Embed Size (px)
Citation preview

The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413
Contents lists available at ScienceDirect
The Egyptian Journal of Radiology and Nuclear Medicine
journal homepage: www.sciencedirect .com/ locate /e j rnm
Original Article
Common interventional techniques (single versus combined)in management of hepatocellular carcinoma
http://dx.doi.org/10.1016/j.ejrnm.2016.07.0010378-603X/� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abbreviations: TACE, transarterial chemoembolization; RFA, radiofre-quency ablation; HCC, hepatocellular carcinoma; PEI, percutaneousethanol injection; US, ultrasonography; CT, computed tomography; PES,post embolization syndrome.
Peer review under responsibility of The Egyptian Society of Radiology andNuclear Medicine.⇑ Corresponding author.
E-mail address: [email protected] (M.M. Shakweer).
Mostafa M. Shakweer a,⇑, Abdelshafy A. Awad Allah a, Abdel-Aziz K. Aun b
aRadiology Department, Faculty of Medicine, Al-Azhar University, New Damietta, EgyptbRadiology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
a r t i c l e i n f o
Article history:Received 25 May 2016Accepted 6 July 2016Available online 25 July 2016
Keywords:Hepatocellular carcinomaRadiofrequency ablationTransarterial chemo-embolization
a b s t r a c t
Objective: To evaluate the role of transarterial chemoembolization ‘‘TACE”, radiofrequencyablation ‘‘RFA” and combination of both techniques in management of hepatocellular car-cinoma ‘‘HCC”. Patients and methods: This study was carried out at Al-Azhar UniversityHospital (New Damietta) during the period from May 2013 to June 2015. It included fortypatients were included in this study (27 males and 13 females), with age ranged from 43 to68 year (mean age 51 year). They were divided into three groups after laboratory and radi-ological assessment: group 1 treated with TACE, group 2 treated with RFA and group 3treated with combined therapy. The response was evaluated by triphasic MDCT, alpha-fetoprotein as well as clinical follow-up and classified as complete and partial response,and the overall survival was recorded. Results: There were no major complicationsdetected. At 3 month follow-up, there was complete response ‘‘CR” in 32 patients (80%),and partial response ‘‘PR” in 8 patients (20%). At 6 months, there was complete responsein 34 patients (85%), and partial response in 3 patients (7.5%). At 12 months, there wascomplete response in 33 patients (82.5%), and partial response in one patient (2.5%). It isproved that complete response with high percentage achieved by combined therapy thaneither by TACE or by RFA (100%, 88.46% and 75% respectively), with the overall survival was85%. Conclusion: The study showed that combined therapy achieved better results regard-ing complete response and overall survival rate than RF or TACE alone.� 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting byElsevier. This is an open access article under the CC BY-NC-ND license (http://creativecom-
mons.org/licenses/by-nc-nd/4.0/).
1. Introduction death worldwide. Considering management of HCC is a
Hepatocellular carcinoma (HCC) constitutes themajority of primary liver tumors, which is the 6th mostcommon tumor and the 3rd most common cause of cancer
challenge, it was reported that a great number of HCCpatients are suitable for curative therapy due, either toadvanced stage of disease or to poor liver functions at timeof the diagnosis [1]. In treatment of hepatocellularcarcinoma (HCC), less than 40% of patients are candidatesfor surgery in early stages, and the rate of recurrence aftercurative surgery is high [2].
So, different strategies are available or being developed forlocoregional therapy, but the largest experience is withtransarterial chemoembolization (TACE) and radiofrequencyablation (RFA). RFA is awell-studiedprocedureproducingbet-ter local tumor control with 2 year recurrence of 2–18% and

1408 M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413
5 year survival of 40–70%orbetterwhen the treatmentgroupshavebeen selected [3]. RFA is aminimally invasive, repeatableprocedurewith few complications. It is performedunder radi-ological guidance [4].
Hepatic arterial chemoembolization (TACE) is one of themost common treatments for unresectable hepatocarci-noma [5]. Each of both techniques has its constrictionsand limitations depending on the tumor growth pattern,size and number of tumors, location and number of seg-ments involved, and response to TACE [6]. It had beenreported that RFA in combination with TACE is an effectivetreatment for inoperable hepatic tumors as it can theoret-ically overcome the limitations of each technique whenused alone [7,8].
In this study we evaluated both techniques eitherseparately or as combined therapy in treatment of HCC.
2. Patients and methods
This study was carried out on forty patients (27 malesand 13 females), with age ranged from 43 to 68 year andthe mean age 51 year. The patients were referred toRadiology Department from General Surgery and InternalMedicine Departments as well as outpatient clinics. LocalEthical Committee approval and patients’ consents wereobtained.
2.1. Pre-treatment assessment
All patients were subjected to the following:
2.1.1. Complete clinical assessment2.1.1.1. Laboratory evaluation.� Liver profile (serum bilirubin, transaminases, alkalinephosphatase and albumin).
� Coagulation profile (prothrombin time, concentrationand INR).
� Complete blood picture to detect thrombocytopenia.� Alpha feto-protein (AFP).� Viral hepatitis seromarkers: HBV seromarkers and HCVantibodies.
2.1.1.2. Radiological assessment.A. Abdominal ultrasonography for detection of HCC
with assessment of hepatic echogenicity, hepaticveins, portal vein radicles and focal lesions werecommented upon. As regard the focal lesions, theirnumber, location, echogenicity and size measuredin two diameters were assessed. Examination ofthe rest of the abdominal organs and the presenceof ascites.
B. Triphasic MDCT scan pre and post procedure, whiletriphasic MDCT exam. Protocol included the usualtriphasic liver protocol in which pre-contrast imageswere obtained; then, images were acquired 20 s,55 s, and approximately 1–3 min after thestart of injection of 100 mL contrast at a rate of4–5 mL/s.
Inclusion criteria were as follows:
(a) Patent with non-thrombosed portal vein and liverfunctions (ALT or AST < 270 IU/L, Albumen > 2.5 g/dl,Bilirubin < 3 mg/dl). (b) No extrahepatic disease. (c)The presence of a single hepatic lesion or multiplelesions (up to 4 lesions 63 cm each). (d) Accessible siteby US and/or CT (in patients with RF treatment). (e)Coagulation profile (prothrombin time more than 60%,and platelet count more than 70,000/mm3). (f) Patientsshould be Child’s A class or Child’s B class, and (g) Alphafeto-protein ‘‘AFP” ranging less than 20 to more than500 ng/mL.
Exclusion criteria were as follows:
(a) Distant metastatic. (b) Thrombosed portal vein. (c)Poor liver functions (Bilirubin > 3 mg/dL, Albumen <2.5 g/dL, ALT or AST > 250 IU/L). (d) Severe debilitation.(e) Active infection, and (f) Poor coagulation profile(prothrombin time less than 60% and platelet count lessthan 70,000/mm3).
The patients were divided into three groups based onclinical, laboratory ‘‘liver functions” and abdominal US aswell as triphasic MDCT.
* Group one, included 26 patients treated by transarterialchemoembolization (TACE) using mixture ofDoxorubicin 50 mg dissolved in 10 cc saline and mixedwith 8 cc lipiodol and 5 cc contrast medium (ultravist300 mL/cc) for all of them with the same concentration.
* Group two, included 12 patients treated by thermalablation (RFA) using RITA RF 1500X system USA andstar burst Xli enhanced with tubing set (electrosurgicaldevice).
* Group three, included two patients treated by com-bined therapy of TACE followed by RFA one week later.
2.1.1.3. Post procedure care. All patients underwentinterventional procedures were hospitalized overnight forobservation of side effects and administration of medica-tions as needed. The patients were discharged within24 h if no side effects were noted.
2.1.1.4. Follow up. Three, Six and 12 months after the pro-cedure, the follow-up included the following:
(A) Clinical: to assess improvement of symptoms suchas fever, abdominal pain, anemia, dyspepsia andabdominal distension.
(B) Laboratory: for monitoring of AFP and liver functiontests.
(C) Imaging: radiological assessment including US andtriphasic CT scan.
Tumor response to treatment was classified intocomplete and partial response, assessed by imaging andAFP values. At imaging tumor response was measuredaccording to the criteria adopted by the European

Table 2Distribution of the studied cases regarding Alpha Feto-protein level (AFP).
Alpha Feto-protein level No Percentage
<20 ng/mL 4 cases 1021–500 ng/mL 29 cases 72.5>500 ng/mL 7 cases 17.5
M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413 1409
Association for the Study of the Liver Disease (EASL) mea-suring the longest diameter of the viable tumor against thelongest total tumor diameter. The percentage of tumornecrosis was also recorded. The necrotic area was identi-fied when a low density/low-echogenicity/fluid signal areathat was non-enhancing in any of the time phases wasseen. The EASL has officially recommended the use ofcontrast enhanced CT in the evaluation of response totreatment, and acknowledged as ‘‘viable areas” those that‘‘present enhancement” and ‘‘necrotic areas” those that‘‘do not present enhancement”. The EASL response criteriawere preferred since they take into account the develop-ment of necrosis and not only the size of the treated lesionas in Response Evaluation Criteria in Solid Tumor (RECIST)criteria (which depends only on shrinkage in size) since itacknowledged that it is common for liver tumors to liquefywithout a significant change in total lesion diameterwithin short follow-up periods. In EASL criteria, completeresponse (CR) is recorded when complete disappearanceof all known disease and no new lesions are seen; partialresponse (PR) when a 50% reduction in viable tumoral areaof all measurable lesions is present; stable disease (SD) inall other cases and progressive disease (PD) when thereis a 25% increase in size of one or more measurable lesionsor if new lesions appear [9].
MDCT images were reviewed by two radiologists. Incases the residual viable tumor was at least 1 cm in maxi-mum axial diameter, and further treatment was scheduled.
3. Results
Frequency and percentages of liver cirrhosis and Child-Pugh classification in the whole sample (Table 1).
These AFP levels had been decreased in most patients tobe less than 20 ng/mL after interventional proceduresexcept in 5 patients ranging from 50 to 100 ng/mL (seeTable 2).
Table 3Patients’ response according to EASL criteria at 3, 6, and 12 months.
Response TACE(n = 26)
RFA(n = 12)
CombinedTh. (n = 2)
3 monthsComplete response 20 (76.92%) 10 (83.33%) 2 (100%)Partial response 6 (23.07%) 2 (16.66%) 0 (0%)
3.1. Group one, included 26 patients treated by TACE
This group showed 24 patients Child’s A class and twopatients Child’s B class. 20 patients of them had solitarytumor and 6 patients had multiple tumors. TACE sessionsranged from 1 to 3 sessions. There was complete responsein 20 patients after 3 months (76.92%), while partialresponse was seen in 6 patients (23.07%). Two out of the6 patients died after 3 months, and two out of the 4patients showed complete response (CR). So the sum 22at 6 months, one of the other 2 patients died after
Table 1Etiology and classification of cirrhosis.
Variant Frequency Percentage
Etiology of cirrhosis HBV 2 5HCV 37 92.5HCV + HBV 1 2.5
Child – Pugh Classification Child’s A 37 92.5Child’s B 3 7.5Child’s C 0 0
6 months and one patient showed partial response (PR)by the end of the year, hence the sum 23 (22 showed CRand one showed PR). Consider addition of the 2 patientstreated by combined therapy, so the sum is 25 patients(24 showed complete response ‘‘CR” and one showed par-tial response ‘‘PR”).
3.2. Group two, included 12 patients treated by thermalablation (RFA)
This group showed 11 patients Child’s A class and onepatient Child’s B class. Eleven patients had solitary tumorand one patient had multiple tumors. RFA sessions wererepeated on demand 1–3 sessions. After 3 months, therewas complete response in 10 patients (83.33%), and par-tial response was seen in 2 patients (16.66%). 1/10patients died after 5 months and further 2/2 patients diedafter 10 months. Hence the sum is 9 survive patients(75%) at the end of one year (all of them showed com-plete response ‘‘CR”).
3.3. Group three, included two patients treated by combinedRFA after TACE
– All patients were Child’s A class with solitary tumor.Complete necrosis was achieved following the first ses-sion in the two patients without further sessions (100%)(see Table 3).
3.4. Complications of TACE
A. Immediate post-treatment side effects (PTS):PTS (fever <38 �C, pain, anorexia, nausea and vomiting)
occurred in 21 patients (80.7%), all of them recovered
Stable disease 0 (0%) 0 (0%) 0 (0%)Progressive disease 0 (0%) 0 (0%) 0 (0%)
6 monthsComplete response 22 (84.6%) 9 (75%) 2 (100%)Partial response 2 (7.7%) 2 (16.66%) 0 (0%)Stable disease 0 (0%) 0 (0%) 0 (0%)Progressive disease 2 (7.7%) 1 (8.33%) 0 (0%)
12 monthsComplete response 22 (84.61%) 9 (75%) 2 (100%)Partial response 1 (3.84%) 0 (0%) 0 (0%)Stable disease 0 (0%) 0 (0%) 0 (0%)Progressive disease 3 (11.53%) 3 (25%) 0 (0%)

Table 4Survival percentages of all 40 patients at 3, 6 and 12 months.
Groups Group I treated by TACE (26 cases) Group II treated by thermalablation (12 cases)
Group III treated by RF after TACE(2 cases)
SurvivalMonths 3 6 12 3 6 12 3 6 12Number of cases 26 24 23 12 11 9 2 2 2
Frequency 100% 92.3% 88.46% 100% 91.66% 75% 100% 100% 100%
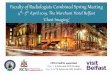
Fig. 1. 58 years-old male with hepatic focal lesion diagnosed HCC ‘‘treated by TACE”. (A) Contrast enhanced CT shows an enhanced lesion at segment IV. (B)TACE showed adequate lipiodol concentration within the lesion. (C) Three months post TACE non-contrast CT study revealed inadequate accumulation oflipiodol within the tumor. Triphasic CT showed small foci of lipiodol with arterial enhancement of the lesion in arterial phase (D) and washout in portalphase (E) and delayed phase (F) denotes inadequate ablation (partial response). AFP = 258 ng/mL before TACE and 200 ng/mL three months after. Thepatient referred to surgery for tumor resection.
1410 M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413
within 3 days after the procedure with administration ofantipyretic and antiemetic.
B. Late post-treatment side effects:
Decompensation occurred in 2 patients in the form ofascites and mild increase in the liver enzymes (treatedmedically). Liver abscess, cholecystitis, pleural effusionand CNS problems were not recorded in any patient tillthe end of the study.
3.4.1. Complications of thermal ablation (RFA)Nearly all the patients experienced post-ablation right
hypochondrial pain that was controlled by analgesics,
and nausea, which was controlled by anti-emetics. Alsoall patients experienced post-ablation pyrexia for 2 days,which was controlled by antipyretics. Major post procedu-ral complications were one patient with reactionary effu-sion, two patients had ascites and liver decompensationand five patients with subcapsular hematoma (seeTable 4).
The survival status of all 40 patients was evaluated andreported at 3, 6 and 12 months after treatment. Fourpatients died from advanced decompensated liver disease,and two patients died from coexisting concomitant illness(chest and cardiac diseases). The overall survival aftertreatment with combined therapy, TACE and RFA was100%, 88.46%, and 75% respectively (see Figs. 1–3).

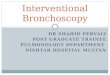
Fig. 2. 54 years-old female with focal lesion diagnosed HCC and treated by RFA. (A) Contrast enhanced CT shows an enhanced lesion at segment VII. Follow-up with Triphasic CT showed no enhanced residual lesion in arterial phase (B) and no washout in portal phase (C) or delayed phase (D) denoting goodablation. AFP = 15 ng/mL before treatment and decreased to <5 ng/mL three months after treatment.
M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413 1411
4. Discussion
High incidence rate of HCC has been reported in Egypt.Several studies were done on the association between HCVand HCC [10,11]. Yates et al. [12] found that among Egyp-tian patients with HCC more than 75% were positive forHCV-Ab. Nearby results (70%) were reported by Darwishet al. [13]. Patients with liver cirrhosis are at greatest riskfor developing HCC and should be monitored every6 months to detect the tumor at an asymptomatic stage[14]. Locoregional therapeutic modalities have been devel-oped and tested clinically over the recent years for treat-ment of HCC [15]. Several studies have shown that RFablation (RFA) is a simple, effective, and less expensivetechnique with a low morbidity compared with surgicaltreatment [16].
In this study, follow-up of the patients over one-yearduration, included reporting the response either complete
or partial (CR, PR), recurrent diseases ‘‘RD” and progressiondiseases ‘‘PD”.
High percentage of complete response (83.33%) inpatients underwent RF ablation ‘‘10/12” after one session.One of the two patients showed complete necrosis after asecond session and the other one died; this agreed withreport by Raut et al. [17].
Teratani et al. [18] reported that RFA for patients withsmall HCC nodules (less than 5 cm) provides favorable sur-vival with excellent local control. Good response withthose underwent RF alone at 3, 6, and 12 months was100%, 91.66% and 75% respectively. This was in accordancewith Chen et al. [19] who reported RFA success rate 93.3%,84.6% and 66.6% respectively.
All patients exposed to RFA experienced post-ablationright hypochondrial pain and nausea that was controlledby analgesics and anti-emetics. Major post proceduralcomplications were one patient with reactionary effusion,

Fig. 3. 45 years-old male with HCC and treated by combined therapy using TACE and RFA. (A) Post-contrast CT showed enhanced lesion at segment V ofright lobe. (B) TACE shows inadequate lipiodol accumulation within the lesion. Three months after TACE, non-enhanced CT revealed a lesion with pooraccumulation of lipiodol in (C) and enhanced lesion ‘‘post contrast CT” in (D). Three months post RF: Arterial phase revealed no enhancement of the lesion in(E), and no washout in portal phase (F) or delayed phase (G) denoting adequate ablation. AFP = 58 ng/mL before treatment and decreased to <20 ng/mLthree months after treatment.
1412 M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413
two patients had ascites and liver decompensation, andthis was in accordance with other reports [20,21].
Use of TACE showed complete response in 20/26(76.92%) after one session, while partial response in 6patients (23.07%) after second session. Three out of the 6patients died (11.53%), 2 showed complete response
(7.7%) and one (3.8%) showed partial response. This agreedwith reports used TACE as an effective palliative treatmentfor unresectable tumors [22,23].
Regarding post TACE complications in this study, PES(fever <38 �C, pain, anorexia, nausea and vomiting)occurred in 21/26 (80.7%) and recovered within 3 days

M.M. Shakweer et al. / The Egyptian Journal of Radiology and Nuclear Medicine 47 (2016) 1407–1413 1413
with administration of antipyretic and antiemetic. Yet, theetiology of PES is not fully understood but it is thought tobe caused by combination of tissue ischemia and aninflammatory response to chemoembolization [24]. Latepost-treatment side effects appear in the form of liverdecompensation with ascites and increased liver enzymes.All of them received one session of TACE and treated med-ically [25]. Patients needed a second sessions of TACE orRFA are those who showed partial response after firstsession.
Combined therapy showed complete necrosis after onesession with no need for further sessions and overall sur-vival rate 100%. However, there were no recurrent lesionsdetected in combined therapy group.
The overall survival rate was 88.46% in TACE group, 75%in RFA group and 100% in combined therapy group; thisagreed with Lo et al. [26] who reported a study of 40patients assigned to chemoembolization with near survivalprobability of 82%, and higher than study by Othman et al.[27] who reported survival rates 75% with TACE, 90% withRFA and 95% with combined therapy.
Post therapy follow-up of Alpha feto-protein showedthat it was decreased gradually to near normal levels inthose patients showed complete response, that agreedwith reports stated by Hu et al. [28].
From this study it was noted that combined therapy issuperior to either TACE or RFA regarding complete responseand survival. TACE has been used to minimize heat loss duetoperfusionmediated tissue cooling and to increase the ther-apeuticeffectofRFablation, thus increasing the rangeof ther-apeutic isotherms because of a greater sensitivity ofneoplastic cells to hyperthermia [29]. HCC therapy can bedivided according to the stage of the disease and degree ofliver impairment into curative versus palliative approaches.Curative treatments are reserved for patients without portalvein invasion or distant metastases. Palliative therapy viatransarterial chemoembolization (TACE) may be offered forunresectable HCC [30]. The patients should be monitoredregularly for exclusion of intrahepatic newly developed/recurrent lesions by follow-up protocol including enhancedMDCT examinations and tumor markers.
Conflict of interest
No conflict of interests.
References
[1] Ming S, Ji-An C, Xiao-Jun L, Rong-Ping G. Transarterialchemoembolization as initial treatment for unresectablehepatocellular carcinoma in southern China. World J Gastroenterol2010;16(2):264–9.
[2] Howard JH, Tzeng CW, Smith JK, et al. Radiofrequency ablation forunresectable tumors of the liver. Am Surg 2008;74(7):594–600.
[3] Shirin E, Nigel H. Contemporary strategies in the management ofhepatocellular carcinoma. HPB Surg 2012. 8 pages 154056.
[4] Brunello F, Veltri A, Carucci P, et al. Radiofrequency ablation versusethanol injection for early hepatocellular carcinoma: a randomizedcontrolled trial. Scand J Gastroenterol 2008;43(6):727–35.
[5] Luigi R, Federica Z, Anselmo P, et al. Current approach in thetreatment of hepatocellular carcinoma. World J Gastrointest Oncol2010;2(9):348–59.
[6] Thomas J, Michael T, Henrik S, Martin M, Adrian S, et al. Transarterialchemoembolization for hepatocellular carcinoma: volumetric and
morphologic CT criteria for assessment of prognosis and therapeuticsuccess-results from a liver transplantation center. Radiology2000;214(2):349–57.
[7] Ohmoto K, Yoshioka N, Tomiyama Y, et al. Comparison of therapeuticeffects between radiofrequency ablation and percutaneousmicrowave coagulation therapy for small hepatocellularcarcinomas. J Gastroenterol Hepatol 2009;24(2):223–7.
[8] Zhu AX, Salem R. Combining transarterial chemoembolization withradiofrequency ablation for hepatocellular carcinoma one stepforward? J Clin Oncol 2013;31:406–8.
[9] Bruix J, Sherman M, Llovet JM, et al. Clinical management ofhepatocellular carcinoma: conclusions of the Barcelona-2000 EASLconference. Barcelona, Spain, September 15–17, 2000. J Hepatol2001;35:421–30.
[10] Mabrouk GM. Prevalence of hepatitis C infection withschistosomiasis in Egyptian patients with hepatocellularcarcinoma. Dis Markers 1997;13(3):177–82.
[11] Khalifa A, Mady EA, Abadeer N, et al. Differential tumor markers andhepatitis markers profile in liver tumors. Anticancer Res 1999;19(4A):2495–500.
[12] Yates SC, Hafez M, Hassan Z, et al. Hepatocellular carcinoma inEgyptians with and without history of hepatitis B virus infection:association with hepatitis C virus infection but not with HCV RNAlevel. Am J Trop Med Hyg 1999;60(4):714–20.
[13] Darwish MA, Amer AF, El-Moeity AA, Darwish NM. Hepatitis C and Bviruses, and their association with hepatocellular carcinoma inEgypt. J Egypt Public Health Assoc 1997;72(5–6):569–89.
[14] Llovet JM, Fuster J, Bruix J. Prognosis of hepatocellular carcinoma.Hepatogastroenterology 2002;49(43):7–11.
[15] Thomas JV, Thomas KH, Martin GM, et al. Percutaneous tumorablation in medical radiology, vol. 1(2). Berlin, Heidelberg: Springer;2008. p. P47–62.
[16] Goldberg SN. Radiofrequency tumor ablation: principles andtechniques. Eur J Ultrasound 2001;13(2):129–47.
[17] Raut CP, Izzo F, Marra P, et al. Significant long-term survival afterradiofrequency ablation of unresectable hepatocellular carcinoma inpatients with cirrhosis. Ann Surg Oncol 2005;12(8):616–28.
[18] Teratani T, Yoshida H, Shiina S. Radiofrequency ablation forhepatocellular carcinoma in so-called high-risk locations.Hepatology 2006;43(5):1101–8.
[19] Chen MH, Yang W, Yan K, et al. Treatment efficacy of radiofrequencyablationof338patientswithhepaticmalignant tumor and the relevantcomplications. World J Gastroenterol 2005;11(40):6395–401.
[20] De Baere T, Risse O, Kuoch V, et al. Adverse events duringradiofrequency treatment of 582 hepatic tumors. AJR Am JRoentgenol 2003;181(3):695–700.
[21] Akahane M, Koga H, Kato N, et al. Complications of percutaneousradiofrequency ablation for hepatocellular carcinoma: imagingspectrum and management. RadioGraphics 2005;25(Suppl 1):S57–68.
[22] Stuart K. Chemoembolization in the management of liver tumors.Oncologist 2003;8(5):425–37.
[23] Raoul JL, Heresbach D, Bretagne JF, et al. Chemoembolization ofhepatocellular carcinomas. A study of the biodistribution andpharmacokinetics of doxorubicin. AJR 2011;197(4):W590–602.
[24] Vogl TJ, Naguib NN, Nour-Eldin NA, et al. Review on transarterialchemoembolization in hepatocellular carcinoma: palliative,combined, neoadjuvant, bridging, and symptomatic indications.Eur J Radiol 2009;72(3):505–16.
[25] Steven AC, Francesco I, Lee ME, et al. Radiofrequency ablation ofhepatocellular cancer in 110 patients with cirrhosis. Ann Surg2000;232(3):381–91.
[26] Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial oftransarterial lipiodol chemoembolization for unresectablehepatocellular carcinoma. J Hepatol 2002;35:1164–71.
[27] Othman HM, Mourad AF, Abdellah MH, Imam HM. Combined versussingle locoregional therapy in the treatment of unresectablehepatocellulaar carcinoma. EJRNM 2014;45(2):395–401.
[28] Hu HT, Kim JH, Lee LS, Kim KA, Ko GY, Yoo HK, et al.Chemoembolization for HCC: multivariate analysis of predictingfactors for tumor response and survival in 362 patient cohort. J VascInterv Radiol 2011;22:917–23.
[29] Nahum GS, Dupuy DE. Image-guided radiofrequency tumorablation: challenges and opportunities – Part I. J Vasc Interv Radiol2001;12(9):1021–32.
[30] Bertelli E, Di Gregorio F, Bertelli L, Civeli L, Mosca S. The arterialblood supply of the pancreas: a review. III. The inferiorpancreaticoduodenal artery. An anatomical review and aradiological study. Surg Radiol Anat 1996;18(2):67–74.