Embed Size (px)
Citation preview
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Comparison of Intraoral Donor Sites for Onlay Grafting Prior to Implant PlacementCraig M. Misch, DDS, MDS
Fifty patients with inadequate bone volume for implant placement were treated with mandibular bone grafts from the symphysis or ramus. The choice of donor site was determined by defect morphology and recipient site location. Although the harvest of bone was associated with low morbidity, the ramus donor site resulted in fewer complications. Implants were placed secondarily following a 4- to 6-month healing period. The onlay grafts exhibited minimal resorption and maintained their dense quality. The symphysis grafts were larger in overall volume, with a corticocancellous morphology. The ramus area provided essentially a cortical graft that was well suited for veneering ridge deficiencies; however, the surgical access in some cases was more difficult than in the anterior mandible. (INT J ORAL MAXILLOFAC IMPLANTS 1997;12:767–776)
Key words: autogenous bone grafting, mandibular bone grafts, ramus, symphysis
A primary diagnostic consideration for implant prostheses is the amount of bone available in edentulous areas. The placement of endosseous dental implants for prosthetic support requires adequate bone volume at the desired locations. If bone volume is inadequate, several surgical techniques may be used to reconstruct the deficient ridge for implant placement. The morphology of a bony defect is an important consideration in the selection of a method for ridge augmentation. The fewer the number of remaining bony walls, the greater the need for osteopromotive techniques. Although allografts and guided bone regeneration techniques have been used in bone repair, these methods have limitations and have been found to produce less favorable results in the treatment of larger bone deficiencies.1-10 Autologous bone grafts continue to represent the gold standard in the repair of alveolar atrophy and bone defects.11-15
The use of autologous bone grafts with osseointegrated implants was originally discussed by Brånemark et al,16 and it is now a well-accepted procedure in oral and maxillofacial rehabilitation.17 Although the iliac crest is used most often in major jaw reconstruction for implants,18-21 various other donor sites have been investigated. Local bone grafts from the maxilla and mandible have also been described.22-34 The obvious advantage of local grafts is their convenient surgical access.27,35,36 The close proximity of donor and recipient sites can reduce operative and anesthesia time, making them ideal for outpatient implant surgery. In addition,
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
patients report minimal discomfort, and these areas may offer decreased morbidity from graft harvest.24,27,31,34,36
Mandibular bone grafts have been used for alveolar repair to allow implant placement with extremely favorable results.22-24,26-31,34,36-40 Block-type grafts may be harvested from the mandibular symphysis, body, or ramus area. However, the different anatomies of these regions result in different graft morphologies. A clinical evaluation and comparison of intraoral harvest sites for grafting prior to implant placement is presented.
Materials and MethodsFifty patients scheduled for implant prostheses presented with inadequate bone volume for implant placement. Clinical and radiographic examinations were performed to evaluate the bone graft donor sites. The choice of donor site, either symphysis or ramus, was determined preoperatively based on defect morphology and recipient site location. A panoramic radiograph was used to map the course of the inferior alveolar canal. Lateral cephalometric, posterior-anterior projections, and periapical radiographs were also used when necessary to assess the donor sites. The recipient site was completely healed prior to graft surgery. Tooth extractions were completed at least 8 weeks before grafting. A surgical template to guide placement of the grafts was used in cases involving restoration of the anterior maxilla.
Surgical Techniques. The surgical techniques for procuring bone grafts from the symphysis and ramus areas have been described previously.27,34 All patients were treated under intravenous or oral conscious sedation. Mandibular nerve blocks with 0.5% bupivacaine containing 1:200,000 epinephrine were used for local anesthesia of the donor sites. Local infiltration of the donor and recipient sites with 2% lidocaine, containing 1:100,000 epinephrine, was also used for hemostasis. At least 1 hour prior to surgery, either 1 g of amoxicillin or, if penicillin allergic, 300 mg of clindamycin was administered to patients. Antibiotic coverage was continued for 1 week postoperatively. A 3-day tapering dose of dexamethasone was used starting the day of surgery. Narcotic analgesics were prescribed to manage postoperative pain.
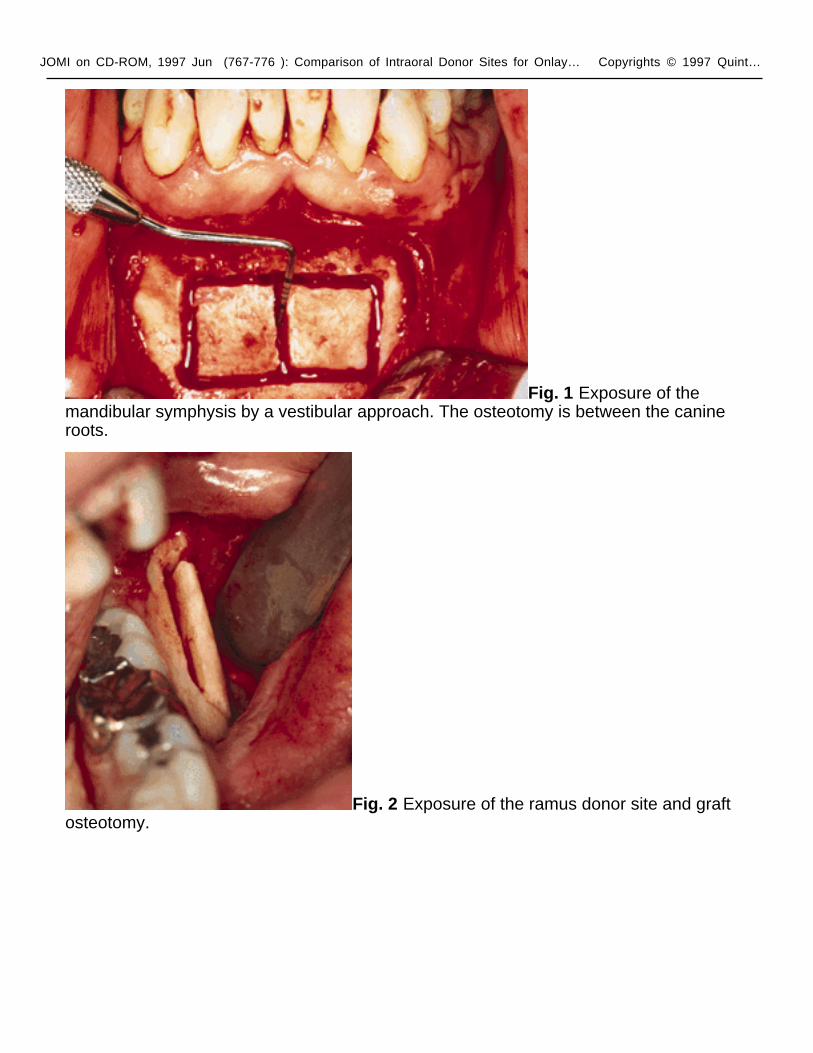
Symphysis Donor Site. Access to the symphysis was obtained via a vestibular incision or sulcular approach (Fig 1). The vestibular incision was made in the mucosa between the canine teeth areas at least 1 cm beyond the mucogingival junction. The mucoperiosteal flap was reflected toward the base of the mandible to the level of pogonion, leaving the most facial aspect of the periosteal attachment intact. After the symphysis was exposed, the osteotomy for graft harvest was planned. Dimensions of the block were determined by the size of the bone defect. The osteotomies were performed with a fissure bur in a surgical handpiece under copious saline irrigation. The superior osteotomy was made at least 5 mm below the tooth apices and the inferior cortex of the mandible was maintained. The depth of the osteotomies extended completely through the outer cortex. A bone chisel was tapped
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
along the osteotomy, with the exception of the inferior border, to deliver the graft. Additional cancellous bone was procured with a rongeur or chisel. Bone wax or hemostatic dressing (collagen or gelatin sponge) was placed into areas of heavy osseous bleeding after bone harvest, and the area was then implanted with resorbable hydroxyapatite. The soft tissue superior to the initial incision was elevated to reduce tension on the flap from edema, and a two-layered closure was used.
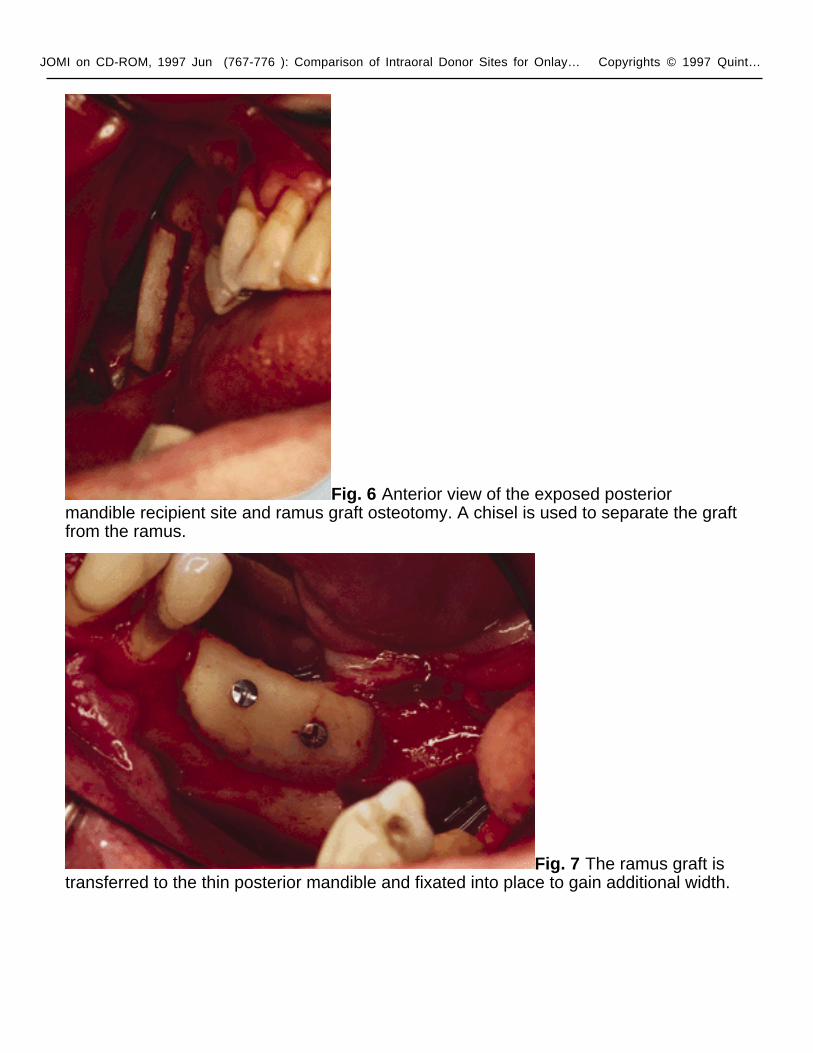
Ramus Donor Site. To access the ramus area, an incision was made in the buccal vestibule medial to the external oblique ridge. It extended anteriorly and lateral to the retromolar pad and into the buccal sulcus of the molar teeth or posterior ridge area. A mucoperiosteal flap was reflected from the mandibular body, exposing the lateral aspect of the ramus. The flap was elevated superiorly along the external oblique ridge to the base of the coronoid process with a notched ramus retractor. The osteotomy was started anterior to the coronoid process at a point where adequate bone thickness developed. A small fissure bur in a straight handpiece was used to cut through the cortex along the anterior border of the ramus medial to the external oblique ridge (Fig 2). The anterior vertical cut was made in the mandibular body in the molar region. The length of this cut was dependent on the size requirements of the graft and on the position of the inferior alveolar canal. The posterior vertical cut was made on the lateral aspect of the ramus, perpendicular to the external oblique osteotomy. The inferior osteotomy connecting the posterior and anterior vertical cuts was made with a round bur in a straight handpiece. This was a shallow cut into the ramus to create a line of fracture. A thin chisel was gently tapped along the entire length of the external oblique osteotomy, and care was taken to parallel the lateral surface of the ramus. A wider wedge chisel was then inserted and levered to pry the buccal segment free and complete the splitting of the graft from the ramus. Following removal of the bone, sharp edges around the ramus were smoothed with a bur or file. Bone wax or a hemostatic dressing (collagen or gelatin sponge) was placed into the donor area and closure of the wound was completed following graft fixation.
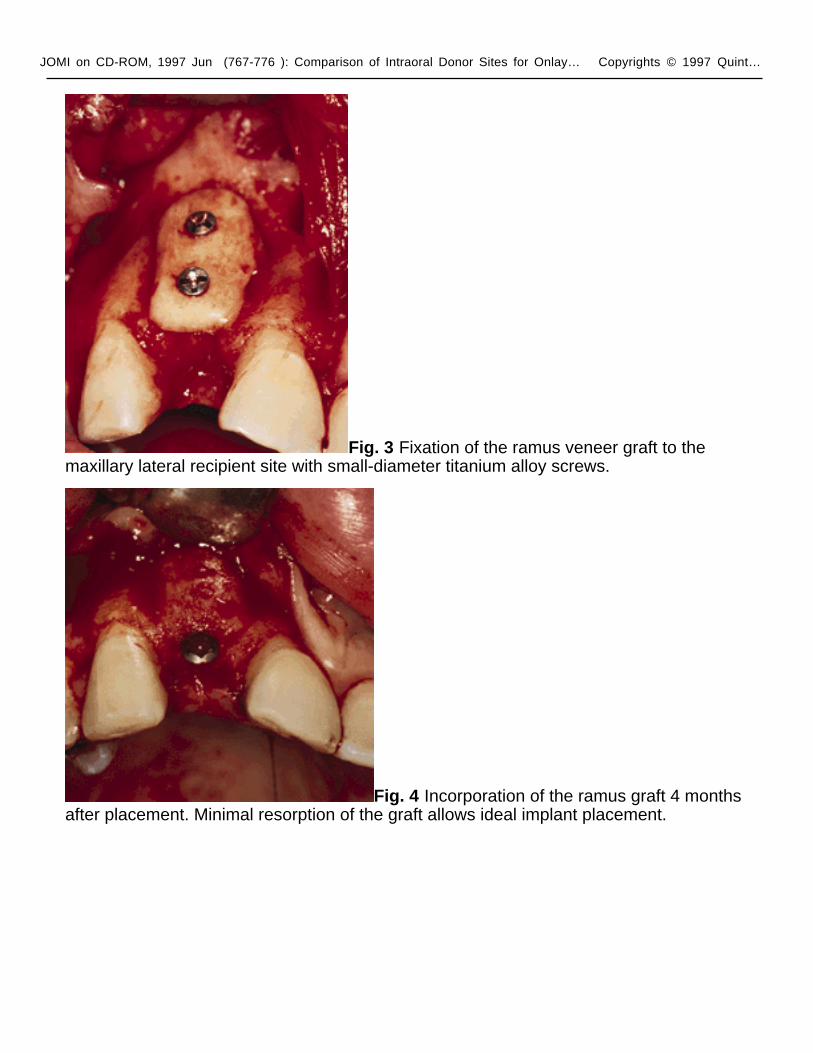
Recipient Site. The proposed recipient site for the graft was exposed prior to graft harvest in all cases. In this manner, the dimensions and morphology of the bony defect were measured, and minimal time elapsed between graft harvest and placement. Incisions slightly distant from the residual ridge crest (facial mandible, palatal maxilla) and divergent releasing incisions remote to the defect were used to facilitate closure and maintain blood supply. The recipient sites were recontoured when necessary to improve bone-to-graft contact. The underlying host bone was also perforated with a small round bur. The block grafts were fixed with small-diameter titanium alloy screws (Osteomed, Irving, TX) (Fig 3). The periosteum at the base of the flap was carefully incised to allow stretching of the mucosa and tension-free adaptation of the wound margins. Removable, soft tissue–supported prostheses were generously adjusted and relined with tissue conditioner. Patients were instructed to use their prostheses for cosmetic appearance rather than for function. The grafted

JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
sites were allowed to heal for 4 to 6 months. At that time patients were scheduled for implant surgery (Fig 4).
Clinical evaluation included graft size and morphology assessed at bone procurement, postoperative complications associated with graft harvest, incorporation and resorption following graft healing, bone quality of the healed graft, and implant placement in the grafted sites. Block graft size was measured following removal from the donor site. The morphology was grossly assessed as cortical or corticocancellous. Postoperative complications were evaluated during the healing phase and included donor incision dehiscence, nerve paresthesia, donor site infection, and complaints of altered sensation of teeth proximal to the graft. Following the 4- to 6-month healing phase, flaps were reflected for implant placement and bone resorption was measured at the fixation screw heads and at the ridge crest. Graft incorporation was evaluated following removal of the fixation screws. Bone quality was assessed during drilling of the implant osteotomy sites. The bone quality classification ranking of types one through four, as proposed by Lekholm and Zarb41 and described by Misch,42 was recorded. Ideal implant sites were diagnosed preoperatively, and successful augmentation was determined by implant placement.
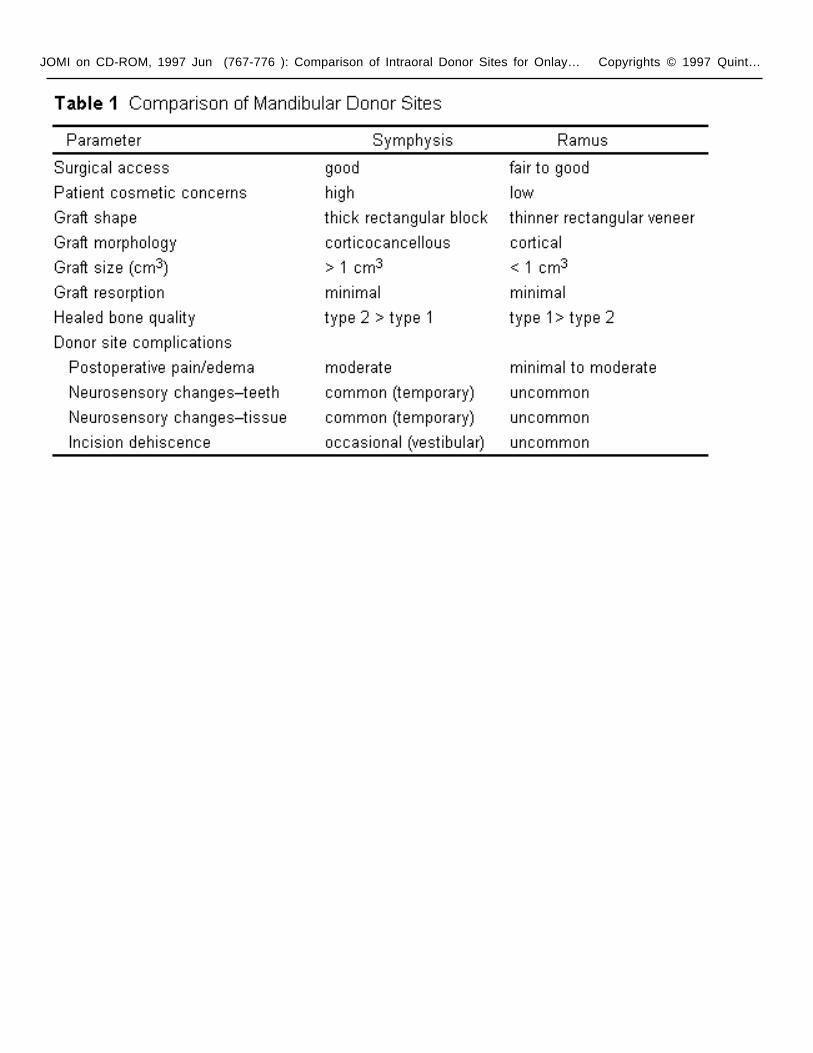
ResultsA comparison of graft sizes (Table 1) revealed that the overall volume from the symphysis was largest (1.74 cm3 versus 0.9 cm3). Onlay graft morphology from the symphysis was corticocancellous; block grafts from the ramus were more cortical. Incision dehiscence occurred in 10.7% (3/28) of the patients, with a vestibular approach to the anterior mandible. Two of the patients with symphyseal dehiscence developed infection of the grafted donor site. No incision-line dehiscence or infection occurred in the ramus graft group or with symphysis grafts harvested through a sulcular approach (3/31). The incidence of temporary mental nerve paresthesia in symphysis graft patients was 9.6% (3/31). No soft tissue sensory deficits were noted by ramus graft patients. Twenty-nine percent (9/31) of symphysis graft patients described altered sensation of the incisor teeth. None of the ramus graft patients noted changes in their molar teeth. All 50 of the block onlay grafts incorporated, and there was no significant clinical difference noted in resorption between graft types. The resorption rate ranged from undetectable to approximately 25%. Bone quality of the sites was more often graded as quality one for the ramus (11/19) and quality two for the symphysis (19/31). None of the grafted sites was noted as quality three or four. Implants were successfully placed in all planned sites (24 ramus, 61 symphysis).
DiscussionLocal grafts from the mandible are a convenient source of autogenous bone for alveolar reconstruction. In addition, bone harvested from the mandible appears to have inherent biologic benefits, which have been attributed to its embryologic origin.43 46
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
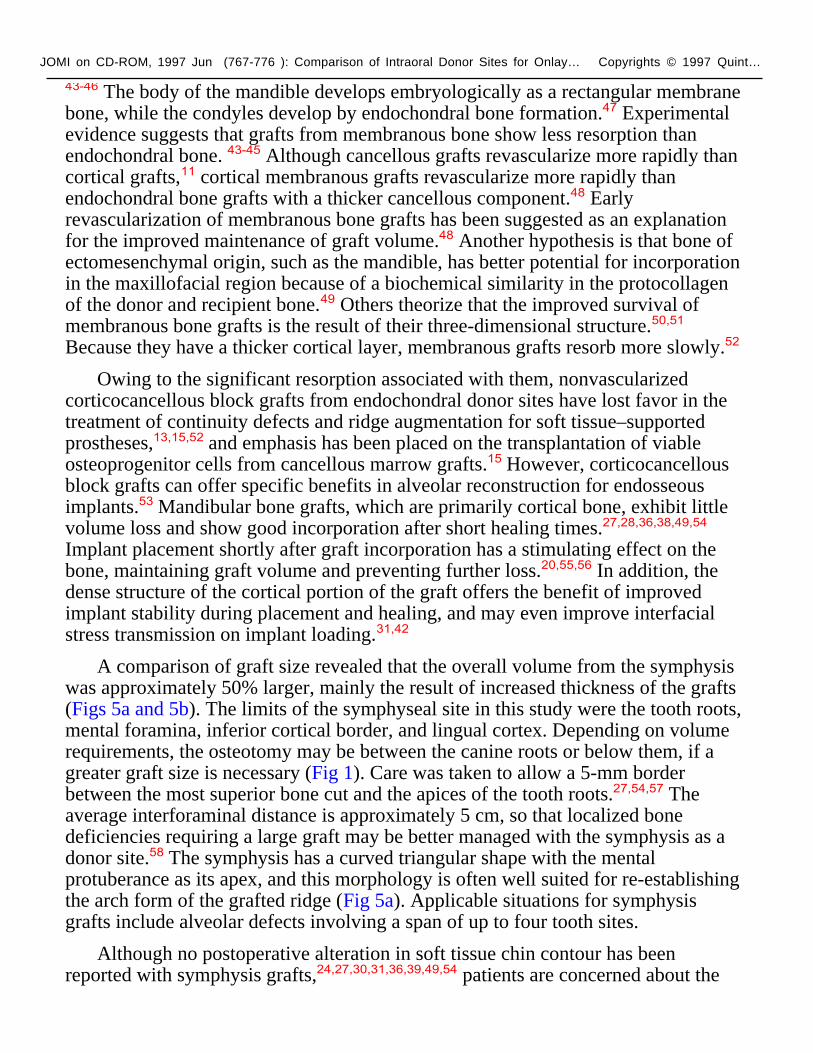
43-46 The body of the mandible develops embryologically as a rectangular membrane bone, while the condyles develop by endochondral bone formation.47 Experimental evidence suggests that grafts from membranous bone show less resorption than endochondral bone. 43-45 Although cancellous grafts revascularize more rapidly than cortical grafts,11 cortical membranous grafts revascularize more rapidly than endochondral bone grafts with a thicker cancellous component.48 Early revascularization of membranous bone grafts has been suggested as an explanation for the improved maintenance of graft volume.48 Another hypothesis is that bone of ectomesenchymal origin, such as the mandible, has better potential for incorporation in the maxillofacial region because of a biochemical similarity in the protocollagen of the donor and recipient bone.49 Others theorize that the improved survival of membranous bone grafts is the result of their three-dimensional structure.50,51 Because they have a thicker cortical layer, membranous grafts resorb more slowly.52
Owing to the significant resorption associated with them, nonvascularized corticocancellous block grafts from endochondral donor sites have lost favor in the treatment of continuity defects and ridge augmentation for soft tissue–supported prostheses,13,15,52 and emphasis has been placed on the transplantation of viable osteoprogenitor cells from cancellous marrow grafts.15 However, corticocancellous block grafts can offer specific benefits in alveolar reconstruction for endosseous implants.53 Mandibular bone grafts, which are primarily cortical bone, exhibit little volume loss and show good incorporation after short healing times.27,28,36,38,49,54 Implant placement shortly after graft incorporation has a stimulating effect on the bone, maintaining graft volume and preventing further loss.20,55,56 In addition, the dense structure of the cortical portion of the graft offers the benefit of improved implant stability during placement and healing, and may even improve interfacial stress transmission on implant loading.31,42
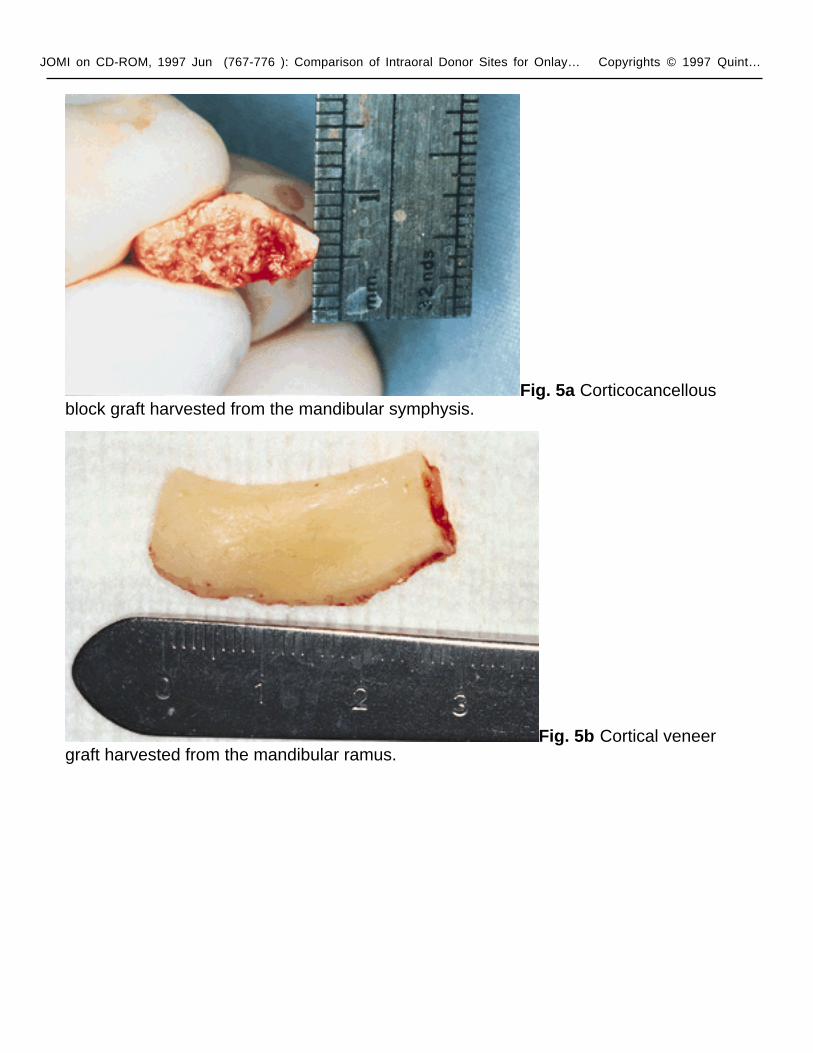
A comparison of graft size revealed that the overall volume from the symphysis was approximately 50% larger, mainly the result of increased thickness of the grafts (Figs 5a and 5b). The limits of the symphyseal site in this study were the tooth roots, mental foramina, inferior cortical border, and lingual cortex. Depending on volume requirements, the osteotomy may be between the canine roots or below them, if a greater graft size is necessary (Fig 1). Care was taken to allow a 5-mm border between the most superior bone cut and the apices of the tooth roots.27,54,57 The average interforaminal distance is approximately 5 cm, so that localized bone deficiencies requiring a large graft may be better managed with the symphysis as a donor site.58 The symphysis has a curved triangular shape with the mental protuberance as its apex, and this morphology is often well suited for re-establishing the arch form of the grafted ridge (Fig 5a). Applicable situations for symphysis grafts include alveolar defects involving a span of up to four tooth sites.
Although no postoperative alteration in soft tissue chin contour has been reported with symphysis grafts,24,27,30,31,36,39,49,54 patients are concerned about the
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
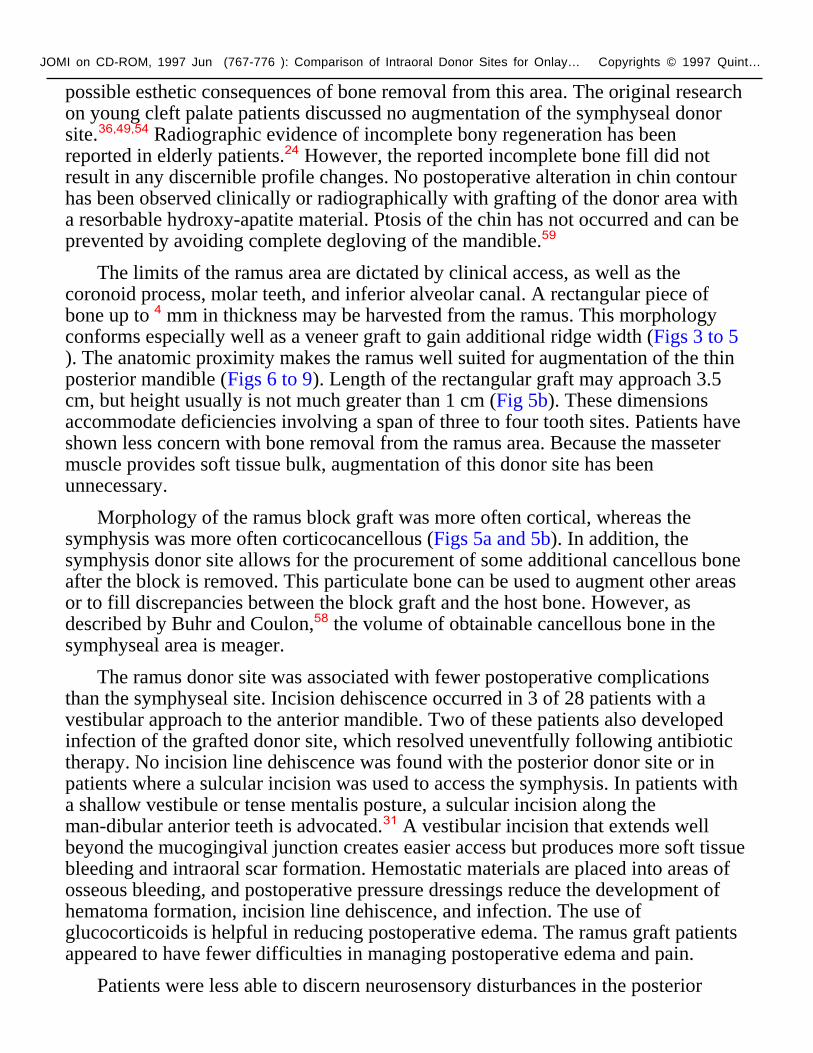
possible esthetic consequences of bone removal from this area. The original research on young cleft palate patients discussed no augmentation of the symphyseal donor site.36,49,54 Radiographic evidence of incomplete bony regeneration has been reported in elderly patients.24 However, the reported incomplete bone fill did not result in any discernible profile changes. No postoperative alteration in chin contour has been observed clinically or radiographically with grafting of the donor area with a resorbable hydroxy-apatite material. Ptosis of the chin has not occurred and can be prevented by avoiding complete degloving of the mandible.59
The limits of the ramus area are dictated by clinical access, as well as the coronoid process, molar teeth, and inferior alveolar canal. A rectangular piece of bone up to 4 mm in thickness may be harvested from the ramus. This morphology conforms especially well as a veneer graft to gain additional ridge width (Figs 3 to 5). The anatomic proximity makes the ramus well suited for augmentation of the thin posterior mandible (Figs 6 to 9). Length of the rectangular graft may approach 3.5 cm, but height usually is not much greater than 1 cm (Fig 5b). These dimensions accommodate deficiencies involving a span of three to four tooth sites. Patients have shown less concern with bone removal from the ramus area. Because the masseter muscle provides soft tissue bulk, augmentation of this donor site has been unnecessary.
Morphology of the ramus block graft was more often cortical, whereas the symphysis was more often corticocancellous (Figs 5a and 5b). In addition, the symphysis donor site allows for the procurement of some additional cancellous bone after the block is removed. This particulate bone can be used to augment other areas or to fill discrepancies between the block graft and the host bone. However, as described by Buhr and Coulon,58 the volume of obtainable cancellous bone in the symphyseal area is meager.
The ramus donor site was associated with fewer postoperative complications than the symphyseal site. Incision dehiscence occurred in 3 of 28 patients with a vestibular approach to the anterior mandible. Two of these patients also developed infection of the grafted donor site, which resolved uneventfully following antibiotic therapy. No incision line dehiscence was found with the posterior donor site or in patients where a sulcular incision was used to access the symphysis. In patients with a shallow vestibule or tense mentalis posture, a sulcular incision along the man-dibular anterior teeth is advocated.31 A vestibular incision that extends well beyond the mucogingival junction creates easier access but produces more soft tissue bleeding and intraoral scar formation. Hemostatic materials are placed into areas of osseous bleeding, and postoperative pressure dressings reduce the development of hematoma formation, incision line dehiscence, and infection. The use of glucocorticoids is helpful in reducing postoperative edema. The ramus graft patients appeared to have fewer difficulties in managing postoperative edema and pain.
Patients were less able to discern neurosensory disturbances in the posterior
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
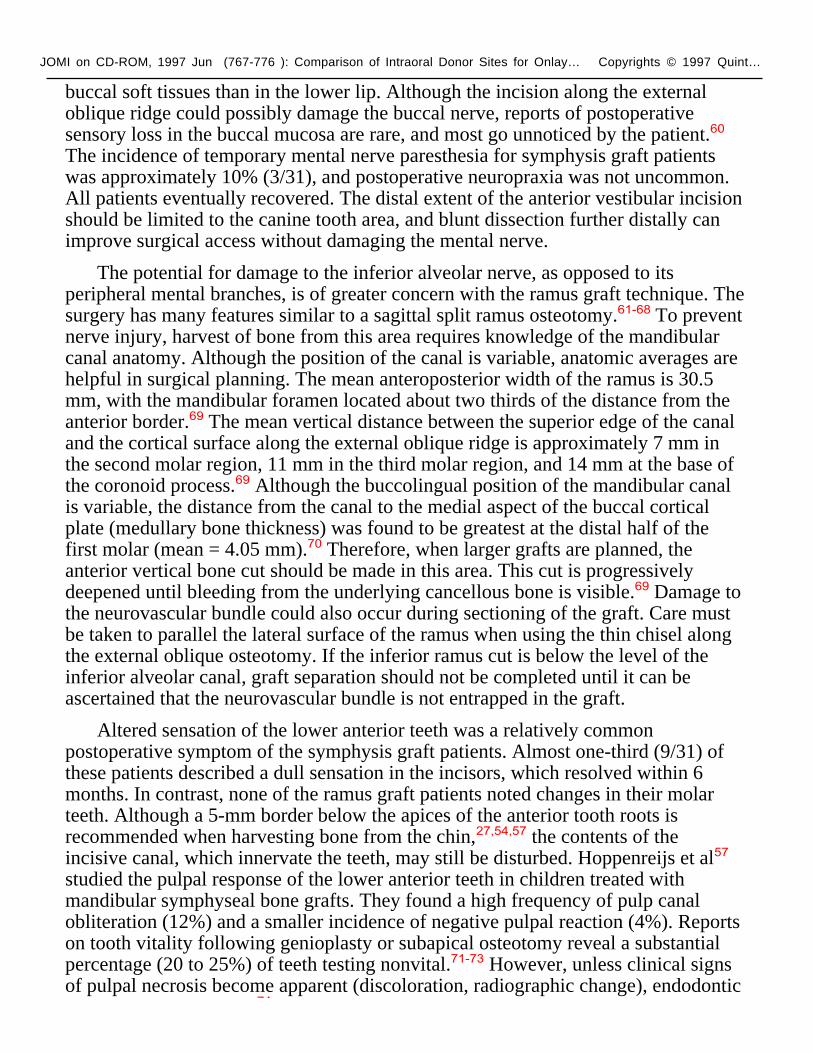
buccal soft tissues than in the lower lip. Although the incision along the external oblique ridge could possibly damage the buccal nerve, reports of postoperative sensory loss in the buccal mucosa are rare, and most go unnoticed by the patient.60 The incidence of temporary mental nerve paresthesia for symphysis graft patients was approximately 10% (3/31), and postoperative neuropraxia was not uncommon. All patients eventually recovered. The distal extent of the anterior vestibular incision should be limited to the canine tooth area, and blunt dissection further distally can improve surgical access without damaging the mental nerve.
The potential for damage to the inferior alveolar nerve, as opposed to its peripheral mental branches, is of greater concern with the ramus graft technique. The surgery has many features similar to a sagittal split ramus osteotomy.61-68 To prevent nerve injury, harvest of bone from this area requires knowledge of the mandibular canal anatomy. Although the position of the canal is variable, anatomic averages are helpful in surgical planning. The mean anteroposterior width of the ramus is 30.5 mm, with the mandibular foramen located about two thirds of the distance from the anterior border.69 The mean vertical distance between the superior edge of the canal and the cortical surface along the external oblique ridge is approximately 7 mm in the second molar region, 11 mm in the third molar region, and 14 mm at the base of the coronoid process.69 Although the buccolingual position of the mandibular canal is variable, the distance from the canal to the medial aspect of the buccal cortical plate (medullary bone thickness) was found to be greatest at the distal half of the first molar (mean = 4.05 mm).70 Therefore, when larger grafts are planned, the anterior vertical bone cut should be made in this area. This cut is progressively deepened until bleeding from the underlying cancellous bone is visible.69 Damage to the neurovascular bundle could also occur during sectioning of the graft. Care must be taken to parallel the lateral surface of the ramus when using the thin chisel along the external oblique osteotomy. If the inferior ramus cut is below the level of the inferior alveolar canal, graft separation should not be completed until it can be ascertained that the neurovascular bundle is not entrapped in the graft.
Altered sensation of the lower anterior teeth was a relatively common postoperative symptom of the symphysis graft patients. Almost one-third (9/31) of these patients described a dull sensation in the incisors, which resolved within 6 months. In contrast, none of the ramus graft patients noted changes in their molar teeth. Although a 5-mm border below the apices of the anterior tooth roots is recommended when harvesting bone from the chin,27,54,57 the contents of the incisive canal, which innervate the teeth, may still be disturbed. Hoppenreijs et al57 studied the pulpal response of the lower anterior teeth in children treated with mandibular symphyseal bone grafts. They found a high frequency of pulp canal obliteration (12%) and a smaller incidence of negative pulpal reaction (4%). Reports on tooth vitality following genioplasty or subapical osteotomy reveal a substantial percentage (20 to 25%) of teeth testing nonvital.71-73 However, unless clinical signs of pulpal necrosis become apparent (discoloration, radiographic change), endodontic
74
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
therapy is not indicated.74 Although the need for endodontic therapy has not arisen, and the risk of damage to the teeth is minimal, patients should be aware of the potential for pathologic changes.
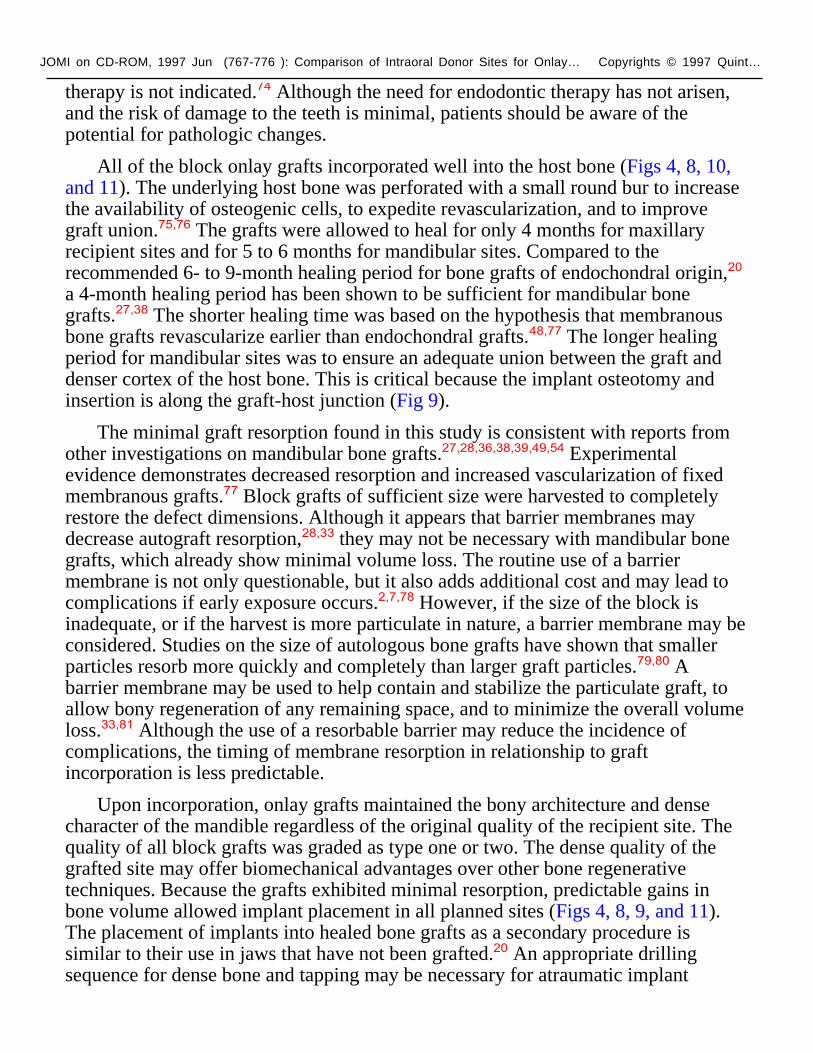
All of the block onlay grafts incorporated well into the host bone (Figs 4, 8, 10, and 11). The underlying host bone was perforated with a small round bur to increase the availability of osteogenic cells, to expedite revascularization, and to improve graft union.75,76 The grafts were allowed to heal for only 4 months for maxillary recipient sites and for 5 to 6 months for mandibular sites. Compared to the recommended 6- to 9-month healing period for bone grafts of endochondral origin,20 a 4-month healing period has been shown to be sufficient for mandibular bone grafts.27,38 The shorter healing time was based on the hypothesis that membranous bone grafts revascularize earlier than endochondral grafts.48,77 The longer healing period for mandibular sites was to ensure an adequate union between the graft and denser cortex of the host bone. This is critical because the implant osteotomy and insertion is along the graft-host junction (Fig 9).
The minimal graft resorption found in this study is consistent with reports from other investigations on mandibular bone grafts.27,28,36,38,39,49,54 Experimental evidence demonstrates decreased resorption and increased vascularization of fixed membranous grafts.77 Block grafts of sufficient size were harvested to completely restore the defect dimensions. Although it appears that barrier membranes may decrease autograft resorption,28,33 they may not be necessary with mandibular bone grafts, which already show minimal volume loss. The routine use of a barrier membrane is not only questionable, but it also adds additional cost and may lead to complications if early exposure occurs.2,7,78 However, if the size of the block is inadequate, or if the harvest is more particulate in nature, a barrier membrane may be considered. Studies on the size of autologous bone grafts have shown that smaller particles resorb more quickly and completely than larger graft particles.79,80 A barrier membrane may be used to help contain and stabilize the particulate graft, to allow bony regeneration of any remaining space, and to minimize the overall volume loss.33,81 Although the use of a resorbable barrier may reduce the incidence of complications, the timing of membrane resorption in relationship to graft incorporation is less predictable.
Upon incorporation, onlay grafts maintained the bony architecture and dense character of the mandible regardless of the original quality of the recipient site. The quality of all block grafts was graded as type one or two. The dense quality of the grafted site may offer biomechanical advantages over other bone regenerative techniques. Because the grafts exhibited minimal resorption, predictable gains in bone volume allowed implant placement in all planned sites (Figs 4, 8, 9, and 11). The placement of implants into healed bone grafts as a secondary procedure is similar to their use in jaws that have not been grafted.20 An appropriate drilling sequence for dense bone and tapping may be necessary for atraumatic implant

JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
placement.
Reports on simultaneous bone grafting and implant placement have revealed complications such as graft fracture and wound dehiscence with exposure of implants and graft, with a higher implant failure rate than that of a staged approach.23,24,27,28,30,36,40 In addition, diminished bone contact has been found around titanium implants placed simultaneously with autologous grafts.10,18,82 A staged surgery permits implant placement for ideal prosthetic alignment without the concern of graft fixation or remodeling (Figs 8 and 11). Staged implant placement also allows for any initial graft resorption and thus should provide a more stable foundation.56
ConclusionAutogenous bone grafts harvested from the mandible offer several advantages in the reconstruction of alveolar ridges for implant placement. These grafts require a short healing period and exhibit minimal resorption, while maintaining their dense quality. The ramus area has some advantages over the mandibular symphysis as a donor site (Table 1). These include minimal patient concern for altered facial contour, lower incidence of incision dehiscence, decreased complaints of postoperative sensory disturbance, and proximity to posterior mandible recipient sites. However, surgical access in some patients is more difficult, and there are limitations to the size and shape of the graft. The symphysis offers the potential for thicker grafts with an increased cancellous component.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
1. Collins T, Small S, Shepard N, Buser D, Parel S. Sinus-floor elevations and the status of membranes. Int J Oral Maxillofac Implants 1994;9(suppl):85–96.
2. Buser D, Bragger U, Lang NP, Nyman S. Regeneration and enlargement of jaw bone using guided tissue regeneration. Clin Oral Implants Res 1990;1:22–32.
3. Lekholm U, Becker W, Dahlin C, Becker B, Donath K, Morrison E. The role of early vs. late removal of GTAM membranes on bone formation around oral implants placed in immediate extraction sockets: An experimental study in dogs. Clin Oral Implants Res 1993;4:121–129.
4. Palmer RM, Floyd PD, Palmer PJ, Smith BJ, Johansson CB, Albrektsson T. Healing of implant dehiscence defects with and without expanded polytetrafluoroethylene membranes: A controlled clinical and histological study. Clin Oral Implants Res 1994;5:98–104.
5. Pinholt EM, Haanaes HR, Donath K, Bang G. Titanium implant insertion into dog alveolar ridges augmented by allogenic material. Clin Oral Implants Res 1994;5:213–219.
6. Becker W, Becker BE, Caffesse R. A comparison of demineralized freeze-dried bone and autologous bone to induce bone formation in human extraction sockets. J Periodontol 1994;65:1128–1133.
7. Simion M, Baldoni M, Rossi P, Zaffe D. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. Int J Periodont Rest Dent 1994;14:167–180.
8. Fritz ME, Malmquist J, Koth D, Jeffcoat M, Hardwick R, Braswell LD, et al. The use of guided bone regeneration to fill large mandibular defects in monkeys: A pilot study. Int J Oral Maxillofac Implants 1994;9:644–652.
9. Jovanovic SA, Schenk RK, Orsini M, Kenney EB. Supracrestal bone formation around dental implants: An experimental dog study. Int J Oral Maxillofac Implants 1995;10:23–31.
10. Becker W, Schenk R, Higuchi K, Lekholm U, Becker B. Variations in bone regeneration adjacent to implants augmented with barrier membranes alone or with demineralized freeze-dried bone or autologous grafts: A study in dogs. Int J Oral Maxillofac Implants 1995;10:143–154.
11. Hammack BL, Enneking WF. Comparative vascularization of autogenous and homogenous bone transplants. J Bone Joint Surg [Am] 1960;42:811.
12. Male AJ, Gasser J, Fonseca RJ, Nelson J. Comparison of onlay autologous and allogenic bone grafts to the maxilla in primates. J Oral Maxillofac Surg 1983;42:487–499.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
13. Boyne PJ. Performance of bone grafts in reconstructive surgery. In: Williams DF (ed). Biocompatibility of Tissue Analogs. Volume II. Boca Raton, FL: CRC, 1985:1–29.
14. Burchardt H. Biology of bone transplantation. Orthop Clin North Am 1987;18:187–195.
15. Marx RE. Biology of bone grafts. In: Kelly JPW (ed). OMS Knowledge Update. Vol 1. Rosemont, IL: American Association of Oral and Maxillofacial Surgeons, 1994;1:RCN3–17.
16. Brånemark P-I, Lindstrom J, Hallen O, Briene U, Jeppson P-H, Ohman A. Reconstruction of the defective mandible. Scand J Plast Reconstr Surg 1975;9:116–128.
17. Tolman DE. Reconstructive procedures with endosseous implants in grafted bone: A review of the literature. Int J Oral Maxillofac Implants 1995;10:275–294.
18. Breine U, Brånemark P-I. Reconstruction of alveolar jaw bone. Scand J Plast Reconstr Surg 1980;14:23–48.
19. Keller EE, van Roekel NB, Desjardins RP, Tolman DE. Prosthetic-surgical reconstruction of the severely resorbed maxilla with iliac bone grafting and tissue-integrated prostheses. Int J Oral Maxillofac Implants 1987;2:155–165.
20. Listrom RD, Symington JM. Osseointegrated dental implants in conjunction with bone grafts. Int J Oral Maxillofac Surg 1988;17:116–118.
21. Kahnberg KE, Nystrom L, Bartholdsson L. Combined use of bone grafts and Brånemark fixtures in the treatment of severely resorbed maxillae. Int J Oral Maxillofac Implants 1989;4:297–304.
22. Wood RM, Moore DL. Grafting of the maxillary sinus with intraorally harvested autogenous bone prior to implant placement. Int J Oral Maxillofac Implants 1988;3:209–214.
23. Collins TA. Onlay bone grafting in combination with Brånemark implants. Oral Maxillofac Surg Clin North Am 1991;3:893–902.
24. Jensen J, Sindet-Pedersen S. Autogenous mandibular bone grafts and osseointegrated implants for reconstruction of the severely atrophied maxilla: A preliminary report. J Oral Maxillofac Surg 1991;49:1277–1287.
25. ten Bruggenkate CM, Kraaijenhagen HA, van der Kwast WAM, Krekeler G, Oostenbeek HS. Autogenous maxillary bone grafts in conjunction with placement of I.T.I. endosseous implants. A preliminary report. Int J Oral Maxillofac Surg 1992;21:81–84.
26. Misch CM. Enhance maxillary implant sites through symphysis bone graft. Dent
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Implantol Update 1991;2:101–104.
27. Misch CM, Misch CE, Resnik R, Ismail YH. Reconstruction of maxillary alveolar defects with mandibular symphysis grafts for dental implants: A preliminary procedural report. Int J Oral Maxillofac Implants 1992;7:360–366.
28. Jensen J, Sindet-Pedersen S, Oliver AJ. Varying treatment strategies for reconstruction of maxillary atrophy with implants: Results in 98 patients. J Oral Maxillofac Surg 1994;52:210–216.
29. Collins TA, Nunn W. Autogenous veneer grafting for improved esthetics with dental implants. Comp Contin Educ Dent 1994;15:370–376.
30. Misch CM, Misch CE. Autogenous mandibular bone grafts for reconstruction of ridge deficiencies prior to implant placement [abstract]. Int J Oral Maxillofac Implants 1993;8:117.
31. Misch CM, Misch CE. The repair of localized severe ridge defects for implant placement using mandibular bone grafts. Implant Dent 1995;4:261–267.
32. Becker W, Becker BE, Polizzi G, Bergstrom C. Autogenous bone grafting of bone defects adjacent to implants placed into immediate extraction sockets in patients: A prospective study. Int J Oral Maxillofac Implants 1994;9:389–396.
33. Buser D, Dula K, Belser UC, Hirt H-P, Berthold H. Localized ridge augmentation using guided bone regeneration. II. Surgical procedure in the mandible. Int J Periodont Rest Dent 1995;15:11–29.
34. Misch CM. Ridge augmentation using mandibular ramus bone grafts for the placement of dental implants: Presentation of a technique. Pract Periodontics Aesthet Dent 1996;8:127–135.
35. Braun TW, Sotereanos GC. Autogenous regional bone grafting as an adjunct in orthognathic surgery. J Oral Maxillofac Surg 1984;42:43–48.
36. Sindet-Pedersen S, Enemark H. Reconstruction of alveolar clefts with mandibular or iliac crest bone grafts. A comparative study. J Oral Maxillofac Surg 1990;48:554–558.
37. Lustmann J, Lewinstein I. Interpositional bone grafting technique to widen narrow maxillary ridge. Int J Oral Maxillofac Implants 1995;10:568–577.
38. Williamson RA. Rehabilitation of the resorbed maxilla and mandible using autogenous bone grafts and osseointegrated implants. Int J Oral Maxillofac Implants 1996;11:476–488.
39. Raghoebar GM, Batenburg RHK, Vissink A, Reintsema H. Augmentation of localized defects of the anterior maxillary ridge with autogenous bone before insertion of implants. J Oral Maxillofac Surg 1996;54:1180–1185.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
40. Triplett RG, Schow S. Autologous bone grafts and endosseous implants: Complementary techniques. J Oral Maxillofac Surg 1996;54:486–494.
41. Lekholm U, Zarb GA. Patient selection and preparation. In: Brånemark PI, Zarb GA, Albrektsson T (eds). Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry. Chicago, Quintessence, 1985:199–209.
42. Misch CE. Density of bone: Effect on treatment plans, surgical approach, healing and progressive bone loading. Int J Oral Implantol 1990;6:23–31.
43. Smith JD, Abramson M. Membranous vs. endochondral bone autografts. Arch Otolaryngol 1974;99:203.
44. Zins JE, Whitaker LA. Membranous vs. endochondral bone autografts: Implications for craniofacial reconstruction. Plast Reconstr Surg 1983;72:778.
45. Lin KY, Bartlett SP, Yaremchuk MJ, Fallon M, Grossman RF, Whitaker LA. The effect of rigid fixation on the survival of onlay bone grafts: An experimental study. Plast Reconstr Surg 1990;86:449–456.
46. Rabie ABM, Dan Z, Samman N. Ultrastructural identification of cells involved in the healing of intramembranous and endochondral bones. Int J Oral Maxillofac Surg 1996;25:383–388.
47. Avery JK. Development of cartilages and bones of the facial skeleton. In: Avery JK (ed). Oral Development and Histology. New York: Thieme, 1994:42–56.
48. Kusiak JF, Zins JE, Whitaker LA. The early revascularization of membranous bone. Plast Reconstr Surg 1985;76:510.
49. Koole R, Bosker H, Noorman van der Dussen F. Secondary autogenous bone grafting in cleft patients comparing mandibular (ectomesenchymal) and iliac crest (mesenchymal) grafts. J Craniomaxillofac Surg 1989;17:28–30.
50. Hardesty RA, Marsh JL. Craniofacial onlay bone grafting: A prospective evaluation of graft morphology, orientation and embryonic origin. Plast Reconstr Surg 1990;85:5–14.
51. Manson PN. Facial bone healing and bone grafts. A review of clinical physiology. Clin Plast Surg 1994;21:331–348.
52. Marx RE. The science of reconstruction. In: Bell WH (ed). Modern Practice in Orthognathic and Reconstructive Surgery. Philadelphia: Saunders, 1992:1449–1452.
53. Lew D, Marino AA, Startzell JM, Keller JC. A comparative study of osseointegration of titanium implants in corticocancellous block and corticocancellous chip grafts in canine ilium. J Oral Maxillofac Surg 1994;52:952–958.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
54. Borstlap WA, Heidbuchel KLWM, Freihofer HPM, Kuijpers-Jagtman AM. Early secondary bone grafting of alveolar cleft defects: A comparison between chin and rib grafts. J Craniomaxillofac Surg 1990;18:201–205.
55. Roberts WE, Garetto LP, DeCastro RA. Remodeling of devitalized bone threatens periosteal margin integrity of endosseous titanium implants with threaded or smooth surfaces: Indications for provisional loading and axially directed occlusion. J Indiana Dent Assoc 1989;68:19–24.
56. Schenk RK. Bone regeneration: Biologic basis. In: Buser D, Dahlin C, Schenk RK (eds). Guided Bone Regeneration in Implant Dentistry. Chicago: Quintessence, 1994:49–100.
57. Hoppenreijs TJM, Nijdam ES, Freihofer HPM. The chin as a donor site in early secondary osteoplasty: A retrospective clinical and radiological evaluation. J Craniomaxillofac Surg 1992;20:199–124.
58. Buhr W, Coulon JP. Limits of the mandibular symphysis as a donor site for bone grafts in early secondary cleft palate osteoplasty. Int J Oral Maxillofac Surg 1996;25:389–393.
59. Rubens BC, West RA. Ptosis of the chin and lip incompetence: Consequences of lost mentalis muscle support. J Oral Maxillofac Surg 1989;4:359–366.
60. Hendy CW, Smith KG, Robinson PP. Surgical anatomy of the buccal nerve. Br J Oral Maxillofac Surg 1996;34:457–460.
61. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. Part I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. J Oral Surg 1957;10:677.
62. DalPont G. Retromolar osteotomy for correction of prognathism. J Oral Surg 1961;19:42.
63. Hunsuck EE. Modified intraoral splitting technique for correction of mandibular prognathism. J Oral Surg 1968;26:250.
64. Epker BN. Modifications in the sagittal osteotomy of the mandible. J Oral Surg 1977;35:157.
65. Bell WH, Schendel SA. Biologic basis for modification of the sagittal ramus split operation. J Oral Surg 1977;34:362.
66. Hall HD. Intraoral surgery. In: Bell WH (ed). Modern Practice in Orthognathic and Reconstructive Surgery. Philadelphia: Saunders, 1992:2111–2139.
67. Heggie AAC. The use of mandibular buccal cortical grafts in bimaxillary surgery. J Oral Maxillofac Surg 1993;51:1282–1283.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
68. Jensen J, Reiche-Fischel O, Sindet-Pedersen S. Autogenous mandibular bone grafts for malar augmentation. J Oral Maxillofac Surg 1995;53:88–90.
69. Smith BR, Rajchel JL II. Anatomic considerations in mandibular ramus osteotomies. In: Bell WH (ed). Modern Practice in Orthognathic and Reconstructive Surgery. Philadelphia: Saunders, 1992:2347–2360.
70. Rajchel J, Ellis E, Fonseca RJ. The anatomical location of the mandibular canal: Its relationship to the sagittal ramus osteotomy. Int J Adult Orthodon Orthognath Surg 1986;1:37.
71. Johnson JV, Hinds EC. Evaluation of teeth vitality after subapical osteotomy. J Oral Surg 1969;27:256.
72. Pepersack WJ. Tooth vitality after alveolar segmental osteotomy. J Maxillofac Surg 1973;1:85–91.
73. Lindquist CC, Obeid G. Complications of genioplasty done alone or in combination with sagittal split-ramus osteotomy. J Oral Surg 1988;66:13–16.
74. Hutchinson D, Macgregor AJ. Tooth survival following various methods of subapical osteotomy. Int J Oral Surg 1972;1:81–86.
75. Whitaker LA. Biological boundaries: A concept in facial skeletal restructuring. Clin Plast Surg 1989;16:1–10.
76. Nyman S, Lang NP, Buser D, Bragger U. Bone regeneration adjacent to titanium dental implants using guided tissue regeneration. A report of 2 cases. Int J Oral Maxillofac Implants 1990;5:9–14.
77. Phillips JH, Rahn BA. Fixation effects on membranous and endochondral onlay bone graft revascularization and bone deposition. Plast Reconstr Surg 1990;85:891–897.
78. Wachtel HC, Langford A, Bernimoulin J-P, Reichart P. Guided bone regeneration next to osseointegrated implants in humans. Int J Oral Maxillofac Implants 1991;6:127–135.
79. Fonseca RJ, Clark PJ, Burkes EJ, Baker RD. Revascularization and healing of onlay particulate autologous bone grafts in primates. J Oral Surg 1980;38:572–577.
80. Dado DV, Izquierdo R. Absorption of onlay bone grafts in immature rabbits: Membranous versus endochondral bone and bone struts versus paste. Ann Plast Surg 1989;23:39–48.
81. Jensen OT. Guided bone graft augmentation. In: Buser D, Dahlin C, Schenk RK (eds). Guided Bone Regeneration in Implant Dentistry. Chicago: Quintessence, 1994:235–264.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
82. Nystrom E, Kahnberg K-E, Albrektsson T. Treatment of the severely resorbed maxillae with bone graft and titanium implants: Histologic review of autopsy specimens. Int J Oral Maxillofac Implants 1993;8:167–172.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Fig. 1 Exposure of the mandibular symphysis by a vestibular approach. The osteotomy is between the canine roots.
Fig. 2 Exposure of the ramus donor site and graft osteotomy.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Fig. 3 Fixation of the ramus veneer graft to the maxillary lateral recipient site with small-diameter titanium alloy screws.
Fig. 4 Incorporation of the ramus graft 4 months after placement. Minimal resorption of the graft allows ideal implant placement.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Fig. 5a Corticocancellous block graft harvested from the mandibular symphysis.
Fig. 5b Cortical veneer graft harvested from the mandibular ramus.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
Fig. 6 Anterior view of the exposed posterior mandible recipient site and ramus graft osteotomy. A chisel is used to separate the graft from the ramus.
Fig. 7 The ramus graft is transferred to the thin posterior mandible and fixated into place to gain additional width.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
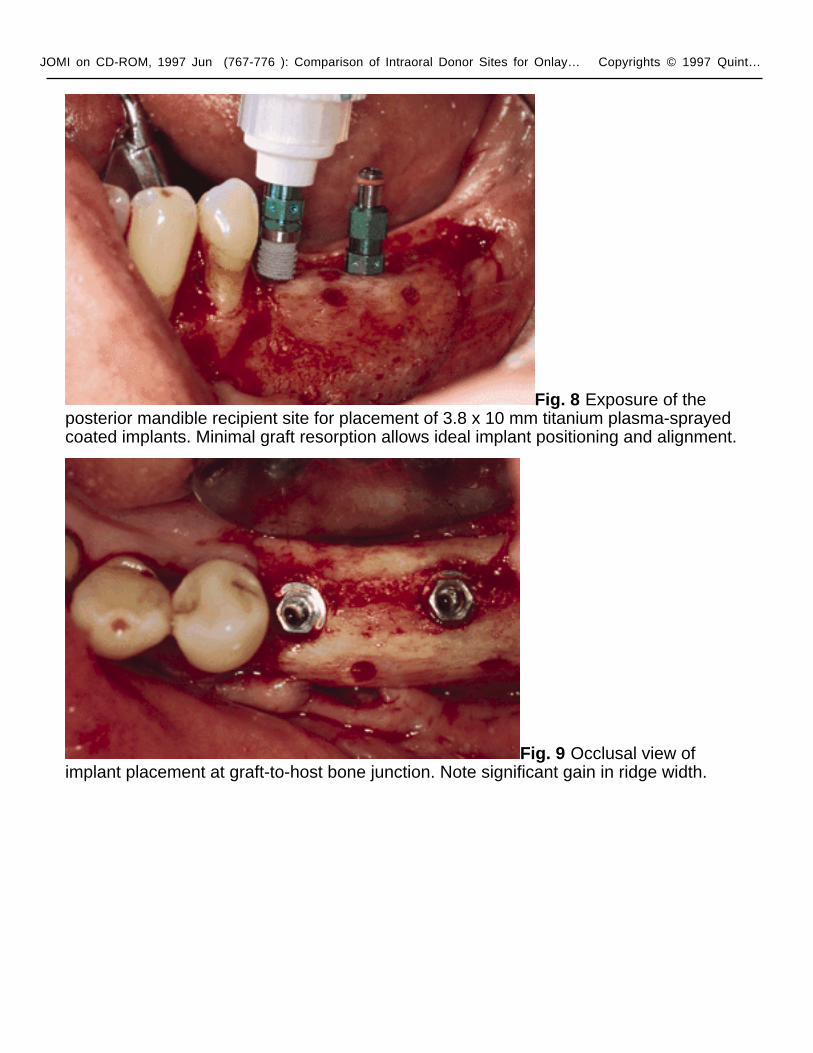
Fig. 8 Exposure of the posterior mandible recipient site for placement of 3.8 x 10 mm titanium plasma-sprayed coated implants. Minimal graft resorption allows ideal implant positioning and alignment.
Fig. 9 Occlusal view of implant placement at graft-to-host bone junction. Note significant gain in ridge width.
JOMI on CD-ROM, 1997 Jun (767-776 ): Comparison of Intraoral Donor Sites for Onlay… Copyrights © 1997 Quint…
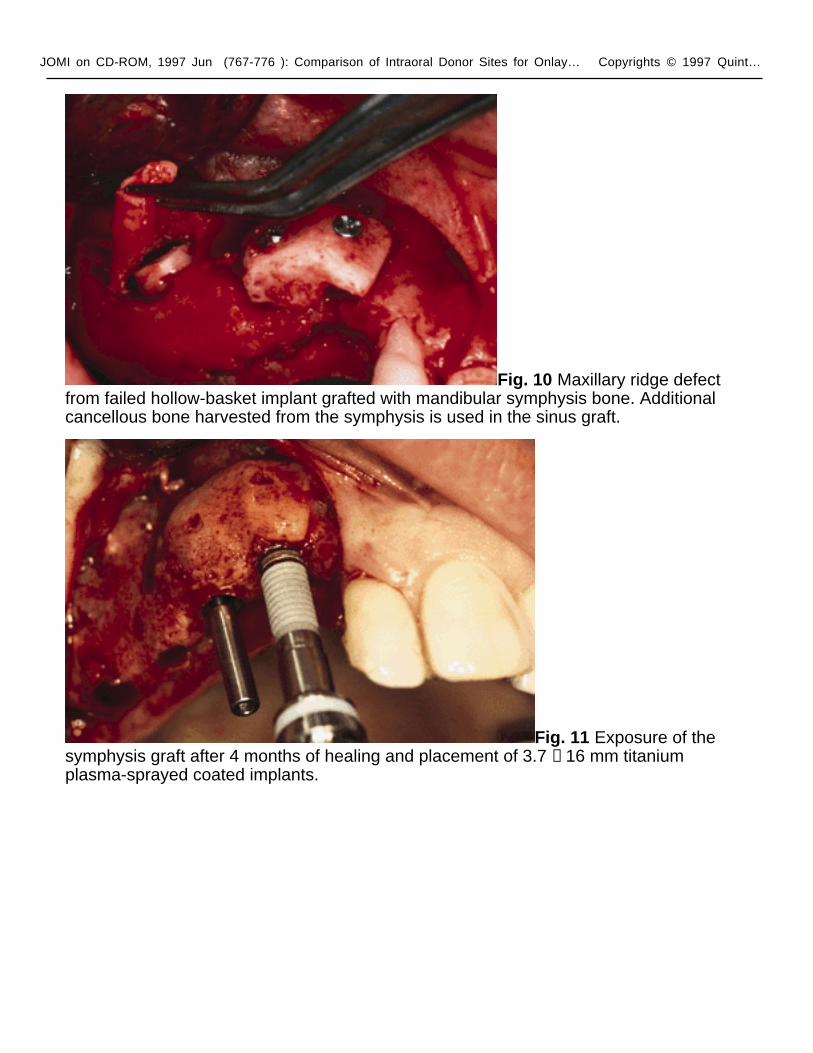
Fig. 10 Maxillary ridge defect from failed hollow-basket implant grafted with mandibular symphysis bone. Additional cancellous bone harvested from the symphysis is used in the sinus graft.
Fig. 11 Exposure of the symphysis graft after 4 months of healing and placement of 3.7 × 16 mm titanium plasma-sprayed coated implants.