Embed Size (px)
Citation preview
FINAL
Deliverable D9.1
Common Data Set and disease-, treatment and other specific modules.
I-Report on the survey on Common Data Elements
Emanuela Mollo, Sabina Gainotti, Luciano Vittozzi, Domenica Taruscio
National Centre for Rare Diseases, National Institute of Health, Rome (Italy)
FINAL
2
CONTENTS
Acknowledgements ............................................................................................. 3
Overview of the documents produced by EPIRARE ............................................... 4
Disclaimer ............................................................................................................ 4
ACRONYMS .......................................................................................................... 5
Executive Summary .............................................................................................. 6
I. Background .................................................................................................... 7
II. Methodology ................................................................................................. 7
III. Results and Discussion ................................................................................... 8
A. The sample of responding registries ..................................................................................................... 8
B. Descriptive analysis of data collection practices .................................................................................. 8
1. Patient’s identifiers and patient unique coding ................................................................................ 8
2. Other information on the patient ................................................................................................... 11
3. Data on centres .............................................................................................................................. 12
4. History of diagnosis ........................................................................................................................ 12
5. Disease coding systems .................................................................................................................. 14
6. Clinical and genetic data ................................................................................................................. 15
7. Data on treatments ........................................................................................................................ 16
8. Disability and quality of life ............................................................................................................ 18
9. Data on donations of biological material ........................................................................................ 19
C. Pre-determined platform indicators, other outputs and their feasibility ........................................... 19
1. Indicators of RD morbidity and mortality ....................................................................................... 20
2. Indicators of socio-economic impact .............................................................................................. 21
1. Indicators of (availability of appropriate) Health Services .............................................................. 21
2. Indicators for information, research and technology development ............................................... 24
3. Indicators on equity and EU initiatives and other indicators based on registry data ...................... 25
IV. Conclusions .................................................................................................. 25
TABLES .............................................................................................................. 26
Table 1 – Selected platform indicators and measures, with the combinations of data elements considered necessary to calculate them ....................................................................................................................... 26
Appendix 1 ........................................................................................................ 29
The questionnaire (separate PDF document) ............................................................................................. 29
APPENDIX 2 ....................................................................................................... 30
List of registries that participated in the EPIRARE Survey on Common Data Elements .............................. 30
FINAL
3
Acknowledgements
The Authors wish to acknowledge the important collaboration provided by the experts who commented and tested the questionnaire and the registry holders who participated in the second EPIRARE survey answering the questionnaire. The list of these experts and the registries which they represent, which is given in Appendix 2, is not only to provide information on the composition of the registry sample which has been analyzed, but rather to witness their essential contribution for casting the information which is presented in this Report.
FINAL
4
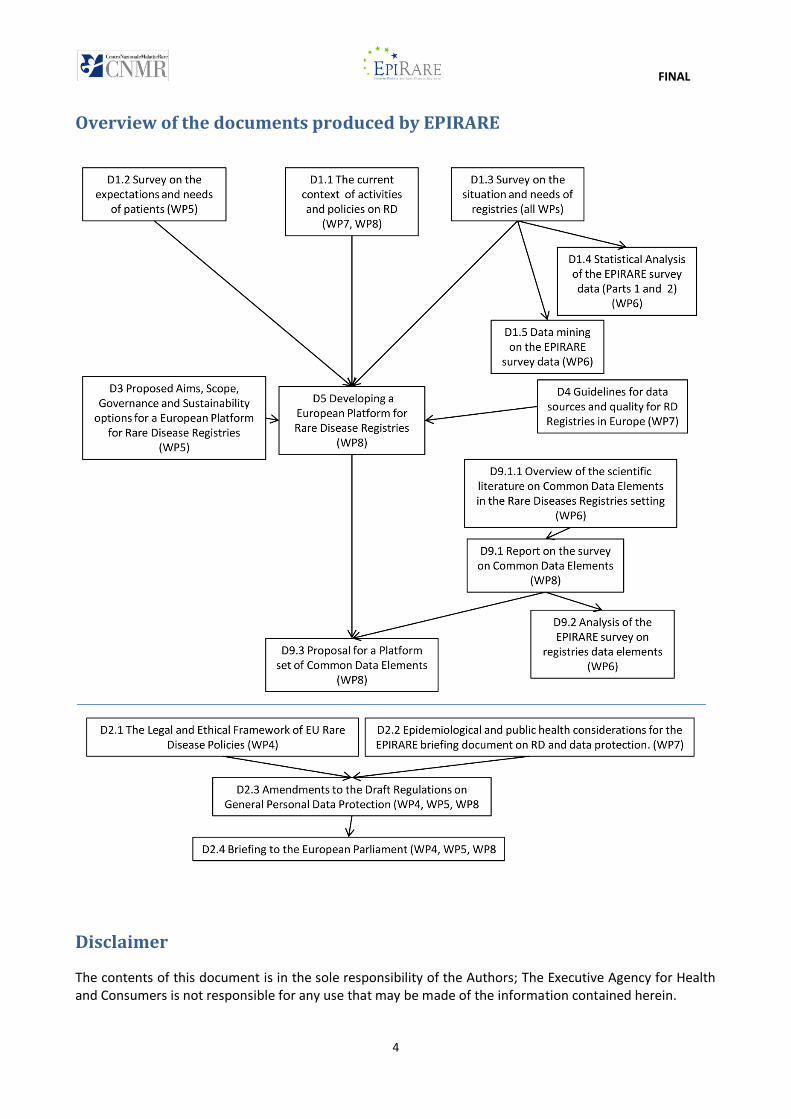
Overview of the documents produced by EPIRARE
Disclaimer
The contents of this document is in the sole responsibility of the Authors; The Executive Agency for Health and Consumers is not responsible for any use that may be made of the information contained herein.
FINAL
5
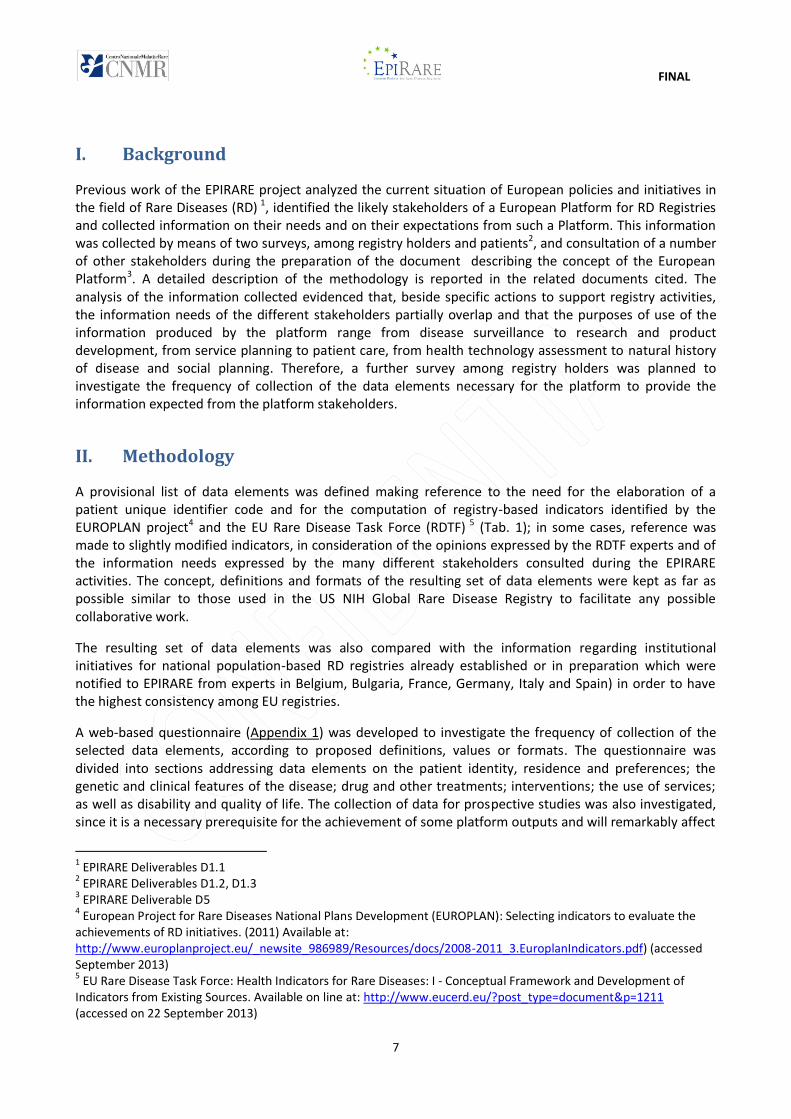
ACRONYMS
Acronym Meaning
GUID Global Unique Identifier
GUIDWS Global Unique Identifyer Web Service for GUID assignement
RD Rare diseases
HGNC HUGO Gene Nomenclature Committee
HGVS Human Genome Variation Society
OD Orphan Drug
ICF International Classification of Functioning, Disability and Health
HRQoL Health Related Quality of Life

FINAL
6
Executive Summary
This report deals with the results of a survey inquiring on the frequency of collection of the data elements necessary for the platform to provide the information expected from the platform stakeholders. The registries replying to the survey were 156, of which 147 were considered valid. The data elements in the scope of the survey related to patient identifiers and other patient information, data on centres which made diagnosis or treating the patient, history of diagnosis, clinical and genetic data, treatments, disability and quality of life, donations. The results obtained were also used to calculate the frequency of the combinations of data elements necessary for the calculation of relevant indicators in the area of RD morbility and mortality, socio-economic impact, health services, research and development, equity.
The results of this survey indicate that the RD patient registration practices currently on-going in the EU are suitable to cover most aspects related to rare disease information and care and show that most registries are ready or can be adapted to use common definitions, values and formats for many relevant rare disease patient data. Information on the use of common coding systems, reference terminologies and questionnaires show a rather fragmented picture and suggesting that the adoption of common reference instruments will impact on most registries.
FINAL
7
I. Background
Previous work of the EPIRARE project analyzed the current situation of European policies and initiatives in the field of Rare Diseases (RD) 1, identified the likely stakeholders of a European Platform for RD Registries and collected information on their needs and on their expectations from such a Platform. This information was collected by means of two surveys, among registry holders and patients2, and consultation of a number of other stakeholders during the preparation of the document describing the concept of the European Platform3. A detailed description of the methodology is reported in the related documents cited. The analysis of the information collected evidenced that, beside specific actions to support registry activities, the information needs of the different stakeholders partially overlap and that the purposes of use of the information produced by the platform range from disease surveillance to research and product development, from service planning to patient care, from health technology assessment to natural history of disease and social planning. Therefore, a further survey among registry holders was planned to investigate the frequency of collection of the data elements necessary for the platform to provide the information expected from the platform stakeholders.
II. Methodology
A provisional list of data elements was defined making reference to the need for the elaboration of a patient unique identifier code and for the computation of registry-based indicators identified by the EUROPLAN project4 and the EU Rare Disease Task Force (RDTF) 5 (Tab. 1); in some cases, reference was made to slightly modified indicators, in consideration of the opinions expressed by the RDTF experts and of the information needs expressed by the many different stakeholders consulted during the EPIRARE activities. The concept, definitions and formats of the resulting set of data elements were kept as far as possible similar to those used in the US NIH Global Rare Disease Registry to facilitate any possible collaborative work.
The resulting set of data elements was also compared with the information regarding institutional initiatives for national population-based RD registries already established or in preparation which were notified to EPIRARE from experts in Belgium, Bulgaria, France, Germany, Italy and Spain) in order to have the highest consistency among EU registries.
A web-based questionnaire (Appendix 1) was developed to investigate the frequency of collection of the selected data elements, according to proposed definitions, values or formats. The questionnaire was divided into sections addressing data elements on the patient identity, residence and preferences; the genetic and clinical features of the disease; drug and other treatments; interventions; the use of services; as well as disability and quality of life. The collection of data for prospective studies was also investigated, since it is a necessary prerequisite for the achievement of some platform outputs and will remarkably affect
1 EPIRARE Deliverables D1.1 2 EPIRARE Deliverables D1.2, D1.3 3 EPIRARE Deliverable D5 4 European Project for Rare Diseases National Plans Development (EUROPLAN): Selecting indicators to evaluate the achievements of RD initiatives. (2011) Available at: http://www.europlanproject.eu/_newsite_986989/Resources/docs/2008-2011_3.EuroplanIndicators.pdf) (accessed September 2013) 5 EU Rare Disease Task Force: Health Indicators for Rare Diseases: I - Conceptual Framework and Development of Indicators from Existing Sources. Available on line at: http://www.eucerd.eu/?post_type=document&p=1211 (accessed on 22 September 2013)
FINAL
8
the data repository organization. It was tested with a few registrars and then a list of 624 registries, made up with the registries invited to the first EPIRARE survey and the new entries in the 2013 update of the ORPHANET Report on Disease Registries in Europe, were invited by e-mail to fill in the questionnaire during the period from 1st March to 15th April 2013. The EPI-Info software was used to calculate the frequency of collection of data elements, individually or in combination.
III. Results and Discussion
A. The sample of responding registries
The registries replying to the survey were 156 (Appendix 2), of which 147 were considered valid answers; 113 registries were part of a network and 31 single-centre registries (three responders did not answered this question). Beside a number of cancer networks, 65 RD networks were represented in the sample; of these, 39 networks had a national dimension. Treat-NMD was represented with 19 registries, EuroCAT was represented with 10 registries, the Italian National RD Registry and the Spanish National RDR were represented with 6 and 5 regional registries, respectively. Fifty networks were represented by only one registry each.
Seventy-three registries addressed one to three named diseases, 62 collected data from groups of related diseases, including congenital anomalies (10 registries), neuromuscular diseases (8 registries) and cancers (7 registries); finally there were 12 health authorities-supported registries addressing very broad collections: 5 Spanish regional registries and 1 national registry (Finland) collecting data on all rare diseases diagnosed, and 6 Italian regional/national registries collecting data on a selection of diseases belonging to 14 ICD-9-CM groups of diseases, encompassing a non exhaustive list of 496 named diseases. All registries collected the name of the diagnosed disease.
The availability of longitudinal observations is critical to get important information of interest to the registry stakeholders. Therefore, a section of the questionnaire was dedicated to get detailed information on the existing practice of longitudinal collection of these data elements. Overall, regularly updated information able to support prospective data collections was collected by 92 registries, and additional 31 registries could be adapted to collect longitudinal data. Therefore, a rather high fraction of the responding registries was able to provide some kind of information during the patient life.
In the next chapters, the availability of longitudinal collections are presented in the figures near to the corresponding data on the frequency of the data element collection.
B. Descriptive analysis of data collection practices
1. Patient’s identifiers and patient unique coding
Johnson et al6, in their paper presenting a study for the definition of a Global Unique Identifier (GUID) and proposing a web service (GUIDWS) for its definition related to the National Database for Autism Research, assessed the performances of a number of combinations of different pieces of information related to the patient. The combination made of the first and last names, complete additional legal name or names at birth, if any (such as a middle name), gender, day of birth and month of birth, all mandatory fields for the patient record, has been considered the most suitable to strike a balance between prevention of false identities (a sufficient number of elements are required, which are collected at a very high degree of
6 Stephen B Johnson, Glen Whitney, Matthew McAuliffe, Hailong Wang, Evan McCreedy, Leon Rozenblit, Clark C Evans (2010) Using global unique identifiers to link autism collections. J Am Med Inform Assoc 2010;17:689e695;
FINAL
9
completeness) and the prevention of false splits (the data elements can be collected with sufficient accuracy to allow matching).
In the EU there are a number of activities developing in the area of eHealth studying the feasibility of patient identification and authentication in the context of the on-line and cross-border provision of health services. These initiatives aim at mainly addressing technological solutions for health service provision across EU. A preliminary goal for the provision of these services is the validation of the identity of a remote “customer”. Although this goal is rather different from the registry platform aim of attributing the same univocal code to the same person whose data are collected in different places, interesting information can be found in a report produced within the framework of the STORK project7. Here, a mapping has been carried out of the identifier data used by Identity Providers delegated by the EU governments to issue electronic identities (eID). Although there might be Country differences in the legal provisions and in operative details for the use of this eID data, the results, regarding the situation at July 2010 of the 17 MS and 1 candidate Country (Iceland) investigated, indicate that the first name, last name, date of birth and a national identification code are present in all eID data sets; the gender is contained in 14 eID data sets; and residence address, nationality and the place of birth (sometimes just the Country of birth) is present in 10 eID data sets.
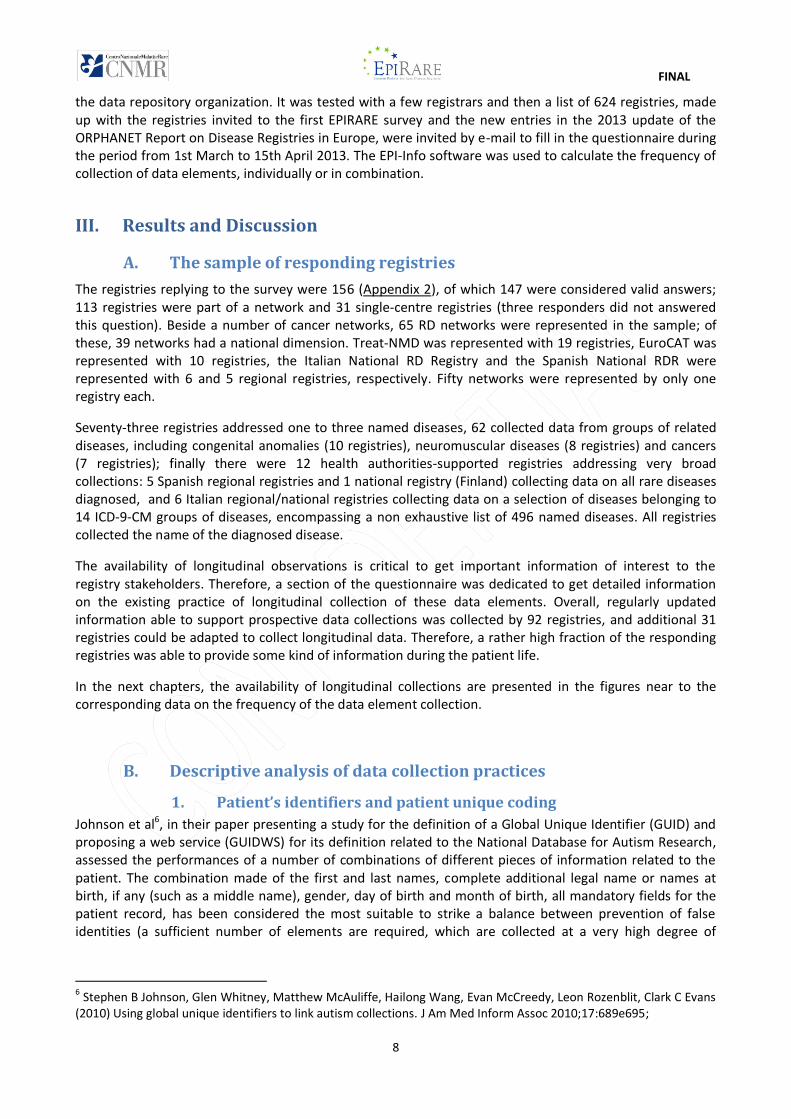
Figure 1 – The patient identifiers and the National Social Security Code
The EPIRARE survey therefore inquired on the most commonly used data in EU or recommended by Johnson et al6 (Fig. 1). The sex8 and date of birth9 were or could be collected by almost all registries, i.e., respectively, 142 and 138 registries out of 147.
7 Jan Eichholz, Adrian Johnston, Herbert Leitold, Marc Stern, John Heppe, Tim Schneider, Bernd Zwattendorfer (2010) D5.1 Evaluation and assessment of existing reference models and common specs. Available on-line at: https://www.eid-stork.eu/index.php?option=com_processes&act=list_documents&s=1&Itemid=60&id=312 [accessed on 10 August 2013]. 8 DEFINITION: "Patient's physical sex at birth"; PERMISSIBLE VALUES: male, female, other (in any format)
FINAL
10
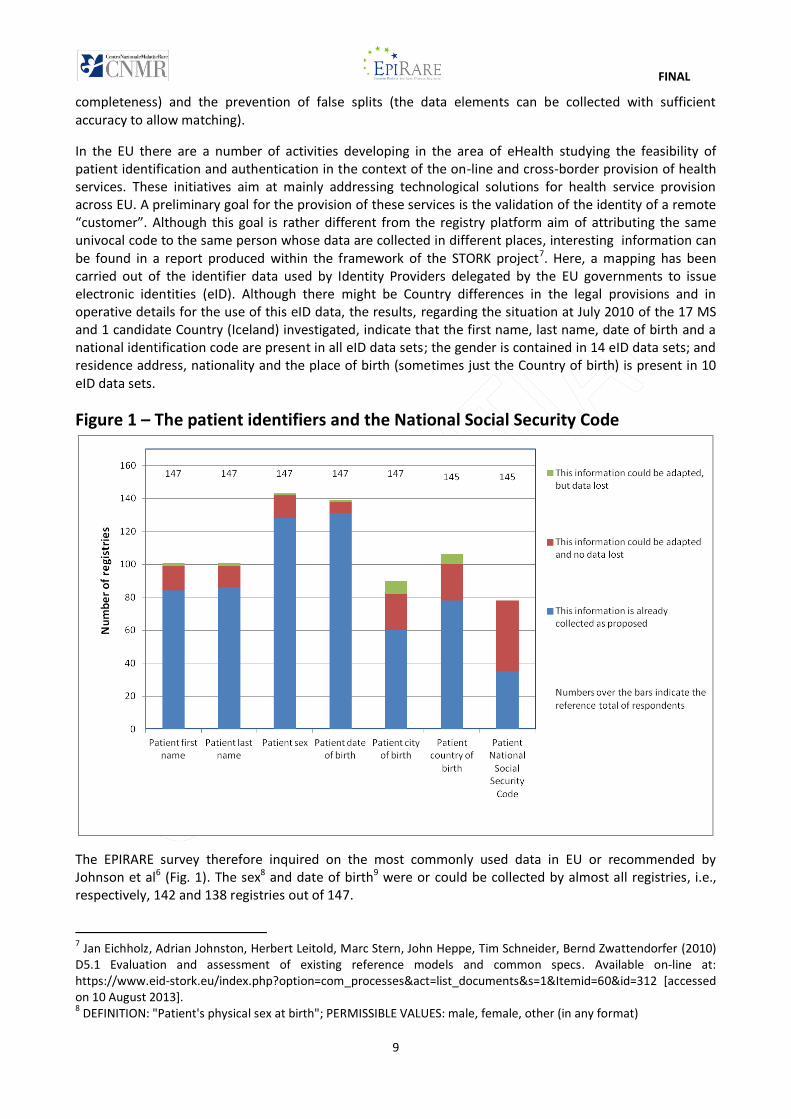
The data least frequently collected according to the proposed format was the city of birth (60 registries) with additional 22 registries, which could adapt their data to this request and further 8, which could adapt with loss of the data already collected. The set of three variables patient’s first name10, surname11 and date of birth9 was currently collected by 83 registries(Fig. 2); the addition of the variable sex8 makes the set collected by 77 registries; however, if the registries which could be adapted to collect these variables are considered in addition, these sets could be collected by 101 registries, (in 2 or 3 registries data already collected will not be compatible). Out of these 101 registries, only 69 collected, or could collect, also the patient’s city of birth12.
The addition of the country of birth13, collected as such or inferred by the city name, does not affect further this number. The collection of the country of birth has been investigated to assess the feasibility to differentiate among cities, which can have the same name in different countries, and could be necessary in the case that data of patients from different continents are merged.
A minority of registries declared to collect the National Social Security Code (35); considering also those which could collect it, this number was increased to 78 registries.
Figure 2 – The feasibility of a Global Unique Identification Code in EU registries14
It is likely that many EU registries avoid the collection of patients identifiers because of compliance with the data protection regulations applying in EU countries. It can be expected that a higher fraction, or even the
9 DEFINITION: "Date of patient's birth recorded in birth certificate, passport or identity card"; FORMAT: complete date (year, month, day) in any format 10 DEFINITION: "First name of patient as recorded in birth certificate, passport or identity card"; FORMAT: full name, not initials 11 DEFINITION: "Last name of patient as recorded in birth certificate, passport or identity card"; FORMAT: full name, not initials 12 DEFINITION: "Name of city/town/village where the patient was born as it appears on the birth certificate, passport or identity card"; FORMAT: full name of city 13 DEFINITION: "Name of country where the patient was born as it appears on the birth certificate, passport or identity card"; FORMAT: full name of country 14 According to the GUID elements identified by Johnson et al (reference 1)
FINAL
11
totality, of registries based on primary sources may collect the full set of the data elements required for univocal patient coding when a GUIDWS, which is devised to be compliant with EU personal data protection rules, would be made available to EU registries. In any case, it is important to recommend that these data elements are collected systematically by all registries or by their data sources (i.e.: not necessarily collected in the central registry database), since the univocal coding of patients is a prerequisite for any merging of data from different registries.
It is to be highlighted that the accuracy of recording of the identifiers recommended by Johnson et al6 may be an issue in the EU context, where different languages, alphabets (latin, greek and cirillic) and character variants exist and could be recorded inaccurately in countries different from the country of origin of the patient. Therefore, the possibility of taking advantage of the patient identification mechanisms being developed in the area of eHealth should not be precluded. Therefore, it should also be recommended that the national identification code be collected by the registry data sources and kept locally until the appropriate mechanism complying with the data protection regulations has been devised and approved. Also with the national identification code, provisions should be made to avoid that different codes are used by the same patient, as could be the case of patients who get a second code in the country to which they have migrated.
2. Other information on the patient
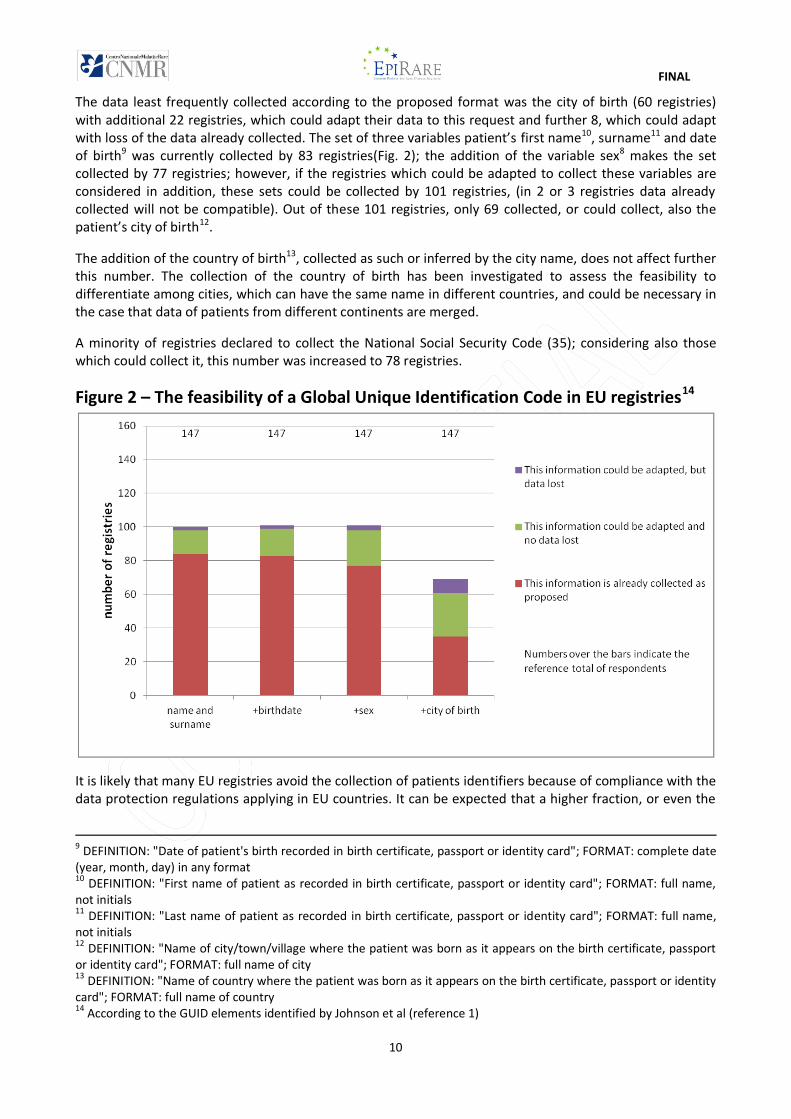
Other data elements regarding the patient, which were collected at rates similar to or higher than the first name, family name and country of birth are the city15 and country16 of residence, date of death17 and other information, stored at central or peripheral registry level, that allows to contact the patient (Fig. 3). It is to
Figure 3 – The collection of demographic and other data of the patient
15 DEFINITION: "Name of city/town where the patient usually lives"; FORMAT: full name of city 16 DEFINITION: "Name of country where the patient usually lives"; FORMAT: full name of country 17 FORMAT: complete date (year, month, day) in any format
FINAL
12
note that information on city and country of residence were updated by the majority of registries collecting this information. The collection of these data should be encouraged since it can be used, beside the calculation of more complex indicators, to analyze different subsets of data referred to the residence of patients.
Information on the patient’s willingness to be contacted for clinical trials or to donate a biospecimen was collected at much lower rates; however, many registries declared that they could be adapted to collect this information, which is rather important for the swift recruitment of patients for research studies.
3. Data on centres
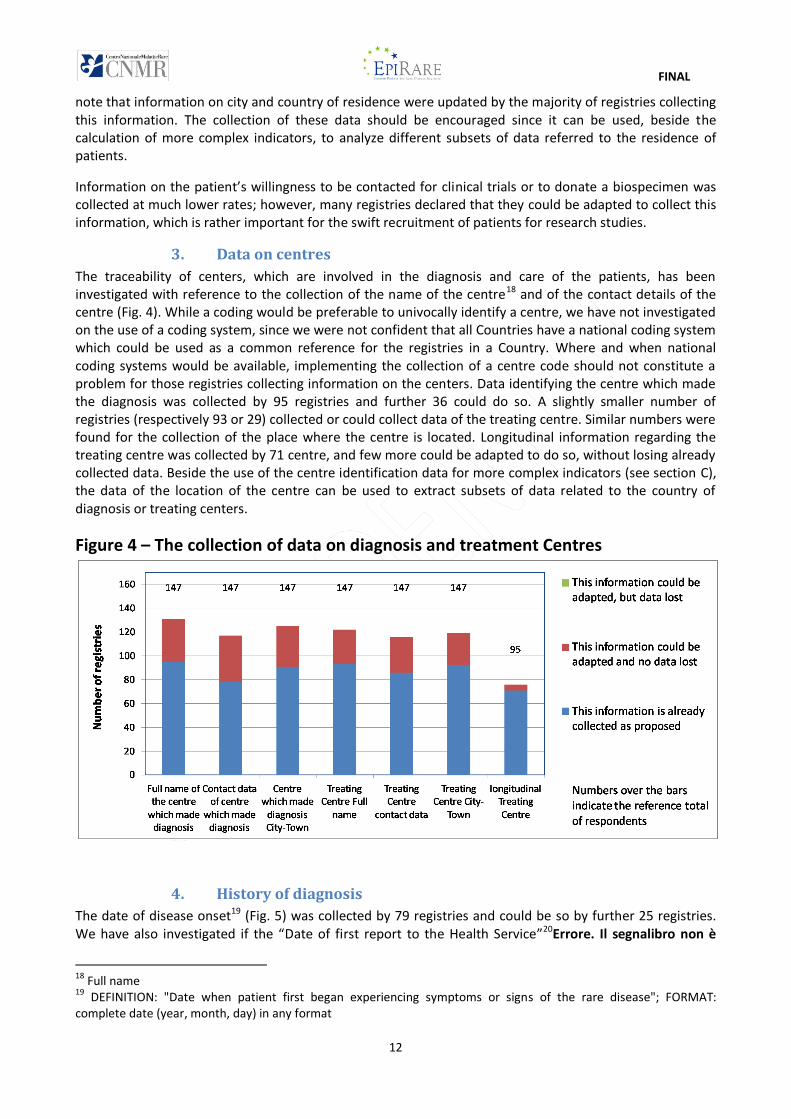
The traceability of centers, which are involved in the diagnosis and care of the patients, has been investigated with reference to the collection of the name of the centre18 and of the contact details of the centre (Fig. 4). While a coding would be preferable to univocally identify a centre, we have not investigated on the use of a coding system, since we were not confident that all Countries have a national coding system which could be used as a common reference for the registries in a Country. Where and when national coding systems would be available, implementing the collection of a centre code should not constitute a problem for those registries collecting information on the centers. Data identifying the centre which made the diagnosis was collected by 95 registries and further 36 could do so. A slightly smaller number of registries (respectively 93 or 29) collected or could collect data of the treating centre. Similar numbers were found for the collection of the place where the centre is located. Longitudinal information regarding the treating centre was collected by 71 centre, and few more could be adapted to do so, without losing already collected data. Beside the use of the centre identification data for more complex indicators (see section C), the data of the location of the centre can be used to extract subsets of data related to the country of diagnosis or treating centers.
Figure 4 – The collection of data on diagnosis and treatment Centres
4. History of diagnosis
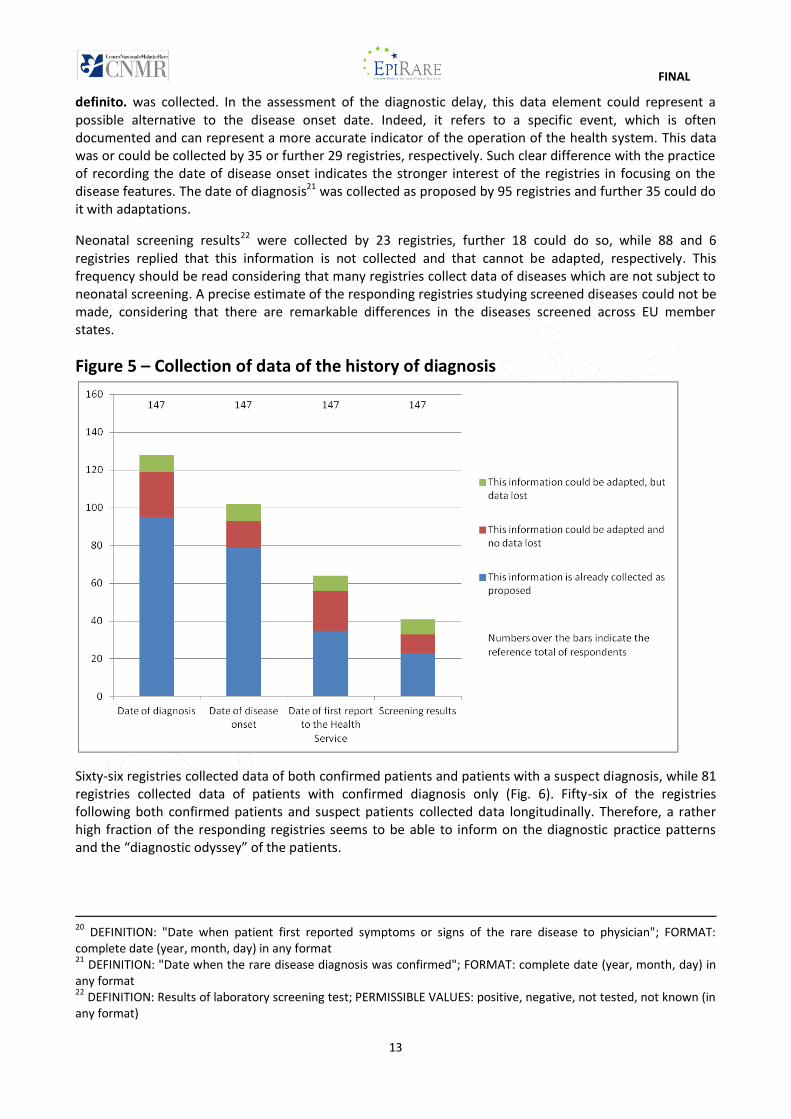
The date of disease onset19 (Fig. 5) was collected by 79 registries and could be so by further 25 registries. We have also investigated if the “Date of first report to the Health Service”20Errore. Il segnalibro non è
18 Full name 19 DEFINITION: "Date when patient first began experiencing symptoms or signs of the rare disease"; FORMAT: complete date (year, month, day) in any format
FINAL
13
definito. was collected. In the assessment of the diagnostic delay, this data element could represent a possible alternative to the disease onset date. Indeed, it refers to a specific event, which is often documented and can represent a more accurate indicator of the operation of the health system. This data was or could be collected by 35 or further 29 registries, respectively. Such clear difference with the practice of recording the date of disease onset indicates the stronger interest of the registries in focusing on the disease features. The date of diagnosis21 was collected as proposed by 95 registries and further 35 could do it with adaptations.
Neonatal screening results22 were collected by 23 registries, further 18 could do so, while 88 and 6 registries replied that this information is not collected and that cannot be adapted, respectively. This frequency should be read considering that many registries collect data of diseases which are not subject to neonatal screening. A precise estimate of the responding registries studying screened diseases could not be made, considering that there are remarkable differences in the diseases screened across EU member states.
Figure 5 – Collection of data of the history of diagnosis
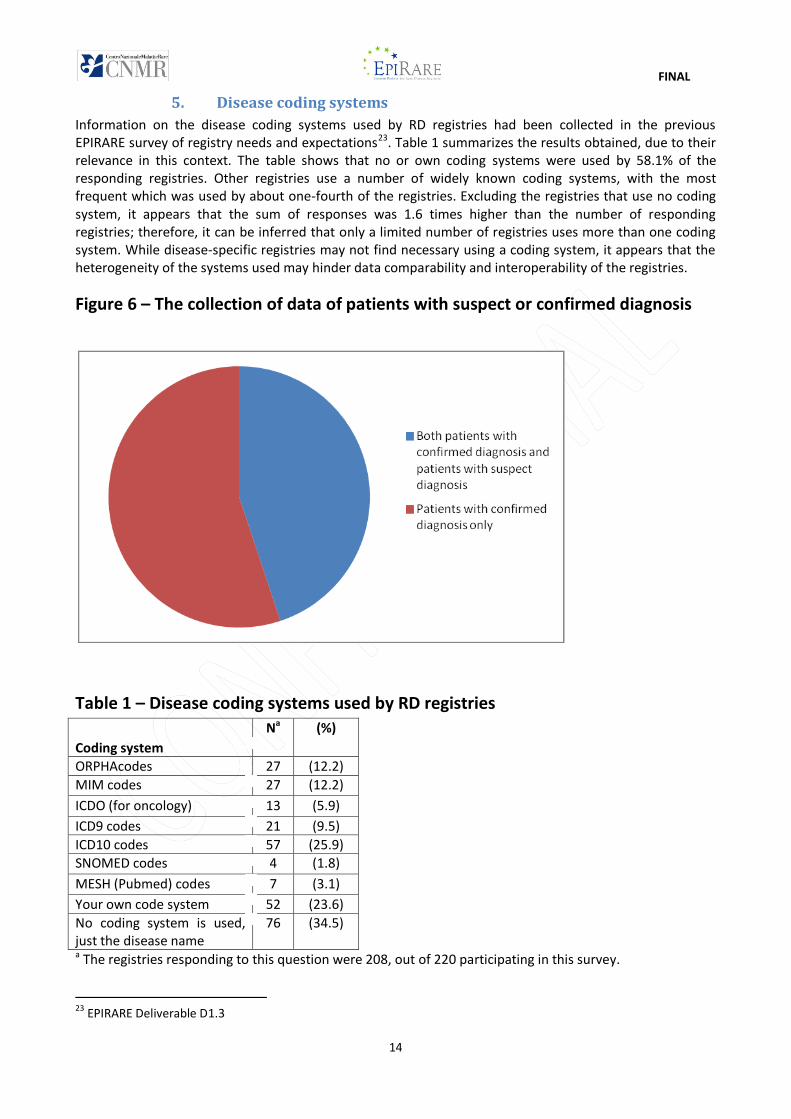
Sixty-six registries collected data of both confirmed patients and patients with a suspect diagnosis, while 81 registries collected data of patients with confirmed diagnosis only (Fig. 6). Fifty-six of the registries following both confirmed patients and suspect patients collected data longitudinally. Therefore, a rather high fraction of the responding registries seems to be able to inform on the diagnostic practice patterns and the “diagnostic odyssey” of the patients.
20 DEFINITION: "Date when patient first reported symptoms or signs of the rare disease to physician"; FORMAT: complete date (year, month, day) in any format 21 DEFINITION: "Date when the rare disease diagnosis was confirmed"; FORMAT: complete date (year, month, day) in any format 22 DEFINITION: Results of laboratory screening test; PERMISSIBLE VALUES: positive, negative, not tested, not known (in any format)
FINAL
14
5. Disease coding systems
Information on the disease coding systems used by RD registries had been collected in the previous EPIRARE survey of registry needs and expectations23. Table 1 summarizes the results obtained, due to their relevance in this context. The table shows that no or own coding systems were used by 58.1% of the responding registries. Other registries use a number of widely known coding systems, with the most frequent which was used by about one-fourth of the registries. Excluding the registries that use no coding system, it appears that the sum of responses was 1.6 times higher than the number of responding registries; therefore, it can be inferred that only a limited number of registries uses more than one coding system. While disease-specific registries may not find necessary using a coding system, it appears that the heterogeneity of the systems used may hinder data comparability and interoperability of the registries.
Figure 6 – The collection of data of patients with suspect or confirmed diagnosis
Table 1 – Disease coding systems used by RD registries
Coding system
Na (%)
ORPHAcodes 27 (12.2)
MIM codes
27 (12.2)
ICDO (for oncology)
13 (5.9)
ICD9 codes 21 (9.5)
ICD10 codes 57 (25.9)
SNOMED codes
4 (1.8)
MESH (Pubmed) codes
7 (3.1)
Your own code system 52 (23.6)
No coding system is used, just the disease name
76 (34.5)
a The registries responding to this question were 208, out of 220 participating in this survey.
23 EPIRARE Deliverable D1.3
FINAL
15
6. Clinical and genetic data
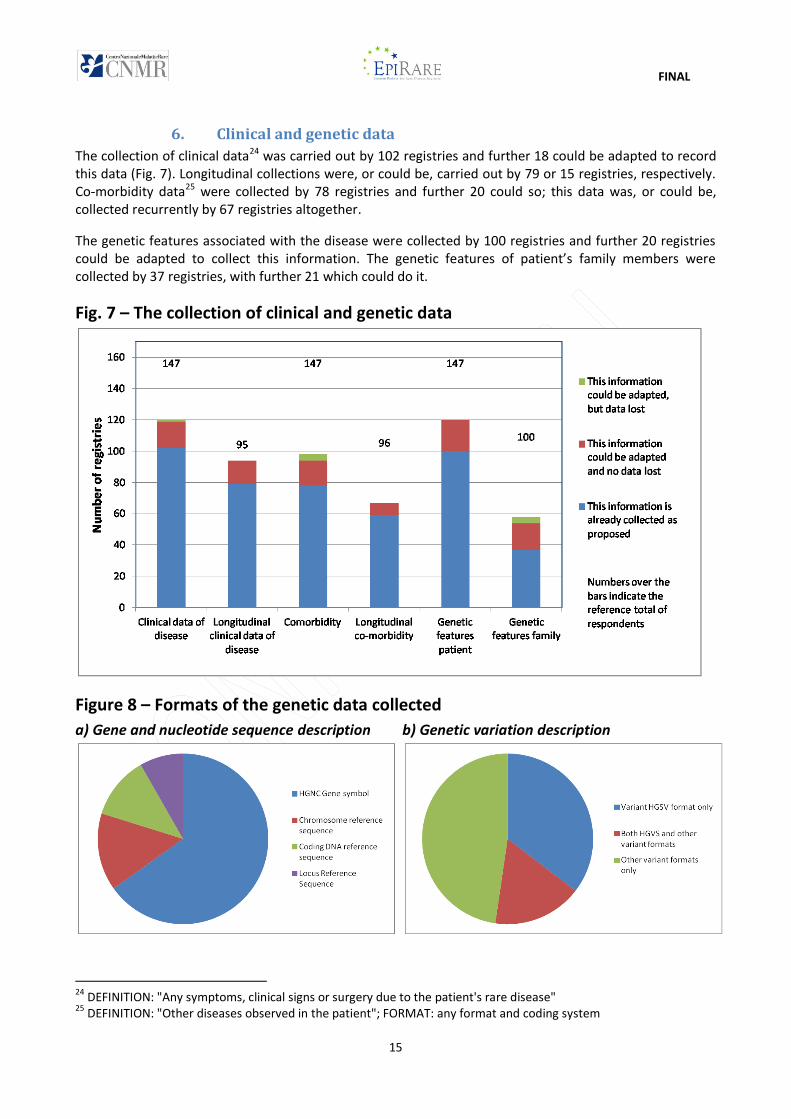
The collection of clinical data24 was carried out by 102 registries and further 18 could be adapted to record this data (Fig. 7). Longitudinal collections were, or could be, carried out by 79 or 15 registries, respectively. Co-morbidity data25 were collected by 78 registries and further 20 could so; this data was, or could be, collected recurrently by 67 registries altogether.
The genetic features associated with the disease were collected by 100 registries and further 20 registries could be adapted to collect this information. The genetic features of patient’s family members were collected by 37 registries, with further 21 which could do it.
Fig. 7 – The collection of clinical and genetic data
Figure 8 – Formats of the genetic data collected
a) Gene and nucleotide sequence description b) Genetic variation description
24 DEFINITION: "Any symptoms, clinical signs or surgery due to the patient's rare disease" 25 DEFINITION: "Other diseases observed in the patient"; FORMAT: any format and coding system
FINAL
16
Out of the 97 registries currently collecting genetic data, the HGNC gene symbol was recorded by 71 registries (Fig. 8a). Twenty-two registries collected nucleotide sequences in at least one of recommended formats (Chromosome reference Sequence; Coding DNA reference sequence; Reference Locus Sequence). The variant description was currently recorded in HGVS format by 34 registries (Fig. 8b), whereas other descriptions were used by 31 registries. From the free text answers (23), it appears that many registries collected information as received by the genetic laboratory, or that they record data of mutations known to be relevant to the disease followed by the registry. Moreover, a few of the registries collecting these data indicated that they were collected if and when available. Therefore it is likely that, at least in some registries, patient records are rather incomplete and not uniform as far as genetic data are concerned.
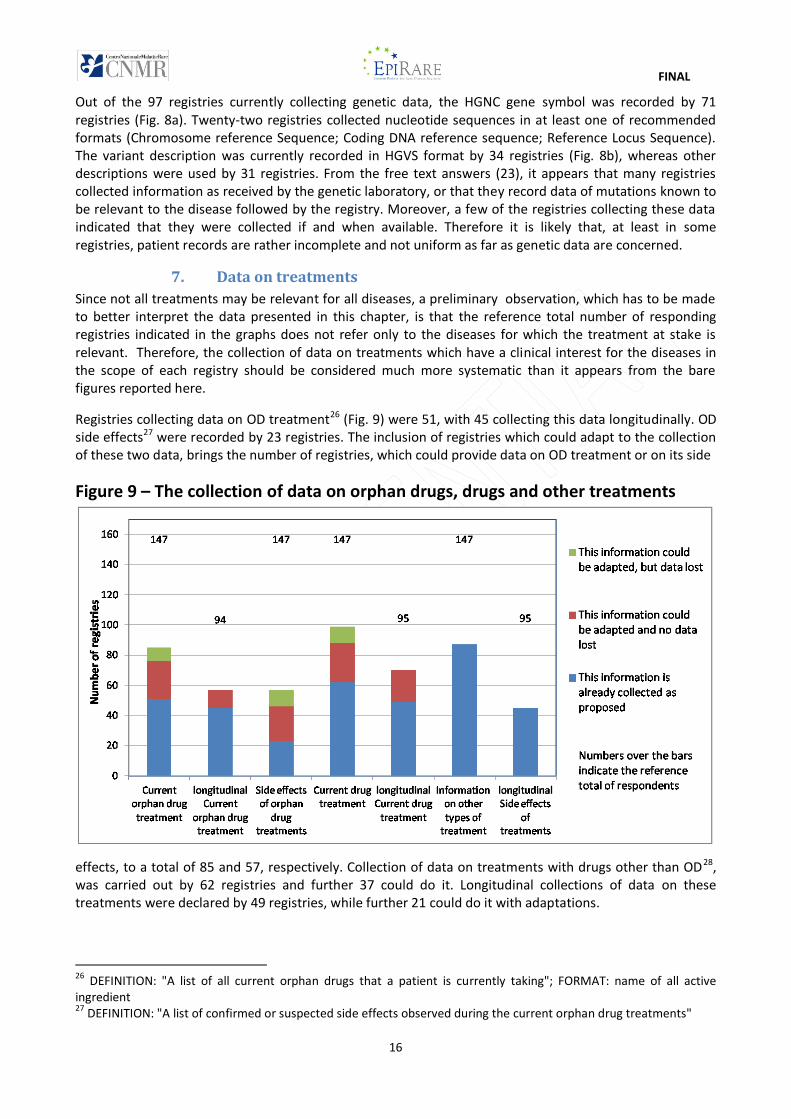
7. Data on treatments
Since not all treatments may be relevant for all diseases, a preliminary observation, which has to be made to better interpret the data presented in this chapter, is that the reference total number of responding registries indicated in the graphs does not refer only to the diseases for which the treatment at stake is relevant. Therefore, the collection of data on treatments which have a clinical interest for the diseases in the scope of each registry should be considered much more systematic than it appears from the bare figures reported here.
Registries collecting data on OD treatment26 (Fig. 9) were 51, with 45 collecting this data longitudinally. OD side effects27 were recorded by 23 registries. The inclusion of registries which could adapt to the collection of these two data, brings the number of registries, which could provide data on OD treatment or on its side
Figure 9 – The collection of data on orphan drugs, drugs and other treatments
effects, to a total of 85 and 57, respectively. Collection of data on treatments with drugs other than OD28, was carried out by 62 registries and further 37 could do it. Longitudinal collections of data on these treatments were declared by 49 registries, while further 21 could do it with adaptations.
26 DEFINITION: "A list of all current orphan drugs that a patient is currently taking"; FORMAT: name of all active ingredient 27 DEFINITION: "A list of confirmed or suspected side effects observed during the current orphan drug treatments"
FINAL
17
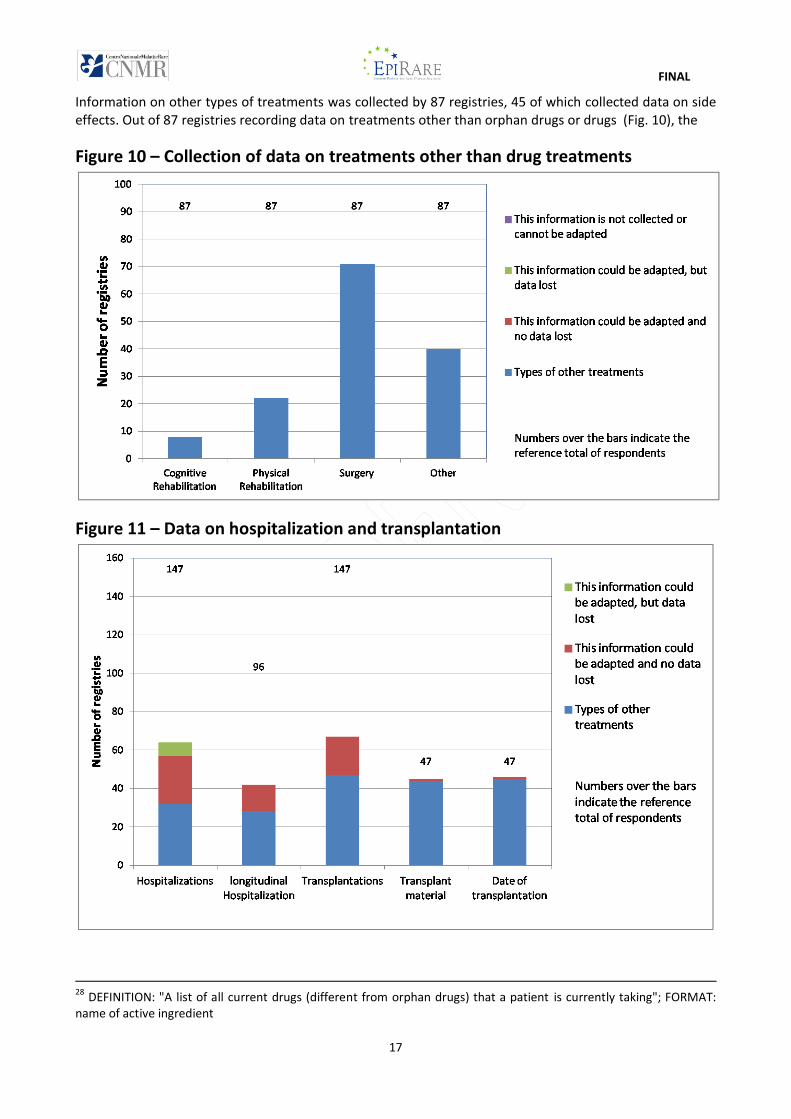
Information on other types of treatments was collected by 87 registries, 45 of which collected data on side effects. Out of 87 registries recording data on treatments other than orphan drugs or drugs (Fig. 10), the
Figure 10 – Collection of data on treatments other than drug treatments
Figure 11 – Data on hospitalization and transplantation
28 DEFINITION: "A list of all current drugs (different from orphan drugs) that a patient is currently taking"; FORMAT: name of active ingredient
FINAL
18
majority (71) referred to surgeries, while 22 and 8 referred, respectively to physical and cognitive rehabilitation. Other treatments (specified in free text) were recorded by 39 registries. The most frequent answer given to specify the type of “other treatment” they observed, referred to transplantations (15 registries), which was the subject of a dedicated group of questions (see here below). Other treatments, such as nutritional care/assisted feeding, cardiac pacing, respiratory assistance, gene therapy, radio- or chemo- therapy, were indicated by no more than 3-4 registries each. One registry collected data of all classified procedures made in the inpatient and outpatient specialized care.
The questionnaire inquired also on the practice of recording information on hospitalizations and transplantations. Figure 11 indicates that 32 registries currently collected data of hospitalization; they could be nearly doubled (57) considering those that could adapt to collect this data. Almost all (28) of these registries did it longitudinally, and further 14 could be adapted to collect hospitalization data longitudinally.
Registries collecting data on transplantations were 47 and they could become 67 considering those that could collect this information. Almost all registries interested in transplantations collected data on transplant material and on the date of transplantation.
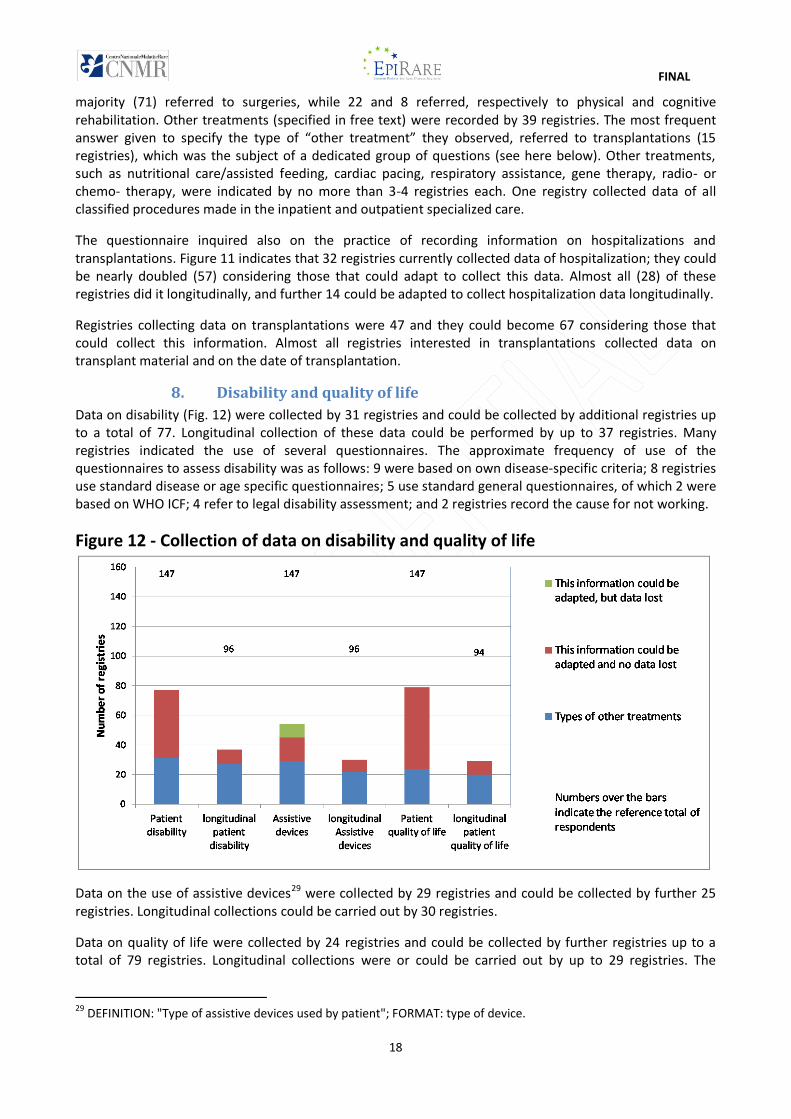
8. Disability and quality of life
Data on disability (Fig. 12) were collected by 31 registries and could be collected by additional registries up to a total of 77. Longitudinal collection of these data could be performed by up to 37 registries. Many registries indicated the use of several questionnaires. The approximate frequency of use of the questionnaires to assess disability was as follows: 9 were based on own disease-specific criteria; 8 registries use standard disease or age specific questionnaires; 5 use standard general questionnaires, of which 2 were based on WHO ICF; 4 refer to legal disability assessment; and 2 registries record the cause for not working.
Figure 12 - Collection of data on disability and quality of life
Data on the use of assistive devices29 were collected by 29 registries and could be collected by further 25 registries. Longitudinal collections could be carried out by 30 registries.
Data on quality of life were collected by 24 registries and could be collected by further registries up to a total of 79 registries. Longitudinal collections were or could be carried out by up to 29 registries. The
29 DEFINITION: "Type of assistive devices used by patient"; FORMAT: type of device.
FINAL
19
questionnaires indicated by these registries were: EQ-5D30 (4 registries); SF-3631 (5 registries); PedsQL32, WHOQOL-BREF33, and Kidscreen-1034 (2 registries each); other questionnaires were disease specific or indicated by one registry only.
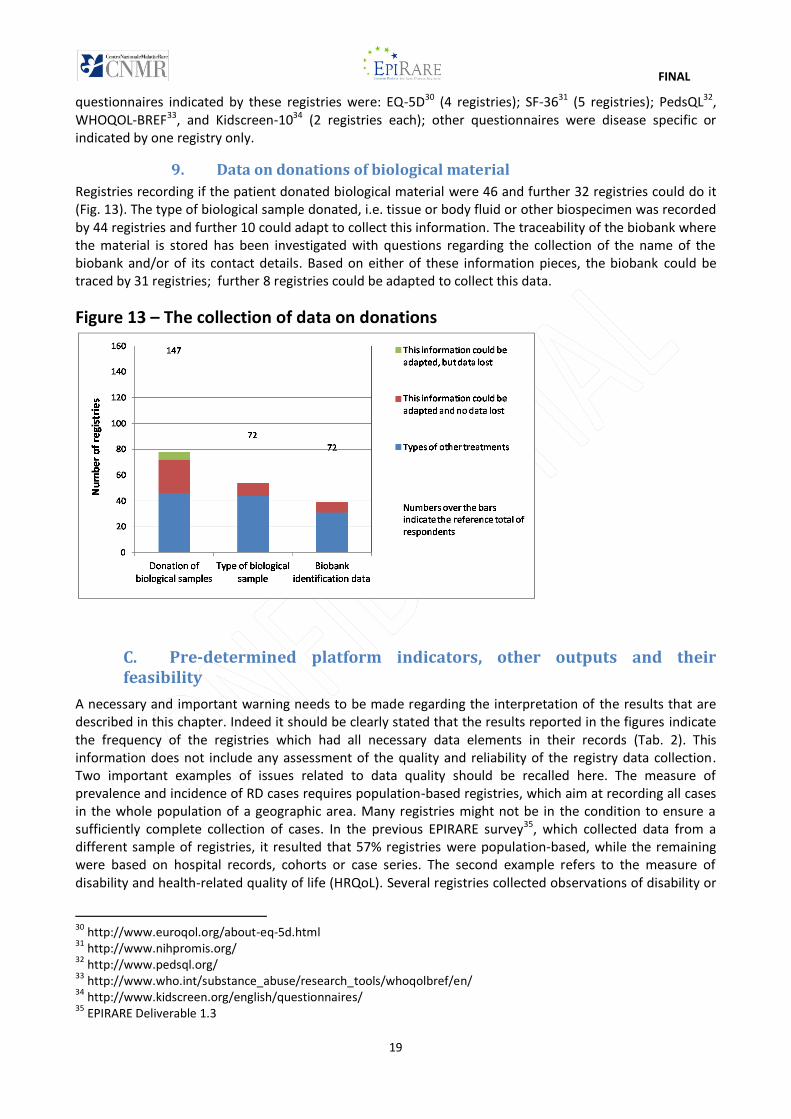
9. Data on donations of biological material
Registries recording if the patient donated biological material were 46 and further 32 registries could do it (Fig. 13). The type of biological sample donated, i.e. tissue or body fluid or other biospecimen was recorded by 44 registries and further 10 could adapt to collect this information. The traceability of the biobank where the material is stored has been investigated with questions regarding the collection of the name of the biobank and/or of its contact details. Based on either of these information pieces, the biobank could be traced by 31 registries; further 8 registries could be adapted to collect this data.
Figure 13 – The collection of data on donations
C. Pre-determined platform indicators, other outputs and their feasibility
A necessary and important warning needs to be made regarding the interpretation of the results that are described in this chapter. Indeed it should be clearly stated that the results reported in the figures indicate the frequency of the registries which had all necessary data elements in their records (Tab. 2). This information does not include any assessment of the quality and reliability of the registry data collection. Two important examples of issues related to data quality should be recalled here. The measure of prevalence and incidence of RD cases requires population-based registries, which aim at recording all cases in the whole population of a geographic area. Many registries might not be in the condition to ensure a sufficiently complete collection of cases. In the previous EPIRARE survey35, which collected data from a different sample of registries, it resulted that 57% registries were population-based, while the remaining were based on hospital records, cohorts or case series. The second example refers to the measure of disability and health-related quality of life (HRQoL). Several registries collected observations of disability or
30 http://www.euroqol.org/about-eq-5d.html 31 http://www.nihpromis.org/ 32 http://www.pedsql.org/ 33 http://www.who.int/substance_abuse/research_tools/whoqolbref/en/ 34 http://www.kidscreen.org/english/questionnaires/ 35 EPIRARE Deliverable 1.3
FINAL
20
of quality of life. However, many of them did not use standard tools. As a consequence no information was available to EPIRARE to assess the validity and comparability of the data collected.
In order to have results with general applicability it is necessary to assure that registries, altogether, are able to collect data from all patients or at least from groups of patients representative of the whole population of patient with a disease. The use of standard tools is also important for the comparability of results. The actions to improve the completeness of data collection, their comparability and the general applicability of the results are largely out of the control of individual registries. The European Platform can contribute to the achievement of more reliable and accurate results by promoting standardization of tools, comparing data obtained by independent collections, facilitating the use of data from different sources, including the promotion of patient registration and its quality, or, where possible, by merging comparable data from different registries. However, these issues should be brought to the attention of the national authorities, for them to consider the possibility and use of adopting dedicated policy measures assuring the completeness of patient registration and accuracy in the estimation of the reference population and use of same standards.
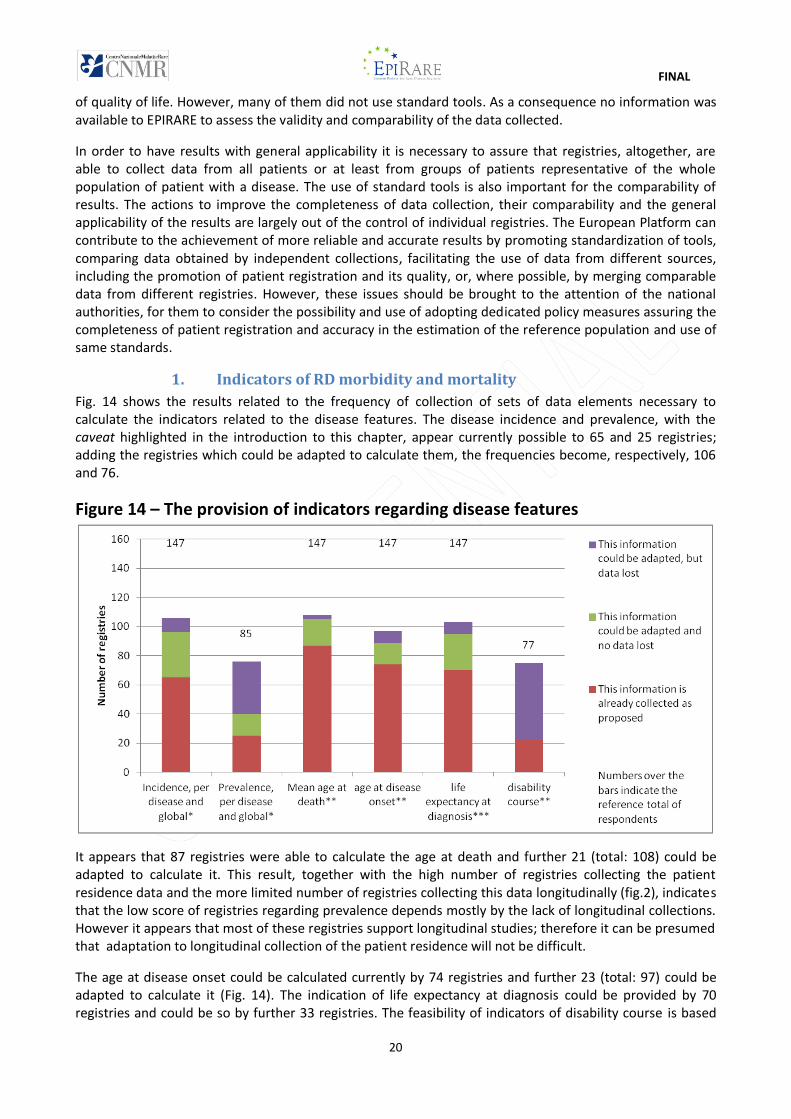
1. Indicators of RD morbidity and mortality
Fig. 14 shows the results related to the frequency of collection of sets of data elements necessary to calculate the indicators related to the disease features. The disease incidence and prevalence, with the caveat highlighted in the introduction to this chapter, appear currently possible to 65 and 25 registries; adding the registries which could be adapted to calculate them, the frequencies become, respectively, 106 and 76.
Figure 14 – The provision of indicators regarding disease features
It appears that 87 registries were able to calculate the age at death and further 21 (total: 108) could be adapted to calculate it. This result, together with the high number of registries collecting the patient residence data and the more limited number of registries collecting this data longitudinally (fig.2), indicates that the low score of registries regarding prevalence depends mostly by the lack of longitudinal collections. However it appears that most of these registries support longitudinal studies; therefore it can be presumed that adaptation to longitudinal collection of the patient residence will not be difficult.
The age at disease onset could be calculated currently by 74 registries and further 23 (total: 97) could be adapted to calculate it (Fig. 14). The indication of life expectancy at diagnosis could be provided by 70 registries and could be so by further 33 registries. The feasibility of indicators of disability course is based
FINAL
21
on data of registries interested in recording disability in longitudinal studies. No consideration has been given to the heterogeneity of disability questionnaires used. This point is not to be overlooked, but its solution requires an action, which, with the agreement of the registries, is able to promote the adoption of reference disease (group)-specific questionnaires or, in their absence, of a single reference generic questionnaire. The results indicate that 22 registries were ready to provide this information and, remarkably, additional 53 could provide it after adaptation of their procedures.
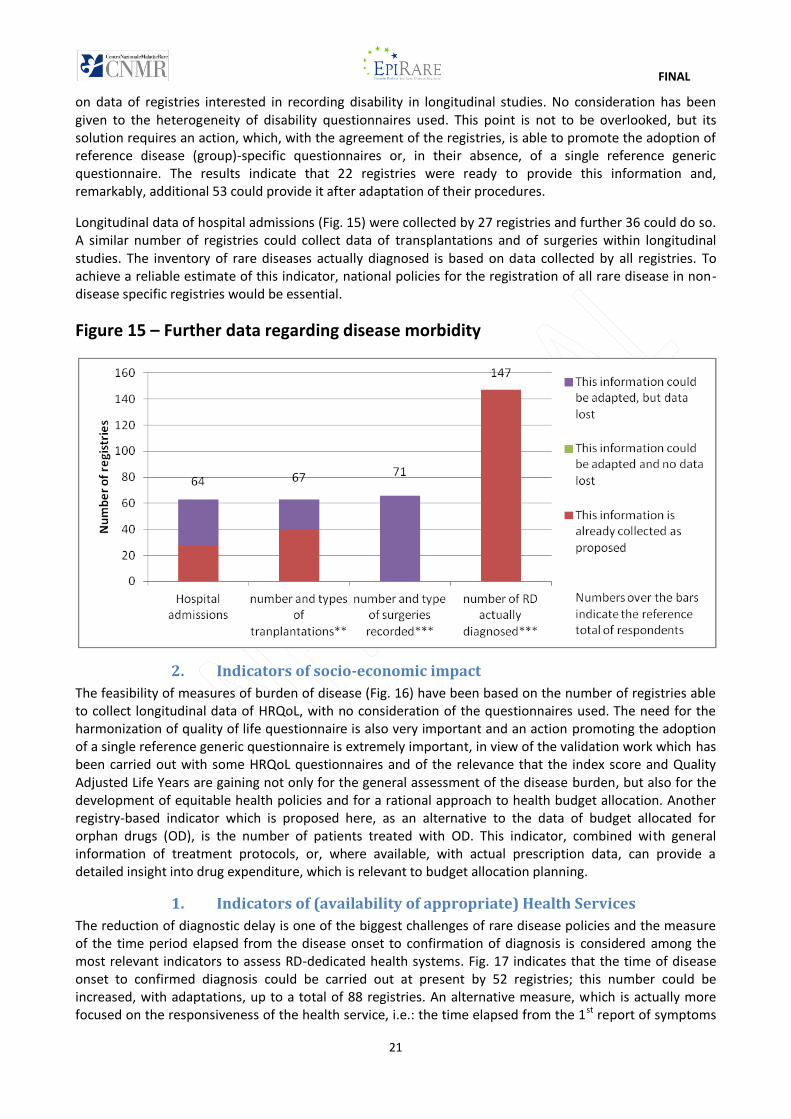
Longitudinal data of hospital admissions (Fig. 15) were collected by 27 registries and further 36 could do so. A similar number of registries could collect data of transplantations and of surgeries within longitudinal studies. The inventory of rare diseases actually diagnosed is based on data collected by all registries. To achieve a reliable estimate of this indicator, national policies for the registration of all rare disease in non-disease specific registries would be essential.
Figure 15 – Further data regarding disease morbidity
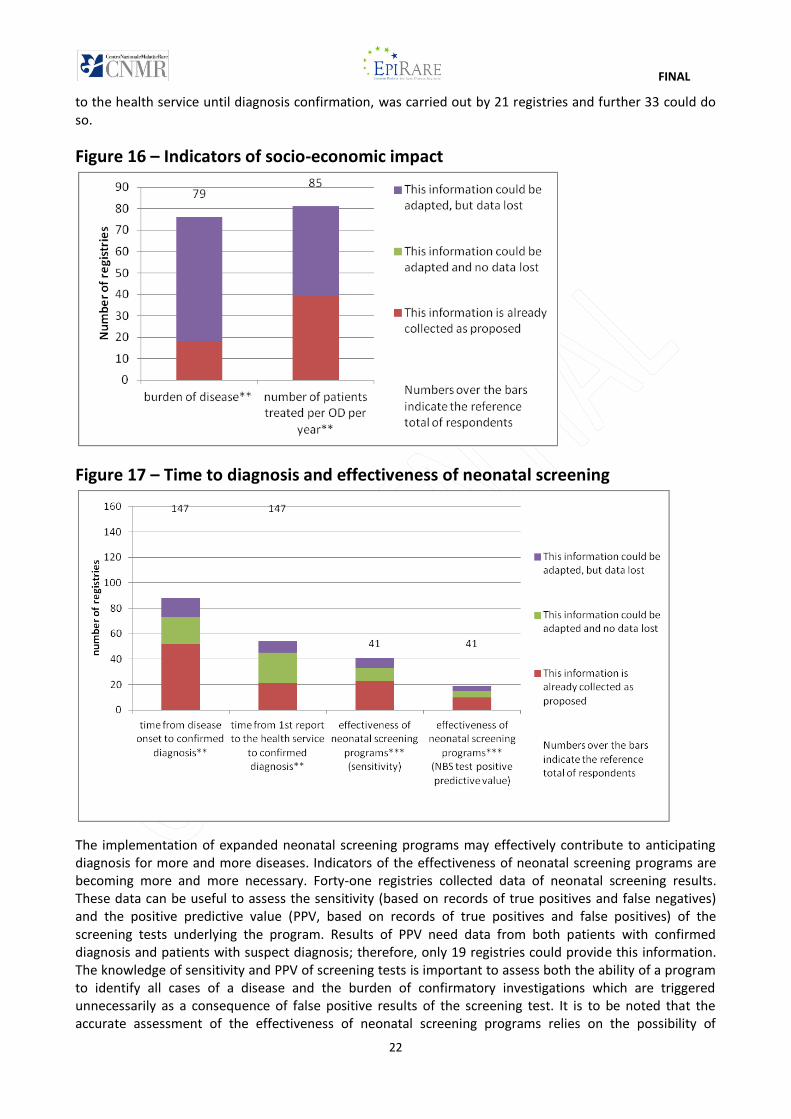
2. Indicators of socio-economic impact
The feasibility of measures of burden of disease (Fig. 16) have been based on the number of registries able to collect longitudinal data of HRQoL, with no consideration of the questionnaires used. The need for the harmonization of quality of life questionnaire is also very important and an action promoting the adoption of a single reference generic questionnaire is extremely important, in view of the validation work which has been carried out with some HRQoL questionnaires and of the relevance that the index score and Quality Adjusted Life Years are gaining not only for the general assessment of the disease burden, but also for the development of equitable health policies and for a rational approach to health budget allocation. Another registry-based indicator which is proposed here, as an alternative to the data of budget allocated for orphan drugs (OD), is the number of patients treated with OD. This indicator, combined with general information of treatment protocols, or, where available, with actual prescription data, can provide a detailed insight into drug expenditure, which is relevant to budget allocation planning.
1. Indicators of (availability of appropriate) Health Services
The reduction of diagnostic delay is one of the biggest challenges of rare disease policies and the measure of the time period elapsed from the disease onset to confirmation of diagnosis is considered among the most relevant indicators to assess RD-dedicated health systems. Fig. 17 indicates that the time of disease onset to confirmed diagnosis could be carried out at present by 52 registries; this number could be increased, with adaptations, up to a total of 88 registries. An alternative measure, which is actually more focused on the responsiveness of the health service, i.e.: the time elapsed from the 1st report of symptoms
FINAL
22
to the health service until diagnosis confirmation, was carried out by 21 registries and further 33 could do so.
Figure 16 – Indicators of socio-economic impact
Figure 17 – Time to diagnosis and effectiveness of neonatal screening
The implementation of expanded neonatal screening programs may effectively contribute to anticipating diagnosis for more and more diseases. Indicators of the effectiveness of neonatal screening programs are becoming more and more necessary. Forty-one registries collected data of neonatal screening results. These data can be useful to assess the sensitivity (based on records of true positives and false negatives) and the positive predictive value (PPV, based on records of true positives and false positives) of the screening tests underlying the program. Results of PPV need data from both patients with confirmed diagnosis and patients with suspect diagnosis; therefore, only 19 registries could provide this information. The knowledge of sensitivity and PPV of screening tests is important to assess both the ability of a program to identify all cases of a disease and the burden of confirmatory investigations which are triggered unnecessarily as a consequence of false positive results of the screening test. It is to be noted that the accurate assessment of the effectiveness of neonatal screening programs relies on the possibility of
FINAL
23
recording this information from all cases in a population which underwent confirmatory investigations for screened RDs. Ensuring an exhaustive recording of cases is not in the reach of individual registries and policy measures should be considered.
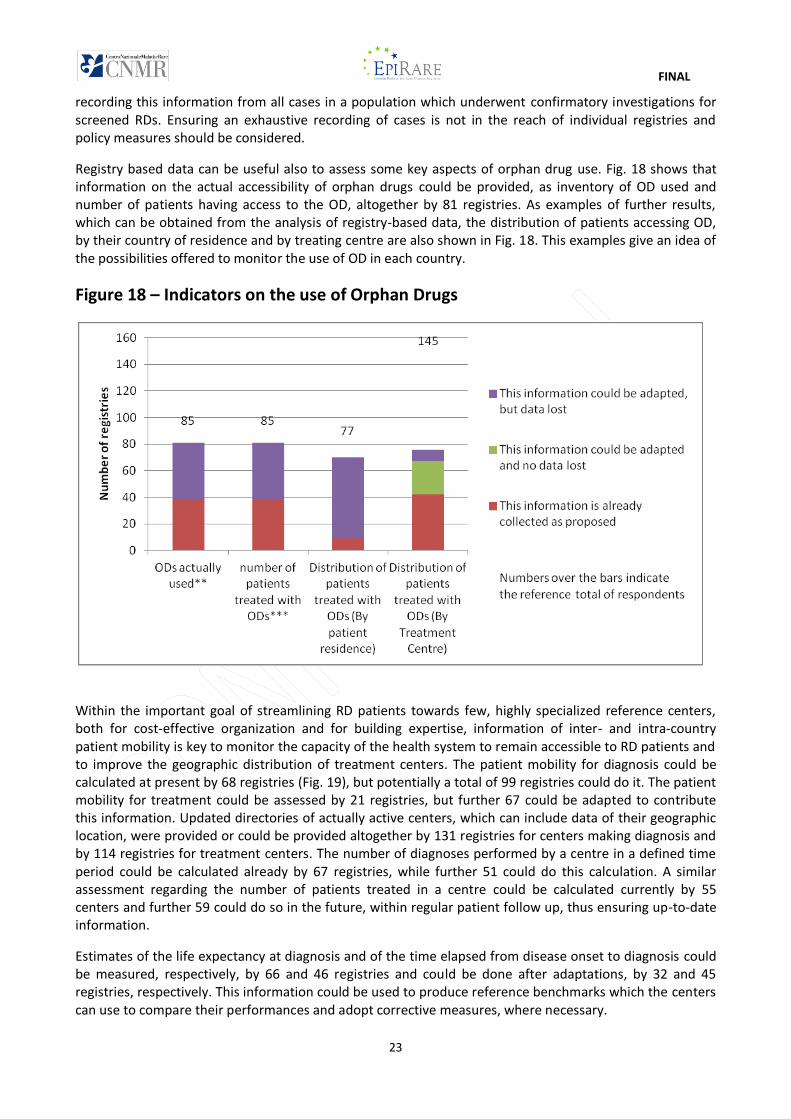
Registry based data can be useful also to assess some key aspects of orphan drug use. Fig. 18 shows that information on the actual accessibility of orphan drugs could be provided, as inventory of OD used and number of patients having access to the OD, altogether by 81 registries. As examples of further results, which can be obtained from the analysis of registry-based data, the distribution of patients accessing OD, by their country of residence and by treating centre are also shown in Fig. 18. This examples give an idea of the possibilities offered to monitor the use of OD in each country.
Figure 18 – Indicators on the use of Orphan Drugs
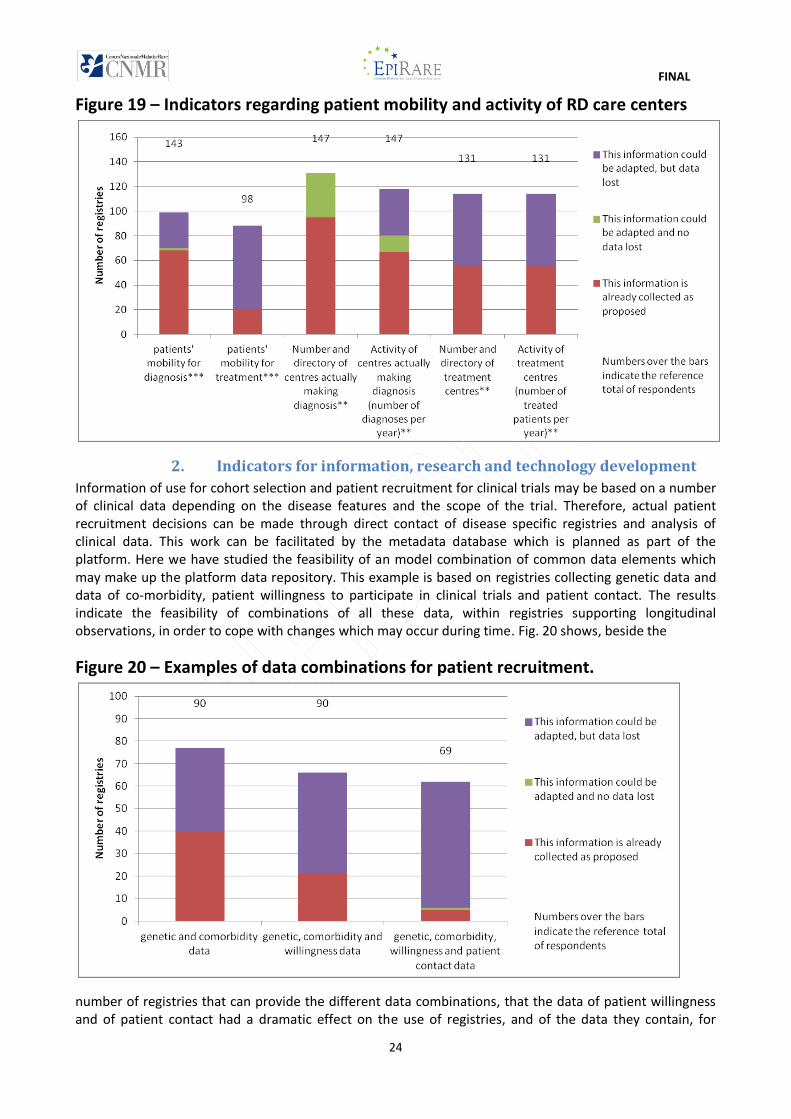
Within the important goal of streamlining RD patients towards few, highly specialized reference centers, both for cost-effective organization and for building expertise, information of inter- and intra-country patient mobility is key to monitor the capacity of the health system to remain accessible to RD patients and to improve the geographic distribution of treatment centers. The patient mobility for diagnosis could be calculated at present by 68 registries (Fig. 19), but potentially a total of 99 registries could do it. The patient mobility for treatment could be assessed by 21 registries, but further 67 could be adapted to contribute this information. Updated directories of actually active centers, which can include data of their geographic location, were provided or could be provided altogether by 131 registries for centers making diagnosis and by 114 registries for treatment centers. The number of diagnoses performed by a centre in a defined time period could be calculated already by 67 registries, while further 51 could do this calculation. A similar assessment regarding the number of patients treated in a centre could be calculated currently by 55 centers and further 59 could do so in the future, within regular patient follow up, thus ensuring up-to-date information.
Estimates of the life expectancy at diagnosis and of the time elapsed from disease onset to diagnosis could be measured, respectively, by 66 and 46 registries and could be done after adaptations, by 32 and 45 registries, respectively. This information could be used to produce reference benchmarks which the centers can use to compare their performances and adopt corrective measures, where necessary.
FINAL
24
Figure 19 – Indicators regarding patient mobility and activity of RD care centers
2. Indicators for information, research and technology development
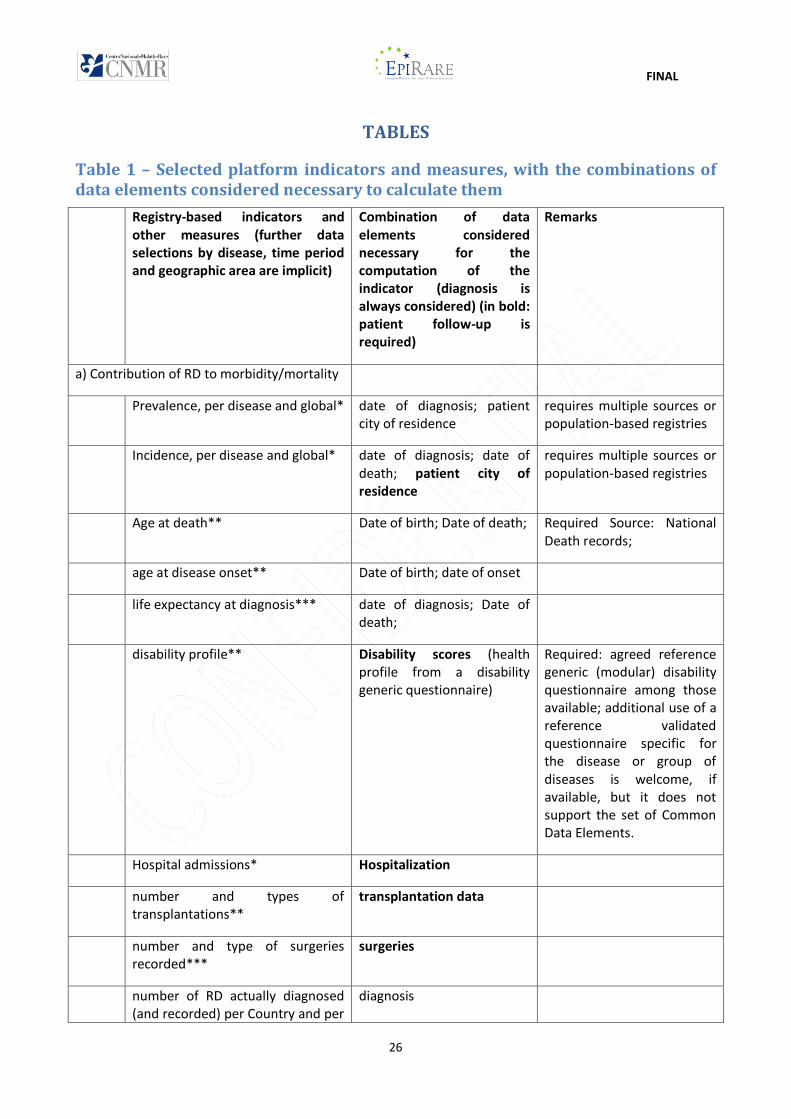
Information of use for cohort selection and patient recruitment for clinical trials may be based on a number of clinical data depending on the disease features and the scope of the trial. Therefore, actual patient recruitment decisions can be made through direct contact of disease specific registries and analysis of clinical data. This work can be facilitated by the metadata database which is planned as part of the platform. Here we have studied the feasibility of an model combination of common data elements which may make up the platform data repository. This example is based on registries collecting genetic data and data of co-morbidity, patient willingness to participate in clinical trials and patient contact. The results indicate the feasibility of combinations of all these data, within registries supporting longitudinal observations, in order to cope with changes which may occur during time. Fig. 20 shows, beside the
Figure 20 – Examples of data combinations for patient recruitment.
number of registries that can provide the different data combinations, that the data of patient willingness and of patient contact had a dramatic effect on the use of registries, and of the data they contain, for

FINAL
25
patient recruitment. These results indicate that the adoption of appropriate ethical procedures in patient registration should be carefully promoted and supported.
3. Indicators on equity and EU initiatives and other indicators based on registry data
The indicators, whose feasibility has been studied above, when applied to cohorts of patients based on time periods, geographic areas or even centers where they are cared, can have several uses, provided that the European platform succeeds in promoting procedures resulting in comparable data. The analysis of variations during time and across countries can give, at EU level, important indications regarding the epidemiology of the disease, equity of treatment, accessibility to care and OD, and can inform of the need for additional policies or of the impact of the current ones; at national level, the analysis of results across regions or centers can contribute to improve healthcare planning and to monitor costs.
IV. Conclusions
The results of this survey indicate that the RD patient registration practices currently on-going in the EU are suitable to cover most aspects related to rare disease information and care and show that most registries are ready or can be adapted to use common definitions, values and formats for many relevant rare disease patient data. Information on the use of common coding systems, reference terminologies and questionnaires has been collected for very few data elements: the results obtained extend previous evidence obtained by EPIRARE23,36 outlining a rather fragmented picture and suggesting that the adoption of common reference instruments will impact on most registries and the activities of data revision may represent a non negligible burden.
This survey has studied also the feasibility of computation of registry-based indicators identified by the EUROPLAN4 and RDTF5 projects and other information outputs which appeared of interest to the stakeholders consulted during the EPIRARE activities. The EUROPLAN and RDTF indicators provide general key information on rare diseases, health care and their trends and the implementation of RD policies; the alternative indicators and additional measures, which have been studied here, complement them, providing a more detailed insight into the actual operation of the health system dedicated to rare diseases, and exemplify how the platform and registry data can fulfill the information needs and expectations of the platform stakeholders. These examples are not exhaustive of the possible platform outputs, and it can be expected that, by combining the selected data elements, several other outputs can be devised, which are of value in the monitoring and management of the overall operation of the RD care system. For example, registry data could allow the monitoring of use of the resources relevant to a disease; data related to actual clinical treatment patterns could allow the monitoring of the penetration of best practice protocols in the common practice; the course of disability and the course of key disease-specific clinical parameters, if agreed by experts, could be used to provide clinical evidence and benchmarks to guide the activity of clinicians. A number of economic assessments also may be in the reach of the platform if billing related coding systems are used. The implementation of these developments may be triggered by a specific interest, or if and when appropriate agreements, validation and training programs are available to achieve a disease-specific or more sophisticated information.
36 Taruscio D, Gainotti S, Mollo E, Vittozzi L, Bianchi R, Ensini M, Posada M: The Current Situation and Needs of Rare Disease Registries in Europe. Public Health Genomics 2013;16(6) (in press)
FINAL
26
TABLES
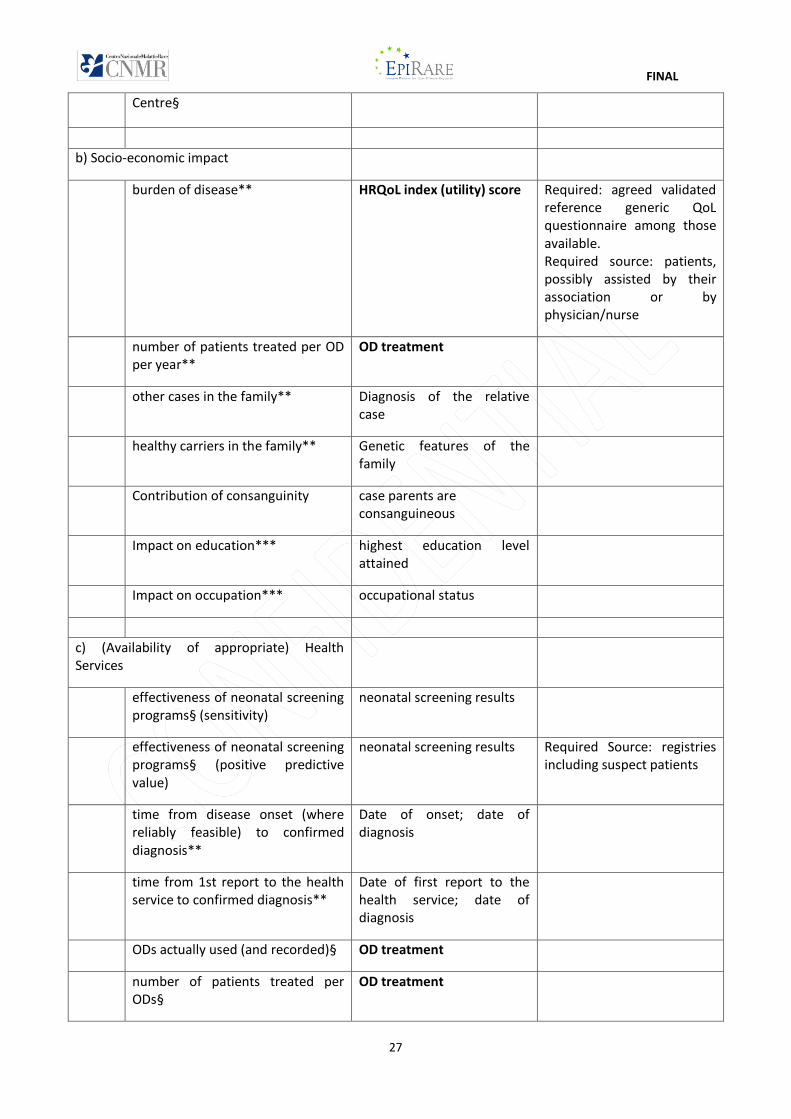
Table 1 – Selected platform indicators and measures, with the combinations of data elements considered necessary to calculate them
Registry-based indicators and other measures (further data selections by disease, time period and geographic area are implicit)
Combination of data elements considered necessary for the computation of the indicator (diagnosis is always considered) (in bold: patient follow-up is required)
Remarks
a) Contribution of RD to morbidity/mortality
Prevalence, per disease and global* date of diagnosis; patient city of residence
requires multiple sources or population-based registries
Incidence, per disease and global* date of diagnosis; date of death; patient city of residence
requires multiple sources or population-based registries
Age at death** Date of birth; Date of death; Required Source: National Death records;
age at disease onset** Date of birth; date of onset
life expectancy at diagnosis*** date of diagnosis; Date of death;
disability profile** Disability scores (health profile from a disability generic questionnaire)
Required: agreed reference generic (modular) disability questionnaire among those available; additional use of a reference validated questionnaire specific for the disease or group of diseases is welcome, if available, but it does not support the set of Common Data Elements.
Hospital admissions* Hospitalization
number and types of transplantations**
transplantation data
number and type of surgeries recorded***
surgeries
number of RD actually diagnosed (and recorded) per Country and per
diagnosis
FINAL
27
Centre§
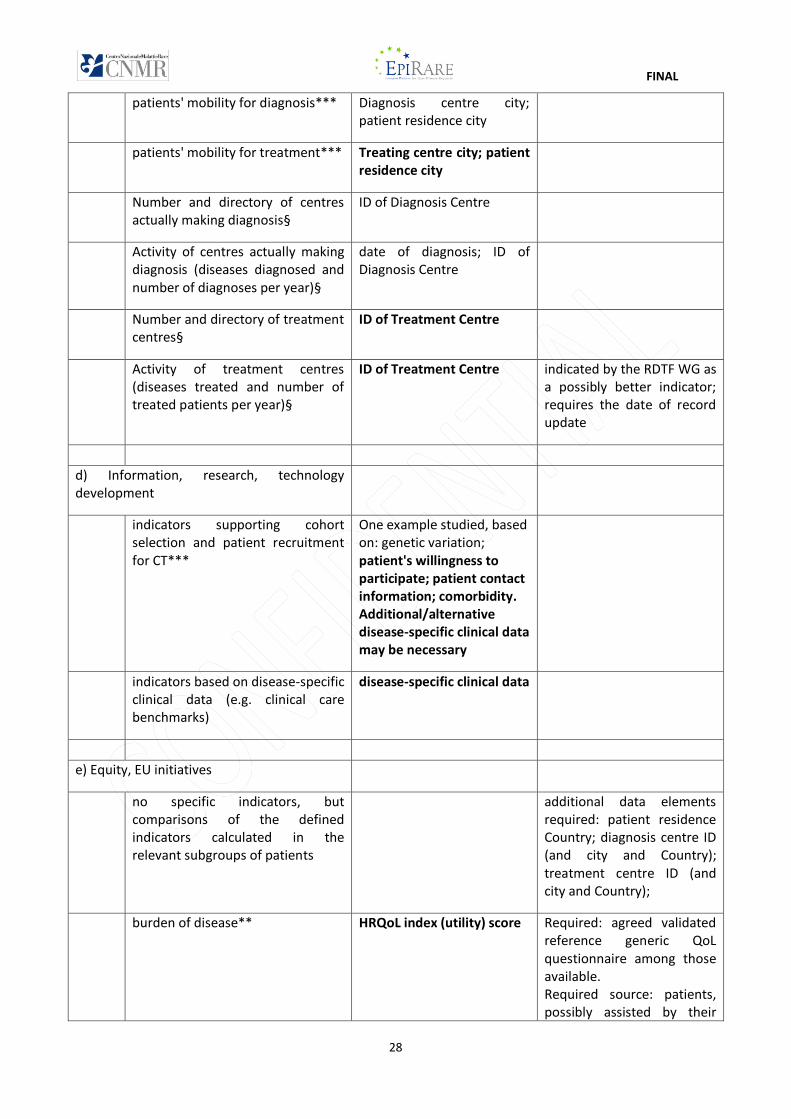
b) Socio-economic impact
burden of disease** HRQoL index (utility) score Required: agreed validated reference generic QoL questionnaire among those available. Required source: patients, possibly assisted by their association or by physician/nurse
number of patients treated per OD per year**
OD treatment
other cases in the family** Diagnosis of the relative case
healthy carriers in the family** Genetic features of the family
Contribution of consanguinity case parents are consanguineous
Impact on education*** highest education level attained
Impact on occupation*** occupational status
c) (Availability of appropriate) Health Services
effectiveness of neonatal screening programs§ (sensitivity)
neonatal screening results
effectiveness of neonatal screening programs§ (positive predictive value)
neonatal screening results Required Source: registries including suspect patients
time from disease onset (where reliably feasible) to confirmed diagnosis**
Date of onset; date of diagnosis
time from 1st report to the health service to confirmed diagnosis**
Date of first report to the health service; date of diagnosis
ODs actually used (and recorded)§ OD treatment
number of patients treated per ODs§
OD treatment
FINAL
28
patients' mobility for diagnosis*** Diagnosis centre city; patient residence city
patients' mobility for treatment*** Treating centre city; patient residence city
Number and directory of centres actually making diagnosis§
ID of Diagnosis Centre
Activity of centres actually making diagnosis (diseases diagnosed and number of diagnoses per year)§
date of diagnosis; ID of Diagnosis Centre
Number and directory of treatment centres§
ID of Treatment Centre
Activity of treatment centres (diseases treated and number of treated patients per year)§
ID of Treatment Centre indicated by the RDTF WG as a possibly better indicator; requires the date of record update
d) Information, research, technology development
indicators supporting cohort selection and patient recruitment for CT***
One example studied, based on: genetic variation; patient's willingness to participate; patient contact information; comorbidity. Additional/alternative disease-specific clinical data may be necessary
indicators based on disease-specific clinical data (e.g. clinical care benchmarks)
disease-specific clinical data
e) Equity, EU initiatives
no specific indicators, but comparisons of the defined indicators calculated in the relevant subgroups of patients
additional data elements required: patient residence Country; diagnosis centre ID (and city and Country); treatment centre ID (and city and Country);
burden of disease** HRQoL index (utility) score Required: agreed validated reference generic QoL questionnaire among those available. Required source: patients, possibly assisted by their
FINAL
29
association or by physician/nurse
*These indicators were considered by the RDTF particularly important for surveillance of status and trends
§ EUROPLAN indicators
**These measures are the proposed alternates to the indicators considered by the RDTF
***These are additional measures of which the registry-based feasibility is studied in this report
Appendix 1
The questionnaire (separate PDF document)
FINAL
30
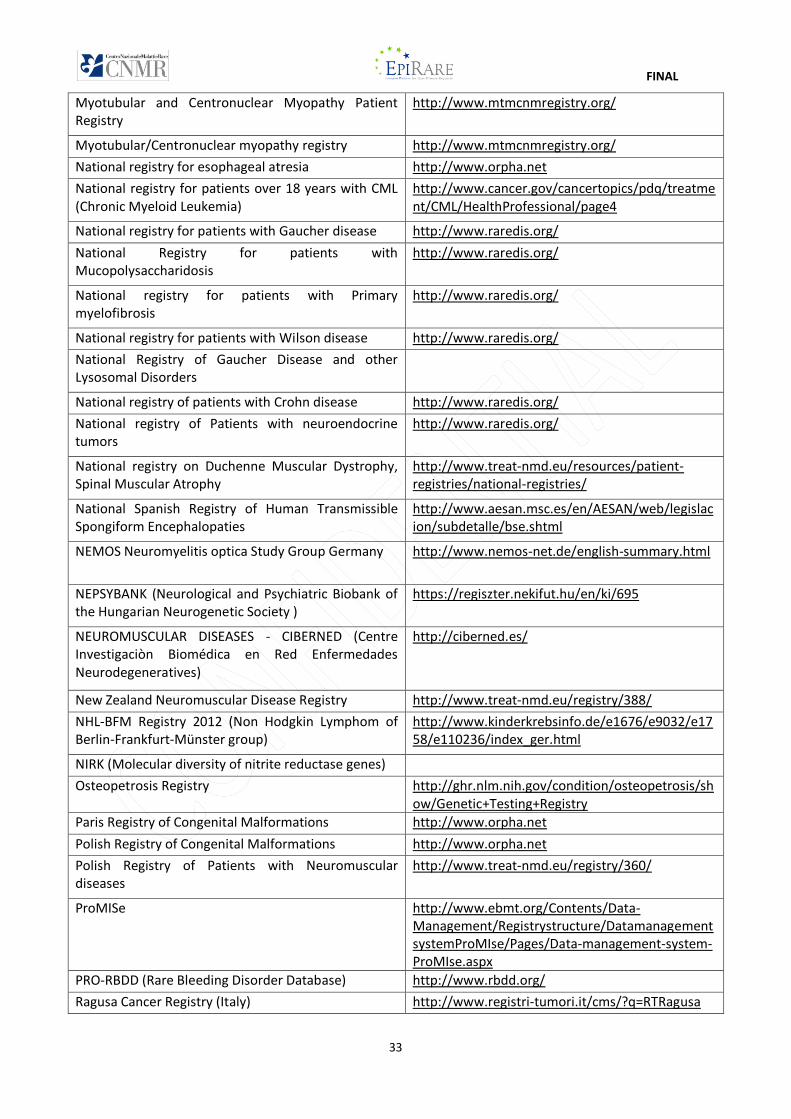
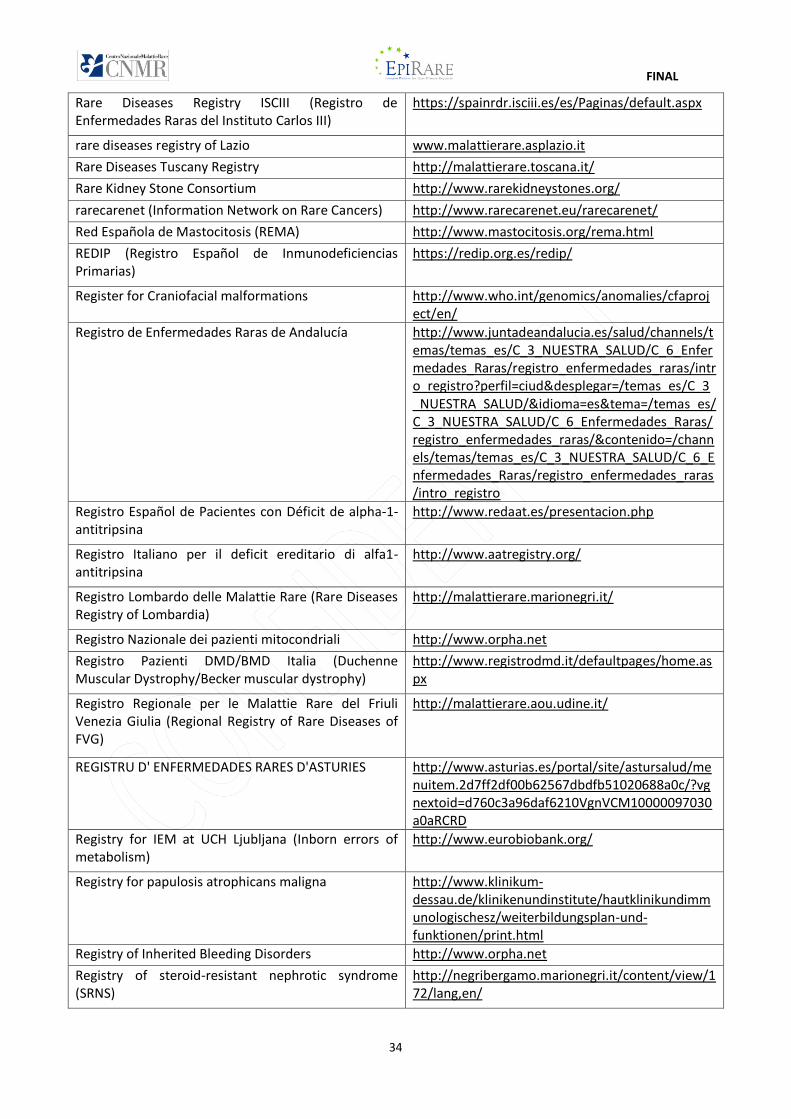
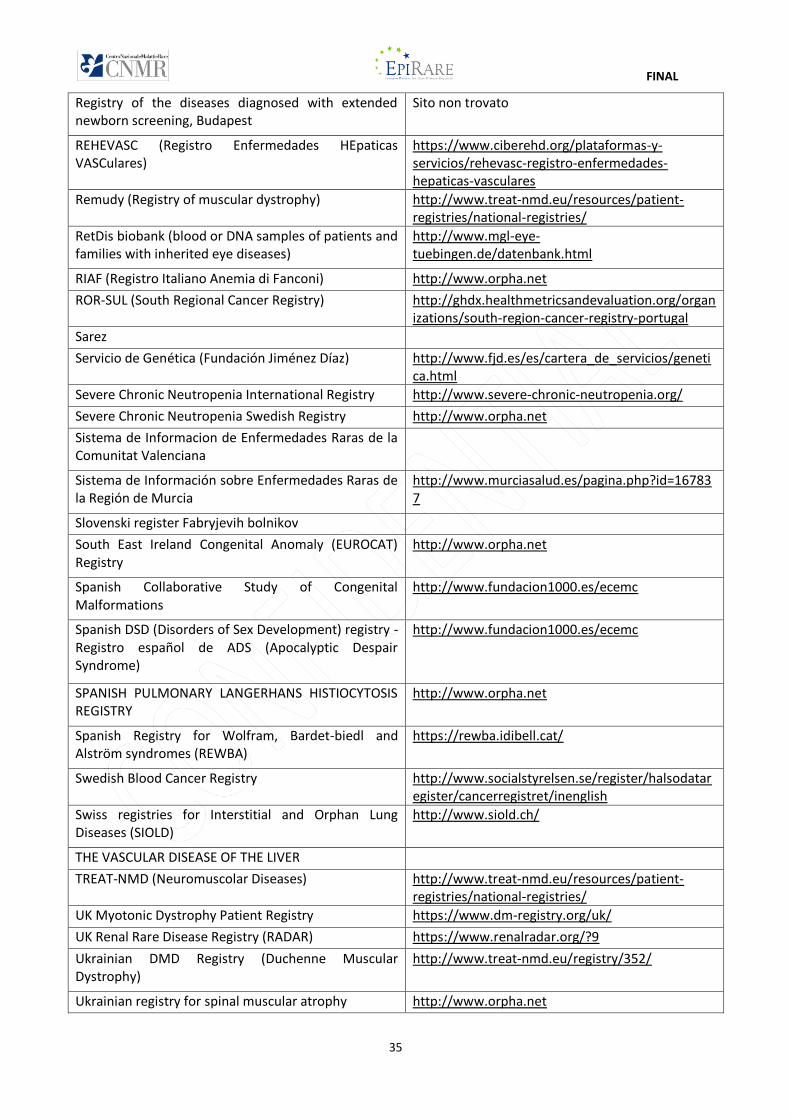
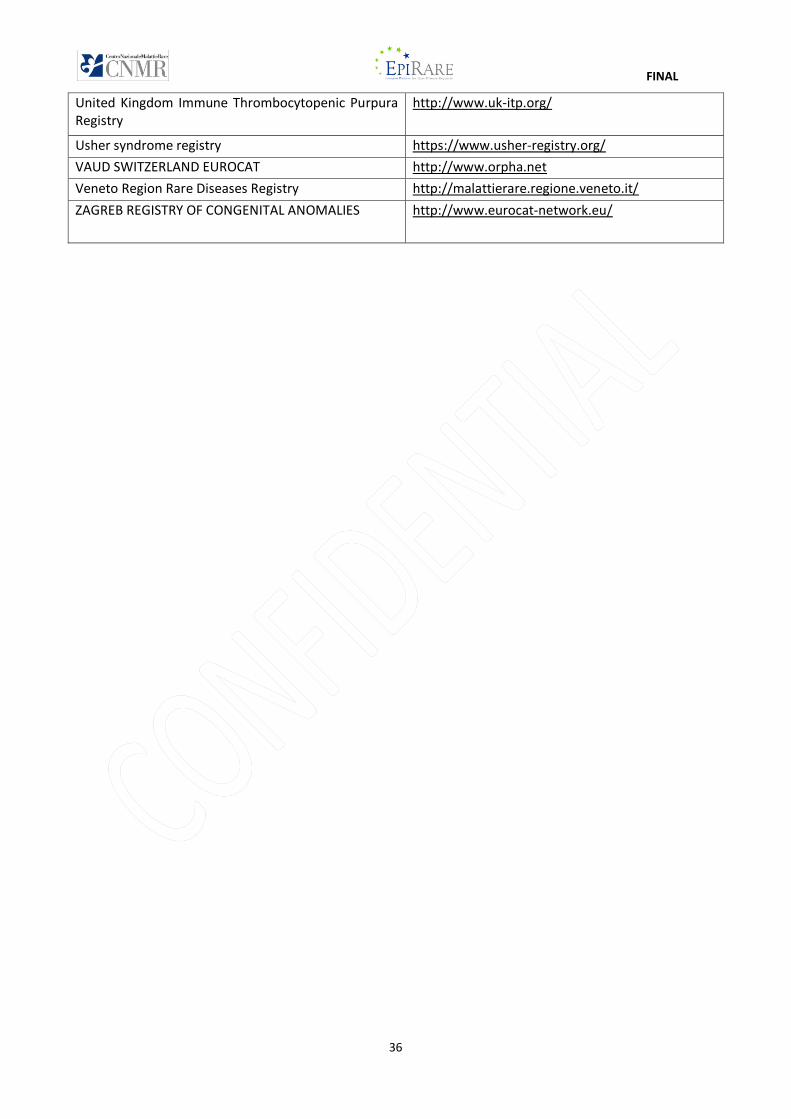
APPENDIX 2
List of registries that participated in the EPIRARE Survey on Common Data Elements
Name of Registry Website or source
Acute Lymphoblastic Leukemia Registry
ADAPT (Association for International and Comparative Studies in the labor law and industrial relations)
http://www.adapt.it/
Adult-Hospital Clínic of Barcelona-Inherited Errors of Metabolism
http://www.ssiem.org/home/welcome.asp
AIS-registry (Androgen insensitivity syndrome) http://ghr.nlm.nih.gov/condition/androgen-insensitivity-syndrome
ALS MND net (Amyotrophic Lateral Sclerosis e (Motor Neurone Disease)
http://www.orpha.net
AMR Registry (Alopecia-Mental Retardation) http://omim.org/entry/203650
Ataxia Database http://www.orpha.net
Ataxia Study Group http://www.orpha.net
Australian DMD and SMA Registry (Duchenne Muscular Dystrophy e Spinal Muscular Atrophy)
https://nmdregistry.com.au/dmd/
Australian Myotonic dytrophy Registry https://nmdregistry.com.au/dmd/
Austrian Hemophilia Registry https://www.studienregister.at/home
Austrian National Cancer Registry https://www.studienregister.at/home
Belgian Cancer Registry http://www.kankerregister.org/
Belgian Neuromuscular Disease Registry http://www.orpha.net
Birdshot Uveitis Registry http://rarediseases.info.nih.gov/gard/5926/birdshot-chorioretinopathy/resources/2
Birth Registry Mainz Model http://www.dkfz.de/en/umwepi/Birth_registry_Mainz_Model.html
Bradykinin induced angioedema http://www.orpha.net
Canadian Neuromuscular Disease Registry http://www.cndr.org/
Cases of human trichinellosis in France http://www.anses.fr/en/content/trichinellosis
Cfdatabasecph (Cystic Fibrosis Database Ph) http://www.genet.sickkids.on.ca/app
CFTR-FRance http://www.umd.fr/CFTR/
Chronic granulomatouse disease national registry http://www.usidnet.org/pub/Disease-Registry
Creutzfeldt-Jakob disease and related disorders http://www.iss.it/rncj/index.php
CURE-Net Registry (National registry for congenital uro-rectal malformations)
http://www.cure-net.de/de/projekte/register
Cystisk Fibrose Register Danmark http://www.orpha.net
Czech CF Registry (Cystic Fibrosis) http://ublg.lf2.cuni.cz/
D4/ phenodent (Diagnostiquer les Défauts Dentaires) http://www.orpha.net
FINAL
31
Deutsches Register Morbus Adamantiades-Behçet e.V.
http://www.behcet.de/
DNSS (Dysplastic nevus syndrome) http://atlasgeneticsoncology.org/Kprones/DysplNevusID10013.html
DuchenneConnect https://www.duchenneconnect.org/
Dutch Diagnosis Registration Metabolic Diseases http://www.metabole-ziekten.nl/
EB-Netzwerk Patientenregister (Epidermolysis bullosa)
http://www.netzwerk-eb.de/e7/index_ger.html
Eurocat Northern Netherlands http://www.eurocat-network.eu/
EUROCAT Registry of Funen County http://www.eurocat-network.eu/
Eurofever (Autoinflammatory Diseases’ Working Group of the Paediatric Rheumatology European Society)
http://www.printo.it/eurofever/
EUROGLYCANET (Congenital Disorders of Glycosylation)
http://www.euroglycanet.org/
European Alport registry http://www.alportsyndrome.org/resources/researchclinical-trials/
European Central Hypoventilation Syndrome Registry http://www.orpha.net
European Cystic Fibrosis Society Patient Registry https://www.ecfs.eu/projects/ecfs-patient-registry/intro
European IPF Registry (Idiopathic pulmonary fibrosis) http://www.pulmonary-fibrosis.net/
European porphyria registry http://www.porphyria-europe.com/04-about/news.asp?intIdArticle=51
European registry and network for intoxication type metabolic diseases
https://www.eimd-registry.org/
European Registry for Primary Immunodeficiencies http://www.esid.org/research-database
EUROWABB (Syndroms of Wolfram, Alström , Bardet-Biedl)
http://www.euro-wabb.org/it/
Finnish Cancer Registry http://www.cancer.fi/syoparekisteri/en/
Finnish Care Register for Health Care http://rekisteritutkimusen.wordpress.com/registers/register-controllers/
Finnish TREAT-NMD Patient Registry (Neuromuscolar Network)
http://www.treat-nmd.eu/registry/331/
French National Reference Center for Primary Immune Deficiencies
French National Registry of Rare Peritoneal Surface Malignancies
http://pmppals.org/peritoneal-surface-malignancies.html
French registry for Thalassemia http://www.orpha.net
French registry on Pulmonary Hypertension
German registry for DMD (Duchenne Muscular Dystrophy)/Dystrophinopathies
http://www.treat-nmd.de/
German Registry for INdividuals with alpha-1-antitrypsin deficiency
http://www.alpha-1-info.com/startseite-fuer-patienten.htm
FINAL
32
German Registry on congenital dyserythropoietc anemias
German SMA patient registry (Spinal Muscular Atrophy)
http://www.treat-nmd.de/
Girona Cancer Registry http://www20.gencat.cat/portal/site/salut/menuitem.003a2436be9bc6ec3bfd8a10b0c0e1a0/?vgnextoid=10450365d14c5310VgnVCM2000009b0c1e0aRCRD&vgnextchannel=10450365d14c5310VgnVCM2000009b0c1e0aRCRD&vgnextfmt=default&newLang=en_GB
Global FKRP Registry (Fukutin-Related Protein) https://www.fkrp-registry.org/
Haemoglobinopathies http://www.orpha.net
Hospital Garrahan, Buenos Aires, Argentina http://www.garrahan.gov.ar/
I-DSD Registry (Disorders of Sex Development) https://tethys.nesc.gla.ac.uk/
International FKRP registry (Fukutin-Related Protein) https://www.fkrp-registry.org/
International Registry of Recurrent and Familial Hemolytic Uremic Syndrome/Thrombotic Thrombocytopenic Purpura
http://negribergamo.marionegri.it/content/view/170/lang,en/
International survey on Congenital diserythropoietic anemias
http://www.orpha.net
Italian Mitochondrial database https://www.mitochondrialdisease.it/login
Italian National Registry of Rare Diseases http://www.iss.it/cnmr/regi/cont.php?id=991&tipo=53&lang=2
Italian Registry of Membranoproliferative Glomerulonephritis
http://negribergamo.marionegri.it/content/view/171/lang,en/
Jain Foundation LGMD2B/Miyoshi registry http://www.jain-foundation.org/patient-physician-resources/clinical-studies-and-trials/clinical-studies-and-trials-lgmd2bmiyoshi-my
Kukas http://www.uskur.com.tr/en/news/muscle-disorders-registration-system-kukas-online
Laminopathy & Emerinopathy
Leiden Muscular Dystrophy pages / LOVD (Leiden Open source Variation Database)
http://www.dmd.nl/
Malattie Rare Lazio www.malattierare.asplazio.it
Malformation Monitoring Centre Saxony-Anhalt http://www.angeborene-fehlbildungen.com/
Marfan and related disorders http://www.orpha.net
Mastocitosis y síndromes de activación mastocitaria http://www.orpha.net
Mastocytosis registry (UK) http://www.patient.co.uk/support/UK-Mastocytosis-Support-Group.htm
MND NET Germany (Motor Neurone Disease) http://www.uniklinik-ulm.de/index.php?id=1418
Mount Sinai School of Medicine http://icahn.mssm.edu/
MTM1-UMD http://www.umd.be/
Myotonic Dystrophy Patient registry for Germany and Switzerland
http://www.myotonic.org/
FINAL
33
Myotubular and Centronuclear Myopathy Patient Registry
http://www.mtmcnmregistry.org/
Myotubular/Centronuclear myopathy registry http://www.mtmcnmregistry.org/
National registry for esophageal atresia http://www.orpha.net
National registry for patients over 18 years with CML (Chronic Myeloid Leukemia)
http://www.cancer.gov/cancertopics/pdq/treatment/CML/HealthProfessional/page4
National registry for patients with Gaucher disease http://www.raredis.org/
National Registry for patients with Mucopolysaccharidosis
http://www.raredis.org/
National registry for patients with Primary myelofibrosis
http://www.raredis.org/
National registry for patients with Wilson disease http://www.raredis.org/
National Registry of Gaucher Disease and other Lysosomal Disorders
National registry of patients with Crohn disease http://www.raredis.org/
National registry of Patients with neuroendocrine tumors
http://www.raredis.org/
National registry on Duchenne Muscular Dystrophy, Spinal Muscular Atrophy
http://www.treat-nmd.eu/resources/patient-registries/national-registries/
National Spanish Registry of Human Transmissible Spongiform Encephalopaties
http://www.aesan.msc.es/en/AESAN/web/legislacion/subdetalle/bse.shtml
NEMOS Neuromyelitis optica Study Group Germany http://www.nemos-net.de/english-summary.html
NEPSYBANK (Neurological and Psychiatric Biobank of the Hungarian Neurogenetic Society )
https://regiszter.nekifut.hu/en/ki/695
NEUROMUSCULAR DISEASES - CIBERNED (Centre Investigaciòn Biomédica en Red Enfermedades Neurodegeneratives)
http://ciberned.es/
New Zealand Neuromuscular Disease Registry http://www.treat-nmd.eu/registry/388/
NHL-BFM Registry 2012 (Non Hodgkin Lymphom of Berlin-Frankfurt-Münster group)
http://www.kinderkrebsinfo.de/e1676/e9032/e1758/e110236/index_ger.html
NIRK (Molecular diversity of nitrite reductase genes)
Osteopetrosis Registry http://ghr.nlm.nih.gov/condition/osteopetrosis/show/Genetic+Testing+Registry
Paris Registry of Congenital Malformations http://www.orpha.net
Polish Registry of Congenital Malformations http://www.orpha.net
Polish Registry of Patients with Neuromuscular diseases
http://www.treat-nmd.eu/registry/360/
ProMISe http://www.ebmt.org/Contents/Data-Management/Registrystructure/DatamanagementsystemProMIse/Pages/Data-management-system-ProMIse.aspx
PRO-RBDD (Rare Bleeding Disorder Database) http://www.rbdd.org/
Ragusa Cancer Registry (Italy) http://www.registri-tumori.it/cms/?q=RTRagusa
FINAL
34
Rare Diseases Registry ISCIII (Registro de Enfermedades Raras del Instituto Carlos III)
https://spainrdr.isciii.es/es/Paginas/default.aspx
rare diseases registry of Lazio www.malattierare.asplazio.it
Rare Diseases Tuscany Registry http://malattierare.toscana.it/
Rare Kidney Stone Consortium http://www.rarekidneystones.org/
rarecarenet (Information Network on Rare Cancers) http://www.rarecarenet.eu/rarecarenet/
Red Española de Mastocitosis (REMA) http://www.mastocitosis.org/rema.html
REDIP (Registro Español de Inmunodeficiencias Primarias)
https://redip.org.es/redip/
Register for Craniofacial malformations http://www.who.int/genomics/anomalies/cfaproject/en/
Registro de Enfermedades Raras de Andalucía http://www.juntadeandalucia.es/salud/channels/temas/temas_es/C_3_NUESTRA_SALUD/C_6_Enfermedades_Raras/registro_enfermedades_raras/intro_registro?perfil=ciud&desplegar=/temas_es/C_3_NUESTRA_SALUD/&idioma=es&tema=/temas_es/C_3_NUESTRA_SALUD/C_6_Enfermedades_Raras/registro_enfermedades_raras/&contenido=/channels/temas/temas_es/C_3_NUESTRA_SALUD/C_6_Enfermedades_Raras/registro_enfermedades_raras/intro_registro
Registro Español de Pacientes con Déficit de alpha-1-antitripsina
http://www.redaat.es/presentacion.php
Registro Italiano per il deficit ereditario di alfa1-antitripsina
http://www.aatregistry.org/
Registro Lombardo delle Malattie Rare (Rare Diseases Registry of Lombardia)
http://malattierare.marionegri.it/
Registro Nazionale dei pazienti mitocondriali http://www.orpha.net
Registro Pazienti DMD/BMD Italia (Duchenne Muscular Dystrophy/Becker muscular dystrophy)
http://www.registrodmd.it/defaultpages/home.aspx
Registro Regionale per le Malattie Rare del Friuli Venezia Giulia (Regional Registry of Rare Diseases of FVG)
http://malattierare.aou.udine.it/
REGISTRU D' ENFERMEDADES RARES D'ASTURIES http://www.asturias.es/portal/site/astursalud/menuitem.2d7ff2df00b62567dbdfb51020688a0c/?vgnextoid=d760c3a96daf6210VgnVCM10000097030a0aRCRD
Registry for IEM at UCH Ljubljana (Inborn errors of metabolism)
http://www.eurobiobank.org/
Registry for papulosis atrophicans maligna http://www.klinikum-dessau.de/klinikenundinstitute/hautklinikundimmunologischesz/weiterbildungsplan-und-funktionen/print.html
Registry of Inherited Bleeding Disorders http://www.orpha.net
Registry of steroid-resistant nephrotic syndrome (SRNS)
http://negribergamo.marionegri.it/content/view/172/lang,en/
FINAL
35
Registry of the diseases diagnosed with extended newborn screening, Budapest
Sito non trovato
REHEVASC (Registro Enfermedades HEpaticas VASCulares)
https://www.ciberehd.org/plataformas-y-servicios/rehevasc-registro-enfermedades-hepaticas-vasculares
Remudy (Registry of muscular dystrophy) http://www.treat-nmd.eu/resources/patient-registries/national-registries/
RetDis biobank (blood or DNA samples of patients and families with inherited eye diseases)
http://www.mgl-eye-tuebingen.de/datenbank.html
RIAF (Registro Italiano Anemia di Fanconi) http://www.orpha.net
ROR-SUL (South Regional Cancer Registry) http://ghdx.healthmetricsandevaluation.org/organizations/south-region-cancer-registry-portugal
Sarez
Servicio de Genética (Fundación Jiménez Díaz) http://www.fjd.es/es/cartera_de_servicios/genetica.html
Severe Chronic Neutropenia International Registry http://www.severe-chronic-neutropenia.org/
Severe Chronic Neutropenia Swedish Registry http://www.orpha.net
Sistema de Informacion de Enfermedades Raras de la Comunitat Valenciana
Sistema de Información sobre Enfermedades Raras de la Región de Murcia
http://www.murciasalud.es/pagina.php?id=167837
Slovenski register Fabryjevih bolnikov
South East Ireland Congenital Anomaly (EUROCAT) Registry
http://www.orpha.net
Spanish Collaborative Study of Congenital Malformations
http://www.fundacion1000.es/ecemc
Spanish DSD (Disorders of Sex Development) registry - Registro español de ADS (Apocalyptic Despair Syndrome)
http://www.fundacion1000.es/ecemc
SPANISH PULMONARY LANGERHANS HISTIOCYTOSIS REGISTRY
http://www.orpha.net
Spanish Registry for Wolfram, Bardet-biedl and Alström syndromes (REWBA)
https://rewba.idibell.cat/
Swedish Blood Cancer Registry http://www.socialstyrelsen.se/register/halsodataregister/cancerregistret/inenglish
Swiss registries for Interstitial and Orphan Lung Diseases (SIOLD)
http://www.siold.ch/
THE VASCULAR DISEASE OF THE LIVER
TREAT-NMD (Neuromuscolar Diseases) http://www.treat-nmd.eu/resources/patient-registries/national-registries/
UK Myotonic Dystrophy Patient Registry https://www.dm-registry.org/uk/
UK Renal Rare Disease Registry (RADAR) https://www.renalradar.org/?9
Ukrainian DMD Registry (Duchenne Muscular Dystrophy)
http://www.treat-nmd.eu/registry/352/
Ukrainian registry for spinal muscular atrophy http://www.orpha.net
FINAL
36
United Kingdom Immune Thrombocytopenic Purpura Registry
http://www.uk-itp.org/
Usher syndrome registry https://www.usher-registry.org/
VAUD SWITZERLAND EUROCAT http://www.orpha.net
Veneto Region Rare Diseases Registry http://malattierare.regione.veneto.it/
ZAGREB REGISTRY OF CONGENITAL ANOMALIES http://www.eurocat-network.eu/