Embed Size (px)
Citation preview

July 2015
Drug saxagliptin and metformin hydrochloride (Komboglyze)
Indication
Saxagliptin/metformin hydrochloride (Komboglyze) is indicated for use as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus in the following situations: 1. In patients who are already treated with saxagliptin and
metformin or who are inadequately controlled on metformin alone.
2. In combination with a sulfonylurea in patients who are already treated with saxagliptin, metformin, and a sulfonylurea or who are inadequately controlled on metformin and a sulfonylurea alone.
3. In combination with premixed or long/intermediate acting insulin in patients who are already treated with saxagliptin, metformin, and premixed or long/intermediate acting insulin or who are inadequately controlled on metformin and premixed or long/intermediate acting insulin alone.
Listing request
For use in patients for whom insulin is not an option and who are already stabilized on therapy with metformin, a sulfonylurea, and saxagliptin, to replace the individual components of saxagliptin and metformin in these patients.
Manufacturer AstraZeneca Canada Inc.
Common Drug Review Fixed-Dose Combination Review Report

This report was prepared by the Canadian Agency for Drugs and Technologies in Health (CADTH). Through the Common Drug Review (CDR) process, CADTH undertakes reviews of drug submissions, resubmissions, and requests for advice, and provides formulary listing recommendations to all Canadian publicly funded federal, provincial, and territorial drug plans, with the exception of Quebec. The report contains an evidence-based clinical and/or pharmacoeconomic drug review, based on published and unpublished material, including manufacturer submissions; studies identified through independent, systematic literature searches; and patient-group submissions. In accordance with CDR Update — Issue 87, manufacturers may request that confidential information be redacted from the CDR Clinical and Pharmacoeconomic Review Reports. The information in this report is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. The information in this report should not be used as a substitute for the application of clinical judgment with respect to the care of a particular patient or other professional judgment in any decision-making process, nor is it intended to replace professional medical advice. While CADTH has taken care in the preparation of this document to ensure that its contents are accurate, complete, and up-to-date as of the date of publication, CADTH does not make any guarantee to that effect. CADTH is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in the source documentation. CADTH is not responsible for any errors or omissions or injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the information in this document or in any of the source documentation. This document is intended for use in the context of the Canadian health care system. Other health care systems are different; the issues and information related to the subject matter of this document may be different in other jurisdictions and, if used outside of Canada, it is at the user’s risk. This disclaimer and any questions or matters of any nature arising from or relating to the content or use (or misuse) of this document will be governed by and interpreted in accordance with the laws of the Province of Ontario and the laws of Canada applicable therein, and all proceedings shall be subject to the exclusive jurisdiction of the courts of the Province of Ontario, Canada. CADTH takes sole responsibility for the final form and content of this document, subject to the limitations noted above. The statements and conclusions in this document are those of CADTH and not of its advisory committees and reviewers. The statements, conclusions, and views expressed herein do not necessarily represent the views of Health Canada or any Canadian provincial or territorial government. Production of this document is made possible by financial contributions from Health Canada and the governments of Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and Labrador, Northwest Territories, Nova Scotia, Nunavut, Ontario, Prince Edward Island, Saskatchewan, and Yukon. You are permitted to make copies of this document for non-commercial purposes, provided it is not modified when reproduced and appropriate credit is given to CADTH. You may not otherwise copy, modify, translate, post on a website, store electronically, republish, or redistribute any material from this document in any form or by any means without the prior written permission of CADTH. Please contact CADTH’s Vice-President of Corporate Services at [email protected] with any inquiries about this notice or other legal matters relating to CADTH’s services.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
i
Common Drug Review July 2015
TABLE OF CONTENTS
ABBREVIATIONS ........................................................................................................................................... iii EXECUTIVE SUMMARY ................................................................................................................................. iv 1. INTRODUCTION ..................................................................................................................................... 1 2. RATIONALE AND PLACE IN THERAPY .................................................................................................... 2
2.1 Manufacturer-Submitted Information on Rationale (Verbatim) .................................................. 2 2.2 Manufacturer-Submitted Information on Place in Therapy (Verbatim) ....................................... 3 2.3 CDR Reviewer Comments ............................................................................................................. 4
3. BIOEQUIVALENCE ................................................................................................................................. 6
3.1 Manufacturer-Submitted Information on Bioequivalence (Verbatim) ......................................... 6 3.2 CDR Reviewer Comments ............................................................................................................. 9
4. HARMS ................................................................................................................................................ 10
4.1 Manufacturer-Submitted Information on Harms (Verbatim) ..................................................... 10 4.2 CDR Reviewer Comments ........................................................................................................... 10
5. COST INFORMATION ........................................................................................................................... 11
5.1 Manufacturer-Submitted Cost Information (Verbatim) ............................................................. 11 5.2 CDR Reviewer Comments ........................................................................................................... 12
6. CURRENT PATENT STATUS .................................................................................................................. 14
6.1 Manufacturer-Submitted Information Regarding Patent Status (Verbatim) ............................. 14 6.2 CDR Reviewer Comments ........................................................................................................... 14
APPENDIX 1: PATIENT INPUT SUMMARY .................................................................................................... 15 REFERENCES ................................................................................................................................................ 18

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
ii
Common Drug Review July 2015
Tables Table 1: Komboglyze Pivotal Trials Involving Saxagliptin 2.5 mg (Plus Metformin) Twice Daily .................. 6 Table 2: Supportive Pivotal Trials with Saxagliptin 5 mg Once Daily ............................................................ 7 Table 3: Summary Statistics for Saxaglitpin and Metformin Pharmacokinetic Parameters ......................... 8 Table 4: Cost Information – Comparison of the Daily, Monthly, and Annual Drug Costs (per Patient), Including Dispensing Fees and Mark-Up, for Komboglyze and Other DPP-4 Inhibitor/Metformin Combinations, Based on Ontario Drug Benefits Prices .................... 11 Table 5: Cost Comparison of Saxagliptin-Metformin FDC With Individual Components and With Metformin Plus Linagliptin or Sitagliptin FDCs (CDR Calculations) ............................................... 13 Table 6: Patent Status for Onglyza (Saxagliptin) ......................................................................................... 14 Figures Figure 1: WMD for Change in A1C Between FDC and CDT in Patients With Type 2 Diabetes Mellitus (8). .................................................................................................................................... 3 Figure 2: Organizations and Foundations That Made donations to the Canadian Diabetes Association between September 2012 and August 2013. ........................................................... 17

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
iii
Common Drug Review July 2015
ABBREVIATIONS
AE adverse event
AUC area under the curve
CDEC Canadian Drug Expert Committee
CDR CADTH Common Drug Review
CDT co-administered dual therapy
CI confidence interval
DPP-4 dipeptidyl peptidase-4
FDC fixed-dose combination
GI gastrointestinal
GLP-1 glucagon-like peptide-1
A1C glycated hemoglobin
LS least squares
MD mean difference
MPR medication-possession ratio
PD pharmacodynamic
PK pharmacokinetic
RCT randomized controlled trial
SAE serious adverse event
SD standard deviation
SU sulfonylurea

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
iv
Common Drug Review July 2015
EXECUTIVE SUMMARY
Many patients with type 2 diabetes mellitus do not achieve satisfactory glycemic control with a single drug and combining drugs from different classes is a recommended strategy to improve glycemic control. The addition of dipeptidyl peptidase-4 (DPP-4) inhibitors to metformin, with or without a sulfonylurea, is one of the newer strategies available to clinicians. Komboglyze is a fixed-dose combination (FDC) product containing saxagliptin, a DPP-4 inhibitor and metformin hydrochloride, a biguanide antidiabetic drug. The objective of this review was to evaluate the manufacturer-submitted evidence on the bioequivalence, safety, and costs of Komboglyze 2.5 per 500 mg, 2.5 per 850 mg, and 2.5 per 1,000 mg for the treatment of type 2 diabetes mellitus in adults inadequately controlled with diet and exercise plus metformin, or in patients already being treated with saxagliptin plus metformin, or in combination with a sulfonylurea.
Indication under review
Komboglyze is indicated as an adjunct to diet and exercise to improve glycemic control in adult patients with type 2 diabetes mellitus in the following situations: 1. In patients who are already treated with saxagliptin and metformin or who are inadequately controlled on
metformin alone. 2. In combination with a sulfonylurea in patients who are already treated with saxagliptin, metformin, and a
sulfonylurea or who are inadequately controlled on metformin and a sulfonylurea alone. 3. In combination with premixed or long/intermediate acting insulin in patients who are already treated with
saxagliptin, metformin, and premixed or long/intermediate acting insulin or who are inadequately controlled on metformin and premixed or long/intermediate acting insulin alone.
Listing criteria requested by sponsor
List for use in patients for whom insulin is not an option and who are already stabilized on therapy with metformin, a sulfonylurea, and saxagliptin to replace the individual components of saxagliptin and metformin in these patients.
FDC may improve adherence to type 2 diabetes mellitus therapy because of reduced pill burden, regimen complexity and costs.1 In Komboglyze, the doses of individual components allow for a range of dosing options often required for patients with type 2 diabetes mellitus. Collective evidence from studies provided by the manufacturer and the Health Canada Reviewer Report indicate that Komboglyze FDC tablets meet the recommended standard for bioequivalence with individually co-administered saxagliptin and metformin tablets.2 The FDC regimens appear to have tolerability and safety profiles similar to the individually co-administered components. Hence, evidence is available for the bioequivalence of Komboglyze to metformin and saxagliptin administered as separate tablets. These studies suggest that the FDC tablet is a rational treatment option in patients with type 2 diabetes mellitus who meet the indicated criteria. Patient adherence to medications for chronic conditions such as diabetes is often suboptimal. The FDC tablet may improve adherence by simplifying the medication regimen, which may result in better outcomes. Studies that formally assess adherence with Komboglyze compared with unfixed combination regimens of metformin and saxagliptin would be useful to determine whether this does, in fact, occur. As with other DPP-4

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
v
Common Drug Review July 2015
metformin products, further investigation of the issue of incidence of pancreatitis is needed to characterize the long-term safety profile of Komboglyze more comprehensively. At the current daily cost of $vvvvvvv, the saxagliptin-metformin FDC is less expensive than the individual components of saxagliptin and metformin and would therefore result in annual cost savings that range from $vvvvvvv to $vvvvvvv (depending on metformin dose) for patients already taking saxagliptin and metformin individually, or for whom saxagliptin and metformin combination therapy is deemed appropriate. The saxagliptin-metformin FDC is less expensive than other FDCs of metformin plus a DPP-4 (i.e., Janumet and Jentadueto).

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
1
Common Drug Review July 2015
1. INTRODUCTION
Komboglyze is a fixed-dose combination (FDC) product containing saxagliptin and metformin hydrochloride.3 Three tablet formulations are available, each containing 2.5 mg of saxagliptin with either 500 mg, 850 mg, or 1,000 mg of metformin. Saxagliptin is an orally active, selective, reversible, dipeptidyl peptidase-4 (DPP-4) inhibitor for the treatment of type 2 diabetes mellitus. Metformin hydrochloride is a biguanide antidiabetic drug recommended as a first-line treatment option for glycemic control in patients with type 2 diabetes mellitus, unless contraindicated or not tolerated.4,5 Komboglyze is indicated for use in adults with type 2 diabetes mellitus, as described below. Komboglyze is administered twice daily with meals. Dosage must be individualized on the basis of the patient’s current regimen and the effectiveness and tolerability of Komboglyze, with gradual dose escalation to reduce the gastrointestinal (GI) adverse effects due to metformin, while not exceeding the maximum recommended daily dose of 5 mg of saxagliptin and 2,000 mg of metformin.3
Indication under review
Komboglyze is indicated as an adjunct to diet and exercise to improve glycemic control in adult patients with type 2 diabetes mellitus in the following situations:
1. In patients who are already treated with saxagliptin and metformin or who are inadequately controlled on metformin alone.
2. In combination with a sulfonylurea in patients who are already treated with saxagliptin, metformin and a sulfonylurea, or who are inadequately controlled on metformin and a sulfonylurea alone.
3. In combination with premixed or long/intermediate acting insulin in patients who are already treated with saxagliptin, metformin, and premixed or long/intermediate acting insulin, or who are inadequately controlled on metformin and premixed or long/intermediate acting insulin alone.
Listing criteria requested by sponsor
List for use in patients for whom insulin is not an option and who are already stabilized on therapy with metformin, a sulfonylurea, and saxagliptin, to replace the individual components of saxagliptin and metformin in these patients.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
2
Common Drug Review July 2015
2. RATIONALE AND PLACE IN THERAPY
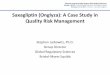
2.1 Manufacturer-Submitted Information on Rationale (Verbatim) Type 2 diabetes mellitus is a progressive disease that often requires treatment intensification (i.e., up-titration of dose or additional medications) for patients not meeting glycemic targets [1]. This leads patients to be treated with multiple diabetes medications to achieve glycemic control. Studies demonstrate that polypharmacy in diabetes can be associated with poor medication adherence and persistence (2,3,4,5). A systematic review of 23 studies revealed that 15% to 33% of patients did not take oral glucose-lowering therapy, and 36% to 38% did not take insulin, as prescribed (5). Several factors were associated with declining adherence, including polytherapy versus monotherapy regimens. Poor adherence has been associated with loss of glycemic control and increased risk of hospitalization and mortality, as well as increased costs in patients with type 2 diabetes mellitus (2,3,4,6,7). The use of a fixed-dose combination (FDC) product, defined as a formulation of two or more active ingredients combined in a single dosage form, is one strategy to improve adherence in type 2 diabetes mellitus, as it is intended to reduce pill burden, regimen complexity, and costs (8,9). In addition to Komboglyze, Janumet (sitagliptin and metformin), and Jentadueto (linagliptin and metformin) are FDC products containing metformin and a DPP-4 inhibitor approved for use in Canada; however, Janumet is the only FDC product currently reimbursed by private formularies in Canada. Several systematic reviews have demonstrated significantly improved adherence rates with the use of FDC therapies compared with co-administered dual therapy (CDT) [8,9,10]. For example, results of a meta-analysis of observational studies involving 70,573 patients with type 2 diabetes mellitus showed that the pooled mean difference (MD) in the medication-possession ratio (MPR) was 8.6% (95% confidence interval [CI], 1.6 to 15.6; P = 0.0163) [8]. The authors also noted that A1C reduction improved in patients treated with FDC versus CDT therapy (MD –0.53%; 95% CI, –0.78 to –0.28%; P <0.0001;
I2 = 52.4%) (Figure 1) [8]. Collectively, evidence demonstrating improved adherence and outcomes (e.g., A1C) strongly support the use of FDCs in diabetes clinical practice. Therefore, increasing the availability of FDC therapies to patients in Canada, through efforts made by payers and physicians, is anticipated to provide an important opportunity to optimize clinical and economic benefits in type 2 diabetes mellitus patients.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
3
Common Drug Review July 2015
FIGURE 1: WMD FOR CHANGE IN A1C BETWEEN FDC AND CDT IN PATIENTS WITH TYPE 2 DIABETES
MELLITUS (8).
A1C = glycated hemoglobin; AE = adverse event; CDT = co-administered dual therapy; CI = confidence interval; FDC = fixed-dose combination; HbA1c (typically written as A1C) = glycated hemoglobin; WMD = weighted mean difference.
2.1.1 Pharmacological Rationale for This Combination Many patients with type 2 diabetes mellitus do not achieve satisfactory glycemic control with a single drug and there is a need for effective combination therapies. Saxagliptin and metformin hydrochloride are two approved antihyperglycemic drugs, which exert improved glycemic control through complementary mechanisms of action. Komboglyze is a fixed-dose combination (FDC) tablet that contains saxagliptin (a potent, selective, reversible, competitive DPP-4 inhibitor) and metformin hydrochloride (antihyperglycemic drug). Komboglyze targets three core defects of type 2 diabetes mellitus: decreased insulin synthesis and release, increased hepatic glucose production, and decreased insulin sensitivity. The saxagliptin component of Komboglyze exerts its actions by inhibiting DDP-4 and enhancing the concentration of incretin hormones, including glucagon-like peptide-1 (GLP-1). This allows for lowered blood-sugar levels after and between meals, decreased hepatic glucose production, decreased intestinal glucose absorption, and increased peripheral glucose uptake and utilization for improved insulin sensitivity and glycemia. The metformin component of Komboglyze improves glucose tolerance in patients by lowering both basal and post-prandial plasma glucose. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization.
2.2 Manufacturer-Submitted Information on Place in Therapy (Verbatim) The option of an FDC product is important in patients requiring DPP-4 inhibitors. This is because DPP-4 inhibitors are often used as second- and third-line therapy and therefore involve patients on more complex treatment regimens (i.e., dosing titration and multiple therapies) who are at risk of poor adherence and associated consequences. In addition to Komboglyze, Janumet (sitagliptin and metformin) and Jentadueto (linagliptin and metformin) are FDC products containing metformin and a

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
4
Common Drug Review July 2015
DPP-4 inhibitor approved for use in Canada, however, Janumet is the only FDC product in Canada that is currently reimbursed. In June of 2010, Janumet received a positive Canadian Drug Expert Committee (CDEC) recommendation for “use in patients for whom insulin is not an option and who are already stabilized on therapy with metformin, an SU [sulfonylurea], and sitagliptin to replace the individual components of sitagliptin and metformin in these patients” (16). This listing criterion therefore includes replacing free-dose sitagliptin and metformin with Janumet, as well as replacing metformin with Janumet in patients stabilized on metformin alone and who require another option such as DPP-4 inhibitors. The reimbursement of FDCs therefore provides physicians with options for optimizing adherence and minimizing pill burden in patients requiring DPP-4 inhibitor therapy. The availability of more than one type of DPP-4 inhibitor FDC product is critical. As individualized responses to drugs within the same class can often vary, having choices can assist physicians with optimizing patient response and tolerability when managing the more complex and progressive profile of patients requiring multiple therapy options for type 2 diabetes mellitus. Therefore, the use of Janumet provides an FDC option for patients stabilized on the free-dose form of sitagliptin and metformin, and Komboglyze provides an option for patients stabilized on the free-dose form of saxagliptin and metformin. Neither FDC is thus intended to be used in patients already stabilized on another DPP-4 inhibitor. In addition to switching from the free-dose co-administration of a DPP-4 inhibitor and metformin, these FDC products provide an option for those inadequately controlled on a maximally tolerated dose of metformin alone. Komboglyze offers the comprehensive range of dosing options often required for patients with type 2 diabetes mellitus. The range of metformin daily doses available with the use of Komboglyze (i.e., 1,000 mg, 1,700 mg, and 2,000 mg) encompasses the majority of the options indicated for metformin use (17). This range allows for low-dose metformin (i.e., 500 mg twice daily.) in patients with low tolerability for metformin side effects, as well as a higher-dose metformin (i.e., 1,000 mg twice daily.) in patients having more advanced disease who are uncontrolled on lower metformin doses. The total daily dose of saxagliptin provided in Komboglyze is 5 mg (2.5 mg twice daily.). Therefore, increasing the dose of the metformin component does not unnecessarily alter the dosing of the saxagliptin component. The dosing options available with Komboglyze are also aligned with Janumet, which offers a consistent daily dose of 100 mg for sitagliptin (i.e., 50 mg twice daily.), with the three twice daily. dosage forms for metformin (i.e., 500 mg, 850 mg, and 1,000 mg).
2.3 CDR Reviewer Comments Clinical guidelines advocate lifestyle interventions (nutrition therapy and physical activity) with or without metformin at diagnosis of type 2 diabetes mellitus.5 When these initial interventions are not enough to produce adequate glycemic control after two to three months, initiating metformin is recommended unless contraindicated or not tolerated.5 Monotherapy will generally result in reducing A1C by about 0.5% to 1.5% after three to six months, depending on the drug selected and baseline A1C.5 When diet, exercise, and metformin (at an optimal dose) are not enough to meet glycemic targets, combination therapy may be needed. Selecting a second antihyperglycemic drug to add depends on several patient and drug characteristics including comorbidities, risk of hypoglycemia, overweight or obesity concerns, efficacy in reducing A1C, contraindications, and cost. A third drug from a different class or intensification of insulin therapy is recommended if targets are not being met with dual therapy in combination with lifestyle changes.5

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
5
Common Drug Review July 2015
CADTH has issued optimal therapy recommendations based on reviews of the clinical and cost-effectiveness of second and third-line drugs for diabetes, stating that sulfonylureas should be used as second-line therapy for most patients inadequately controlled on metformin alone, and that neutral protamine Hagedorn insulin should be used for most patients who are inadequately controlled on metformin and a sulfonylurea.6,7 Saxagliptin belongs to the DPP-4 inhibitor class and the efficacy, safety, and cost-effectiveness have been evaluated by the CADTH Common Drug Review (CDR).8 CDEC recommended that saxagliptin (Onglyza) be listed as a third drug added on to metformin and a sulfonylurea in patients with inadequate glycemic control on metformin and a sulfonylurea and for whom insulin is not an option.9 Hence, a patient with inadequately controlled type 2 diabetes mellitus is likely to receive a rather complex treatment regimen at the time saxagliptin is initiated. Polypharmacy has been associated with patient non-compliance. The primary advantage of the FDC product is patient convenience because of reduced pill burden and simplification of the medication regimen. Increasing patient convenience is expected to promote patients’ acceptance for and adherence to therapy, thereby potentially resulting in improved outcomes.1 Each of the three different tablet formulations of Komboglyze contains a submaximal dose of the individual components, which allows for dose adjustment depending on patient response and to manage adverse effects. Based on product monographs, it is recommended that single-entity immediate-release metformin be given in doses of 500 mg three or four times per day, or 850 mg two or three times per day respectively.10 However, in clinical practice, twice-daily dosing is most common, regardless of tablet strength. It is suggested that initial treatment begin at 1,000 mg daily, with gradual dose escalation (500 mg per week) up to a maximum of 2,000 mg daily.11 The recommended dose for saxagliptin is 5 mg once daily with normal renal function. The FDC tablet of saxagliptin plus metformin provides the same total daily dose of saxagliptin, although it is divided into a 2.5 mg twice-daily regimen. It has been demonstrated that saxagliptin 2.5 mg given twice daily is bioequivalent to 5 mg given once daily (see following sections).2,3 Therefore, the recommended dosing of the FDC meets both the daily requirements of saxagliptin and the flexibility of metformin dosing available in a free-dose co-administered regimen.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
6
Common Drug Review July 2015
3. BIOEQUIVALENCE
3.1 Manufacturer-Submitted Information on Bioequivalence (Verbatim) Several randomized controlled trials have evaluated the individual components of Komboglyze (saxagliptin 2.5 mg twice daily with metformin), as well as the Komboglyze FDC tablet. Collectively, these trials have demonstrated the therapeutic equivalence of saxagliptin 2.5 mg twice daily to saxagliptin 5 mg once daily; the efficacy and safety of saxagliptin 2.5 mg twice daily twice daily in combination with metformin; and the bioequivalence of the FDC tablet (saxagliptin 2.5 mg and metformin 500 mg) compared with individually administered saxagliptin and metformin (Table 1 and Table 2).
TABLE 1: KOMBOGLYZE PIVOTAL TRIALS INVOLVING SAXAGLIPTIN 2.5 MG (PLUS METFORMIN) TWICE DAILY
Trial Trial Focus Patients Comparators/Dosing Key End Points
CV181-091 PK and PD Saxa b.i.d.
Healthy patients without diabetes
Saxa 2.5 mg b.i.d. (n = 12)
Cmax, Tmax, AUC, Imax, AUEC; trough (DPP-4) (7 days, multiple dose)
CV181-152 PK and PD Saxa b.i.d. vs. q.d.
Healthy patients without diabetes
Saxa 2.5 mg b.i.d. Saxa 5 mg q.d.
(n = 16; each treatment once)
Cmax, Tmax, AUC, Imax, AUEC; trough (DPP-4) (7 days, multiple dose)
CV181-118 Bioequivalence FDC Komboglyze
vs. free-form tablets
Healthy patients without diabetes
27 patients (each treated once) Fed state (single dose) Saxa 2.5 mg plus met
500 mg Saxa 2.5 mg plus met
500 mg FDC Fasted state (single dose) Saxa 2.5 mg plus met
500 mg Saxa 2.5 mg plus met
500 mg FDC
Bioequivalence: AUC, Cmax (single dose)
CV181-080 Efficacy and safety Saxa plus met Saxa b.i.d.
Inadequate glycemic control on met; A1C > 7% and < 10%
Saxa 2.5 mg b.i.d. plus met (n = 74)
Placebo b.i.d. plus met (n = 86)
Primary: Δ A1C (12 weeks)
AUC = area under the curve; AUEC = area under the effect curve; b.i.d. = twice daily; Cmax = maximum concentration; DPP-4 = dipeptidyl peptidase-4 inhibitor; FDC = fixed-dose combination; Imax = maximum inhibition; met = metformin; PD =
pharmacodynamic; PK = pharmacokinetic; q.d. = once daily; saxa = saxagliptin; Tmax = time after administration when the
maximum plasma concentration is reached.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
7
Common Drug Review July 2015
TABLE 2: SUPPORTIVE PIVOTAL TRIALS WITH SAXAGLIPTIN 5 MG ONCE DAILY
Trial Trial Focus Patients Comparators/Dosing Key Endpoints
CV181-014 Efficacy and safety
Various doses of saxa plus met
Saxa q.d.
Inadequate glycemic control on met; A1C > 7% and < 10%;
Saxa 2.5 mg q.d. plus met (n = 192)
Saxa 5 mg q.d. plus met (n=191)
Saxa 10 mg q.d. plus met (n=181)
Placebo q.d. plus met (n=179)
Primary: Δ A1C at 24 weeks; data out to 102 weeks
D1680L00006 Efficacy and safety
Saxa q.d. plus met and SU
Inadequate glycemic control; A1C > 7% and < 10%; n = 257
Saxa 5 mg q.d. plus met plus SU (n = 129)
Placebo q.d. plus met plus SU (n = 128)
Primary: Δ A1C at 24 weeks
met = metformin; q.d. = once daily; saxa = saxagliptin; SU = sulfonylureas.
Saxagliptin has uncomplicated pharmacokinetics (PKs) with a variability typical of most small molecules. Metformin has non-linear PK (less-than-proportional increase in exposure with increase in dose), so it is classified as complicated PK, but not highly variable. An overview of the findings of these clinical studies is provided below: CV181-091 was an open-label, non-randomized study of 12 healthy patients that characterized the
steady-state PK and pharmacodynamic (PD) of the saxagliptin-dosing regimen used in Komboglyze (i.e., 2.5 mg saxagliptin twice daily) (11). Results showed that timing of tablet administration did not influence absorption and plasma exposure and that saxagliptin strongly inhibited plasma DPP-4 activity when given twice daily.
CV181-152 compared the steady-state PK and PD of the 2.5 mg saxagliptin twice daily. dosing regimen used in Komboglyze with a 5 mg saxagliptin q.d. regimen in an open-label, randomized crossover study with 16 healthy patients over 7 days (12). Over the study period, results showed that 2.5 mg saxagliptin twice daily. was equivalent to saxagliptin 5 mg once daily with respect to total daily exposure. DPP-4 inhibition was also equivalent between the two dosing regimens.
CV-181-118 was an open-label, randomized study in fasted and fed patients (n = 27 healthy) that assessed the bioequivalence of a single dose of an FDC tablet of 2.5 mg saxagliptin and 500 mg metformin relative to 2.5 mg saxagliptin and 500 mg metformin tablets administered separately (13). Results showed that the FDC tablet was bioequivalent to the 2.5 mg saxagliptin and 500 mg metformin tablets administered together for patients in both the fasted and fed states.
CV-181-080 was a double-blind, randomized, 12-week study of 152 patients with inadequate glycemic control on metformin alone that assessed the efficacy and safety of saxagliptin 2.5 mg twice daily. compared with placebo, each in combination with metformin (14). This study showed a statistically significant reduction for mean change in A1C from baseline to week 12 in the saxagliptin group, compared with placebo (i.e., a placebo-adjusted difference of –0.34; P = 0.0063). In addition, other measures of glycemic control (e.g., percentage with A1C < 7.0%) were also improved with saxagliptin. Saxagliptin 2.5 mg twice daily. added to metformin was also well tolerated.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
8
Common Drug Review July 2015
D168L00006: This was a 24-week, multi-centre, randomized, double-blind trial in 257 patients with type 2 diabetes mellitus with inadequate glycemic control comparing saxagliptin 5 mg once daily versus placebo, each as an add-on therapy to a stable dose of metformin and an SU (15). Results showed that saxagliptin was superior to placebo in lowering A1C from baseline to week 24 (i.e., a placebo-adjusted difference of –0.66%; 95% CI, –0.86% to –0.47%; P < 0.0001). Further, a lower proportion of patients treated with saxagliptin experienced an adverse event compared with placebo. This trial provides supportive evidence for Komboglyze in third-line use (i.e., metformin, SU, and saxagliptin).
The FDC tablet of 2.5 mg saxagliptin and 500 mg metformin was bioequivalent to the separately administered 2.5 mg saxagliptin and 500 mg metformin tablets for patients in the fasted and fed states. Both comparators were safe and tolerated by healthy patients.
TABLE 3: SUMMARY STATISTICS FOR SAXAGLITPIN AND METFORMIN PHARMACOKINETIC PARAMETERS
Parameter (Unit)
Treatment N Geometric LS Mean
Ratio (%) of Geometric LS Means (B/A or D/C) and
90% CI of the Ratio
Saxagliptin
AUC0-t (ng·h/mL) A Free dose (fasted) 27 50.34 102.34 (97.96, 106.91)
B FDC (fasted) 26 51.52
C Free dose (fed) 26 59.10 99.78 (96.61, 103.05)
D FDC (fed) 26 58.97
AUC0-inf (ng·h/mL)
A Free dose (fasted) 27 52.23 102.64 (98.31, 107.16)
B FDC (fasted) 26 53.61
C Free dose (fed) 26 61.39 99.22 (96.48, 102.04)
D FDC (fed) 26 60.91
Cmax (ng/mL) A Free dose (fasted) 27 10.52 109.53 (102.67, 116.85)
B FDC (fasted) 26 11.52
C Free dose (fed) 26 12.70 100.37 (85.70, 117.56)
D FDC (fed) 26 12.75
Metformin
AUC0-t (ng·h/mL) A Free dose (fasted) 27 8,045 98.27 (91.96, 105.03)
B FDC (fasted) 26 7,906
C Free dose (fed) 26 7,506 101.82 (96.10, 107.88)
D FDC (fed) 26 7,643
AUC0-inf (ng·h/mL)
A Free dose (fasted) 26 8,150 99.04 (92.90, 105.59)
B FDC (fasted) 26 8,072
C Free dose (fed) 25 7,606 102.77 (96.82, 109.09)
D FDC (fed) 25 7,817
Cmax (ng/mL) A Free dose (fasted) 27 1,059 99.02 (91.29, 107.41)
B FDC (fasted) 26 1,049
C Free dose (fed) 26 810 100.21 (96.86, 103.76)
D FDC (fed) 26 812
AUC = area under the curve; CI = confidence interval; Cmax = maximum concentration; FDC = fixed-dose combination; LS = least squares. Note: Treatment A: single-dose 2.5 mg saxagliptin and 500 mg metformin tablets administered together in the fasted state. Treatment B: single-dose 2.5 mg saxagliptin/500 mg metformin FDC tablet administered in the fasted state Treatment C: single-dose 2.5 mg saxagliptin and 500 mg metformin tablets administered together in the fed state Treatment D: single-dose 2.5 mg saxagliptin/500 mg metformin FDC tablet administered in the fed state.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
9
Common Drug Review July 2015
3.2 CDR Reviewer Comments The manufacturer provided an overview of findings from four pivotal studies (CV-181-091, CV-181-152, CV-181-118, and CV-181-080) in support of using a saxagliptin-metformin FDC in place of individually administered saxagliptin and metformin for glycemic control in type 2 diabetes mellitus patients.3 The pharmacokinetic characteristics of saxagliptin-metformin FDC tablets have been tested against the single tablets administered together in a phase I study of healthy volunteers. In study CV-181-118, the saxagliptin-metformin FDC was shown to be bioequivalent to the individual drugs administered separately in accordance with standard criteria for bioequivalence in 27 healthy participants in both fasted and fed states; however, only the fixed-dose 2.5 per 500 mg tablet was compared with the equivalent doses of the individual components; the 2.5 per 850 mg and 2.5 per 1,000 mg dosage forms were not evaluated. One potential concern with the FDC tablet is the alternative dosing of saxagliptin 2.5 mg twice daily rather than 5 mg once daily. CV-181-091 was an open-label, non-randomized study of 12 healthy participants. The study showed that saxagliptin 2.5 mg twice daily achieved plasma DPP-4 inhibition and that twice-daily administration did not affect absorption and plasma concentrations of saxagliptin. Another study (CV-181-152) comparing twice-daily saxagliptin 2.5 mg with once-daily 5 mg for 7 days in 16 healthy participants demonstrated equivalency between the two dosing regimens with respect to total daily exposure and DPP-4 inhibition. The Health Canada reviewer’s report2 accepted that saxagliptin 2.5 mg given twice daily for 7 days was comparable to a 5 mg dose given once daily for 7 days, with similar 24-hour exposure determined by area under the curve. The adjusted ratio of geometric least square (LS) means vvvvvvvv and the 90% confidence intervals (CIs) of the ratios vvvvvvv vvv vvvvvvv were within the acceptance range of 80% to 125% for bioequivalence.2 Both dosage regimens also resulted in a comparable pharmacodynamic response with mean maximum DPP-4 inhibition (Imax) at approximately vvv for both treatments. Average DPP-4 inhibition was reported as vvvvvvv, and the 90% CI of the ratio was vvvvvvv vv vvvvvvvv Peak DPP-4 inhibition (Imax) was reported as vvvvvvvv with 90% CI of the ratio of vvvvvv vv vvvvvvv.2 From these reported results, the pharmacokinetic and pharmacodynamics of saxagliptin 2.5 mg appear to be similar to saxagliptin 5 mg given once daily. Also, the FDC tablet (saxagliptin 2.5 mg and metformin 500 mg) has been shown to be bioequivalent to the individual drugs administered separately in accordance with standard criteria for bioequivalence.2 Therefore, administration of the two drugs in a FDC did not materially affect the pharmacokinetics of either drug.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
10
Common Drug Review July 2015
4. HARMS
4.1 Manufacturer-Submitted Information on Harms (Verbatim) CV181-118 sought to demonstrate the bioequivalence of the Komboglyze FDC tablet of 2.5 mg saxagliptin and 500 mg metformin relative to separately co-administered (i.e., free-dose combination) 2.5 mg saxagliptin and 500 mg metformin (Glucophage) tablets given orally as a single dose in the morning to fasted or fed healthy patients (18). This was an open-label, randomized, four-period, four-treatment, 4-way crossover, single-dose study, where 28 patients were planned, 27 patients were dosed for seven days per treatment, and 26 patients completed the study. Regarding safety endpoints, single, oral doses of the FDC tablet and the co-administered 2.5 mg saxagliptin and 500 mg metformin tablets were safe and well tolerated in healthy patients in both fasted and fed states. There were no deaths, serious adverse events (SAEs), or discontinuations due to AEs. Most AEs were mild in severity and resolved without treatment. Nine (33.3%) patients reported at least 1 AE. Of the 9 patients with AEs, 6 patients (22.2%) reported at least 1 AE (e.g., diarrhea, nausea, and abdominal distension) that was considered to be related to the study drug. AEs related to the study drug were reported by 5 patients (19.2%) receiving 2.5 mg saxagliptin and 500 mg metformin tablets administered together in the fed state.
4.2 CDR Reviewer Comments The combined use of free-dose form saxagliptin and metformin has been widely characterized in the medical literature as well tolerated and safe.2,12 The AE and SAE profiles of saxagliptin were reported in a randomized controlled clinical trial to be similar to placebo.13 Common adverse events of metformin include gastrointestinal effects consistent with information presented by the manufacturer (diarrhea, nausea, and abdominal distension).14 It should be noted that patients in the study (CV181-118) for which harms were reported by the manufacturer were dosed for seven days per treatment. This period is typically not long enough to detect important adverse events in a patient population receiving therapy for a chronic illness; however, this limitation is somewhat mitigated by the range of evidence demonstrating a favourable safety profile for the free-dose combination of saxagliptin and metformin. The Komboglyze product monograph15 reports a finding in a placebo-controlled clinical study in which patients who received saxagliptin 5 mg as an add-on to metformin and a sulfonylurea had less incidence (2.3%) of SAEs than those who received placebo as an add-on (5.5%). The respective rates of discontinuation of therapy due to adverse events were 0.8% and 2.3% of patients; hypoglycemia, hypertension, and diarrhea were the most commonly reported adverse events, regardless of causality.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
11
Common Drug Review July 2015
5. COST INFORMATION
5.1 Manufacturer-Submitted Cost Information (Verbatim) TABLE 4: COST INFORMATION – COMPARISON OF THE DAILY, MONTHLY, AND ANNUAL DRUG COSTS
(PER PATIENT), INCLUDING DISPENSING FEES AND MARK-UP, FOR KOMBOGLYZE AND OTHER DPP-4
INHIBITOR/METFORMIN COMBINATIONS, BASED ON ONTARIO DRUG BENEFITS PRICES
Drug / Comparator Strength Daily Frequency
Unit Cost
Daily Drug Cost
a
Monthly Drug Cost
b
Annual Drug Cost
c
Fixed-Dose Combination
Komboglyze (saxagliptin and metformin)
2.5 mg/500 mg 2.5 mg/850 mg
2.5 mg/1,000 mg
b.i.d. b.i.d. b.i.d.
$vvvvvv $vvvvvv $vvvvvv
$vvvvvv $vvvvvv $vvvvvv
$vvvvvvv $vvvvvvv $vvvvvvv
$vvvvvvvvvv $vvvvvvvvvv $vvvvvvvvvv
Janumet (sitagliptin and metformin)
50 mg/500 mg 50 mg/850 mg
50 mg/1,000 mg
b.i.d. b.i.d. b.i.d.
$1.6015 $1.6015 $1.6015
$3.7466 $3.7466 $3.7466
$112.3972 $112.3972 $112.3972
$1,367.4993 $1,367.4993 $1,367.4993
Free-Dose Combination of Other DPP-4 Inhibitor and Metformin Combinations
Sitagliptin 100 mg q.d. $2.9527 $3.4762 $104.2875 $1,268.8310
Linagliptin 5 mg q.d. $2.5500 $3.0413 $91.2400 $1,110.0867
Metformin
500 mg 850 mg
d
500 mg
b.i.d. b.i.d. q.i.d.
$0.0587 $0.1075 $0.0587
$0.4141 $0.5195 $0.5409
$12.4238 $15.5860 $16.2275
$151.1557 $189.6297 $197.4348
Sitagliptin plus metformin
100 mg q.d. + 500 mg b.i.d. 100 mg q.d. + 850 mg b.i.d. 100 mg q.d. + 500 mg q.i.d.
– $3.8904 $3.9958 $4.0172
$116.7112 $119.8734 $120.5150
$1,419.9868 $1,458.4607 $1,466.2658
Linagliptin plus metformin
5 mg q.d. + 500 mg b.i.d. 5 mg q.d. + 1,700 mg b.i.d. 5 mg q.d. + 2,000 mg b.i.d.
– $3.4555 $3.5609 $3.5823
$103.6638 $106.8260 $107.4675
$1,261.2424 $1,299.7163 $1,307.5215
AB = Alberta; BC = British Columbia; b.i.d = twice daily; NLPDP = Newfoundland and Labrador Prescription Drug Program; q.d. = once daily; q.i.d. = four times daily; SK = Saskatchewan. a Daily cost with markup of 8% and dispensing fee (i.e., $8.62/30 days).
b Daily costs are multiplied by 30 days to get monthly cost.
c Daily costs are multiplied by 365 days to get annual cost.
d Metformin 850 mg is not a benefit covered by Ontario Drug Benefits; therefore, the cost for this treatment (0.1169/unit)
reflects the average price among public plans (i.e., BC, AB, SK, NLPDP).
When compared with the free-dose combination of saxagliptin and metformin, calculations of the drug costs for each of the comparators indicate that Komboglyze provides a cost saving for all dosing regimens, considering drug costs with mark-up and dispensing fees (see Table 2A and Table 2B in section 3.01 of the comprehensive pharmacoeconomic model of the Komboglyze submission). When considering mark-up and dispensing fees, the cost savings range from $vvvvvvv to $vvvvvvv per patient per day, an annual cost saving of $vvvvvvv to $vvvvvvv) (see Table 2A and Table 2B), depending on the dosing regimen utilized. Considering all metformin regimens collectively, approximately vv% of the cost savings generated by Komboglyze is due to lower unit cost and vv% of the cost savings is due to the reduction of dispensing fees.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
12
Common Drug Review July 2015
When considering the average expected utilization of the three daily regimen options, Komboglyze provides a monthly cost saving of $vvvvvvv per patient (i.e., an annual cost saving of $vvvvvvv per patient). Again, the majority of the cost savings (vv%) generated by Komboglyze is due to the lower unit cost. For the total daily cost of a triple-therapy regimen, the daily cost of a sulfonylurea ranges from $0.346 to $0.736 (including mark-up and dispensing fees). When a sulfonylurea is used in combination with Komboglyze, the total cost of daily therapy ranges from $vvvvvvv to $vvvvvvv. Please refer to section 3.01 of the comprehensive pharmacoeconomic model of the Komboglyze submission for further details of the analysis.
5.2 CDR Reviewer Comments While patients who are prescribed a saxagliptin-metformin FDC would indeed incur a single dispensing fee (rather than two such fees each time a claim was made), the manufacturer’s assumption that each claim would be for 30 days could potentially overestimate the savings that could be realized by this reduction in fees. This is because some patients (e.g., seniors in Ontario) can claim for longer periods of time (up to 100 days). Considering the aforementioned limitation, CDR reviewers recalculated the cost of treatments assuming that claims range from 30 to 100 days. Consequently, the scenario considered by CDR reviewers to be most likely was one in which the saxagliptin-metformin FDC produced annual costs savings of $vvvvvvv to $vvvvvvv per patient per year compared with the individual components (Table 5). The manufacturer did not include a linagliptin-metformin FDC (Jentadueto) as a comparator because it is not reimbursed by any public plans in Canada; however, CDEC issued a positive recommendation for Jentadueto in October 2013,16 and it is likely to be a valid comparator in the near future. Consequently, CDR reviewers considered Jentadueto to be an appropriate comparator to the saxagliptin-metformin FDC. Based on the wholesale price of Jentadueto ($2.57 per patient per day),17 CDR reviewers calculated the cost difference between the saxagliptin-metformin FDC and Jentadueto. Based on this analysis, reimbursement of the saxagliptin-metformin FDC would produce an annual cost saving relative to Jentadueto of $vvvvvvv (vvv%) (Table 5).

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
13
Common Drug Review July 2015
TABLE 5: COST COMPARISON OF SAXAGLIPTIN-METFORMIN FDC WITH INDIVIDUAL COMPONENTS AND WITH
METFORMIN PLUS LINAGLIPTIN OR SITAGLIPTIN FDCS (CDR CALCULATIONS)
Drug /Comparator Strength Unit Price
a ($)
Annual Drug
Cost ($)
Annual Drug Cost ($) (plus markup/fee)
b,c
Annual Savings With Komboglyze ($)
c
Metformin (generic) 500 mg 850 mg
500 mg b.i.d
0.06
0.11e
0.06
42.85 78.48 85.70
77.74 to 151.16 116.22 to 189.63 124.02 to 197.43
NA
Saxagliptin 5 mg 2.84 1,036.13 1,150.48 to 1,223.89 NA
Saxagliptin plus metformin (individual components)
5/500 mg 5/850 mg
5/1,000 mg
NA 1,078.98 1,114.60 1,121.83
1,228.22 to 1,375.05 1,266.69 to 1,413.52 1,274.50 to 1,421.33
vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv
Saxagliptin-metformin FDC (Komboglyze)
2.5/500 mg 2.5/850 mg
2.5/1,000 mg
vvvvvvd
vvvvvvv vvvvvvvv–vvvvvvvv Ref.
Sitagliptin 100 mg 2.95 1,077.74 1,195.42 to 1,268.83 NA
Sitagliptin plus metformin (individual components)
100/500 mg 100/850 mg 100/500 mg
NA 1,120.59 1,156.21 1,163.44
1,273.16 to 1,419.99 1,311.63 to 1,458.46 1,319.43 to 1,466.27
vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv
Sitagliptin-metformin FDC (Janumet)
50/500 mg 50/850 mg
50/1,000 mg
1.60 1,169.10 1,294.08 to 1,367.50 0
Linagliptin 5 mg 2.55 930.75 1,036.67 to 1,110.09 NA
Linagliptin plus metformin (individual components)
5/500 mg 5/850 mg 5/500 mg
NA 973.60 1,009.23 1,016.45
1,114.42 to 1,261.24 1,152.89 to 1,299.72 1,160.69 to 1,307.52
vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv vvvvvvv to vvvvvvv
Linagliptin-metformin FDC (Jentadueto)
2.5/500 mg 2.5/850 mg
2.5/1,000 mg
1.28f
937.54 1,044.01 to 1,117.42 vvvvvvv
AB = Alberta; BC = British Columbia; b.i.d. = twice daily; CDR = CADTH Common Drug Review; FDC = fixed-dose combination; NA = not applicable; NLPDP = Newfoundland and Labrador Prescription Drug Program; SK = Saskatchewan.
a Prices are from the Ontario Drug Benefit Formulary (May 2013) unless otherwise indicated.
b Based on Ontario Drug Benefits rules of 8% mark-up and $8.62 dispensing fee.
c Assumes claims range from 30 to 100 days; thus, dispensing fees would be paid 12.16667 to 3.65 times per year. CDR
calculated the annual drug cost assuming claims every 100 days; the manufacturer provided the cost assuming claims every 30 days. d
Manufacturer-submitted price. e Metformin 850 mg is not a benefit covered by the Ontario Drug Benefits; therefore, the unit cost was based on the average
price among public plans (i.e., BC, AB, SK, NLPDP). f McKesson Canada wholesale price (January 2014).

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
14
Common Drug Review July 2015
6. CURRENT PATENT STATUS
6.1 Manufacturer-Submitted Information Regarding Patent Status (Verbatim)
TABLE 6: PATENT STATUS FOR ONGLYZA (SAXAGLIPTIN)
Patent Granted Expiry Date
2402894 April 17, 2012 March 5, 2021
2568391 May 14, 2013 May 26, 2025
Data protection ends on September 14, 2017.
The patent for metformin components has already expired.
6.2 CDR Reviewer Comments No comments.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
15
Common Drug Review July 2015
APPENDIX 1: PATIENT INPUT SUMMARY
This section was summarized by CADTH Common Drug Review staff based on the input provided by patient groups. It has not been systematically reviewed. It has been reviewed by the submitting patient group. 1. Brief Description of Patient Group(s) Supplying Input The Canadian Diabetes Association (CDA) provides education and services, advocates on behalf of people with diabetes, supports research, and translates research into practical applications. The Association is supported in its efforts by a community-based network of volunteers, employees, health care professionals, researchers, and partners. The CDA solicits and receives unrestricted educational grants from manufacturers or vendors of medications, supplies, and devices for diabetes and its complications. See Figure 2 at the end of this appendix for list of funders. These funds are used to help the CDA support community programs and services for people with diabetes and to fund research and advocacy across Canada. The CDA declared no conflicts of interest in the preparation of this submission. 2. Condition and Current Therapy-Related Information The information in this submission was gathered through a patient survey distributed through physicians involved in Komboglyze clinical trials in Canada and posted on Facebook and Twitter. There were 232 responses to the survey and 139 respondents completed the full questionnaire. Of the 232 survey respondents, 87.9% identified themselves as living with type 2 diabetes, 6.1% as caregivers for people with type 2 diabetes, 2.7% as having type 1 diabetes, and 3.4% as “other”. One hundred and seventy participants had taken medication for diabetes. When asked about DDP-4 inhibitors, 93 people reported never taking them and 38 had direct experience with them, with 69% currently using the treatment. The remainder of respondents had discontinued use of DDP-4 inhibitors for various reasons, including the conclusion of the clinical trial. For the purposes of the submission, responses from patients who have taken any type of DDP-4 inhibitor have been combined (unless stated). Approximately two-thirds of respondents with DDP-4 experience were using metformin and/or sulfonylurea and approximately 40% were taking insulin. Regarding the impact of the condition on patients’ lives, feedback was solicited from Canadians living with, or caring for, someone with type 2 diabetes. Respondents frequently mentioned the psychological and emotional impact of diabetes on their lives (effect on mood, stress, anxiety, adjusting to changes in diet and lifestyle, medication and treatment management) as well as fatigue, lack of energy, and pain. Patients are often prescribed medications to help them achieve glucose control. Treatment is often initiated with metformin but over time, most patients will require the addition of a second or third agent to reach glycemic control. Many second-line therapies cause significant weight gain and gastrointestinal side effects. Almost 25% of respondents found it somewhat difficult, difficult, or very difficult to take multiple medications through the day, resulting in poor medication adherence, which increases the risks of complications and costs. The majority of patients indicated that blood sugar was the most important aspect of diabetes to control during the day and overnight. Several indicated the desire to avoid insulin injections. Uncontrolled

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
16
Common Drug Review July 2015
diabetes and stigma associated with the disease can result in reduced quality of life. Adequate control of the condition could help improve quality of life, reduce anxiety, and avoid or delay complications. Overall respondents were more satisfied than dissatisfied with their current medications in managing blood sugar levels; however, they did identify issues with side effects and administration of drugs, with patients on DDP-4 inhibitors expressing fewer concerns than those not on DDP-4 inhibitors. 3. Related Information About the Drug Being Reviewed The availability of Komboglyze would offer effective therapy while reducing pill burden and promoting adherence, especially for patients stabilized on metformin and saxagliptin (with a sulfonylurea or insulin) . One-quarter of survey respondents indicated that they found it difficult to take multiple medications to manage their illness. The CDA stated there is medical literature that shows poor adherence has been associated with loss of glycemic control, and increased risk of complications and costs in patients with type 2 diabetes. Most patients were not familiar with DDP-4 inhibitors. Among the 5% to 10% with experience, the most frequent expectation was to have better blood glucose control, including fewer instances of hyperglycemia and hypoglycemia. While most indicated the expectation of fewer side effects (including hypoglycemia and weight gain), others indicated they worry about more serious side effects. Side effects were not frequently experienced by DDP-4 inhibitor users who responded to the survey. About two-thirds of those with DDP-4 inhibitor experience reported they were mostly satisfied with having their blood sugar levels kept at target. Two people said that their blood sugars had remained high. Most of the concerns raised from this group were related to the need for multiple medications. About 70% of those not experienced with DDP-4 inhibitors said it was “not at all” or “a little” difficult to take several tablets and 25% responded that it was “somewhat difficult, difficult, or very difficult.” Of the DDP-4 inhibitor users, about 40% said it was “somewhat difficult, difficult, or very difficult,” while 60% reported multiple tablets were “not at all” or “a little” difficult to manage. When asked about the importance of access to Komboglyze, 63% of non–DDP-4 inhibitor users and 68% of DDP-4 inhibitor users rated this as “somewhat important,” “important,” or “very important.” Only 8% of non–DDP-4 inhibitor users and 13% of DDP-4 inhibitor users said it was “not at all” or “a little” important to have a combined pill. In summary, there are clear expectations among those with experience with DDP-4 inhibitors that these medications offer better blood glucose control, and hope that there will also be better weight control. In the literature, gastrointestinal side effects appear to be of concern, but were not experienced by survey respondents who have used DDP-4 inhibitors. A substantial proportion of respondents identified taking several medications as a concern and were very supportive of the availability of a pill combining two medicines. 4. Additional Information The CDA indicated that responses to this survey reinforce the understanding that most patients will make several changes in their drug regimen over the course of their disease, and their preference of therapy is influenced by many individual factors. Having access to multiple medications that allow individualization of therapy could optimize outcomes.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
17
Common Drug Review July 2015
FIGURE 2: ORGANIZATIONS AND FOUNDATIONS THAT MADE DONATIONS TO THE CANADIAN DIABETES
ASSOCIATION BETWEEN SEPTEMBER 2012 AND AUGUST 2013.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
18
Common Drug Review July 2015
REFERENCES
Manufacturer-Submitted References
1. Canadian Agency for Drugs and Technologies in Health. CADTH Optimal Therapy Report: Current utilization of second- and third-line therapies in patients with type 2 diabetes. Volume 4, Issues 3, August 2010.
2. Bailey CJ, Kodack M. Patient adherence to medication requirements for therapy of type 2 diabetes. Int J Clin Pract 2011; 65: 314-22.
3. Rozenfeld Y, Hunt JS, Plauschinat C, et al. Oral antidiabetic medication adherence and glycemic control in managed care. Am J Manag Care 2008; 14: 71-75.
4. Rhee MK, Slocum W, Ziemer DC et al. Patient adherence improves glycemic control Diabetes Educ 2005; 31: 240-50.
5. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care 2004; 27(5): 18-24.
6. Ho PM, Rumsfeld JS, Masoudi FA et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med 2006; 166: 1836-41.
7. Hansen RA, Farley JF, Droege M et al. A retrospective cohort study of economic outcomes and adherence to monotherapy with metformin, pioglitazone, or a sulfonylurea among patients with type 2 diabetes in the United States from 2003 to 2005. Clin Ther 2010; 32: 1308-19
8. Han S, K, Davies MJ et a. Glycemic effectiveness and medication adherence with fixed-dose combination or coadministered dual therapy of antihyperglycemic regimens: a meta-analysis. Curr Med Res Opin 2012; 28(6): 969-977.
9. Bangalore S, Kamalakkannan G, Parkar S et al. Fixed-dose combinations improve medication compliance: A meta-analysis. Am J Med 2007; 120: 713-719
10. Hutchins V, Zhang B, Fleurence RL et al. A systematic review of adherence, treatment satisfaction, and costs in fixed-dose combination regimens in type II diabetes. Curr Med Res Opin 2011; 27: 1157-68.
11. Bristol-Myers Squibb. A Study to Characterize the Steady-state Pharmacokinetics and Pharmacodynamics of 2.5 mg Saxagliptin Administered Twice Daily with Meals to Healthy Subjects: Clinical Study Report.[Internal document: unpublished study]. 2009; CV181091.
12. Bristol-Myers Squibb. A Pharmacokinetics/Pharmacodynamics Study of Saxagliptin Following Multiple Dose Administration of 2.5 mg Twice Daily as Compared to 5 mg Once Daily When Administered with Standard Meals to Healthy Subjects: Clinical Study Report. [Internal document: unpublished study]. 2011; CV181152.
13. Bristol-Myers Squibb. Bioequivalence Study of the Fixed Dose Combination of 2.5 mg Saxagliptin and 500 mg Metformin Tablet Relative to a 2.5 mg Saxagliptin (Onglyza) Tablet and a 500 mg Metformin (Glucophage Marketed in Canada by Sanofi-Aventis) Tablet Co-Administered to Healthy Subjects in the Fasted and Fed States: Clinical Study Report. [Internal document: unpublished study]. 2010; CV181118.
14. Bristol-Myers Squibb. A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Parallel-Group. Phase 3 Trial to Evaluate the Efficacy and Safety of 2.5-mg Saxagliptin, PO, BID, in Combination with Metformin in Subjects with Type 2 Diabetes Mellitus Who Have Inadequate Glycemic Control on Metformin, Alone: Clinical Study Report. [Internal document: unpublished study]. 2010; CV181080.

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
19
Common Drug Review July 2015
15. Bristol-Myers Squibb and AstraZeneca. A 24-week, Multicentre, Randomised, Double-Blind, Placebo-Controlled Phase IIIb Study to Evaluate the Efficacy and Safety if Saxagliptin in Combination with Metformin and Sulfonylurea in Subjects with Type 2 Diabetes who have Inadequate Glycaemic Control with the Combination of Metformin and Sulfonylurea: Clinical Study Report. [Internal document: unpublished study]. 2012; D1680L00006.
16. CDEC final recommendation. Sitagliptin/Metformin. CDEC Meeting – March 24, 2010. Notice of CEDAC Final Recommendation: June 23, 2010.
17. Health Canada Drug Database Query. Available at: http://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsp. Accessed March 8, 2013.
18. Bristol-Myers Squibb. Bioequivalence Study of the Fixed Dose Combination of 2.5 mg Saxagliptin and 500 mg Metformin Tablet Relative to a 2.5 mg Saxagliptin (Onglyza) Tablet and a 500 mg Metformin (Glucophage Marketed in Canada by Sanofi-Aventis) Tablet Co-Administered to Healthy Subjects in the Fasted and Fed States: Clinical Study Report. [Internal document: unpublished study]. 2010; CV181118
CDR Reviewer References
1. Bangalore S, Kamalakkannan G, Parkar S, Messerli FH. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007 Aug;120(8):713-9.
2. Health Canada reviewer's report: Komboglyze (saxagliptin/metformin HCL) [CONFIDENTIAL internal report]. Ottawa: Therapeutic Products Directorate, Health Canada; 2012.
3. CDR submission binder: Komboglyze™ (saxagliptin & metformin hydrochloride tablet) 2.5mg/500mg, 2.5mg/850mg, 2.5mg/1000mg; Company: Bristol-Myers Squibb Canada [CONFIDENTIAL manufacturer's submission]. Montreal (QC): Bristol-Myers Squibb Canada; 2013 Aug.
4. Derosa G, Maffioli P. Patient considerations and clinical utility of a fixed dose combination of saxagliptin/metformin in the treatment of type 2 diabetes. Diabetes Metab Syndr Obes [Internet]. 2011 [cited 2013 Dec 19];4:263-71. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3139534/pdf/dmso-4-263.pdf
5. Harper W, Clement M, Goldenberg R, Hanna A, Main A, Retnakaran R, et al. Pharmacologic management of type 2 diabetes. Can J Diabetes [Internet]. 2013 [cited 2014 Jan 21];37(Suppl 1):S61-S68. Available from: http://guidelines.diabetes.ca/App_Themes/CDACPG/resources/cpg_2013_full_en.pdf
6. Canadian Agency for Drugs and Technologies in Health. Second-line pharmacotherapy for type 2 diabetes: update [Internet]. Ottawa: The Agency; 2013 Jul. (CADTH optimal use report; vol. 3, issue 1a). [cited 2013 Dec 17]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0061000/
7. Canadian Agency for Drugs and Technologies in Health. Third-line pharmacotherapy for type 2 diabetes: update [Internet]. Ottawa: The Agency; 2013 Jul. (CADTH optimal use report; vol. 3, issue 1b). [cited 2013 Dec 17]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0061000/
8. Common Drug Review. Clinical review report: Saxagliptin (Onglyza) [Internet]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2013 Nov. [cited 2014 Feb 25]. Available from: http://www.cadth.ca/media/cdr/clinical/SR0329_Onglyza_CL_Report_e.pdf
9. Common Drug Review. CDEC final recommendation: Saxagliptin (Onglyza - Bristol-Myers Squibb Canada and AstraZeneca Canada) Indication: Type 2 Diabetes Mellitus [Internet]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2013 Nov. [cited 2014 Feb 25]. Available from: http://www.cadth.ca/media/cdr/complete/complete_SR0329_Onglyza-preNOC_19-Nov-13_e.pdf

CDR FIXED-DOSE COMBINATION REVIEW REPORT FOR KOMBOGLYZE
20
Common Drug Review July 2015
10. Glucophage®: metformin hydrochloride, manufacturer's standard 500 mg and 850 mg tablets [product monograph]. Laval (QC): sanofi-aventis Canada Inc.; 2009.
11. Metformin hydrochloride tablets [Internet]. Silver Spring (MD): U.S. Food and Drug Administration; 2014. [cited 2014 Mar 4]. Available from: http://www.fda.gov/ohrms/dockets/dailys/02/May02/053102/800471e6.pdf
12. Scheen AJ. Metformin + saxagliptin for type 2 diabetes. Expert Opin Pharmacother. 2012 Jan;13(1):139-46.
13. Barnett AH, Charbonnel B, Donovan M, Fleming D, Chen R. Effect of saxagliptin as add-on therapy in patients with poorly controlled type 2 diabetes on insulin alone or insulin combined with metformin. Curr Med Res Opin. 2012 Apr;28(4):513-23.
14. Minze MG, Klein MS, Terrell BT. Saxagliptin and metformin in fixed combination for the treatment of type 2 diabetes in adults. Clin Med Insights Endocrinol Diabetes [Internet]. 2013 [cited 2013 Dec 19];6:15-24. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738378/pdf/cmed-6-2013-015.pdf
15. Komboglyze™ (saxagliptin hydrochloride and metformin hydrochloride tablets) 2.5mg/500mg, 2.5mg/850mg, 2.5mg/1000mg [product monograph]. Montreal (QC): Bristol-Myers Squibb Canada; 2013 Aug.
16. Common Drug Review. Linagliptin/metformin hydrochloride (Jentadueto - Boehringer Inghelheim Canada Ltd.). Indication: type 2 diabetes mellitus. CDEC final recommendation [Internet]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2013 Oct 17. [cited 2014 Jan 23]. Available from: http://www.cadth.ca/media/cdr/complete/cdr_complete_Jentadueto_October-21-13_e.pdf
17. McKesson Canada [Internet]. Saint-Laurent (QC): McKesson Canada. 2014 [cited 2014 Jan 28]. Available from: http://www.mckesson.ca/en/