Embed Size (px)
Citation preview

European Journal of Obstetrics & Gynecology and Reproductive Biology 177 (2014) 106–109
Common determinants of breech presentation at birth in singletons: apopulation-based study
Hendrik Cammu a,b,*, Noëlie Dony b, Guy Martens a, Roos Colman c
a Study Centre of Perinatal Epidemiology, Brussels, BelgiumbDepartment Obstetrics & Gynaecology, University Hospital, VU Brussels, BelgiumcBiostatistics Unit, University Ghent, Belgium
A R T I C L E I N F O
Article history:Received 17 December 2013Received in revised form 10 March 2014Accepted 8 April 2014
Keywords:Determinants breech presentationParturition
A B S T R A C T
Objective: To estimate common determinants of breech presentation at parturition.Study design: A population-based cohort study (between 1/1/2001 and 31/12/2010) was conductedamong all women who delivered a singleton baby in breech presentation from 22 completed weeks ofgestation. A binary logistic regression was used to determine independent feto–maternal characteristicsof breech presentation at birth, adjusted odds ratios and 95% confidence intervals. Variables were:gestational age, birth weight, maternal age, parity and gender of the baby, presence or absence of ahistory of cesarean section, gestational diabetes, gestational hypertension, pregnancy after assistedreproduction technology and congenital malformations.Results: From a population of 611,021 women; 28,059 were delivered in breech presentation (4.59%).Independent determinants of breech presentation at delivery were: gestational age and birth weight (thelower, the higher the incidence of breech at birth), parity (the frequency of breech decreased withincreasing parity) and maternal age (the older the mother, the higher the odds for breech presentation).Women who had a scarred uterus, due to a previous cesarean section, women who gave birth to a femaleoffspring and women whose baby showed a congenital malformation, were more prone to be delivered inbreech presentation.Conclusion: Low gestational age and birth weight, advanced maternal age, a scarred uterus, a female babyand a baby with a congenital malformation increased the odds for singleton breech presentation atparturition. The latter gradually decreased with increasing parity.
ã 2014 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
journal homepage: www.else vie r .com/ locat e/e jogrb
Introduction
The overall incidence of breech presentation at birth isbetween 4 and 5%. The lower the gestational age, the morefrequent the baby lies in the breech position. At 28 weeks, forinstance, 22% present by breech, at term it is less than 4% [1]. Themost common cause of breech presentation is therefore pretermdelivery. Nearer term, a breech presentation must be the result ofsomething preventing a spontaneous version to the vertexposition. This may be due to mechanical factors such as uterineabnormalities or a contracted pelvis. Fetal growth retardation,oligo- or polyhydramnios and fetal malformations such ashydrocephalus are also recognized causes of breech presentation.However, all these factors are found in only a small amount ofbreech presentations and usually no single cause of the breech
* Corresponding author at: Academic Hospital VU Brussels, Laarbeeklaan 101,1090 Brussels, Belgium. Tel.:+ +32 479 38 21 92.
E-mail address: [email protected] (H. Cammu).
http://dx.doi.org/10.1016/j.ejogrb.2014.04.0080301-2115/ã 2014 Elsevier Ireland Ltd. All rights reserved.
presentation can be identified [2]. This study aimed at making aninventory of common obstetrical characteristics that are inde-pendently associated with breech presentation at parturition. Tothat end we conducted a population-based cohort study.
Materials and methods
Flanders, the Dutch speaking northern part of the constitution-ally federal state of Belgium, has 6.2 million inhabitants and onaverage 62,000 births per year of which 99% take place in thehospital maternity units. All of the following data were derivedfrom the computer files of the Study Centre for PerinatalEpidemiology (SPE). The SPE is an independent, regionally funded,centre that registers all births of >500 g and/or 22 weeks gestation.For each newborn, a standard perinatal form is completed (mostlyby the midwife) and sent to the SPE where all data are checked byan error detection program and feedback is given. During the studyperiod 1/1/2001–31/12/2010, 613,356 singleton births wereregistered of which 4.6% were born in breech presentation. We

H. Cammu et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 177 (2014) 106–109 107
excluded 2335 records due to missing values for the response orexplanatory variables, leaving 611,021 records in the final model.
Approval by the ethics committee was not obtained since thestudy extracted anonymous data from an existing dataset of theSPE for which appropriate permissions have already been obtained(www.zorg-en-gezondheid.be/). It is not possible to identifyindividuals from the information provided.
Categorical variables were compared with chi-square tests (SASsoftware, version 9.3). The level of statistical significance was set ata probability value of <0.01. A multiple binary logistic regressionanalysis was done to assess interrelations between risk factors.Results were expressed as adjusted odds ratios (OR) andcorresponding 95% confidence intervals (CIs).
Results
Of the 611,021 singleton infants, born from 22 weeks on, 28,059were delivered in breech presentation (4.59%). Table 1 shows thedistribution of the frequency of birth in breech presentationaccording to the gestational age. There is a gradual decline inbreech delivery that is consistent with the increase in gestationalage. However, compared to weeks 35–37, we found a smallincrease in breech presentation at week 38. Beyond 39 weeksgestation, breech presentation at delivery dropped to 0.9%(Table 1).
In order to elucidate independent characteristics of breechpresentation at birth, we performed a multiple binary logisticregression with presentation (breech/no breech) as outcomevariable and the variables gestational age category, birth weightcategory, maternal age category, parity, history of cesarean section,gestational diabetes or hypertension, pregnancy after assistedreproduction technology (in vitro fertilisation/intracytoplasmaticsperm injection), gender (male/female), and congenital malfor-mations (yes/no), as predictors.
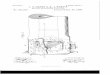
The predictors which significantly correlated with breechpresentation at birth are shown in Table 2 and the Fig. 1.Gestational age and birth weight were the most importantdeterminants of breech presentation at parturition. The odds forhaving a birth in breech presentation rose with the increasing ageof the mother. But with parity, the odds for breech decreased. Ahistory of cesarean section independently increased the odds forbreech by 44%. Giving birth to a baby with a congenitalmalformation in the current pregnancy increased the odds by24%. Table 2 also shows that the odds for breech were 1.28 timeshigher in female compared to male babies after being controlledfor relevant characteristics such as gestational and maternal age,parity, history of cesarean section (yes/no) and congenitalmalformations (yes/no).
Table 1The SAS system.
Gestational age(weeks)
Proportionbreech
LowerCL UpperCL Numberbreech
Total
22–24 35.3% 29.5% 41.6% 84 23825–26 33.6% 29.9% 37.4% 201 59927–28 25.2% 22.6% 28.1% 234 92729 22.3% 18.9% 26.1% 112 50330 20.4% 17.7% 23.3% 158 77631 19.4% 17.0% 22.0% 188 97132 14.1% 12.5% 16.0% 215 152333 13.0% 11.7% 14.4% 302 233134 11.6% 10.6% 12.5% 511 442335 9.4% 8.8% 10.1% 723 765236 8.0% 7.7% 8.5% 1378 1712537 8.1% 7.9% 8.4% 3435 4237038 9.5% 9.4% 9.7% 10482 11002839 4.7% 4.6% 4.8% 7867 168157>39 0.9% 0.8% 0.9% 2169 253398
Breech presentation at birth was not significantly morecommon in women who had gestational diabetes or hypertension.Breech presentation at parturition was more frequently seen afterassisted reproduction technology (5.91%) than after spontaneouslyconceived pregnancies (4.44%, chi-square p < 0.01) However afteradjustment for all the aforementioned relevant confoundingfactors, the significant difference abated.
Comments
This large cohort study aimed at elucidating commonindependent determinants of breech presentation at birth. Ourresults are in line with previous, less extensive, population-basedcohort studies [1,3–8]. Factors associated with increased risk ofbreech delivery in Flanders (northern Belgium) are: low gestation-al age and low birth weight, increasing maternal age, primiparity,history of cesarean section, female gender and presence of acongenital malformation.
The earlier the gestational age, the higher the prevalence ofbreech presentation will be. We found a small increase of breechpresentation at week 38 compared to weeks 35–37 (Fig. 1). Thisincrease was iatrogenic. It was the result of the policy ofperforming elective pre-labor cesarean sections for breech from38 weeks on. By doing so, we created an artificial peak in thenumber of births in breech presentation in that specific week andwe certainly prevented some fetuses the opportunity as yet to turnspontaneously. Subsequently, beyond 39 weeks, there were almostno women with a baby in breech position left to give birth.Therefore the decrease in breech delivery beyond 39 weeks wasalso iatrogenic.
Gestational age and birth weight are interrelated. However, atbirth, breech neonates weighed less than vertex neonates afterbeing controlled for relevant factors. This is found on severaloccasions [2,7,8]. The relationship between intrauterine growthretardation and breech presentation in both preterm and terminfants has been clearly demonstrated [2,7–9].
Multiparity and a female gender are associated with breechpresentation at birth. It has been suggested that this is a fetal sizeeffect [7]. Indeed, infants born to primiparous women are lighterthan those born to multiparous women, and girls, on average, aresmaller than boys [10]. However, in this study, parity and genderwere independent determinants. Factors, other than birth weightmust play a role. A report from Norway [11] suggests that womenwho delivered a baby in breech presentation, mostly after cesareansection, less frequently decide to have another pregnancy. This mayexplain the higher frequency of primiparity in breech presentation[11]. Witkop [12] et al. performed prenatal ultrasound in 7045women and found that a non-vertex fetus at 35 weeks innulliparous women had twice the risk of staying in that positionat delivery compared to multiparous women. This is probably dueto the more relaxed muscle tone of the uterine and abdominal wallin multiparous women [6]. And it may also be the reason why thesuccess rate of external cephalic version is significantly higher inmultiparous women. [13].
Half a century ago, Morgan and Kane [2] reported a higherincidence of breech presentation in female compared to maleoffspring. Other studies have supported this finding [5,7,8,14–16]but no clear aetiology has been put forward to elucidate thisassociation. Soernes and Bakke showed that, due to differences inintrauterine fetal motor activity, the umbilical cord is shorter inbabies born in breech than in vertex presentations [15]. They alsoreported that the mean cord length is somewhat shorter in femalecompared to male infants, suggesting a higher fetal activity in boys.Consequently, female babies are more prone to be born in breechpresentation [15].

Table 2Independent predictors of breech presentation at birth in singletons.
Oddsratioa
95% Confidence intervalsa
Gestational age (39 w = reference)22–28 w vs 39 w 4.13 3.42–4.9829–32 w vs 39 w 2.31 2.02–2.6333–36 w vs 39 w 1.53 1.45–1.6137–38 w vs 39 w 1.93 1.87–1.99>39 w vs 39 w 0.18 0.17–0.19
Birth weight (3000–3500 g = reference)
500–1499 g vs 3000–3500 g 1.93 1.64–2.261500–1999 g vs 3000–3500 g 1.56 1.41–1.742000–2499 g vs 3000–3500 g 1.34 1.27–1.422500–2999 g vs 3000–3500 g 1.18 1.14–1.21>3500 g vs 3000–3500 g 0.80 0.77–0.82
Maternal age (25–29 y = reference)<20 y vs 25–29 y 0.50 0.45–0.5520–24 y vs 25–29 y 0.68 0.65–0.7130–34 y vs 25–29 y 1.28 1.24–1.3235–39 y vs 25–29 y 1.34 1.28–1.39>40 y vs 25–29 y 1.47 1.35–1.61
Parity (para 1 = reference)Para 2 vs para 1 0.50 0.48–0.51Para 3 vs para 1 0.36 0.35–0.38Para >3 vs para 1 0.34 0.32–0.36
History of cesarean sectionYes vs no 1.44 1.38–1.50
Gender offspringFemale vs male 1.28 1.25–1.31
Congenital malformationsYes vs no 1.24 1.14–1.35
w = weeks, g = gram, vs = versus, y = year.a Multivariate analysis.
108 H. Cammu et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 177 (2014) 106–109
A previous cesarean section increased the risk for breechpresentation by 44 percent (Table 2). Two studies, one from France[17] and one from Greece [18] showed that women with previouscesarean deliveries had double risk of breech presentation at termcompared to women with previous vaginal deliveries. Unfortunatelywe were unable to identify the reason for the previous cesarean
Fig. 1. Independent predictors of breech presentation at birth in si
section.Awomanwitha fetus inbreech ismore likely to have anotherbreech in a subsequent pregnancy [16]. Therefore, just having ascarred uterus may not be the only reason for the breech position inthis subgroup knowing that about 85–90% (SPE yearbooks2001–2010) of all babies in breech positions is born by cesareansection.
The presence of a congenital anomaly was an independentpredictor of being born in breech position. This is also found byothers [5–7,16] and may be attributed to the higher probability offetal neuromuscular dysfunction in association with congenitalmalformations. Indeed, as fetuses mature, a progressive calcifica-tion of the fetal skull bones occurs. The head becomes heavier andmost fetuses move into cephalic position before delivery. An intactneuromuscular system is essential for the fetus to be able to “kickitself around”, i.e. to establish a spontaneous version to cephalicpresentation. Studies on the relationship between breech presen-tation, fetal behavior, and neurologic maturation provide conflict-ing evidence [19–21]. Kean et al. [19] showed with Dopplerultrasound that breech fetuses showed subtle behavioral differ-ences and are therefore neurologically different from their cephaliccounterparts. Bartlett et al. [20] found minor transient neurologicaldifferences post-partum in breech-presenting infants, differencesthat did not persist at 18 months. Park et al. compared, by means ofthe fetal heart rate variability, the cardiovascular autonomicnervous system in breech and cephalic fetuses [21]. The authorscautiously concluded that the neurologic maturation of breechfetuses was not inferior to cephalic ones [21].
Uterine related issues (anomalies, abnormal placentation,oligo- or polyhydramnios) offer another mechanism to explainwhy the spontaneous version does not occur. There are severalreports on the relationship between breech position and uterineabnormalities [22–23] or placental location [24]. In a study of 108uterine anomalies (mostly septate or bicornuate uteri), breechpresentation amounted to 50%, though the overall incidence of theabove mentioned uterine anomalies in the studied population wasonly 0.7% [22]. Stout et al. [23] found a fifty percent higherincidence in breech presentation (OR: 1.5, CI: 1.3–1.9) in womenwith leiomyomas. The incidence of leiomyomas in their studygroup was 3.2%. Sekulic et al. reported on the relationship betweenthe cornual-fundal location of the placenta and the frequency ofbreech presentation [24]. A cornual-fundal located placenta canmechanically prevent the turning of the fetus and is associatedwith a very high (27–39%) frequency of breech presentation [24].
ngletons plotted on a logarithmic scale (multivariate analysis).

H. Cammu et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 2 177 (2014) 106–109 109
However, Luterkort et al. [2] did not find a difference in placentallocation between breech and cephalic presentation.
We found a higher risk of breech presentation in singletonsconceived by IVF/ICSI. In accordance with the results of Romund-stad et al. [25], this significance disappeared after having beencontrolled for maternal age, gestational age and parity, factors thatdiffer between spontaneously and artificially (IVF/ICSI) conceivedpregnancies [26].
An important shortcoming of this study is that we had noinformation about acknowledged albeit rare factors linked to thebreech presentation such as uterine anomalies. Population-basedstudies of risk factors for breech presentation with large numbersof participants, allow a more precise estimate of true risk afterother factors have been controlled for [1,3–8]. However, aretrospective population-based cohort maybe not the bestinstrument to study infrequent causes of breech presentationssince the true incidence of these causes in the population (=thedenominator) is mostly unknown. A case-control study is then abetter option [2,6]. Another shortcoming is that we had no data onthe recurrence risk of breech presentation in consecutive singletonpregnancies and therefore we did not know whether this riskfactor would have affected the other independent determinants.Finally, we were in limbo with regard to the correct number ofbreech-presenting infants for we had no data on the impact ofexternal cephalic version (ECV). Indeed, a successful ECV wasregistered as a cephalic presentation at birth.
We are aware that this study adds no new predictive factors forbreech presentation. All aforementioned independent determi-nants have already been described. The strength of the paper isthat it is a population-based study with a large number of fetusesin breech presentation where the most important determinants ofbirth in breech presentation were studied simultaneously. Thelarge sample size made the relative risks solid and the confidenceintervals close.
Conflict of interest
The authors report no conflicts of interest.
Acknowledgment
The authors thank the “Flemish Agency Care & Health” (VlaamsAgentschap Zorg & Gezondheid www.zorg-en-gezondheid.be/cijfers/cijfers-over-geboorte-en-bevalling/) for access to the data-bases of the Study Centre for Perinatal Epidemiology.
References
[1] Hickok DE, Gordon DC, Milberg JA, Williams MA, Daling JR. The frequency ofbreech presentation by gestational age at birth: a large population-basedstudy. Am J Obstet Gynecol 1992;166:851–2.
[2] Luterkort M, Persson PH, Weldner BM. Maternal and fetal factors in breechpresentation. Obstet Gynecol 1984;64:55–9.
[3] Morgan HS, Kane SH. An analysis of 16,327 breech births. JAMA 1964;187:262–4.[4] Hill LM. Prevalence of breech presentation by gestational age. Am J Perinatol
1990;7(1):92–3.[5] Jonas O, Roder D. Breech presentation in South Australia,1987–1989. Aust N Z J
Obstet Gynaecol 1993;33(1):17–21.[6] Rayl J, Gibson J, Hickok DE. A population-based case-control study of risk
factors for breech presentation. Am J Obstet Gynecol 1996;174:28–32.[7] Roberts CL, Algert CS, Peat B, Henderson-Smart D. Small fetal size: a risk factor
for breech birth at term. Int J Gynaecol Obstet 1999;67(1):1–8.[8] Fruscalzo A, Londero AP, Salvador S, Bertozzi S, Biasioli A, Della Martina M,
Driul L, Marchesoni D. New and old predictive factors for breech presentation:our experience in 14,433 singleton pregnancies and a literature review. JMatern Fetal Neonatal Med 2013, doi:10.3109/14767058.2013.806891 (Epubahead of print).
[9] Sherer DM, Spong CY, Minior VK, Salafia CM. Increased incidence of fetalgrowth restriction in association with breech presentation in pretermdeliveries <32 weeks. Am J Perinatol 1997;14(1):35–7.
[10] Devlieger H, Martens G, Bekaert A, Eeckels R. Standaarden van geboortege-wicht voor zwangerschapsduur voor de Vlaamse boreling. Tijdschr Geneesk2000;56:1–14 (article in Dutch).
[11] Albrechtsen S, Rasmussen S, Dalaker K, Irgens L. Reproductive career afterbreech presentation: subsequent pregnancy rates, interpregnancy interval andrecurrence. Obstet Gynecol 1998;92:345–50.
[12] Witkop CT, Zhang J, Sun W, Troendle J. Natural history of fetal position duringpregnancy and risk of nonvertex delivery. Obstet Gynecol 2008;111(4):875–80.
[13] Kok M, Cnossen J, Gravendeel L, van der Post J, Opmeer B, Mol BW. Clinicalfactors to predict the outcome of external cephalic version: a metaanalysis. AmJ Obstet Gynecol 2008;199(6):630.e1–7.
[14] Schrage R. Are more girls than boys born in breech presentation comparedwith head presentation?. Z Geburtshilfe Perinatol 1976;180(2)145–8 (article inGerman).
[15] Soernes T, Bakke T. The length of the umbilical cord in vertex and breechpresentations. Am J Obstet Gynecol 1986;154:1086–7.
[16] Ford JB, Roberts CL, Nassar N, Giles W, Morris JM. Recurrence of breechpresentation in consecutive pregnancies. BJOG 2010;117(7):830–6.
[17] Vendittelli F, Rivière O, Crenn-Hébert C, et al. Is a breech presentation at termmore frequent in women with a history of cesarean delivery?. Am J ObstetGynecol 2008;198:521.e1–6.
[18] Kalogiannidis I, Masouridou N, Dagklis T, Masoura S, Goutzioulis M, Prapas Y,Prapas N. Previous cesarean section increases the risk for breech presentationat term pregnancy. Clin Exp Obstet Gynecol 2010;37(1):29–32.
[19] Kean LH, Suwanrath C, Gargari SS, Sahota DS, James DK. A comparison of fetalbehaviour in breech and cephalic presentations at term. Br J Obstet Gynaecol1999;106:1209–13.
[20] Bartlett DJ, Okun NB, Byrne PJ, Watt JM, Piper MC. Early motor development ofbreech- and cephalic-presenting infants. Obstet Gynecol 2000;95(3):425–32.
[21] Park Y-S, Ryu K-Y, Shim S-S, Hoh J-K, Park M-I. Comparison of fetal heart ratepatterns using nonlinear dynamics in breech versus cephalic presentation atterm. Early Hum Dev 2013;89:101–6.
[22] Zlopasa G, Skrablin S, Kalafatic D, Banovic V, Lesin J. Uterine anomalies andpregnancy outcome following resectoscope metroplasty. Int J Gynecol Obstet2007;98:129–33.
[23] Stout MJ, Odibo AO, Graseck AS, Macones GA, Crane JP, Cahill AG. Leiomyomasat routine second-trimester ultrasound examination and adverse obstetricoutcomes. Obstet Gynecol 2010;116(5):1056–63.
[24] Sekulic S, Ilincic M, Radeka G, Novakov-Mikic A, Simic S, Podgorac J, Kekovic G.Breech presentation and the corneal-fundal location of the placenta. CroatMed J 2013;54:198–202.
[25] Romundstad LB, Romundstad PR, Sunde A, von Düring V, Skjaerven R, VattenLJ. Assisted fertilization and breech delivery: risks and obstetric management.Hum Reprod 2009;24(12):3205–10.
[26] Pandey S, Shetty A, Hamilton M, Bhattacharya S, Maheshwari A. Obstetric andperinatal outcomes in singleton pregnancies resulting from IVF/ICSI: asystematic reviewand meta-analysis.HumReprod Update 2012;18(5):485–503.