Embed Size (px)
Citation preview

CPT
J
Ivfpatatnctt
msts
©3
T
omparison of the Molecular Adsorbent Recirculating System andlasmapheresis for Patients With Graft Dysfunction After Liverransplantation
.Y. Lee, S.B. Kim, J.W. Chang, S.-K. Park, S.-W. Kwon, K.W. Song, S. Hwang, and S.G. Lee
ABSTRACT
Background. Graft dysfunction after liver transplantation (OLT) is a life- threateningcondition. Molecular adsorbent recirculating system (MARS) or plasmapheresis (PLP)may be effective supportive therapy of graft dysfunction for patients who cannot undergoretransplantation. The aim of this study was to compare the effects of MARS and PLP inpatients with graft dysfunction after OLT.Methods. Between January 2002 and July 2007, 31 OLT recipients who experiencedgraft dysfunction, defined as hyperbilirubinemia (�10 mg/dL) without bile duct obstruc-tion and/or presence of hepatic encephalopathy, were treated with MARS or PLP.Biochemical and hemodynamic data and survival were compared in MARS and PLPgroups.Results. Fifteen patients were treated with 41 MARS sessions and 16 with 105 PLPsessions. After a single MARS session, patients showed significant reductions in creatinine,urea nitrogen, bilirubin, and ammonia. After a single PLP session, patients showedsignificant improvements in prothrombin time, bilirubin, alanine aminotransferase, alka-line phosphatase, and albumin. After the completion of treatment, Both MARS and PLPsignificantly improved bilirubin values. at 90 days there were no differences in overallsurvival rates; 53% in MARS versus 56% in PLP.Conclusion. Both MARS and PLP are alternative supportive treatments for graft
dysfunction after OLT.rl
wlgl
MLS(C
c
N RECENT YEARS, the results of liver transplantationhave improved markedly, with the current 5-year sur-
ival rates exceeding 70%.1 However, postoperative graftailure or primary nonfunction affects 7%–10% of trans-lantations, an important cause of posttransplant morbiditynd mortality.2 Despite advances in immunosuppressiveherapy and operative skills, few treatment options arevailable for patients with graft dysfunction. Retransplan-ation has improved patient prognosis, but all patients areot suitable for the procedure because of their seriousondition and the limited availability of grafts. Therefore,here is a need for artificial liver support systems to allowime for graft recovery or to find a suitable graft.
The molecular adsorbent recirculating system (MARS), aodified dialysis system, uses an albumin-enriched dialy-
ate that removes both albumin-bound and water-solubleoxins from the blood. The use of MARS has resulted in
ignificant improvements in biochemical and clinical pa- s2010 by Elsevier Inc. All rights reserved.60 Park Avenue South, New York, NY 10010-1710
ransplantation Proceedings, 42, 2625–2630 (2010)
ameters and short-term survival for patients with acuteiver failure3 and graft dysfunction after transplantation.4,5
Plasmapheresis (PLP) could be an adjunct for patientsith immune- mediated causes of graft dysfunction after
iver transplantation. For example, resistant hepatic allo-raft rejection and graft dysfunction and ABO-incompatibleiver transplants have been treated successfully with PLP.6,7
From the Division of Nephrology, Department of Internaledicine (J.Y.L., S.B.K., J.W.C., S.-K.P.), the Department of
aboratory Medicine (S.-W.K.), and the Division of Hepatobiliaryurgery and Liver Transplantation, Department of Surgery
K.W.S., S.H., S.G.L.), Asan Medical Center, University of Ulsan,ollege of Medicine, Seoul, Republic of Korea.Supported by Green Cross Company.Address reprint requests to Sung Gyu Lee, MD, Asan Medical
enter 388-1 Pungnap-dong, Songpa-gu, Seoul, Korea. E-mail:
[email protected]0041-1345/–see front matterdoi:10.1016/j.transproceed.2010.04.070
2625

Pcnbdtw
MP
Bpa3dba1
or
M
MbwSmaupit
(cpc�
R
2626 LEE, KIM, CHANG ET AL
LP may also have some benefit in the treatment of hepaticoma and nonimmune-mediated consequences of fulmi-ant liver failure.8 These observations have suggested thatoth MARS and PLP may be used in the treatment of graftysfunction after liver transplantation. We have retrospec-ively analyzed the effects of MARS and PLP in patientsith graft dysfunction after liver transplantation.
ATERIALS AND METHODSatients
etween January 2002 and July 2007, the medical records of 68atients who underwent extracorporeal liver support treatmentfter liver transplantation were retrospectively reviewed, showing1 patients receiving treatment because of graft dysfunction. Graftysfunction was defined as liver failure, including hyperbiliru-inemia (total bilirubin �10 mg/dL) without bile duct obstructionnd/or hepatic encephalopathy (grade �3). Among the 31 patients,5 underwent MARS and 16 PLP treatments. Liver biopsies were
Table 1. Baseline Characteristics of
MARS
Recipient characteristicsGender (male:female) 1Age (y) 49.7Cause of liver transplantation
HBV liver cirrhosisHBV hepatocellular carcinomaPrimary nonfunction of graftAlcoholic liver cirrhosisFulminant hepatitis
Cause of graft dysfunctionRejection 7
Acute rejectionChronic rejection
IschemiaPrimary nonfunction of graftHBV recurrence
Donor characteristicsAge (y) 36.2Graft weight ratio 1.07Types of donor
Living donorDual living donorCadavaric donor
Hemodialysis 10Vasopressor 7Sessions of treatment per patient 2.9Treatment days after LT (d) 39.3Laboratory findings
Serum bilirubin (mg/dL) 26.4Serum creatinine (mg/dL) 2.0INR 1.81Serum albumin (g/L) 3.2AST (IU/L) 850.7ALT (IU/L) 337.9Ammonia (�mol/L) 91.2
Abbreviations: AST, aspartate aminotransferase; ALT, alanine aminotransfer
atio; MARS, molecular adsorbent recirculating system; PLP, plasmapheresis.*Number and percentage or median and range.btained from all patients before treatment; no patient underwentetransplantation.
ethods
ARS was performed through a double-lumen catheter with alood flow of 200–250 mL/min for 6–8 hours. The MARS systemas coupled to a standard hemodialysis machine AK 95s (Gambro,tockholm, Sweden). The albumin dialysate circuit consisted of 600L of 20% human albumin with a circuit flow rate of 250 mL/min
nd a dialysate flow rate of 500 mL/min. No patient was anticoag-lated during MARS dialysis; 100–200 mL of saline washing waserformed every hour to prevent dialyzer clotting. Treatment
ntervals were every other day. Decisions on the continuation ofreatment were based on clinical status and laboratory findings.
PLP was performed using a centrifuge-driven cell separatorCobe Spectra, Gambro BCT, Lakewood, Co) via a double-lumenentral venous catheter. In a typical procedure, an average 1:1 ofatient plasma volume was exchanged with fresh frozen plasma byontinuous flow apheresis. If the serum albumin concentration was2.5 g/dL, fresh frozen plasma and 5% albumin were used as
ARS and PLP Treatment Groups*
15) PLP (n � 16) P
7:9 .06647.8 � 13.2 .627
82213
) 6 (38%) .72233730
33.6 � 7.9 .4226 1.08 � 0.19 .904
1321
) 8 (50%) .473) 6 (37%) .273
6.6 � 3.6 .002.3 38.8 � 36.7 .975
21.6 � 9.9 .0721.2 � 0.8 .011
8 1.62 � 0.41 .2443.1 � 0.2 .379
77.3 1273.2 � 3759.2 .7320.5 859.9 � 1707.0 .297.9 81.9 � 37.2 .507
BV, hepatitis B virus; LT, liver transplantation; INR, International Normalized
the M
(n �
2:3� 7.5
86100
(47%34521
� 8.5� 0.2
951
(67%(46%� 2.1� 53
� 8.8� 0.7� 0.4� 0.3� 29� 87� 59
ase; H
ruva3b
tbawi
S
DDamec
R
Facowmraihdc
gtMBM
bsber(scMp
bbccga
tasgdgPbt
B
H
M
MARS VS PLP IN GRAFT DYSFUNCTION 2627
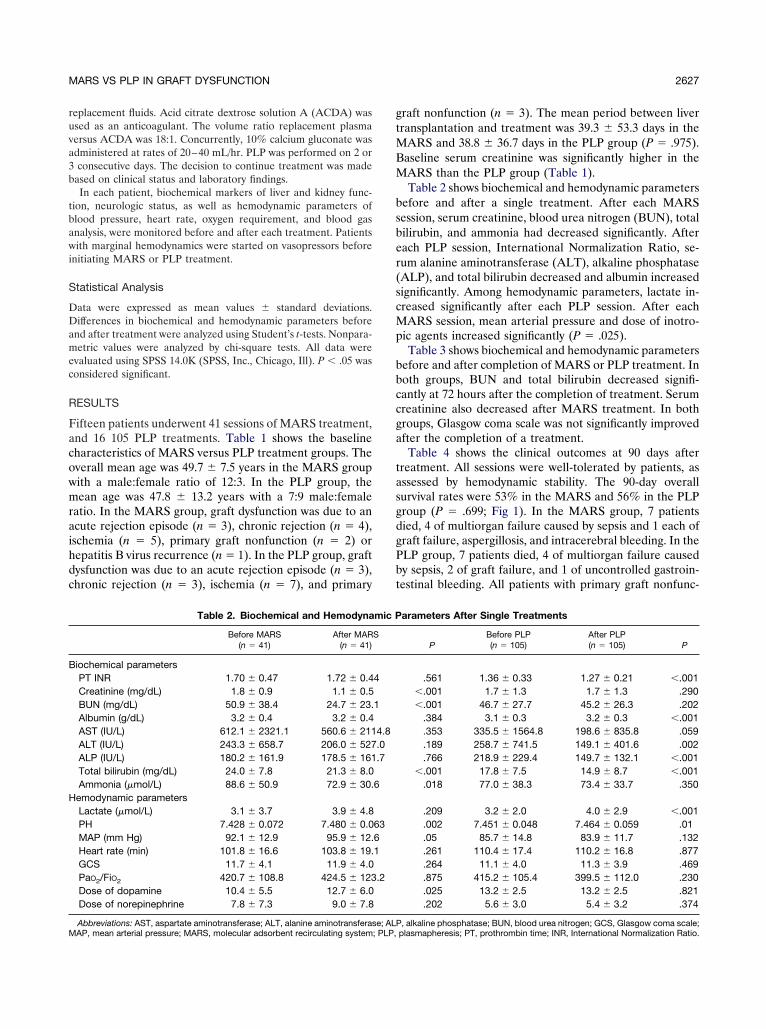
eplacement fluids. Acid citrate dextrose solution A (ACDA) wassed as an anticoagulant. The volume ratio replacement plasmaersus ACDA was 18:1. Concurrently, 10% calcium gluconate wasdministered at rates of 20–40 mL/hr. PLP was performed on 2 orconsecutive days. The decision to continue treatment was made
ased on clinical status and laboratory findings.In each patient, biochemical markers of liver and kidney func-
ion, neurologic status, as well as hemodynamic parameters oflood pressure, heart rate, oxygen requirement, and blood gasnalysis, were monitored before and after each treatment. Patientsith marginal hemodynamics were started on vasopressors before
nitiating MARS or PLP treatment.
tatistical Analysis
ata were expressed as mean values � standard deviations.ifferences in biochemical and hemodynamic parameters before
nd after treatment were analyzed using Student’s t-tests. Nonpara-etric values were analyzed by chi-square tests. All data were
valuated using SPSS 14.0K (SPSS, Inc., Chicago, Ill). P � .05 wasonsidered significant.
ESULTS
ifteen patients underwent 41 sessions of MARS treatment,nd 16 105 PLP treatments. Table 1 shows the baselineharacteristics of MARS versus PLP treatment groups. Theverall mean age was 49.7 � 7.5 years in the MARS groupith a male:female ratio of 12:3. In the PLP group, theean age was 47.8 � 13.2 years with a 7:9 male:female
atio. In the MARS group, graft dysfunction was due to ancute rejection episode (n � 3), chronic rejection (n � 4),schemia (n � 5), primary graft nonfunction (n � 2) orepatitis B virus recurrence (n � 1). In the PLP group, graftysfunction was due to an acute rejection episode (n � 3),hronic rejection (n � 3), ischemia (n � 7), and primary
Table 2. Biochemical and Hemodyna
Before MARS(n � 41)
After MAR(n � 41)
iochemical parametersPT INR 1.70 � 0.47 1.72 � 0.4Creatinine (mg/dL) 1.8 � 0.9 1.1 � 0.5BUN (mg/dL) 50.9 � 38.4 24.7 � 23.Albumin (g/dL) 3.2 � 0.4 3.2 � 0.4AST (IU/L) 612.1 � 2321.1 560.6 � 211ALT (IU/L) 243.3 � 658.7 206.0 � 527ALP (IU/L) 180.2 � 161.9 178.5 � 161Total bilirubin (mg/dL) 24.0 � 7.8 21.3 � 8.0Ammonia (�mol/L) 88.6 � 50.9 72.9 � 30.
emodynamic parametersLactate (�mol/L) 3.1 � 3.7 3.9 � 4.8PH 7.428 � 0.072 7.480 � 0.0MAP (mm Hg) 92.1 � 12.9 95.9 � 12.Heart rate (min) 101.8 � 16.6 103.8 � 19.GCS 11.7 � 4.1 11.9 � 4.0PaO2/FiO2 420.7 � 108.8 424.5 � 123Dose of dopamine 10.4 � 5.5 12.7 � 6.0Dose of norepinephrine 7.8 � 7.3 9.0 � 7.8
Abbreviations: AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALPAP, mean arterial pressure; MARS, molecular adsorbent recirculating system; PLP,
raft nonfunction (n � 3). The mean period between liverransplantation and treatment was 39.3 � 53.3 days in the
ARS and 38.8 � 36.7 days in the PLP group (P � .975).aseline serum creatinine was significantly higher in theARS than the PLP group (Table 1).Table 2 shows biochemical and hemodynamic parameters
efore and after a single treatment. After each MARSession, serum creatinine, blood urea nitrogen (BUN), totalilirubin, and ammonia had decreased significantly. Afterach PLP session, International Normalization Ratio, se-um alanine aminotransferase (ALT), alkaline phosphataseALP), and total bilirubin decreased and albumin increasedignificantly. Among hemodynamic parameters, lactate in-reased significantly after each PLP session. After each
ARS session, mean arterial pressure and dose of inotro-ic agents increased significantly (P � .025).Table 3 shows biochemical and hemodynamic parameters
efore and after completion of MARS or PLP treatment. Inoth groups, BUN and total bilirubin decreased signifi-antly at 72 hours after the completion of treatment. Serumreatinine also decreased after MARS treatment. In bothroups, Glasgow coma scale was not significantly improvedfter the completion of a treatment.
Table 4 shows the clinical outcomes at 90 days afterreatment. All sessions were well-tolerated by patients, asssessed by hemodynamic stability. The 90-day overallurvival rates were 53% in the MARS and 56% in the PLProup (P � .699; Fig 1). In the MARS group, 7 patientsied, 4 of multiorgan failure caused by sepsis and 1 each ofraft failure, aspergillosis, and intracerebral bleeding. In theLP group, 7 patients died, 4 of multiorgan failure causedy sepsis, 2 of graft failure, and 1 of uncontrolled gastroin-estinal bleeding. All patients with primary graft nonfunc-
arameters After Single Treatments
PBefore PLP(n � 105)
After PLP(n � 105) P
.561 1.36 � 0.33 1.27 � 0.21 �.001�.001 1.7 � 1.3 1.7 � 1.3 .290�.001 46.7 � 27.7 45.2 � 26.3 .202
.384 3.1 � 0.3 3.2 � 0.3 �.001
.353 335.5 � 1564.8 198.6 � 835.8 .059
.189 258.7 � 741.5 149.1 � 401.6 .002
.766 218.9 � 229.4 149.7 � 132.1 �.001�.001 17.8 � 7.5 14.9 � 8.7 �.001
.018 77.0 � 38.3 73.4 � 33.7 .350
.209 3.2 � 2.0 4.0 � 2.9 �.001
.002 7.451 � 0.048 7.464 � 0.059 .01
.05 85.7 � 14.8 83.9 � 11.7 .132
.261 110.4 � 17.4 110.2 � 16.8 .877
.264 11.1 � 4.0 11.3 � 3.9 .469
.875 415.2 � 105.4 399.5 � 112.0 .230
.025 13.2 � 2.5 13.2 � 2.5 .821
.202 5.6 � 3.0 5.4 � 3.2 .374
mic P
S
4
1
4.8.0.7
6
6361
.2
, alkaline phosphatase; BUN, blood urea nitrogen; GCS, Glasgow coma scale;plasmapheresis; PT, prothrombin time; INR, International Normalization Ratio.

t3g
D
Gmpvpbsepatbv
vM8tdrs
tppept
MpbmitpiPtcsP
F
PCBAAATALMG
R system
MC
m
2628 LEE, KIM, CHANG ET AL
ion died, despite extracorporeal liver support treatment, at–6 days in the MARS group and at 7–12 days in the PLProup (Table 5).
ISCUSSION
raft dysfunction is associated with increased postoperativeorbidity and mortality. The conventional treatment of
rimary graft dysfunction has been retransplantation. Pre-ious studies have suggested that MARS effectively sup-orted graft dysfunction with improvements in hyperbiliru-inemia and hepatic encephalopathy.4,9–11 One reporthowed MARS dialysis to improve hyperbilirubinemia andncephalopathy owing to chronic rejection after liver trans-lantation.12 Recently, PLP has shown encouraging resultss a temporary liver support for graft dysfunction after liverransplantation with correction of coagulopathy and hyper-ilirubinemia.13,14 However, whether PLP provides a sur-ival benefit for graft dysfunction patients was uncertain.15
Previous studies have reported a 50%–60% overall sur-ival rate among patients with graft dysfunction undergoingARS treatments without retransplantation10,11 and 60%–
0%, after PLP treatments with or without retransplanta-ion.13,14 We observed that the 90-day overall survival rateid not differ between MARS and PLP groups withoutetransplantation (53% vs 56%, respectively). The presenttudy showed a greater mortality rate among the patients
Table 3. Comparison of Biochemical and Hemodynamic Param
Before MARS72 Hours After
All Sessions of MAR
T INR 1.73 � 0.48 1.50 � 0.44reatinine (mg/dL)* 1.88 � 0.7 1.37 � 0.4UN (mg/dL) 55.6 � 39.1 38.7 � 27.2lbumin (g/dL) 3.2 � 0.3 3.3 � 0.5LT (IU/L) 114.9 � 870.5 121.5 � 287.7LP (IU/L) 180.7 � 170.0 205.9 � 157.1otal bilirubin (mg/dL) 27.6 � 8.8 23.3 � 8.1mmonia (�mol/L) 83.2 � 59.9 77.0 � 43.1actate (�mol/L) 3.0 � 1.2 4.0 � 4.7AP (mm Hg) 89.6 � 13.5 92.4 � 16.0CS 12.4 � 4.1 12.9 � 4.1
Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; BUatio; MAP, mean arterial pressure; MARS, molecular adsorbent recirculating*P � .05 compared with before treatment.
Table 4. Clinical Outcomes After 90 Days
MARS(n � 15)
PLP(n � 16)
ortality rate 47% (7/15) 43% (7/16)auses of deathSepsis 4 4Bleeding — 1Graft failure 1 2Aspergillosis 1 —Intracerebral bleeding 1 —
uAbbreviations: MARS, molecular adsorbent recirculating system; PLP, plas-apheresis.
han observed in previous studies, because we excludedatients who had received retransplantations. Since retrans-lantation is beneficial for patients with graft dysfunction,specially primary nonfunction grafts, the exclusion ofatients receiving retransplantation caused a higher mor-ality rate in this study.
Consistent with previous reports, we noted that bothARS and PLP decreased total bilirubin among graft
atients with dysfunction.4,5,10,11,13,14,16,17 Hyperbiliru-inemia itself does not cause multiple organ failure, butay represent an important cofactor potentiating other
nsults, such as infection, rejection, or operative complica-ions. In addition, bilirubin has neurotoxic and encephalo-athic effects.18 However, we did not observe improvement
n neurologic status or ammonia level after either MARS orLP, in contrast with previous reports showing that both
reatments improved neurological status.4,5,10,19–21 This dis-repancy may be due to the large number of patients in ourtudy who received mechanical ventilation and sedatives.revious studies have shown various findings on the effect
ig 1. Comparison of 90-day overall survival rates of patients
s Before and After Completion of MARS and PLP Treatment
P Before PLP72 Hours After
All Sessions of PLP P
.005 1.52 � 0.41 1.63 � 0.66 .740
.019 1.3 � 0.8 1.4 � 0.9 .647
.05 50.6 � 25.1 41.7 � 26.7 .034
.538 3.1 � 0.2 3.2 � 0.4 .538
.745 581.5 � 1292.5 119.3 � 115.3 .223
.144 383.5 � 475.4 187.0 � 96.3 .138
.006 23.7 � 9.9 15.3 � 8.7 �.001
.682 73.3 � 37.2 74.1 � 34.9 .950
.582 2.6 � 1.5 3.9 � 7.9 .523
.340 83.8 � 14.0 80.3 � 12.0 .542
.640 10.7 � 4.0 12.0 � 4.1 .286
od urea nitrogen; GCS, Glasgow Coma Scale; INR, International Normalization; PLP, plasmapheresis; PT, prothrombin time.
eter
S
N, blo
ndergoing MARS and PLP treatment.

otdtMawcwpiBa
tttwatMMs
ptoia
tMgthsen1Patlt
R
D
L
H
feraseN
MARS VS PLP IN GRAFT DYSFUNCTION 2629
f MARS on serum ammonia concentrations.3,9,10,16 Al-hough we observed that each MARS session significantlyecreased serum ammonia concentrations, it was not sus-ained after the completion of the MARS treatment.
ARS also did not improve ammonia concentrationsmong patients with hyperacute hepatic failure3 or thoseith liver failure admitted to the intensive care unit whoould not receive a liver transplantation.16 Our patientsere susceptible to hyperammonemia resulting from he-atic failure owing to graft dysfunction, were receiving
mmunosuppressive agents and suffering sepsis or bleeding.ecause ammonia is dialyzable, MARS treatment immedi-tely decreased these levels, but it could not maintain them.
Renal dysfunction either as acute kidney injury or hepa-orenal syndrome is a common complication among pa-ients with hepatic graft dysfunction. We found that MARSreatment decreased creatinine levels, a finding consistentith previous reports,10,22 whereas PLP treatment did notffect them. Because some patients received hemodialysisreatments during MARS or PLP treatments (67% in
ARS vs 50% in PLP), our data have limitations. However,ARS treatment may support kidney function by removing
Table 5. Comparison of Characteristics and Parameters Bet
MARS
Survivor (n � 8) Nonsurvivor (
ecipient characteristicsGender (male:female) 8:0 4:3Age (y) 48.1 � 6.6 51.4 � 8Cause of graft dysfunction
Rejection 5 (63%) 2 (29%Acute rejection 1 2Chronic rejection 4 0
Ischemia 2 3Primary nonfunction 0 2HBV recurrence 1 0Hemodialysis 4 (50%) 6 (86%
onor characteristicsGender (male:female) 5:3 4:3Donor age (y) 33.9 � 9.9 39.0 � 6Graft weight ratio 1.08 � 0.21 1.07 � 0
aboratory findingsSerum bilirubin (mg/dL) 28.9 � 7.7 23.6 � 9Serum creatinine (mg/dL) 2.1 � 0.6 1.7 � 0INR 1.68 � 0.44 1.94 � 0Serum albumin (g/L) 3.2 � 0.3 3.3 � 0AST (IU/L) 79.4 � 57.1 1732.3 � 2ALT (IU/L) 118.4 � 101.4 588.8 � 1Ammonia (�mol/L) 90.3 � 60.3 98.8 � 6emodynamic parametersLactate (�mol/L) 2.7 � 1.2 3.1 � 1pH 7.449 � 0.012 7.425 � 0MAP (mm Hg) 93.9 � 5.8 84.8 � 1Heart rate (/min) 106.4 � 16.5 108.6 � 1GCS 14.1 � 1.2 9.0 � 4PaO2/FiO2 258.8 � 158.1 377.9 � 1
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransormalization Ratio; MAP, mean arterial pressure.
mall molecules and supporting liver function. M
We also noted that PLP transiently corrected coagulopathy,erhaps by replacing clotting factors. PLP has also been showno dilute serum aminotransferases and bilirubin.23 Indeed, webserved that ALT, ALP, and total bilirubin concentrations
mproved after every PLP session, but were not maintainedfter completion of PLP except for the bilirubin.
This study had 2 limitations. The first was its retrospec-ive design, which may have biased comparisons between
ARS and PLP. The serum creatinine levels of the MARSroup were higher than those of the PLP group suggestinghat MARS tended to be preferred to PLP when patientsad renal dysfunction. Furthermore there were more PLPessions than MARS treatments. Because MARS is morexpensive than PLP ($4185 vs $957, with neither covered byational insurance) and required a much longer time (6 vs.5 hours), it may be difficult to maintain as many MARS asLP sessions. The second limitation of our study was thatll patients with primary graft nonfunction died, irrespec-ive of that treatment method, indicating that the cause ofiver dysfunction may have a greater effect on outcomeshan the treatment method.
In conclusion, among patients with graft dysfunction
Survivors and Nonsurvivors in the MARS and PLP Groups
PLP
) P Survivor (n � 9) Nonsurvivor (n � 7) P
.077 4:5 3:4 .949
.420 48.4 � 11.6 46.9 � 15.9 .821
.722 3 (33%) 3 (42%) .8561 22 16 10 30 0
.282 3 (33%) 5 (71%) .315
.736 4:5 5:3 .809
.301 35.6 � 4.8 31.0 � 10.6 .296
.949 1.07 � 0.11 1.11 � 0.27 .721
.250 20.3 � 8.1 23.2 � 12.4 .581
.407 1.4 � 0.9 1.0 � 0.7 .363
.314 1.39 � 0.16 1.91 � 0.44 .022
.256 3.2 � 0.3 3.1 � 0.2 .278
.354 113.8 � 103.4 2764.0 � 5541.1 .253
.366 148.4 � 125.6 1774.7 � 2351.1 .117
.814 80.3 � 26.1 83.4 � 48.0 .882
.547 2.2 � 1.4 3.6 � 1.3 .110
.596 7.403 � 0.045 7.468 � 0.036 .021
.246 87.4 � 15.9 80.1 � 11.4 .324
.795 103.9 � 23.2 113.9 � 14.2 .343
.023 12.9 � 2.8 8.7 � 4.2 .033
.479 449.7 � 77.3 430.7 � 103.1 .736
; GCS, Glasgow Coma Scale; HBV, hepatitis B virus; INR, International
ween
n � 7
.7
)
)
.5
.33
.6
.8
.52
.2977.3272.21.6
.2
.0598.33.4.592.2
ARS treatments improved hyperbilirubinemia and co-

aTMm
R
ot
fa
nlc
ra2
mlc
ap
eAT
p1
se
tM
bft4
dr
at
p3
p1
ae
ec2
tw
pl
al
ea
sP
2630 LEE, KIM, CHANG ET AL
gulopathy; PLP treatments improved hyperbilirubinemia.he 90-day overall survival rates were similar in both theARS and PLP groups, suggesting that both treatmentsay support graft dysfunction after liver transplantation.
EFERENCES
1. Bismuth H, Farges O, Castaing D, et al: [Evaluation of resultsf liver transplantation: experience based on a series of 1052ransplantations]. Presse Med 24:1106, 1995
2. Ploeg RJ, D’Alessandro AM, Knechtle SJ, et al: Risk factorsor primary dysfunction after liver transplantation—a multivariatenalysis. Transplantation 55:807, 1993
3. Schmidt LE, Wang LP, Hansen BA, et al: Systemic hemody-amic effects of treatment with the molecular adsorbents recircu-
ating system in patients with hyperacute liver failure: a prospectiveontrolled trial. Liver Transpl 9:290, 2003
4. Hetz H, Faybik P, Berlakovich G, et al: Molecular adsorbentecirculating system in patients with early allograft dysfunctionfter liver transplantation: a pilot study. Liver Transpl 12:1357,0065. Kellersmann R, Gassel HJ, Buhler C, et al: Application ofolecular adsorbent recirculating system in patients with severe
iver failure after hepatic resection or transplantation: initial single-entre experiences. Liver 22(suppl 2):56, 2002
6. Evrard HM, Miller C, Schwartz M, et al: Resistant hepaticllograft rejection successfully treated with cyclophosphamide andlasmapheresis. Transplantation 50:702, 19907. Mor E, Skerrett D, Manzarbeitia C, et al: Successful use of an
nhanced immunosuppressive protocol with plasmapheresis forBO-incompatible mismatched grafts in liver transplant recipients.ransplantation 59:986, 19958. Buckner CD, Clift RA, Volwiler W, et al: Plasma exchange in
atients with fulminant hepatic failure. Arch Intern Med 132:487,9739. Chiu A, Chan LM, Fan ST: Molecular adsorbent recirculating
ystem treatment for patients with liver failure: the Hong Kongxperience. Liver Int 26:695, 2006
10. Steiner C, Mitzner S: Experiences with MARS liver support
herapy in liver failure: analysis of 176 patients of the InternationalARS Registry. Liver 22(suppl 2):20, 2002sS
11. Gaspari R, Cavaliere F, Sollazzi L, et al: Molecular adsor-ent recirculating system (MARS) in patients with primary non-unction and other causes of graft dysfunction after liver transplan-ation in the era of extended criteria donor organs. Transplant Proc1:253, 200912. Schachschal G, Morgera S, Kupferling S, et al: MARS
ialysis in the state of chronic rejection in a liver transplantecipient. Am J Gastroenterol 97:1059, 2002
13. Mandal AK, King KE, Humphreys SL, et al: Plasmapheresis:n effective therapy for primary allograft nonfunction after liverransplantation. Transplantation 70:216, 2000
14. Camci C, Akdogan M, Gurakar A, et al: The impact of totallasma exchange on early allograft dysfunction. Transplant Proc6:2567, 200415. Skerrett D, Mor E, Curtiss S, et al: Plasmapheresis in
rimary dysfunction of hepatic transplants. J Clin Apher 11:10,99616. Gaspari R, Avolio AW, Zileri Dal Verme L, et al: Molecular
dsorbent recirculating system in liver transplantation: safety andfficacy. Transplant Proc 38:3544, 2006
17. Kawagishi N, Ohkohchi N, Fujimori K, et al: Indications andfficacy of apheresis for liver transplant recipients: experience of 16ases in 34 living-related liver transplants. Transplant Proc 32:2111,00018. Morimoto T, Matsushima M, Sowa N, et al: Plasma adsorp-
ion using bilirubin-adsorbent materials as a treatment for patientsith hepatic failure. Artif Organs 13:447, 198919. Bektas M, Idilman R, Soykan I, et al: Adjuvant therapeutic
lasma exchange in liver failure: assessments of clinical andaboratory parameters. J Clin Gastroenterol 42:517, 2008
20. Novelli G, Rossi M, Pretagostini R, et al: MARS (moleculardsorbent recirculating system): experience in 34 cases of acuteiver failure. Liver 22(suppl 2):43, 2002
21. Ozdemir FN, Tutal E, Sezer S, et al: Effect of supportivextracorporeal treatment in liver transplantation recipients anddvanced liver failure patients. Hemodial Int 10(suppl 2):S28, 2006
22. Novelli G, Rossi M, Pretagostini M, et al: One hundredixteen cases of acute liver failure treated with MARS. Transplantroc 37:2557, 200523. Singer AL, Olthoff KM, Kim H, et al: Role of plasmaphere-
is in the management of acute hepatic failure in children. Annurg 234:418, 2001