Embed Size (px)
Citation preview

Dow
nloadedfrom
http://journals.lww.com
/psychosomaticm
edicineby
m7j+Lz0A3Xt3G
AEMxe9Q
PIKKgtfQDefByxgj8+O
e4K4QC2V+VhH
lFeJDtBW
KJTTmOPfD
vBRxi65aM
IG34bF3dM
ZuHi405EN
vLjUwjnEU
x5CrCif7VQ
izeKq06+Dhj/C
8on
04/06/2020
Downloadedfromhttp://journals.lww.com/psychosomaticmedicinebym7j+Lz0A3Xt3GAEMxe9QPIKKgtfQDefByxgj8+Oe4K4QC2V+VhHlFeJDtBWKJTTmOPfDvBRxi65aMIG34bF3dMZuHi405ENvLjUwjnEUx5CrCif7VQizeKq06+Dhj/C8on04/06/2020
Comparison of Food Cue–Evoked and Resting-StateFunctional Connectivity in ObesityShannon D. Donofry, PhD, John M. Jakicic, PhD, Renee J. Rogers, PhD, Jennifer C. Watt, MS,Kathryn A. Roecklein, PhD, and Kirk I. Erickson, PhD
ABSTRACT
Objective:Obesity is associated with differences in task-evoked and resting-state functional brain connectivity (FC). However, no studieshave compared obesity-related differences in FC evoked by high-calorie food cues from that observed at rest. Such a comparison couldimprove our understanding of the neural mechanisms of reward valuation and decision making in the context of obesity.Methods: The sample included 122 adults (78% female; mean age = 44.43 [8.67] years) with body mass index (BMI) in the overweight orobese range (mean = 31.28 [3.92] kg/m2). Participants completed a functional magnetic resonance imaging scan that included a restingperiod followed by a visual food cue task. Whole-brain FC analyses examined seed-to-voxel signal covariation during the presentation ofhigh-calorie food and at rest using seeds located in the left and right orbitofrontal cortex, left hippocampus, and left dorsomedial prefrontal cortex.Results: For all seeds examined, BMI was associated with stronger FC during the presentation of high-calorie food, butweaker FC at rest.Regions exhibiting BMI-related modulation of signal coherence in the presence of palatable food cues were largely located within the de-fault mode network (z range = 2.34–4.91), whereas regions exhibiting BMI-related modulation of signal coherence at rest were locatedwithin the frontostriatal and default mode networks (z range = 3.05–4.11). All FC results exceeded a voxelwise threshold of p < .01and cluster-defining familywise error threshold of p < .05.Conclusions: These dissociable patterns of FC may suggest separate neural mechanisms contributing to variation in distinct cognitive,psychological, or behavioral domains that may be related to individual differences in risk for obesity.Key words: obesity, functional connectivity, food, reward, frontostriatal network, default mode network.
INTRODUCTION
Components of executive function may be impaired in obesity(1). For instance, obesity is associated with impaired perfor-
mance on tasks that require inhibition of primed responses (e.g.,flanker tasks) as well as cognitive flexibility (e.g., Wisconsin CardSorting Task (2–5)). Adults with obesity also show a preference forsmaller, immediate rewards over larger, delayed rewards relative tonormal-weight individuals (6). Importantly, steeper discounting ofdelayed future rewards has been associated with increased purchas-ing (7) and consumption (7,8) of highly palatable, calorie-densefoods, as well as binge eating disorder (4). Furthermore, greater ca-pacity for self-regulation has been associated with more frequentconsumption of healthy low-calorie foods and regular engagementin physical activity, both in healthy weight adults and adults withobesity (9–11). These findings indicate that impaired self-regulation and reward processing may predispose some individ-uals to obesity by influencing decisions regarding diet and exercise.
Impaired self-regulation and reward-related decision making inobesity may be indicative of altered signaling in the frontostriatalneural circuit linking prefrontal cortical (PFC) regions involvedin inhibitory control to midbrain regions such as the ventral striatum
and nucleus accumbens (NAc) that are involved in reward valuation(12,13). Indeed, body mass is inversely associated with activationof regions of the PFC involved in inhibitory control in response topalatable food cues (14) and during attempts to regulate cravingfor unhealthy foods (15). This is accompanied by greater activa-tion in frontostriatal regions involved in reward processing duringreward valuation tasks including high-calorie food cues (16–19).Altered signaling in frontostriatal regions is also prospectively asso-ciated with weight gain and response to weight loss interventions(16,19,20). These findings are consistent with the hypothesis thatvulnerability to obesity is linked to underrecruitment of PFC-supported inhibitory control coupled with overvaluation of rewardsas reflected by overrecruitment of medial PFC and ventral striatum.However, further work is necessary to evaluate whether the connec-tivity between these regions is also altered in obesity.
From the Department of Psychiatry (Donofry), University of Pittsburgh School of Medicine; Departments of Psychology (Donofry, Watt, Roecklein,Erickson) and Health and Physical Activity (Jakicic, Rogers), and Healthy Lifestyle Institute (Jakicic, Rogers), University of Pittsburgh; and The Centerfor the Neural Basis of Cognition (Roecklein, Erickson), Pittsburgh, Pennsylvania.
Address correspondence to Shannon D. Donofry, PhD, NHLBI T32 Postdoctoral Scholar, Department of Psychiatry, University of Pittsburgh, 3811O’Hara Street, Pittsburgh, PA 15213. E-mail: [email protected]; [email protected]
Received for publication January 17, 2019; revision received September 16, 2019.DOI: 10.1097/PSY.0000000000000769Copyright © 2019 by the American Psychosomatic Society
ACC = anterior cingulate cortex, BMI = body mass index,BOLD = blood oxygen level dependent, DMN = default modenetwork, dmPFC = dorsomedial prefrontal cortex, FD = framewisedisplacement,GLM = general linear model, IGT = Iowa GamblingTask, mPFC = medial prefrontal cortex, NAc = nucleus accum-bens, OFC = orbitofrontal cortex, PFC = prefrontal cortex,PPI = psychophysiological interaction, ROI = region of interest,vmPFC = ventromedial prefrontal cortex➢ See related articles on pages 258–60
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 261 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

There are also abnormal brain connectivity patterns among adultswith obesity, both in the context of specific task demands and at rest.For instance, obesity is associated with altered signal coherence be-tween regions in the frontostriatal network during the processing ofmonetary (21,22) and food rewards (22–24). Interestingly, successfulregulation of craving, as well as successful response inhibition, are as-sociated with the opposite pattern of cortical-subcortical connectivityamong adults with obesity, with stronger coupling predictive of moresuccessful attenuation of craving and response inhibition (25–27).
Resting-state brain networks also exhibit obesity-related differ-ences in connectivity (28–30). Obesity has been associated withdecreased global and local efficiency, as well as modularity offunctional networks throughout the brain (23,31), including thedefault mode network (DMN (32)). Furthermore, individuals withobesity show enhanced resting-state connectivity between regionsinvolved in reward valuation and decision making such as theNAc, the anterior cingulate cortex (ACC), and ventromedial PFC(vmPFC (33)), suggesting that altered reward network functionin obesity is not specific to valuation of food cues but may reflectmore fundamental context-independent disruptions. Importantly,several studies have demonstrated that diet, exercise, and weightloss surgery modify resting-state functional connectivity patterns(34–36), indicating that differences in resting-state functional con-nectivity may be mechanistically linked to obesity and are modifi-able with weight loss.
Despite this prior work, several questions remain. First, studieshave not analyzed task-evoked and resting-state connectivity in thesame individuals or examined whether differences in functionalconnectivity at rest correspond to variation in connectivity of thesesame regions during the processing of food cues. Furthermore,most studies have compared functional connectivity among adultswith obesity with that of healthy-weight individuals. Implicit inthis approach is the assumption that individuals characterized asobese are a homogenous group, which may obscure potentiallymeaningful individual differences among those who meet the clini-cal criteria for overweight or obesity. Finally, few studies have deter-mined whether weight-related differences in connectivity predictperformance on tasks that evaluate the cognitive processes thoughtto be supported by the affected networks. To address these gaps,we used a hypothesis-driven seed-based approach to determine
whether body mass was associated with variation in frontostriatalconnectivity with other brain areas during the processing of high-calorie food cues and at rest. Furthermore, we tested whethervariation in functional connectivity of these networks mediated therelationship between body mass and performance on a reward task.
METHODS
ParticipantsParticipants were recruited from a behavioral weight loss intervention fo-cused on cardiovascular outcomes. Of the 383 individuals enrolled in theintervention, 125 (32.6%) participated in this neuroimaging study. Partici-pants who completed the neuroimaging arm of the intervention did not dif-fer significantly from the parent sample on any clinical or demographicindicator, with the exception of systolic blood pressure; however, this dif-ference was not clinically meaningful (parent sample, 120.2 [11.7] mmHg;neuroimaging sample, 118.4 [11.7] mm Hg). Comparisons of the two sam-ples are provided in Table 1. The results from this study are from the datacollected at baseline, within 1 month of the start of the intervention. Datafor the neuroimaging arm of the study were collected between November2013 and July 2016. Participants for the parent study were primarily re-cruited through direct mailings and research registries at the University ofPittsburgh. The study was approved by the University of Pittsburgh Institu-tional Review Board, and all participants provided informed consent beforeinitiation of any procedures.
ProceduresExclusion criteria were as follows: women who were currently pregnant,breastfeeding, or reported planning a pregnancy in the next 12 months; his-tory of bariatric surgery; report of current medical condition or treatment ofa medical condition that could affect body weight (e.g., diabetes mellitus,hyperthyroidism or hypothyroidism, etc.); report of a current cardiovascu-lar condition, myocardial infarction, or cardiac surgery in the previous12 months; resting systolic blood pressure ≥160 mmHg or resting diastolicblood pressure ≥90 mm Hg or taking medication that would influenceblood pressure; eating disorders; substance abuse; current psychologicaltreatment; taking psychotropic medication in the previous 12 months; hos-pitalization for depression within the previous 5 years; and contraindica-tions to having a magnetic resonance imaging (MRI) assessment (e.g.,metallic implants, report of claustrophobia, etc.). Additional exclusioncriteria for this ancillary study included left-handed individuals or individ-uals with any form of traumatic brain injury or neurological illness. Given
TABLE 1. Comparison of Participants in the Neuroimaging Arm of the Study to Total Intervention Sample
Total Sample (n = 383) MRI Ancillary Study (n = 125) p
Age, M (SD), y 45.0 (7.9) 44.3 (8.6) .274a
Weight, M (SD), kg 90.9 (13.7) 91.3 (14.1) .687a
Body mass index, M (SD), kg/m2 32.4 (3.8) 32.4 (3.9) .801a
Resting systolic blood pressure, M (SD), mm Hg 120.2 (11.7) 118.5 (11.63) .044a
Resting diastolic blood pressure, M (SD), M (SD), mm Hg 72.2 (8.9) 71.1 (8.9) .077a
Waist circumference, M (SD), cm 106.4 (9.9) 106.1 (9.8) .680a
Cardiorespiratory fitness, M (SD), ml kg−1 min−1 22.6 (4.4) 22.9 (4.4) .381a
% Female 79.4 78.4 .743b
% White 72.8 76.8 .226b
MRI = magnetic resonance imaging; M = mean.a p Value based on independent t test.b p Value based on χ2 test.
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 262 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

these exclusion criteria, the sample was in generally good health apart fromhaving overweight or obesity.
Assessments
Body Mass IndexParticipants’ height and weight were obtained to calculate body mass index(BMI) according to the standard formula: kg/m2.
MRI Visual Food Cue Stimuli and DesignMRI was performed using a Siemens Verio 3-Tesla MRI scanner. For theresting-state scan, participants viewed a fixation point for 5 minutes and28 seconds. Participants then completed a visual food cue paradigm(37,38) that was adapted from Killgore et al. (38). Briefly, participants pas-sively viewed 24 second blocks of high-calorie food images (e.g., pizza),low-calorie food images (e.g., carrots), and images of neutral nonfood itemsof similar visual complexity, texture, and color (e.g., houses), with 20-second rest periods between blocks. During each block, 12 images weredisplayed for 2000 milliseconds each. Each block type was presented threetimes. Participants also rated their level of hunger on a scale ranging from 0(not at all hungry) to 10 (very hungry) between blocks. This was done toensure that participants were awake and attending to the task.
Iowa Gambling TaskThe Iowa Gambling Task (IGT) is a monetary decision-making task thatquantifies the degree to which individuals learn the decision-making strat-egy leading to the highest earnings, as well as disadvantageous selections(39). Briefly, participants completed a computerized version of the IGT inwhich they selected 100 cards one at a time from four possible decks, withthe goal of maximizing the amount of money won at the end of the task.Card selections were divided into five blocks to permit evaluation of deci-sion making trajectories over the course of the task. Two metrics were de-rived based from this. First, a net payoff score was calculated by subtractingthe total number of cards selected from the disadvantageous decks from thetotal number of cards selected from the advantageous decks ((C + D) −(A + B)). Higher payoff scores are indicative of a greater proportion of se-lections from advantageous decks. Second, a difference score was calcu-lated by subtracting the net payoff score in block one from the net payoffscore in block five to quantify change in decision making over the task.Higher difference scores suggest a positive learning curve, such that feed-back on early trials informs the adoption of a more successful decision-making strategy in later trials.
MRI Data Acquisition and PreprocessingFor the visual food cue task, 204 T2*-weighted volumes were obtainedusing a fast echo-planar imaging sequence with blood oxygen level–dependent (BOLD) contrast (time repetition, 2000 milliseconds; echo time,28 milliseconds; flip angle, 90 degrees). Thirty-four slices were collected at3.2-mm thickness in the posterior to anterior direction. For the resting-statescan, 210 T2*-weighted volumes were obtained using an echo-planar im-aging sequence with BOLD contrast (time repetition, 1540 milliseconds;echo time, 25 milliseconds; flip angle, 90 degrees). Thirty slices were col-lected at 3.5-mm thickness in the posterior to anterior direction. High-resolution T1-weighted anatomical volumes were also collected in thesagittal plane using a magnetization-prepared rapid gradient-echo sequencefor each participant (256 slices, voxel dimensions 1 � 0.976 � 0.976 mm).
Task-related and resting-state functional data were preprocessed usingFEAT version 5.98, part of FSL (FMRIB’s Software Library). Motion cor-rection was conducted using MCFLIRT (40). Functional volumes from thevisual food cue task were temporally filtered with a Gaussian high-pass cut-off of 100 seconds. Conversely, a band-pass temporal filter between 0.01and 0.1 Hz was applied to resting-state volumes to remove noise attrib-utable to physiological processes (e.g., respiration) and noise due toscanner drift. Images from both scans were spatially smoothed with a
5-mm full-width half-maximum three-dimensional Gaussian kernel.Non–brain matter (i.e., skull) was removed using the robust brain extrac-tion technique (41). Functional images were registered to Montreal Neuro-logical Institute space using 12-parameter affine transformations usingFMRIB’s linear image registration tool (FLIRT (40,42)). No errors wereobserved in image registration.
Analysis of Visual Food Cue Data
Regional Activation and Region-of-Interest SelectionSubject- and group-level analyses of neuroimaging data were conductedusing general linear models (GLMs) in FSL (FMRIB, Oxford, UnitedKingdom). Data from the visual food cue task were deconvolved using agamma function. A GLM using multiple regression examined signalchange for each condition (i.e., neutral images, high-calorie images, andlow-calorie images). Contrast parameters compared high- and low-calorieconditions relative to neutral conditions and relative to one another. Indi-viduals with motion displacement exceeding 1 mm were included as nui-sance covariates of no interest in first-level models (n = 32).
Results from these first-level comparisons were then forwarded tohigher-level mixed-effects group analyses. Age, sex, and framewise dis-placement (FD) were included as covariates. To be more inclusive in thegeneration of seeds (described hereinafter), the statistical parametric mapsfrom the visual food cue contrasts were thresholded using a voxelwisethreshold of p < .01 and a cluster extent threshold of 25 contiguous voxels.Seed regions were chosen based on regional activation patterns observedduring the task according to the following criteria: a) a region exhibited dif-ferential activation in response to food images (high or low calorie) relativeto neutral images, b) activation in response to food imageswas significantlycorrelated with BMI, and c) the region had been previously linked withobesity or to processes known to be disrupted in obesity. This approach cir-cumvents the potential problems of “double dipping” for several reasons.First, the selection of seeds based on activity during the visual food cue par-adigm does not bias or inflate BMI associations with measures of connec-tivity during the task or at rest. That is, the demonstration of a relationshipbetween BMI and regional activation in response to food cues does notreveal information or bias the likelihood that BMI relates to the mannerin which these regions communicate with the rest of the brain. Indeed,examination of task activation and task-evoked connectivity has beenshown to provide complementary rather than redundant informationon the function of a given region (43–45) and therefore should be regardedas independent approaches.
Analysis of Task-Evoked Functional ConnectivityFunctional connectivity during the visual food cue task was assessed usinga psychophysiological interaction (PPI) approach. A PPI analysis quantifiesBOLD signal covariation between a seed region and all voxels across thebrain, and determines the degree to which seed-to-voxel covariation ismodulated by contextual factors like task condition (46).
Seed masks were created for regions meeting the criteria specified pre-viously by placing a 10-mm sphere around detected maxima coordinates.The BOLD signal time series from each seed was then extracted for eachindividual. These time series were then entered into a GLM along withthe task contrast of interest and a PPI term representing the interaction be-tween the seed region time series and the task contrast. In this case, the con-trast of interest was BOLD responses to high-calorie food images versusBOLD responses during the baseline fixation. The GLM including theseterms was then applied, which generated correlation maps for each individ-ual. The β values for the PPI term represented the degree to which task-evoked variation during high-calorie foods corresponded to task-evokedvariation in the seed.
The β values were then forwarded to higher level GLMs to examinewhether BMI was associated with variation in seed-to-voxel correlationsduring the presentation of high-calorie images. Age, sex, and FD were also
Functional Connectivity in Obesity
Psychosomatic Medicine, V 82 • 261-271 263 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

included as covariates of no interest. The statistical parametric maps gener-ated for each contrast were thresholded using a voxelwise threshold ofp < .01 and a cluster familywise error threshold of p < .05 (47).
Resting-State AnalysesWe examined whether the connectivity patterns during the visual food cueparadigm were also different during rest. Thus, we used a seed-based ap-proach to assess resting-state functional connectivity, with the same seedsused in the task-evoked connectivity analysis described previously.
To reduce the influence of physiological confounds, functional vol-umes were segmented into gray matter, white matter, and cerebrospinalfluid. Using a nine-parameter denoising model (48), physiological noiseas represented by the first two principal components from white matterand cerebrospinal fluid voxels were regressed out of the whole-brain timeseries. The global signal and motion parameters were also regressed outof the whole-brain time series. Signal time series were then extracted fromeach seed and entered into a GLM using multiple regression to model BOLDsignal covariation between the seed region and all other voxels controlling forthe six motion parameters. Contrast parameters examined which voxels posi-tively and negatively covaried with the seed region time series. The β valuesderived from these analyses were then forwarded to higher level GLMs to ex-amine whether BMIwas associated with variation in seed-to-voxel correlationsat rest. Age, sex, and FD were used as covariates. The statistical parametricmaps generated for each contrast were thresholded using a voxelwise thresholdof p < .01 and a cluster familywise error threshold of p< .05.
Mediation AnalysesTo assess the relationship between IGT performance and functional con-nectivity, regions of interest (ROIs) exhibiting significant BMI-related sig-nal covariation were selected for further analysis with IGT performance.The mean parameter estimates for the identified ROIs were extracted andindependent multiple linear regression analyses were conducted using thePROCESS macro with bias-corrected bootstrapped confidence intervals((49); model 4) in SPSS version 25.0 (IBM Corp., Armonk, NY). This anal-ysis examined whether the relationship between BMI and IGT performance(total score and change score) was mediated by task-evoked or resting-statefunctional connectivity. Hunger was included as a covariate in these models.
RESULTS
Participant CharacteristicsOf the sample of 125, 3 did not complete the visual food cue task.Therefore, the final sample size was 122 (mean [SD] age = 44.43[8.67] years; 78.7% female) with BMI in the overweight and obese
range (mean [SD] BMI = 32.41 [3.95] kg/m2, range = 25.10–40.29kg/m2). The sample was predominantly white (74.6%) and non-Hispanic (97.5%). BMI was not significantly associated with race(β = −0.02, p = .86), ethnicity (β = −0.04, p = .68), sex (β = 0.04,p = .69), age (β = −0.12, p = .19), average hunger rating during the task(β = 0.14, p = .13), likelihood of having functional MRI (fMRI) datacorrected for excess motion (odds ratio = 0.334, p = .52), or IGTnet payoff score (β = −0.03, p = .76). BMI was marginally associ-ated with change in net payoff score from block one to block five(β = −0.16, p = .081), with lower BMI predicting greater improve-ments in decision making over the course of the task.
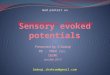
Seed Selection: Regional Activation During the VisualFood Cue TaskConsistent with prior work using the visual food cue paradigm, adiverse set of regions were active during the task. Specifically,BMI was inversely associated with activation in regions located inthe left orbitofrontal cortex (OFC), right OFC, and left dorsomedialPFC (dmPFC) during the presentation of food compared with neu-tral images. These regions were selected as seeds to be used for thetask-evoked and resting-state connectivity analyses and are depictedin Figure 1 and listed in Table 2.
Aim 1: BMI-Related Variation in FunctionalConnectivity Evoked by High-Calorie FoodIt was hypothesized that, during the presentation of high-caloriefood cues, higher BMI would be associated with reduced connec-tivity between regions involved in reward valuation (e.g., amyg-dala, medial PFC [mPFC] and OFC) and lateral regions of PFC,but with increased connectivity between regions involved inmotorplanning and execution (e.g., premotor cortex, inferior parietalcortex, and cerebellum) and those involved in reward valuation.These hypotheses were partially supported. Specifically, BMIwas associated with stronger task-evoked functional connectivitybetween regions involved in reward valuation and motor planning(e.g., OFC, dmPFC, and basal ganglia). However, contrary to ourhypotheses, there were no negative associations between BMI andtask-evoked connectivity between prefrontal cognitive control re-gions and reward valuation regions. Given that the direction of therelationship between BMI and task-evoked connectivity was con-sistent across seeds, results obtained using the left lateral OFC seed
FIGURE 1. Regional activation patterns during the visual food cue task from which seeds were selected for connectivity analyses. A,Contrast map for activation that was negatively correlated with BMI during high-calorie + low-calorie food > neutral blocks, with theseeds derived from that contrast. The left dmPFC seed is depicted in red, the right OFC seed depicted in green, and the left lateral OFCseed depicted in light blue. B, Contrast map for activation that was positively correlated with BMI during high-calorie > low-caloriefood blocks, with the left medial OFC seed derived from that contrast depicted in dark blue. C, Contrast map for activation that wasnegatively correlated with BMI during high-calorie > low-calorie food blocks, with the left hippocampus seed derived from thatcontrast depicted in yellow. BMI = body mass index; dmPFC = dorsomedial prefrontal cortex; OFC = orbitofrontal cortex; MNI =Montreal Neurological Institute; ROI = region of interest.
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 264 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

will serve as an exemplar of these effects (Figure 2). However, de-tails regarding the regions that exhibited significant BMI-related in-creases in connectivity with each seed during the presentation ofhigh-calorie food are described in Table 3.
For the left lateral OFC seed, BMIwas associated with strongerleft lateral OFC functional connectivity with regions involved insensory processing, memory formation and recall, reward valuation,and self-directed thinking during the presentation of high-caloriefood cues. These regions included the left medial frontal gyrus righthippocampus, right medial temporal gyrus, right thalamus, medialposterior cingulate cortex, and medial precuneus. Figure 2 depictsthe networks exhibiting BMI-related increases in engagement withthe left lateral OFC seed during the processing of high-calorie food.
Aim 2: BMI-Related Variation in Resting-StateFunctional ConnectivitySimilar to the hypotheses regarding the relationship between BMIand task-evoked connectivity, it was predicted that, at rest, higherBMI would be associated with reduced connectivity between re-gions involved in reward valuation (e.g., amygdala, mPFC, andOFC) and lateral regions of PFC, but with increased connectivitybetween regions involved in motor planning and execution (e.g.,premotor cortex, inferior parietal cortex, and cerebellum) and thoseinvolved in reward valuation. Across each seed selected, BMI wasassociated with weaker seed-to-ROI connectivity, but not in a man-ner consistent with our hypotheses. BMIwas consistently associatedwith weaker connectivity between regions involved in sensoryprocessing, reward valuation, and conflict monitoring, includingregions of the basal ganglia, vmPFC, NAc, and ACC. Further-more, BMI was not associated with resting connectivity betweenlateral prefrontal regions and regions involved in reward valuation,as had been predicted. It was also hypothesized that the relation-ship between BMI and resting-state functional connectivity wouldbe similar to patterns observed during the presentation of food cues.However, there was very limited overlap in the regions exhibitingBMI-related variation in connectivity during the visual food cuestask as compared with rest, and BMI predicted opposing patternsof connectivity in each of these contexts. Again, because the direc-tion of the relationship between BMI and resting connectivity didnot vary by seed, the patterns of connectivity observed using the leftlateral OFC are presented in more detail as an exemplar of the ef-fects observed in each seed. Networks exhibiting BMI-related
TABLE 2. MNI Coordinates (in mm) of Local Maxima inRegions Used as Seeds Based on Regional Activation Duringthe Visual Food Cues Task
Maximum z Score x y z
Left lateral orbitofrontal cortex 3.6 −36 24 −14Right orbitofrontal cortex 3.5 18 20 −18Left dorsomedial prefrontal cortex 3.47 −16 58 22
Left medial orbitofrontal cortex 3.35 −30 20 −16Left hippocampus 2.99 −32 −14 −20
MNI = Montreal Neurological Institute.
Regions met a voxelwise threshold of z > 2.3 and cluster extent threshold of 25contiguous voxels.
FIGURE 2. Networks exhibiting BMI-related increases in engagement with the left lateral OFC seed (MNI coordinates −36, 24, −14)during the presentation of high-calorie food cues. Map was cluster thresholded at z > 2.3 and p < .05. B, Scatterplots of the relationshipbetween BMI and seed-to-ROI signal covariation during the presentation of high-calorie food cues. BMI = body mass index; OFC =orbitofrontal cortex; MNI = Montreal Neurological Institute; ROI = region of interest.
Functional Connectivity in Obesity
Psychosomatic Medicine, V 82 • 261-271 265 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

differences in intrinsic connectivity with the left lateral OFC are il-lustrated in Figure 3. The relationship between BMI and regionalresting-state connectivity for all seeds examined is described inmore detail in Table 4.
Mediation AnalysesIn an effort to contextualize the observed associations of BMI withfunctional connectivity, additional analyses were conducted to de-termine whether task-evoked or resting-state functional connectivity
TABLE 3. MNI Coordinates (in mm) of Local Maxima in Regions Showing BMI-Related Increases in Functional ConnectivityWithEach Seed During the Presentation of High-Calorie Food
Seed Region Maximum z Score x y z
Left lateral orbitofrontal cortex Left middle frontal gyrus 3.15 −40 12 28
Right hippocampus 3.32 24 −18 −22Right thalamus 3.66 18 −26 4
Posterior cingulate cortex 3.26 −4 −36 32
Precuneus 3.49 0 −54 12
Right medial temporal gyrus 2.79 60 −20 −10Right orbitofrontal cortex Right medial temporal gyrus 4.45 62 −16 −16
Right hippocampus 3.15 28 −22 −14Left dorsomedial prefrontal cortex Left caudate 3.30 −12 −2 18
Left hippocampus 3.36 −30 −12 20
Left putamen 3.15 −28 0 0
Right putamen 3.31 18 10 −2Right pallidum 4.22 18 2 0
Medial subcallosal cortex 3.44 −2 12 −10Left medial orbitofrontal cortex Right superior temporal sulcus 2.34 60 −20 −10
Right postcentral gyrus 3.20 60 −14 34
Left supramarginal gyrus 3.51 −62 −38 34
Left hippocampus Left dorsomedial prefrontal cortex 4.91 −4 66 16
Right inferior temporal gyrus 3.74 62 −42 −16Left dorsolateral prefrontal cortex 3.30 −38 50 12
MNI = Montreal Neurological Institute; BMI = body mass index.
Regions met a cluster threshold of z > 2.3 and p < .05.
FIGURE 3. A, Networks exhibiting BMI-related decreases in intrinsic connectivity with the left lateral OFC seed (MNI coordinates −36,24, −14). Map was cluster thresholded at z > 2.3 and p < .05. B, Scatterplots of the relationship between BMI and seed-to-ROI signalcovariation at rest. BMI = body mass index; OFC = orbitofrontal cortex; MNI = Montreal Neurological Institute; ROI = region of interest.
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 266 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

differences were associated with IGT performance. Although the di-rect pathway (path c) between BMI and IGT performance was notsignificant, this is not considered a necessary condition for proceed-ing to test for mediation (50).
No indices of seed-to-ROI connectivity during the visual foodcue task were associated with IGT performance or emerged as sig-nificant mediators of the relationship between BMI and IGT per-formance. In contrast, resting-state functional connectivity withseveral OFC seeds was associated with IGT performance, withstronger connectivity consistently being associated with more ad-vantageous decision making. Interestingly, the strength of restingconnectivity for several seed-to-ROI pathways significantly medi-ated the relationship between BMI and IGT performance, withBMI being associated with lower net payoff and lesser improve-ments in performance over the course of the task (Table 5). Theseresults suggest that weaker resting connectivity between regionsinvolved in reward processing and decision making is associatedwith impaired monetary decision making overall, as well as theadoption of less advantageous monetary decision making strate-gies in response to performance feedback, with the effects beingmore pronounced with increasing BMI.
DISCUSSIONWe examined the association between BMI and functional connec-tivity during the processing of high-calorie food cues, as well as atrest, to determine whether the association between body mass andpatterns of neural connectivity is only apparent in specific contexts(i.e., in the presence of high-calorie food cues) or is evident even inthe absence of external demands or exogenous cues. Comparisonof task-evoked and intrinsic network organization revealed inter-esting though somewhat unexpected patterns of network connec-tivity. For each seed, higher BMI was associated with greaterregional connectivity in the presence of high-calorie food butweaker connectivity at rest. This suggests that regions that partic-ipate in reward valuation, learning, and memory are organized intodissociable context-dependent functional networks among indi-viduals who are overweight or obese. Furthermore, these networksmaymediate distinct cognitive, affective, and behavioral processesknown to be disrupted in obesity. In support of this hypothesis,weakened resting-state functional connectivity between subdivi-sions of the mPFC and regions involved in reward valuation(NAc, vmPFC) and conflict monitoring (ACC) was associatedwith impaired monetary decision making, whereas there was no
TABLE 4. MNI Coordinates (in mm) of Local Maxima in Regions Showing BMI-Related Decreases in Intrinsic FunctionalConnectivity With Each Seed at Rest
Seed Region Maximum z Score x y z
Left lateral orbitofrontal cortex Left thalamus 3.64 −10 −10 14
Right ventromedial prefrontal cortex 3.91 32 56 4
Right nucleus accumbens 3.21 14 18 −8Medial ACC 3.16 0 34 22
Right orbitofrontal cortex Right caudate 4.11 16 18 12
Left paracingulate gyrus 3.91 −4 50 0
Left amygdala 3.86 −28 −6 −16Right ACC 3.63 4 40 8
Left ventromedial prefrontal cortex 3.56 −10 50 −6Right nucleus accumbens 3.41 14 18 −8
Medial posterior cingulate cortex 3.24 −4 −36 38
Medial precuneus 3.05 −4 −58 18
Left dorsomedial prefrontal cortex Right putamena 3.44 30 6 −2Left dorsomedial prefrontal cortex 3.43 −10 66 14
Right dorsomedial prefrontal cortex 3.20 22 44 34
Right insula 3.14 40 −6 8
Medial posterior cingulate 3.10 0 −42 26
Right palliduma 2.96 16 6 0
Left medial orbitofrontal cortex Right ACC 3.04 10 42 18
Right putamen 2.77 22 8 −10Right superior frontal gyrus 3.03 24 40 32
Right nucleus accumbens 3.07 12 20 −6Left hippocampus Medial ACC 3.64 −4 32 22
Medial paracingulate gyrus 3.17 10 46 12
Ventromedial prefrontal cortex 3.14 −4 48 −10
MNI = Montreal Neurological Institute; BMI = body mass index; ACC = anterior cingulate cortex.
Regions met a cluster threshold of z > 2.3 and p < .05.a Denotes regions that showed BMI-related differences in functional connectivity with a given seed both at rest and during the visual food cue task.
Functional Connectivity in Obesity
Psychosomatic Medicine, V 82 • 261-271 267 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

relationship between functional connectivity during the presenta-tion of high-calorie food and monetary decision making. There isevidence that adults with obesity engage discrete functional net-works when evaluating food cues as compared with monetaryrewards (22), a finding that is consistent with the patterns offunctional connectivity observed in the present study.
Functional Connectivity During the Processing ofHigh-Calorie Food Cues
Modulation of DMN ConnectivityMany of the regions that exhibited BMI-related increases in con-nectivity in the presence of high-calorie food cues are locatedwithin the DMN, including the precuneus, posterior cingulate gy-rus, medial temporal gyrus, and hippocampus. This was particu-larly the case when examining regional connectivity with theOFC, which is also a major hub of the DMN. The DMN supportsinternally guided and self-referential cognitive processes (51,52).Weight-related associations with task-induced connectivity to re-gions of the DMN may reflect more thorough engagement withand enhanced processing of high-calorie food cues that extends be-yond the experience of reward or pleasure, but may also includerecall of personal memories about food (e.g., sharing meals withfriends) and the affective states associated with these memories(see more hereinafter). Furthermore, elevated DMN activationduring moderately demanding cognitive tasks has been associatedwith poor task performance and attentional difficulties (53,54). Itis possible that increased engagement of the DMN in the presence
of food cues in overweight and adults with obesity may come atthe expense of optimal performance with higher cognitive de-mands. Additional research will be necessary to characterizethe cognitive and behavioral correlates of altered functionalconnectivity, including whether these patterns predict problem-atic eating behavior.
Involvement of the Hippocampus in Processingof Food CuesIn addition to increased coupling of the hippocampus with theOFC described previously, unique functional pathways linkingthe hippocampus to other regions of the brain were revealed whenusing this region as a seed. Body mass was associated with greaterhippocampal connectivity to the dmPFC, inferior frontal gyrus,and dorsolateral PFC in the presence of high-calorie food, an asso-ciation not previously reported. In the context of exposure to high-calorie food, increased signal coherence between the hippocampusand dorsolateral PFC may suggest that adults with obesity are notonly recalling food-related memories with strong affective content(as indicated by increased OFC-hippocampal connectivity) but alsomore thoroughly processing the details of these memories. Hippo-campal connectivity with the inferior frontal gyrus and dmPFC,two regions supporting working memory (55,56), may similarly re-flect enhanced processing of memories involving palatable food athigher body mass. These findings suggest that it may be importantto address the way in which an individual engages with cues associ-ated with unhealthy eating during weight loss treatment, perhaps by
TABLE 5. Indirect Effect of BMI on Overall IGT Performance and on Change in IGT Performance From the First to the Final Blockof the Task Operating Through Resting-State Seed-to-ROI Connectivity Values
B SE 95% ULCI 95% LLCI
Mediating effects on overall igt performance
Right orbitofrontal cortex
Left paracingulate gyrus −0.191 0.086 −0.402 −0.050Left ventromedial prefrontal cortex −0.178 0.090 −0.397 −0.037Medial posterior cingulate cortex −0.170 0.086 −0.377 −0.034Medial anterior cingulate cortex −0.108 0.064 −0.282 −0.017Right nucleus accumbens −0.232 0.092 −0.449 −0.075
Left dorsomedial prefrontal cortex
Right pallidum −0.178 0.099 −0.411 −0.021Mediating effects on change in IGT performance
Left lateral orbitofrontal cortex
Medial anterior cingulate cortex −0.345 0.181 −0.820 −0.081Left thalamus −0.022 0.010 −0.045 −0.005Right nucleus accumbens −0.283 0.168 −0.731 −0.036Right ventromedial prefrontal cortex −0.442 0.185 −0.861 −0.134
Right orbitofrontal cortex
Left ventromedial prefrontal cortex −0.266 0.160 −0.673 −0.030Left medial orbitofrontal cortex
Medial anterior cingulate cortex −0.212 0.145 −0.631 −0.021Right ventral striatum −0.407 0.187 −0.886 −0.130
BMI = body mass index; IGT = Iowa Gambling Task; LLCI = lower limit of confidence interval; ULCI = upper limit of confidence interval.
Confidence intervals were computed using bias-corrected bootstrapping with 5000 samples. Seeds with which ROI connectivity values were not associated with IGT performanceare not included in the table.
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 268 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

incorporating elements of cognitive behavioral therapy for bingeeating disorder (57).
Functional Connectivity at Rest
Disruption of Reward NetworksMany of the regions exhibiting BMI-related reductions in signalcoherence have been previously linked to reward valuation, deci-sion making, and reward-guided action selection, including theNAc, vmPFC, caudate, pallidum, putamen, amygdala, ACC, andparacingulate gyrus. Weakened functional integration of regionsinvolved in reward processing and reward-related decision makingin the absence of externally directed processing has been observedin multiple populations with impairments in reward-related deci-sionmaking (58–60). It is possible that reduced intrinsic functionalconnectivity between regions that support reward valuation, deci-sion making, and action selection may be indicative of impairedreward processing and contingency learning in overweight andobesity. Furthermore, given that weaker resting connectivity be-tween several of these regions was associated with impaired mon-etary decisionmaking, and that these patterns were not observed inthe presence of high-calorie food, it is possible that the observeddisruptions in functional connectivity reflect a generalized rewardprocessing deficit with increasing body mass.
Disruption of the DMNSignal coherence between regions of the DMN at rest was alsofound to be inversely associated with body mass, replicating find-ings reported by several previous studies (28,30,32). Reducedfunctional cohesion of the DMN at rest may lead to less effectiveintegration of signals from spatially distributed regions, and subse-quent dysregulation of processes dependent on such integration(32,51,52). It is possible that reduced functional connectivity inthis network leads to a diminished capacity to effectively plan andexecute new behaviors that would promote weight loss, and a con-sequent reliance on habitual yet unhealthy behaviors.
Intrinsic and Evoked Modulation of BasalGanglia ConnectivityHigher body mass was associated with differences in connectivitybetween the dmPFC and several regions of the basal ganglia, in-cluding the dorsal caudate nucleus, putamen, and pallidum, bothat rest and during the presentation of high-calorie food cues. ThedmPFC is involved in planning and selecting context-appropriatebehavioral responses thatmaximize the probability of goal attainment,including the receipt of a valued reward such as food (61–63). Assuch, it is possible that increased signal coherence between thedmPFC and regions of the basal ganglia during the processing ofhigh-calorie food cues may be indicative of a stronger tendencyto imagine physically interacting with the food as it is presented.This may be one mechanism through which food cues in the envi-ronment influence eating behavior, and may contribute to biasingof attention toward food cues in obesity (64,65).
In contrast, BMI was associated with weaker connectivity be-tween these regions at rest. Previous research has suggested thatfunctional interactions between the dmPFC and basal ganglia sup-port performance monitoring and flexible adjustment of behaviorto prevent future errors (66), and is also thought to promote the ac-quisition of action-outcome contingencies (67) necessary for the
execution of behaviors that lead to optimal outcomes. In the con-text of overweight and obesity, weaker signal coherence betweenthe dmPFC and the basal ganglia at rest may contribute to diffi-culty adopting healthy life-style behaviors and the failure to de-value high-calorie food despite the negative medical and socialconsequences associated with overconsumption of such foods. Itwill be important to examine whether dmPFC–basal ganglia con-nectivity predicts weight loss, as well as adherence to physical ac-tivity and dietary prescriptions.
SUMMARYAND CONCLUSIONSThere are several strengths of the present study, including a com-paratively large sample and a multimodal approach to examinethe associations between body mass and functional connectivity.Nevertheless, results should be interpreted in the context of severallimitations. One limitation is the use of a cross-sectional design,which precludes the ability to draw inferences about causality.To determine the temporal relationship between body mass andfunctional network organization, it will be necessary to use longi-tudinal approaches in future research. One such approach is to exam-ine how network-level signaling dynamics change after successfulweight loss (68–71). This experimental approach will provide someindication as to whether abnormal functional network architectureis a modifiable state marker of excess weight, or whether it repre-sents a stable characteristic of individuals who are prone to weightgain. Importantly, each of these possible outcomes has differentmechanistic implications and may yield alternative approaches totreatment and prevention.
Another important limitation of the current study is that, by de-sign, analyses were constrained to those networks exhibiting sig-nificant signal covariation with a relatively small number of seedregions, with the selection of seeds further being constrained by re-gional activation during a single task, albeit a highly disease rele-vant one. This approach was adopted to test specific mechanistichypotheses regarding the pathways underlying weight gain andweight maintenance. However, it is likely that obesity exerted aneffect on functional connectivity in other networks that were notassessed in the present study. Future studies may consider usinga combination of analytic approaches to simultaneously assess mul-tiple facets of network integrity. Relatedly, it is worth noting thatthere are alternative approaches to computing task-evoked connec-tivity (e.g., gPPI (72)) as well as for comparing task-evoked andresting-state connectivity (e.g., (73)). It is possible that the patternof results observed in the present study may have differed shouldanother approach have been used to compute task-evoked connec-tivity metrics, or to compare connectivity across task and restingstates. As such, it unclear to what extent the differences betweenpatterns of connectivity observed during the task and those ob-served during rest could be attributed to the analytical proceduresadopted in the present study. It has yet to be resolved which ana-lytic approach is most valid, highlighting the need for additionalresearch directly comparing each.
The present study was also limited by the exclusion of healthy-weight individuals. Although the results suggest that there are im-portant individual differences among adults with obesity that areobscured by the use of weight categories, it would be informativeto compare patterns of functional connectivity across the full rangeof BMI. Doing so may reveal important weight-related differences
Functional Connectivity in Obesity
Psychosomatic Medicine, V 82 • 261-271 269 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

in functional network organization that could have importantmechanistic implications regarding the transition from healthyweight to overweight or obese. Furthermore, we used traditionalapproaches for statistical thresholding of fMRI images, althoughrecent criticism of these approaches (74) suggests that it may beimportant in future work to apply other (e.g., nonparametric) ap-proaches for determining thresholds of fMRI data in the contextof obesity and weight loss. In addition, we did not standardizethe menstrual cycle phase in which we collected data from femaleparticipants, although there is evidence that circulating sex hor-mones influence indices of functional connectivity (75). Finally,the time elapsed between a participant’s last meal and their MRIvisit was not standardized across participants. Given that the inclusionof hunger ratings in statistical models did not modify the relationshipbetween BMI and indices of functional connectivity, it is unlikely thatsubjective reports of hunger account for the patterns of BMI-relatedfunctional connectivity. However, lack of information on meal timeleaves open the possibility that variation in circulating glucoseand insulin levels may have influenced reactivity to food cues.
To conclude, our results indicate that higher body mass is asso-ciated with altered functional connectivity of several networks.During the presentation of high-calorie food cues, higher bodymass was associated with greater functional connectivity betweenregions involved in reward valuation, contingency learning, mem-ory formation and recall, and self-referential cognitive processes.In contrast, higher body mass was associated with weaker restingconnectivity of the same seeds with regions that support rewardvaluation, decision making, and reward-guided action selection.This suggests that neural mechanisms underlying obesity may bemodulated by contextual factors. It is possible that the weight-related disruptions in connectivity observed in one context (e.g.,processing of high-calorie food cues) may contribute to deficits insome cognitive domains (e.g., attentional control) but not others.These findings may be leveraged to develop treatments that directlytarget the processes supported by these networks, a strategy that willideallymaximize treatment efficacy bymodifying the underlying neu-robiological systems. For example, there is growing interest in usingindices of brain function as a form of biofeedback to teach individualshow to develop volitional control over the function of regions and net-works that may be responding in suboptimal ways (76). Identificationof aberrant patterns of functional connectivity in obesity will informneurofeedback approaches to modifying network connectivity to sup-port weight loss efforts. This may represent a novel treatment approachto specifically target disruptions in self-regulation, reward-relateddecision making, and attentional biases for food that could be ap-plied in conjunction with more traditional behavioral weight lossinterventions. Furthermore, should future research find evidencethat differences in functional network architecture precede the de-velopment of obesity, it would suggest that these differences reflecta biomarker of risk for obesity that may be useful for identifyinghigh risk groups that would benefit from early intervention. Addi-tional research exploring the effect of obesity and weight loss onfunctional network organization will help further the developmentof innovative approaches to addressing obesity and related disease.
Source of Funding and Conflicts of Interest: J.M.J. received anhonorarium for serving on the Scientific Advisory Board forWeight Watchers International and was a coinvestigator on a
grant award to the University of Pittsburgh by Human Scale anda grant awarded to the University of Pittsburgh by WeightWatchers International. No other authors have conflicts of interestto report. This research was supported by the National Institutes ofHealth (R01-HL103646 and R01-DK095172), the National Sci-ence Foundation graduate research fellowship (DGE 124-7842[S.D.D.]), and the University of Pittsburgh Clinical and Transla-tional Science Institute (UL1 TR001857), which is supported bythe National Institutes of Health. The funding sources had no in-volvement in the study design, the collection, analysis, or interpre-tation of data; in the writing of the manuscript; or in the decisionto submit the manuscript for publication.
REFERENCES1. Schag K, Schönleber J, Teufel M, Zipfel S, Giel KE. Food-related impulsivity in
obesity and binge eating disorder—a systematic review: food-related impulsivity.Obes Rev 2013;14:477–95.
2. Yang Y, Shields GS, Guo C, Liu Y. Executive function performance in obesityand overweight individuals: a meta-analysis and review. Neurosci BiobehavRev 2018;84:225–44.
3. Batterink L, Yokum S, Stice E. Body mass correlates inversely with inhibitorycontrol in response to food among adolescent girls: an fMRI study. Neuroimage2010;52:1696–703.
4. Davis C, Patte K, Curtis C, Reid C. Immediate pleasures and future conse-quences. A neuropsychological study of binge eating and obesity. Appetite2010;54:208–13.
5. Gunstad J, Paul RH, Cohen RA, Tate DF, Spitznagel MB, Gordon E. Elevatedbody mass index is associated with executive dysfunction in otherwise healthyadults. Compr Psychiatry 2007;48:57–61.
6. Weller RE, Cook EW, Avsar KB, Cox JE. Obese women show greater delaydiscounting than healthy-weight women. Appetite 2008;51:563–9.
7. Nederkoorn C, Guerrieri R, Havermans RC, Roefs A, Jansen A. The interactiveeffect of hunger and impulsivity on food intake and purchase in a virtual super-market. Int J Obes (Lond) 2009;33:905–12.
8. Appelhans BM, Woolf K, Pagoto SL, Schneider KL, Whited MC, Liebman R.Inhibiting food reward: delay discounting, food reward sensitivity, and palatablefood intake in overweight and obese women. Obesity 2011;19:2175–82.
9. Will Crescioni A, Ehrlinger J, Alquist JL, Conlon KE, Schatschneider C, DuttonGR. High trait self-control predicts positive health behaviors and success inweight loss. J Health Psychol 2011;16:750–9.
10. Gerrits JH, O’Hara RE, Piko BF, Gibbons FX, de Ridder DT, Keresztes N,Kamble SV, de Wit JB. Self-control, diet concerns and eater prototypes influencefatty foods consumption of adolescents in three countries. Health Educ Res 2010;25:1031–41.
11. Wills TA, Isasi CR, Mendoza D, Ainette MG. Self-control constructs related tomeasures of dietary intake and physical activity in adolescents. J Adolesc Health2007;41:551–8.
12. Volkow ND, Wang GJ, Tomasi D, Baler RD. Obesity and addiction: neurobiologi-cal overlaps: overlaps between drug and food addiction. Obes Rev 2013;14:2–18.
13. Volkow ND, Baler RD. NOW vs LATER brain circuits: implications for obesityand addiction. Trends Neurosci 2015;38:345–52.
14. Kullmann S, Pape AA, Heni M, Ketterer C, Schick F, Häring HU, Fritsche A,Preissl H, Veit R. Functional network connectivity underlying food processing:disturbed salience and visual processing in overweight and obese adults. CerebCortex 2013;23:1247–56.
15. Giuliani NR, Mann T, Tomiyama AJ, Berkman ET. Neural systems underlyingthe reappraisal of personally craved foods. J Cogn Neurosci 2014;26:1390–402.
16. DemosKE, Heatherton TF, KelleyWM. Individual differences in nucleus accum-bens activity to food and sexual images predict weight gain and sexual behavior. JNeurosci 2012;32:5549–52.
17. Stice E, Yokum S, Blum K, Bohon C. Weight gain is associated with reducedstriatal response to palatable food. J Neurosci 2010;30:13105–9.
18. Stoeckel LE, Weller RE, Cook EW, Twieg DB, Knowlton RC, Cox JE. Wide-spread reward-system activation in obese women in response to pictures ofhigh-calorie foods. Neuroimage 2008;41:636–47.
19. Yokum S, Ng J, Stice E. Attentional bias to food images associated with elevatedweight and future weight gain: an fMRI study. Obesity 2011;19:1775–83.
20. Yokum S, Ng J, Stice E. Relation of regional gray and white matter volumes tocurrent BMI and future increases in BMI: a prospective MRI study. Int J Obes(Lond) 2012;36:656–64.
21. García-García I, Jurado MA, Garolera M, Segura B, Marqués-Iturria I, Pueyo R,Vernet-Vernet M, Sender-Palacios MJ, Sala-Llonch R, Ariza M, Narberhaus A,Junqué C. Functional connectivity in obesity during reward processing. Neuroimage2013;66:232–9.
ORIGINAL ARTICLE
Psychosomatic Medicine, V 82 • 261-271 270 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.

22. Verdejo-Román J, Fornito A, Soriano-Mas C, Vilar-López R, Verdejo-García A.Independent functional connectivity networks underpin food and monetary re-ward sensitivity in excess weight. Neuroimage 2017;146:293–300.
23. Geha P, Cecchi G, Todd Constable R, Abdallah C, Small DM. Reorganization ofbrain connectivity in obesity: obesity and altered brain connectivity. Hum BrainMapp 2017;38:1403–20.
24. Stoeckel LE, Kim J,Weller RE, Cox JE, Cook EW, Horwitz B. Effective connec-tivity of a reward network in obese women. Brain Res Bull 2009;79:388–95.
25. Dietrich A, HollmannM,Mathar D, Villringer A, Horstmann A. Brain regulationof food craving: relationships with weight status and eating behavior. Int J Obes(Lond) 2016;40:982–9.
26. Filbey FM, Yezhuvath US. A multimodal study of impulsivity and body weight:integrating behavioral, cognitive, and neuroimaging approaches: elevated bodyweight and impulsivity. Obesity 2017;25:147–54.
27. Tuulari JJ, Karlsson HK, Hirvonen J, Salminen P, Nuutila P, Nummenmaa L.Neural circuits for cognitive appetite control in healthy and obese individuals:an fMRI study. PLoS One 2015;10:e0116640.
28. Beyer F, Kharabian Masouleh S, Huntenburg JM, Lampe L, Luck T, Reidel-Heller SG, Loeffler M, Schroeter M, Stumvoll M, Villringer A, Witte AV. Higherbody mass index is associated with reduced posterior default mode connectivityin older adults: obesity and the default mode network in aging [published onlineApril 2017]. Hum Brain Mapp [online serial]. Available at: http://doi.wiley.com/10.1002/hbm.23605. Accessed January 16, 2019.
29. García-García I, Jurado MÁ, Garolera M, Segura B, Sala-Llonch R, Marqués-Iturria I, Pueyo R, Sender-Palacios MJ, Vernet-Vernet M, Narberhaus A, ArizaM, Junqué C. Alterations of the salience network in obesity: a resting-state fMRIstudy. Hum Brain Mapp 2013;34:2786–97.
30. Kullmann S, Heni M, Veit R, Ketterer C, Schick F, Häring HU, Fritsche A, PreisslH. The obese brain: association of body mass index and insulin sensitivity with rest-ing state network functional connectivity. Hum Brain Mapp 2012;33:1052–61.
31. Baek K,Morris LS, Kundu P, VoonV. Disrupted resting-state brain network prop-erties in obesity: decreased global and putaminal cortico-striatal network effi-ciency. Psychol Med 2017;47:585–96.
32. Doucet GE, Rasgon N, McEwen BS, Micali N, Frangou S. Elevated body massindex is associated with increased integration and reduced cohesion of sensory-driven and internally guided resting-state functional brain networks [published onlineJanuary 23, 2017]. Cereb Cortex [online serial]. Available at: https://academic.oup.com/cercor/article-lookup/doi/10.1093/cercor/bhx008. Accessed January 16, 2019.
33. Coveleskie K, Gupta A, Kilpatrick LA, Mayer ED, Ashe-McNalley C, Stains J,Labus JS, Mayer EA. Altered functional connectivity within the central rewardnetwork in overweight and obese women. Nutr Diabetes 2015;5:e148.
34. Frank S,Wilms B, Veit R, Ernst B, ThurnheerM, Kullmann S, Fritsche A, BirbaumerN, Preissl H, Schultes B. Altered brain activity in severely obese women may recoverafter Roux-en Y gastric bypass surgery. Int J Obes (Lond) 2014;38:341–8.
35. Legget KT, Wylie KP, Cornier MA, Melanson EL, Paschall CJ, Tregellas JR.Exercise-related changes in between-network connectivity in overweight/obeseadults. Physiol Behav 2016;158:60–7.
36. McFadden KL, Cornier M-A,Melanson EL, Bechtell JL, Tregellas JR. Effects ofexercise on resting-state default mode and salience network activity in overweight/obese adults. Neuroreport 2013;24:866–71.
37. Beaver JD. Individual differences in reward drive predict neural responses to im-ages of food. J Neurosci 2006;26:5160–6.
38. Killgore WDS, Young AD, Femia LA, Bogorodzki P, Rogowska J, Yurgelun-Todd DA. Cortical and limbic activation during viewing of high- versus low-calorie foods. Neuroimage 2003;19:1381–94.
39. Bechara A, Damasio H, Tranel D, Damasio AR. The Iowa Gambling Task andthe somatic marker hypothesis: some questions and answers. Trends Cogn Sci2005;9:159–62.
40. Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the ro-bust and accurate linear registration and motion correction of brain images.Neuroimage 2002;17:825–41.
41. Smith SM. Fast robust automated brain extraction. Hum Brain Mapp 2002;17:143–55.
42. JenkinsonM, Smith S. A global optimisationmethod for robust affine registrationof brain images. Med Image Anal 2001;5:143–56.
43. Andric M, Goldin-Meadow S, Small SL, Hasson U. Repeated movie viewingsproduce similar local activity patterns but different network configurations.Neuroimage 2016;142:613–27.
44. King DR, de Chastelaine M, Elward RL, Wang TH, Rugg MD. Recollection-related increases in functional connectivity predict individual differences in mem-ory accuracy. J Neurosci 2015;35:1763–72.
45. Gerchen MF, Kirsch P. Combining task-related activation and connectivity anal-ysis of fMRI data reveals complex modulation of brain networks: complex taskmodulation of brain networks. Hum Brain Mapp 2017;38:5726–39.
46. Friston KJ, Buechel C, Fink GR, Morris J, Rolls E, Dolan RJ. Psychophysiolog-ical and modulatory interactions in neuroimaging. Neuroimage 1997;6:218–29.
47. Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL.Neuroimage 2012;62:782–90.
48. Ciric R, Wolf DH, Power JD, Roalf DR, Baum GL, Ruparel K, Shinohara RT,ElliottMA, Eickhoff SB, Davatzikos C, Gur RC, Gur RE, Bassett DS, SatterthwaiteTD. Benchmarking of participant-level confound regression strategies for the
control of motion artifact in studies of functional connectivity. Neuroimage2017;154:174–87.
49. Hayes AF. PROCESS: A Versatile Computational Tool for Observed VariableMediation, Moderation, and Conditional Process Modeling. Lawrence, KS: Uni-versity of Kansas; 2012.
50. Hayes AF. Beyond Baron and Kenny: statistical mediation analysis in the newmillennium. Commun Monogr 2009;76:408–20.
51. Gu S, Satterthwaite TD, Medaglia JD, Yang M, Gur RE, Gur RC, Bassett DS.Emergence of system roles in normative neurodevelopment. Proc Natl AcadSci 2015;112:13681–6.
52. Vatansever D,Menon DK,ManktelowAE, Sahakian BJ, Stamatakis EA. Defaultmode dynamics for global functional integration. J Neurosci 2015;35:15254–62.
53. Fassbender C, Zhang H, BuzyWM, Cortes CR,Mizuiri D, Beckett L, SchweitzerJB. A lack of default network suppression is linked to increased distractibility inADHD. Brain Res 2009;1273:114–28.
54. Liddle EB, Hollis C, Batty MJ, GroomMJ, Totman JJ, Liotti M, Scerif G, LiddlePF. Task-related default mode network modulation and inhibitory control inADHD: effects of motivation and methylphenidate: default mode network mod-ulation in ADHD. J Child Psychol Psychiatry 2011;52:761–71.
55. Horst NK, Laubach M. The role of rat dorsomedial prefrontal cortex in spatialworking memory. Neuroscience 2009;164:444–56.
56. Liakakis G, Nickel J, Seitz RJ. Diversity of the inferior frontal gyrus—a meta-analysis of neuroimaging studies. Behav Brain Res 2011;225:341–7.
57. Agras WS, Telch CF, Arnow B, Eldredge K, Marnell M. One-year follow-up ofcognitive-behavioral therapy for obese individuals with binge eating disorder. JConsult Clin Psychol 1997;65:343–7.
58. Motzkin JC, Baskin-Sommers A, Newman JP, Kiehl KA,KoenigsM.Neural cor-relates of substance abuse: reduced functional connectivity between areas under-lying reward and cognitive control: neuropsychological correlates of SUD. HumBrain Mapp 2014;35:4282–92.
59. Wilcox CE, Pommy JM, Adinoff B. Neural circuitry of impaired emotion regula-tion in substance use disorders. Am J Psychiatry 2016;173:344–61.
60. Yuan K,Yu D, Cai C, FengD, Li Y, Bi Y, Liu J, Zhang Y, Jin C, Li L, QinW, TianJ. Frontostriatal circuits, resting state functional connectivity and cognitive con-trol in internet gaming disorder. Addict Biol 2017;22:813–22.
61. Fuchs RA, Evans KA, Ledford CC, ParkerMP, Case JM,Mehta RH, See RE. Therole of the dorsomedial prefrontal cortex, basolateral amygdala, and dorsal hippocam-pus in contextual reinstatement of cocaine seeking in rats. Neuropsychopharmacology2005;30:296–309.
62. JaffardM, LongcampM,Velay JL, Anton JL, RothM,Nazarian B, Boulinguez P.Proactive inhibitory control of movement assessed by event-related fMRI.Neuroimage 2008;42:1196–206.
63. Narayanan NS, Laubach M. Top-down control of motor cortex ensembles bydorsomedial prefrontal cortex. Neuron 2006;52:921–31.
64. Castellanos EH, Charboneau E, Dietrich MS, Park S, Bradley BP, Mogg K,CowanRL. Obese adults have visual attention bias for food cue images: evidencefor altered reward system function. Int J Obes (Lond) 2009;33:1063–73.
65. Werthmann J, Roefs A, Nederkoorn C, Mogg K, Bradley BP, Jansen A. Can(not)take my eyes off it: attention bias for food in overweight participants. HealthPsychol 2011;30:561–9.
66. Ullsperger M, Fischer AG, Nigbur R, Endrass T. Neural mechanisms and tempo-ral dynamics of performance monitoring. Trends Cogn Sci 2014;18:259–67.
67. Kim BK, Shin MS, Kim CJ, Baek SB, Ko YC, Kim YP. Treadmill exercise im-proves short-term memory by enhancing neurogenesis in amyloid beta-inducedAlzheimer disease rats. J Exerc Rehabil 2014;10:2–8.
68. Hinkle W, Cordell M, Leibel R, Rosenbaum M, Hirsch J. Effects of reducedweight maintenance and leptin repletion on functional connectivity of the hypo-thalamus in obese humans. PLoS One 2013;8:e59114.
69. Lepping RJ, Bruce AS, FranciscoA,YehHW,Martin LE, Powell JN, Hancock L,Patrician TM, Breslin FJ, Selim N, Donnelly JE, Brooks WM, Savage CR,Simmons WK, Bruce JM. Resting-state brain connectivity after surgical and be-havioral weight loss: weight loss brain connectivity. Obesity 2015;23:1422–8.
70. Tregellas JR, Wylie KP, Rojas DC, Tanabe J, Martin J, Kronberg E, Cordes D,Cornier MA. Altered default network activity in obesity. Obesity 2011;19:2316–21.
71. Weygandt M,Mai K, Dommes E, Leupelt V, Hackmack K, Kahnt T, RothemundY, Spranger J, Haynes JD. The role of neural impulse control mechanisms for di-etary success in obesity. Neuroimage 2013;83:669–78.
72. McLaren DG, Ries ML, Xu G, Johnson SC. A generalized form of context-dependent psychophysiological interactions (gPPI): a comparison to standard ap-proaches. Neuroimage 2012;61:1277–86.
73. Cole MW, Bassett DS, Power JD, Braver TS, Petersen SE. Intrinsic and task-evoked network architectures of the human brain. Neuron 2014;83:238–51.
74. EklundA, Nichols TE, KnutssonH. Cluster failure: why fMRI inferences for spa-tial extent have inflated false-positive rates. ProcNatl Acad Sci 2016;113:7900–5.
75. Peper JS, van denHeuvelMP,Mandl RC, PolHE, vanHonk J. Sex steroids and connec-tivity in the human brain: a review of neuroimaging studies. Psychoneuroendocrinology2011;36:1101–13.
76. Kohl SH, Veit R, Spetter MS, Günther A, Rina A, LührsM, Birbaumer N, PreisslH, Hallschmid M. Real-time fMRI neurofeedback training to improve eating be-havior by self-regulation of the dorsolateral prefrontal cortex: a randomized con-trolled trial in overweight and obese subjects. Neuroimage 2019;191:596–609.
Functional Connectivity in Obesity
Psychosomatic Medicine, V 82 • 261-271 271 April 2020
Copyright © 2020 by the American Psychosomatic Society. Unauthorized reproduction of this article is prohibited.