Embed Size (px)
Citation preview

1680
recovered his health and strength he gained no sight.The other eye held a promising-looking cataract and thelight projection was good, so I advised its extractionand performed the operation. The course of the case wasfairly normal and the resule was a good eye with media clearand fundus quite normal, but V. = o. I frequently see thisman. He is able to get about and to do his work as a piano-tuner and teacher of music in a small way and he has, so faras I know, no other lesion from his attack of influenza.Two other cases only are worthy of special notice. No. 9
is a diabetic and there is no discoverable reason in her eye",which are surgically excellent, for the poor result. In No. 11there is good reason for thinking that the second eye wasalways amblyopic from squint, and she is also interesting inthat she has borne four children who have been the subjectsof lamellar cataract and upon whom I have operated. Herfifth and youngest is up to now free from cataract but hasnot yet reached the age at which the others developed it.The general conclusion at which I arrive from this small
series of cases is that one may reasonably hope, other thingsbeing equal, for at least as good a result from the secondoperation as from the first, the figures working out as
follows :-Similar result in both eyes ............ 53 84 per cent.Better result in the spcond eye ......... 1538 "
Worse result ........................ 27’23 "
No record of second eye ............... 384 "
This gives 69 per cent. of results at least as good in thesecond eye as in the first and if the two doubtful cases,Cases 11 and 13, are eliminated the figures will be betterstill.Exeter.
________________
COMPENSATORY COLLATERAL CIRCULA-TION WITH "CAPUT MEDUSÆ" IN
CIRRHOSIS OF THE LIVERWITHOUT ASCITES.
BY U. N. BRAHMACHARI, M.A., M.D.,TEACHER OF MEDICINE AT THE CAMPBELL MEDICAL SCHOOL,
CALCUTTA.
CASES of cirrhosis of the liver without ascites have beenoccasionally met with. Such cases are of special interest, astheir occurrence gave rise to the idea of the Drummond-Talma-Morison operation.l Generally speaking, the collateralcirculation in cirrhosis of the liver is not capable of carryingoff all the surplus of blood and of re-establishing a normalvascularity and in this way removing the ascites.2 Thelatter, according to some, occurs in at least 80 per cent. ofthe cases.3 The number must be greater still when weconsider those cases in which there is complete absence ofhasmatemesis and melaena which frequently vary inverselywith the amount of ascites present. The following case istherefore of considerable interest, showing a perfect col-lateral circulation without the least ascites and withoutany hsematemesis and me]aena.The patient, a Bengalee, aged 35 years, was first ex-
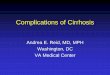
amined by me about four years ago for the treatmentof enlarged spleen. He gave a history of attacks of feverresembling malaria. There was no history of hasmatemesis,melsena, or jaundice. On examination the superficialveins of the abdomen were found enormously enlarged,especially the right epigastrics, which were tortuous andvery prominent (Fig. 1). The veins round the umbilicus
were somewhat dilated. There was a mark of a scar in the
right hypochondrial region-the result of an operation in theMedical College Hospital, Calcutta, for an inflamed thrombusin the dilated veins situated here. The spleen was enlarged,extending about two inches below the costal arch. The liverdulness extended from the seventh intercostal space to oneinch below the costal arch. The left lobe of the liver felthard and rough. There was no ascites. A loud systolicbruit was audible over the right superficial and superiorepigastric veins. A systolic bruit was also audible at thepulmonary area of the heart. The patient was somewhatanaemic and had some evening pyrexia. Digestion was good.
1 Brit. Med. Jour., September, 1896.2 Nothnagel’s Encyclopædia of Practical Medicine (Diseases of the
Liver, &c.).3 Allbutt’s System of Medicine, vol. iv.
The urine was scanty and high-coloured. The patient wasunder my observation for some months. The fever graduallydisappeared, the appetite increased, and the only symptomwhich afterwards he complained of was the presence of theenormously dilated veins. Since then I have seen thepatient from time to time improved in general health andwithout any ascites.
FM. 1.
Cirrhosis of the liver without ascites. 1903.
The patient came to me the last time in March, 1907,complaining of the enlargement of the veins in theabdominal wall, which were a source of inconvenience tohim and which were getting EO progressively enlarged thathe feared they might rupture. He asked for their completeremoval by surgical interference. He looked better inhealth than when I saw him, about four years previously.He was only slightly anemic, the systolic bruit at the pul.monaxy region of the heart having completely disappeared.The spleen extended two inches below the costal arch. Therliver dulness was smaller than before and the edge of theliver was not felt below the costal arch. The dulness couldjust be made out in the seventh intercostal space in theright mammary line. There was no ascites. The patient hadno fever and his appetite was good. The following was theoondition of the venous anastomosis in the abdominal wall(Fig. 2). 1. The right superficial epigastric was enormouslydilated, looking almost like coils of intestines and anasto-mosing with the superficial branches of the superiorepigastric which were also very much enlarged. 2. Theright superficial epigastric anastomosed directly with thebranches of the long thoracic which was also very prominentand enlarged. 3. The left superficial epigastric was moredilated and the anastomosis between it and the left superiorepigastric more prominent than when observed about fouryears previously. 4. The presence of dilated veins roundthe umbilicus gave rise to a well-marked " caput Medusas.’One point that struck me was the fairly good health which
the patient was enjoying during all these years. Could the

1681
complete absence of ascites account for this fact 7 Ascitesmay do harm in more ways than one. 1. By pressing uponthe vena cava it may interfere with the venous circulationof the lower extremities, giving rise to oedema in these parts.2. By pressing upon the renal vessels and kidneys. 3. Bysetting up a vicious circle by pressing upon the branches ofthe portal vein and thus interfering with the functions ofthe stomach and the intestines and also offering moreobstruction to the portal system. 4. By pressing upon thediaphragm and interfering with respiration and cardiacaction. 5. By abstracting from the blood a large quantityof albuminous fluid.
It remains for me to give a brief account of the collateralcirculation which may be developed in cirrhosis so as toenable the blood of the portal system to reach the
systemic vtins. 1. Hsemorrhoidal branches of the inferiormesenteric anastomosing with those of the internal iliac.2. Mesenteric veins anastomosing with those of the abdominalwall. 3. Coronary veins anastomosing with the oesophagealveins and thus communicating with the azygos veins.4. Coronary veins and veins of Glisson’s capsule on the onehand and the phrenic veins on the other. 5. One or moreveins in the round ligament (the accessory portal vein or
parumbilical vein or rudimentary umbilical vein of differentauthors) connecting the portal with the epigastric and otherveins of the abdominal wall. 6. Veins of the pancreas, theduodenum, the colon, and the rectum communicating withthe retroperitoneal branches. 7. Veins lying in the sub-peritoneal tissue, between the folds of the hepatic ligamentsand the peritoneal folds round the liver communicating withthe portal system on the one hand and the phrenic veins andazygos major on the other (the minor accessory portal veins
FIG. 2.
Cirrhosis of the liver without ascites. March, 1907.
of Sappey 4). Many of these penetrate the capsule of theliver. 8. Left renal veins and the veins of the intestines,especially those of the colon and the duodenum. 9. Super-ficial branches of the portal veins of the liver and the
4 Sappey : Centralblatt fur Chirurgie, 1901.
phrenic veins. 10. Very rarely communication between theparumbilical vein through an abdominal vein with the rightiliac vein.3 Besides the foregoing there may be innumerablenew vessels that may develop from adhesions.
I shall mention here another cause besides the collateralcirculation mentioned above which may prevent theoccurrence of ascites, namely, the increased exudation offluid into the peritoneal cavity may be reabsorbed by thelymphatics of the diaphragm and the parietal peritoneum,which are independent of the portal system.6Calcutta.
_________________
THE SYNCHRONOUS MOVEMENTS OF THELOWER EYELIDS WITH THE TONGUEAND LOWER JAW OBSERVED IN
CERTAIN DISEASES:A SIGN OF DISEASE IN CONNEXION WITH THE LOWER
EYELIDS.
BY HERBERT J. ROBSON, M.R.C.S. ENG., L.R.C.P. LOND.
ON Oct. 28th, 19(5, at the Leeds and West Riding Medico-Chirurgical Society I reported eight cases in which a pheno-menon connected with the lower eyelids had been obstrved ;and since then it has been teen in several other cases, not
only by myself, but by several other medical men. The
phenomenon referred to is a slight eversion of the lowereyelids made evident upon protrusion of the tongue or
depression of the lower jaw, the lids resuming their normalstate when the tongue is retracted or the mouth shut-inother words, the lower eyelids become displaced from the
eyeballs or are protruded from the eyeballs to the extent ofone or two millimetres upon protrusion of the tongue ordepression of the lower jaw. This phenomenon is appa-rently never present in health ; furthermore, it appa-rently comes and goes with the onset and cure ofdisease, and therefore I think that it must be a signof disease ; and, since I can find no record of it in anypublished work or writing, I regard it as a new sign ofdisease with some distinct significance, and one worthy offurther consideration. I do not think that it is a reflex actof disease. It is evidently produced by the contraction ofthe malaris fibres of the orbicularis palpebrarum muscle-the malaris muscle as described by Henle. From the factthat the facial nerve supplies the malaris muscle and thedigastric and mylo-hyoid muscles, and the hypoglossal nervesupplies the genio-hyoid and the genio-hyoglossus muscles,and that the facial nerve communicates in the latter musclewith the hypoglossal nerve; and furthermore, from the factthat the nuclei of origin of the hypoglossal nerve and of thefacial nerve are in close proximity in the medulla and thepons Varolii respectively, it is easy to see how the ccördinatemuscular acts of the simultaneous protrusion of the tongueand depression of the lower jaw with the eversion of thelower eyelids are produced.
In acute cases I am inclined to think that the presenceof the sign may be caused by the circulation in the blood ofsome toxin, or that at other times it may be some nervous
impulse acting directly upon the common nuclei of origin ofthe hypoglossal nerve and of those fibres of the facial nervesupplying the orbicularis palpebrarum and its offshoot themalaris muscle. In chronic cases it is obviously caused bysome change in the deeper structures of the skin.
Probably if the phenomenon or sign is regularly looked outfor it will be often found present in acute cases as quite atransitory sign and as indicating a severely ill condition ; forinstance, in a case of influenza complicated with acutelaryngitis, in which the patient was extremely ill, the lowereyelid sign was present one night, but it had disappeaiedthe next day when the urgent symptoms had been relieved,and it was not afterwards observed in that case. Of course,a healthy eyelid is referred to, and not the condition cfeversion of the lower eyelid sometimes seen in old peoplewith or without granular lids and with marked epiphora, andwho, like their lower lids, their figure, and their facultiesgenerally are gradually dropping down in response to gravityand other laws of nature.Some general eonclusions.-l. The phenomenon cannot be
detected unless it is specially looked out for, because the
5 Drummond : Brit. Med. Jour., February, 1888.6 Quincke; Ascites, Deutsches Archiv für Klinische Medicin, 1882.





![Clinical efficacy of tolvaptan for treatment of refractory ascites in ...€¦ · Ascites is one of the most common complications of liv-er cirrhosis[1]. Refractory ascites occur](https://img.pdfslide.net/doc/110x75/5f0c3caf7e708231d43468bd/clinical-efficacy-of-tolvaptan-for-treatment-of-refractory-ascites-in-ascites.jpg)