Embed Size (px)
Citation preview
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
55 Emergency (2016); 4 (2): 55-64
REVIEW ARTICLE
Comparison of Ultrasonography and Radiography in Detection of Thoracic
Bone Fractures; a Systematic Review and Meta-Analysis
Mahmoud Yousefifard1, Masoud Baikpour2, Parisa Ghelichkhani3, Hadi Asady4, Abolfazl Darafarin5,
Mohammad Reza Amini Esfahani5, Mostafa Hosseini6, 7*, Mehdi Yaseri6, Saeed Safari5
1. Department of Physiology, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran. 2. Department of Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
3. Department of Intensive Care Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran. 4. Department of Occupational Health Engineering, Faculty of Public Health, Tehran University of Medical Sciences, Tehran, Iran. 5. Department of Emergency Medicine, Shohadaye Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
6. Sina Trauma and Surgery Research Center, Tehran University Medical Sciences, Tehran, Iran. 7. Department of Epidemiology and Biostatistics, school of Public Health, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Mostafa Hosseini, Department of Epidemiology and Biostatistics School of Public Health, Tehran University of Medical Sciences,
Poursina Ave, Tehran, Iran; Email: [email protected]; Tel: +982188989125; Fax: +982188989127. Received: June 2015; Accepted: August 2015
Abstract
Introduction: The potential benefit of ultrasonography for detection of thoracic bone fractures has been proven
in various surveys but no comprehensive conclusion has been drawn yet; therefore, the present study aimed to
conduct a thorough meta-analytic systematic review on this subject. Methods: Two reviewers independently car-
ried out a comprehensive systematic search in Medline, EMBASE, ISI Web of Knowledge, Scopus, Cochrane Library,
and ProQuest databases. Data were summarized as true positive, false positive, true negative and false negative
and were analyzed via STATA 11.0 software using a mixed-effects binary regression model. Sources of heterogene-
ity were further assessed through subgroup analysis. Results: Data on 1667 patients (807 subjects with and 860
cases without thoracic fractures), whose age ranged from 0 to 92 years, were extracted from 17 surveys. Pooled
sensitivity and specificity of ultrasonography in detection of thoracic bone fractures were 0.97 (95% CI: 0.90-0.99;
I2= 88.88, p<0.001) and 0.94 (95% CI: 0.86-0.97; I2= 71.97, p<0.001), respectively. The same measures for chest
radiography were found to be 0.77 (95% CI: 0.56-0.90; I2= 97.76, p<0.001) and 1.0 (95% CI: 0.91-1.00; I2= 97.24,
p<0.001), respectively. The sensitivity of ultrasonography was higher in detection of rib fractures, compared to
fractures of sternum or clavicle (97% vs. 91%). Moreover, the sensitivity was found to be higher when the proce-
dure was carried out by a radiologist in comparison to an emergency medicine specialist (96% vs. 90%). Conclu-
sion: Base on the findings of the present meta-analysis, screening performance characteristic of ultrasonography
in detection of thoracic bone fractures was found to be higher than radiography. However, these characteristics
were more prominent in detection of rib fractures and in cases where was performed by a radiologist.
Key words: Thoracic fractures; ultrasonography; radiography; diagnostic tests, routine
Cite this article as: Yousefifard M, Baikpour M, Ghelichkhani P, et al. Comparison of ultrasonography and radiography in detec-tion of thoracic bone fractures; a systematic review and meta-analysis. Emergency. 2016; 4(2):55-64.
Introduction: arly diagnosis of rib fractures can rapidly indicate
the source of thoracic pain and be helpful in pain
management of trauma patients. Other than pain,
rib fractures have been reported to be associated with
morbidity and mortality in elderly patients (3-5). In
most emergency departments, ultrasonography is con-
sidered as one of the most useful screening tools for
rapid evaluation of trauma patients (6). Application of
ultrasonography for assessment of chest wall injuries
has been reported from 1980s (7). Since then the tech-
nology of ultrasound devices has significantly improved
so that images with higher resolutions are obtained. In
light of these improvements, the diagnostic value of this
modality has been considerably enhanced (9). In this re-
gard, studies have illustrated a considerably high diag-
nostic value of ultrasonography in detection of thoracic
fractures, even higher than that of chest radiography (8,
10-12). For instance in his narrative review, Chan re-
ferred to ultrasonography as a reliable diagnostic tool
E
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
Yousefifard et al 56
for detection of thoracic bone fractures (13). Neverthe-
less, still no comprehensive review has been carried out
comparing the diagnostic values of chest ultrasonogra-
phy and radiography in detection of thoracic fractures.
One solution is to perform a meta-analysis on the availa-
ble evidence (15, 16). Accordingly, the present system-
atic review and meta-analysis aimed to determine the di-
agnostic values of chest ultrasonography and radiog-
raphy in detection of thoracic bone fractures.
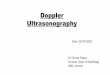
Methods: Search strategy and selection criteria The study protocol was established based on the guide-lines of Meta-analysis of Observational Studies in Epide-miology statement (MOOSE) (19). After selection of key-words from Medical Subject Heading (MeSH) terms and EMTREE, two reviewers (M.Y, P.G) independently car-ried out an extended systematic search in databases of Medline (via PubMed), EMBASE (via OvidSP), ISI Web of Knowledge, Scopus, Cochrane Library, and ProQuest
without any time or language limitations. The keywords included “Ultrasonography” OR “Sonography” OR “Ultra-sound” OR “Radiography” OR “Chest Film” OR “Chest Ra-diograph” combined with “Rib Fractures” OR “Chest Wall Fracture” OR “Sternum Fracture” OR “Sternal Fracture” OR “Clavicle Fracture” OR “Scapula Fracture”. Addition-ally, the bibliographies of original and review articles as well as Google Scholar were also searched. All the studies evaluating the diagnostic accuracy of ultrasonography or chest radiography in detection of chest wall fractures were assessed. Review and editorial articles, case re-ports and studies with sample populations of less than 10 patients were excluded. Data extraction Two reviewers (M.Y, P.G) independently worked on summarizing the data regarding assessing quality of studies, baseline characteristics of patients (age, gender, the number of patients with and without hemothorax, the etiology of hemothorax), the characteristics of ultra-sonography device (transducer, frequency), physicians in charge of imaging interpretation, blinding status, sam-pling method (consecutive, convenience), study design
Figure 1: Flowchart of the study.
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
57 Emergency (2016); 4 (2): 55-64
Ta
ble
1: C
har
ecte
rist
ics
of
incl
ud
ed s
tud
ies
Stu
dy
N
o. o
f p
ati
en
t (+
/ -
) A
ge
1 (
ye
ars
) M
ale
(%
) R
efe
ren
ce /
In
de
x
Tra
nsd
uce
r /
Op
era
tor
Sa
mp
lin
g /
F
ract
ure
W
ea
kn
ess
es
He
nd
rich
1
99
5 (
1)
15
/ 3
0
45
(2
9-6
1)
57
.8
CX
R /
US
7.5
MH
z /
R
adio
logi
st
Co
nv
enie
nce
/
ster
nu
m
Lo
w s
amp
le s
ize
Po
ssib
ilit
y o
f se
lect
ion
bia
s
En
gin
20
00
(2
) 1
8 /
5
35
.4 (
18
-75
) 8
2.6
C
XR
/ U
S 7
.5 M
Hz
/
Rad
iolo
gist
C
on
ven
ien
ce /
St
ern
um
Ret
rosp
ecti
ve
des
ign
L
ow
sam
ple
siz
e P
oss
ibil
ity
of
sele
ctio
n b
ias
Hu
rle
y 2
00
4
(8)
15
/ 5
3
1 (
16
-55
) 7
8.6
C
T /
US,
CX
R
12
.5 M
Hz
/
Rad
iolo
gist
C
on
secu
tiv
e /
Rib
L
ow
sam
ple
siz
e
Ra
ine
r 2
00
4
(11
) 7
6 /
12
51
± 1
9
59
C
T /
US,
CX
R
5-t
o 1
0-M
Hz
/ R
adio
logi
st
Co
nv
enie
nce
/
Ster
nu
m
Jin
20
06
(1
0)
23
/ 1
6
45
.2 (
15
-82
) 5
2
CT
/ U
S, C
XR
5
-to
9-M
Hz
/ R
a-d
iolo
gist
C
on
ven
ien
ce /
M
ult
iple
L
ow
sam
ple
siz
e P
oss
ibil
ity
of
sele
ctio
n b
ias
Tra
ub
20
07
(1
4)
68
/ 7
3
47
.2 (
18
-89
) 7
5
CT
/ C
XR
N
A /
R
adio
logi
st
Co
nv
enie
nce
/
Rib
R
etro
spec
tiv
e d
esig
n
Po
ssib
ilit
y o
f se
lect
ion
bia
s W
oo
tto
n-
Go
rge
s 2
00
8 (
17
) 1
31
/ 9
4
0.2
(0
.1-0
.5)
4
1.7
C
T /
CX
R
NA
/
Rad
iolo
gist
C
on
secu
tiv
e /
Rib
Ret
rosp
ecti
ve
des
ign
P
oss
ibil
ity
of
sele
ctio
n b
ias
Lo
w s
amp
le s
ize
Cro
ss 2
01
0
(18
) 4
3 /
57
10
.7 (
1-1
7)
87
.3
CX
R /
US
10
- to
15
-MH
z/
EP
C
on
ven
ien
ce /
C
lav
icle
P
oss
ibil
ity
of
sele
ctio
n b
ias
We
inb
erg
2
01
0 (
20
) 2
5 /
18
7
13
(3
-23
) N
R
CT
/ U
S 7
.5-
to 1
0-M
Hz/
E
P
Co
nv
enie
nce
/
Cla
vic
le a
nd
rib
P
oss
ibil
ity
of
sele
ctio
n b
ias
Yo
u 2
01
0
(21
) 2
4 /
12
4
3 (
8-7
3)
52
.8
CT
/ U
S 7
-to
12
-MH
z /
Rad
iolo
gist
C
on
secu
tiv
e /
Rib
L
ow
sam
ple
siz
e
Szu
cs-F
ar-
ka
s 2
01
1
(22
) 3
9 /
24
64
.4 ±
14
.7
73
C
T /
CX
R
NA
/
Rad
iolo
gist
C
on
ven
ien
ce /
R
ib
Ret
rosp
ecti
ve
des
ign
L
ow
sam
ple
siz
e P
oss
ibil
ity
of
sele
ctio
n b
ias
Ya
zka
n
20
12
(2
3)
83
/ 8
3
40
.8 (
16
-92
) 7
3.5
C
T /
CX
R
NA
/
Surg
eon
C
on
secu
tiv
e /
Rib
R
etro
spec
tiv
e d
esig
n
Bła
siń
ska
2
01
3 (
24
) 3
4 /
26
N
R
NR
C
T /
CX
R
NA
/
Rad
iolo
gist
C
on
secu
tiv
e /
Mu
ltip
le
Lo
w s
amp
le s
ize
Ch
ard
oli
2
01
3 (
25
) 5
1 /
14
9
37
.9 (
16
- 9
0)
84
C
T /
CX
R
NA
/ E
P
Co
nv
enie
nce
/
Rib
Th
e in
terp
reta
tio
n o
f th
e C
XR
an
d C
T w
ere
no
t in
bli
nd
fas
hio
n
Po
ssib
le s
elec
tio
n b
ias
U
zun
20
13
(1
2)
92
/ 8
2
8 (
15
- 4
0)
73
C
T /
US,
CX
R
NR
/
Rad
iolo
gist
C
on
secu
tiv
e /
Rib
P
oss
ibil
ity
of
rep
ort
ing
bia
s
Ho
ffst
ett
er
20
14
(2
6)
15
/ 2
4
61
(2
4-8
7)
60
.7
CT
/ C
XR
N
A /
R
adio
logi
st
Co
nse
cuti
ve
/ M
ult
iple
R
etro
spec
tiv
e d
esig
n
Lo
w s
amp
le s
ize
Pa
rk 2
01
5
(27
) 5
5 /
55
5
6.2
(1
6.9
) 5
7.4
C
T /
CX
R
NA
/
Rad
iolo
gist
C
on
secu
tiv
e /
Rib
L
ow
sam
ple
siz
e
1, (
+ /
-):
nu
mb
er o
f p
atie
nt
wit
h f
ract
ure
/ n
um
ber
of
pa
tien
t w
ith
ou
t fr
actu
re; 2
, Nu
mb
er a
re p
rese
nte
d a
s m
ean
± s
tan
dar
d d
evia
tio
n o
r (r
ange
).
CT
: Co
mp
ute
d t
om
og
rap
hy
; CX
R: C
hes
t ra
dio
gra
ph
y; E
P:
Em
erge
ncy
ph
ysi
cian
; NA
: No
t ap
pli
cab
le;
NR
: No
t R
epo
rted
; US:
Ult
raso
no
gra
ph
y.

This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
Yousefifard et al 58
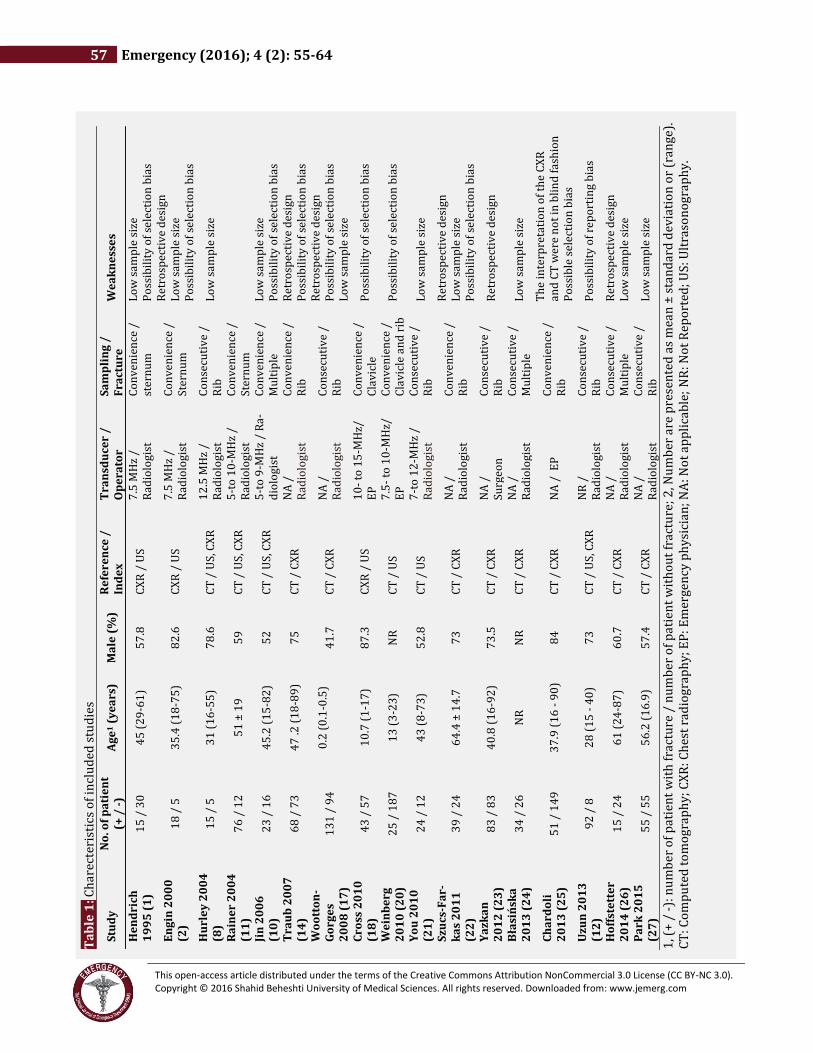
(retrospective, prospective). Finally the number of true positive (TP), true negative (TN), false positive (FP), and false negative (FN) cases were extracteded. Disagree-ments were discussed with the third reviewer (M.H) and a solution was proposed. In cases of data inaccessibility, the corresponding authors of the articles were con-tacted. Data presented as charts were extracted via the method proposed by Sistrom and Mergo (28). In cases where only the sensitivity and specificity were pre-sented, reliable web-based programs were used to calcu-late the number of TP, TN, FP, and FN cases. Quality assessment Quality of the studies were assessed based on the guide-lines of 14-Item Quality Assessment of Diagnostic Accu-racy Studies (QUADAS2) tool (29). The quality assess-ment were performed based on following items: ac-ceptable reference tests, accounting for indeterminate results, avoiding differential verification bias, disease progression bias, incorporation bias and verification bias, blind index test interpretation, blind interpretation of reference test, explained withdrawal, relevant clinical data available, and representative spectrum. A total grading of poor, fair, and good was attributed to each survey and only the fair and good studies were included in the meta-analysis. Statistical analysis Analysis was performed using STATA 11.0 statistical software via MIDAS module. To evaluate the screening performance characteristics of ultrasonography and ra-diography in detection of chest wall fractures, summary receiver operative curves (SROCs) were drawn and pooled sensitivity, specificity, positive likelihood ratio and negative likelihood ratio with 95% confidence inter-val (95% CI) were calculated. Due the high heterogeneity between the included studies, mixed-effects binary re-gression model was used. Heterogeneity was evaluated through calculations of I2 and χ2 tests and a P value of less than 0.1 together with an I2 greater than 50% were considered as positive heterogeneity (30). Subgroup analysis was performed to identify the source of hetero-geneity. Deek’s asymmetry funnel plot was used to search for publication bias. In all the analyses, p value of less than 0.05 was considered as statistically significant. Results: Study characteristics 17 out of 3894 studies found in the comprehensive search were included in the systematic review and meta-analysis (1, 2, 8, 10-12, 14, 17, 18, 20-27). 5 studies had assessed the diagnostic accuracy of ultrasonography in detection of thoracic bone fractures (1, 2, 18, 20, 21), 8 diagnostic value of chest radiography (14, 17, 22-27), and 4 diagnostic values of ultrasonography and radiog-raphy simultaneously (8, 10-12). 1667 cases (807 with and 860 without fractures) were extracted from the 17
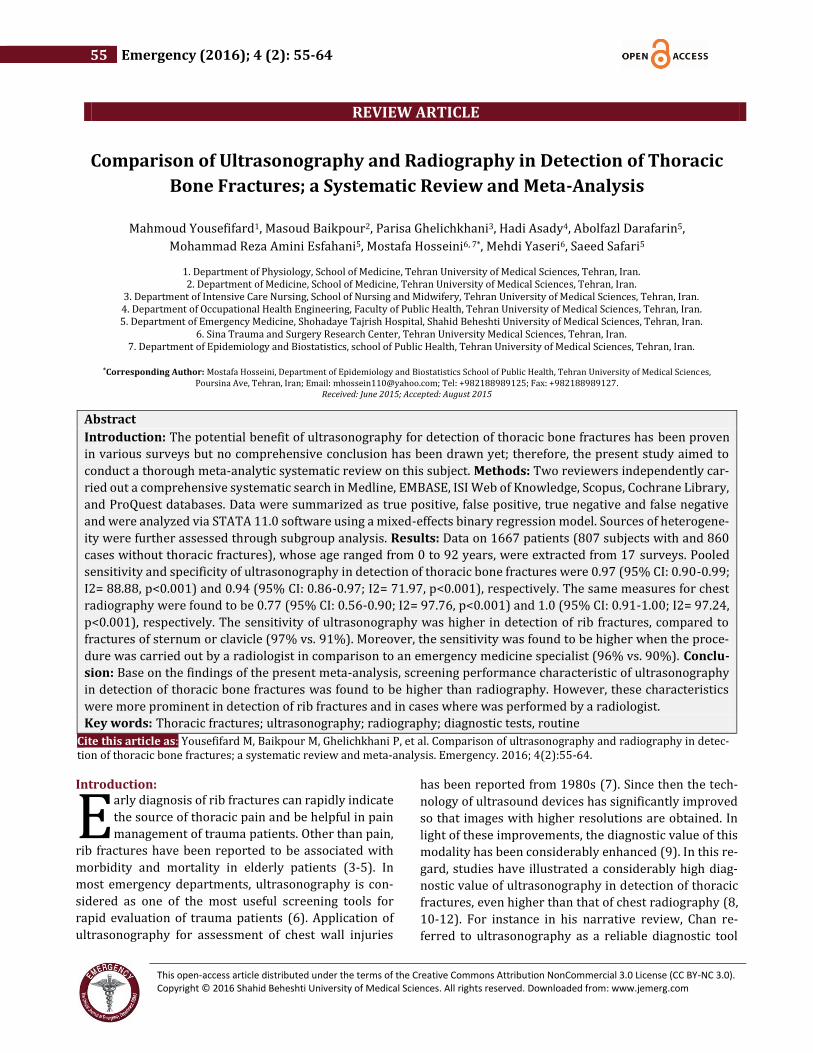
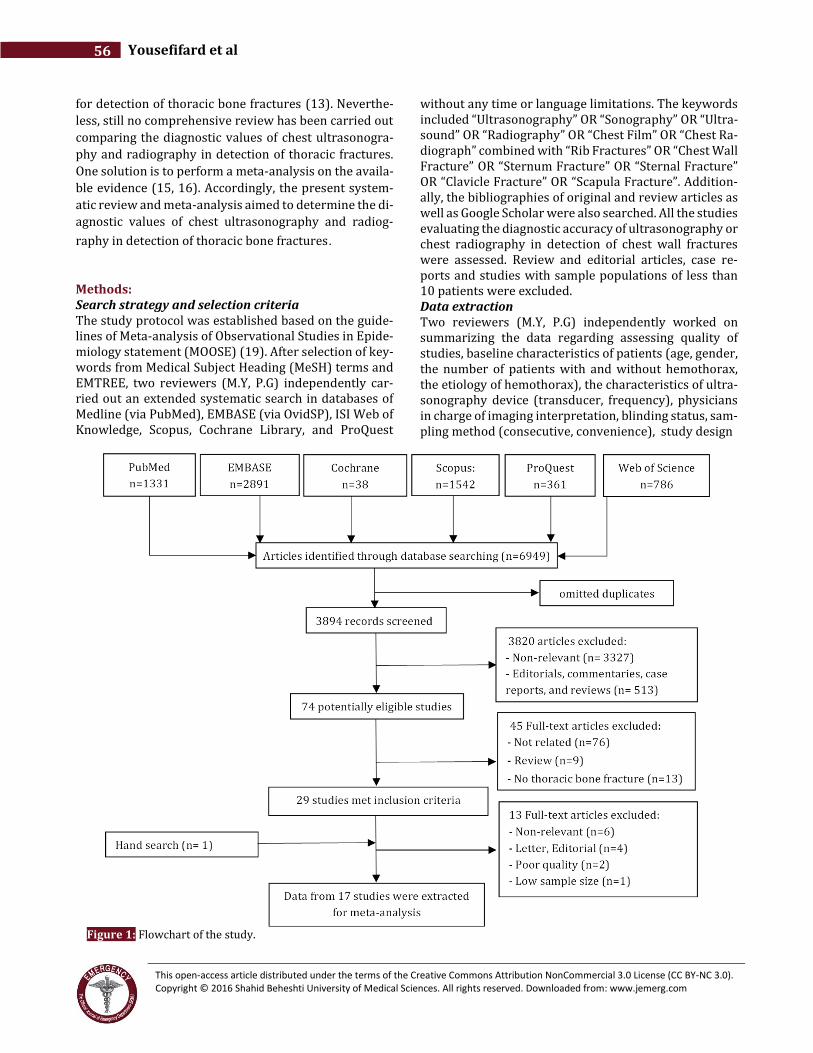
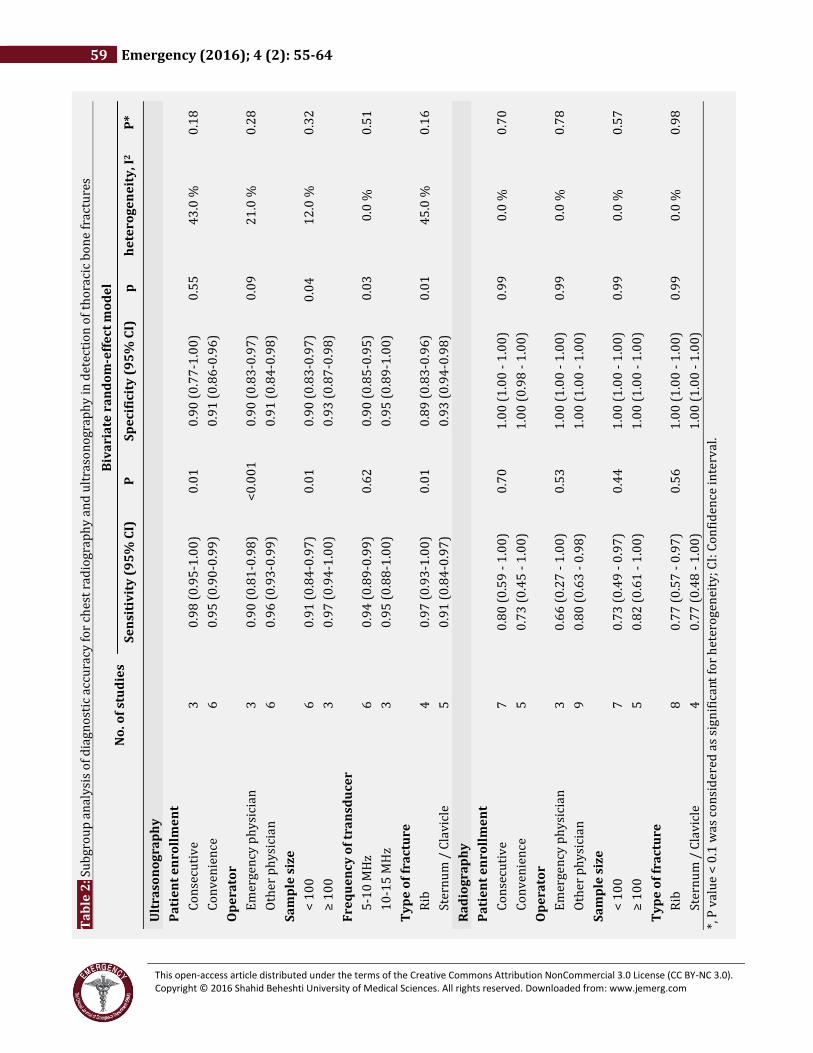
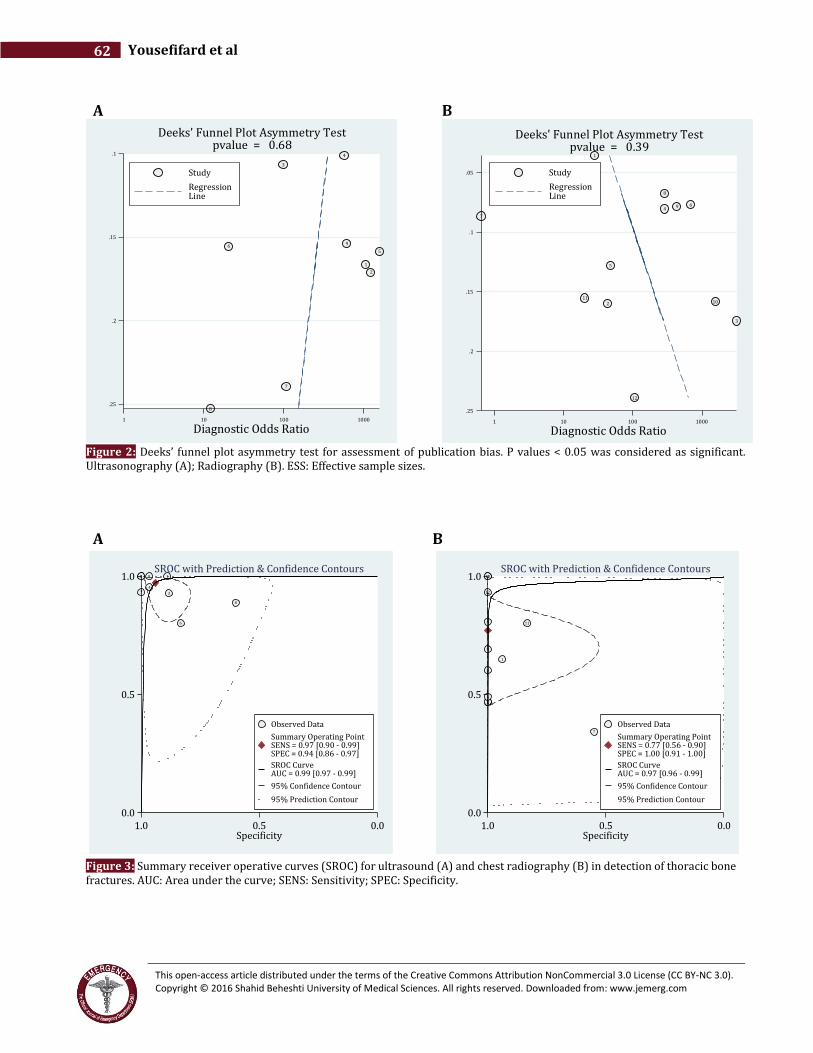
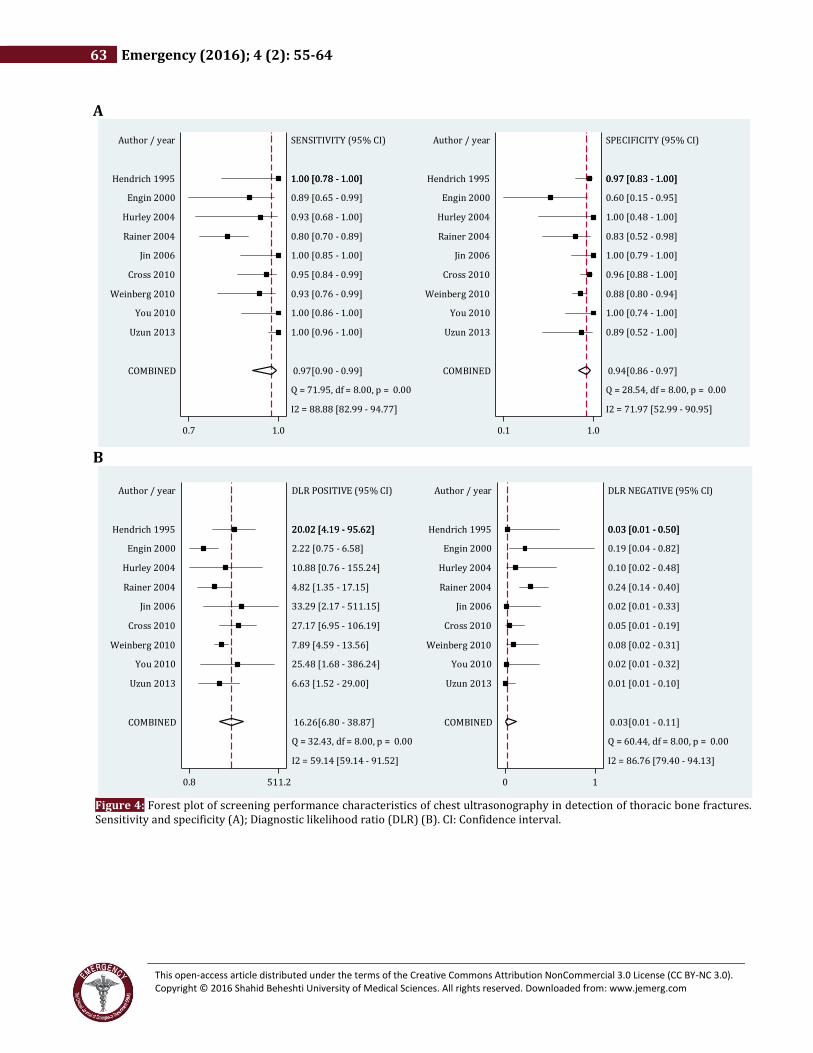
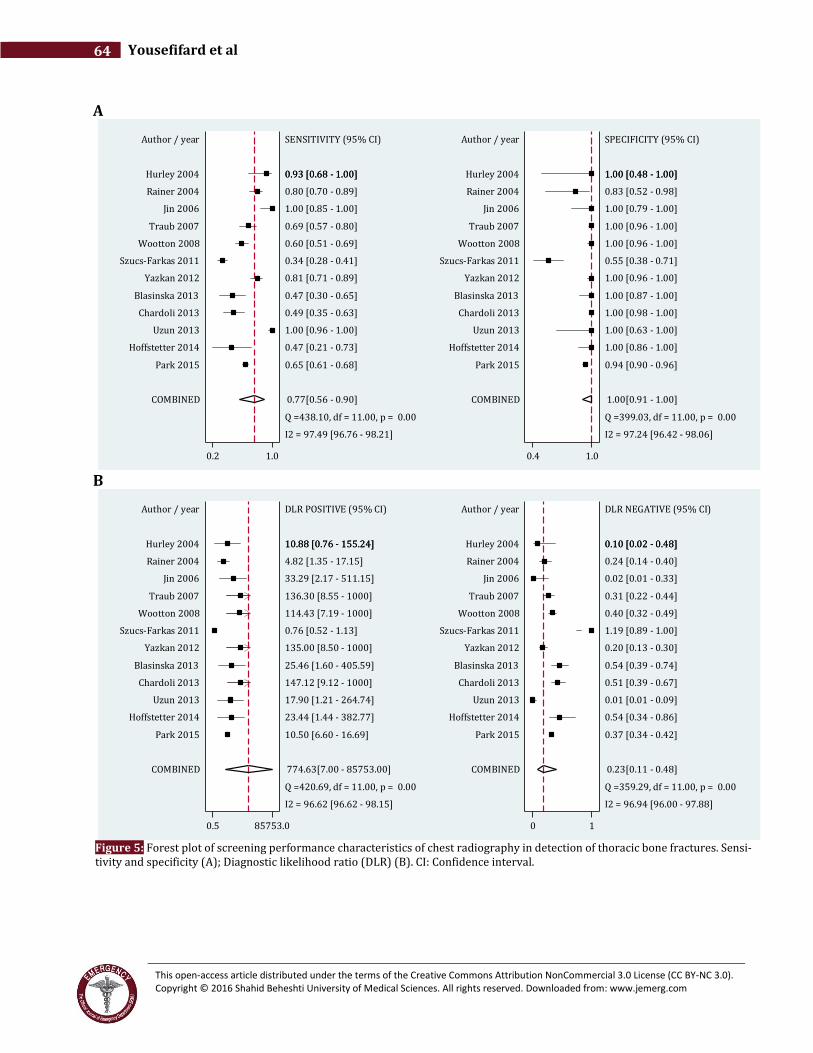
mentioned articles, whose age ranged from 0 to 92 years old. Figure 1 shows the inclusion process of articles and table 1 summarizes the characteristics of included stud-ies. No publication bias was observed (Figure 2). Meta-analysis The results of the analyses are presented as SROCs and Funnel plots in Figures 3 to 5. The area under the curve of SROC for ultrasonography and radiography in detec-tion of chest wall fractures were found to be 0.99 (95% CI: 0.97-0.99) and 0.97 (95% CI: 0.96-0.99), respectively (Figure 3). Pooled sensitivity and specificity of ultraso-nography in detection of thoracic bone fractures were 0.97 (95% CI: 0.90-0.99; I2= 88.88, p<0.001) and 0.94 (95% CI: 0.86-0.97; I2= 71.97, p<0.001), respectively (Figure 4-A). These characteristics for radiography were found to be 0.77 (95% CI: 0.56-0.90; I2= 97.76, p<0.001) and 1.0 (95% CI: 0.91-1.00; I2= 97.24, p<0.001), respec-tively (Figure 5-A). In addition, pooled positive and neg-ative likelihood ratios of ultrasonography were 16.26 (95% CI: 6.26-38.87; I2= 59.14, p<0.001) and 0.03 (95% CI: 0.01-0.11; I2= 86.76, p<0.001), respectively (Figure 4-B), while these measures for radiography were re-ported to be 774.63 (95% CI: 7.0-8573.0; I2= 96.62, p<0.001) and 0.23 (95% CI: 0.11-0.48; I2= 96.94, p<0.001), respectively (Figure 5-B). Subgroup Analysis There were significant heterogeneity between the arti-cles (Figure 4 and 5). Subgroup analysis was performed to remove its effects and find its probable sources. Table 2 presents the results of this analysis. Specificity of ultra-sonography in detection of thoracic bone fractures was directly correlated with frequency of transducer (90% vs. 95%). The sensitivity of this modality was found to be higher in detection of rib fractures rather than fractures of clavicle or sternum (97% vs. 91%). Moreover it was found that the sensitivity would be higher if the proce-dure is performed by a radiologist (96%) compared to an emergency medicine specialist (90%). Sample size was another source of heterogeneity. Studies with sam-ple sizes of greater than 100 patients reported higher di-agnostic accuracies for ultrasonography in detection of thoracic bone fractures (97% vs. 91%). As can be seen in Table 2, the most important factor af-fecting sensitivity of chest radiography is the interpret-ing physician. The sensitivity was found to be 66% when the radiogram was interpreted by an emergency medi-cine specialist while it was 80% when interpreted by a radiologist. Furthermore, consecutive sampling method compared with convenience (80% vs. 73%) and sample size of more than 100 patients (82% vs. 73%) were also found to be sources of heterogeneity. Discussion: Base on the results of the present meta-analysis sensitiv-ity of chest ultrasonography in detection of thoracic
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
59 Emergency (2016); 4 (2): 55-64
Ta
ble
2:
Sub
gro
up
an
aly
sis
of
dia
gn
ost
ic a
ccu
racy
fo
r ch
est
rad
iogr
aph
y a
nd
ult
raso
no
grap
hy
in d
etec
tio
n o
f th
ora
cic
bo
ne
frac
ture
s
N
o. o
f st
ud
ies
Biv
ari
ate
ra
nd
om
-eff
ect
mo
de
l
Se
nsi
tiv
ity
(9
5%
CI)
P
S
pe
cifi
city
(9
5%
CI)
p
h
ete
rog
en
eit
y, I
2
P*
Ult
raso
no
gra
ph
y
Pa
tie
nt
en
roll
me
nt
Co
nse
cuti
ve
3
0.9
8 (
0.9
5-1
.00
) 0
.01
0
.90
(0
.77
-1.0
0)
0.5
5
43
.0 %
0
.18
Co
nv
enie
nce
6
0
.95
(0
.90
-0.9
9)
0
.91
(0
.86
-0.9
6)
Op
era
tor
Em
erge
ncy
ph
ysi
cian
3
0
.90
(0
.81
-0.9
8)
<0
.00
1
0.9
0 (
0.8
3-0
.97
) 0
.09
2
1.0
%
0.2
8
Oth
er p
hy
sici
an
6
0
.96
(0
.93
-0.9
9)
0
.91
(0
.84
-0.9
8)
Sa
mp
le s
ize
< 1
00
6
0
.91
(0
.84
-0.9
7)
0.0
1
0.9
0 (
0.8
3-0
.97
) 0
.04
1
2.0
%
0.3
2
≥ 1
00
3
0
.97
(0
.94
-1.0
0)
0
.93
(0
.87
-0.9
8)
Fre
qu
en
cy o
f tr
an
sdu
cer
5-1
0 M
Hz
6
0.9
4 (
0.8
9-0
.99
) 0
.62
0
.90
(0
.85
-0.9
5)
0.0
3
0.0
%
0.5
1
10
-15
MH
z 3
0
.95
(0
.88
-1.0
0)
0
.95
(0
.89
-1.0
0)
Ty
pe
of
fra
ctu
re
Rib
4
0
.97
(0
.93
-1.0
0)
0.0
1
0.8
9 (
0.8
3-0
.96
) 0
.01
4
5.0
%
0.1
6
Ster
nu
m /
Cla
vic
le
5
0.9
1 (
0.8
4-0
.97
)
0.9
3 (
0.9
4-0
.98
)
Ra
dio
gra
ph
y
Pa
tie
nt
en
roll
me
nt
Co
nse
cuti
ve
7
0.8
0 (
0.5
9 -
1.0
0)
0.7
0
1.0
0 (
1.0
0 -
1.0
0)
0.9
9
0.0
%
0.7
0
Co
nv
enie
nce
5
0
.73
(0
.45
- 1
.00
)
1.0
0 (
0.9
8 -
1.0
0)
Op
era
tor
Em
erge
ncy
ph
ysi
cian
3
0
.66
(0
.27
- 1
.00
) 0
.53
1
.00
(1
.00
- 1
.00
) 0
.99
0
.0 %
0
.78
Oth
er p
hy
sici
an
9
0
.80
(0
.63
- 0
.98
)
1.0
0 (
1.0
0 -
1.0
0)
Sa
mp
le s
ize
< 1
00
7
0
.73
(0
.49
- 0
.97
) 0
.44
1
.00
(1
.00
- 1
.00
) 0
.99
0
.0 %
0
.57
≥ 1
00
5
0
.82
(0
.61
- 1
.00
)
1.0
0 (
1.0
0 -
1.0
0)
Ty
pe
of
fra
ctu
re
Rib
8
0
.77
(0
.57
- 0
.97
) 0
.56
1
.00
(1
.00
- 1
.00
) 0
.99
0
.0 %
0
.98
Ster
nu
m /
Cla
vic
le
4
0.7
7 (
0.4
8 -
1.0
0)
1
.00
(1
.00
- 1
.00
)
*, P
val
ue
< 0
.1 w
as c
on
sid
ered
as
sig
nif
ican
t fo
r h
eter
og
enei
ty; C
I: C
on
fid
ence
in
terv
al.

This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
Yousefifard et al 60
bone fractures following trauma was prominently higher than radiography (97% vs. 77%). Yet, the specificity of radiography was found to be significantly higher than ul-trasonography in this regard (100% vs. 94%). On this ba-sis and according to calculated likelihood ratios, a nega-tive result of ultrasonography in detection of thoracic fracture is more reliable than radiography (negative likelihood ratio=0.03), while a positive result of chest ra-diography is more reliable than ultrasonography (posi-tive likelihood ratio=774.63). Ultrasonography had a higher sensitivity in diagnosis of rib fractures rather than other chest wall bones, while the type of fracture had no effect on diagnostic value of radiography. This finding can be ascribed to the higher attention that physicians pay to rib fractures rather than other chest wall bones such as scapula and sternum. Fractures are diagnosed via ultrasonography based on observation of cortical bone disruption. In cases of small fractures, detection of this sign in sonogram and distin-guishing it from other findings is highly dependent on the skills of the operator. The role of operator’s skills in detection of injuries via ultrasonography was verified in the present study as well (31-34). Ultrasonography by a radiologist has a higher sensitivity compared to emer-gency medicine specialist. The present study found that the specificity of this modality increased with frequen-cies of higher than 10MHz which might be due to the higher resolution obtained with higher frequencies (35), making it easier to detect the signs of fracture. Some narrative review articles and qualitative system-atic reviews are indicative of the potential benefit of ul-trasonography in detection of chest wall fractures. In this regard, Chan, in his systematic review conducted on studies indexed in Medline, declares that ultrasonogra-phy has a higher sensitivity in detection of thoracic bone fractures compared to radiography (13). Finding the di-agnostic accuracy of ultrasonography to be two times the ability of radiography in fracture diagnosis, Dietrich et al. also referred to ultrasonography as a useful diagnostic tool for detection of rib fractures (36). The results of the present meta-analysis were congruent with these find-ings. Presence of considerable heterogeneity between the in-cluded articles and simultaneous inclusion of retrospec-tive and prospective studies in the meta-analysis were major limitations of this study. Subgroup analysis was performed to overcome the heterogeneity problem. Conclusion: Base on the findings of the present meta-analysis, screening performance characteristic of ultrasonogra-phy in detection of thoracic bone fractures was found to be higher than radiography. However, these characteris-tics were more prominent in detection of rib fractures and in cases where was performed by a radiologist.
Acknowledgments: None Conflict of interest: None Funding support: This research has been supported by Tehran University of Medical Sciences & health Services grant number: 93-02-38-25618. Authors’ contributions: All authors passed four criteria for authorship contribu-
tion based on recommendations of the International
Committee of Medical Journal Editors.
References: 1. Hendrich C, Finkewitz U, Berner W. Diagnostic value of ultrasonography and conventional radiography for the assessment of sternal fractures. Injury. 1995;26(9):601-4. 2. Engin G, Yekeler E, Güloǧlu R, Acunaş B, Acunaş G. US versus conventional radiography in the diagnosis of sternal fractures. Acta Radiol. 2000;41(3):296-9. 3. Barnea Y, Kashtan H, Skornick Y, Werbin N. Isolated rib fractures in elderly patients: mortality and morbidity. Can J Surg. 2002;45(1):43-6. 4. Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma Acute Care Surg. 2003;54(3):478-85. 5. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in the elderly. J Trauma Acute Care Surg. 2000;48(6):1040-7. 6. Forouzanfar MM, Safari S, Niazazari M, et al. Clinical decision rule to prevent unnecessary chest X-ray in patients with blunt multiple traumas. Emerg Med Australas. 2014;26(6):561-6. 7. Wongwaisayawan S, Suwannanon R, Prachanukool T, Sricharoen P, Saksobhavivat N, Kaewlai R. Trauma Ultrasound. Ultrasound Med Biol. 2015:[In press]. 8. Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful in the detection of rib fractures? Injury. 2004;35(6):562-6. 9. Saraogi A. Lung ultrasound: Present and future. Lung India. 2015;32(3):250-7. 10. Jin W, Yang DM, Kim HC, Ryu KN. Diagnostic values of sonography for assessment of sternal fractures compared with conventional radiography and bone scans. J Ultrasound Med. 2006;25(10):1263-8. 11. Rainer TH, Griffith JF, Lam E, Lam PKW, Metreweli C. Comparison of thoracic ultrasound, clinical acumen, and radiography in patients with minor chest injury. J Trauma. 2004;56(6):1211-3. 12. Uzuna M, Beksaça B, Karab A, Küçükdurmazc F, Kırcalıd BA, Tetika C. Ultrasonography as a better diagnostic efficiency in rib fracture. J Experiment Clin Med. 2013;30:133-5. 13. Chan SS. Emergency bedside ultrasound for the diagnosis of rib fractures. Am J Emerg Med. 2009;27(5):617-20. 14. Traub M, Stevenson M, McEvoy S, et al. The use of chest computed tomography versus chest X-ray in patients with major blunt trauma. Injury. 2007;38(1):43-7. 15. Ebrahimi A, Yousefifard M, Mohammad Kazemi H, et al. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Meta-Analysis. Tanaffos. 2014;13(4):29-40. 16. Hosseini M, Yousefifard M, Aziznejad H, Nasirinezhad F. The Effect of bone marrow derived mesenchymal stem cell transplantation on allodynia and hyperalgesia in neuropathic

This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
61 Emergency (2016); 4 (2): 55-64
animals: A systematic review with meta-analysis. Biol Blood Marrow Transplant. 2015: [In press]. 17. Wootton-Gorges SL, Stein-Wexler R, Walton JW, Rosas AJ, Coulter KP, Rogers KK. Comparison of computed tomography and chest radiography in the detection of rib fractures in abused infants. Child Abuse Negl. 2008;32(6):659-63. 18. Cross KP, Warkentine FH, Kim IK, Gracely E, Paul RI. Bedside ultrasound diagnosis of clavicle fractures in the pediatric emergency department. Acad Emerg Med. 2010;17(7):687-93. 19. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-12. 20. Weinberg ER, Tunik MG, Tsung JW. Accuracy of clinician-performed point-of-care ultrasound for the diagnosis of fractures in children and young adults. Injury. 2010;41(8):862-8. 21. You JS, Chung YE, Kim D, Park S, Chung SP. Role of sonography in the emergency room to diagnose sternal fractures. J Clin Ultrasound. 2010;38(3):135-7. 22. Szucs-Farkas Z, Lautenschlager K, Flach PM, et al. Bone images from dual-energy subtraction chest radiography in the detection of rib fractures. Eur J Radiol. 2011;79(2):e28-32. 23. Yazkan R, Ergene G, Tulay CM, Güneş S, Han S. Comparison of Chest Computed Tomography and Chest X-Ray in the Diagnosis of Rib Fractures in Patients with Blunt Chest Trauma. JAEM. 2012;11:171-5. 24. Błasińska-Przerwa K, Pacho R, Bestry I. Pneumonol Alergol Pol. Pneumonologia Alergologia Polska. 2013;81(6):518-26. 25. Chardoli M, Hasan-Ghaliaee T, Akbari H, Rahimi-Movaghar V. Accuracy of chest radiography versus chest computed tomography in hemodynamically stable patients with blunt chest trauma. Chin J Traumatol. 2013;16(6):351-4. 26. Hoffstetter P, Dornia C, Schafer S, et al. Diagnostic significance of rib series in minor thorax trauma compared to
plain chest film and computed tomography. J Trauma Manag Outcomes. 2014;8:10. 27. Park JB, Cho YS, Choi HJ. Diagnostic accuracy of the inverted grayscale rib series for detection of rib fracture in minor chest trauma. Am J Emerg Med. 2015;33(4):548-52. 28. Sistrom CL, Mergo PJ. A simple method for obtaining original data from published graphs and plots. Am J Roentgenol. 2000;174(5):1241-4. 29. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-36. 30. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557. 31. Abbasi S, Farsi D, Hafezimoghadam P, Fathi M, Zare MA. Accuracy of emergency physician-performed ultrasound in detecting traumatic pneumothorax after a 2-h training course. Eur J Emerg Med. 2013;20(3):173-7. 32. Bui-Mansfield LT, Chen DC, O'Brien SD. Accuracy of ultrasound of musculoskeletal soft-tissue tumors. Am J Roentgenol. 2015;204(2):W218. 33. Fine D, Perring S, Herbetko J, Hacking C, Fleming J, Dewbury K. Three-dimensional (3D) ultrasound imaging of the gallbladder and dilated biliary tree: reconstruction from real-time B-scans. Br J Radiol. 1991;64(767):1056-7. 34. Lee JH, Jeong YK, Park KB, Park JK, Jeong AK, Hwang JC. Operator-dependent techniques for graded compression sonography to detect the appendix and diagnose acute appendicitis. Am J Roentgenol. 2005;184(1):91-7. 35. Majumdar S, Kumar PS, Pandit A. Effect of liquid-phase properties on ultrasound intensity and cavitational activity. Ultrason Sonochem. 1998;5(3):113-8. 36. Dietrich CF, Mathis G, Cui XW, Ignee A, Hocke M, Hirche TO. Ultrasound of the pleurae and lungs. Ultrasound Med Biol. 2015;41(2):351-65.
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
Yousefifard et al 62
A B
Figure 2: Deeks’ funnel plot asymmetry test for assessment of publication bias. P values < 0.05 was considered as significant. Ultrasonography (A); Radiography (B). ESS: Effective sample sizes.
A B
Figure 3: Summary receiver operative curves (SROC) for ultrasound (A) and chest radiography (B) in detection of thoracic bone fractures. AUC: Area under the curve; SENS: Sensitivity; SPEC: Specificity.
1
2
3
4
56
7
8
9
.1
.15
.2
.25
1/r
oo
t(E
SS)
1 10 100 1000
Diagnostic Odds Ratio
Study
RegressionLine
Deeks' Funnel Plot Asymmetry Testpvalue = 0.68
1
2
3
4
5
6
7
8
9
1011
12
.05
.1
.15
.2
.25
1/r
oo
t(E
SS)
1 10 100 1000
Diagnostic Odds Ratio
Study
RegressionLine
Deeks' Funnel Plot Asymmetry Testpvalue = 0.39
12
3
4
5
6
7
8
9
0.0
0.5
1.0
Sen
siti
vit
y
0.00.51.0Specificity
Observed Data
Summary Operating PointSENS = 0.97 [0.90 - 0.99]SPEC = 0.94 [0.86 - 0.97]
SROC CurveAUC = 0.99 [0.97 - 0.99]
95% Confidence Contour
95% Prediction Contour
SROC with Prediction & Confidence Contours
1
2
3
45
6
7
8
9
10
11
12
0.0
0.5
1.0
Sen
siti
vit
y
0.00.51.0Specificity
Observed Data
Summary Operating PointSENS = 0.77 [0.56 - 0.90]SPEC = 1.00 [0.91 - 1.00]
SROC CurveAUC = 0.97 [0.96 - 0.99]
95% Confidence Contour
95% Prediction Contour
SROC with Prediction & Confidence Contours
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
63 Emergency (2016); 4 (2): 55-64
A
B
Figure 4: Forest plot of screening performance characteristics of chest ultrasonography in detection of thoracic bone fractures. Sensitivity and specificity (A); Diagnostic likelihood ratio (DLR) (B). CI: Confidence interval.
SENSITIVITY (95% CI)
Q = 71.95, df = 8.00, p = 0.00
I2 = 88.88 [82.99 - 94.77]
0.97[0.90 - 0.99]
1.00 [0.96 - 1.00]
1.00 [0.86 - 1.00]
0.93 [0.76 - 0.99]
0.95 [0.84 - 0.99]
1.00 [0.85 - 1.00]
0.80 [0.70 - 0.89]
0.93 [0.68 - 1.00]
0.89 [0.65 - 0.99]
1.00 [0.78 - 1.00]1.00 [0.78 - 1.00]
Author / year
COMBINED
Uzun 2013
You 2010
Weinberg 2010
Cross 2010
Jin 2006
Rainer 2004
Hurley 2004
Engin 2000
Hendrich 1995
0.7 1.0
SPECIFICITY (95% CI)
Q = 28.54, df = 8.00, p = 0.00
I2 = 71.97 [52.99 - 90.95]
0.94[0.86 - 0.97]
0.89 [0.52 - 1.00]
1.00 [0.74 - 1.00]
0.88 [0.80 - 0.94]
0.96 [0.88 - 1.00]
1.00 [0.79 - 1.00]
0.83 [0.52 - 0.98]
1.00 [0.48 - 1.00]
0.60 [0.15 - 0.95]
0.97 [0.83 - 1.00]0.97 [0.83 - 1.00]
Author / year
COMBINED
Uzun 2013
You 2010
Weinberg 2010
Cross 2010
Jin 2006
Rainer 2004
Hurley 2004
Engin 2000
Hendrich 1995
0.1 1.0
DLR POSITIVE (95% CI)
Q = 32.43, df = 8.00, p = 0.00
I2 = 59.14 [59.14 - 91.52]
16.26[6.80 - 38.87]
6.63 [1.52 - 29.00]
25.48 [1.68 - 386.24]
7.89 [4.59 - 13.56]
27.17 [6.95 - 106.19]
33.29 [2.17 - 511.15]
4.82 [1.35 - 17.15]
10.88 [0.76 - 155.24]
2.22 [0.75 - 6.58]
20.02 [4.19 - 95.62]20.02 [4.19 - 95.62]
Author / year
COMBINED
Uzun 2013
You 2010
Weinberg 2010
Cross 2010
Jin 2006
Rainer 2004
Hurley 2004
Engin 2000
Hendrich 1995
0.8 511.2
DLR NEGATIVE (95% CI)
Q = 60.44, df = 8.00, p = 0.00
I2 = 86.76 [79.40 - 94.13]
0.03[0.01 - 0.11]
0.01 [0.01 - 0.10]
0.02 [0.01 - 0.32]
0.08 [0.02 - 0.31]
0.05 [0.01 - 0.19]
0.02 [0.01 - 0.33]
0.24 [0.14 - 0.40]
0.10 [0.02 - 0.48]
0.19 [0.04 - 0.82]
0.03 [0.01 - 0.50]0.03 [0.01 - 0.50]
Author / year
COMBINED
Uzun 2013
You 2010
Weinberg 2010
Cross 2010
Jin 2006
Rainer 2004
Hurley 2004
Engin 2000
Hendrich 1995
0 1
This open-access article distributed under the terms of the Creative Commons Attribution NonCommercial 3.0 License (CC BY-NC 3.0). Copyright © 2016 Shahid Beheshti University of Medical Sciences. All rights reserved. Downloaded from: www.jemerg.com
Yousefifard et al 64
A
B
Figure 5: Forest plot of screening performance characteristics of chest radiography in detection of thoracic bone fractures. Sensi-tivity and specificity (A); Diagnostic likelihood ratio (DLR) (B). CI: Confidence interval.
SENSITIVITY (95% CI)
Q =438.10, df = 11.00, p = 0.00
I2 = 97.49 [96.76 - 98.21]
0.77[0.56 - 0.90]
0.65 [0.61 - 0.68]
0.47 [0.21 - 0.73]
1.00 [0.96 - 1.00]
0.49 [0.35 - 0.63]
0.47 [0.30 - 0.65]
0.81 [0.71 - 0.89]
0.34 [0.28 - 0.41]
0.60 [0.51 - 0.69]
0.69 [0.57 - 0.80]
1.00 [0.85 - 1.00]
0.80 [0.70 - 0.89]
0.93 [0.68 - 1.00]0.93 [0.68 - 1.00]
Author / year
COMBINED
Park 2015
Hoffstetter 2014
Uzun 2013
Chardoli 2013
Blasinska 2013
Yazkan 2012
Szucs-Farkas 2011
Wootton 2008
Traub 2007
Jin 2006
Rainer 2004
Hurley 2004
0.2 1.0
SPECIFICITY (95% CI)
Q =399.03, df = 11.00, p = 0.00
I2 = 97.24 [96.42 - 98.06]
1.00[0.91 - 1.00]
0.94 [0.90 - 0.96]
1.00 [0.86 - 1.00]
1.00 [0.63 - 1.00]
1.00 [0.98 - 1.00]
1.00 [0.87 - 1.00]
1.00 [0.96 - 1.00]
0.55 [0.38 - 0.71]
1.00 [0.96 - 1.00]
1.00 [0.96 - 1.00]
1.00 [0.79 - 1.00]
0.83 [0.52 - 0.98]
1.00 [0.48 - 1.00]1.00 [0.48 - 1.00]
Author / year
COMBINED
Park 2015
Hoffstetter 2014
Uzun 2013
Chardoli 2013
Blasinska 2013
Yazkan 2012
Szucs-Farkas 2011
Wootton 2008
Traub 2007
Jin 2006
Rainer 2004
Hurley 2004
0.4 1.0
DLR POSITIVE (95% CI)
Q =420.69, df = 11.00, p = 0.00
I2 = 96.62 [96.62 - 98.15]
774.63[7.00 - 85753.00]
10.50 [6.60 - 16.69]
23.44 [1.44 - 382.77]
17.90 [1.21 - 264.74]
147.12 [9.12 - 1000]
25.46 [1.60 - 405.59]
135.00 [8.50 - 1000]
0.76 [0.52 - 1.13]
114.43 [7.19 - 1000]
136.30 [8.55 - 1000]
33.29 [2.17 - 511.15]
4.82 [1.35 - 17.15]
10.88 [0.76 - 155.24]10.88 [0.76 - 155.24]
Author / year
COMBINED
Park 2015
Hoffstetter 2014
Uzun 2013
Chardoli 2013
Blasinska 2013
Yazkan 2012
Szucs-Farkas 2011
Wootton 2008
Traub 2007
Jin 2006
Rainer 2004
Hurley 2004
0.5 85753.0
DLR NEGATIVE (95% CI)
Q =359.29, df = 11.00, p = 0.00
I2 = 96.94 [96.00 - 97.88]
0.23[0.11 - 0.48]
0.37 [0.34 - 0.42]
0.54 [0.34 - 0.86]
0.01 [0.01 - 0.09]
0.51 [0.39 - 0.67]
0.54 [0.39 - 0.74]
0.20 [0.13 - 0.30]
1.19 [0.89 - 1.00]
0.40 [0.32 - 0.49]
0.31 [0.22 - 0.44]
0.02 [0.01 - 0.33]
0.24 [0.14 - 0.40]
0.10 [0.02 - 0.48]0.10 [0.02 - 0.48]
Author / year
COMBINED
Park 2015
Hoffstetter 2014
Uzun 2013
Chardoli 2013
Blasinska 2013
Yazkan 2012
Szucs-Farkas 2011
Wootton 2008
Traub 2007
Jin 2006
Rainer 2004
Hurley 2004
0 1