Embed Size (px)
Citation preview

Arch Gynecol Obstet (2012) 286:287–293
DOI 10.1007/s00404-012-2268-8MATERNAL-FETAL MEDICINE
Comparison of magnesium sulfate and mannitol in treatment of eclamptic women with posterior reversible encephalopathy syndrome
Bilge Cetinkaya Demir · Kemal Ozerkan · Sevda Erer Ozbek · Nalan YÂldÂrÂm EryÂlmaz · Gokhan Ocakoglu
Received: 4 May 2011 / Accepted: 20 February 2012 / Published online: 17 March 2012© Springer-Verlag 2012
AbstractObjective To evaluate and compare the eVectiveness ofmagnesium sulfate (MgSO4) and mannitol in the treatmentof posterior reversible encephalopathy syndrome (PRES) ineclamptic women.Study design This retrospective analysis includes 62eclamptic women between 22 and 40 weeks of gestationwho were diagnosed with PRES in a tertiary care center. Totreat neurological symptoms, 34 women received magne-sium sulfate (Group 1) and the remaining 28 received 20%mannitol (Group 2) at the discretion of treating physician.Results Ten patients from both Group 1 (29%) and Group2 (35.7%) were normotensive at admission. 59 of 62patients presented with seizure. All patients underwent Xuidattenuated inversion recovery (FLAIR) magnetic resonanceimaging (MRI). Parietooccipital region and cerebellumwere the most commonly aVected areas. The duration oftreatment was signiWcantly shorter in Group 1 than Group 2(p < 0.001). Neurological examinations and the recovery
after treatment were signiWcantly better in favor of MgSO4
group (p = 0.039).Conclusion Mannitol is not superior to magnesium sul-fate in achieving neurological recovery. Magnesium sulfateseems to be the agent of choice for treatment of PRES.
Keywords Eclampsia · PRES · Pregnancy · MgSO4 · Mannitol
Introduction
Eclampsia is the occurrence of seizures unrelated to othercerebral conditions with signs and symptoms of preeclamp-sia. The diagnosis of eclampsia is obvious in the presenceof generalized edema, hypertension, proteinuria, and sei-zures in pregnant women [1]. However, 60–75% ofeclamptic women presents with persistent occipital or fron-tal headaches, blurred vision, photophobia, epigastric and/or right upper quadrant pain, and altered mental status[1, 2].
Several pathologic mechanisms have been implicatedwhether the neurologic symptoms of eclampsia arise from“over autoregulation” of blood brain barier (BBB) whichcauses vasospasm and ischemia (cytotoxic) or from hyper-perfusion (vasogenic) that leads to cerebral edema [3].Autoregulation is an intrinsic function of cerebral vascula-ture which is designed to maintain a stable blood Xow in theface of Xuctuating blood pressure [4]. Cytotoxic edemapreferentially aVects gray matter, and vasogenic edematends to predominate in the white matter. However, theclinical manifestations of cerebral edema are similarregardless of whether the edema is cytotoxic or vasogenic.The current paradigm suggests that neurological symptomsin pregnant women are due to severe hypertension with
B. C. Demir (&) · K. OzerkanDepartment of Obstetrics and Gynecology, Faculty of Medicine, Uludag University, Nilufer, 16059 Bursa, Turkeye-mail: [email protected]; [email protected]
S. E. OzbekDepartment of Neurology, Faculty of Medicine, Uludag University, Bursa, Turkey
N. YÂldÂrÂm EryÂlmazDepartment of Radiology, Faculty of Medicine, Uludag University, Bursa, Turkey
G. OcakogluDepartment of Biostatistics, Faculty of Medicine, Uludag University, Bursa, Turkey
123

288 Arch Gynecol Obstet (2012) 286:287–293
failed autoregulation, injury to the capillary bed, and hyper-perfusion leading to cerebral edema [5]. This condition rep-resents a form of reversible posterior leukoencephalopathysyndrome [6] or in other words posterior reversible enceph-alopathy syndrome (PRES) [7]. PRES is a clinicoradiologicentity which is characterized by certain imaging patternsand is associated with many diverse clinical entities includ-ing (pre)eclampsia. PRES was Wrst described by Hinchey asa neurological syndrome which manifests with a variety ofsymptoms and is a reversible condition when promptly rec-ognized and correctly treated [6]. Delayed or erroneousdiagnosis may lead to irreversible damage [8]. Symptomsof this syndrome are similar to eclampsia and include head-ache, nausea and vomiting, decreased alertness, alteredmental functioning, seizures and visual disturbances suchas blurred vision or cortical blindness [9]. The typicalimaging Wnding of PRES is hyperintensity on Xuid attenu-ated inversion recovery (FLAIR) magnetic resonance imag-ing (MRI) [10]. DiVusion weighted MRI (DWI), includingquantiWcation of apparent diVusion coeYcient (ADC)maps, is more sensitive to changes in distribution of waterin the brain. DWI can better detect white matter edema andit is reliable for diVerentiation of vasogenic and cytotoxicedema [11]. Imaging of obstetric patients with PRES(eclampsia and some cases of preeclampsia) is not distinctfrom other causes of PRES [7]. The pathophysiology ofPRES is poorly understood. But it shares same pathophysi-ological mechanisms of eclampsia [12]. Several aspects ofthe cerebral vasculature and its regulating mechanisms playan important role in the pathophysiology of eclampsia orPRES. The conditions associated with PRES are typicallysystemic processes, which have some degree of endothelialdysfunction and an inXammatory response [12]. Possibly,the causative conditions (and other unidentiWed processes)predispose to an increased vulnerability of the cerebral vas-culature to loss autoregulation. This may be a result ofincreased permeability of the blood–brain barrier, or a shiftof the cerebral autoregulation curve to the left, or both [12].The management of PRES depends on the removal of trig-gering factors [9].
Regarding the aforementioned hypotheses, it is impor-tant to diVerentiate between vasogenic and cytotoxicedema, as the optimal management of the two entities isdiVerent. While blood pressure control and supportive careare the Wrst-line treatments of vasogenic edema; womenwith cytotoxic edema and infarction require a more aggres-sive approach. Magnesium sulfate (MgSO4) is regarded asthe treatment of choice to prevent the occurrence of vaso-genic edema in cerebral tissue and neurological symptoms.Mannitol is another antiedema agent which can be used todecrease intracranial pressure in pregnant women withPRES. The aim of the present study is to compare the eVec-tiveness of mannitol and magnesium sulfate in ameliorating
vasogenic edema, when used concomitantly with antihyper-tensive therapy.
Materials and methods
This study included 62 eclamptic women who were diag-nosed with PRES at the obstetrics clinic of the Uludag Uni-versity Hospital between February 2006 and February2009. The study protocol was approved by the ResearchEthics Committee of the School of Medicine of the UludagUniversity.
153 preeclamptic women hospitalized and 80 of themwith symptoms of seizure, headache, blurred vision, highblood pressure had neuroimaging studies (CT or MRI)within the Wrst 12 h. The other 73 did not have neurologicalsymptoms. 62 of 80 patients were included in the study.The remaining 18 women were excluded since they did nothave typical neuroimaging Wndings of PRES. A 1.5-T MRIequipment (Magneton Vision, Siemens, Erlangen, Ger-many) was used to acquire T1-weighted sagittal and axial,T2-weighted axial and FLAIR-weighted, T2-weighted gra-dient echo, and axial diVusion (i.e., DWI and ADC scores)images. The medical records of pregnant women (symp-tom, age, gravida, parity, mode of delivery, past medicaland obstetric history, blood pressure at admission and post-partum period, laboratory levels), neurological symptomsand signs and Wndings of neuroimaging study were allnoted and retrieved from the hospital records. The systolicblood pressure (BP) at admission was classiWed into fourgroups; normal (<140 mm Hg), mildly elevated (140–169 mm Hg), moderately elevated (170–199 mm Hg), andseverely elevated (¸200 mm Hg). The mode and timing ofdelivery were determined according to obstetric conditions.Antihypertensive treatment was administered as deemednecessary. All patients were examined by two neurologistspre- and post-treatment. The choice of antiedema treatment,MgSO4 or mannitol, was decided at the discretion of thirdphysician (SEO) by chance.
Group 1 consisted of women who received intravenousMgSO4 at a rate of 2 gr/hour for a period of 48 h. Group 2included women who received 20% mannitol intravenouslyat a starting dose of 50 mg every 4 h and the dosage wastapered in the following 6 days. The treatment agents werestarted immediately after neuroimagings of the patients(i.e., before they gave birth).
All patients were classiWed into two categories accordingto neurological outcome. The “full recovery” groupincluded women who had no abnormal neurological Wnd-ings at discharge. The patients who had persistent neurolog-ical Wndings such as positive Babinski sign, blurred vision,or limited eye movements at discharge were included in the“partial recovery” group.
123
Arch Gynecol Obstet (2012) 286:287–293 289
Continuous variables were deWned with median, mini-mum and maximum values, and the interquartile range.Mann–Whitney U test was used to compare continuousvariables between the study groups. Pre- and post-treatmentvalues of systolic and diastolic blood pressures were com-pared with paired Wilcoxon signed rank test within eachgroup. Percent changes between pre- and post-treatmentblood pressure values were calculated and comparedbetween the treatment groups with Mann–Whitney U test.Categorical variables were deWned as frequency and per-centages, and Pearson Chi square and Fisher’s exact testswere used to compare those variables between groups. Sta-tistical signiWcance was set at p < 0.05. All statistical analy-ses were conducted with SPSS v.13 for Windows (SPSS,Chicago, IL, USA).
Results
34 women were given magnesium sulfate (Group 1) and 28women received mannitol treatment (Group 2). The gesta-tional age at admission to the hospital ranged between 22and 40 weeks, with median values of 34 and 33 weeks forGroups 1 and 2, respectively (Table 1). 25 (73.5%) womenin Group 1 and 11 (39.3%) women in Group 2 were nullip-arous, respectively (p < 0.01). At admission, 10 patients ineach group (29% of Group 1 and 35.7% of Group 2) werenormotensive (Table 2), and 33 (97%) women in Group 1and 26 (92.8%) women in Group 2 had generalized tonic–clonic seizures. None of the patients had a history ofepilepsy before pregnancy. Other symptoms which were
present at admission are presented in Table 3. The route ofdelivery was not signiWcantly diVerent between two groups(p = 0.84).
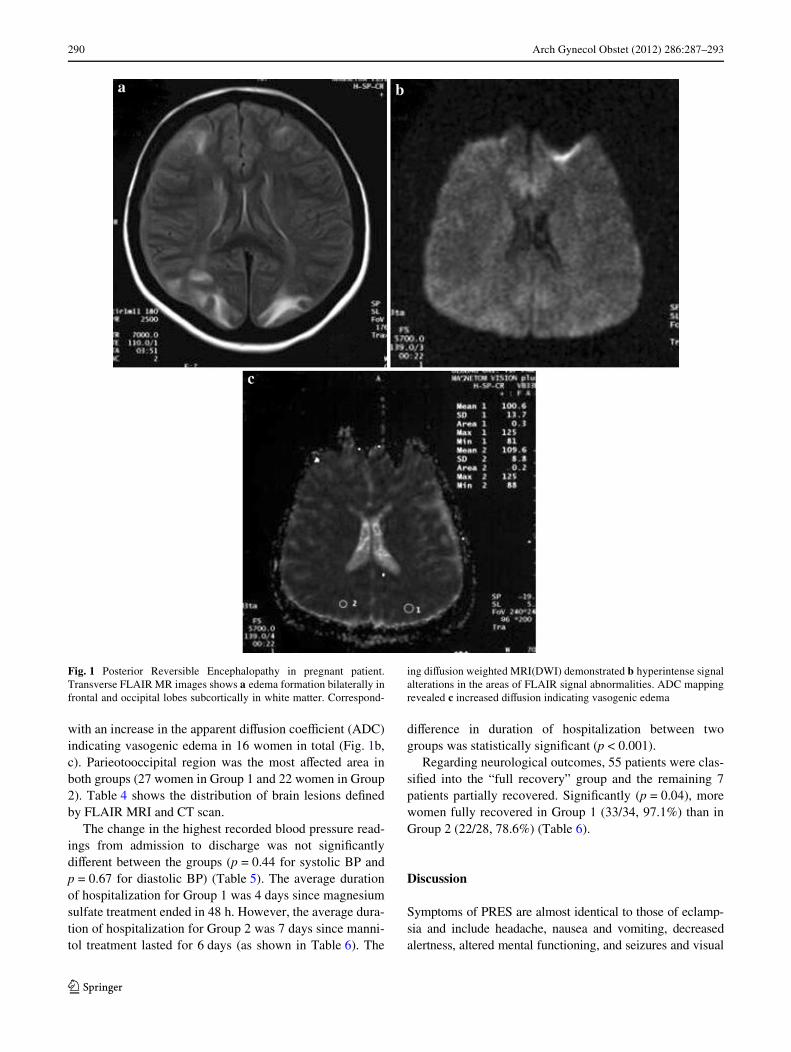
MRI investigations of the patients revealed hyperintensesignal changes especially at parietooccipital areas (72.9%in group 1 and 78% in group 2) and cerebellar area (8.1% ingroup 1 and 7.1% in group 2) in FLAIR sequences(Fig. 1a). DiVusion weighted MRI imaging showed signalisointensity and slight hyperintensity of the aVected areas
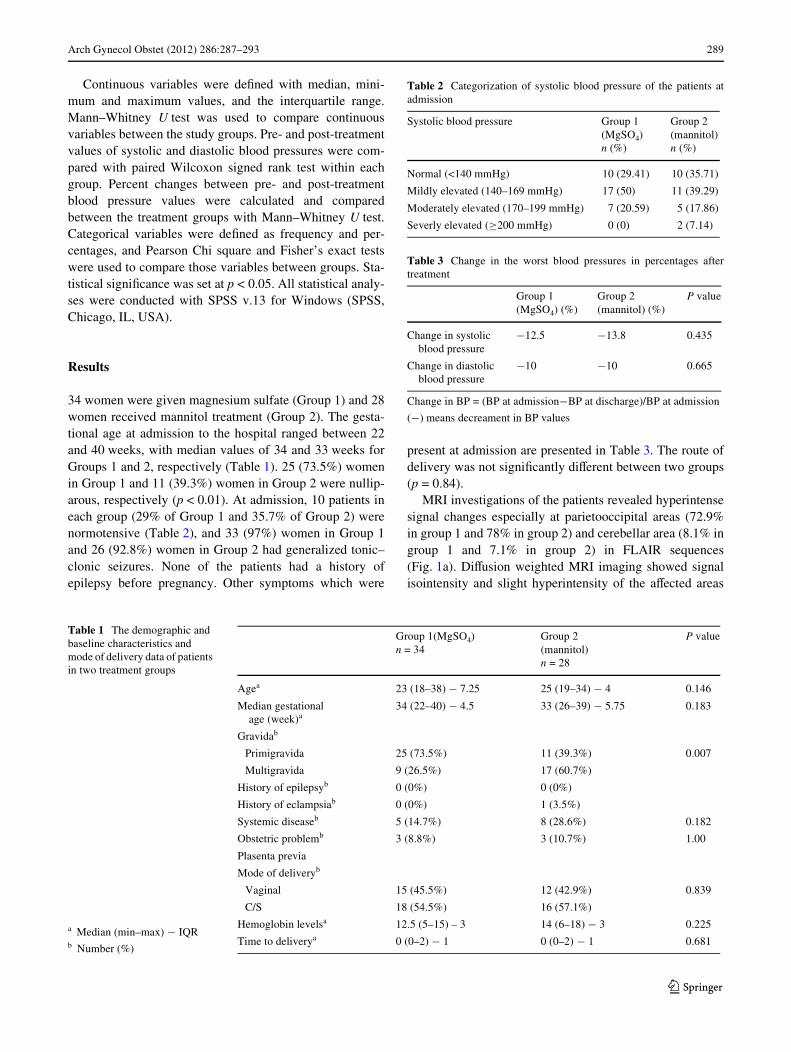
Table 1 The demographic and baseline characteristics and mode of delivery data of patients in two treatment groups
Group 1(MgSO4) n = 34
Group 2 (mannitol) n = 28
P value
Agea 23 (18–38) ¡ 7.25 25 (19–34) ¡ 4 0.146
Median gestational age (week)a
34 (22–40) ¡ 4.5 33 (26–39) ¡ 5.75 0.183
Gravidab
Primigravida 25 (73.5%) 11 (39.3%) 0.007
Multigravida 9 (26.5%) 17 (60.7%)
History of epilepsyb 0 (0%) 0 (0%)
History of eclampsiab 0 (0%) 1 (3.5%)
Systemic diseaseb 5 (14.7%) 8 (28.6%) 0.182
Obstetric problemb 3 (8.8%) 3 (10.7%) 1.00
Plasenta previa
Mode of deliveryb
Vaginal 15 (45.5%) 12 (42.9%) 0.839
C/S 18 (54.5%) 16 (57.1%)
Hemoglobin levelsa 12.5 (5–15) – 3 14 (6–18) ¡ 3 0.225
Time to deliverya 0 (0–2) ¡ 1 0 (0–2) ¡ 1 0.681a Median (min–max) ¡ IQRb Number (%)
Table 2 Categorization of systolic blood pressure of the patients atadmission
Systolic blood pressure Group 1 (MgSO4)n (%)
Group 2 (mannitol)n (%)
Normal (<140 mmHg) 10 (29.41) 10 (35.71)
Mildly elevated (140–169 mmHg) 17 (50) 11 (39.29)
Moderately elevated (170–199 mmHg) 7 (20.59) 5 (17.86)
Severly elevated (¸200 mmHg) 0 (0) 2 (7.14)
Table 3 Change in the worst blood pressures in percentages aftertreatment
Change in BP = (BP at admission¡BP at discharge)/BP at admission
(¡) means decreament in BP values
Group 1 (MgSO4) (%)
Group 2(mannitol) (%)
P value
Change in systolic blood pressure
¡12.5 ¡13.8 0.435
Change in diastolic blood pressure
¡10 ¡10 0.665
123
290 Arch Gynecol Obstet (2012) 286:287–293
with an increase in the apparent diVusion coeYcient (ADC)indicating vasogenic edema in 16 women in total (Fig. 1b,c). Parieotooccipital region was the most aVected area inboth groups (27 women in Group 1 and 22 women in Group2). Table 4 shows the distribution of brain lesions deWnedby FLAIR MRI and CT scan.
The change in the highest recorded blood pressure read-ings from admission to discharge was not signiWcantlydiVerent between the groups (p = 0.44 for systolic BP andp = 0.67 for diastolic BP) (Table 5). The average durationof hospitalization for Group 1 was 4 days since magnesiumsulfate treatment ended in 48 h. However, the average dura-tion of hospitalization for Group 2 was 7 days since manni-tol treatment lasted for 6 days (as shown in Table 6). The
diVerence in duration of hospitalization between twogroups was statistically signiWcant (p < 0.001).
Regarding neurological outcomes, 55 patients were clas-siWed into the “full recovery” group and the remaining 7patients partially recovered. SigniWcantly (p = 0.04), morewomen fully recovered in Group 1 (33/34, 97.1%) than inGroup 2 (22/28, 78.6%) (Table 6).
Discussion
Symptoms of PRES are almost identical to those of eclamp-sia and include headache, nausea and vomiting, decreasedalertness, altered mental functioning, and seizures and visual
Fig. 1 Posterior Reversible Encephalopathy in pregnant patient.Transverse FLAIR MR images shows a edema formation bilaterally infrontal and occipital lobes subcortically in white matter. Correspond-
ing diVusion weighted MRI(DWI) demonstrated b hyperintense signalalterations in the areas of FLAIR signal abnormalities. ADC mappingrevealed c increased diVusion indicating vasogenic edema
123
Arch Gynecol Obstet (2012) 286:287–293 291
disturbances such as blurred vision and cortical blindness [5].The symptoms usually develop quite quickly over a fewhours, reaching their worst in 12–48 h. Progression over sev-eral days is common, and the symptoms usually resolvewithin a week but may persist for longer in a few cases. Mostauthors have emphasized the visual loss and headache inpatients with PRES but seizure is the most frequent, in up to90% of cases and often preceding any of the other manifesta-tions [9]. All patients in this study had neurological signs atadmittance with seizure being mostly the main symptom(97% of patients in Group 1 and 92.8% in Group 2).
Since MRI is safe to use in pregnancy, its widespreadutilization enhanced the diagnosis of PRES in pregnantwomen with neurological Wndings. PRES is usually charac-terized by parietooccipital white matter edema on FLAIRMRI [13]. In our study, parieto-occipital edema was themostly detected area of involvement (72.9 and 78% ofwomen in Group 1 and Group 2, respectively), but otherless frequently involved areas such as temporal and frontallobes, cerebellum, periventricular, and supraventricularareas were detected. Only in one study [14], the obstetricpatients demonstrated involvement of the basal gangliamore often, but this was not observed in a larger study [15].
In previous studies, PRES was often reported to be areversible condition but in some cases, unfavorable out-comes arose after a correct treatment [6, 7]. The long-termpresence of brain lesion in formerly eclamptic women wasstudied [16]. It was found that 41% of formerly eclampticwomen demonstrated white matter lesions compared to17% of control women with an average of 5.3 years follow-ing a contemporaneous non-eclamptic pregnancy.
PRES can develop without a signiWcant elevation inblood pressure [9] like eclampsia can occur at blood pres-sures that are considered as normal. In cases with highblood pressure, the treatment should start with lowering theblood pressure. In this study, 20 of 68 (32.3%) eclampticwomen were normotansive (<140 mmHg systolic). It was alittle bit higher in other reports in which 6–16% of PRESpatients had normal blood pressure measurements [17]. Theoccurrence of cerebral edema and encephalopathy ineclamptic women with normal blood pressure suggests thatautoregulatory breakthrough is not mandatory but thesymptoms may be more related to either diminishedautoregulatory capacity, or enhanced BBB permeability, oreven a combination of both. In any case, the cerebral circu-lation is the primary eVector of the observed symptoms andthus central to the pathogenesis of eclampsia [18]. PREShas the same possible pathopysiological mechanismsdepending on the causative problem—breakdown of cere-bral autoregulation due to a rapid rise in blood pressureleading to disruption of the blood–brain barrier [5, 9, 12],endothelial dysfunction due to circulating toxins which ismore pertinent for triggers such as immunosuppressivetherapy, sepsis [9] and thirdly focal vasospasm leading todecreased blood Xow and ischemia with resultant edema[9, 12].
The treatment of seizure in eclamptic women is the mainstep of the treatment, where magnesium sulfate is the drugof choice although there are other antiedema medicationsthat can be considered (such as mannitol and dexametha-sone) [19]. The International Magpie Trial showed thatMgSO4 is the preferred safe medication for preventing sei-zures in eclamptic patients [20]. Its eVect in preeclampsiacould, in reality, be vasodilation with “PRES prevention”
Table 4 Symptoms of patients at admittance
Group1 (MgSO4) n (%)
Group 2 (mannitol) n (%)
Total n (%)
Seizure (tonic–clonic) 33 (97) 26 (92.8) 59 (95.1)
Headache 13 (38.2) 7 (25) 20 (32.2)
Blurred vision 5 (14.7) 6 (21.4) 11 (17.7)
Nausea and vomitting 0 (0) 5 (17.8) 6 (9.6)
Edema 3 (0.8) 0 (0) 1 (1.6)
Elevated blood pressure 1 (0.2) 0 (0) 1 (1.6)
Babinski sign patellar reXex 5 (14.7) 9 (32.1) 14 (22.5)
Table 5 Distribution of brain lesions in neuroimaging modalities(MRI, CT scan)
Group1 (MgSO4) n (%)
Group 2 (mannitol) n (%)
P value
MRI 31 (91.2) 26 (92.9)
Parietooccipital area 27 (72.9) 22 (78) 0.60
Occipital area 1 (2.7) 0 (0) 1.00
Cerebellum 3 (8.1) 2 (7.1) 1.00
Occipitotemporal area 0 (0) 1 (3.5) 0.43
Temporoparietal area 2 (5.4) 2 (7.1) 1.00
Periventpricular area 3 (8.1) 0 (0) 0.25
DiVuse 1 (2.7) 1 (3.5) 1.00
CT scan 3 (8.8) 2 (7.1)
Total 34 (100) 28 (100)
Table 6 The duration of hospitalization and prognosis of patients
a Median (min–max) ¡ IQRb Number (%)
Group 1 (MgSO4)
Group 2 (mannitol)
P value
Duration of hospitalization (day)a
4 (3–9) ¡ 2 7 (4–18) ¡ 3 <0.001
Prognosisb
Full recovery 33 (97.1%) 22 (78.6%) 0.039
Partial recovery 1 (2.9%) 6 (21.4%)
123

292 Arch Gynecol Obstet (2012) 286:287–293
[12]. Magnesium sulfate is known to decrease cerebraledema formation, protects blood–brain barrier [21]. Manni-tol can also be used as antiedema agent. Mannitol cannotcross the blood–brain barrier, but can lower intracranialpressure by decreasing the overall water content and cere-brospinal Xuid volume [22]. Mannitol can also increaseintravascular tonicity which causes its osmotic action [23].To the best of our knowledge, there exists no study wheremannitol was given to treat edema in PRES patients. In ourstudy, we did not observe any diVerence at worst bloodpressure change before and after treatment between magne-sium sulfate and mannitol groups. Although pretreatmentlocalization of leucoencephalopathy did not diVer betweenthe groups, the diVerence with respect to neurologicalrecovery was statistically signiWcant (p = 0.039). In themannitol treated group, 6 patients (21.4%) did not fullyrecover.
Magnesium sulfate treatment was concluded 48 h afteradministration but mannitol dosage was tapered in 6 days.The diVerence in duration of treatment between two groupsresulted in a signiWcant diVerence (p < 0.001) in hospital-ization time. The patients in the Wrst group were dischargedfrom the hospital between 3 and 9 days (median 4 days),whereas those in the second group were discahargedbetween 4 and 18 days (median 7 days.). Even though thelonger treatment and hospitalization duration cost extramoney, mannitol gives no additional contribution to prog-nosis. The symptoms of PRES usually seem to resolvewithin a week while recovery of the MRI abnormalitiestakes longer—several days to weeks, the treatment shouldfocus on the causative reason [9]. Almost all of the patientsin the Wrst group (97%) were fully recovered within 2 days,thus MgSO4 treatment accelerated the recovery time ofpatients with PRES.
In view of these considerations, posterior reversible leu-coencephalopthy should be considered in eclamptic patientin postpartum period. Magnesium sulfate treatment shouldstill be the Wrst line treatment strategy for pre(eclamptic)patients even with PRES. Mannitol does not additionallycontribute to prognosis of patients beside its longer treat-ment duration and additional costs.
The main drawback of this study is that it was a retro-spective study. Comparing the eVectiveness of mannitoland magnesium sulfate in a prospective study might givemore accurate results. However, in the literature, thereexists no study that evaluated a high number of obstetricpatients with PRES and thus is comparable to our studyon 62 patients. More in-depth future studies are requiredto determine what the main treatment strategy foreclamptic patients with PRES should be. Therefore, asobstetricians become more aware of this entity, studiesreporting alternative treatment strategies would beincreased.
Conclusion
Posterior reversible encephalopathy should be consideredin preeclamptic women having neurological Wndings.Increasing awareness of PRES among obstetricians’ isexpected to increase the detection rate of this probablyunder-recognized condition. Based on our Wndings, manni-tol does not seem to improve prognosis over that achievedwith magnesium sulfate. Unless future studies report other-wise, magnesium sulfate remains the treatment of choicefor eclamptic patients with PRES.
ConXict of interest None.
References
1. Sibai BM, Eclampsia VI (1990) Maternal-perinatal outcome in254 consecutive cases. Am J Obstet Gynecol 163:1049–1055
2. Chames MC, Livingston JC, Ivester TS, Barton JR, Sibai BH(2002) Late postpartum eclampsia: a preventable disease? Am JObstet Gynecol 186:1174–1177
3. Easton DJ (1998) Severe preeclampsia/eclampsia hypertensiveencephalopathy of pregnancy? Cerebrovasc Dis 8:53–58
4. Guyton AC (2006) Cerebral blood Xow, cerebrospinal Xuid andbrain metabolism. In: Gutyton AC (ed) Textbook of medical phys-iology, 11th edn. Elsevier Saunders, Philadelphia, pp 761–768
5. Schwartz RB, Jones KM, Kalina P, Bajakian RL, Mantello MT,Garada B et al (1992) Hypertensive encephalopathy: Wndings onCT, MR imaging, and SPECT imaging in 14 cases. AJR Am JRoentgenol 159:379–383
6. Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A et al(1996) A reversible posterior leukoencephalopathy syndrome.N Engl J Med 334:494–500
7. Servillo G, Striano P, Striano S, Tortora F, De Robertis E, RossanoF et al (2003) Posterior reversible encephalopathy syndrome(PRES) in obstetric critically ill patients. Intensive Care Med29:2323–2326
8. Antunes NL, Small TN, George D, Boulad F, Lis E (1999) Poster-ior leukoencephalopathy syndrome may not be reversible. PediatrNeurol 20:241–243
9. Roth C, Ferbert A (2011) The posterior reversible encephalopathysyndrome: what’s certain, what’s new? Pract Neurol 11:136–144
10. Casey SO, Sampaio RC, Michel E, Truwit CL (2000) Posteriorreversible encephalopathy syndrome: utility of Xuid-attenuatedinversion recovery MR imaging in the detection of cortical andsubcortical lesions. Am J Neuroradiol 21:1199–1206
11. Loureiro R, Leite CC, Kahhale S, Freire S, Sousa B, Cardoso EFet al (2003) DiVusion imaging may predict reversible brain lesionsin eclampsia and severe preeclampsia: initial experience. Am JObstet Gynecol 189:1350–1355
12. Bartynski WS (2008) Posterior reversible encephalopathysyndrome, part 2: controversies surrounding pathophysiology ofvasogenic edema. AJNR Am J Neuroradiol 29:1043–1049
13. Mckinney AM, Short J, Truwit LC, Mckinney ZJ, Kozak OS,SantaCruz KS et al (2007) Posterior reversible encephalopathysyndrome: incidence of atypical regions of involvement and imag-ing Wndings. Am J Radiol 189:904–912
14. Mueller-Mang C, Mang T, Pirker A, Klein K, Prchla C, Prayer D(2009) Posterior reversible encephalopathy syndrome: dopredisposing risk factors make a diVerence in MRI appearance?Neuroradiology 51:373–383
123

Arch Gynecol Obstet (2012) 286:287–293 293
15. Fugate JE, Claassen DO, Cloft HJ, Kallmes DF, Kozak OS, Rabin-stein AA (2010) Posterior reversible encephalopathy syndrome:associated clinical and radiologic Wndings. Mayo Clin Proc85:427–432
16. Aukes AM, de Groot JC, Aarnoudse JG, Zeeman GG (2009) Brainlesions several years after eclampsia. Am J Obstet Gynecol200(5):504 (e1–e5)
17. Mattar F, Sibai BM (2000) Eclampsia. VIII. Risk factors of mater-nal morbidity. Am J Obstet Gynecol 182:307–312
18. Cipolla MJ (2007) Cerebrovascular function in pregnancy andeclampsia. Hypertension 50:14–24
19. Narbone MC, Musolino R, Granata F, Mazzù I (2006) PRES: pos-terior or potentially reversible encephalopathy syndrome? NeurolSci 27:187–189
20. The Magpie Trial Collaborative Group (2002) Do women withpre-eclampsia, and their babes, beneWt from magnesium sulfate?The Magpie Trial: a randomised placebo-controlled trial. Lancet359:1877–1890
21. Euser AG, Cipolla MJ (2009) Magnesium sulfate for the treatmentof eclampsia. Stroke 40:1169–1175
22. Pollay M (1996) Blood–brain barrier, cerebral edema. In: WilkinsRH, Rengachary SS (eds) Neurosurgery, 2nd edn. Mc Graw HillBook Co., NewYork, pp 335–344
23. Donato T, Shapira Y, Artru A, Powers K (1994) EVect of mannitolon cerebrospinal Xuid dynamics and brain tissue edema. AnesthAnalg 78:58–66
123





























