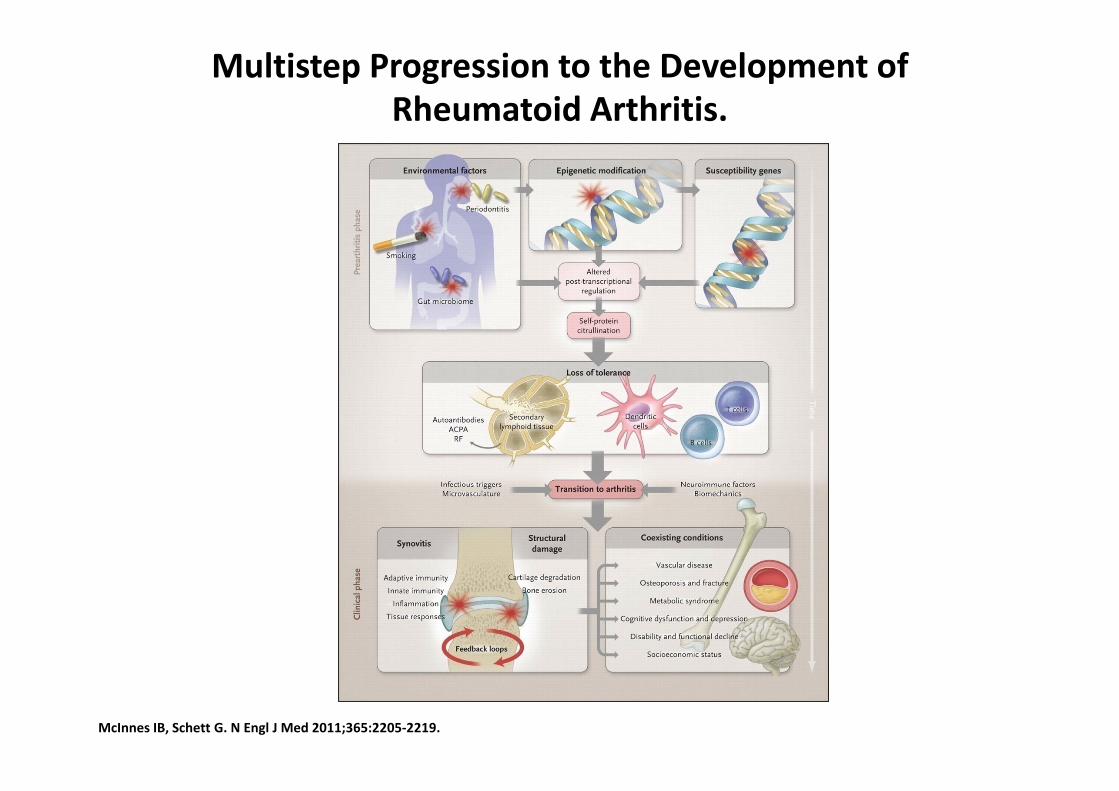
Multistep Progression to the Development of Rheumatoid Arthritis.
McInnes IB, Schett G. N Engl J Med 2011;365:2205‐2219.
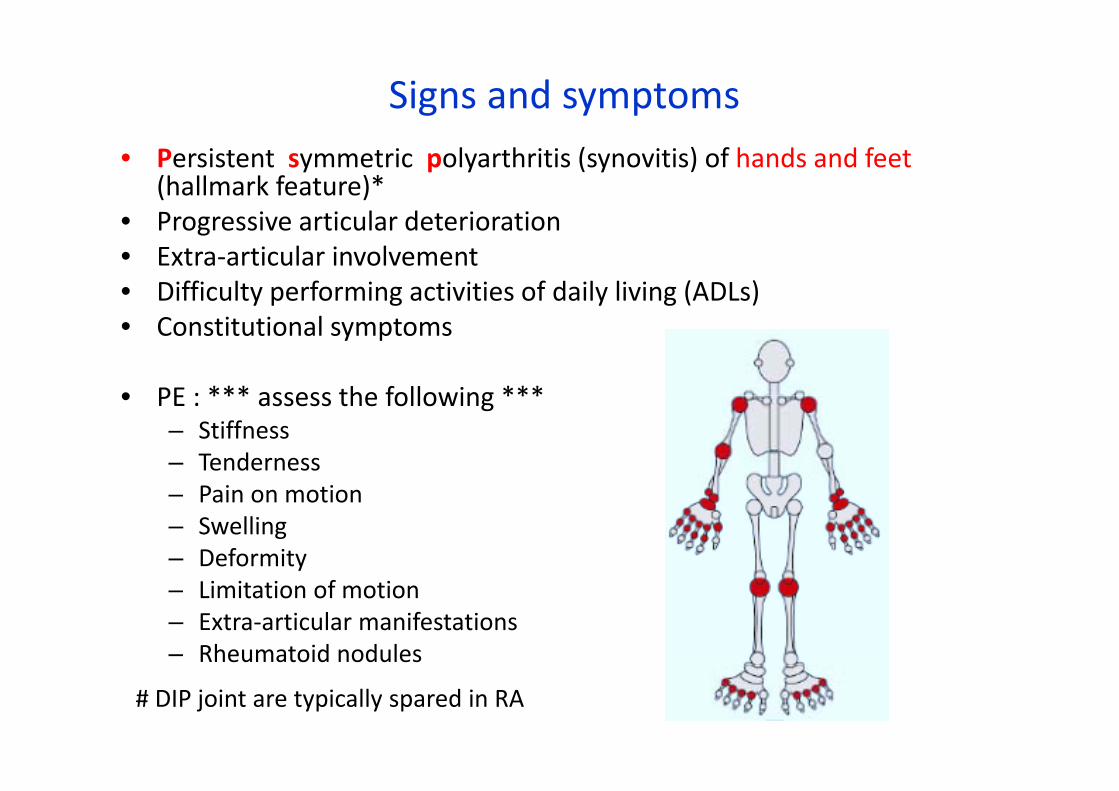
Signs and symptoms• Persistent symmetric polyarthritis (synovitis) of hands and feet
(hallmark feature)* P i ti l d t i ti• Progressive articular deterioration
• Extra‐articular involvement • Difficulty performing activities of daily living (ADLs) • Constitutional symptoms
• PE : *** assess the following ***• PE : *** assess the following ***– Stiffness – Tenderness
i i– Pain on motion – Swelling – Deformity – Limitation of motion – Extra‐articular manifestations – Rheumatoid nodules
# DIP joint are typically spared in RA


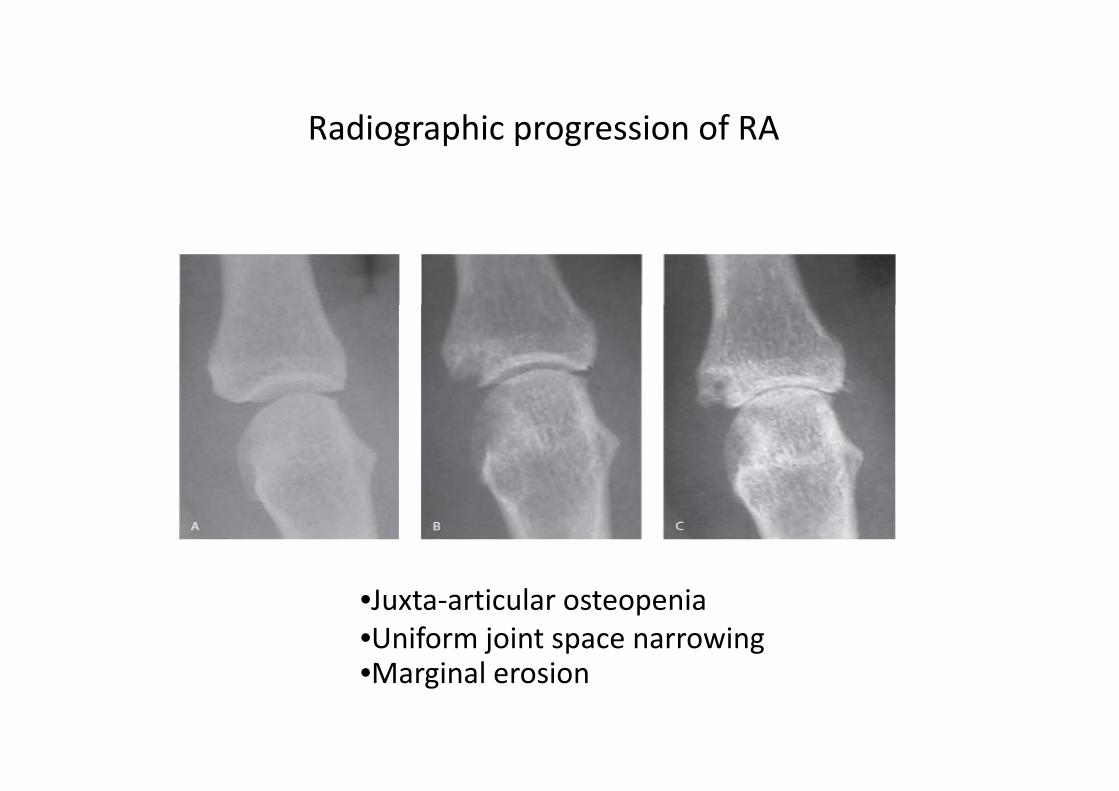
Radiographic progression of RARadiographic progression of RA
•Juxta‐articular osteopenia•Uniform joint space narrowingM i l i•Marginal erosion

Extra‐articular manifestationExtra‐articular manifestation
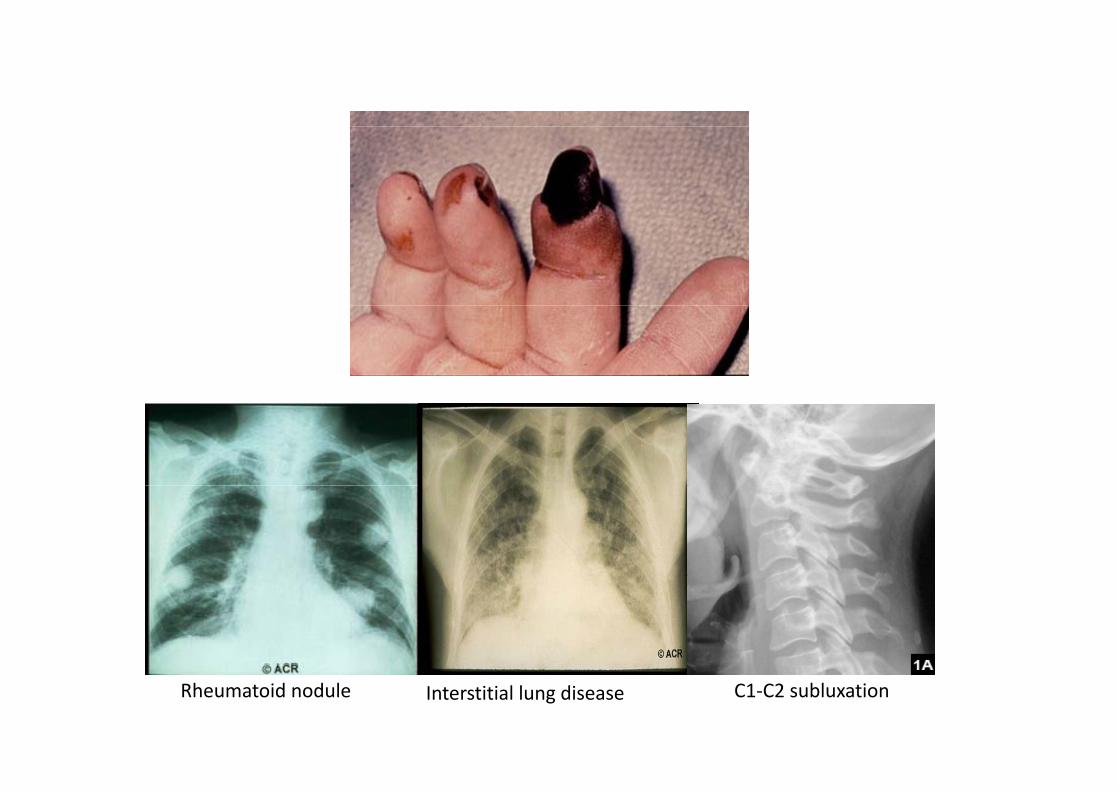
Rheumatoid nodule Interstitial lung disease C1‐C2 subluxation
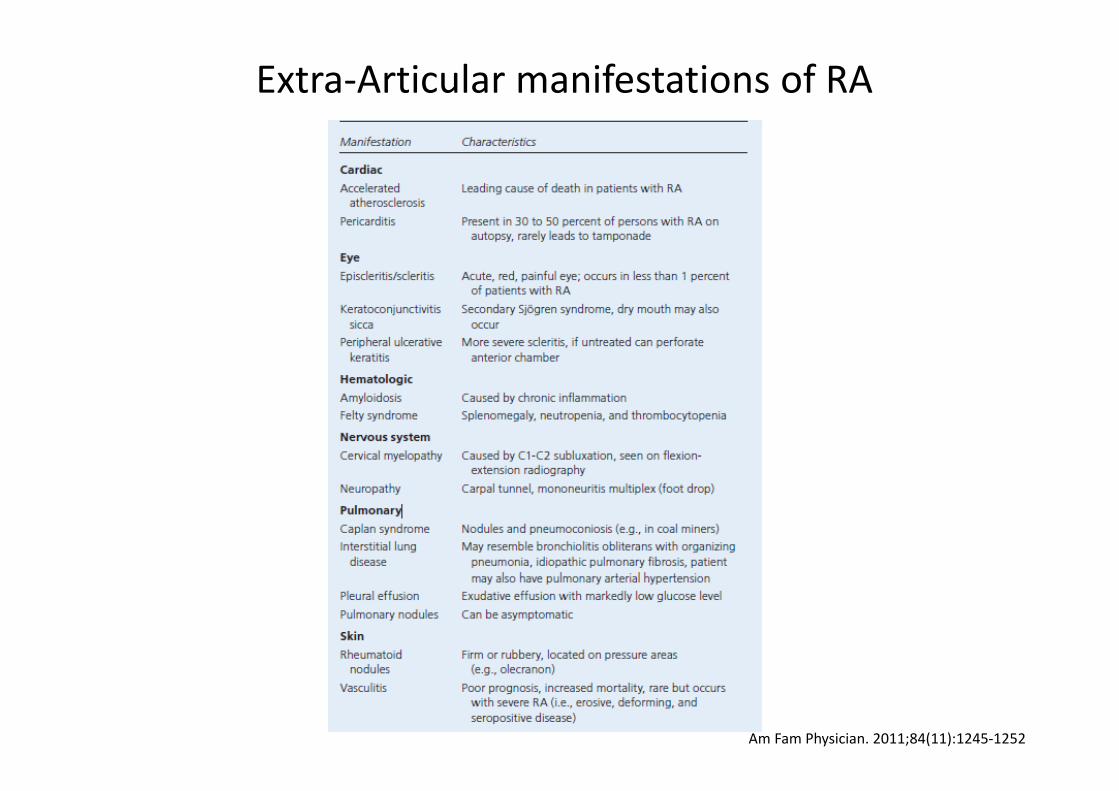
Extra‐Articular manifestations of RA
Am Fam Physician. 2011;84(11):1245‐1252

Rheumatoid factor (RF)Rheumatoid factor (RF)Rheumatoid factor (RF)Rheumatoid factor (RF)
• Autoantibodies reactive with epitopes in the Fc portion of IgG
• 70% of patients with RA have RF positive • The titer does NOT correlate with disease activity• High titer RF are more likely to have erosive joint disease more• High titer RF are more likely to have erosive joint disease, more
radiographic abnormalities, extra‐articularmanifestations, and greater functional disability
• Not specific for RA : chronic infections, cirrhosis, malignancy, and other rheumatic diseaseand other rheumatic disease
l• Female 40 years
• 8 weeks, joint pain and morning stiffness 60 min.
• Arthritis of Lt wrists all Rt PIP and MCP jointsArthritis of Lt. wrists, all Rt. PIP and MCP joints
• No rheumatoid nodule
ESR 60 /h• ESR 60 mm/hr
• Film hands : periarticular osteopenia, no erosion
• RF negative
ANTI–CYCLIC CITRULLINATED PEPTIDE ANTI–CYCLIC CITRULLINATED PEPTIDE (Anti CCP) (Anti CCP)
• sensitivity 70‐80%, specificity 95‐98%*** (more than RF)
• Anti CCP
present in early disease
highly specific for rheumatoid arthritis
predict development of more‐erosive RA
• anti‐CCP could be detected in variety of diseases




















