Embed Size (px)
DESCRIPTION
physiotherapy
Citation preview

7/02/2015
1
Community physiotherapy + working in teams
OPPORTUNITIES FOR PHYSIOTHERAPISTS
Loretta Andersen
http://www.forbes.com/sites/theyec/2012/12/12/can-working-in-teams-build-your-intelligence/
Explore………
• Thinking about where CDM is best delivered…
• Who are CDM team members….
• What role does physiotherapy have in CDM….
• What opportunities exist for physiotherapists
working in CDM teams ……
Example…Osteoarthritis chronic Care Program (OACCP)
Learning Outcomes
2. Justify the role of PT in the prevention +/or management of chronic illness or disease
3. Critically reflect on the contributions of an �interdisciplinary team
4. Research + determine a client-centred approach in the design of a physiotherapy management plan for the management of CD

7/02/2015
2
Explore………
Thinking about where CDM is best delivered…
QUIZ ACUTE HEALTH CARE CHRONIC HEALTH CARE
Specialist care
PATIENT & Carers
emotional
CVD
MSK
Chronic Care
Primary Care
Diabetes
Respiratory
cancer
functional
Adhere to treatment
Manage impact
Physical Activity Weight control
Monitor
Self management
Education

7/02/2015
3
Level 1
High complexity
Level 2
High Risk
Disease management
Level 3
Self-management
70-80%
Levels of
health care in
CD
Where can CDM be provided…
• GP surgeries
• Homes
• Workplaces
• Schools / Playgrounds
• Social + Sport clubs + Youth Centres
• Outpatient clinics
• Specialist program venues
• Hospitals
OPPORTUNITIES
CHALLENGE EXISTING PHILOSOPHIES of PRACTICE + DELIVERY

7/02/2015
4
Explore………
Who are CDM team members….
Individual with Chronic Disease
diabetes
Medical Nursing Dietician Occupat. Th
Physio Ex. Phys.
Psych Social W.
cardiac
CVD
arthritis
MSK respiratory cancer
cognitive/
emotional
Ms. “M” • 54 year old lady, advanced hip OA, smoker
• Married with 2 x children: Ages 8 and 14 (asperger’s)
• Husband. Works FT. Ms.� “M” reports little empathy
• Carer for in-laws both with dementia (live in own home + declining provided package of care)
• Works part time as cook in ACF
• Awaits left total hip replacement. Requires crutches x 2 to ambulate secondary to extreme pain
• Difficulties driving due to pain
• MHx: HT, tingling in both feet past 3/12 + 1 x recent fall, recent weight gain 5kg.
7/02/2015
5
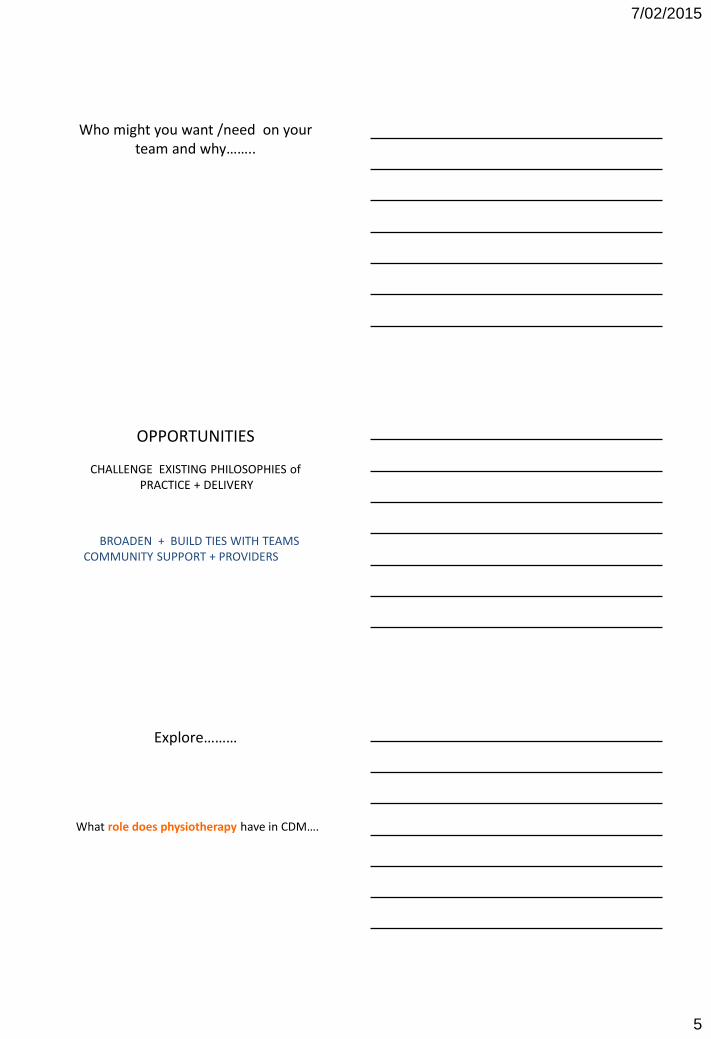
Who might you want /need on your
team and why……..
OPPORTUNITIES
CHALLENGE EXISTING PHILOSOPHIES of PRACTICE + DELIVERY
BROADEN + BUILD TIES WITH TEAMS COMMUNITY SUPPORT + PROVIDERS
Explore………
What role does physiotherapy have in CDM….

7/02/2015
6
Ms. “M” • 54 year old lady, advanced hip OA, smoker
• Married with 2 x children: Ages 8 and 14 (asperger’s)
• Husband. Works FT. Miss “M” reports little empathy
• Carer for in-laws both with dementia (live in own home + declining provided package of care)
• Works part time as cook in ACF
• Awaits left total hip replacement. Requires crutches x 2 to ambulate secondary to extreme pain
• Difficulties driving due to pain
• MHx: HT, tingling in both feet past 3/12 + 1 x recent fall, recent weight gain 5kg.
What questions need to be clarified�?
• Medical History, meds + CD Manage’t� plans
• Social situation + responsibilities
• Function + Mobility + exercise/ activity levels
• Support networks (services)
• Emotional wellbeing / support/ needs
• Priorities / goals
• Values/ beliefs/ barriers/ facilitators
Physiotherapy roles……
• broad based ‘needs’ assessment / screening
• treatment / advice (professional boundaries)
• Referral / interdisciplinary approaches
• Build personal capacity
• health-coaching (goal setting)
• harm-minimisation
• health promotion
• Assisted navigation service delivery systems

7/02/2015
7
Where can I get more information?
OPPORTUNITIES
CHALLENGE EXISTING PHILOSOPHIES of PRACTICE + DELIVERY
BROADEN + BUILD TIES WITH TEAM COMMUNITY SUPPORT + PROVIDERS
EXTEND TRADITIONAL ASSESSMENT + TREATMENT ROLES, SKILLS +
KNOWLEDGE
Explore………
• Where CDM is best deliverer ✓
• Who are CDM team members ✓
• What role does physiotherapy have in CDM ✓
• What opportunities exist for physiotherapists
working in CDM teams ✓

7/02/2015
8
Tsunami of chronic disease
By 2020 ¾ of all deaths will be from chronic disease
WHO
78% with arthritis report having at least one other chronic disease
http://www.aci.health.nsw.gov.au/models-of-care/osteoarthritis-chronic-care-program
Managing Arthritis with the
OSTEOARTHRITIS CHRONIC
CARE PROGRAM
Background
Unsustainable increase in personal, societal + health care costs (ageing, obesity and injury)
Increasing burden
( OA leading cause of disability among older Australians)
International/National/State = ACTION

7/02/2015
9
EVIDENCE: Zhang et al 2010, OARSI recommendations for the management of hip and knee osteoarthritis Part III: changes in evidence following systematic cumulative update of research published through January 2009, Osteoarthritis and Cartilage, vol, 18, no. 4, pp. 476-499. Hochberb et al , 2012, American college of Rheumatology 2012 recommendations for the use of Non- pharmacologic and Pharmacologic Therapies in Osteoarthritis of the hand, Hip and Knee, Arthritis care & Research, vol. 64, no. 4, pp. 465-474. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis, 2013, Ann Rheum Dis, vol. 72, pp. 1125-1135
• Exercise (aerobic + resistance): land or water
• Injury avoidance �
• Weight control
• Pharmacologic treatment
• Timely access to surgery
• �Psychosocial
safe and cost effective TREATMENT
Osteoarthritis chronic care program OACCP
• Point of access
• Conversation
• Interdisciplinary
• Co-ordinated
• Conservative
• Responsive
OACCP aims:
• Manage symptoms
• Optimise function / QOL
• Limitation disease progression
• Screen/ Identify co-morbidity risk
• Maximise self-management
• Dispel myths about OA
• Effective health care utilisation
7/02/2015
10
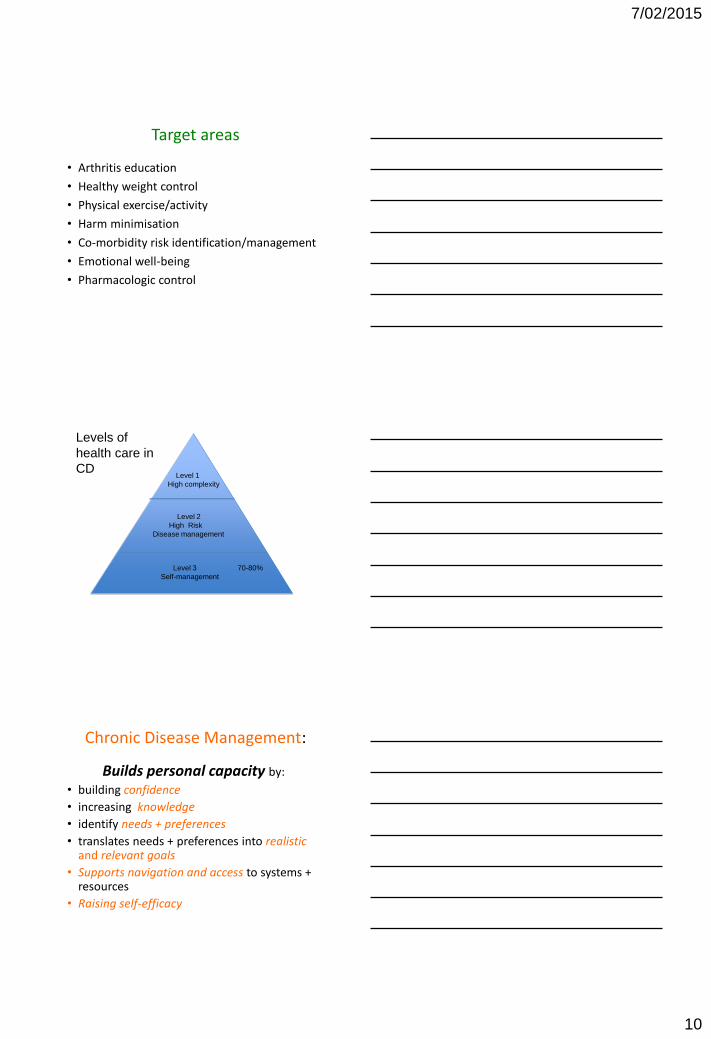
Target areas
• Arthritis education
• Healthy weight control
• Physical exercise/activity
• Harm minimisation
• Co-morbidity risk identification/management
• Emotional well-being
• Pharmacologic control
Level 1
High complexity
Level 2
High Risk
Disease management
Level 3
Self-management
70-80%
Levels of
health care in
CD
Builds personal capacity by:
• building confidence
• increasing knowledge
• identify needs + preferences
• translates needs + preferences into realistic and relevant goals
• Supports navigation and access to systems + resources
• Raising self-efficacy
Chronic Disease Management:

7/02/2015
11
PHILOSOPHY
• Access to safe, effective and timely care
• Participants are expert – opportunity
• Health practitioners are facilitators
advise support guide
• Self-management is key
“you have + are the solution”
• Window of opportunity
What CAN I do ??
Unalterable
• Age
• Gender
• Race
• Genetics
Modifiable
• Body Weight
• Diet
• Muscle Weakness
• Injury
• Mechanical load
• Control of other chronic disease
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:

7/02/2015
12
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:
Medication
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:
Walking aids
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline: Healthy Eating / Weight Control

7/02/2015
13
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:
Negative Emotions
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:
Exercise
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Other Conditions
Timeline:

7/02/2015
14
Family Doctor
Surgery Surgeon = Ortho waiting list for joint replacement
Timeline:
Medication Exercise
Walking aids
Healthy Eating / Weight Control
Negative Emotions Other Conditions
Learning
CHALLENGE EXISTING PHILOSOPHIES
of PRACTICE + DELIVERY
Shared decision-making
Building personal capacity
Thinking outside the “box”
Work in “teams of partnership”
EXTEND TRADITIONAL ASSESSMENT + TREATMENT
ROLES, SKILLS + KNOWLEDGE
Broad based needs based assessment
Dual ‘expert role’
Goal orientated evidence based treatment
Recognition of professional boundaries + limits
Communication quality and content
Explore wide + varied learning opportunities
7/02/2015
15
BROADEN + BUILD TIES WITH TEAM COMMUNITY SUPPORT +
PROVIDERS
Identify and nurture key partnerships
Refer appropriately + timely
Think more broadly than ‘health’ for partnerships
Be familiar with support networks + local champions
Advocate
Learning Outcomes
2. Justify the role of PT in the prevention +/or management of chronic illness or disease ✓
3. Critically reflect on the contributions of a interdisciplinary team ✓
4. Research a client-centred approach in the design of a physiotherapy management plan for the management of CD ✓
The bottom line…
Not rocket science
Complex + Challenging
Dual ‘expert’ role
Extend self as practitioner
Highly Rewarding
Community based: anywhere and anytime
Wont have all the answers
Building personal capacity
Foster partnerships of care
Have fun

7/02/2015
16
References: 1. Australian government: Department of Health and Ageing, National Physical
Activity Guidelines, accessed September 10th 2011,
http://www.health.gov.au/internet/main/publishing.nsf/Content/health-
pubhlth-strateg-phys-act-guidelines#rec older
2. Depression Anxiety Stress Scale (DASS (21)
viewed: 26th January 2013
http://www2.psy.unsw.edu.au/groups/dass//
3. Euro Quality of life (EQ-5D-5L)
viewed 26th January 2013
http://www.euroquol.org/
4. Hip and Knee disability and osteoarthritis outcome score (HOOS)
viewed 26th January 2013
http://koos.nu/index.html
5. Levels in healthcare
viewed 26th January 2013
http://www.health.gov.au/internet/main/publishing.nsf/content/7E7E9140A3D3A3BCCA257140007AB32B/$File/stratal3.pdf
6. National Health Priority Action Council (NHPAC) 2006, National Chronic Disease Strategy
viewed 15th March 2010,
http://www.health.gov.au/internet/main/publishing.nsf/Content/7E7E9140A3D3A3BCCA257140007AB32B/$File/stratal3.pdf
.
References:
7. NSW Chronic Care Program: rehabilitation for chronic disease volume 1.& 2, (2006), NSW Department of Health: North Sydney
8. Osteoarthritis Chronic care Program
Viewed 17th September 2012
http://www.aci.health.nsw.gov.au/models-of-care/osteoarthritis-chronic-care-program
9. Taylor, Foster & Fleming, 2008, Health care Practice in Australia, Oxford University Press, Oxford, UK
10. The Dreaded Stairs
Viewed 26th January 2013,
http://www.youtube.com/watch?v=Qx_8gxh76iM
11. Zhang, W, Moskowitz, R, Nuki, G, Abramson, S, Altman, R, Arden, N, Bierma-Zeinstra, S, Brandt, K,Croft, P, Doherty, M, Dougados, M, Hochberg, M, Hunter, D, Kwoh, K, Lohmander, S & Tugwell, P 2008, ‘OARSI recommendations for the management of hip and knee osteoarthritis, Part 2: OARSI evidence-based, expert consensus guidelines, ‘ Osteoarthritis and Cartilage, vol. 16, pp. 137-162
12. Zhang, W., Nuki, G., Moskowitz, r.W., Abramson, S., Altman, r.D., Arden, N.k., Bierma-Zeinstra, S., Brandt, k.D., Croft, P., Doherty, M., Dougados, M., Hochberg, M., Hunter, D.J., kwoh, k., Lohmander, L.S. and Tugwell, P. (2010), OArSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis and Cartilage. 18(4):
p. 476-499
Screening tools:
1. DASS(21)
2. Mini mental state examination (MMSE)
3. Timed up and Go (TUG)
4. Mini nutritional Assessment (MNA)
5. Opioid risk tool (ORT)










![Chest physiotherapy compared to no chest physiotherapy for ... · [Intervention Review] Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis Cees P van der](https://img.pdfslide.net/doc/110x75/5cc2dd0188c99389538bb642/chest-physiotherapy-compared-to-no-chest-physiotherapy-for-intervention.jpg)