Embed Size (px)
Citation preview

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
94
Comparison of intrusive effect of miniscrew implants versus intrusion arch mechanics on maxillary anterior teeth : A Finite Element Analysis
Pavitra Waikasetkorn1
Associate professor Dr. Boonsiva Suzuki2
[email protected] Dr. Eduardo Yugo Suzuki3
1Master candidate, Department of Orthodontics, Faculty of Dentistry, Bangkokthonburi University, Bangkok, Thailand
[email protected] 2Associate professor, Department of Orthodontics, Faculty of Dentistry,
Bangkokthonburi University, Bangkok, Thailand, 3Lecturer, Department of Orthodontics, Faculty of Dentistry,
Bangkokthonburi University, Bangkok, Thailand,
Abstract The purpose of this study was to compare biomechanical effect of the anterior teeth intrusion between miniscrew implants and intrusion arch, using Finite element (FE) analysis. The FE model of maxilla was constructed. Two intrusion mechanics were simulated, sixty grams of intrusive forces were applied from the archwire to the miniscrew implants or intrusion arch. The initial displacement of anterior teeth and first molars and stress distribution of periodontal ligament (PDL) were evaluated. In both scenarios, anterior teeth were intruded and proclined labially with the similar amount and pattern. First molars in the intrusion arch mechanic were extruded and tipped distally. Compressive stress was observed at apical-palatal area in the PDL of anterior teeth and along mesial surface of first molars. Stress on the first molars of intrusion arch was 10 times higher than that of miniscrew implants scenario. Miniscrew implants and intrusion arch provide same intrusive movement of the anterior teeth. Keywords: FINITE ELEMENT ANALYSIS, MINISCREW, INTRUSION

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
95
Introduction Maxillary anterior intrusion, one of the challenge mechanics in orthodontics, has been
proceeded to correct several problems in patients with deepbite and high gingival display. The suitable appliances, mechanics, and treatment modality to treat deepbite through intrusion maxillary anterior teeth, or extrusion the posterior segment, or a combination of both depend on the diagnosis and treatment goals. Conventional intrusion mechanic can be used through continuous or segmental archwire for example, Burstone intrusion arch (C. J. Burstone, 1962, 1966) or Utility archwire (R. Ricketts, 1979; R. M. Ricketts, 1976), which allow intrusion of the anterior teeth and extrusion of the posterior teeth. On the other hands, the total intrusion of maxillary anterior teeth can be obtained by applying the intrusive force from the main archwire direct to the miniscrew implants placed between the interradicular spaces of the anterior teeth. (Kaku et al., 2012; Saxena, 2010)
A true intrusion takes place when forces are directed through the center of resistance. (C. R. Burstone, 1977) If the intrusive force is applied anteriorly to the center of resistance of a unit, the anterior teeth will displace labially. Although miniscrew implants and intrusion arch have been reported as successful treatment modalities to effectively intrude anterior teeth. (C. R. Burstone, 1977; Papageorgiou, 2012) However, the controversies regarding labial displacement of anterior teeth between these two mechanics are discussed. (Kahraman, 2017; Polat-Özsoy, 2011) Clinical studies reported that miniscrew implants provided significantly greater amount of intrusion than intrusion arch. (Jain, 2014; Polat-Özsoy et al., 2011) In terms of labial displacement, some studies showed miniscrew implants provided higher labial movement while intruding than intrusion arch mechanics (Senışık & Türkkahraman, 2012), but others showed opposite result. (Polat-Özsoy et al., 2011) These controversies might related to several factors; the difference on force application settings, point of intrusive force on archwire versus intrusive force engaged to the brackets (Polat-Özsoy et al., 2011), and the different amount of intrusive force on miniscrews versus on intrusion arch. (Polat-Özsoy et al., 2011; Senışık, 2012)
The clinical studies might have limitation in comparing these intrusive mechanics regarding controlling amount, point of force application, and direction of intrusive force in the individual patients. Finite element analysis is a preferable method to analyze change in the alveolar bone, the surrounding structures, and the stress distribution on the anterior and posterior teeth following orthodontic tooth movement. (Cheng, 2004; Cifter, 2011; Park et al., 2011)
การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
96
The purpose of this study To compare initial tooth displacement and stress distribution on anterior teeth and first molars between miniscrew implants and intrusion arch using Finite element (FE) analysis. Scope of research Finite element method was used to analyze two intrusion mechanics. Descriptive analysis of the initial displacement in the X, Y, and Z planes, the pattern of principle stress in the periodontal ligament (PDL), and the maximum von Mises stress in the PDL of anterior teeth and first molar was reported. Research Methodology
3D finite element (FE) Model of maxilla was constructed by CT scan of 21-year-old patient. The information of 3D construction then was used to generate CAD Model by NX V10.0 (Siemens Product Life cycle software Inc., Texas, USA). The virtually constructed model was combined with maxillary dentition, 0.25-mm periodontal ligament, cortical and cancellous bone, brackets (0.018 x 0.025-inch Roth prescription), main archwire (0.016 x 0.022-inch stainless steel), intrusion archwire (0.017 x 0.025-inch TMA), miniscrew implants (1.6 x 6 mm).
The model was meshed by using tetrahedral elements. The final model is consisted of 6,085,470 elements and 1,144,752 nodes with edge length ranging from 0.125 mm to 0.50 mm. This file was exported to Ls-dyna Version 971R (Livermore Software Technology Corporation, Livermore, CA, USA) using for final model result analysis. All material in the finite element analysis were assumed to be homogenous, isotropic, and linearly elastic. The mechanical properties of the materials have been described in previous studies (Cifter, 2011; Tanne, 1987) as shown in Table 1.
Table 1 Mechanical properties of the materials
Young’s modulus (MPa) Poisson’s ratio (μ) Cortical bone 13700 0.26 Cancellous bone 1370 0.3 Tooth 19613.3 0.15 PDL 0.6668 0.49 Stainless steel 200000 0.3 TMA 66000 0.3
Model with two different scenarios of intrusion forces were simulated. the selected
points of force application were assigned based on the previous study (Polat-Ozsoy, 2009) and

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
97
considering points which the clinicians used to intrude maxillary anterior teeth. For miniscrew implants scenario, miniscrews were placed at 12 mm superior to the main archwire between lateral incisor and canine roots, the collar of the miniscrew implants were 1 mm external to the bone to simulate labial gingival thickness. For intrusion arch scenario, 0.017 x 0.025-inch TMA was inserted to the buccal tube of maxillary first molars (Figure 1).
Intrusion arch Miniscrew implant
Figure 1 The finite element model with intrusion arch and miniscrew implant scenarios.
Sixty grams of intrusive forces were applied from the main archwire, midpoint between lateral incisors and canines, to the miniscrew implants or intrusion arch. Contact condition and fixed condition was set between teeth, main archwire, and bracket. The initial displacement of anterior teeth was measured from the nodes at midpoints of the incisal edges and root apices of individual teeth. That of first molar was measured from the nodes at mesio-buccal cusp tip, palatal cusp tip and palatal root apex. The patterns of stress distribution on PDL were demonstrated by principle stress and the magnitude of stress was compared between models by maximum von Mises’s stress.
Boundary conditions were assigned to the nodes on the superior and posterior surface of cortical bone as zero-displacement and zero-rotation in all directions. The x-axis was set in the mesial-distal direction, the y-axis was set in the labio-palatal direction, the z-axis was set as inciso-apical direction. Descriptive analysis was used to analyze the initial displacement in the x, y, z-axis and also stress distribution on PDL of central, lateral incisors, canine, and first molars. Research Finding
Stress distribution patterns and magnitudes on PDL of maxillary anterior teeth and first molars
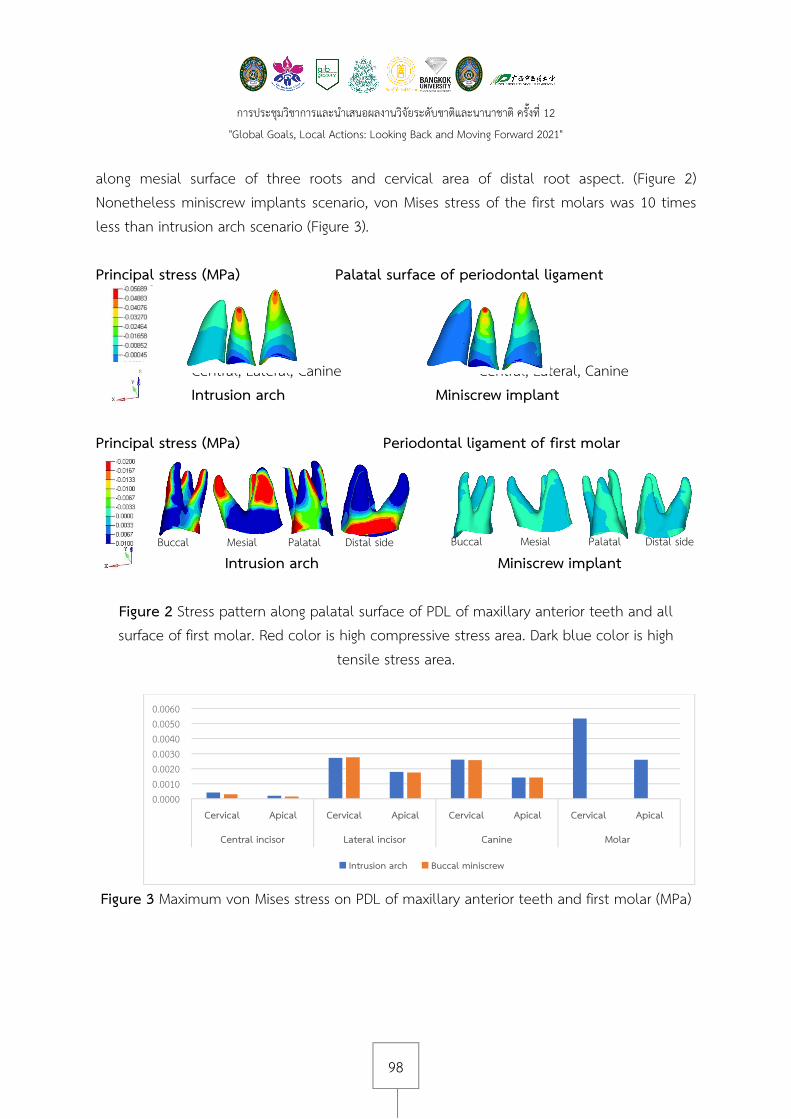
In both scenarios, the pattern of stress distribution on PDL of anterior teeth showed similarly compressive stress (red color) at apical-palatal area and tensile stress (blue color) on 1/3 cervical-palatal of lateral incisor and canine teeth (Figure 2). Both scenarios showed that lateral incisor had von Mises stress similar to canine but central incisor had the lowest value. (Figure 3) For the first molars, intrusion arch scenario showed the highest compressive stress
Intrusive force
การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
98
along mesial surface of three roots and cervical area of distal root aspect. (Figure 2) Nonetheless miniscrew implants scenario, von Mises stress of the first molars was 10 times less than intrusion arch scenario (Figure 3).
Principal stress (MPa) Palatal surface of periodontal ligament
Central, Lateral, Canine Central, Lateral, Canine Intrusion arch Miniscrew implant
Principal stress (MPa) Periodontal ligament of first molar
Intrusion arch Miniscrew implant
Figure 2 Stress pattern along palatal surface of PDL of maxillary anterior teeth and all surface of first molar. Red color is high compressive stress area. Dark blue color is high
tensile stress area.
Figure 3 Maximum von Mises stress on PDL of maxillary anterior teeth and first molar (MPa)
0.00000.00100.00200.00300.00400.00500.0060
Cervical Apical Cervical Apical Cervical Apical Cervical Apical
Central incisor Lateral incisor Canine Molar
Intrusion arch Buccal miniscrew
Buccal Mesial Palatal Distal side Buccal Mesial Palatal Distal side
การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
99
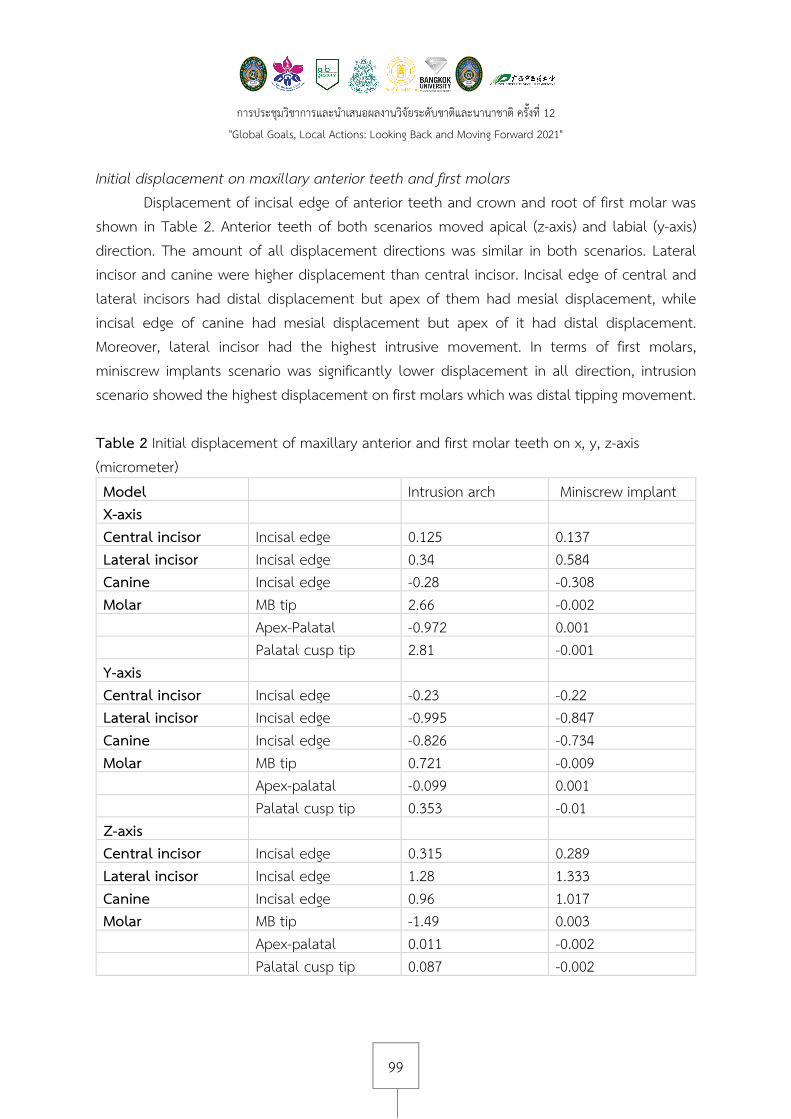
Initial displacement on maxillary anterior teeth and first molars Displacement of incisal edge of anterior teeth and crown and root of first molar was
shown in Table 2. Anterior teeth of both scenarios moved apical (z-axis) and labial (y-axis) direction. The amount of all displacement directions was similar in both scenarios. Lateral incisor and canine were higher displacement than central incisor. Incisal edge of central and lateral incisors had distal displacement but apex of them had mesial displacement, while incisal edge of canine had mesial displacement but apex of it had distal displacement. Moreover, lateral incisor had the highest intrusive movement. In terms of first molars, miniscrew implants scenario was significantly lower displacement in all direction, intrusion scenario showed the highest displacement on first molars which was distal tipping movement.
Table 2 Initial displacement of maxillary anterior and first molar teeth on x, y, z-axis (micrometer) Model Intrusion arch Miniscrew implant X-axis Central incisor Incisal edge 0.125 0.137 Lateral incisor Incisal edge 0.34 0.584 Canine Incisal edge -0.28 -0.308 Molar MB tip 2.66 -0.002 Apex-Palatal -0.972 0.001 Palatal cusp tip 2.81 -0.001 Y-axis Central incisor Incisal edge -0.23 -0.22 Lateral incisor Incisal edge -0.995 -0.847 Canine Incisal edge -0.826 -0.734 Molar MB tip 0.721 -0.009 Apex-palatal -0.099 0.001 Palatal cusp tip 0.353 -0.01 Z-axis Central incisor Incisal edge 0.315 0.289 Lateral incisor Incisal edge 1.28 1.333 Canine Incisal edge 0.96 1.017 Molar MB tip -1.49 0.003 Apex-palatal 0.011 -0.002 Palatal cusp tip 0.087 -0.002

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
100
X-axis, (+) distal, (-) mesial direction; Y-axis, (-) labial, (+) palatal direction; Z-axis, (+) apical, (-) incisal direction. Discussion This study was conducted to evaluate the biomechanical effect of intrusion arch on the anterior teeth intrusion comparing with the miniscrew implants by means of FE method which provides the understanding of stress distribution on anterior teeth, PDL, surrounding bone, as well as, initial displacement of anterior and first molar teeth. (Farah, 1973) There are several factors which effect on pattern, amount of displacement and stress distribution on anterior teeth. From this study, both scenarios showed similar intrusive effects because the results were based on the same line of action and a point of force application. First, the line of action of intrusive force on both scenarios was applied anteriorly to center of resistance of six maxillary anterior teeth which lied half way between lateral incisor and canine and 8-10 mm apical to the bracket position. (Farah et al., 1973; Melsen, 1990; Sia, 2007) (Figure 4) As a result, the displacement of anterior teeth did not show the absolute intrusion but intrusion with some amount of labial tipping. Similarly to Cho et al, 2016, presented 50 gram intrusive force from main archwire to miniscrew implants with variable force application and alveolar bone loss, the labial tipping were illustrated by the concentrated stresses on the cervical and root tip of anterior teeth on every models. However, other studies (Park et al., 2011; Cho et al, 2016) reported that the amount of labial tipping can be decreased by applied distro-intrusive force instead of vertical force direction.
Figure 4 The illustration of force and moment of maxillary dentition with intrusive force from intrusion arch
Second, the points of force application, from the main archwire to intrusion arch or
miniscrew implants was also one of the important factors affect the pattern of tooth displacement. The force applied on the main archwire, adjacent teeth next to the force were found intrusion as well as mesial-distal angulation change. Also, stress concentrated more on
CR CR

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
101
the teeth near the point of force application. When the force application was between lateral and canine, these teeth showed high stress concentration and more displacement, moreover the smaller size of lateral incisor caused the greater stress and displacement than canine. (Salehi et al., 2015) The result agrees with Salehi, 2015 study, the apical region of lateral incisor experienced the highest stress levels. This site should be considered as the most susceptible site to resorption. Although, the anterior teeth of both scenarios showed the similar results, the first molars of miniscrew implants scenario displayed the least displacement due to the applied intrusive force located in the anterior section as the miniscrews were used as an anchorage. On the contrary, intrusion arch presented the highest von Mises stress in PDL and highest mesial extrusion of first molar due to the side effect of intrusion arch which used molars as an anchorage. However the side effect of molar extrusion might be beneficial in the modification of vertical dimension of the patient’s face. (Papageorgiou, 2012) The decision depends on the diagnosis and treatment objective of individual case. Conclusion Miniscrew implants and intrusion arch provide same intrusive movement of the anterior teeth. Intrusion arch presented a distal tipping movement on the first molars. References 1. Burstone CJ. (1962). Rationale of the segmented arch. Am J Orthod. 48, 805-22. 2. Burstone CJ. (1966). The mechanics of the segmented arch techniques. Angle Orthod. 36(2), 99-120. 3. Ricketts RM. (1976). Bioprogressive therapy as an answer to orthodontic needs Part II. American journal of orthodontics. 70(4), 359-97. 4. Ricketts R, Bench R, Gugino C, Hilgers J. Schulhof RJ. (1979). Bioprogressive therapy. Denver: Rocky Mountain Orthodontics. 5. Kaku M, Kojima S, Sumi H, et al. (2012). Gummy smile and facial profile correction using miniscrew anchorage. Angle Orthod. 82(1), 170-7. 6. Saxena R, Kumar PS, Upadhyay M, Naik V. (2010). A clinical evaluation of orthodontic mini-implants as intraoral anchorage for the intrusion of maxillary anterior teeth. World J Orthod. 11(4), 346-51. 7. Burstone CR. (1977). Deep overbite correction by intrusion. Am J Orthod. 72(1), 1-22.

การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
102
8. Papageorgiou SN, Zogakis IP, Papadopoulos MA. (2012). Failure rates and associated risk factors of orthodontic miniscrew implants: a meta-analysis. American Journal of Orthodontics and Dentofacial Orthopedics. 142(5), 577-95. e7. 9. Polat-Özsoy Ö, Arman-Özçırpıcı A, Veziroğlu F, Çetinşahin A. (2011). Comparison of the intrusive effects of miniscrews and utility arches. Am J Orthod Dentofacial Orthop.139(4), 526-32. 10. Kahraman F, KiliÇ N, Dağsuyu I. (2017). A THREE-DIMENSIONAL EVALUATION OF THE EFFECTS OF DIFFERENT INCISOR INTRUSION MECHANICS TO THE PERMANENT MAXILLARY FIRST MOLAR TEETH BY USING CONE BEAM COMPUTED TOMOGRAPHY. Cumhuriyet Dental Journal. 113-21. 11. Jain RK, Kumar SP, Manjula WS. (2014). Comparison of intrusion effects on maxillary incisors among mini implant anchorage, j-hook headgear and utility arch. J Clin Diagn Res. 8(7), Zc21-4. 12. Senışık NE, Türkkahraman H. (2012). Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofacial Orthop. 141(6), 723-33. 13. Cheng S-J, Tseng I-Y, Lee J-J, Kok S-H. (2004), A prospective study of the risk factors associated with failure of mini-implants used for orthodontic anchorage. International Journal of Oral & Maxillofacial Implants. 19(1). 14. Cifter M, Sarac M. (2011). Maxillary posterior intrusion mechanics with mini-implant anchorage evaluated with the finite element method. Am J Orthod Dentofacial Orthop. 140(5), e233-41. 15. Park H-K, Sung E-H, Cho Y-S, et al. (2011). 3-D FEA on the intrusion of mandibular anterior segment using orthodontic miniscrews. Korean Journal of Orthodontics. 41(6), 384-98. 16. Tanne K, Sakuda M, Burstone CJ. (1987). Three-dimensional finite element analysis for stress in the periodontal tissue by orthodontic forces. Am J Orthod Dentofacial Orthop. 92(6), 499-505. 17. Polat-Ozsoy O, Arman-Ozcirpici A, Veziroglu F. (2009). Miniscrews for upper incisor intrusion. Eur J Orthod. 31(4), 412-6. 18. Farah JW, Craig RG, Sikarskie DL. (1973). Photoelastic and finite element stress analysis of a restored axisymmetric first molar. J Biomech. 6(5), 511-20. 19. Sia S, Koga Y, Yoshida N. (2007). Determining the center of resistance of maxillary anterior teeth subjected to retraction forces in sliding mechanics. An in vivo study. Angle Orthod. 77(6), 999-1003. 20. Melsen B, Fotis V, Burstone CJ. (1990). Vertical force considerations in differential space closure. J Clin Orthod. 24(11), 678-83.
การประชุมวิชาการและนําเสนอผลงานวิจัยระดับชาติและนานาชาติ คร้ังท่ี 12
"Global Goals, Local Actions: Looking Back and Moving Forward 2021"
103
21. Cho SM, Choi SH, Sung SJ, Yu HS, Hwang CJ. (2016). The effects of alveolar bone loss and miniscrew position on initial tooth displacement during intrusion of the maxillary anterior teeth: Finite element analysis. Korean J Orthod. 46(5), 310-22. 22. Salehi P, Gerami A, Najafi A, Torkan S. (2015). Evaluating Stress Distribution Pattern in Periodontal Ligament of Maxillary Incisors during Intrusion Assessed by the Finite Element Method. J Dent (Shiraz). 16(4), 314-22. 23. Wheeler RC, Ash MM. (1984). Wheeler's Dental anatomy, physiology, and occlusion. Philadelphia: Saunders.





























