Embed Size (px)
Citation preview

Common Hip
And Pelvic
Injuries in
Sports Medicine DAVID BUCK, MD, CAQ SM
NOVEMBER 13, 2015

Objectives
Review diagnosis of common hip and
pelvic injuries.
Review treatment of common hip and
pelvic injuries.
Review appropriate diagnostic tests for hip
and pelvic injuries.
Review return to play issues for common
hip and pelvic injuries.

Which muscle is not associated
with the correct Apophyses?
A) Sartorius – Anterior Superior Iliac Spine (ASIS)
B) Transversus abdominus and Gluteal muscles –
Iliac Crest
C) Rectus Femoris – Anterior Inferior Iliac Spine
(AIIS)
D) Adductor and Gracilis – Inferior pubic rami
E) Iliopsoas – Greater Trochanter

Apophysis
Definition
Natural protuberance from a bone for
the attachment of muscles
Bony process with an independent
center of ossification and growth plate
which serves as an attachment for a
ligament or tendon

Hip Apophyses: Locations
Iliac Crest – Transversus Abdominus/Glutes
Ischial Tuberosity – Hamstring muscles
Anterior Superior Iliac Spine (ASIS) - Sartorius
Anterior Inferior Iliac Spine (AIIS) – Rectus Femoris
Lesser Trochanter - Iliopsoas
Greater Trochanter – Gluteus medius and
minimus
Inferior pubic rami – Adductor and Gracilis

Hip Apophyses: Locations
Image retrieved from http://www2.luriechildrens.org/ce/online/article.aspx?articleID=101

Ages of Fusion of Hip Apophyses
Iliac Crest – 15 to 17 years
Ischial Tuberosity – 19 to 25 years
ASIS – 21 to 25 years
AIIS – 16 to 18 years
Lesser Trochanter – 16 to 18 years
Greater Trochanter – 16 to 18 years

Apophysitis
Definition
Overuse injury
Inflammation at sites of tendon
attachment
Traction forces
Growth plate is the weak link

Iliac Crest Apophysitis
Most common
Involves abdominal and gluteal muscles
Presents with anterior and superior hip pain with
activity
Iliac crest ossification center closes anterior to
posterior
Females between 14 to 18
Males between 16 to 20
Long distance runners and dancers

Image retrieved from http://eorif.com/iliac-apophysitis-7329

Hip Apophysitis: Clinical Presentation
Tenderness to palpation over anterior half of iliac crest, ASIS, or AIIS, lesser trochanter or greater trochanter
Reproducible pain with resisted hip abduction or trunk rotation
Tenderness is over bony prominences rather than muscles or tendons
X-rays should be obtained to rule out an avulsion fracture

Hip Apophysitis: Differential Diagnosis
Sports hernia
Hip strains
Stress fractures
Osteitis pubis
Intra-articular hip pathology
Labral tears, hip osteoarthritis, chondral
lesions, and femoroacetabular impingement
Tumors

Hip Apophysitis: Treatment
Treatment
Relative rest
May participate in sport at a level that does not
produce pain
Rest
Ice
Analgesics (anti-inflammatory medication)
Cross training
Slow progression of activities over 4 to 6 weeks
Aggressive hip and abdominal flexibility program

Avulsion Fracture of Hip and Pelvis

When should you consider Surgery
for an Avulsion Fracture?
A. Greater than 1 cm displacement
B. Greater than 2 cm displacement
C. Greater than 3 cm displacement
D. Greater than 4 cm displacement
E. All fractures regardless of displacement

Avulsion Fracture
At-risk athletes:
Sprinters
Soccer players
Gymnasts
Dancers
Football players

Avulsion Fracture of Hip and Pelvis
Skeletally immature athlete
Caused by a sudden violent contraction
Accounts for 11% to 40% of all hip and
pelvis fractures in pediatrics
ASIS (Sartorius) and Ischial Tuberosity
(Hamstrings) most common = 60%

Avulsion Fracture Hip and Pelvis:
Clinical Presentation
Presentation
Athlete will note a sudden pull or
pop during activity
Localized pain and swelling over
bony attachment
Loss of motion

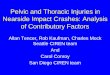
“The following pelvic x-ray is from a 15 year old male. He was running when he heard a ‘pop’ sound and collapsed onto the ground, following which he noted pain around the right groin and down to the knee. What can you note in the x-ray?”
Image and case retrieved from http://www.emergucate.com/2014/01/20/imaging-case-of-the-week-84/

Avulsion Fracture Hip and Pelvis:
Diagnostic Tests
Radiographs
Essential for diagnosis
Comparison views of the
uninvolved side should be obtained

Avulsion Fractures of Hip and Pelvis:
Treatment
Rest, ice, analgesics
Gentle active and passive range of motion
Progressive resistance exercises when 75% of
ROM and 50% strength are reached
Stretching and strengthening combined with
patterned motions
Surgery – rare; consider when displacement is
2 cm or greater

Avulsion Fractures of Hip and Pelvis:
Return to Sport
Full pain free range of motion
Full strength
Able to walk, jog, run, and sprint without
pain
Able to jump on the injured leg without
pain
Usually requires 5 to 10 weeks

Which type of Bursitis is most
common in Sports Medicine?
A. Ischial
B. Trochanteric
C. Iliopectineal
D. Ischiogluteal

Image retrieved from http://www.drlox.com/greater-trochanteric-bursitis/

Hip Bursitis
Definition = An inflammation of fluid filled
sacs over bony prominences and joints
Causes
Repetitive Overuse
Post traumatic or direct injury
Degenerative changes
Systemic disease

Hip Bursitis
3 major hip bursa
Trochanteric
Ischial
Ischiogluteal

Trochanteric Bursitis: Presentation
Pain and tenderness over greater trochanter worsened by hip flexion and extension
Pain may radiate to knee, ankle, or into the buttock
Pain worsened by rising from a seated or recumbent position
Pain improves after a few steps; but, recurs after walking for more than 30 minutes
Pain at night
Most common in athletes especially runners

Trochanteric Bursitis
Causes
Muscle Imbalance between hip abductors and adductors
Leg-length discrepancy
Excessive training
Foot hyperpronation
External factors
Hard surface
Banked track
Shoes

Trochanteric Bursitis: Tests
X-rays of Pelvis and Lateral Hip
Rule out bony abnormalities and intra-
articular hip pathology
Bone scans and MRI
Rarely needed
Helpful to rule out occult fractures,
tumors, or osteonecrosis of the femoral
head

Trochanteric Bursitis: Differential
Diagnosis
Metastatic Tumor
Osteoarthritis of the Hip
Sciatica
Septic arthritis of the hip
Snapping hip
Trochanteric fracture

Trochanteric Bursitis: Treatment
Rest
Ice
Analgesics
Injection of steroid and lidocaine
Stretching program
Address IT band and hip adductors
Address internal causes
Slow progression and return to sport
Surgical management rarely indicated

Traumatic Osteitis Pubis involves the
bony origin of which muscle?
A. Gracilis
B. Iliopsoas
C. Hamstrings
D. Adductor magnus

Osteitis Pubis
Cause of chronic groin pain in athletes
Athletes at risk
Distance runners
Football players
Soccer players
Basketball players
Weight lifters
Fencers

Osteitis Pubis
Caused by repetitive trauma to the pubic
symphysis from muscle strain of the
Gracilis
Leads to inflammatory response
Described as a fatigue fracture
Pathophysiology compared to medial
tibial stress syndrome
Referred to Gracilis Syndrome

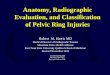
Osteitis Pubis: Radiology Findings
Image retrieved from http://www.radpod.org/2007/10/12/osteitis-pubis/

Osteitis Pubis: Clinical Symptoms
Slow insidious onset of dull groin pain
Pain may be midline, unilateral or bilateral
Absence of systemic symptoms
Pain may radiate into lower abdomen,
proximal medial thigh or inguinal area
Can be chronic and incapacitating
Worse with activity
Relieved by rest

Osteitis Pubis: Clinical Findings
Athlete walks with wide based or waddling gait
Tenderness to palpation over pubic symphysis or
pubic tubercle
Pain over pubic symphysis with passive
abduction
Pain with resisted adductor testing
One legged hop test may reproduce groin pain

Osteitis Pubis: Differential Diagnosis
Osteomyelitis
Hip Strain
Hernia
Stress Fracture
Intra-articular hip disease
Referred low back pain
Endometriosis/PID/Tumor

Osteitis Pubis: Diagnostic Tests
X-rays
Rule out avulsion fractures or other bony abnormalities
May lag behind clinical findings by 2 to 4 weeks
MRI
High sensitivity and readily available
Confirmatory test
Ultrasound
Help rule out hernia and has low cost
Bone scan
Obtain when MRI and Ultrasound are equivocal

Osteitis Pubis: Treatment
Condition is generally self-limited
Relative Rest - mainstay of treatment
NSAIDs
Physical Therapy – 6 to 8 weeks
Main goal: strengthen and stabilize the pelvis
and pubic symphysis
Cortisone injections or oral glucocorticoids
Surgical debridement and arthrodesis of pubic
symphysis

Osteitis Pubis: Return to Sport
Can occur when athlete is pain-free
Usually 2 to 3 months with
conservative measures
If surgery needed, could take 1-2
years for athletes to return

Groin Strain
(Adductor muscle strain) Common injury, caused by forceful twisting or pivoting of
the lower extremity
Common sports
Football
Ice hockey
Soccer
Baseball
Karate
Gymnastics
Track sports

Groin Strain
Mechanism of Injury – Forceful contraction of an
overstretched adductor muscle against another
player, the ground or the ball
Risk factors for injury
Older athlete
Inflexibility
Muscle imbalance
Inadequately warmed up muscles
Early in the season

Image retrieved from http://orthopedicsurgerysandiego.com, McKesson Health Solutions

Groin Strain: Presentation
Varied presentation
Pain dull or sharp
Pain localized or diffuse
Radiation into scrotum, hip, medial thigh,
or deep pelvis
Pain worsened by activities involving
forced adduction of the hip

Groin Strain: Physical Exam and
Diagnostic Tests
Tenderness to palpation over pubic bone
Discomfort on passive abduction of the
thigh and resisted adduction of the thigh
Radiographs should be obtained
Bone scan or MRI should be reserved for
rare cases

Groin Strain: Differential Diagnosis
Osteitis pubis
Sports hernia (Athletic pubalgia)
Apophysitis
Lower abdominal muscle strains
Stress fractures
Nerve impingement
Ilioinguinal nerve
Obturator nerve
Intra-articular hip pathology

Groin Strain: Treatment
RICE
Passive stretching and Physical therapy
Isometrics and cycling or walking
Strengthening and weight lifting
Sports specific training and return to sport
Rehab program may take 4 to 6 weeks up
to months or years

Groin Strain: Return to Sport
Full pain free Range of Motion
90% to 95% of preinjury strength as compared to
uninjured leg
Completion of all sports specific activities
Advise athletes to wear pair of compression
shorts or neoprene wrap
Supplies warmth
Supplies support
Supplies proprioceptive assistance


What is the typical Return to Play
for a Grade 2 Hip Strain?
A. 1 to 2 weeks
B. 2 to 3 weeks
C. 3 to 4 weeks
D. 4 to 6 weeks
E. 8 to 12 weeks

Hip Strains: Mechanism of Injury
Hip Flexor Strains
Forceful Contraction of hip flexors while being stretched
Iliopsoas, Sartorius, or Rectus Femoris
Quadriceps Strains
Sudden deceleration of the leg
Violent contraction of the quadriceps
Rapid deceleration of an overstretched muscle
Hamstring Strains
An opposite force applied to a fully stretched hamstring
Sudden stretch applied to hamstring muscle

Hip Strains: Risk Factors
Muscle imbalance between the quadriceps and
hamstrings
Inadequate flexibility
Inadequate warm-up
Strength imbalance between legs
History of previous injury
Muscle fatigue
Poor running form
Overuse injuries

Hip Strains: Clinical Symptoms
Audible pop may be heard or felt
Tenderness to palpation over injured
muscle
Sometimes bruising, swelling, or
palpable gap

Hip Strains: Physical Exam
Hip Flexors
Pain worse with flexion of the hip against
resistance or with passive extension of the hip
Quadriceps
Pain exacerbation with passive flexion of the knee or resisted extension of the knee
Hamstrings
Pain exacerbation with passive extension of the knee and hip flexion and resisted flexion of the
knee and hip extension

Hip Strains: Diagnostic Tests
Plain X-rays
Rule out avulsion fractures, bony
abnormalities, or myositis ossificans
Generally normal
MRI
Can differentiate between Grade 2 and
Grade 3 Strains
Not cost effective
Reserved for elite athletes

Hip Strains: Differential Diagnosis
Hip Avulsion Fractures
Sartorius Strain – avulsion of ASIS
Rectus Femoris Strain – avulsion of AIIS
Osteonecrosis of Hip
Pelvic or proximal femoral tumors

Hip Strains: Treatment
RICE protocol – first 24 to 48 hours
Crutch walking
Anti-inflammatory analgesics
Physical Therapy
Passive stretching and gentle active range of motion
Isometric strengthening
Cross training
Surgical intervention - rare
Steroid injections – Not advisable

Hip Strains: Return to Sport
Full pain-free Range of motion
Quadriceps to Hamstring strength ratio is 0.60 or more
Strength ratio 0.55 or less has 33% chance of reinjury
Strength is 90% to 95% of the uninvolved side
Can complete sports specific activities
Dependent upon Grade
Grade 1 – 1 to 2 weeks
Grade 2 – 3 to 4 weeks
Grade 3 – 8 to 12 weeks

Image retrieved from
http://www.radiologyassistant.nl/en/p4bc9b8ab8ec80/bone-tumor-p-z.html

Which type of Stress Fracture
should be treated Surgically?
A. Compression Side Femoral Neck
B. Femoral Shaft
C. Pelvic
D. Tension Side Femoral Neck

Stress Fracture of Femur and Pelvis
Caused by repetitive micro-traumatic forces to
the bone
Disrupts cycle of bone resorption and bone
repair
Common in military recruits and endurance
athletes
Often misdiagnosed or missed
Classified based on the anatomic location of
the fracture

Stress Fracture: Risk Factors
Training errors
Change in running surface
Inadequate footwear
Osteopenia
Pes planus

Stress Fracture: Clinical Symptoms
Vague pain in the groin, anterior thigh or knee
Pain with activity or weight bearing
Pain resolves with rest
Tenderness to palpation of affected area
Decreased range of motion of hip to IR
Antalgic gait
Pain may develop at a consistent time or
distance
Precipitated by recent increase in activity level

Stress Fracture: Diagnostic Tests
X-rays – usually negative in the first 2 to 4 weeks
Plain films only show changes during the reparative phase
Classic Radiographic signs
Radiolucent lines
Sclerosis
Periosteal new bone formation
Bone scan
Detect stress fractures as soon as 24-48 hours after injury
MRI
Extremely sensitive for Femoral Neck Stress Fracture

Stress Fracture: Differential Diagnosis
Acute fracture of the femoral neck
Muscle strain or groin pull
Hip Osteoarthritis
Hip Osteonecrosis
Pathologic fracture
Pelvic fracture
Acetabular labral tear

Image retrieved from
http://www.eorthopod.com/stress-fracture-
of-the-hip/topic/55

Stress Fracture: Treatment
Pelvic stress fracture
Rest
Protected weight-bearing
Flexibility exercises
Nonimpact activity such as swimming or
cycling
Return to sport may be delayed up to 6
months

Stress Fracture: Treatment
Tension side Femoral neck fracture
Transverse fracture in superior cortex of femur
Older patients
Can progress to displaced fracture – surgical
emergency
Should have internal fixation
Surgery for all

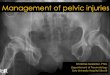
“Compression side femoral stress fracture in a long-distance runner.” Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3495575/figure/bjr-85-1148-g009/ The British Institute of Radiology

Stress Fracture: Treatment
Compression side Femoral neck fracture
Bone changes or fracture line on medial aspect
Younger athletes
Usually treated conservatively
Cessation of activity
Non-weight bearing with crutches
Healing usually occurs in 6 to 8 weeks
Serial Radiographs essential
Surgery rarely necessary

Stress Fracture: Treatment
Femoral shaft
Conservative Tx
Full rest until pain free
Crutch-walk and slowly progress to full
weight bearing when pain free
Cross training with biking or swimming after
6 weeks

Stress Fracture: Return to Sport
Address any intrinsic or extrinsic factors
Dependent upon age, sex, bone density,
and location of fracture
Follow X-rays monthly for the first 3 months
May take up to 2 years for complete healing
Return to sport
Compression and femoral shaft – 6 to 8 weeks
Pelvic and Tension – 6 months to 2 years

What is the most common
Snapping Hip Syndrome?
A. Iliopsoas tendon passing over Iliopectineal
eminence or Lesser Trochanter
B. Iliotibial band passing over the Greater
Trochanter
C. Long head of biceps femoris passing over
Ischial Tuberosity
D. Iliofemoral Ligaments passing over the Femoral
Head

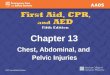
Snapping Hip: Definition
Characterized by a snapping or popping sensation that
occurs as tendons move over bony prominences
Common sites
Iliotibial band snapping over the greater trochanter
Most common
Iliopsoas tendon sliding over the iliopectineal
eminence or lesser trochanter
Long head of biceps femoris sliding over Ischial
Tuberosity
Iliofemoral ligaments over the Femoral head

Image retrieved from
http://www.parkclinic.com.au/home/co
nditions-treatment/hip/snapping-hip/

Snapping Hip: Clinical Symptoms
Snapping sensation with walking or rotation of hip
Snapping when lying with affected side up and
rotation of leg
Associated with trochanteric bursitis
May have pain upon rising in the morning and at
night
Difficulty lying on affected side
Iliopsoas subluxation
Groin pain when hip extends from flexed position
(rising from chair)

Snapping Hip: Clinical Presentation
IT band subluxation recreated by having
the athlete stand and rotate hip while
holding it in an adducted position
Iliopsoas subluxation may be noted as the
hip extends from a flexed position (rising
from chair)

Snapping Hip: Tests
Diagnostic Tests
X-rays of the Pelvis and Lateral Hips
Usually normal
CT Arthrogram
Rule out intra-articular loose bodies
MRI with Gadolinium
Rule out a tear of the acetabular labrum

Snapping Hip: Differential Diagnosis
Osteoarthritis of the hip (limited Internal
Rotation)
Osteochondral loose body
Osteonecrosis of the femoral head
Tear of the Acetabular Labrum

Snapping Hip: Treatment
Education and Reassurance
Activity modification
Short course of non-steroidal anti-inflammatories
Stretching and strengthening exercises
Focus on IT band, hip abductors, hip adductors and
hip flexors
Corticosteroid injections
Trochanteric bursa or Psoas tendon sheath
Surgery – rare
Return to Sport – Immediate

Which muscle is not associated
with the correct Apophyses?
A) Sartorius – Anterior Superior Iliac Spine (ASIS)
B) Transversus abdominus and Gluteal muscles –
Iliac Crest
C) Rectus Femoris – Anterior Inferior Iliac Spine
(AIIS)
D) Adductor and Gracilis – Inferior pubic rami
E) Iliopsoas – Greater Trochanter

When should you consider Surgery
for an Avulsion Fracture?
A. Greater than 1 cm displacement
B. Greater than 2 cm displacement
C. Greater than 3 cm displacement
D. Greater than 4 cm displacement
E. All fractures regardless of displacement

Which type of Bursitis is most
common in Sports Medicine?
A. Ischial
B. Trochanteric
C. Iliopectineal
D. Ischiogluteal

Traumatic Osteitis Pubis involves the
bony origin of which muscle?
A. Gracilis
B. Iliopsoas
C. Hamstrings
D. Adductor magnus

What is the typical Return to Play
for a Grade 2 Hip Strain?
A. 1 to 2 weeks
B. 2 to 3 weeks
C. 3 to 4 weeks
D. 4 to 6 weeks
E. 8 to 12 weeks

Which type of Stress Fracture
should be treated Surgically?
A. Compression Side Femoral Neck
B. Femoral Shaft
C. Pelvic
D. Tension Side Femoral Neck

What is the most common
Snapping Hip Syndrome?
A. Iliopsoas tendon passing over Iliopectineal
eminence or Lesser Trochanter
B. Iliotibial band passing over the Greater
Trochanter
C. Long head of biceps femoris passing over
Ischial Tuberosity
D. Iliofemoral Ligaments passing over the Femoral
Head

QUESTIONS?

REFERENCES
The British Institute of Radiology. Compression side femoral stress fracture in a long-distance runner. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3495575/figure/bjr-85-1148-g009/
D'Souza, MD, Donna. Osteitis pubis. Retrieved from http://www.radpod.org/2007/10/12/osteitis-pubis/ eORIF. Iliac Apophysitis. Retrieved from http://eorif.com/iliac-apophysitis-7329 Imaging case of the week 84. Retrieved from http://www.emergucate.com/2014/01/20/imaging-case-of-the-week-84/ LaBella, C. R. (2005). Location of apophyses in the pelvis and hip. Retrieved from http://www2.luriechildrens.org/ce/online/article.aspx?articleID=101 Lox, Dennis. Greater trochanteric bursitis. Retrieved from http://www.drlox.com/greater-trochanteric-bursitis/ McKesson Health Solutions. Groin strain. Retrieved from http://orthopedicsurgerysandiego.com Orthopod. Stress fracture of the hip. Retrieved from http://www.eorthopod.com/stress-fracture-of-the-hip/topic/55 Park Clinic Orthopedics. Snapping hip. Retrieved from http://www.parkclinic.com.au/home/conditions-treatment/hip/snapping-hip/ van de Woude, Henk Jan & Smithuis, Robin. Typical stress fracture of medial side of the femoral neck. Retrieved from http://www.radiologyassistant.nl/en/p4bc9b8ab8ec80/bone-tumor-p-z.html

References
Peck D, McKeag D, Moeller J: Pelvis, Hip and Upper Leg. ACSM’s
Primary Care Sports Medicine 447-460, 2007
Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and
treatment. J Am Acad Orthop Surg 8:344-353, 2000
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J
Sports Med 13:349-358, 1985
Anderson K, Strickland SM, Warren R: Hip and groin injuries in
athletes. Am J Sports Med 29:521-533, 2001
Owens B, Busconi B: Pelvis, Hip and Thigh. Sports Medicine Just the
Facts 337-342, 2005