-
8/2/2019 Community-Based Distribution the Distributive Potential
And
1/15
Community-Based Distribution: The Distributive Potential and
Economics of a SocialMarketing Approach to Family
PlanningAuthor(s): T. R. L. BlackReviewed work(s):Source:
Proceedings of the Royal Society of London. Series B, Biological
Sciences, Vol. 195, No.1118, A Discussion on Contraceptives of the
Future (Dec. 10, 1976), pp. 199-212Published by: The Royal
SocietyStable URL: http://www.jstor.org/stable/77170 .
Accessed: 19/03/2012 05:06
Your use of the JSTOR archive indicates your acceptance of the
Terms & Conditions of Use, available at
.http://www.jstor.org/page/info/about/policies/terms.jsp
JSTOR is a not-for-profit service that helps scholars,
researchers, and students discover, use, and build upon a wide
range of
content in a trusted digital archive. We use information
technology and tools to increase productivity and facilitate new
forms
of scholarship. For more information about JSTOR, please contact
[email protected].
The Royal Society is collaborating with JSTOR to digitize,
preserve and extend access to Proceedings of the
Royal Society of London. Series B, Biological Sciences.
http://www.jstor.org
http://www.jstor.org/action/showPublisher?publisherCode=rslhttp://www.jstor.org/stable/77170?origin=JSTOR-pdfhttp://www.jstor.org/page/info/about/policies/terms.jsphttp://www.jstor.org/page/info/about/policies/terms.jsphttp://www.jstor.org/stable/77170?origin=JSTOR-pdfhttp://www.jstor.org/action/showPublisher?publisherCode=rsl
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
2/15
Proc. R. Soc. Lond. B. 195, 199-212 (1976)Printed in Great
Britain
Community-baseddistribution:the
distributivepotentialandeconomics of a social marketing approachto
family planning
BY T. R. L. BLACKPopulation Services International, London
Because of the shortage of medical manpower in the developing
worldfuture family planning programmes will increasingly be
supplementedby the use of non-clinical resources through what is
known as community-based distribution (c.b.d.) programmes.
Currently the c.b.d. resourcesbeing mobilized range from church
groups to the commercial marketingindustry. The use of marketing
techniques in this way to distribute con-traceptives at subsidized
prices is an example of social marketing. Thisapproach has the
advantage of being able to use the world's ubiquitousshop system
and of being highly cost-effective. Fragmentary data suggeststhat
in most countries there is one store for every 25 to 120 fertile
couples.Evidence on the number and distribution of stores in
various countries isdiscussed. Cost-effectiveness figures for the
Preethi and Nirodh condomc.b.d. programmes are presented. These
show that in 1973 the Nirodhprogramme was providing a couple-year
of protection for $1.78. Com-parable evidence on cost performance
figures for clinic programmessuggests that c.b.d. marketing
programmes are substantially more cost-effective in purely
quantitative terms. Finally, the most importantfuture development
in this field is the recognition that an appropriatemanagerial
environment for c.b.d. programmes would have a greaterdemographic
impact than any foreseeable development in
contraceptivetechnology.
INTRODUCTIONWhatever the nature of future contraceptives they
will have to be distributed tothe fertile. Traditionally this has
meant the use of doctors and clinics. But world-wide, according to
W.H.O. statistics, there are no more than 2.5 million doctors(Doan
1974). Of these less than 500000 come from the developing areas of
LatinAmerica, Africa and Asia. And probably not more than 50-60 000
work as primaryhealth physicians in the rural areas of these
continents. Because of this acuteshortage future family planning
programmes will continue the present trend andevolve along three
lines. Activities requiring physician skills will be
channelledthrough services which naturally bring the at-risk
fertile patients in contact withdoctors such as in post-partum and
maternal and child health clinics. Secondly,a widening range of
family planning functions will be delegated to paramedical
andauxilliary personnel. While clinical activities will
increasingly be supplemented bythe use of non-medical resources to
promote and deliver contraceptives, a processwhich has been given
the generic term community-based distribution (c.b.d.).
[ 199 ]
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
3/15
T. R. L. Black (Discussion Meeting)At the present time there are
c.b.d. programmes or pilot projects of one kind oranother under way
in 34 countries (People 1975; Huber et al. I975). The catalogueof
resources being mobilized range through religious institutions such
as with theChurch of Christ programme in the Philippines, women's
organizations as in Nepal,teachers in Thailand, the postal services
in Sri Lanka and Kenya, and as in the
pioneering Nirodh condom programme in India, the commercial
marketingindustry. Some of these programmes are relying principally
on volunteers todistribute contraceptives free, such as with the
Benfam programme in northernBrazil. Others sell contraceptives at
near commercial prices, as the JapaneseFamily Planning Association
is doing with its door-to-door saleswomen, or athighly subsidized
prices either through groups such as the welfare workers of
HongKong or through the normal retailing system of shops as, for
example, in India,Sri Lanka, Jamaica, Indonesia, Fiji, Kenya and
Bangladesh.Critics of the use of volunteers argue that it is a
retrograde step in the face of apopulation crisis; that it is not
capable of massive expansion and that the highturnover of
volunteers makes for inefficiencies and intermittency of supply
whichnaturally is undesirable with contraceptives. Critics of the
sale of contraceptivesmaintain that it is commercializing family
planning and that however low theselling price this will
effectively deny contraceptives to the extremely poor.
Suchcriticisms are only partially valid. Apparently volunteers can
be mobilized effec-tively in some political environments such as
China (Chen 1975). The sale of contra-ceptives can be totally
subsidized where necessary by the use of coupon systems,an approach
which is currently being tried with some success in Costa Rica
(IsaacsI975)-Advocates of community-based distribution maintain
that the implications forfamily planning go beyond non-clinical
distribution. They see it as an importantstep to involving the
grass-roots community actually in the process of program-ming. In
this way family planning can be promoted on a continuing basis
fromwithin the society. This is in direct contrast to the
prevailing situation in whichbirth control, a preventive community
service, is being delivered from urbanbased clinic systems in the
manner and style of curative medicine.
My experience over the last 5 years has been almost exclusively
with c.b.d.programmes which use commercial resources. Therefore in
this paper I propose tolook at the distributive potential and
economics of a social marketing approach tofamily planning and
speculate briefly on the future.
CONTRACEPTIVE SOCIAL MARKETINGThe commercially purchased
contraceptives were available long before theadvent of family
planning clinics (Peel I963; Levin 1968). In most countries
more
people still buy their contraceptives from shops than obtain
them from organizedfamily planning services (Sollins & Belsky
1970; A. D. Little 1972). It was thisobservation that led the
Indian Institute of Management in 1963 to the concept
200
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
4/15
Social marketingapproachtofamily planningof distributing
contraceptives through commercial channels at subsidized
prices(Indian Inst. Management I963). The result of this work was
the launch of thepioneering Indian Nirodh condom programme in 1968
(for details see FrandaI972).The Nirodh programme is an example of
what is now known as social marketing,or the use of marketing
techniques and resources to further social as distinct
fromcommercial objectives (Kotler & Zaltman I97I). This
approach to social changeis being used not only in family planning
but also in agriculture, nutrition (Wick-strom I974), health care
(Zaltman & Vertinsky I97I) and education. For thoseunfamiliar
with the social marketing model as applied to family planning it is
aprogramme organized along the lines of a consumer sales
organization (Roberto1972). This consists of a small management
cadre which acts as a flexible, coord-inating nerve centre
controlling programme activities through contracting, inter-acting
and cooperating institutions usually from the private sector. In
this waythe programming functions of research, promotion and
distribution are undertakenby specialist agencies hired for the
purpose, thus avoiding the necessity ofinstitution building.The key
to successful social marketing of family planning is the use of
consumerproduct distributors who can channel contraceptives
nationally at very little costfrom urban wholesalers to village
shops. Since a product increases in price by nomore than 50-60 % as
it passes through this distributive pipeline it is possible
byselling distributors contraceptives at subsidized prices to make
them available onshop counters at nominal prices. For example, the
Nirodh Programme which usesthe services of manufacturer
distribution organizations such as Brooke Bond,India Tobacco,
Lipton Tea Ltd, Hindustan Lever, is able to sell condoms in packsof
3 to the fertile for 3 U.S. cents or just over one penny. Similarly
condoms arebeing sold 3 to a pack for 4 cents in Sri Lanka, 7 cents
in Kenya and 10 cents inGhana, while in Bangladesh both condoms and
pills are now on sale for 2.8 centsand 5 cents respectively.
Apart from mobilizing the technical and physical assets of the
established anddemonstrably effective marketing industry for family
planning purposes there aretwo advantages claimed for the social
marketing of contraceptives. The distribu-tion of contraceptives
through consumer goods channels can overcome the weakestaspect of
current family planning programmes: the limited number of
serviceoutlets. Secondly, the use of contracted services in this
way is cost effective.
THE DISTRIBUTIVE POTENTIALEvery developing country has an
extensive network of shops, through whichcondoms and pills can be
distributed. The limited data available suggests that inmost
countries there is probably one store of some kind for every 25 to
120 fertilecouples. In addition there are usually hawkers, fairs
and a highly developed systemof daily and periodic markets, such as
the Mammi markets of West Africa. Curi-
201
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
5/15
202 T. R. L. Black (Discussion Meeting)ously enough, unlike the
retail shop system, fairs and periodic markets have beenthe subject
of exhaustive study world-wide, primarily by anthropologists
andgeographers (for bibliography see Bromley I974). The extent of
national retailingsystems is difficult to verify. Stores are
usually unlicensed or only licensed locallyso that statistics are
mostly unobtainable. But fragmentary data are available. An
TABLE 1. THE URBAN-RURALDISTRIBUTIONOF GENERALRETAILSHOPSIN
KENYA 1972
area number people per shopNairobi 2131 235Mombasa 1231
203Nakuru 257 195Kisumu 201 164rest of Kenya 20165 529total 24585
508
Source: Min. Finance & Planning Nairobi 1973; Corcoran&
Tyrrel 1974.TABLE 2. CENSUS OF RETAILOUTLETS N CEYLON 1972
(Courtesy the Sri Lanka Institute of Marketing.)number
ofoutlets
government co-operative wholesalers 13government co-operative
retail branches 89all-Ceylon Consumer Co-op Union (milk
distribution) 1primary Co-op Societies (wholesalers) 370Co-op
retail branches 5716marketing department shops 55restaurants,
cafes, eating houses 12193general retailers, large 4725general
retailers, small 37275general wholesalers 450semi-wholesalers
350chemists (pharmacies) 290drapers (textile shops) 2503bakeries
2020bars, cinemas, clubs 783hawkers, mobile vendors 8444
total 75277Egyptian study by Boyd et al. (196I) found that in
1960 there was a general storefor every 25 fertile couples. In
Thailand a store census indicates that in 1966 therewas a sales
outlet to every 46 fertile couples (Anderson 1970). Kenya, a
countryin which stores are licensed annually, is the source of the
data shown in table 1,illustrating the relative urban-rural
distribution of shops (Corcoran & TyrrellI974). In Jamaica
commercial brewers claim to sell to 15000 outlets, or one forevery
140 people (Westinghouse I973a). Shop census figures from Sri
Lankaindicate one general store for every 348 people and provide a
detailed picture of
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
6/15
Social marketingapproachtofamily planning 203the typical
spectrum of outlet in a developing country (see table 2). In
practicalterms it is evident that unlike clinics the shop is the
outlet of a system that clearlydoes have intimate contact with the
fertile.
A retailer may be defined as someone selling to the general
public from a shopestablished within a permanent structure. This
excludes market stalls, panwallahs,kiosks and hawkers. Obviously
with so many shops available the retailer plays amajor role in
people's lives. A survey of 856 rural respondents in Kenya
showedthat nearly three-quarters had visited a shop within the
previous 48 h (P.S.I.I97zb).The developing country retailer is very
different from your local storekeeper.He or she is usually
semi-literate and keeps few records and carries a small amountof
stock of surprisingly wide range. The typical East African 'duka',
for example,stocks staple items such as maize, sugar, rice, spices,
tea, salt and bread. It alsodeals in cigarettes, matches, kerosene,
soap, baby food, cheap confectionery,cooking fat or oil, soft
drinks, assorted cheap tinned foods and nowadays soappowders. A
high proportion also sell patent medicines. A survey of 60 stores
inrural Kenya showed that 72 % carried analgesics, 90 %
anti-malarials, 42 % anti-worm preparations, 48 % laxatives, 70 %
cough medicines and incidentally 68 %also sold sanitary napkins
(P.S.I. 1972a). Personal observation reveals that inWest Africa and
Asia many shops openly sell abortifacients and occasionally
thepill. With this range of stock the addition of contraceptives to
the store shelfshould present no problems.The sales turnover for
developing country shops is very low. A survey by Harper(I972) of
130 rural shops in Kenya showed that 70 % had total sales of no
morethan ?1000 per year, of which about ?120 was profit. In
Thailand, according toAnderson (I97o), the average turnover of
urban retailers in 1966 was only ?3700,while that for rural
retailers was less than ?700. There are no reasons to suspectthat
such figures are atypical. With such sales levels we cannot expect
individualretailers to sell large numbers of contraceptives. The
prospect is of a large numberof retailers each selling a small
number of contraceptives.But to what extent are shopkeepers willing
to participate in family planning?A survey by Westinghouse of a
sample of retailers in eight developing countriessuggests
shopkeepers are probably better informed about family planning,
andpossibly more liberal than the general public as a whole, and
that more would bewilling to stock contraceptives than not
(Westinghouse 1973b). Surveys of retailersin Kenya and Sri Lanka
support these findings (see table 3) (P.S.I. 1972a, I974).They also
revealed that retailers willing to stock and display contraceptives
do soprimarily for materialistic reasons.
In practice the recruiting of retailers as contraceptive
salesmen has not provedto be a problem whether it be in rural
Kenya, Sri Lanka, Bangladesh, India orJamaica. In the Kinga condom
social marketing experiment in a large rural areaof Kenya just
under 400 village retailers or one-third of all outlets in the
districtwere stocking the product within two months of its launch
(Black & Harvey 1976).
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
7/15
204 T. R. L. Black (Discussion Meeting)The main deciding factors
of whether to stock Kinga or not was the availabilityof cash when a
salesman called (a major problem), and reassurance that the
productwould be well promoted. Few shopkeepers refused to stock the
product because itwas a contraceptive. In Sri Lanka within one
month of the launch of the Preethinational condom programme the
distributors, Reckitt & Colman Ltd, had thisproduct on the
shelves of 3177 outlets (P.S.I. I974). Whatever family
plannersmight like to think, most shopkeepers seem to regard
contraceptives as just anotherproduct line and accordingly they ask
the usual questions - how much do I make?,does it sell?, and will
you advertise it? Their doubts appear to be predominantlycommercial
rather than moral or religious.
TABLE 3. ATTITUDES OF A SAMPLE OF 30 PHARMACISTSAND 200
RETAILERS INSRI LANKA AND 60 RURAL RETAILERSIN KENYA TO FAMILY
PLANNING IN 1972AND 1973 SriLanka 1973 ruralKenya...-. ..
1972pharmacist retailer retailer% % %awarenessof familyplanning 100
99 90awareof pills 95 69 63awareof condoms 97 61 67no.
stockingcondoms 93 3 5willingto displaycondoms 77 57 93approveof
condomadvertising 93 75 93
Source:P.S.I. preprogrammemarketresearchKenya and SriLanka.In
our experience stockists are eager to learn about the
contraceptives they sellso that they can advise their customers,
just as they do very ably with, say, anti-malarials. But getting
the shopkeeper to become a promoter of contraceptives ismore
difficult. A survey of Nirodh stockists showed that only 21 %
claimed to
actively sell the product (Mohammed I969). The principal reasons
cited for notdoing so were shyness and fear of offending customers.
In the Kenya experimentthe shopkeepers were entirely passive
salesmen unless questioned by customers,but this is how they sell
all products. Sales experience in Kenya and Sri Lankahas shown that
if stockists are educated about contraceptives, the products areon
display, and they are strongly supported by point-of-purchase
promotionalmaterials, then customers are stimulated to ask
questions as well as purchase.The other significant finding from
the Kenyan project was confirmation thatthe pattern of
contraceptive sales follows the general rule of thumb in
marketingthat approximately one-third of outlets achieves
two-thirds of all sales in a givenarea. These high sales shops
tended to be bigger, better stocked and owned byyounger, more
outgoing people. This suggests that programmes should adopt
aselective distribution strategy, at least initially, an approach
that was used togood effect by the Preethi programme in Sri
Lanka.
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
8/15
Social marketingapproachtofamily planningProvided commercial
considerations are appreciated, experience indicates thatthere are
no practical barriers to making condoms and pills readily available
con-sumer goods through the ubiquitous shop system described, or to
prevent therecruitment of shopkeepers as grass-roots advocates and
educators for family
planning. Instead, the problems lie with the medical profession,
family planningadministrators and the funding sources.THE ECONOMICS
OF SOCIAL MARKETING
Performance budgeting studies in family planning are highly
political, heavilyreliant on secondary data, and measure output on
the basis of a variety of non-standard assumptions in terms of
acceptors, couple-year of protection, or birthsaverted. Therefore,
such studies are hardly routine. Yet with official funds world-wide
for family planning, seemingly plateaued at about $500 million and
no longerkeeping pace with the eroding effects of inflation and
population growth, pro-gramme economics are more important than
ever.
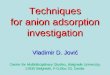
15.6% 20.4%
FIGURE 1. The allocation of funds from all sources for the
Korean family planning programmefor the years 1964 to 1968.
(Source: Penstate study I969.)Theoretically social marketing
programmes should be highly cost effective. Theuse of contractors
whose overheads are spread over a range of commercial
activities
means that funds are spent primarily on contraceptives and
promotion, rather thanon supporting an institutional establishment
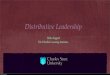
as is the case with clinic programmes.The resulting difference in
the deployment of funds is well illustrated by twoprogramme budgets
for which detailed data are available; the 1968 Korean
clinicprogramme (figure 1), and the 1969 Nirodh social marketing
programme (figure 2).
205
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
9/15
T. R. L. Black (Discussion Meeting)On the other hand, social
marketing programmes to date have been confined todistributing only
a male related, not very effective or popular means of
contra-ception, the condom (or in the case of Ghana, condom and
foam), which hasnaturally meant high distribution and promotional
costs for any given measureof outnut.
Advertisingand Promotion45%
Contraceptive Supplies 45% \
FIGURE 2. The allocation of the 1969 Nirodh programme budget.
(Source: Government ofIndia Paper 1969.)One programme for which
detailed cost and performance data is available is theSri Lanka
Preethi (the brand name means 'happiness') condom social
marketing
programme. This was funded by the International Planned
Parenthood Federationand managed by Population Services
International, a specialist non-profit familyplanning organization.
Following a 6 months start-up period involving marketresearch and
the creation of a promotional campaign, the programme was
launchedin October 1973. Preethi was distributed nationally by
Reckitt & Colman CeylonLtd and supported by a heavy advertising
campaign created and managed by alocal agency. The lubricated
condoms were sold in packets of three for 40 localcents or about 2
pence and promoted through a multi-media campaign involvingpress,
cinema, radio and heavy point-of-sale promotion. In the first 9
months ofthe programme 2.9 million condoms were distributed, of
which 96% were soldthrough shops, 2% sold by mail-order and 2%
given away as samples. After a full18 months of marketing 5875000
condoms had been sold, and it is for this launchperiod that
detailed budget figures are available.For the 2-year programme
including the initial 6 months start-up the totalinput or local
programming expenditure (excluding commodities) was $390500,of
which approximately 19% can be attributed to start-up costs and 35%
to
206
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
10/15
Social marketingapproachtofamily planningPreethi promotion.
During this period the income to the programme from Preethisales
was $23 000 which means the net subsidy required was $367 500 for 2
years.Thus on sales of 5875000 items the subsidy required was 6.25
U.S. cents or justover 3.4 pence per condom sold. However, this
excludes the actual cost of thecondom which was 2.2 cents or 1
penny an item, making a total cost of 8.45 centsof 4.2 pence per
protected act of intercourse. Adopting the assumption used bythe
one major cost-benefit study (Penstate 1969), that 100 condoms
distributedis equivalent to one couple-year of protection (c.y.p.),
suggests that 58750 c.y.p.were provided during the first 18 months
of marketing, assuming only nominallevels of wastage. This means
that the Preethi programme was delivering onec.y.p. for a subsidy
cost of $8.45 or about ?4.20*, figures which are summarizedalong
with the budget in table 4.TABLE 4. A SUMMARY OF THE COST AND
PERFORMANCE OF THE PREETHI CONDOM
MARKETING PROGRAMME FOR THE PERIOD MARCH 1972 TO MARCH 1974sales
subsidy per subsidyOct. 1973 to condom perlocal budget March 1975
U.S. cents c.y.p.
start-up costs $75000promotion $138000 5875000 2.35 $2.35other
$177500$390500sales income $23 000net cost $367500 5875000 6.25
$6.25cost of condoms $129500total cost $497000 5875000 8.46
$8.46
Source: P.S.I.In interpreting these input-output figures it must
be remembered that thePreethi programme was new. It was a major
innovation for family planning in SriLanka. In other words these
are the costs of launching a new programme which
are naturally higher than those for an established one, since
with time costs wouldfall substantially as more new customers are
recruited and old ones repurchase.In addition, the initial start-up
costs would normally be written off over a 5-yearperiod.
Furthermore, it was planned to launch an oral contraceptive in 1976
withthe brand name Mithuri (which means 'friend'). The introduction
of a pill com-ponent to such a programme would substantially
increase the number of couple-years of protection (13 cycles = 1
c.y.p.), without significant increases in non-product related
costs.Some indication of the impact of pill sales on
cost-effectiveness can be deduced.Mithuri was successfully test
marketed in the spring of 1975 (Davies & Louis I975).On the
basis of this test, 1976 sales projections were conservatively
forecast at350000 cycles. Anticipated condom sales were
pessimistically projected at4250000 or 0.3 per capita (0.27 in
1974). Assuming the programme was to achieve* $2.015 = ?1.
207
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
11/15
T. R. L. Black (Discussion Meeting)these sales targets then it
would be providing 26 900 pill and 42 500 condom couple-years of
protection, or a total of 69400 c.y.p. in all. The budget required
for the1976 programme was $305000 inclusive of contraceptive
supplies. Thus if theprogramme were to achieve the sales forecast
it would be providing a c.y.p. for$4.39 or ?2.18. On the other hand
the anticipated cost for a c.y.p. for a condom-only programme at
this level of condom sales and a budget of $227000 wouldbe $5.34 or
?2.65.The Indian Nirodh programme provides a second example of
contraceptivesocial marketing economics. In 1969, the second year
of the programme, 29.51million Nirodh condoms were sold (or 0.03
per capita) at a cost of $950000, ofwhich 45 % was for commodities
and 45 % promotion (but excluding start-upcosts). This means that
in its second year the programme was providing a c.y.p.for $3.23 or
?1.60. In 1973 the programme sold 116 million condoms (or 0.21
percapita) for a total cost of $2070000, of which 84 % was for the
condoms sold.Therefore, in 1973 the Nirodh programme was providing
a c.y.p. for $1.78 or?0.88, a reduction of 45 % in costs within 5
years. Some of the differences betweenthe costs of the Nirodh and
Preethi programmes can be attributed to the effectsof a larger
market, the forces of inflation, a lower level of promotional
expenditure,and cheaper condoms. For example, the 1969-70 Nirodh
promotional budget was0.07 U.S. cents per capita as compared to the
1974 Preethi promotion expenditureof about 1 cent. The unlubricated
Nirodh condom cost 1.5 cents each as comparedto 2.2 cents for the
lubricated Preethi product.
Attempts to compare these cost performance figures with those of
clinic pro-grammes are fraught with difficulty. Obviously it is
simpler to measure the inputsand outputs of a social marketing
programme than it is for a clinical one. Thebudget is well defined
and output is measured in terms of the sale of only one ortwo
products, whereas clinic programmes have a multitude of hidden
inputs suchas the uncosted use of buildings, supporting
administrative services and capitalinvestment which spill over from
health budgets. There is also the 'joint-cost'problem such as when
health nurses provide family planning services. These andother
difficulties associated with performance budgeting studies of
clinic familyplanning programmes have been thoroughly reviewed
elsewhere (Economic Com-mission I969). Cost comparisons are further
complicated by the fact that the mostcommonly used measure of
output in clinic cost-benefit studies has been acceptors- a rather
ill defined and unreliable measure generated from service
statisticswhich cannot be satisfactorily derived from contraceptive
sales figures. Suchstudies have reported clinic programme costs
ranging from $3.61 to $39 peracceptor (Lapham & Mauldin I972;
Slavin & Bilsbarrow I974).
One major study, however, has measured clinic programme output
in terms ofcouple-years of protection. In 1969 Pennsylvania State
University compared thecost inputs including foreign aid of six
national programmes and measured outputin terms of couple-years of
protection on the basis of contraceptives distributed
orsterilizations performed, using assumptions such as 100 condoms
or 13 pill cycles
208
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
12/15
Social marketingapproachtofamily planningdistributed equals one
c.y.p. On this basis the cost of a couple-year of protectionin the
countries studied ranged from $2.21 to $20 (Penstate 1969). By
applyingthe same assumptions to three of the countries studied for
which recent budget,contraceptive distribution and sterilization
figures are available (Watson &Lapham1974; Nortman 1975), we
can derive some indication of present costs of providinga c.y.p.
through clinic services. The result of this exercise is shown in
table 5,which is based on a constant 1968 rate of exchange for
local currency budgets.TABLE 5. THE COST OF PROVIDING A COUPLE-YEAR
OF PROTECTION FOR THREENATIONALCLINICPROGRAMMESN 1968 AND 1974 AT A
CONSTANT 1968 RATE OFEXCHANGE country 1968 1974
India $3.10 $9.45Korea $2.48 $8.06Taiwan $2.21 $2.80Source:
derived from Penstate (I969), Watson & Lapham (I974), Nortman
(1975).100 condom or 13 pill cycles = 1 c.y.p. I i.u.d. = 2.5
c.y.p. Sterilization = 7.5 c.y.p.
On the basis of these figures, the apparent cost is between
$8.00 to $9.45 to providea c.y.p. through the Korean and Indian
clinic programmes in 1974. Obviouslythese figures, which unlike the
earlier Penstate study are based solely on localgovernment
statistics, must be interpreted with caution. But they do suggest
thatinitially social marketing programmes may be no more
cost-effective than theclinic programmes they are designed to
supplement. However, as markets developand other contraceptives are
introduced it would seem that this type of programmewill be
substantially more cost-effective, at least in purely quantitative
terms. Ifnothing else such comparison indicates an urgent need for
an entirely independentlook at this whole cost-effectiveness
question, preferably by an international firmof auditors.
FtUTURE DEVELOPMENTSThe future of contraceptive social marketing
will depend entirely on the extentof high level appreciation of the
concepts involved and commitment to thisapproach. Fostering
supportive attitudes alone will be a major public relationstask.
And it will have to be appreciated that the very language, style
and tempoof marketing must be adjusted to cater for the biases of
politicians and adminis-trators who currently perceive family
planning in clinical terms. But there are twokey developments which
would have a major impact on cost and demographiceffectiveness of
these programmes.The first is the advent of a physician-free post
facto or hindsight contraceptivesuch as the 'week-after' pill. Any
product which can put the clock back andcorrect a mistake will be
an instant success.The second fundamental development is the
question of appropriate manage-ment. Of all family planning
variables the one which has been virtually ignored
209
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
13/15
210 T. R. L. Black (Discussion Meeting)by researchers is the
issue of management and performance. Yet management is aparameter
which is adjustable and which must have enormous influence on
pro-gramme output. Since no controlled studies exist the extent of
this influence indemographic terms remains unknown. However, on the
basis of informed judge-ment we can speculate.
Marketing is still an art, not a science. Empirical evidence
tells us that successfulsales operations require a particular set
of talents which operate best in a flexible,dynamic, consumer
orientated environment attuned to taking reasonable risks, asetting
not usually associated with family planning, which is, of course,
subject toprofessional, political, religious, cultural and social
contraints. But the questionremains to what extent would the
provision of such an environment for programmemanagers influence
sales performance. Some years ago Ford Foundation expertsexamined
the implications of changing the managerial setting for the
Nirodhprogramme (Ford Foundation I969). They maintained that the
optimal settingfor the Nirodh managers would be a specially created
independent corporation.
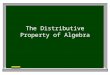
-2with proposed effort
600-
00 decision1" to change 5rangeofexectations
x 068-69 69-70 70-71 71-72 72-73 73-74 74-75
eeardFIGURE. Nih mketingme: sales experience and projecs.co 200-
[ ' ......xMinistryocorporat eetting would thpresead t efforto
68-69 69-70 70-71 71-72 72-73 73-74 74-75yearFIGURE.
Nirodhmarketingprogramme: alesexperienceandprojections.
In their considered opinion the effect of relocating the
management from a HealthMinistry to a corporate setting would have
had the effect on sales shown in figure3: that is an increase in
sales over the ensuing 5 years of between 300 and 600 %.In other
words, changing the managerial environment to one conducive to
free-range decision making would have had a far greater impact than
any other likelydevelopments.This observation on the role of a
non-bureaucratic managerial environment is
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
14/15
Social marketingapproachtofamily planning 211not to be construed
as an anti-government statement. It is merely a comment onsomething
that we in family planning are choosing to ignore. This, I submit,
isthat over the next decade the greatest gains in birth control are
likely to resultnot from developments in contraceptive technology
but the adoption of appro-priate and liberated management for
community-based distribution programmes.
REFERENCES (Black)Anderson, D. A. I970 Marketing and
development,theThai experience,pp. 158-159. MichiganState
University.Boyd, H. W. et al. I961 Channels of distribution for
consumer goods in Egypt. J. Marketing25, 26-33.Black, T. &
Harvey, P. 1976 A report on a rural contraceptive social marketing
experiment
in Kenya. Studies in Family Planning 7, no. 3.Bromley, R. J.
I974 Periodic Markets, Daily Markets and Fairs: a Bibliography,
Monashpublications in Geography, no. 6, Melbourne, Australia.Chen
Pi-Chao 1975 Lessons from the Chinese experience: China's planned
parenthoodprogram and its transferability. Studies in Family
Planning 6, no. 10.Corcoran & Tyrrell I974 A marketing man's
guide to Kenya, p. 41. Nairobi, Kenya.Doan, B. D. H. 1974 World
trends in medical manpower. World Health Statistical Report27, no.
2. Geneva: W.H.O.Davies, J. & Louis, T. D. J. 1975 Doctors and
community based pill promotion in Sri Lanka.I.P.P.F. Med. Bull. 9,
1-3.Economic Commission for Far East and Asia 1969 Reportof
theexpertgroup meeting on socio-economic returns of family planning
programmes. Asian Population Studies Series, no.12, Bangkok.Franda,
M. F. I972 Marketing condoms in India: the Nirodh Programme.
American Univer-sity Field Staff Reports 16, no. 8.Ford Foundation
I969 The Nirodh Marketing Programme: the case for a new
organizationalbase, New Delhi.Harper, M. I972 The discoveryand
satisfaction of theperceivedand actual needs of rural shop-keepers
in Kenya. Institute of Development Studies, Working Paper no. 16,
Nairobi,Kenya.Huber, S. C. et al. 1975 Contraceptive distribution
taking supplies to villages and households.Population
Reports,Series 3, no. 5.Institute of Marketing 1972 Census of
retail outlets in Ceylon. Colombo, Sri Lanka.Indian Institute of
Management I965 A proposal for family planning promotion: a
marketingplan. Studies in Family Planning 6, 7-12.Isaacs, S. 1975
Non-physican distribution of contraceptives in Latin America and
theCaribbean. Family Planning Perspectives 7, no. 4.Kotler, P.
& Zaltman, G. I971 Social marketing: an approach to planned
social change.J. Marketing 34, 3-72.Lapham, R. & Maudlin, P. W.
1972 National family planning programmes: review andevaluation.
Studies in Family Planning 3, 29-52.Levin, H. I968 Commercial
distribution of contraceptives in developing countries,
past,present and future. Demography 5, 941-946.Mohammed, P. S. 1969
The Nirodh Marketing Programme - a post-launch retailer
survey.Report, the Ford Foundation, New Delhi.Nortman, D. 1975
Population and family planning programmes: a factbook. Reports
onpopulation/Family Planning 2, 7.Peel, J. 1963 The manufacture and
retailing of contraceptives in England. Population Studies18,
113-125.Pennsylvania State University 1969 Cost-benefitand cost
effectiveness evaluation of familyplanning programs. Dept.
Economics, Phase II Report, University Park, Pennsylvania.
-
8/2/2019 Community-Based Distribution the Distributive Potential
And
15/15
212 T. R. L. Black (Discussion Meeting)People 1975 Distributing
contraceptives. People 2, no. 4.P.S.I., Population Services
International 1972a A survey into the attitudes of Duka ownersin
the Meru district to family planning and the marketing of condoms.
Report, Nairobi,
Kenya.Population Services International I972b A
pre-programmeknowledge, attitude and practicesurvey of 506
respondentsin the Meru and 350 in the Kirinyaga Districts, vol. 1.
ResearchBureau Ltd, Nairobi, Kenya.Population Services
International 1974 Preethi, a social marketing programme or
theadvance-ment of family planning. A report, Colombo, Sri
Lanka.Roberto, E. L. 1972 Social marketing strategies for diffusing
the adoption of family planning.Social Sci. Quarterly53,
33-51.Slavin, S. L. & Bilsbarrow, R. E. 1974 The Barbados
Family Planning Association andfertility decline in Barbados.
Studies in Family Planning 5, no. 10.U.N.F.P.A. 1974 Theroleof
international assistance in thepopulation fields. Report, New
York.Watson, W. B. & Lapham, R. J. (eds) 1974 Family planning
programmes, world review1974. Studies in Family Planning, 6,
205-324.Westinghouse Population Centre 1973 Distribution of
contraceptives n the commercialsector,see reports on Jamaica, Iran,
Panama, Thailand, Korea, Venezuela and Turkey.Columbia,
Maryland.Wickstrom, B. 1974 Thefunction of promotion in social
marketing. Paper presented F.A.O./S.I.D.A. Regional Workshop on
Food Promotion, Nairobi, East Africa, 22-27 April.Zaltman, G.
&Vertinsky, I. 1971 Health Services Marketing: a suggested
model. J. Marketing35, 19-27.