Embed Size (px)
Citation preview

Communicating Health Story Project Value
A Series of Roundtable Meetings Focused on Educating our Membership

Agenda
Overview
1. The historical view
2. The key components of a standard presentation
3. Varying the presentation by audience
4. The basic elements of a Health Story Project elevator speech
5. Questions and Answer Session

PanelistsName Company and Contact Information
Juergen Fritsch M*Modal, Chief [email protected]
Liora Alschuler Lantana Consulting Group, [email protected]
Mark L. Morsch Optum360, VP of Technology, NLP [email protected]
Nick Mahurin InfraWare, [email protected]
Alex Lippitt HIMSS, Sr. Director of Interoperability and [email protected]

Overview1. Purposes of Today’s Roundtable
• How to Communicate Health Story Project Value • How to Represent the Health Story Project to Different
Groups
2. Format
• Panel presents; questions will be held to the end of presentations; please put your questions in the WebEx chat window
3. Follow up• Resources• Try It – Be Bold!

1. The historical view: The beginning, the middle and the end, and where we are going next
Juergen Fritsch

Clinical Documentation Challenge
• Tedious manual process,
• Time-consuming,
• Documentation lacks expressiveness of natural language
• Transcription can be expensive
• Subject to longer turn-around times
• Clinical data lost, because documents are neither structured nor encoded.
Direct Data Entry: Structured and encoded information.
Dictation: Fast and easy, expressive.

JAMA 2012; 307 (23): 2497-2498

Health Story - Vision
• Comprehensive Electronic Records that Tell a Patient’s Complete Health Story
• 1.2B narrative clinical documents produced by US healthcare system annually
• Constitutes 60% of all clinical data
• Narrative documents underutilized in today’s EHR systems

Health Story - Beginnings
• Health Story started in 2006 as an alliance of healthcare vendors, providers and associations
• Pooled resources in a rapid development initiative
• Produced Health Level 7 (HL7) data standards for the flow of information between
• common types of healthcare documents, and
• EHR systems
• Building on HL7 CDA standard
• CDA for Common Document Types (CDA4CDT)

Health Story - Continued
• Joining forces with Integrating the Healthcare Enterprise USA (IHE) and
• The Office of the National Coordinator’s Standards and Interoperability Framework
• Harmonized work across organizations to produce
• Consolidated Clinical Document Architecture standard (C-CDA)
• Now included in Meaningful Use Stage 2
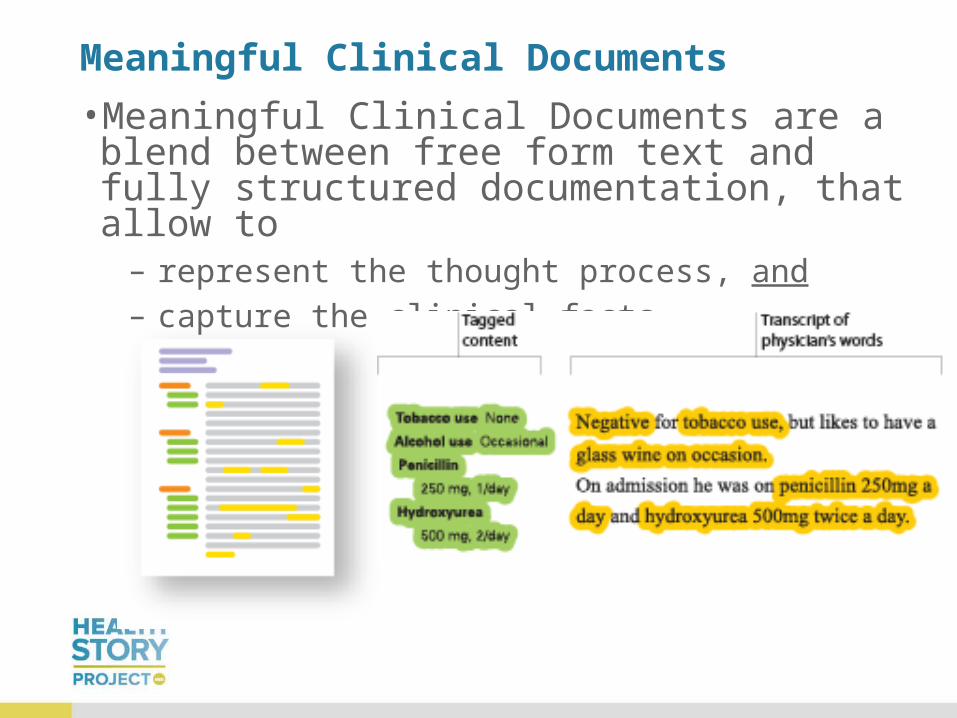
Meaningful Clinical Documents
• Meaningful Clinical Documents are a blend between free form text and fully structured documentation, that allow to
– represent the thought process, and – capture the clinical facts

Consolidated CDA
• CCD
• Consultation Note
• Diagnostic Imaging Report
• Discharge Summary
• H&P
• Operative Note
• Procedure Note
• Progress Note
• Unstructured Document

Health Story – New Umbrella
• HIMSS takes on management of Health Story project in January 2013
• Providing global leadership and greater exposure among healthcare IT community
• Any HIMSS member can opt-in at no charge
• Sponsors can continue to promote and expand the project

Health Story - Constituency
• Spanning Clinical Documentation Lifecycle:
• Electronic Information Capture
• Dictation/Transcription/Voice Recognition
• Natural Language Processing
• Computer Assisted Coding (CAC)
• Narrative Data Mining & Analytics
• Document Management
Health Story – Mission Moving Forward
• Establish a strong and effective coalition of members and partners
• Maintain relevance & adoption in nationally-recognized standards bodies
• Raise awareness and foster adoption of the Health Story approach to improve information exchange in three areas:
• Coordinated patient care
• Payer-provided integration
• Population health
2. The key components of a standard presentation, the key messages
Liora Alschuler

Key Points
• Problem Statement • The migration from paper to
electronic records has to work for everyone
• Today, clearly not the case• Response
• Standards that integrate narrative, coded elements
• Align policy with standards, technology
“It was so much easier when I could just say what I wanted.”
John Spinosa, MD, quoting a colleague
Interoperability for Everyone

Challenge
“I have never seen…a checkbox for apprehension…”
“The medical record is not data. It contains data… but it is not data, nor is it simply a repository into which data are poured.”
And who does it serve? Clinician & patient or…
“... a small army of people who “need” to knowwhat happened in the examination room or at the bedside…”
JAMA, Internal Medicine, published online, May 27, 2013

Challenge
JAMIA, published online, January 12, 2011
Structured data capture can be at odds with the expressivity, workflow, and usability factors preferred by clinicians.
Authors recommend choice in data capture and text processing modalities.

Key Points: Response
• We can create an electronic record that ensures value for
– Care delivery
– Evidence-based medicine
– And which endures over time, as technology evolves
• Vision
– Comprehensive electronic records that
– Tell a patient’s complete health story.

How?
• Use simple, stable, established formats for information exchange.
• Mix data and narrative.
• Go Big
• This will be:
– Less disruptive
– More useful

Investing in Information
• CDA can be simple• CDA can be complex• Simple encoding relatively inexpensive, complex encoding costs
more
• Gall's Law is a rule of thumb from John Gall's Systemantics:
How Systems Really Work and How They Fail:
– A complex system that works is invariably found to have
evolved from a simple system that worked.
– The inverse proposition also appears to be true: A complex
system designed from scratch never works and cannot be
made to work. You have to start over, beginning with a
working simple system.

CDA Basics
• A Header + Body
• CDA Header: metadata
• CDA Body
• narrative (free-text) form required and
• coded (computable) form optional

Incremental Approach
NarrativeText
HL7 CDA Structured Documents
Coded Discrete Data Elements
Decision Support
Meaningful Use!
Clinical Applications
SNOMED CT
Disease, DF-00000
Metabolic Disease, D6-00000
Disorder of glucose metabolism, D6-50100
Diabetes Mellitus, DB-61000
Type 1, DB-61010
Insulin dependant type IA, DB-61020
Neonatal, DB75110
Carpenter Syndrome, DB-02324
Disorder of carbohydrate metabolism, D6-50000
Quality Reporting
1. Get the data flowing, get the data flowing, get the data flowing.
2. Incrementally add structure, where cost effective to do so.

We are looking for a shift in policy
• Lower the threshold for information exchange so that
– all may participate
– approach 100% of the records for 100% of patients
• Incentivize participation at all levels of interoperability
• Recognize diversity of applications
• Respect the clinical voice
• Provide value back to those who incur the costs

• A health record is the patient’s “health story”
• The primary purpose of the record is to support care delivery
• Electronic records must produce a longitudinal record of lasting value: expressive, data conversion-proof
• Clinical records must be complete, well organized, easy to navigate, concise, logical, adaptable to the needs of the user, sharable, and secure.
• Electronic records and new technologies
– support shared decision-making,
– document use of practice guidelines, and
– support evidence-based practice.
Value Statement

Here is how to vary the value statement by audience…

3. Varying the presentation by audience / key value for each
Mark Morsch
Varying the presentation by audience / key value for each
• CXOs of Health Systems• Clinicians• Care Managers• Patients• Payers• Researchers and Analysts• HIM• EHR Vendors

Highlights of Value Statement
• Quality of Documentation
• Ease of Use
• Support for Clinical Decision Making
• Continuity of Care
• Accurate and Complete Electronic Record
• New era of participation by patients, families, and their caregivers
• Providing authorized access to a complete record
• Recognizes and Supports secondary use of data
• Articulating a comprehensive roadmap for interoperable electronic records
• Encouraging and supporting development of cohesive, harmonized specifications

Matching the Value
• CXOs of Health Systems
• Clinicians
• Care Managers
• Patients
• Payers
• Researchers and Analysts
• HIM
• EHR Vendors
• Quality of Documentation
• Ease of Use
• Support for Clinical Decision Making
• Continuity of Care
• Accurate and Complete Electronic Record
• New era of participation by patients, families, and
their caregivers
• Providing authorized access to a complete record
• Recognizes and Supports secondary use of data
• Articulating a comprehensive roadmap for
interoperable electronic records
• Encouraging and supporting development of
cohesive, harmonized specifications

Matching the Value - Clinicians
• CXOs of Health Systems
• Clinicians
• Care Managers
• Patients
• Payers
• Researchers and Analysts
• HIM
• EHR Vendors
• Quality of Documentation
• Ease of Use
• Support for Clinical Decision Making
• Continuity of Care
• Accurate and Complete Electronic Record
• New era of participation by patients, families, and
their caregivers
• Providing authorized access to a complete record
• Recognizes and Supports secondary use of data
• Articulating a comprehensive roadmap for
interoperable electronic records
• Encouraging and supporting development of cohesive,
harmonized specifications

Matching the Value - Patients
• CXOs of Health Systems
• Clinicians
• Care Managers
• Patients
• Payers
• Researchers and Analysts
• HIM
• EHR Vendors
• Quality of Documentation
• Ease of Use
• Support for Clinical Decision Making
• Continuity of Care
• Accurate and Complete Electronic Record
• New era of participation by patients,
families, and their caregivers
• Providing authorized access to a complete
record
• Recognizes and Supports secondary use of
data
• Articulating a comprehensive roadmap for
interoperable electronic records
• Encouraging and supporting development of
cohesive, harmonized specifications

Matching the Value - HIM
• CXOs of Health Systems
• Clinicians
• Care Managers
• Patients
• Payers
• Researchers and Analysts
• HIM
• EHR Vendors
• Quality of Documentation
• Ease of Use
• Support for Clinical Decision Making
• Continuity of Care
• Accurate and Complete Electronic Record
• New era of participation by patients, families, and
their caregivers
• Providing authorized access to a complete
record
• Recognizes & Supports secondary use of data
• Articulating a comprehensive roadmap for
interoperable electronic records
• Encouraging and supporting development of
cohesive, harmonized specifications

4. The basic elements of a Health Story Project elevator pitch
Nick Mahurin

Goal
Create a hook so they want to follow up to learn more.

View from Space
Risk: Don’t try to accomplish too much.
Two pillars:• Concept• Relevance

Concept
Started by an industry consortium dedicated to preserving narrative (as the EMR era took hold with it’s emphasis on structured data) by developing templates for common medical report types using a healthcare specific implementation of XML called CDA.

Relevance
• In addition to creating these templates under an associated charter agreement with HL7, the Department of HHS included Consolidated CDA in Meaningful Use Stage 2 requirements for EMRs.
• The powerful implication is that, arguably for the first time ever, we have a common electronic record that all EMRs are required to be able to send and receive.
• This is a monumental achievement in health information and will support providers sharing information as well as service providers.

Vary by Audience
Even more essential in a shorter presentation.
Examples:
• XML – Only for IT people you expect already understand the Health Story Project
• Narrative/ Structured – Need to be spelled out for some audiences.
www.himss.org/health-story-projectListen to our recordings from Past Roundtable Meetings Online
Resources
• Health Story Project Website
– www.himss.org/health-story-project
• For more information or assistance contact:
– Alex Lippitt at [email protected]
– Nancy Ramirez at [email protected]





























