-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
1/13
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
2/13
n engl j med 373;5 nejm.org July 30,
2015416
T h e n e w e n g l a n d j o u r n a l o
f medicine
Pneumonia is a leading infectious
cause of hospitalization and death amongadults in the United
States,1,2 with medical
costs exceeding $10 billion in 2011.3 Routine
ad-ministration of the pneumococcal conjugate vac-cine in children
has resulted in an overall reductionin the rate of invasive disease
and pneumonia
among adults, owing to herd immunity.4-8 The lastU.S.
population–based incidence estimates ofhospitalization due to
community-acquired pneu-monia were made in the 1990s,9 before
the avail-ability of the pneumococcal conjugate vaccine andmore
sensitive molecular and antigen-based labo-ratory diagnostic tests.
Thus, contemporary pop-ulation-based etiologic studies involving
U.S. adults with pneumonia are needed.10-13
The Centers for Disease Control and Prevention(CDC) Etiology of
Pneumonia in the Community(EPIC) study was a prospective,
multicenter, pop-ulation-based, active surveillance study.
Radio-graphic confirmation and extensive diagnosticmethods were
used to determine the incidence andmicrobiologic causes of
community-acquiredpneumonia requiring hospitalization among
U.S.adults.
Methods
Active Population-Based Surveillance
From January 1, 2010, to June 30, 2012, adults 18
years of age or older were enrolled at three hos-pitals in
Chicago (John H. Stroger, Jr., Hospitalof Cook County, Northwestern
Memorial Hospi-tal, and Rush University Medical Center) and attwo
in Nashville (University of Tennessee HealthScience Center–Saint
Thomas Health and Vander-bilt University Medical Center). We sought
toenroll all eligible adults; therefore, trained staffscreened
adults for enrollment at least 18 hoursper day, 7 days per week.
Written informed con-sent was obtained from all the patients or
theircaregivers before enrollment. The study protocol
was approved by the institutional review boardat each
participating institution and at the CDC.Weekly teleconferences,
enrollment reports, dataaudits, and annual study-site visits were
con-ducted to ensure uniform procedures among thestudy sites.
Patients or their caregivers provideddemographic and epidemiologic
data, and medi-cal charts were abstracted for clinical data. All
theauthors vouch for the accuracy and completenessof the data and
analyses reported and for the
fidelity of the study to the protocol. All the au-thors made the
decision to submit the manuscriptfor publication.
Adults were eligible for enrollment if they were admitted
to a study hospital on the basis ofa clinical assessment by the
treating clinician;resided in the study catchment area (see the
Sup-
plementary Appendix, available with the full textof this article
at NEJM.org); had evidence ofacute infection, defined as reported
fever orchills, documented fever or hypothermia, leuko-cytosis or
leukopenia, or new altered mental sta-tus; had evidence of an acute
respiratory illness,defined as new cough or sputum production,chest
pain, dyspnea, tachypnea, abnormal lungexamination, or respiratory
failure; and had evi-dence consistent with pneumonia as assessed
bymeans of chest radiography by the clinical team within 48
hours before or after admission.
Patients were excluded if they had been hos-pitalized recently
(
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
3/13
n engl j med 373;5 nejm.org July 30, 2015
417
Pneumonia Requir ing Hospitalization among U.S. Adults
asked to return 3 to 10 weeks after enrollment
forconvalescent-phase serum collection.
Radiographic Confirmation
Initial enrollment was based on the clinical inter-pretation of
chest radiographs that were ob-tained at admission. Inclusion in
the final study
analyses required independent confirmation bya board-certified
chest radiologist who reviewedall the chest radiographs and
computed tomo-graphic scans obtained within 48 hours beforeor after
admission; these radiologists, who arecoauthors of the study, were
unaware of the clini-cal data. Radiographic evidence of pneumonia
wasdefined as the presence of consolidation (a denseor fluffy
opacity with or without air broncho-grams), other infiltrate
(linear and patchy alveolaror interstitial densities), or pleural
effusion.5,15,16
Controls
From November 1, 2011, to June 30, 2012, a con- venience
sample of asymptomatic adults from theNashville study catchment
area who presentedfor nonacute care to a general medicine clinic
atVanderbilt University Medical Center was enrolled weekly.
Nasopharyngeal and oropharyngeal swabs were obtained to assess
the prevalence of respi-ratory pathogens among asymptomatic
adults.Exclusion criteria were the same as those for theadults with
pneumonia, except that controls were
also excluded if they had fever or respiratorysymptoms within 14
days before or after enroll-ment (on the basis of information
obtained dur-ing a telephone interview) or had received
liveattenuated influenza vaccination within 7 daysbefore
enrollment.
Laboratory Testing
Bacterial culture was performed, with the use ofstandard
techniques, on blood samples, pleuralfluid, high-quality sputum
samples and endotra-cheal aspirates, and quantified
bronchoalveolar-
lavage specimens.17,18
A real-time polymerase-chain-reaction (PCR) assay for
legionella wasperformed on sputum regardless of the qualityof the
sample.19,20 PCR assays targeting Entero-bacteriaceae,
Haemophilus influenzae , pseudomonas,Staphylococcus
aureus , Streptococcus anginosus , S. mitis ,S.
pneumoniae , and S. pyogenes were also performedon
pleural fluid.21-23 Urinary antigen testing wasperformed for
the detection of Legionella pneumophi-la and S.
pneumoniae (BinaxNOW, Alere).20,24
A PCR assay was performed on nasopharyn-geal and oropharyngeal
swabs with the use ofCDC-developed methods for the detection of
ad-enovirus; Chlamydophila pneumoniae ; coronaviruses229E,
HKU1, NL63, and OC43; human metapneu-movirus (HMPV); human
rhinovirus; influenzaA and B viruses; Mycoplasma pneumoniae ;
parain-
Figure 1. Screening, Eligibility, and Enrollment of Patients with Pneumonia.
CT denotes computed tomography.
2488 (68%) Were enrolled
3634 Were eligible
1146 (32%) Were not enrolled795 (69%) Declined to participate152
(13%) Were not approached108 (9%) Were not able to provide
informed consent, and asurrogate was not available
91 (8%) Did not speak English, andan interpreter was not
available
168 (7%) Were excluded from finalanalysis
161 (96%) Did not have radiographicevidence of pneumonia7 (4%)
Withdrew consent
100,050 Adults underwent screening
2320 (93%) Had radiographic evidenceof pneumonia
2241 (97%) Had chest radiographs thatmet final radiographic
inclusioncriteria of consolidation, infiltrate,or effusion
71 (3%) Had a chest radiograph com-pleted that did not meet the
criteriafor radiographic evidence of pneumonia, but had CT
scans thatmet the criteria
8 (
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
4/13
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
5/13
n engl j med 373;5 nejm.org July 30, 2015
419
Pneumonia Requir ing Hospitalization among U.S. Adults
was detected in a nasopharyngeal or oropharyn-geal swab by
means of PCR assay or if a patho-gen-specific antibody titer was
increased by afactor of 4 or more between the acute-phase se-rum
specimen and the convalescent-phase serum
specimen for all viruses except human rhinovi-rus and
coronaviruses. Fungal or mycobacterialdetections were determined
according to clinicalguidelines (see the Supplementary
Appendix).
Statistical Analysis
Annual incidence rates were calculated from July1, 2010, to June
30, 2011, and from July 1, 2011,to June 30, 2012. The number of
enrolled adults with radiographic evidence of pneumonia
was
adjusted, according to age group, for the propor-tion of
eligible adults enrolled at each study siteand for the estimated
proportion of admissionsof adults for pneumonia to study hospitals
in thecatchment area (i.e., the market share, which was
based on discharge-diagnosis codes). The adjustednumber was then
divided by the U.S. Census popu-lation estimates in the catchment
area for thecorresponding year (see the Supplementary
Ap-pendix).33
We calculated pathogen-specific incidencerates by multiplying
the total incidence of pneu-monia by the proportion of each
pathogen de-tected among adults with radiographic evidenceof
pneumonia who had samples available for the
Characteristic
Adults with Radiographic Evidence of Pneumonia
(N = 2320)
Pneumonia severity index∥
Median 76
Interquartile range 52–103
Risk class — no. (%)
1–3 1510 (65)
4 606 (26)
5 204 (9)
* Race and ethnic group were self-reported.† Data were missing
for three patients.‡ Any underlying medical condition included
chronic lung disease (asthma, chronic obstructive pulmonary
disease, or
obstructive sleep apnea), chronic heart disease (i.e., coronary
artery disease or congestive heart failure, but not hyper-tension),
immunosuppression (either due to chronic condition or medication,
cancer [but not skin cancer], or humanimmunodeficiency virus [HIV]
infection with a CD4 cell count of >200 per cubic millimeter),
diabetes mellitus, chronickidney disease (with or without
dialysis), neurologic disorders (epilepsy, cerebral palsy,
dementia, or history of stroke),
chronic liver disease (hepatitis, cirrhosis, or hepatic
failure), and splenectomy. The specific conditions that affected
atleast 25% of patients are l isted here. Among the 685 patients
with immunosuppression, 416 had nondermatologic can-cer (but did
not have neutropenia), 381 had immunosuppression due to a chronic
condition or a medication, and 68had HIV infection with a CD4 cell
count of more than 200 per cubic millimeter. The groups were not
mutually exclusive.
§ Data were based on verified vaccine information and not
self-report. For influenza vaccine, the season was defined
asSeptember 1 through August 31 of the following year, and the
percentage of patients vaccinated was based on the 1898of 2320
adults (82%) for whom information was available. For pneumococcal
polysaccharide vaccine, the percentage ofpatients vaccinated was
based on 704 of 832 adults (85%) who were 65 years of age or older
and had available infor-mation. For both vaccines, patients were
considered to be vaccinated if they had received the vaccine at
least 2 weeksbefore admission. Outpatient antibiotics were defined
as those received within 5 days before admission. Inpatient
anti-biotics were defined as those received at any point during the
hospitalization.
¶ The categories were not mutually exclusive and therefore do
not sum to 100%. Only 23 adults (1%) had pleural effu-sion alone.
Among all the patients with pleural effusion, 481 had unilateral
pleural effusion, 232 had bilateral pleural ef-fusion, and 1 had
unknown status. Among the 853 patients in whom a pathogen was
detected, 65% had consolidation,38% had infiltrate, and 26% had
pleural effusion. There were radiographic differences between the
530 patients whohad only viruses detected and the 247 who had only
bacteria detected with respect to consolidation (59% vs. 73%),
in-
filtrate (42% vs. 31%), and pleural effusion (23% vs.
33%).∥ The pneumonia severity index is a clinical prediction
rule for mortality related to community-acquired pneumonia that
is based on sex, age, nursing home status, mental status, heart
rate, respiratory rate, blood pressure, temperature, se-lected
underlying medical conditions, selected laboratory values, and the
presence or absence of pleural effusion.34 Theindex is divided
into five classes, with higher class indicating greater risk. Class
1 to 3 indicates a low risk of death,class 4 moderate risk, and
class 5 high risk.
Table 1. (Continued.)
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
6/13
n engl j med 373;5 nejm.org July 30,
2015420
T h e n e w e n g l a n d j o u r n a l o
f medicine
P a t i e n t s w i t h a P o s i t i v e R e s u l t ( % )
9
8
7
6
4
3
1
5
2
0
P a t i e n t s ( n o . )
160
140
120
100
60
40
80
20
0
30
25
20
15
5
0
10
15
10
5
0
H u m a
n r h i n
o v i r u
s
J a n. F e
b.
M a r c
h A p
r i l M a y
J u n e
J u l y
A u g .
S e p t.
O c
t. N o
v. D e
c.
I n f l u e
n z a A
o r B
S . p n
e u m o
n i a e
H u m a n
m e t a
p n e u
m o v i r
u s
R e s p i r a t o
r y s y n
c y t i a l
v i r u
s
P a r a i
n f l u e
n z a v
i r u s
C o r o
n a v i r
u s
M y c o p l a
s m a p
n e u m
o n i a e
S . a u
r e u s
A d e n
o v i r u
s
L e g i o n
e l l a p
n e u m
o p h i l
a
E n t e r
o b a c
t e r i a c
e a e
O t h e
r
B
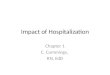
A Specific Pathogens Detected
Pathogens Detected, According to Month and Year
Copathogen
Single pathogen
Pathogen
Detected
2010 2011 2012
J a n. F e
b.
M a r c
h A p
r i l M a y
J u n e
J u l y
A u g .
S e p t.
O c
t. N o
v. D e
c.
J a n. F e
b.
M a r c
h A p
r i l M a y
J u n e
194
132
115
88
68 67
53
3732 32 31
74
43
Viral pathogen only (22%)
Viral–viral co-detection (2%)
Bacterial–viral co-detection (3%)
Bacterial pathogen only (11%)
Fungal or mycobacterial detection (1%)
No pathogendetected(62%)
Influenza A or B
Human rhinovirus
Respiratory syncytial virus
S. pneumoniae
S. aureus
Human metapneumovirus
All causes of pneumonia
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
7/13
n engl j med 373;5 nejm.org July 30, 2015
421
Pneumonia Requir ing Hospitalization among U.S. Adults
detection of both bacterial and viral pathogens.
Bootstrap methods with 10,000 samples wereused to calculate 95%
confidence intervals.
Results
Study Population
Of 3634 eligible adults, 2488 (68%) were enrolled(Fig. 1). As
compared with persons who wereeligible but not enrolled, the
enrolled patients were significantly less likely to be 65
years of ageor older and less likely to require invasive
me-chanical ventilation; in addition, a smaller propor-
tion of the enrolled patients subsequently died(Table S1 in the
Supplementary Appendix).
Of 2488 enrolled patients, 2320 (93%) hadradiographic evidence
of pneumonia (Fig. 1).The median age of the patients with
radiographicevidence of pneumonia was 57 years (interquar-tile
range, 46 to 71) (Table 1), and the medianlength of hospital stay
was 3 days (interquartile
range, 2 to 6). A total of 498 patients (21%) re-quired
admission to the intensive care unit (ICU),131 (6%) required
invasive mechanical ventilation,and 52 (2%) died during
hospitalization.
Detection of Pathogens
Nasopharyngeal and oropharyngeal swabs were
obtained from 2272 of the 2320 adults (98%) with
radiographic evidence of pneumonia, bloodfor culturing from 2103
(91%), a specimen for uri-nary antigen detection from 1973 (85%), a
sputumspecimen from 960 (41%) (of whom 272 had ahigh-quality
specimen), paired serum specimensfrom 859 (37%), a
bronchoalveolar-lavage speci-men from 84 (4%), a pleural-fluid
specimenfrom 78 (3%), and an endotracheal aspirate from4 (
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
8/13
n engl j med 373;5 nejm.org July 30,
2015422
T h e n e w e n g l a n d j o u r n a l o
f medicine
tary Appendix). A pathogen was detected less fre-quently in
nasopharyngeal and oropharyngealswabs obtained from 238
asymptomatic controlsthan in swabs obtained from 192 patients
withpneumonia who were enrolled during the sameperiod in the same
catchment area (2% vs. 27%,P
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
9/13
n engl j med 373;5 nejm.org July 30, 2015
423
Pneumonia Requir ing Hospitalization among U.S. Adults
the increased specificity of radiographic confir-mation in our
case definition.1,2,6
Despite our efforts to use more sensitive andspecific diagnostic
methods than had beenavailable previously,11-13,19-29
pathogens were de-tected in only 38% of adults. Possible reasons
forsuch few detections include an inability to ob-tain lower
respiratory tract specimens, antibioticuse before specimen
collection, insensitive diag-
nostic tests for known pathogens, a lack of test-ing for other
recognized pathogens (e.g., coxi-ella), unidentified pathogens, and
possiblenoninfectious causes (e.g., aspiration
pneumoni-tis).10,13,35,36 We may also have missed
precedingmicrobiologic insults that triggered a subse-quent
hospitalization for pneumonia. Neverthe-less, our
pathogen-detection yield is within therange (20 to 76%) of the
yield in other etiologic
Figure 3. Estimated Annual Pathogen-Specific
Incidence Rates of Community-Acquired Pneumonia Requiring Hospitalization,
According to Age Group.
Circles indicate the annual number of hospitalizations for
pneumonia per 10,000 adults, and the horizontal lines 95%
confidence inter-
vals. Rates are based on 10,511,911 person-years of observation.
Note the differences in the scale of the x axis for the groups of
pa-tients 65 to 79 years of age and 80 years of age or older, as
compared with the groups of patients 18 to 49 years of age and 50
to 64
years of age.
Adenovirus
M. pneumoniae
Coronavirus
Respiratory
syncytial virusParainfluenza
virus
Human meta-pneumovirus
Influenza A or B
L. pneumophila
S. aureus
S. pneumoniae
Humanrhinovirus
0.0 0.5 1.0 1.5 2.0 2.5
Incidence per 10,000 Persons
C Persons 65–79 Yr of Age
D
Persons ≥80 Yr of Age
A
Persons 18–49 Yr of AgeAdenovirus
M. pneumoniae
Coronavirus
Respiratorysyncytial virus
Parainfluenzavirus
Human meta-pneumovirus
Influenza A or B
L. pneumophila
S. aureus
S. pneumoniae
Humanrhinovirus
0.0 0.5 1.0 1.5 2.0 2.5
Incidence per 10,000 Persons
B
Persons 50–64 Yr of Age
Adenovirus
M. pneumoniae
Coronavirus
Respiratorysyncytial virus
Parainfluenzavirus
Human meta-pneumovirus
Influenza A or B
L. pneumophila
S. aureus
S. pneumoniae
Humanrhinovirus
0 5 10 15 20
Incidence per 10,000 Persons
Adenovirus
M. pneumoniae
Coronavirus
Respiratorysyncytial virus
Parainfluenzavirus
Human meta-pneumovirus
Influenza A or B
L. pneumophila
S. aureus
S. pneumoniae
Humanrhinovirus
0 5 10 15 20
Incidence per 10,000 Persons
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
10/13
n engl j med 373;5 nejm.org July 30,
2015424
T h e n e w e n g l a n d j o u r n a l o
f medicine
studies of pneumonia in adults, although it iscloser to the
lower end of the range9,37-43 andcontrasts with the detection
yield in the pediat-ric EPIC study, in which pathogens were
detectedin 81% of children who had been hospitalized with
community-acquired pneumonia.44 The lowpathogen-detection
yield among adults who were
hospitalized for pneumonia highlights the needfor more sensitive
diagnostic methods and in-novative discovery of pathogens.45
Viruses were detected in 27% of the patients.Human rhinovirus
was the most commonly de-tected virus in patients with pneumonia
but wasrarely detected in asymptomatic controls, a f ind-ing
similar to that in other studies.37,46 Althoughour
understanding of human rhinovirus remainsincomplete, these data
suggest a role for humanrhinovirus in adult
pneumonia.35,47 Influenza vi-rus was the second most common
pathogendetected, despite mild influenza seasons duringthe
study.48 The incidence of influenza virus wasalmost twice that
of any other pathogen (exceptfor human rhinovirus) among adults 80
years ofage or older, which underscores the need forimprovements in
influenza-vaccine uptake andeffectiveness.49
Together, HMPV, RSV, parainfluenza viruses,coronaviruses, and
adenovirus were detected in13% of the patients, a proportion
similar to thosefound in other PCR-based etiologic studies of
pneumonia in adults (11 to 28%).
11,37-41
Amongadults 80 years of age or older, the incidence ofRSV,
parainfluenza virus, and coronavirus each was similar to that
of S. pneumoniae . Our studyadds to the growing evidence of
the contributionof viruses to hospitalizations of adults,
high-lighting the usefulness of molecular methodsfor the detection
of respiratory pathogens.35,47,50,51 The lower circulation of
respiratory viruses in the2011–2012 season (Fig. 2B), as compared
with theprevious year, probably contributed to the lowerincidence
of pneumonia in that year and is sup-
ported by national surveillance data.48
Bacterial pathogens were detected in 14% ofthe patients. S.
pneumoniae was the most commonlydetected bacterium, with
an incidence that wasalmost 5 times as high among adults 65 years
ofage or older as among younger adults. Theprevalence of
pneumococcal disease of 5% that was observed in our study was
lower than the 13%found by Marston et al.9 Although both
studiesused sputum culture, our study included only
high-quality sputum specimens for the detectionof non-legionella
bacteria, which probably im-proved specificity but decreased
sensitivity.17 Bac-terial cultures, especially in the context
of antimi-crobial use, are insensitive.13,52 Urinary
antigentests for pneumococcus, which were not availablefor the
study by Marston et al., were responsible
for the majority (67%) of pneumococcal detec-tions in our study.
These tests are more sensitivethan blood culture and improve the
detection ofnonbacteremic pneumococcal pathogens with areported
sensitivity of 70 to 80% and a specific-ity of more than
90%.9,13,24,52 Moreover, the indi-rect protection of adults as
a result of pediatricpneumococcal vaccination in the United
Statesprobably contributed to the lower observed inci-dence of
pneumococcal infection in our studythan in the study by Marston et
al.4-9 Our esti-mates provide an important benchmark to
mon-itor the effect of the 2014 vaccination recommen-dations for
the 13-valent pneumococcal conjugate vaccine in persons 65
years of age or older.53
M. pneumoniae , L. pneumophila, and C.
pneumoniae combined were detected in 4% of the adults.
Mar-ston et al. found that these pathogens wereidentified in 10% of
patients with definitecases of pneumonia and in 44% of those
withpossible cases.9 Although both our study andthat of
Marston et al. used urinary antigen testsfor L. pneumophila, the
detections of M. pneumoniae
and C. pneumoniae in the study by Marston et
al.relied exclusively on serologic testing, whichhas less
specificity than the PCR assay used inour study.9,19,20,54-56
Overall S. aureus was detected in 2% of adults— a
lower rate than that of S. pneumoniae or vi-ruses. The
low prevalences of Enterobacteriaceae(1%) and other gram-negative
bacteria were prob-ably due to the exclusion of patients with
knownrisk factors for these bacteria (e.g., patients withrecent
hospitalization, patients with severe immu-nosuppression, and
functionally dependent nurs-
ing home residents), which is consistent with thecontemporary
concept of community-acquiredpneumonia.10 S. pneumoniae ,
S. aureus , and Entero-bacteriaceae were significantly more
commonamong severely ill patients, accounting for 16%of the
detected pathogens among patients in theICU, as compared with 6%
among patients notin the ICU.
This study has limitations. First, we were notable to enroll
every eligible patient; patients who
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
11/13
n engl j med 373;5 nejm.org July 30, 2015
425
Pneumonia Requir ing Hospitalization among U.S. Adults
were 65 years of age or older and those who wereundergoing
invasive mechanical ventilation wereless likely to be enrolled; a
greater proportion ofnonenrolled patients than of enrolled
patientsdied during hospitalization. Although the inci-dence
calculations were adjusted for the enroll-ment differences
according to age, market share
data on severity were not available and preventedthe
calculations of severity-related incidence.
Second, specimens were not obtained frompatients who were not
enrolled, and amongthose who were enrolled, not all specimen
types were available, which could have led to underes-timation
or overestimation of the pathogen-spe-cific rates, including the
rates associated withsevere disease and older age. Owing to
ethicaland feasibility considerations, invasive proceduresto obtain
specimens directly from the lung werenot usually performed, which
may have reducedthe microbiologic yield.35 However, 97% of
theadults had at least one specimen type availablefor bacterial and
viral detection.
Third, the sensitivities and specificities of theavailable
diagnostic tests were imperfect. Al-though the majority of
blood-culture samples were collected before the administration
of anti-biotics, the yield was lower in the samples col-lected
after the administration of antibiotics.Thus, despite extensive
testing, pathogens mayhave been missed. Moreover, molecular
detec-
tion of viruses and atypical bacteria in the naso-pharynx and
oropharynx does not necessarilyindicate causation and could
represent infectionthat is limited to the upper respiratory tract
orconvalescent-phase shedding. Similarly, urinarypneumococcal
antigen can be present for weeksafter the onset of pneumococcal
pneumonia,and recent pneumococcal vaccination can leadto false
positive results.52
Fourth, we were not able to enroll asymptom-atic controls for
the entire study period or inboth Chicago and Nashville, so it is
possible that
we missed detecting pathogens that were morecommonly
circulating at other times or in otherplaces. However, as in other
studies,37,40,46 patho-gens were rarely detected among adult
asymp-tomatic controls, which suggests that the respi-ratory
viruses and atypical bacteria that wereidentified in patients with
pneumonia may havecontributed to disease.
Fifth, the clinical and radiographic featuresof pneumonia
overlap with those of other syn-
dromes, including chronic lung disease and con-gestive heart
failure, such that even strict defini-tions may not accurately
distinguish amongthese entities, resulting in potential
misclassifi-cation. However, this situation is consistent withthe
real-world challenges of diagnosing pneu-monia and of its
subsequent management. Fi-
nally, data from our five urban hospitals (threeacademic, one
public, and one community), al-though inclusive of diverse
communities, may notbe representative of the entire U.S. adult
popula-tion or generalizable to other settings, since
thecirculation of respiratory pathogens varies ac-cording to
geographic region, timing, and otherfactors.
In conclusion, the burden of community-acquired pneumonia
requiring hospitalizationamong adults is substantial and is
markedlyhigher among the oldest adults. Although patho-gens were
not detected in the majority of pa-tients, respiratory viruses were
more frequentlydetected than bacteria, which probably reflectsthe
direct and indirect benefit of bacterial vac-cines and relatively
insensitive diagnostic tests.These data suggest that improving the
coverageand effectiveness of recommended influenzaand pneumococcal
vaccines and developing ef-fective vaccines and treatments for
HMPV, RSV,and parainfluenza virus infection could reducethe burden
of pneumonia among adults. Further
development of new rapid diagnostic tests thatcan accurately
identify and distinguish amongpotential pneumonia pathogens is
needed.45
The views expressed in this article are those of the authorsand
do not necessarily represent the views of the Centers forDisease
Control and Prevention (CDC).
Supported by the Influenza Division of the National Centerfor
Immunizations and Respiratory Diseases at the CDCthrough
cooperative agreements with each study site. The study was
based on a competitive research funding opportunity.
Dr. Self reports receiving fees for serving on an advisory
boardfrom BioFire Diagnostics, research supplies from
CareFusion,grant support through his institution from bioMérieux,
AffiniumPharmaceuticals, Astute Medical, Crucell Holland, Thermo
FisherScientific, Pfizer, Rapid Pathogen Screening, Venaxis, and
Cem-
pra, and holding a pending patent (13/632,874) related to a
sterileblood-culture collection system; Dr. Wunderink, receiving
con-sulting fees from Roche, the Medicines Company, Vical,
CubistPharmaceuticals, Bayer, Cerexa, and Visterra; Dr. Grijalva,
receiv-ing consulting fees from Pfizer; Dr. Anderson, receiving
grantsupport through his institution from MedImmune, editorial
sup-port for an unrelated study from Roche, and consulting fees
fromAbbVie; Dr. Courtney, receiving fees through his institution
fromThermo Fisher Scientific; Dr. Chappell, holding a patent
(U.S.8,293,498 B2) related to a system for generation of viable
reovirusfrom cloned complementary DNA and a pending
patent(13/639,564) related to reovirus vaccines and methods of
usetherefor; Dr. Arnold, receiving grant support from
GlaxoSmith-
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
12/13
n engl j med 373;5 nejm.org July 30,
2015426
T h e n e w e n g l a n d j o u r n a l o
f medicine
Kline; Dr. Ampofo, receiving fees through his institution
fromGlaxoSmithKline and Cubist Pharmaceuticals for the enrollmentof
patients in other studies, and collaborating with BioFire
Diag-nostics on grants funded by the National Institutes of Health;
Dr.Katz, receiving grant support through her institution f rom
JuvarisBioTherapeutics and GlaxoSmithKline; Dr. Pavia, receiving
feesfor serving on an advisory board from BioFire Diagnostics,
feesfor the preparation of educational material from Medscape,
androyalties from Antimicrobial Therapy; and Dr. Edwards,
serving
on a data and safety monitoring board for Novartis for which
herinstitution receives fees. No other potential conflict of
interestrelevant to this article was reported.
Disclosure forms provided by the authors are available withthe
full text of this article at NEJM.org.
We thank the patients who consented to participate in thisstudy;
Suzette Bartley, Bernie Beall, Nicole Burcher, Robert
Da- vidson, Michael Dillon, Barry Fields, Phalasy Juieng, and
ShelleyMagill of the CDC; Bharat Reddy Dhanireddy and Pinal Modi
of John H. Stroger, Jr., Hospital of Cook County; Alison
Chevrier,Ashraf Luqman, Cecilia Scholcoff, and Jill Sears of
Northwest-ern Memorial Hospital; Alexander Baldridge, Kelly Harris,
RajivMidha, and Denetra Smith of University of Tennessee
HealthScience Center–Saint Thomas Health; and Heather Diggs,
Regi-
na Ellis, Timothy Girard, Charity Graves, Angela
Harbeson,Deborah Hunter, Donna Jones, Romina Libster, Karen
Miller,Kelly Moser, Deborah Myers, Rabon Lee Smalling, Tanya
Stein-back, Scott Taylor, and Sandy Yoder of the Vanderbilt
UniversityMedical Center.
Appendix
The authors’ full names and academic degrees are as follows:
Seema Jain, M.D., Wesley H. Self, M.D., M.P.H., Richard G.
Wunderink,M.D., Sherene Fakhran, M.D., M.P.H., Robert Balk, M.D.,
Anna M. Bramley, M.P.H., Carrie Reed, Ph.D., Carlos G. Grijalva,
M.D.,M.P.H., Evan J. Anderson, M.D., D. Mark Courtney, M.D., James
D. Chappell, M.D., Ph.D., Chao Qi, Ph.D., Eric M. Hart, M.D.,
FrankCarroll, M.D., Christopher Trabue, M.D., Helen K. Donnelly,
R.N., B.S.N., Derek J. Williams, M.D., M.P.H., Yuwei Zhu, M.D.,
San-dra R. Arnold, M.D., Krow Ampofo, M.D., Grant W. Waterer, M.B.,
B.S., Ph.D., Min Levine, Ph.D., Stephen Lindstrom, Ph.D., Jonas
M.Winchell, Ph.D., Jacqueline M. Katz, Ph.D., Dean Erdman, Dr.P.H.,
Eileen Schneider, M.D., M.P.H., Lauri A. Hicks, D.O., Jonathan
A.McCullers, M.D., Andrew T. Pavia, M.D., Kathryn M. Edwards, M.D.,
and Lyn Finelli, Dr.P.H., for the CDC EPIC Study Team
The authors’ affiliations are as follows: the Centers for
Disease Control and Prevention, Atlanta (S.J., A.M.B., C.R., M.L.,
S.L., J.M.W., J.M.K., D.E., E.S., L.A.H., L.F.); Vanderbilt
University School of Medicine (W.H.S., C.G.G., J.D.C., F.C.,
D.J.W., Y.Z., K.M.E.) andUniversity of Tennessee Health Science
Center–Saint Thomas Health (C.T.), Nashville, and Le Bonheur
Children’s Hospital (S.R.A., J.A.M.), University of Tennessee
Health Science Center (S.R.A., J.A.M.), and St. Jude Children’s
Research Hospital (J.A.M.), Memphis— all in Tennessee; Northwestern
University Feinberg School of Medicine (R.G.W., E.J.A., D.M.C.,
C.Q., E.M.H., H.K.D., G.W.W.), John H. Stroger, Jr., Hospital
of Cook County (S.F.), and Rush University Medical Center (R.B.) —
all in Chicago; University of UtahHealth Sciences Center, Salt Lake
City (K.A., A.T.P.); and University of Western Australia, Perth
(G.W.W.).
References
1. Pfuntner A, Wier LM, Stocks C. Mostfrequent conditions
in U.S. hospitals,2011. HCUP statistical brief #162.
Rock- ville, MD: Agency for Healthcare Re-search and Quality,
2013 (http://www.hcup-us.ahrq.gov/reports/statbriefs/
sb162.pdf).2. Health, United States, 2012: with spe-cial
features on emergency care. Hyatts- ville, MD: National Center
for Health Sta-tistics, 2013:297-9.3. Pfuntner A, Wier LM,
Steiner C. Costsfor hospital stays in the United States,2011. HCUP
statistical brief #168. Rock- ville, MD: Agency for Healthcare
Re-search and Quality, 2013
(http://www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-United-States-2011.pdf).4.
Grijalva CG, Nuorti JP, Arbogast PG,Martin SW, Edwards KM, Griff in
MR. De-cline in pneumonia admissions after rou-tine childhood
immunisation with pneu-mococcal conjugate vaccine in the USA:
atime-series analysis. Lancet 2007;369:1179-86.5. Nelson JC,
Jackson M, Yu O, et al. Im-pact of the introduction of
pneumococcalconjugate vaccine on rates of communityacquired
pneumonia in children andadults. Vaccine 2008;26:4947-54.6.
Griff in MR, Zhu Y, Moore MR, Whit-ney CG, Grijalva CGUS. U.S.
hospitaliza-tions for pneumonia after a decade of
pneumococcal vaccination. N Engl J Med2013;369:155-63.7.
Lexau CA, Lynfield R, Danila R, et al.Changing epidemiology of
invasive pneu-mococcal disease among older adults inthe era of
pediatric pneumococcal conju-
gate vaccine. JAMA 2005;294:2043-51.8. Pilishvil i T,
Lexau C, Farley MM, et al.Sustained reductions in invasive
pneumo-coccal disease in the era of conjugate vac-cine. J Infect
Dis 2010;201:32-41.9. Marston BJ, Plouffe JF, File TM Jr,
etal. Incidence of community-acquiredpneumonia requiring
hospitalization: re-sults of a population-based active
surveil-lance study in Ohio. Arch Intern
Med1997;157:1709-18.10. Mandell LA, Wunderink RG, AnzuetoA,
et al. Infectious Diseases Society ofAmerica/American Thoracic
Society con-sensus guidelines on the management
ofcommunity-acquired pneumonia inadults. Clin Infect Dis
2007;44:Suppl 2:S27-S72.11. Pavia AT. Viral infect ions of
the lowerrespiratory tract: old viruses, new viruses,and the role
of diagnosis. Clin Infect Dis2011;52:Suppl
4:S284-S289.12. Caliendo AM. Multiplex PCR andemerging
technologies for the detectionof respiratory pathogens. Clin Infect
Dis2011;52:Suppl 4:S326-S330.13. Bartlet t JG. Diagnostic
tests foragents of community-acquired pneumo-
nia. Clin Infect Dis 2011;52:Suppl 4:S296-S304.14. Katz S,
Ford AB, Moskowitz RW, Jack-son BA, Jaffe MW. Studies in the aged:
theindex of ADL: a standardized measure ofbiological and
psychological function.
JAMA 1963;185:914-9.15. Cherian T, Mulholland EK,
Carlin JB,et al. Standardized interpretation of pae-diatric chest
radiographs for the diagno-sis of pneumonia in
epidemiologicalstudies. Bull World Health Organ
2005;83:353-9.16. Watt JP, Moïsi JC, Donaldson RLA, etal.
Measuring the incidence of adult com-munity-acquired pneumonia in a
NativeAmerican community. Epidemiol
Infect2010;138:1146-54.17. Bartlett RC. Medical
microbiology:quality, cost and clinical relevance. NewYork: John
Wiley, 1974:24-31.18. Pollock HM, Hawkins EL, Bonner
JR,Sparkman T, Bass JB Jr. Diagnosis of bac-terial pulmonary
infections with quanti-tative protected catheter cultures ob-tained
during bronchoscopy. J ClinMicrobiol 1983;17:255-9.19.
Thurman KA, Warner AK, Cowart KC,Benitez AJ, Winchell JM. Detect
ion of My-coplasma pneumoniae, Chlamydia pneu-moniae, and
Legionella spp. in clinicalspecimens using a single-tube
multiplexreal-time PCR assay. Diagn Microbiol In-fect Dis
2011;70:1-9.
The New England Journal of Medicine
Downloaded from nejm.org by carlos gonzalez on January 9, 2016.
For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights
reserved.
-
8/18/2019 Community-Acquired Pneumonia Requiring Hospitalization
Among U.S. Adults
13/13
n engl j med 373;5 nejm.org July 30, 2015
427
Pneumonia Requir ing Hospitalization among U.S. Adults
20. Murdoch DR. Diagnosis of Legionella infection.
Clin Infect Dis 2003;36:64-9.21. Carvalho MGS, Tondella ML,
Mc-Caustland K, et al. Evaluation and im-provement of real-time PCR
assays target-ing lytA, ply, and psaA genes for
detectionof pneumococcal DNA. J Clin
Microbiol2007;45:2460-6.22. Blaschke AJ, Heyrend C, Byington
CL,
et al. Molecular analysis improves patho-gen identification and
epidemiologicstudy of pediatric parapneumonic empy-ema. Pediatr
Infect Dis J 2011;30:289-94.23. Blaschke AJ, Heyrend C,
Byington CL,et al. Rapid identification of pathogensfrom positive
blood cultures by multiplexpolymerase chain reaction using the
Fil-mArray system. Diagn Microbiol InfectDis
2012;74:349-55.24. Murdoch DR, Laing RTR, Mills GD, etal.
Evaluation of a rapid immunochro-matographic test for detection of
Strepto-coccus pneumoniae antigen in urine samplesfrom
adults with community-acquiredpneumonia. J Clin Microbiol
2001;39:
3495-8.25. Weinberg GA, Schnabel KC, ErdmanDD, et al. Field
evaluation of TaqMan Ar-ray Card (TAC) for the simultaneous
de-tection of multiple respiratory viruses inchildren with acute
respiratory infection. J Clin Virol
2013;57:254-60.26. Dare RK, Fry AM, Chittaganpitch
M,Sawanpanyalert P, Olsen SJ, Erdman DD.Human coronavirus
infections in ruralThailand: a comprehensive study usingreal-time
reverse-transcription poly-merase chain reaction assays. J Infect
Dis2007;196:1321-8.27. Sawatwong P, Chittaganpitch M, HallH,
et al. Serology as an adjunct to poly-merase chain reaction assays
for surveil-lance of acute respiratory virus infect ions.Clin
Infect Dis 2012;54:445-6.28. Feikin DR, Njenga MK, Bigogo G,
etal. Additional diagnostic yield of addingserology to PCR in
diagnosing viral acuterespiratory infections in Kenyan patients5
years of age and older. Clin Vaccine Im-munol
2013;20:113-4.29. Manual for the laboratory diagnosisand
virological surveillance of influenza.Geneva: World Health
Organization,2011:43-77
(http://www.who.int/influenza/gisrs_laboratory/manual_diagnosis_surveillance_influenza/en).
30. Monto AS, Maassab HF. Ether treat-ment of type B
influenza virus antigen forthe hemagglutination inhibition
test. J Clin Microbiol 1981;13:54-7.31. Kendal AP, Cate
TR. Increased sensi-tivity and reduced specificity of
hemag-glutination inhibition tests with ether-treated influenza
B/Singapore/222/79. J Clin Microbiol 1983;18:930-4.
32. Fiore AE, Bridges CB, Katz JM, CoxNJ. Inactivate inf
luenza vaccines. In: Plot-kin SA, Orenstein WA, Off it PA, eds.
Vac-cines. 6th ed. Philadelphia: Elsevier,
2012:257-93.33. Vintage 2012 postcensal estimates ofthe
resident population of the UnitedStates by year, county,
single-year of age,bridged race, Hispanic origin, and sex.
Atlanta: National Center for Health Sta-tistics, 2012
(http://www.cdc.gov/nchs/nvss/bridged_race.htm).34. Fine MJ,
Auble TE, Yealy DM, et al. Aprediction rule to identify low-risk
pa-tients with community-acquired pneumo-nia. N Engl J Med
1997;336:243-50.35. Karhu J, Ala-Kokko TI, Vuorinen T,Ohtonen
P, Syrjälä H. Lower respiratorytract virus findings in mechanical
ly venti-lated patients with severe community-acquired pneumonia.
Clin Infect Dis2014;59:62-70.36. Lanspa MJ, Peyrani P,
Wiemken T,Wilson EL, Ramirez JA, Dean NC. Charac-teristics
associated with clinician diagno-
sis of aspiration pneumonia: a descriptivestudy of afflicted
patients and their out-comes. J Hosp Med 2015;10:90-6.37.
Jennings LC, Anderson TP, BeynonKA, et al. Incidence and
characteristics of viral community-acquired pneumonia
inadults. Thorax 2008;63:42-8.38. Johansson N, Kalin M,
Tiveljung-Lin-dell A, Giske CG, Hedlund J. Etiology
ofcommunity-acquired pneumonia: in-creased microbiological yield
with newdiagnostic methods. Clin Infect Dis 2010;50:202-9.39.
Johnstone J, Majumdar SR, Fox JD,Marrie TJ. Viral infection in
adults hospi-talized with community-acquired pneu-monia:
prevalence, pathogens, and pre-sentation. Chest
2008;134:1141-8.40. Lieberman D, Shimoni A, Shemer-Avni Y,
Keren-Naos A, Shtainberg R, Li-eberman D. Respiratory viruses in
adults with community-acquired pneumonia.Chest
2010;138:811-6.41. Templeton KE, Scheltinga SA, van denEeden
WC, Graffelman AW, van denBroek PJ, Claas EC. Improved diagnosis
ofthe etiology of community-acquiredpneumonia with real-time
polymerasechain reaction. Clin Infect Dis
2005;41:345-51.42. Charles PGP, Whitby M, Fuller AJ, et
al. The etiology of community-acquiredpneumonia in Australia:
why penicillinplus doxycycline or a macrolide is themost
appropriate therapy. Clin Infect Dis2008;46:1513-21.43. Musher
DM, Thorner AR. Communi-ty-acquired pneumonia. N Engl J
Med2014;371:1619-28.44. Jain S, Williams DJ, Arnold SR, et
al.
Community-acquired pneumonia requir-ing hospitalization among
U.S. children.N Engl J Med 2015;372:835-45.45. Caliendo AM,
Gilbert DN, GinocchioCC, et al. Better tests, better care:
im-proved diagnostics for infectious diseas-es. Clin Infect Dis
2013;57:Suppl 3:S139-S170.46. Fry AM, Lu X, Olsen SJ, et al.
Human
rhinovirus infections in rural Thailand:epidemiological evidence
for rhinovirusas both pathogen and bystander. PLoSOne
2011;6(3):e17780.47. Ruuskanen O, Järvinen A. What is thereal
role of respiratory viruses in severecommunity-acquired pneumonia?
ClinInfect Dis 2014;59:71-3.48. FluView: a weekly influenza
surveil-lance report prepared by the InfluenzaDivision. Atlanta:
Centers for DiseaseControl and Prevention
(http://www.cdc.gov/flu/ weekly).49. Prevention and
control of seasonalinfluenza with vaccines: recommenda-tions of the
Advisory Committee on Im-
munization Practices (ACIP) — UnitedStates, 2014–2015. MMWR Morb
MortalWkly Rep 2014;63:691-7.50. Falsey AR, Hennessey PA,
FormicaMA, Cox C, Walsh EE. Respiratory syncy-tial virus infection
in elderly and high-risk adults. N Engl J Med
2005;352:1749-59.51. Walsh EE, Peterson DR, Falsey AR.Human
metapneumovirus infections inadults: another piece of the puzzle.
ArchIntern Med 2008;168:2489-96.52. Werno AM, Murdoch DR.
Medical mi-crobiology: laboratory diagnosis of inva-sive
pneumococcal disease. Clin InfectDis 2008;46:926-32.53. Use of
13-valent pneumococcal conju-gate vaccine and 23-valent
pneumococcalpolysaccharide vaccine among adultsaged ≥65 years:
recommendations of theAdvisory Committee on ImmunizationPractices
(ACIP). MMWR Morb MortalWkly Rep 2014;63:822-5.54. Kumar S,
Hammerschlag MR. Acuterespiratory infection due to Chlamydia
pneum oniae : current status of diagnosticmethods.
Clin Infect Dis 2007;44:568-76.55. Nilsson AC, Björkman P,
Persson K.Polymerase chain reaction is superior toserology for the
diagnosis of acute Myco-
plasma pneumoniae infection and reveals ahigh
rate of persistent infect ion. BMC Mi-crobiol
2008;8:93.56. Nir-Paz R, Michael-Gayego A, Ron M,Block C.
Evaluation of eight commercialtests for Mycoplasma
pneumoniae antibod-ies in the absence of acute
infection. ClinMicrobiol Infect 2006;12:685-8.
Copyright © 2015 Massachusetts Medical Society.
The New England Journal of Medicine