Embed Size (px)
Citation preview

Comparative Quantitative Analysis of theElectrocardiogram and the Vectorcardiogram
Correlations with the Coronary Arteriogram
By DAVID R. MCCONAHAY, M.D., BEN D. MCCALLISTER, M.D.,
FRANZ J. HALLERMANN, M.D., AND RALPH E. SMITH, M.D.
SUMMARYSimultaneously recorded standard electrocardiograms (ECG) and Frank vector-
cardiograms (VCG) were correlated with the coronary arteriograms and the leftventiiculograms of 210 patients. Quantitative criteria were applied to ECG measure-
ments made by manual technics and to VCG measurements obtained by computer
technics.As the extent of significant arteriographic disease increased, the frequency of ECG
and VCG evidence of "definite" myocardial infarction (MI) increased. The VCGwas diagnostic of MI in a greater number of patients than the ECG (50 versus 39,P < 0.01) and excelled in the detection of multiple areas of infarction in a greater
number of patients (13 versus -six, P <0.05). This increased sensitivity was gainedin anterior, inferior, and true posterior infarcts. Excluding patients with myocar-
diopathy, all MIs diagnosed from the VCG and all but one from the ECG were
associated with significant arteriographic disease in the distribution of the predictednutrient artery.
Quantitative VCG analysis appears superior to the usual ECG analysis in the ac-
curate detection of MI. When MI is diagnosed by either technic, significant associatedcoronary artery disease can be anticipated in a predictable anatomic distribution.
Additional Indexing Words:Coronary heart disease
SELECTIVE cinecoronary arteriographyhas offered the clinician a unique oppor-
tunity to demonstrate the anatomy of thecoronary arteries in the living patient and tocorrelate this anatomy with the clinicalmanifestations of coronary artery disease. Anystudy correlating electrocardiographic datawith coronary arteriographic findings must bemade with a full awareness that informationfrom arteriography is limited to a demonstra-tion of the anatomic distribution and extent ofmajor coronary atherosclerosis and collateral
From the Mayo Clinic and Mayo Foundation,Departments of Internal Medicine and Roentgenology,and the Mayo Graduate School of Medicine(University of Minnesota), Rochester, Minnesota.Received March 3, 1970; revision accepted for
publication April 30, 1970.
Circulation, Volume XLII, August 1970
Computer Ventriculography
vessels and can only inferentially suggest thepresence of associated myocardial ischemia ornecrosis.1 2 In contrast, the conventionalscalar electrocardiogram (ECG) and correct-ed orthogonal vectorcardiogram (VCG) candetect evidence of myocardial ischemia andassociated infarction but provide no directinformation about the coronary arterial anato-my which underlies such ischemia. Neverthe-less, such a study correlating the electrocar-diographic findings and the associated in vivocoronary anatomy would permit an assess-ment of the screening value of the ECG andthe VCG and allow a valid comparison of theability of various ECG and VCG criteria todetect myocardial damage accurately.
Despite early reports3-5 purporting theoreti-cal superiority of the VCG over the
245
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCONAHAY ET AL.
0 0
*
t.:q C'
0
to O
+ usyD~ ~ ~ c
~ ~ ~ 14~
c3aa.Cu4
us
X0aCu
kC
"0 _;-u
Cu
eQus=
o0 rB-X*_1usC40-a
0C;*s t
Cs"0.4-a
Cs Q
+4 +
C):
C.+
5 +4
C- z f
..~
o3 us1Cua<
B4 +4
GCQ._.P Q
*~ ¢~"C,
ECG, subsequent carefully controlled compari-sons-8 failed to reveal a significant clinicallyapplicable difference between these twomethods. Recently, however, quantitativeVCG criteria have been described,'-15 present-ing the possibility that application of suchquantitative criteria might give more sensitiveand selective results than either qualitativeloop analysis of the VCG or conventionalanalysis of the ECG.The present study was therefore designed to
compare the results of an ECG analysis usingcriteria applied to manual measurements anda VCG analysis using criteria applied todiscrete voltage data derived from a computerprogram, and to correlate these results and theclinical history with the associated cinecoro-nary arteriogram and left ventriculogram.
MethodsTwo hundred ten patients who underwent
selective cinecoronary arteriography of satisfac-tory diagnostic quality following simultaneousresting ECG and VCG evaluation at the MayoClinic are represented in this report. Of thesepatients, 172 were men and 38 were women(table 1), and ages ranged from 21 to 76 years(mean 48.2). Arteriographic examination wasperformed (1) to establish or exclude thepresence of significant coronary artery disease inpatients with a diagnostic chest pain problem,(2) to evaluate the extent of coronary arterydisease in patients with aortic valvular diseaseand angina, or (3) to define the location andseverity of coronary disease in patients beingconsidered for coronary artery surgery. Clinicalinformation including the character and durationof the associated chest pain was recorded in eachinstance as part of a prospective study.Coronary Arteriogram andLeft Ventriculogram
Cinecoronary arteriograms and cine-left ven-triculograms were obtained by means of a dualmode Siemens 6/10-inch image intensifier with anattached 35-mm Arriflex camera and a 100-mm overframing lens. The x-ray source was aBiangulix grid-pulsed 150/30/50 R x-ray tube ofwhich the 0.6-mm focal spot was used exculsive-ly. Kodak double X negative film was used, beingprocessed at 72 F at 132 to 2 feet/min. The leftventriculograms were recorded in the rightanterior oblique projection using the 10-inchmode of the amplifier at 48 or 60 frames/sec,with injection of 40 to 50 ml of meglumine
Circulation, Volume XLII, August 1970
246
aoA
0
0
-
0
0
*d
S.(I3
A
[a*Os03¢ <
,is,a
o *-z 0Oe
a
.0
u
dS
U
C)
0
C)
us
0o
C.
0c)-
c)
C.
C.
0Qt0e
bo,.,
:<>03 - li
>r4
xa4cc
o .C
**g.0o 0444
6 cq r-
en4
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
Table 2Grading of Occlusion of Coronary Arteries
Occlusion (%) Grade
1-25 126-50 251-75 376-95 496-99 5100 6
diatrizoate (Renografin 76%) within 3 to 4 sec.Selective coronary arteriograms taken at 60frames/sec using the magnifying mode of theamplifier were recorded in multiple right and leftanterior oblique positions with hand injections of8 to 10 ml of this contrast medium utilizing thetechnic described by Sones and Shirey.'6
Each study was interpreted independently byat least two of the authors without knowledge ofthe patient's clinical or electrocardiographicstatus. In each instance the major coronaryarteries and their branches including the left maincoronary artery, the left anterior descending andleft circumflex arteries and their diagonalbranches, and the right coronary artery and itsmarginal branch were studied, and each wasassigned a grade based on the most severeluminal narrowing noted (table 2). The locationand extent of collateral vessels were alsorecorded. Arterial dominance (right, left, orbalanced) was defined by which vessel (rightcoronary, left circumflex, or both arteries)supplied the posterior descending coronary artery.
Based on pathologic studies by James,17 theexpected arterial supply to the various areas ofleft ventricular myocardium is summarized intable 3.The right anterior oblique projection of each
left ventriculogram was qualitatively evaluatedfor localized and generalized disorders of myocar-dial contraction. This visual analysis was facili-
Table 3Expected Location of Arteriographic OcclusionsAssociated With Myocardial Infarctions17
Site of infarct Associated arterial disease*
Anteroseptal LADAnterior LADAnterolateral LAD + LCxHigh lateral LCxInferior RCA (if right coronary dominant)
LCx (if left coronary dominant)True posterior RCA (if right coronary dominant)
LCx (if left coronary dominant)
*Abbreviations as defined in tables 1 and 5.Circulation, Volume XLII, August 1970
tated by recording single end-systolic and end-diastolic tracings of the internal contour of theleft ventricular chamber.
Electrocardiogram and VectorcardiogramElectrocardiograms and vectorcardiograms were
obtained simultaneously by methods previouslydescribed.'8' 19 During a 10-sec recordingperiod, six channels of analog data were acquiredon-line in storage buffers of a digital computer.*During this acquisition, analog to digital conver-
sion resulted in discrete voltage measurements foreach lead at 4-msec intervals. Modified Frankorthogonal electrocardiograms4 were recordedcontinuously with the patient supine and thethoracic electrodes at the level of the fifthintercostal space. Standard electrocardiographicleads in four sets (I, II, III; aVR, aVL, aVF; V1 toV3; V4 to V6) were switched electronically every2.5 sec.
Automatic digital recognition and measurementprograms were then applied to the Frankorthogonal electrocardiogram. Individual waveswere recognized, and their onsets and termina-tions were determined. All of the waves of eachkind (P, QRS, T) were compared, and a typicalcomplex was automatically selected for furtheranalysis. The voltages of the X, Y, and Z leads ofthis complex were printed in segments timed fromthe start of the R wave (fig. 1).The location of the initial 20-msec QRS vector,
the amplitude and duration of the initial right-ward, anterior, and superior QRS forces, themagnitude of the maximal leftward deviation ofthe initial superior QRS forces, and the maximalanterior QRS accession time were derived as
shown in figure 1. The VCG was then analyzedby application of quantitative criteria to thesedata provided by the computer readout. Inaddition, the VCG loops were automaticallyinscribed as illustrated in figure 2, using Helm'ssystem of notation,20 and the X, Y, and Z leadswere displayed in scalar form with a time base of100 mm/sec. These reconstructed loops were
used only to facilitate analysis of their contourand to derive the direction of the maximal QRSvector.
Characteristic ECG complexes from each of thefour sets of leads also were selected by computerprograms and displayed using digital-to-analogplotting programs with a time base of 50 mm/secand the voltage-height relationships recom-
mended by the American Heart AssociationCommittee on ECG Standards21 (fig. 2). Theseelectrocardiograms were measured subsequentlyby the usual manual technics.
*IBM 1800.
247
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

248x
MILLISECOND MILLISECOND MICROVOLTSSEGMENT TOTAL +10
McCONAHAY ET AL.Y z
MIICROVOLTS MICROVOLTS-10 +10
2 1 84 5 -5 -35
Initial Rightward 3n OSDrto
RS Duration 16 msec U Ant QRS DurationR-WAVE
2 112 \ 11 1 143 1 16 \ 10 2 222-4 120 0O -1 222
z-->5 124 21 -9 -17/t ~~~ ~ ~~ ~~~1286/ -19 1 13/
Location Initial 136 3 -48 -620 msec Vector 44
Ant., Inferior, a Leftwar 28 Ant. ORS Magnitude 0.22 mv156 Max. Ant. QRS Accession
15 16 Time = 12 msecInitial Superior 3 -9-
0 -6 -7QRS Duration -15 msec 0 0 -1
T-WAVE Initial Superior Leftward 0 -2 -1
Deviation = 0 mv -2 -2 -1-5 0 -3
4- 196 ~~ ~ ~ ~~-50 -15 200 -4 0 06 204 -4 0 07 208 -6 0 -1
Figure 1
Portion of prinxtout from computer program (terminal part of P-R segment, R wave, and initialpart of T wave) with discrete voltage measurements in X, Y, and Z leads obtained at 4-msecsampling intervals, illustrating source of certain data from a patient with a normal VCG. Thepolarity is such that a vector directed leftward, anteriorly, and superiorly inscribes a poxitivedeflection. Onset of the R wave in this example occurs at 108 msec and is directed anteriorly,superiorly, and to the right.
Scalar Electrocardiographic CriteriaThe "definite" criteria were selected from
generally accepted sources in the literature, butthe "possible" criteria were arbitrarily conceivedby the authors to extend the sensitivity of the"definite" criteria. These criteria may be outlinedas follows:Anteroseptal myocardial infarction
Definite: One of the following (in the absenceof left ventricular hypertrophy or left bundle-branch block):(1) QS deflection in leads V1, V2, and V3,22
or(2) QS deflection in V1 with qR in V2 and
V3(3) QS or QR in V1 with QR in V2 and V3
(Q of 0.04-sec duration and amplitudegreater than 25% of following R wave)
Possible:(1) Above criteria in presence of left ven-
tricular hypertrophy, or(2) QS deflection in V1 with qR in V. and V3
Anterior myocardial infarctionDefinite:11 Presence of normal septal q waves
in leads I, V5, and V8 with one of following:(1) Presence of an initial R in V1 followed
in V2 to V4 by a Q of 0.04-sec durationand amplitude greater than 25% of Rwave
(2) In absence of left ventricular hyper-trophy or left bundle-branch block, adecreasing amplitude of initial R waveon going from V1 to V4
Possible: Normal septal forces + Q in V2 to V4of 0.02 to 0.04-sec duration or1 amplitude of10 to 24% of following R wave
Anterolateral myocardial infarctionDefinite: 12 rS deflection in V1 anld V., with a
decrease in amplitude of R wvave in V: aniddevelopment of a Q in V4, V aand V, of0.04-sec duration aind depth greater tlan 15%of total amplitude of QRS comiplex
Possible: Q wave in leads V,, V,-, anid V,. of0.03 to 0.04-sec durationi and depth greatertlhain 10% of total amplittude of QRS complex
Circ -idation, Volume XLII. August 19(7)
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTlTATIVE ANALYSIS OF ECG AND VCG
.i.A
N
p
I M
20M ^r ,
Figure 2Patient with RCA (grade 4) and LAD (grade 3) disease annd a normal left ventrictnlogran. FECGreveals only repolari-zation abnormalities. VCG is conisistent wvith truie posterior infarct (an-tenior QRS magnituide - 0.56 my, anzterior QRS dturationz = 80 riisec, maximnal anterior QRSaccession timle = 52 msec, aniteriorldisplacenment of afferent limib in transvese plane) and ftulfillsall criteriia for inferiori infarct except contouti of inzitial superior QRS forces (iniitial stuperior QRSdluration = 25 insec, iniitial superior leftwar-d deviation 0.30 mv).
High lateral myocardial infarctionDefin-ite:'2 One or both of folloxving:
(1) Q wave in aV71r of 0.04-sec duration anid50% of amplitude of followving R wave(in the presence of upriglht P waves inthe same lead anid in the abseince ofsevere left venitricular hlypertrophy)
(2) Q 'wave in lead I of 0.04-sec durationiand greater thani 10% of amplitude oftotal QRS complex (in absence of se-vere left ventricularl hypertrophy)
Possible: Q wave in lead I or aVLj of 0.03 to0.04-sec duratioi
Iniferior myocardial infarctioniDefinite: Onie or 1)oth of followinig:
(1) Q vave in leads III anid aV,. of morethani 0.04-sec duration xvitlh a deptlhgreater thaini 25% of amplitude of fol-loxving R vave in same lead22
(2) Iniitial R wave in aVj1 exceeding 1 mIm(0.1 mv)23
Possible: Q wave in leads III and aV1. of 0.03to 0.04-sec duration and 10 to 24% of ampli-tude of R wave in same lead
True posterior inyocardial inifarctioniDefinite:1' Iniitial R wave in V, or V2 or both
of 0.04-see duration with RV, /SV1 equalto or greater than 1 (in patienits over 30
Circulation, Volumiie XLII, August 1970
years of age and in absenice of riglht bunidle-branich block, right ventricular hypertropby,or \Wolff-Parkinson-White synidrome)
Left venitricular- hypertrophy: Onle or more offolloxving:
(1) Amiiplitude of S wave in lead VI + maxi-mal R vave in lead V5- or V(; greatertlhan 35 mmn 4
(2) Maximal R wave in lead Vr- or V6greater than 26 mm24
(3) 'Maximal S xxave in lead V1 or V2. + Rwvave in lead VN greater than- 40 mm25
Vectorcardiographic CriteriaQuanititative VCG criteria for the diagnosis of
myocardial inifaretion based inimost inistanices onaniatomic correlative studies but in some instancesoni souind cliniical correlative efforts were selectedfrom the recenit literature for application in thisreport. Certaini modifications wvere rnade in somecriteria in ani attempt to reduce the iniciden-ce offalse positive diagnoses. Againi, the possiblecriteria wvere arbitrarily selected to extend thesensitivity of the definite criteria. The VCGcriteria are as follovs:Aniteroseptal myocardial inifarctioin
Definite: Absent initial aniterior QRS forces'with either posterior an-d leftward displace-
249
.T
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCONAHAY ET AL.
ment of initial 20-msec QRS vector if septalforces are absent or posterior and reducedrightward displacement of initial 20-msecvector if septal forces are only diminished9' 10
Possible: Initial posterior displacement of QRSvector for less than 20-msec duration
Anterior myocardial infarctionDefinite: Preservation of initial septal forces
but reduced anterior QRS forces with dis-placement of 20-msec QRS vector and ef-ferent limb posteriorly and to left of E point(in absence of left ventricular hypertrophyor left bundle-branch block)9-11
Anterolateral myocardial infarctionDefinite: Displacement of 20-msec QRS vector
to right and displacement of efferent limb toright and posterior with initial rightwardQRS forces of greater than 22 msec induration and greater than 0.16 mv in am-plitude10
Possible: Initial rightward displacement of QRSloop for a duration greater than 22 msec
High lateral myocardial infarctionDefinite: Displacement of initial QRS deflection
and efferent limb inferiorly and slightly toright with counterclockwise inscription ofQRS in frontal plane despite a verticallydisplaced maximal QRS vector greater than+40010, 12, 13
Possible: Displacement of initial QRS deflec-tion and efferent limb superiorly and to rightwith counterclockwise inscription of QRS infrontal plane despite a maximal QRS vectorgreater than +400
Inferior myocardial infarctionDefinite:14 Frontal plane criteria:
(1) With initial superiorly directed QRSforces:One or more of the following:(a) Early superior QRS forces must be
completely clockwise in rotation,have an upwardly convex contourlocated more leftward than initialsuperior forces, and be 20 msecor more in duration and more than0.25 mv in leftward deviation-ifalmost comnpletely clockwise in ro-tation, then early superior forcesmust be 25 msec or longer
(b) Completely clockwise early supe-rior QRS forces associated with amaximal QRS vector above +100
(2) With initial inferiorly directed QRSforces: Initial inferior QRS forces mustbe rightward and completely clockwisein rotation and must be followed byearly superior QRS forces of an up-wardly convex contour located moreleftward than initial superior forces-
early superior forces must be 25 msecor more in duration and more than0.25 mv in their most leftward deviation
Possible: One or more of the following:(1) Initial superior displacement of QRS
loop for a duration greater than 25 msec(2) Completely clockwise early superior
QRS forces in frontal plane with maxi-mal QRS vector between +200 and+100
True posterior myocardial infarctionDefinite: All of following:
(1) Maximal anterior QRS voltage of 0.5mv or more15
(2) Accession time of maximal anterior QRSforces of 30 msec or more15
(3) Ratio of maximal anterior QRS voltageto maximal posterior QRS voltage great-er than 115
(4) Total anterior QRS duration of 42 msecor more15
(5) Anterior displacement of agerent limbof QRS loop in transverse plane'0
Possible: Four of the above criteriaLeft ventricular hypertrophy: Maximal QRSmagnitude in transverse plane greater than 2.2mv if below 50 years of age, or greater than1.8 mv if 50 years old or older (in absenceof left bundle-branch block)26In both the ECG and the VCG analyses, de-
polarization and repolarization abnormalities wereassigned a grade based on the criteria in table 4.ECGs and VCGs were interpreted independentlyof each other and without knowledge of the pa-tient's clinical or coronary arteriographic findings.
ResultsSixty-two patients had no stenotic lesions
exceeding 50% of the arterial lumen and werethus considered in this study to be functionallynormal. Thirty-seven patients had significantobstructive disease (>50% luminal narrow-ing) limited to a single vessel and its branches;37 had such involvement of two major arteriesand their branches; 74 had such obstruc-tive lesions in all major coronary arteries(table 1). Of 122 patients in whom coronarydominance was determined, 94 (77%) hadright coronary dominance, 24 (20%) left coro-nary dominance, and four (3%) a balanced cir-culation.As expected, the character of the presenting
chest pain became more typical of anginapectoris as the extent of coronary arterydisease increased (table 1). Only two of 50
Circulation, Volume XLII, August 1970
250
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
Table 4Grading of ECG and VCG Abnormalities
ECG-VCG abnormality Grade
None 0Nonspecific repolarization abnormality 1Localized "ischemic" repolarization abnormality 2Possible myocardial infarction 3Definite myocardial infarction 4Grades 4 and 2 in same location 5
patients with normal arteriograms and with-out evidence of obstruction of the leftventricular outflow tract complained of typicalangina pectoris. In contrast, 68 of 74 patientswith diffuse coronary disease presented withsymptoms typical of angina pectoris.The longer a patient had experienced
angina the more likely he was to haveextensive arteriographic disease. Forty-one of74 patients with diffuse coronary arterydisease had experienced angina pectoris forlonger than 48 months. However, only five of25 patients with isolated disease of the leftanterior descending or right coronary arterywithout aortic valve disease had noted typicalangina for more than 36 months prior tostudy. Thus the likelihood of finding an
Correlation of Incidence of DefiniteArteriographic Coronary Disease
isolated lesion in a single coronary vessel atarteriography in the preoperative evaluationof a patient who has experienced typicalangina for more than 3 years is small.Nevertheless one patient in this study experi-enced angina for more than 10 years prior toarteriographic demonstration of single-vesseldisease.
Five of 74 patients with diffuse arterio-graphic disease and four of 37 patients withtwo-vessel disease had experienced typicalangina for less than 12 months but only seven
of 37 patients with single-vessel disease had a
similarly brief duration of typical angina.The eight patients in this series with left
bundle-branch block and the 10 with eitheridiopathic hypertrophic subaortic stenosis or
idiopathic myocardiopathy are excluded fromthe subsequent results but will be discussedseparately.
Correlation of ECG and VCGWith Coronary ArteriogramOne hundred forty-nine patients in this
series had neither ECG evidence of leftventricular hypertrophy nor clinical evidenceof rheumatic heart disease (table 5). Of thisgroup, 110 had arteriographic coronary dis-
Table 5Infarctions on ECG and VCG With Extent of
No. of patientsWith definite infarcts
Arteriogram Total ECG VCG Combined
Normal 39 0 0 0Single-vessel diseaseLAD 15 3 3 3RCA 10 2 3 3
Double-vessel diseaseLCA or LAD-LCx 11 2 4 4RCA + LAD or LCx 16 1 6 6
Diffuse 3-vessel disease 58 23 24 26TotalsExcluding RHD and LVH 149 31 40 42Including RHD and LVH 192 39 50 53Patients with abnormal arteriograms 143 39 50 53
(27.3)* (35.0) (37.1)
*Figures in parentheses indicate percentages.Abbreviations: LCA = main left coronary artery; LAD = left anterior descending artery and
its diagonal branch; LCx = left circumflex artery and its diagonal branch; RCA = right coronaryartery; RHD = rheumatic heart disease; LVH = left ventricular hypertrophy.
Circulation, Volume XLII, August 1970
2S1,
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from
McCONAHAY ET AL.
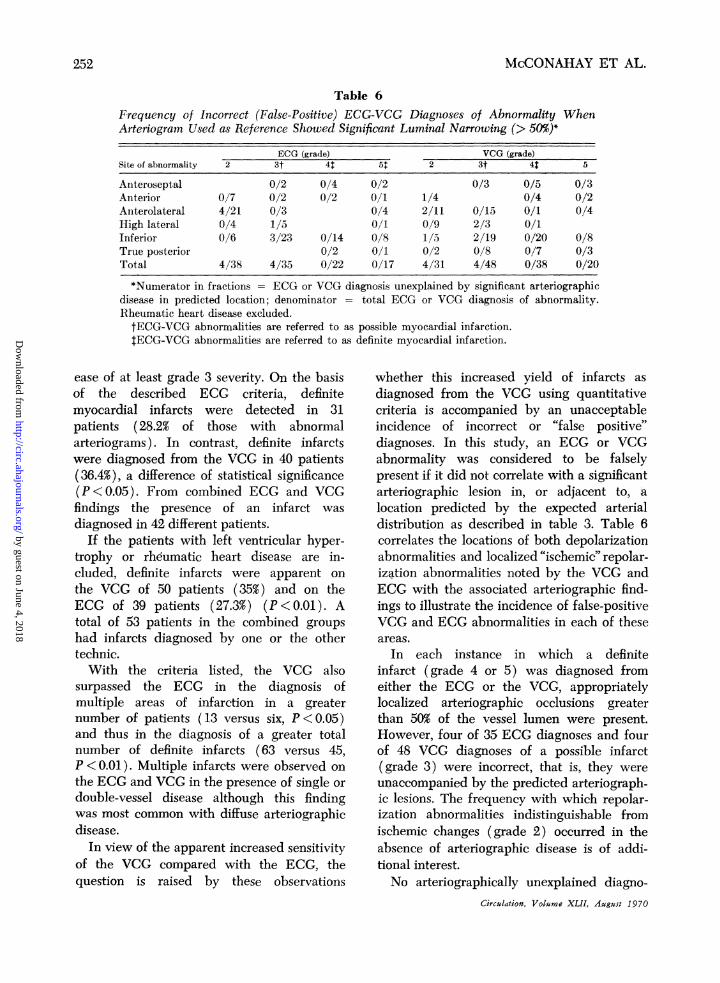
Table 6Frequency of Incorrect (False-Positive) ECG-VCG Diagnoses of Abnormality WhenArteriogram Used as Reference Showed Significant Luminal Narrowing (> 50%)*
ECG (grade) VCG (grade)Site of abnormality 2 3t41 51 2 3t 4t 5
Anteroseptal 0/2 0/4 0/2 0/3 0/5 0/3Anterior 0/7 0/2 0/2 0/1 1/4 0/4 0/2Anterolateral 4/21 0/3 0/4 2/11 0/15 0/1 0/4High lateral 0/4 1/5 0/1 0/9 2/3 0/1Inferior 0/6 3/23 0/14 0/8 1/5 2/19 0/20 0/8True posterior 0/2 0/1 0/2 0/8 0/7 0/3Total 4/38 4/35 0/22 0/17 4/31 4/48 0/38 0/20
*Numerator in fractions = ECG or VCG diagnosis unexplained by significant arteriographicdisease in predicted location; denominator = total ECG or VCG diagnosis of abnormality.Rheumatic heart disease excluded.tECG-VCG abnormalities are referred to as possible myocardial infarction.tECG-VCG abnormalities are referred to as definite myocardial infarction.
ease of at least grade 3 severity. On the basisof the described ECG criteria, definitemyocardial infarcts were detected in 31patients (28.2% of those with abnormalarteriograms). In contrast, definite infarctswere diagnosed from the VCG in 40 patients(36.4%), a difference of statistical significance(P< 0.05). From combined ECG and VCGfindings the presence of an infarct wasdiagnosed in 42 different patients.
If the patients with left ventricular hyper-trophy or rheumatic heart disease are in-cluded, definite infarcts were apparent onthe VCG of 50 patients (35%) and on theECG of 39 patients (27.3%) (P<0.01). Atotal of 53 patients in the combined groupshad infarcts diagnosed by one or the othertechnic.With the criteria listed, the VCG also
surpassed the ECG in the diagnosis ofmultiple areas of infarction in a greaternumber of patients (13 versus six, P <0.05)and thus in the diagnosis of a greater totalnumber of definite infarcts (63 versus 45,P < 0.01). Multiple infarcts were observed onthe ECG and VCG in the presence of single ordouble-vessel disease although this findingwas most common with diffuse arteriographicdisease.
In view of the apparent increased sensitivityof the VCG compared with the ECG, thequestion is raised by these observations
whether this increased yield of infarcts asdiagnosed from the VCG using quantitativecriteria is accompanied by an unacceptableincidence of incorrect or "false positive"diagnoses. In this study, an ECG or VCGabnormality was considered to be falselypresent if it did not correlate with a significantarteriographic lesion in, or adjacent to, alocation predicted by the expected arterialdistribution as described in table 3. Table 6correlates the locations of both depolarizationabnormalities and localized "ischemic" repolar-ization abnormalities noted by the VCG andECG with the associated arteriographic find-ings to illustrate the incidence of false-positiveVCG and ECG abnormalities in each of theseareas.
In each instance in which a definiteinfarct (grade 4 or 5) was diagnosed fromeither the ECG or the VCG, appropriatelylocalized arteriographic occlusions greaterthan 50% of the vessel lumen were present.However, four of 35 ECG diagnoses and fourof 48 VCG diagnoses of a possible infarct(grade 3) were incorrect, that is, they wereunaccompanied by the predicted arteriograph-ic lesions. The frequency with which repolar-ization abnormalities indistinguishable fromischemic changes (grade 2) occurred in theabsence of arteriographic disease is of addi-tional interest.No arteriographically unexplained diagno-
Circulation, Volume XLII, August 1970
2L52
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
Table 7Frequency of Incorrect (False-Positive) ECG-VCG Diagnoses of Abnormality WhenArteriogram Used as Reference Showed Significant Luminal Narrowing (> 75%)*
ECG (grade) VCG (grade)Site of abnormality 2 3 4 5 2 3 4 5
Anteroseptal 0/2 0/4 0/2 0/3 0/5 0/3Anterior 0/7 0/2 0/2 0/1 1/4 0/4 0/2Anterolateral 4/21 0/3 0/4 3/11 0/15 0/1 0/4High lateral 0/4 1/5 0/1 0/9 3/3 0/1Inferior 1/6 4/23 0/14 0/8 1/5 2/19 2/20 0/8True posterior 1/2 0/1 0/2 1/8 2/7 0/3Total 5/38 5/35 1/22 0/17 5/31 6/48 4/38 0/20
*Numerator in fractions = ECG or VCG diagnosis unexplained by significant arteriographicdisease in predicted location; denominator = total ECG or VCG diagnosis of abnormality.Rheumatic heart disease excluded.
ses occurred when either the VCG or the ECGcriteria for possible (grade 3) anterolateralinfarct or for possible (grade 3) anteroseptalinfarct were used. However, the excessivefrequency of false-postive diagnoses in usingthe VCG criterion for possible high lateralinfarct suggests that this criterion should bediscarded. Three patients had definite ECGevidence of both anterolateral and inferiorinfarets but only definite VCG evidence ofanterolateral infarct. Each had initially direct-ed superior QRS forces of greater than 25-msec duration on the VCG which wereinscribed, however, in a counterclockwisedirection, thus excluding a VCG diagnosis ofdefinite inferior infarct with the criteria used.Perhaps in the presence of a lateral infarct,prolonged initial superior QRS forces shouldsuffice for the VCG diagnosis of an associatedinferior infarct.
Table 6 also reveals that the VCG mani-fested its diagnostic superiority in the detec-tion of infarcts in three regions, namelyanterior, inferior, and true posterior, andapparently did so without sacrificing accuracy.The possibility that the criteria used for theECG diagnosis of inferior or anterior infarctswere too restricted was examined. However,extension of these criteria to include possibleinfarcts (grade 3) would be associated withthe appearance of an increased incidence ofdiagnoses which were unaccompanied by thepredicted arteriographic lesions.
If the arteriograms are reclassified so thatCirculation, Volume XLII, August 1970
an arterial occlusion must exceed 75% of theluminal diameter to be considered functional-ly significant, an occasional grade 4 definiteinfarct is then unexplained by arteriography(table 7). A single such instance on the ECGwas true posterior in location, and twoinstances each on the VCG were inferior andtrue posterior in location.A similar extrapolation of the data using
nearly complete (grade 5) and complete(grade 6) arteriographic occlusions revealedan increasing incidence of arteriographicallyunexplained ECG and VCG diagnoses, butnevertheless when only complete arterialocclusions were considered significant, thegrade 5 ECG and VCG categories maintainedtheir accuracy. Sixteen of 17 ECGs and 18 of20 VCGs of grade 5 severity were accountedfor by complete occlusion of an appropriatenutrient artery. Many grade 4 ECG and VCGlesions, however, were unexplained by arterio-graphic abnormalities of this severity.
In those patients with aortic valve disease(excluded from tables 6 and 7), one of the sixpatients with definite evidence of an infarcton the ECG had no arteriographic basis forthis finding. No similar false positive diagno-ses were noted in the five patients with aorticvalve disease and with VCG evidence of adefinite infarct.
It was apparent from this study that thelocalization of infarcts by either ECG or VCGcorrelated well with the location of significantcoronary occlusive disease. This correlation is
253
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCONAHAY ET AL.
Table 8Depolarization ECG-VCG Abnormalities Associated With Grade 6 ArteriographicLesions (Complete Occlusions)*t
InfarctNormal orInatArterio- grade 1 Anteroseptal and Anterolateral and Inferior andgraphic Collat- ECG or anterior high lateral true posterior Totalsite erals VCG Possible Definite Possible Definite Possible Definite infarets
ECG abnormalitiesRICA No 1 1
Yes 18 1 10 16$ 29
LAD No 0Yes 22 1 6 1 2 10
LCx No 1Yes 13 2 2 4;
VCG abnormalitiesRCA No 1 2 1
31
Yes 17 1 8 19
LAI) No 01
Yes 19 1 9 1 1 1 13
LCx No 1 1 )Yes 7 1 6 1 2 8 19
*One ECG and one VCG entry per arteriographic lesion. Grade 2 ECG and VCG abnormalitiesomitted.
tAbbreviations as defined in table 5.
implied by the data analysis in table 6 as
indicated by the infrequency of falsely local-ized infarcts. Further support is provided intable 8 in which the ECG and VCGdepolarization abnormalities associated withcomplete arteriographic occlusion of individu-al arteries are correlated. Table 8 alsoemphasizes the frequency with which com-
plete arterial occlusions leave no residualevidence of myocardial damage detectable byECG or VCG. Conversely, although theincidence of ECG and VCG changes consis-tent with infarction increases as the extent ofarteriographic disease increases (table 5), theECG and VCG commonly reveal definiteinfarct patterns in the presence of significantbut incomplete arterial occlusion.
Intuitively, one might expect that severedisease of the left anterior descending arterywould be more easily detected by electrocar-diography because the anteroseptal and ante-rior infarcts likely to be associated would bejust beneath the exploring electrodes. How-ever, table 8 shows that in this study severe
disease of the right coronary artery was
associated with a greater frequency of detect-able infarcts than was severe occlusive diseaseof the left anterior descending artery, suggest-ing that either the criteria for diagnosis ofinferoposterior infarcts are superior to thosefor anterior infarcts or myocardial infarction isa more common sequela of right coronaryartery occlusion than left anterior descendingartery occlusion.
Table 9Incidence of Collateral Vessels With IncreasingExtent of Arteriographic Disease
PatientsArteriogram Total With collaterals
Normal 49 0Single-vessel diseaseLAD 19 10
(52.9%)IRCA 13 8
Double-vessel diseaseLCA or LAD-LCx 14 9
(68.6% )RCA + LAD or LCx 21 13
Diffuse disease 74 65 (87.8% )Total 192 107 (74.8%)*
*Per cent of abnormal arteriograms.Circulation, Volume XLII, August 1970
254
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
The frequency with which collateral vesselswere noted increased significantly as theextent of arteriographic disease increased(P <0.01; table 9). No patient with a normalarteriogram had evidence of collateralization,whereas 53% of patients with single-vesseldisease, 69% with double-vessel disease, and88% with diffuse disease had collaterals. Therewas no evidence that the presence of such
collateral vessels reduced the likelihood thateither the ECG or the VCG would detect an
inifarct. In fact, as the incidence of collateralvessels increased coincident with the increasein extent and severity of arterial disease, an
associated increase in the incidence of infarctswas also noted.Twenty-seven of the 192 patients without
myocardiopathy or left bundle-branch blockhad ECG evidence of left ventricular hyper-trophy, and in all but two instances character-istic repolarization abnormalities were associ-ated. Only 19 of these patients also fulfilledthe VCG criteria for left ventricular hypertro-phy. The incidence of left ventricular hyper-
trophy increased with increasing extent ofarteriographic disease from 10% of the patientswith normal arteriograms and 9% with single-vessel disease to 14% with double-vesseldisease and 19% with diffuse arteriographicdisease. However, only an occasional patientwith ECG evidence of left ventricular hyper-
trophy was free of either underlying mitral or
aortic valvular disease or systemic diastolichypertension.
Correlation of Ventriculogram withECG, VGG, and Coronary Arteriogram
As the extent of arteriographically demon-strated disease increased, the incidence ofboth localized (asynergic)27 and generalizedabnormalities of myocardial contraction signifi-cantly increased (P < 0.01; table 10). Onlyone of 49 (2%) patients with normal arterio-grams had an abnormality such as a localizedor generalized reduction in myocardial con-
traction or a localized zone of akinesis or
dyskinesis recognized on ventriculography.This patient had associated aortic stenosis andinsufficiency. Twenty-six and a half per cent of
Table 10Correlation of Localized and Generalized Disorders of Myocardial Contraction With Increasing Extentof Arteriographic Disease
Patients with disorders of Incidence (%) of collateralscontraction in patients
Total % of total With disorders Without disordersArteriogram patients Localized Generalized patients* of contraction of contraction
Normal 49(10)t 0 1(1) 2.0 0 0Single-vessel disease 34(9) 6(2) 5(3) 26.5 66.7 44.0Double-vessel disease 35(5) 10(2) 9(2) 34.3 75.0 52.2Diffuse disease 74(6) 28(2) 24(2) 52.7 87.2 80.0Total 192(30) 44(6) 39(8) 31.6 80.3
*Some patients had both localized and generalized disorders.tParentheses indicate patients with rheumatic valvular disease.
Table 11
Correlation of Localized Disorders of Myocardial Contraction With ArteriographicDisease*
Arteriographic diseaseZone of RCA (grade) LCA (grade)t LAD (grade) LCx (grade)tasynergy 3-4 5-6 5-6 3-4 5-6 5-6
Anterior 1 4 8Apical 4 9 4Inferior 1 14 3
*Single arteriographic entry per ventriculographic abnormality.tNo patients with grade 3 or 4 disease in this category.
Circulation, Volume XLII, August 1970
255
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCONAHAY ET AL.
Table 12Correlation of Localized Disorders of Myocardial Contraction With ECG and VCG Abnormalities*t
InfarctNormal or Anteroseptal- Anterolateral- Inferior-
Zone of grade 1 anterior high lateral posteriorasynergy ECG or VCG Possible Definite Possible Definite Possible Definite
ECG abnormalitiesAnterior 3 1 1 1Apical 4 2 2 2 4 3Inferior 6 5 6
VCG abnormalitiesAnterior 2 3 1Apical 3 1 3 6 4Inferior 4 1 6 6
*Grade 2 ECG and VCG abnormalities are omitted. Single ECG and VCG entry per ventriculographic abnormality.tAbbreviations as defined in table 5.
the patients with single-vessel disease, 34.3%with double-vessel disease, and 52.7% withdiffuse disease had either localized or general-ized disorders of myocardial contraction.
In table 11, each zone of localized contrac-tion disturbance (asynergy) is correlated withthe associated arteriographic abnormality.Four patients had two areas each of asynergy.Each ventriculographic abnormality was con-sistently explained by occlusive disease in anappropriately located nutrient artery.
It is also apparent that the likelihood ofhaving a disorder of contraction was notreduced by the presence of associated collat-eral vessels (table 10). Although the numbersare small, there was no statistically significantdifference at the various levels of arteriograph-ic disease between the incidence of collateralsin those patients with contraction disordersand those without such disorders. No differ-ence in severity of the individual arteriallesions was noted between these two groups ofpatients.
Table 12 correlates the relationship oflocalized areas of asynergy with associatedECG and VCG findings. Satisfactory localiza-tion was accomplished by electrocardiographyalthough some overlap is noted in the apicalzone. It is apparent that a myocardial infarct,at least as diagnosed by ECG or VCG, is not aconsistent finding in the presence of ventricu-lar asynergy. Many ventriculographic abnor-malities associated with coronary artery dis-
ease would thus seem to occur on a basis ofmyocardial ischemia rather than gross scar-ring.
In five instances, characteristic ST-segmentelevation on the ECG suggested the likelihoodof a ventricular aneurysm. Two of thesepatients had a dyskinetic (paradoxical) aneu-rysm in the predicted location, two hadakinetic (noncontractile) areas in or adjacentto the predicted location, and one had asevere generalized reduction in myocardialcontraction.
Left Bundle-Branch Block
Eight patients in this series had ECGevidence of complete left bundle-branchblock. Coronary arteriographic findings werenormal in six of these patients, and in each theECG and VCG revealed only a typicalcomplete left bundle-branch block. The singleinstance of atypical complete left bundle-branch block28 29 (absence of anterior QRSforces) was associated with complete occlu-sion of the left anterior descending artery.
MyocardiopathyFive of the six patients with idiopathic
hypertrophic subaortic stenosis included inthis study had normal coronary arteriograms.The sixth patient had complete occlusion ofthe proximal part of the right coronary arteryand evidence of a possible inferior infarct onECG and VCG and a definite true posteriorinfarct on VCG. None of the patients with
Circulation, Volume XLIIJ, August 1970
256
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
normal arteriograms had electrocardiographicevidence of definite infarct although leftventricular hypertrophy was diagnosed inthree patients. Four other patients had nonob-structive myocardiopathy of uncertain origin.A diagnosis of definite infarct was made in theabsence of associated arteriographic disease intwo cases from the ECG (inferior andanteroseptal) and in one case from the VCG(anteroseptal).
DiscussionSelective cinecoronary arteriography pro-
vides the most definitive antemortem demon-stration of the coronary arterial anatomypresently available, and as such has served as
our reference for establishing the presence
and extent of arterial disease and as the basisfor evaluation and comparison of the ECGand VCG criteria in this study. However,detailed postmortem coronary arteriographicstudies30' 31 and similar antemortem and post-mortem correlative studies32 performed undermore optimal technical conditions have em-
phasized that arteriography offers an imper-fect appraisal of occlusive lesions and thatwhen errors do occur they tend to be ones ofunderestimation of both the percentage ofluminal reduction and the length of arterialstenoses.Although we have considered a 50% reduc-
tion in luminal diameter (approximately 75%reduction in luminal cross-sectional area) tobe functionally significant33 and potentiallycapable of causing gross myocardial necrosis,we have also analyzed our data considering as
functionally significant increasing degrees ofarterial occlusion (grades 4 through 6).However, it would be erroneous to concludethat a partial or complete occlusion of a
coronary artery is necessarily accompanied bya myocardial infarct. The presence of severe
coronary occlusive disease only provides a
basis for such damage. A pathologic studywould be necessary to extend the correlationsin this report to the associated myocardialanatomy.
In the group of patients without leftbundle-branch block or a myocardiopathyCirculation, Volume XLII, August 1970
who had abnormal arteriograms, 37.1% hadevidence of a myocardial infarct on eitherECG or VCG. Nine of 34 patients with single-vessel disease, 11 of 35 with double-vesseldisease, and 33 of 74 with diffuse arteriograph-ic disease had definite evidence of an infarcton ECG or VCG. There was no evidence thatthe presence of left ventricular hypertrophy,valvular heart disease, or collateral vesselsaltered the ability of either ECG or VCG todetect an infarct. On the contrary, theincidence of both collaterals and infarctstended to increase with increasing extent ofarteriographic disease.
It is of great interest that although thecombined use of the ECG and VCG wassuperior to either technic alone, VCG criteriawere apparently superior to ECG criteriain the diagnosis of myocardial infarcts.Not only did the VCG yield a diag-nosis of definite infarcts in a greaternumber of patients (50 versus 39, P<0.01),but it also excelled in the diagnosis of multipleareas of infarcts in a greater number ofpatients ( 13 versus six, P < 0.05) and thus inthe diagnosis of a greater total number ofdefinite infarcts (63 versus 45, P < 0.01).Infarcts in the anterior, inferior, and trueposterior areas were better detected byquantitative computer analysis of the VCGthan by a conventional analysis of the ECG.As shown in table 6, this VCG advantage wasattained without sacrificing specificity and, infact, there were no patients without myocar-diopathy or aortic valve disease in whom adefinite (grade 4) infarct was diagnosed inthese sites on either ECG or VCG without thepresence of associated appropriately localizedsignificant arterial occlusions.The excessive incidence of arteriographical-
ly unexplained diagnoses of infarcts by eitherECG or VCG in the four patients withidiopathic myocardiopathy, however, sug-gests that electrocardiographic interpretationshould be approached with caution in thisparticular group. The possibility exists thatfocal electrically inactive areas of myocardialfibrosis or replacement unassociated withatherosclerosis of the major coronary vessels
257
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

McCONAHAY ET AL.
may account for this apparent inaccuracy.One of the six patients with aortic valvedisease and ECG evidence of a definite infarcthad no arteriographic basis for the finding,but all patients with a VCG diagnosis of suchan infarct in the presence of valvular heartdisease had the expected arterial occlusions.
Ventriculographic abnormalities also wereobserved more frequently with increasingextent of arteriographic disease, and theirpresence did not appear to be muted byassociated collateral vessels. Each localizedzone of altered myocardial contractility occur-red in the distribution of a predicted compro-mised nutrient artery. Furthermore, whenECG or VCG abnormalities were also noted inthe presence of localized ventriculographicfindings, they tended to occur in the samelocation as the zones of asynergy. However,disturbances of contraction often occurredwithout revealing their presence on theelectrocardiogram.The disagreement between the results of
our comparison of the ECG and VCG andthose obtained in earlier studies-8 in which nosignificant difference was appreciated betweenthese two technics is most likely explained bythe differences in the method of interpretationof the VCG and in the criteria applied to theVCG. The present study supports the conclu-sions of recent studies that a quantitativeanalysis of the corrected orthogonal VCG is animprovement over conventional analysis of theECG. It also suggests that the VCG may offera superior representation of the phasicchanges in the depolarization process whichcan be exploited by appropriate criteria,particularly criteria applied to discrete voltagedata provided by a computer.
This apparent superiority of quantitativeVCG analysis over analysis of the conven-tional scalar ECG iin the diagnosis of residuaof previous infarctions emphasizes the needfor evaluating these criteria with a moredefinitive pathologic correlative study on theone hand and an analysis of a larger group ofnormal patients on the other. If the resultsreported herein are confirmed by such ap-proaches, an expanded application of the
VCG and these criteria would seem war-ranted.
References1. Ross RS, FRIESINGER GC: Coronary arteriogra-
phy. Amer Heart J 72: 437, 19662. HERMAN MV, ELLIOTr WC, GORLIN R: An
electrocardiographic, anatomic, and metabolicstudy of zonal myocardial ischemia in coronaryheart disease. Circulation 35: 834, 1967
3. PIPBERGER HV, LILIENFIELD LS: Application ofcorrected electrocardiographic lead systems inman. Amer J Med 25: 539, 1958
4. FRANK E: An accurate, clinically practical systemfor spatial vectorcardiography. Circulation 13:737, 1956
5. SCHMITT OH, SIMONSON E: The present statusof vectorcardiography. Arch Intern Med 96:574, 1955
6. BURCH GE, HORAN LG, ZISKIND J, Er AL: Acorrelative study of postmortem, electrocardio-graphic, and spatial vectorcardiographic datain myocardial infarction. Circulation 18: 325,1958
7. JOHNSTON FD: The clinical value of vectorcar-diography. Circulation 23: 297, 1961
8. SIMONSON E, TUNA N, OKAMOTO N, ET AL:Diagnostic accuracy of the vectorcardiogramand electrocardiogram: A cooperative study.Amer J Cardiol 17: 829, 1966
9. HUGENHOLTZ PG, RYAN TJ, WOERNER T, Er AL:Recognition of anterior wall infarction inpatients with left ventricular hypertrophy: Astudy by the Frank vectorcardiogram. Circula-tion 27: 386, 1963
10. CHOU T, HELM RA: Clinical Vectorcardiography.New York, Grune & Stratton, Inc., 1967, 314pp
11. MASSIE E, WALSH TJ: Clinical Vectorcardiogra-phy and Electrocardiography. Chicago, YearBook Publishers, Inc., 1960, 592 pp
12. GUNNAR RM, PIETRAS RJ, BLACKALLER J, ET AL:Correlation of vectorcardiographic criteria formyocardial infarction with autopsy findings.Circulation 35: 158, 1967
13. HUGENHOLTZ PG, FoRKNER CE JR, LEVINE HD:A clinical appraisal of the vectorcardiogram inmyocardial infarction: II. The Frank system.Circulation 24: 825, 1961
14. YOUNG E, WILLIAMS C: The frontal planevectorcardiogram in old inferior myocardialinfarction: Criteria for diagnosis and electro-cardiographic correlation. Circulation 37: 604,1968
15. HOFFMAN I, TAYMOR RC, MoRus MH, ET AL:Quantitative criteria for the diagnosis of dorsalinfarction using the Frank vectorcardiogram.Amer Heart J 70: 295, 1965
Circulation, Volume XLII, August 1970
258
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

QUANTITATIVE ANALYSIS OF ECG AND VCG
16. SONES FM JR, SHIREY EK: Cine coronaryarteriography. Mod Conc Cardiovase Dis 31:735, 1962
17. JAMES TN: The coronary circulation andconduction system in acute myocardial infarc-tion. Progr Cardiovasc Dis 10: 410, 1968
18. SMITH RE, HYDE CM: A computer system forelectrocardiographic analysis. Third AnnualRocky Mountain Bioengineering Symposium.Boulder, Colorado, 1966
19. SMITH RE, HYDE CM: Computer analysis of theelectrocardiogram in clinical practice. InGW Manning, SP Ahuja: Electrical Activity ofthe Heart. Springfield, Illinois, Charles CThomas, Publisher, 1969, pp 305-315
20. HELM RA: Vectorcardiographic notation. Circu-lation 13: 581, 1956
21. Report of Committee on Electrocardiography,American Heart Association: Recommendationsfor standardization of leads and of specifica-tions for instruments in electrocardiographyand vectorcardiography. Circulation 35: 583,1967
22. HUGENHOL1z PG, WHIPPLE GH, LEVINE HD: Aclinical appraisal of the vectorcardiogram inmyocardial infarction: I. The cube system.Circulation 24: 808, 1961
23. OKAMOTO N, SIMONsoN E, AHUJA S, ET AL:Significance of the initial R wave in lead aVRof the electrocardiogram in the diagnosis ofmyocardial infarction. Circulation 35: 126,1967
24. GRUBSCHMIDT HA, SOKOLOW M: The reliability
of high voltage of the QRS complex as adiagnostic sign of left ventricular hypertrophyin adults. Amer Heart J 54: 689, 1957
25. GRANT RP: Clinical Electrocardiography: TheSpatial Vector Approach. New York, McGraw-Hill Book Co., Inc., 1957, 225 pp
26. ROMHILT DW, GREENFIELD JC JR, ESTEs EHJR: Vectorcardiographic diagnosis of leftventricular hypertrophy. Circulation 37: 15,1968
27. HERMAN MV, HEINLE RA, KLEIN MD, ET AL:Localized disorders in myocardial contraction.New Eng J Med 277: 222, 1967
28. NEUMAN J, BLACKALLER J, TOBIN JR, ET AL: Thespatial vectorcardiogram in left bundle branchblock. Amer J Cardiol 16: 352, 1965
29. DOUCET P, WALSH TJ, MASSIE E: A vectorear-diographic and electrocardiographic study ofleft bundle branch block with myocardialinfarction. Amer J Cardiol 17: 171, 1966
30. GRAY CR, HOFFMAN HA, HAMMOND WS, ET AL:Correlation of arteriographic and pathologicfindings in the coronary arteries in man.Circulation 26: 494, 1962
31. ROBBINS SL, RODRIGUEZ FL: Problems in thequantitation of coronary arteriosclerosis. AmerJ Cardiol 18: 153, 1966
32. KEMP HG, EVANS H, ELuorI WC, ET AL:Diagnostic accuracy of selective coronarycinearteriography. Circulation 36: 526, 1967
33. SEWELL WH: Coronary cinearteriography forrecognition of "demand" for collateral arteries.JAMA 186: 224, 1963
Notice to Authors
Manuscripts for CIRCULATION should now be submitted to:Dr. Charles K. FriedbergRoom 5552 East 103rd StreetNew York, New York 10029
Circulation, Volume XLII, August 1970
259
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from

and RALPH E. SMITHDAVID R. MCCONAHAY, BEN D. MCCALLISTER, FRANZ J. HALLERMANN
Vectorcardiogram: Correlations with the Coronary ArteriogramComparative Quantitative Analysis of the Electrocardiogram and the
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.42.2.245
1970;42:245-259Circulation.
http://circ.ahajournals.org/content/42/2/245located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 4, 2018http://circ.ahajournals.org/
Dow
nloaded from





























