-
8/8/2019 compilation of grand case
1/51
Introduction
As it was written and said by the many, disease and illness have
plagued
human race since ancient time. Through years, people were full
of queries and
speculations that why some individuals become sick physically
weak while
other remain healthy. Why a condition turns out to a severe one?
Why an organ
complicates another at a later time? From that, people became
more curious on
how it can affect the body and how it can be cured.
Various disease and illness exist nowadays, just like on this
case that the
researchers studied. Through its complexity they were puzzled
on, how can
these bacteria affects the body? What manifestation and
complications may
arise? This brings their attention to focus. From this study,
they can then fully
understand the cause, its schematic flow and how it can alter a
persons body.
Pulmonary Tuberculosis, a chronic sub-acute or acute respiratory
disease
commonly affecting the lungs characterized by the formation of
tubercles in the
tissue which tend to undergo cessation, necrosis and
calcification. It is also
known as a poor mans disease or consumption disease. The
causative agent in
this disease is Mycobacterium tuberculosis, a rod shaped
bacteria that has
plagued humans since the Neolithic times. The bacteria usually
attack the lungs,but they can also damage other parts of the body.
TB spreads through the air
when a person with TB on the lungs or throat coughs, sneezes or
talks.
If left untreated, each person with active TB disease will
infect an average
of 10 to 15 people every year. But people infected with TB
bacilli will not
necessarily become sick, only if the immune system " walls off "
the TB bacilli
which, protected by a thick waxy coat, can lie dormant for
years. When the
immune system is weakened, the chances of becoming sick are
greater.
Global and Regional Incidence
Tuberculosis continues to be a major health problem worldwide.
In 2008,
the World Health Organization (WHO) estimated that the largest
number of new
TB cases occurred in the South-East Asia Region, which accounted
for 35% of
incident cases globally. However, the estimated incidence rate
in sub-Saharan
Africa is nearly twice that of the South-East Asia Region with
over 350 cases per
100, 000 populations.
An estimated 1.7 million people died from TB in 2009. The
highest number
of deaths was in the Africa Region. More than 90% of TB cases
occur in
developing nations that have poor hygiene and health-care
resources, and high
1
-
8/8/2019 compilation of grand case
2/51
numbers of people infected with HIV. The highest case rates
occur in non-white
males over 30 years of age and non-white females over 60.
National and Regional Incidence
TB is one of the top 10 leading cause of morbidity and mortality
rates in
the country. In 2007, the Philippines recorded over 86,000 TB
cases based on
the 2009 World Health Organization Report but the trend is
increasing as for this
year, it is estimated that 133 people out of 100, 000 population
has TB.
Cebu, Philippines - has the highest number of cases of
tuberculosis in the
region while Central Visayas is included in the top 10 regions
nationwide with the
highest incidence rate of TB cases.
The Philippines ranks 9th worldwide in the incidence of the
ordinary TB
disease which can easily be treated. And remember, a new
infection occurs
every second.
Risk Factors for TB:
Low socioeconomic status
Homelessness Alcoholism
HIV patient
Weakened immune system
Crowded living conditions
Person who frequently travel to place with high incidence
rate
Health-care workers
Ethical Consideration
Oral informed consent was obtained from the patient and her
significant
others for the case discussion and physical assessment. The
study was
approved by the Clinical Instructor and the staff of CUMC
Station 4.
Study Design and Data Collection
Interview was conducted and answered by the patient and her
significant
others.
Rationale for Choosing the Case
The researchers decided to choose this case because they wanted
to:
2
-
8/8/2019 compilation of grand case
3/51
Acquire more knowledge about Pulmonary Tuberculosis.
Know the factors why and how the patient was affected by
PTB.
Use the acquired knowledge in promoting awareness to the people
(to
seek for medical care in order to prevent the progression of the
disease).
Significance of the Study
This study will help the nursing profession by providing
information about
the proper management and care for PTB patient. It will also
educate the people
to seek medical care in order to prevent PTB.
It will increase awareness about the importance of having a
healthy
lifestyle and clean environment. And will also elaborate the
inter relatedness of
lifestyle habits, environment and acquiring Pulmonary
Tuberculosis.
Objectives
After the completion of this study, the researchers will have
been able to:
Perform the thorough assessment and implementation of care to a
PTB
patient.
Review the background of the disease and the signs and
symptoms.
Reassess the risk factors, the diagnostic procedures and the
needed
medical treatment.
Formulate nursing care plan based on the nursing process.
Perform the needed nursing care and intervention to better the
health of
the patient.
Provide information about the disease: occurrence and
contributing
factors.
Give health teachings and the importance of family involvement
to better
the health of the patient.
Scope and Limitations of the Study
This study is focused on the nursing aspect of care to those
patients who
have Pulmonary Tuberculosis. This study will only be used in the
nursing
profession.
The researchers only focused their attention on medications,
diagnostics,
nursing care plan, pathophysiology and discharge planning.
This study is not limited to PTB patients only, but it is also
for all people
who are interested in PTB. We are more focused on primary
preventions through
health teachings because primary prevention is the true
prevention.
3
-
8/8/2019 compilation of grand case
4/51
Authors Contributions
The group did their interview and physical assessment last
January 04,
2011. Discussion and interpolations was raised. Each of the
authors was given
assignments and submitted their drafts. And final brain-storming
was
scheduled.
Conceptual Frameworks
This study is anchored on these following theories:
Abraham Maslow's Hierarchy of Needs
Maslow's hierarchy of needs is often portrayed in the shape of a
pyramid,
with the largest and most fundamental levels of needs at the
bottom, and the
need forself-actualization at the top.
Florence Nightingales Environmental Theory
The act of utilizing the environment of the patient to assist in
his recovery
Focuses on changing and manipulating the environment in order to
put the
patient in the best possible conditions for nature to act.
Identified 5 environmentalfactors: fresh air, pure water, efficient
drainage, cleanliness/sanitation and
light/direct sunlight. Considered a clean, well-ventilated,
quiet environment
essential for recovery.
4
http://en.wikipedia.org/wiki/Self-actualizationhttp://en.wikipedia.org/wiki/Self-actualization
-
8/8/2019 compilation of grand case
5/51
Deficiencies in these 5 factors produce illness or lack of
health, but with a
nurturing environment, the body could repair itself.
SITUATION
Man needs care, has capacity to
mend
Health altered condition
Environment inefficient drainage,
poor sanitation
Nursing holistic approach
ACTION
- Attended physiologic needs (e.g.
supplement air, adequate water,
etc.)
- Medication regimen
- Provided with clean, quiet and well
ventilated environment
- Nursing care and intervention
This model will help the researchers to compare and contrast
their
findings based on the patients condition and how those needs
being attended.
Conclusion
Findings from our study indicate that knowledge and awareness of
PTB
are still unsatisfactory in Filipino population.
Gender issues should be considered in promoting patients'
health-care.
Results of this study are derived from Patient X, but could be
discussed also in
relation to other similar condition.
5
-
8/8/2019 compilation of grand case
6/51
Clients Profile
A. Demographic Data
This is a case of Patient X, a 17-year-old single female and a
Roman Catholic
affiliate residing at Opol, Misamis Oriental. Admitted at
Capitol University Medical
City last January 2, 2011 at 5:30pm Station 4; room 421.
B. Vital Signs
The client has the following vital signs and physical exam
during the series of
Vital Signs E.R. Admission
assessment
1st week of
assessment
2nd week of
assessment
Blood Pressure
(lying)
150/60 mmHg 100/60 mmHg 100/70 mmHg
Respiratory rate 37cpm 36cpm 34cpm
Pulse rate 120bpm 108bpm 102bpm
Temperature
(Axillary)
37.5 C 39.6 C 36.5 C
O2 saturation 92% 98% 99%
C. Health Perception Assessment:
1. Health Perception and Health Management (Pertinent Clinical
History
and Physical examination, Chief complaint, History of Present
Illness,
Previous Hospitalization/ Surgeries, other health problems and
things done to
manage health)
Chief complaint:
Cough/Fever
History of present illness:
Condition started since 4 months prior to admission as onset
ofhard and
productive cough with yellowish phlegm, no shortness of breath,
sought
consultation at community health center and sputum test was
done. A result of
negative PTB and was given a medication (unremembered brand) for
cough,
regimen was not completed due to financial stability and the
condition was
getting well.
6
-
8/8/2019 compilation of grand case
7/51
-
8/8/2019 compilation of grand case
8/51
Mouth:
Patients lips and gums was pale, tongue is midline with complete
teeth.
Pharynx:
Tonsils are not inflamed.
Neck:
Trachea is midline.
Skin:
General color of the patient is pale, with rough texture, with
poor skin
turgor, and temperature was warm.
Week 2 (January 11, 2011)
The patient takes in 5-6 glasses of water a day. The client eats
3 meals in
a day with fair appetite and a combination of 1 cup of rice with
different viand,
served with DAT with strict aspiration precaution. Upon
assessment, the client
had pale skin and body nourishment was maintained. She has an
ongoing
intravenous fluid of PLR1L regulated at 20gtts/min, infusing
well at the left arm.
Mouth:Patients lips, gums and mucosa were pale; tongue is
midline with
complete teeth.
Pharynx:
Tonsils are not inflamed.
Neck:
Trachea is midline.
Skin:
General color of the patient is pallor, still with rough
texture, with poor skin
turgorand temperature on normal range.
3. ELIMINATION PATTERN
Week 1 (January 4, 2011)
Patient X has a normal elimination pattern. She defecates once a
day or
every other day with moderate amount, formed light brown in
color. No
discomforts in the usual bowel pattern.
There was no problem in control upon urination. She urinates 4-5
times a
day with yellowish colored urine for about 150 200cc per
urination.
Week 2 (January 11, 2011)
8
-
8/8/2019 compilation of grand case
9/51
This week the patient defecated 4 times per week with soft brown
stool in
moderate amount. No discomforts in the usual bowel pattern.
There was no problem in control upon urination. She urinates 3-5
times a
day with yellowish colored urine for about 150 200cc per
urination.
4. ACTIVITY AND EXERCISE PATTERN
Week 1 (January 4, 2011)
According to the SO the patient has a sedentary lifestyle, her
leisure
activities include watching television and listening to
music.
Cardiovascular Status:
There was no signs of chest pain, point of maximal impulse
best
appreciated at 5th ICS left midclavicular line, heart sounds
were distinct and
regular in intervals. Peripheral pulses were symmetrical with
Capillary refill time
of 2 seconds.
Respiratory Status:
Breathing Pattern is irregular with 31 cycles per minute,
asymmetrical lung
expansion at right lung field; rales at right lung field are
heard upon auscultation,with productive cough, plenty of yellowish
sputum. The patient is on Oxygen
inhalation regulated at 2 LMP via nasal cannula.
Activities of daily living:
The patient is in assist with person to Feeding, bathing,
dressing,
grooming, meal preparations, cleaning, laundry, toileting, bed
mobility, chair/toilet
transfer, ambulation and in active-passive R.O.M. The reasons
for ADL/mobility
limitations are due to weakness in the lower extremities as well
as due to IVF line
connected to the patient.
Week 2 (January 11, 2011)
Cardiovascular Status:
There was no signs of chest pain, point of maximal impulse
best
appreciated at 5th ICS left midclavicular line, heart sounds
were distinct and
regular in intervals. Peripheral pulses were symmetrical with
Capillary refill time
of 2 seconds.
Respiratory Status:
9
-
8/8/2019 compilation of grand case
10/51
Breathing Pattern is irregularwith 34 cycles per minute,
asymmetrical lung
expansion at right lung field, rales are minimally heard upon
auscultation, with
less productive cough of yellowish sputum. Oxygen inhalation was
removed.
Activities of daily living:
The patient is in assist with person to Feeding, bathing,
dressing,
grooming, meal preparations, cleaning, laundry, toileting, bed
mobility, chair/toilet
transfer, ambulation and in active-passive R.O.M. The reasons
for ADL/mobility
limitations are due to weakness in the lower extremities as well
as due to IVF line
connected to the patient.
5. COGNITIVE- PERCEPTUAL PATTERN
Week 1 (January 4, 2011)
The client was conscious and oriented to time/person/place. The
patients
capillary refill is 2-3 seconds.
The client was calm and relaxed. The clients primary language is
Bisaya
and she dropped out of school during her 1st year in high school
due to illness.
Week 2 (January 11, 2011)The client was conscious and oriented
to time/person/place. The patients
capillary refill is 2 seconds.
The client was calm in emotional state. The clients primary
language is
Bisaya and she dropped out of school during her 1st year in high
school due to
illness.
6. SLEEP-REST PATTERN
Week 1 (January 4, 2011)
When she was not yet admitted, her usual sleep/rest pattern was
6-8hours
a day. The longest time for her to rest is eight hours. And now
that she is sick,
she normally rest for about 4-6hours which is inadequate on her
body needs as
verbalized by the patient. Relieving the cough with medication
as prescribed and
providing calm environment was one of the ways to make the
patient rest.
Week 2 (January 11, 2011)
There was already an improvement of the clients sleep and rest
pattern
patient can sleep for 6-8 hours according to the SO. Relieving
the cough with
10
-
8/8/2019 compilation of grand case
11/51
medication as prescribed and providing calm environment was one
of the ways
to make the patient rest.
7. SELF- PERCEPTION AND SELF-CONCEPT PATTERN
Week 1 (January 4, 2011)
Luyahan ug kapoi pud, as patient described herself was worried
with her
conditio . The patient feels the she reduced weight since
illness/ hospitalization.
The clients non-verbal actions showed minimal self
expression.
Week 2 (January 11, 2011)
Okay, raman ako pamati, as verbalized the patient. The patient
feels
good and positive that she will be well. The Clients non-verbal
behavior showed
that she was eager to participate in achieving health goals.
8. SEXUALITY REPRODUCTIVE PATTERN
Week 1 and Week 2 (January 4&11, 2011)
The patient has irregular menstrual pattern. Her Last Menstrual
Period
(LMP) was October 2010, 2 months delayed. No history of birth
control use. No
monthly self breast exam. Breasts are bilaterally equal;
surfaces are smooth withno lesions, tenderness and masses.
9. COPING-STRESS TOLERANCE PATTERN
Week 1 (January 4, 2011)
The financial difficulty was one of the clients stresses other
than her
illness.
Week 2 (January 11, 2011)
The financial difficulty was one of the clients stressors other
than her
illness. She usually managed stress by doing diversional
activities such as
watching TV and listening to music. She finds time with herself
in her room to
relax and rest. She uses her family and friends as her support
groups and they
are very helpful emotionally.
11
-
8/8/2019 compilation of grand case
12/51
11. VALUE-BELIEF PATTTERN
Week 1 (January 4, 2011)
The client is a Roman Catholic affiliate; believes that faith
and miracle was
very vital in her life. Hospitalization does not interfere,
visit prayer meeting was
done.
Week 2 (January 11, 2011)
The client is a Roman Catholic; hospitalization would not
interfere in any
medical intervention.
-
8/8/2019 compilation of grand case
13/51
Anatomy and Physiology
UPPER RESPIRATORY TRACT
Respiration is defined in two ways. In common usage, respiration
refers to
the act of breathing, or inhaling and exhaling. Biologically
speaking, respiration
strictly means the uptake of oxygen by an organism, its use in
the tissues, and
the release of carbon dioxide. By either definition, respiration
has two main
functions: to supply the cells of the body with the oxygen
needed for metabolism
and to remove carbon dioxide formed as a waste product from
metabolism. This
lesson describes the components of the upper respiratory
tract.
The upper respiratory tract conducts air from outside the body
to the lower
respiratory tract and helps protect the body from irritating
substances. The upper
respiratory tract consists of the following structures:
The nasal cavity, the mouth, the pharynx, the epiglottis, the
larynx, and the
upper trachea. The oesophagus leads to the digestive tract.
One of the features of both the upper and lower respiratory
tracts is themucociliary apparatus that protects the airways from
irritating substances, and is
composed of the ciliated cells and mucus-producing glands in the
nasal
epithelium. The glands produce a layer of mucus that traps
unwanted particles as
http://nursingcrib.com/wp-content/uploads/respiratory-system.gif
-
8/8/2019 compilation of grand case
14/51
they are inhaled. These are swept toward the posterior pharynx,
from where they
are swallowed, spat out, sneezed, or blown out.
Air passes through each of the structures of the upper
respiratory tract on
its way to the lower respiratory tract. When a person at rest
inhales, air enters via
the nose and mouth. The nasal cavity filters, warms, and
humidifies air. The
pharynx or throat is a tube like structure that connects the
back of the nasal
cavity and mouth to the larynx, a passageway for air, and the
esophagus, a
passageway for food. The pharynx serves as a common hallway for
the
respiratory and digestive tracts, allowing both air and food to
pass through before
entering the appropriate passageways.
The pharynx contains a specialized flap-like structure called
the epiglottis
that lowers over the larynx to prevent the inhalation of food
and liquid into the
lower respiratory tract.
The larynx, or voice box, is a unique structure that contains
the vocal
cords, which are essential for human speech. Small and
triangular in shape, the
larynx extends from the epiglottis to the trachea. The larynx
helps control
movement of the epiglottis. In addition, the larynx has
specialized muscular foldsthat close it off and also prevent food,
foreign objects, and secretions such as
saliva from entering the lower respiratory tract.
The larynx, or voice box, is a unique structure that contains
the vocal
cords, which are essential for human speech. Small and
triangular in shape, the
larynx extends from the epiglottis to the trachea. The larynx
helps control
movement of the epiglottis. In addition, the larynx has
specialised muscular folds
that close it off and also prevent food, foreign objects, and
secretions such as
saliva from entering the lower respiratory tract.
LOWER RESPIRATORY TRACT
The lower respiratory tract begins with the trachea, which is
just below the
larynx. The trachea, or windpipe, is a hollow, flexible, but
sturdy air tube that
contains C-shaped cartilage in its walls. The inner portion of
the trachea is called
the lumen.
The first branching point of the respiratory tree occurs at the
lower end of
the trachea, which divides into two larger airways of the lower
respiratory tract
called the right bronchus and left bronchus. The wall of each
bronchus contains
-
8/8/2019 compilation of grand case
15/51
substantial amounts of cartilage that help keep the airway open.
Each bronchus
enters a lung at a site called the hilum. The bronchi branch
sequentially into
secondary bronchi and tertiary bronchi.
The tertiary bronchi branch into the bronchioles. The
bronchioles branch
several times until they arrive at the terminal bronchioles,
each of which
subsequently branches into two or more respiratory
bronchioles.
The respiratory bronchiole leads into alveolar ducts and
alveoli. The
alveoli are bubble-like, elastic, thin-walled structures that
are responsible for the
lungs most vital function: the exchange of oxygen and carbon
dioxide.
Each structure of the lower respiratory tract, beginning with
the trachea,
divides into smaller branches. This branching pattern occurs
multiple times,
creating multiple branches. In this way, the lower respiratory
tract resembles an
upside-down tree that begins with one trachea trunk and ends
with more than
250 million alveoli leaves. Because of this resemblance, the
lower respiratory
tract is often referred to as the respiratory tree.
THE LUNGS
The thoracic cage, or ribs, and the diaphragm bound the thoracic
cavity.
There are two lungs that occupy a significant portion of this
cavity.
http://nursingcrib.com/wp-content/uploads/lungs.gif
-
8/8/2019 compilation of grand case
16/51
The diaphragm is a broad, dome-shaped muscle that separates
the
thoracic and abdominal cavities and generates most of the work
of breathing.
The inter-costal muscles, located between the ribs, also aid in
respiration. The
internal intercostal muscles lie close to the lungs and are
covered by the external
intercostal muscles.
The lungs are cone-shaped organs that are soft, spongy and
normally
pink. The lungs cannot expand or contract on their own, but
their softness allows
them to change shape in response to breathing. The lungs rely on
expansion and
contraction of the thoracic cavity to actually generate
inhalation and exhalation.
This process requires contraction of the diaphragm.
To facilitate the movements associated with respiration, each
lung is
enclosed by the pleura, a membrane consisting of two layers, the
parietal pleura
and the visceral pleura.
The parietal pleura comprise the outer layer and are attached to
the chest
wall. The visceral pleura are directly attached to the outer
surface of each lung.
The two pleural layers are separated by a normally tiny space
called the pleural
cavity. A thin film of serous or watery fluid called pleural
fluid lines and lubricatesthe pleural cavity. This fluid prevents
friction and holds the pleural surfaces
together during inhalation and exhalation.
-
8/8/2019 compilation of grand case
17/51
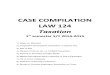
I. Pathophysiology
Mycobacterium Tuberculosis
Small airborne
Droplet spread
Subsequentphagocytosis by
macrophages
Predisposing factors:
Age
Heredity
Precipitating factors:
Repeated contact
with infected
persons
Part of low
income
population(lack
of medical care)
Low Body
weight (37 kg)
Environment
Infectious droplet settle throughout
airways and majority are trapped in
the upper parts of the airway
Successful control of
infection
Bacterial cell
division still
Inhallation
of particles
Progression of active
disease(Primary progressive
TB
Bacteria in droplets
that bypass
mucocilliary systemand reach alveoli
NOTE:
Outcome isdetermined by
quality of host
defense andm cobacteria
Complement system
also performsphagocytosis(Protein
C3
Binds to cell wall and
enhances recognition of
mycobacterium bymacro ha es
Rapidly surrounded
and engulfed bymacrophages
Production of protolytic enzymes
and cytokines by macrophages in
an attempt to control bacteria
DX: (+)
tuberculin skin
test
Cytokines attracts T
lymphocytes to the
site(synthesized T cells)
Microorganisms continue to
grow until cell-mediated
immune response is fully
Constitutescell mediated
Immunity
Formation of granulomas
around the M. Tuberculosisorganism
Limits replication
Spread Of
mycobacteria
Arrest of phagosome
Bacilli
replication
Low grade
Fever
Weight
loss
AnorexiaSleep
Hyperhid
rosis
>Paracetamol
-
8/8/2019 compilation of grand case
18/51
Acquired immunity leads to further
growth of bacilli and devpt. Of
active infection
Drainage of necrotic materials into thetrachiobronchial
tree(eruption of
coughing,formation of lesions ) Primary
infection
Bronchopneumonia develops in the
lung tissue (Phagocytosed tubercle
bacilli are ingested by macrophages)
General:
Anorexia
Vomitting
Weight loss
Low grade fever
with chills(39.6C)
Bacterial cell wall binds
with macrophages
Necrotic degeneration occurs(production of
cavities filled with cheese like mass of tuberclebacilli, dead
WBCs, necrotic lung tissue)
Tubercle bacilli immunity develops(2-6 weeks after infection).
Maintains
in the body as long as living bacilli
remains in the body.
As infection progresses in
which immune response wasnot capable of destroying it
Pulmonary:
Dyspnea (31-34
CPM)
productive cough
with yellowish
phlegm)
Hemoptysis(blood
Lesions may calcify (GhonsComplex ) and forms scars and
may heal over period of time.
Signs and Symptoms:
Productive
cough
Mucus
consolidation
Dyspnea
Rales
Rupture of alveolar-capillary beds
Hemoptysis
>Fluimucil
>Combivent
>Benadryl
>Ceftriaxone
-
8/8/2019 compilation of grand case
19/51
With medical Treatment:
Early detection and
diagnosis of case
Multi-antibacterial
Therapy
Without Medical treatment :
Reactivation of
tubercle bacilli(due
to repeatedexposure to infected
individuals,
immunosuppression
)
NO reccurence Recurrence
Good
Prognosis
Bad
Prognosis
LEGEND:
INFECTION
PROCESS
IMMUNOLO
GIC
PROCESS OF
LUNGS and
Treatment
Medications
NOTES ANDEXPLANATI
ONS
SYMPTOMS
PRESENTED
BY PATIENT
WHILE
ASSESSMEN
T
Continuation at
next page
>Fixcom>Peprasan
>Levoflaxacin
-
8/8/2019 compilation of grand case
20/51
Laboratory and Diagnostics
X-ray
An X-ray is a quick, painless test that produces images of the
structures
inside your body particularly your bones. X-ray beams can pass
through your
body, but they are absorbed in different amounts depending on
the density of the
material they pass through. The air in your lungs shows up as
black. Fat and
muscle look like varying shades of gray.
CHEST X-RAY PA (December 28, 2010 at COMC)
Nodule hazed densities altered in both lungs more in the Right
partially
obscuring the bilateral cardiac margins.
Heart is not enlarged.
Aorta is not dilated.
Diaphragm and both costrophrenic sulci are intact.
The rest of the visualized chest structures are
unremarkable.
Impression:
PTB, far advanced, bilateral
CHEST X-RAY (January 5, 2011 at CUMC)
Reticulo nodular densities are seen in both lungs, more
confluent on the
Right.
Heart is within normal limits in size.
Aorta is not dilated.
Diaphragm and sulci are intact.
The rest of the visualized chest structures are
unremarkable.
Impression:
Pulmonary Tuberculosis VS. Pneumonia Bilateral
CHEST X-RAY (January 9, 2010 at CUMC)
Follow up study since 1/5/11 shows no significant interval
change in the
previously noted reticulo nodular densities in both lungs, more
confluent
on the Right.
Heart is within normal limits in size.
Aorta is not dilated.
Diaphragm and sulci are intact.
The rest of the visualized chest structures are
unremarkable.
-
8/8/2019 compilation of grand case
21/51
Impression:
To consider Pulmonary Tuberculosis Bilateral. Please correlate
clinically.
Complete Blood Count
A complete blood count (CBC), also known as full blood count
(FBC) or
full blood exam (FBE) or blood panel, is a test requested by a
doctor or other
medical professional that gives information about the cells in a
patient's blood. A
lab technician (diploma holder) or technologist (bachelor
holder) performs the
requested testing and provides the requesting Medical
Professional with the
results of the CBC. A CBC is also known as a "hemogram".
COMPLETE BLOOD COUNT (January 2, 2011)
TEST RESULT REFERENCE INDICATION INTERPRETATION
WBC 16,7005,000-10,000
Cell/mm
Determines anyinflammation andinfection.
Result is above thenormal range whichindicates
presenceinfection.
RBC 4.184.2-5.010^6/L
Determines thepresence ofbleeding.
Result is belownormal range, thusindicating presenceof
bleeding.
Hemoglobin 10.711.7-14.5
g/dL
Usually done to a pt.with renal disease to
determine if thekidneys ability toreleaseerythropoietin factoris
already affected
Result is below thenormal range, thus
the patientexperiencedbleeding causinganemia.
Hematocrit 32.034.1-44.3
gm%
Used to measureRBC number andvolume. It is anintegral part of
theevaluation of anemicpatients.
Result is below thenormal range thus,showing anemia anddue to
blood loss.
MCV 70.6 80.0-96.0 fL
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range ,implicatingpresence of
infection
MCH 21.9 27.0-31.0 pg
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence of
infection
MCHC 31.132.0-36.0
g/dL
Determines anychronic bacterialinfection or viral
infection.
Result is below thenormal range,implicating
presence of infection
Lymphocyte 17.0 18-45 %
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence of
infection
Segmenters 81.0 45-70 % Determines anychronic bacterial
The result is abovethe normal range.
-
8/8/2019 compilation of grand case
22/51
infection or viralinfection.
Indicates presenceof infection.
Monocyte 1.0 4-8 %
Determines anyacute bacterialinfection.
Result is below thenormal range,implicating
presence of infection
Eosinophil 1.0 2-3 %
Determines anyacute bacterialinfection.
Result is below thenormal range,implicatingpresence of
infection
Platelet 566,000174,000-390,00010^3/L
To diagnose and/ormonitor bleeding andclotting disorders.
Results above thenormal range,implicating tendencyof acute
infection.
-
8/8/2019 compilation of grand case
23/51
COMPLETE BLOOD COUNT (January 5, 2011)
TEST RESULT REFERENCE INDICATION INTERPRETATION
WBC 19,0005,000-10,000
Cell/mm
Determines anyinflammation andinfection.
Result is above thenormal range whichindicates presence
infection.
RBC 3.334.2-5.010^6/L
Determines thepresence of bleeding.
Result is belownormal range, thusindicating presenceof
bleeding.
Hemoglobin 8.211.7-14.5
g/dL
Usually done to a pt.with renal disease todetermine if
thekidneys ability torelease erythropoietinfactor is
alreadyaffected
Result is below thenormal range, thusthe
patientexperiencedbleeding causinganemia.
Hematocrit 25.034.1-44.3
gm%
Used to measure RBCnumber and volume. Itis an integral part
ofthe evaluation ofanemic patients.
Result is below thenormal range thus,showing anemiaand due to
bloodloss.
MCV 70.1 80.0-96.0 fL
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence
ofinfection
MCH 22.9 27.0-31.0 pg
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence
ofinfection
MCHC 32.2 32.0-36.0 g/dL
Determines anychronic bacterialinfection or viralinfection.
Result is normalrange. Indicatingabsence ofbacterial
infection.
Lymphocyte 16.0 18-45 %
Determines any
chronic bacterialinfection or viralinfection.
Result is below the
normal range,implicatingpresence ofinfection
Segmenters 82.0 45-70 %
Determines anychronic bacterialinfection or viralinfection.
The result is abovethe normal range.Indicates presenceof
infection.
Monocyte 1.0 4-8 %
Determines any acutebacterial infection.
Result is below thenormal range,implicating
presence ofinfection
Eosinophil 1.0 2-3 %
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
Platelet 635,000 174,000- To diagnose and/or Results above
the
-
8/8/2019 compilation of grand case
24/51
390,00010^3/L
monitor bleeding andclotting disorders.
normal range,implicatingtendency of acuteinfection.
-
8/8/2019 compilation of grand case
25/51
COMPLETE BLOOD COUNT (January 6, 2011)
TEST RESULT REFERENCE INDICATION INTERPRETATION
WBC 23,2005,000-10,000
Cell/mm
Determines anyinflammation andinfection.
Result is above thenormal range whichindicates presence
infection.
RBC 3.574.2-5.010^6/L
Determines thepresence of bleeding.
Result is belownormal range, thusindicating presenceof
bleeding.
Hemoglobin 9.711.7-14.5
g/dL
Usually done to a pt.with renal disease todetermine if
thekidneys ability torelease erythropoietinfactor is already
affected
Result is below thenormal range, thusthe
patientexperiencedbleeding causinganemia.
Hematocrit 29.034.1-44.3
gm%
Used to measure RBCnumber and volume. Itis an integral part
ofthe evaluation ofanemic patients.
Result is below thenormal range thus,showing anemiaand due to
bloodloss.
MCV 69.9 80.0-96.0 fL
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
MCH 22.4 27.0-31.0 pg
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
MCHC 32.1 32.0-36.0 g/dL
Determines any acutebacterial infection.
Result is normal.Indicating absenceof bacterialinfection.
Lymphocyte 15.0 18-45 %
Determines anychronic bacterial
infection or viralinfection.
Result is below thenormal range,
implicatingpresence ofinfection
Segmenters 81.0 45-70 %
Determines anychronic bacterialinfection or viralinfection.
The result is abovethe normal range.Indicates presenceof
infection.
Monocyte 2.0 4-8 %
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence of
infection
Eosinophil 2.0 2-3 %
Determines any acutebacterial infection.
Result is normal.Indicating absenceof bacterialinfection.
Platelet 675,000 174,000-390,000
To diagnose and/ormonitor bleeding and
Results above thenormal range,
-
8/8/2019 compilation of grand case
26/51
10^3/L
clotting disorders. implicatingtendency of acuteinfection.
COMPLETE BLOOD COUNT (January 7, 2011)
TEST RESULT REFERENCE INDICATION INTERPRETATION
WBC 22,1005,000-10,000
Cell/mm
Determines anyinflammation andinfection.
Result is above thenormal range whichindicates
presenceinfection.
RBC 3.974.2-5.010^6/L
Determines thepresence of bleeding.
Result is belownormal range, thusindicating presence
of bleeding.
Hemoglobin 10.711.7-14.5
g/dL
Usually done to a pt.with renal disease todetermine if
thekidneys ability torelease erythropoietinfactor is
alreadyaffected
Result is below thenormal range, thusthe
patientexperiencedbleeding causinganemia.
Hematocrit 32.034.1-44.3
gm%
Used to measure RBCnumber and volume. Itis an integral part
of
the evaluation ofanemic patients.
Result is below thenormal range thus,showing anemia
and due to bloodloss.
MCV 74.0 80.0-96.0 fL
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence
ofinfection
MCH 23.7 27.0-31.0 pg
Determines anychronic bacterialinfection or viralinfection.
Result is below thenormal range,implicatingpresence of
infection
MCHC 32.1 32.0-36.0 g/dL
Determines anychronic bacterialinfection or viralinfection.
Result is normal.Indicating absenceof bacterialinfection.
Lymphocyte 19.0 18-45 %
Determines anychronic bacterialinfection or viralinfection.
Result is normal.Indicating absenceof bacterialinfection.
Segmenters 76.0 45-70 %
Determines anychronic bacterial
infection or viralinfection.
The result is abovethe normal range.
Indicates presenceof infection.
Monocyte 4.0 4-8 %
Determines any acutebacterial infection.
Result is normal.Indicating absenceof bacterialinfection.
Eosinophil 1.0 2-3 % Determines any Result is below the
-
8/8/2019 compilation of grand case
27/51
chronic bacterialinfection or viralinfection.
normal range,implicatingpresence ofinfection
Platelet 657,000174,000-390,00010^3/L
To diagnose and/or
monitor bleeding andclotting disorders.
Results above the
normal range,implicatingtendency of acuteinfection.
-
8/8/2019 compilation of grand case
28/51
COMPLETE BLOOD COUNT (January 8, 2011)
TEST RESULT REFERENCE INDICATION INTERPRETATION
WBC 23,5005,000-10,000
Cell/mm
Determines anyinflammation andinfection.
Result is above thenormal range whichindicates presence
infection.
RBC 4.034.2-5.010^6/L
Determines thepresence of bleeding.
Result is belownormal range, thusindicating presenceof
bleeding.
Hemoglobin 10.811.7-14.5
g/dL
Usually done to a pt.with renal disease todetermine if
thekidneys ability torelease erythropoietinfactor is already
affected
Result is below thenormal range, thusthe
patientexperiencedbleeding causinganemia.
Hematocrit 32.034.1-44.3
gm%
Used to measure RBCnumber and volume. Itis an integral part
ofthe evaluation ofanemic patients.
Result is below thenormal range thus,showing anemiaand due to
bloodloss.
MCV 74.5 80.0-96.0 fL
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
MCH 24.0 27.0-31.0 pg
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
MCHC 32.2 32.0-36.0 g/dL
Determines any acutebacterial infection.
Result is normal.Indicating absenceof bacterialinfection.
Lymphocyte 24.0 18-45 %
Determines anychronic bacterial
infection or viralinfection.
Result is normal.Indicating absence
of bacterialinfection.
Segmenters 72.0 45-70 %
Determines anychronic bacterialinfection or viralinfection.
The result is abovethe normal range.Indicates presenceof
infection.
Monocyte 2.0 4-8 %
Determines any acutebacterial infection.
Result is below thenormal range,implicatingpresence
ofinfection
Eosinophil 2.0 2-3 %Determines any acutebacterial infection.
Result is normal.Indicating absenceof bacterialinfection.
Platelet 728,000 174,000-390,00010^3/L
To diagnose and/ormonitor bleeding andclotting disorders.
Results above thenormal range,implicating
-
8/8/2019 compilation of grand case
29/51
tendency of acuteinfection.
HEMATOLOGY
January 2, 2011
ABO TYPING B Rh+
Blood Chemistry Test
Blood Chemistry is needed to assess a wide range of conditions
and the
function of organs. It also a test to check electrolytes, the
minerals that help keep
the bodys fluid level in balance, and are necessary to help the
muscles, heart,
and other organs work properly. This also helps assess kidney
function and
blood sugar, and other substances in the blood.
CLINICAL CHEMISTRY
January 2, 2011
Test Result Reference
Creatinine 0.70 0.60-1.30 mg/dL
SGPT 25.10 10-40 Iu/LSodium 125.50 135-148 mmol/L
Potassium 3.07 3.5-5.3 mmol/L
Interpretation: The result of the Potassium and Sodium are
slightly decreased.
So the patient is hypokalemic and hyponatremic, a condition in
which the
concentration of potassium and sodium in the blood is low
January 5, 2011
Test Result ReferenceUric Acid 4.60 2.6-7.2
Sodium 129.90 135-148 mmol/L
Potassium 3.95 3.5-5.3 mmol/L
Interpretation: The result of the Sodium is still decreased but
compared to
previous laboratory result (01/02/11); it has increased by 0.88.
Still the patient is
hyponatremic.
January 6, 2010
Test Result Reference
FBS 104.00 75-115
-
8/8/2019 compilation of grand case
30/51
Interpretation: The FBS result is within normal range.
January 8, 2011
Test Result Reference
Potassium 4.25 3.5-5.3 mmol/LInterpretation: The Potassium is
within normal Range.
AFB Stain
AFB smears and cultures are used to determine whether you have
an
active Mycobacterium tuberculosis infection, an infection due to
another member
of the Mycobacterium family, orTB-like symptoms due to another
cause. They
are used to help determine whether the TB is confined to the
lungs (pulmonary)
or has spread to organs outside the lungs (extrapulmonary). AFB
cultures can be
used to monitor the effectiveness of treatment and can help
determine when a
patient is no longer infectious.
AFB STAIN REPORT
January 3, 2010 January 6, 2011
Result
Interpretation
Result Grading No of fields
examine
More than 10 AFB/oil immersion field Positive 3+ 20
1-10 AFB 10 AFB/oil immersion field Positive 2+ 5010-99 AFB in
100 oil immersion field Positive 1+ 100
1-9 AFB in 100 oil immersion field Scanty Record
actual #
200
No AFB in 100 oil immersion field Negative 0 100
January 6, 2011
Specimen sputum
Result No microorganism seen
Polymorphonuclear cells few
Epithelial cells few
Positive
Grade 3+
Specimen Sputum
http://www.labtestsonline.org/understanding/conditions/tuberculosis-2.htmlhttp://www.labtestsonline.org/understanding/conditions/tuberculosis-2.html
-
8/8/2019 compilation of grand case
31/51
CULTURE REPORT (January 7, 2011)
Preliminary Report
Findings: No growth after 2 days of incubation
Urinalysis
A physical, microscopic, or chemical examination of urine. The
specimen
is physically examined for color, turbidity, and specific
gravity. Then it is spun in a
centrifuge to allow collection of a small amount of sediment,
which is examined
microscopically for blood cells, casts, crystals, pus, and
bacteria. Chemical
analysis may be performed to measure the pH and to identify and
measure the
levels of ketones, sugar, protein, blood components, and many
other substances.
URINALYSIS (January 3, 2011)
Color Orange
Transparency Hazy
Reaction 6.0
Sp gravity 1.015Sugar negative
Protein trace
PUS cell 3-6 cells/HFP
RBC 0-2 cells/HPF
EPITHELIAL CELLS
Squamous epithelial moderate
Bacteria moderate
MUCUOS THREADS few
Fecalysis
Fecalysis is also known as stool analysis. It refers to a series
of laboratory
tests done on fecal samples to analyze the condition of a
person's digestive tract
in general. Among other things, a fecalysis is performed to
check for the
presence of any reducing substances such as white blood cells
(WBCs), sugars,
or bile and signs of poor absorption as well as screen for colon
cancer.
-
8/8/2019 compilation of grand case
32/51
FECALYSIS (January 3, 2011)
Consistency soft
Color dark brown
RBC
Pus cells
Ascaris
Hook worm
Amoeba No Parasite seen
Trichuris
Fat globules
Bacteria
-
8/8/2019 compilation of grand case
33/51
Nursing Care Management
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSING DIAGNOSIS(Problem and Etiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
Subjective:Galisod ko ug ginhawatungod sa akong ubo,
asverbalized by the patient.
Objective/s:
Productive cough noted,yellowish in color
RR= 31 cpm, tachypnea(16-24cpm)
O2 saturation= 98%
With O2 inhalation vianasal cannula at 2LPM
Lab:
CXRAY = Dec. 28, 2010@COMC
CXRAY = Jan. 5, 2011@CUMC
Impression: PTB Far advanced bilateral
(Right lung)
Ineffective AirwayClearance related toaccumulation ofsecretions
at the rightlower field of the lungs.
Short term:Within 15 minutes ofNursing Care andinterventions,
patient will:
Maintain orimproved airwaypatency.
Expectorate/clearsecretions readily.
Long term:Within 1-2 daysof Nursing Care andinterventions,
patient will:
improve oxygenexchange.
INDEPENDENT:1. Auscultate breath sounds andassess air
movement.R: to ascertain status and noteprogress.2. Position head
midline with flexionappropriate for age/condition.R: to open or
maintain openairway in at-rest or compromisedindividual.3. Elevate
head of the bed/ changeposition every 2hours.R: to take advantage
of gravitydecreasing pressure on thediaphragm and enhancingdrainage
of ventilation to differentlung segments.4. Encourage
deep-breathing andcoughing exercises.
R: to promote lung expansion.5. Increase fluid intake to at
least2000 ml/day within level of cardiac
After 30 minutes ofNursing Care andinterventions, GOALWAS
PARTIALLYMET, patient was ableto maintain airwaypatency
andexpectorate/ clearsecretions readily.
After 2-3 days ofNursing Care andinterventions, GOALWAS MET,
patientwas:
Able to improveoxygen exchang asevidenced by removal
of 02 supplementationlast Jan. 9, 2011.
-
8/8/2019 compilation of grand case
34/51
tolerance; encourage/provide warmversus cold liquids as
appropriate.R: to help liquefy secretions.6. Monitor vital signs,
noting bloodpressure/pulse changes.R: to note any
changes/complications.
7. Encourage and provideopportunities for rest; limit
activities
to level of respiratory tolerance.R: to prevent and lessen
fatigue.
COLLABORATIVE:1. Give expectorant/bronchodilatorsas ordered
(Combivent neb. + 1ccNSS, Nebulization every 8 hours).R: to treat
underlying conditions.
-
8/8/2019 compilation of grand case
35/51
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSINGDIAGNOSIS
(Problem andEtiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
SUBJECTIVE:Dili naku gaka-hurot akongpagkaon, wala koi gana,
asverbalized by the patient.
OBJECTIVES:
Weight= 37.5 kg(17/Female ; normal 39-41kg)BMI= 17.9)
Height= 147 cm
BMI= 17.9 (NormalBMI: 18.5 24.5)
Pale conjunctiva and mucusmembrane
inability to consume fullshare of food
IVF: PLR@20gtts/min
LAB: Clinical chemistry:Jan 2,2011
Na = 125.50 Below normalrange(135-148mmol/L)K = 3.07: Below
normal
Imbalanced Nutrition:less than bodyrequirements relatedto lack
of interest in
food.
Short term:Within 8 hours of NursingCare and
interventions,patient will:
Regain normalappetite
Increase foodintake.
Long term:Within 2 weeks ofNursing Care andInterventions,
patient will:
Demonstrateprogressive weightgain toward goal.
Displaynormalization oflaboratory values.
IINDEPENDENT:1. Assess the weight; Followingprotocol in weighing
a patientR: to establish baseline
parameters.2. Ascertain understanding ofindividual nutritional
needsR: to determine informationalneeds of the client.3. Discuss
eating habits, includingfood preferences,intolerance/aversions.R:
to appeal to clientslikes/dislikes.
After 8 hours of NursingCare and interventions,GOAL WAS MET,
patientwas able to improve
appetite and consumed fullshare of food.
After 2 weeks of NursingCare and interventions,GOAL PARTIALLY
MET,
Patient was able togain weight of450gm(Stillunderweight18.35Kg,
Normal:18.5Kg Female 17years old)
LAB: ClinicalchemistryJan 5,2011 Na levelfrom 125.50 to
129.90 increase by4.4mmol/L
-
8/8/2019 compilation of grand case
36/51
range(3.5-5.3mmol/L) K level from 3.07 to3.95 increase
by0.88mmol/L
NURSING CARE MANAGEMENT
-
8/8/2019 compilation of grand case
37/51
ASSESSMENT DATA(Subjective andObjective Cues)
NURSINGDIAGNOSIS
(Problem andEtiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
SUBJECTIVE:Gapamugnaw ko, medyolabad akong ulo, initakong
paminaw sa lawasas verbalized by the
patient.
OBJECTIVE:
Febrile; Temp=39.6C
Flushed skin ; warm totouch
Tachypnea RR =31cpm(Normal 16 24cpm)
Tachcardia =108bpm(Normal 60 100bpm)
Hyperthermia relatedto disease process.
Short term:Within 30 to 60 minutes ofnursing care
andinterventions the patient willbe able to:
Maintain coretemperature withinnormal range andlower
bodytemperature from39.6C-36.5C.
Demonstratebehaviors to monitorand promotenormothermia.
Long term:Within 2-3days nursing careand interventions the
patientwill be able to:
Be free of
INDEPENDENT:1. Vital signs taken and recordR: to note any
changes and/orcomplications and as baseline.2. Perform TSB to lower
down Body
temperature to normal: (36.5 37.5C)3. Maintain bed rest.R: to
reduce metabolic demands/oxygen consumption4. Provide adequate
sleep.R: to regain back body strength.5. Provide adequate fluid
intake.R: to prevent dehydration.
COLLABORATIVE:1. Administer medications, as indicated,such as
antipyretics and antibiotics (forinfection).R: to treat underlying
cause.
After 1hour of nursing careand interventions,
patientstemperature was loweredfrom 39.6 to 36.9 degreeCelsius and
demonstrated
behaviors to monitor andpromote normothermia.GOAL WAS MET
After 2-3days nursing careand interventions, thepatient able
to:
Free fromcomplications andfree from seizures
-
8/8/2019 compilation of grand case
38/51
complications suchas infection.
Be free of seizureactivity.
-
8/8/2019 compilation of grand case
39/51
-
8/8/2019 compilation of grand case
40/51
R: to promote muscle tone
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSING DIAGNOSIS(Problem and Etiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
SUBJECTIVE: Gakaulaw ko sa akong
sakit as verbalized bypatient.
OBJECTIVES:
Developmental changes
Functional impairment
Physical illness
Delayed educationalattainment: Drop out fromschool during 1st
year in
highschool.
Situational low selfesteem related to socialrole changes.
Long term:Within 2weeks ofnursing care andintervention the
patientwill be able to:
Acknowledgefactors that leadto possibility offeelings of lowself
esteem.
Verbalize view asworthwhile,important personwho
functionswellinterpersonally
Demonstrate selfconfidence bysetting realistic
INDEPENDENT:1. Assess nonverbal body language.R: incongruencies
betweenverbal/nonverbal communicationsrequire clarification.2.
Identify previous adaptations toillness/disruptive events in
life.R: May be predictive of currentoutcome.3. Ascertain sense of
control. Clienthas over self and situation todetermine clients
trust to self.4. Identify the strength of the clientR: to reinforce
self-view5. Encourage verbalization offeelings.R: to promote
positive sense of
self.
COLLABORATIVE:
After 2 weeks of nursingcare and intervention,GOAL WASPARTIALLY
MET, thepatient was be able to:
Acknowledgedfactors that leadto possibility offeelings of
lowself esteem.
Verbalized viewas worthwhile,important personwho
functionswellinterpersonally.
Demonstratedself confidenceby setting
-
8/8/2019 compilation of grand case
41/51
goals and activelyparticipating in lifesituation.
1. Promote attendance in therapy orinvolvement of familyR: to
provide appropriate supportto client.
realistic goalsand activelyparticipating inlife situation.
-
8/8/2019 compilation of grand case
42/51
-
8/8/2019 compilation of grand case
43/51
Identify/use availableresources.
participation in planning and evaluatingprocess.R: enhances
commitment to plan,optimizing outcomes.
Identify/use availableresources.
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSING DIAGNOSIS(Problem and Etiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
SUBJECTIVE:Galisud ko ug ginhawa sahay,tungod sa akong plemas
asverbalized by the patient.
OBJECTIVE:
Tachypnea; RR= 31cpm
Productive cough noted
Abnormal skin color (pale)
Impaired gas exchangerelated to retainedbronchial
secretions.
Short term:Within 5-10 minutes ofnursing care andintervention
the patientwill be able to:
Maintain airwaypatency.
Long term:Within 1-2days nursingcare and interventionsthe
patient will be ableto:
Demonstrate
improvedventilation and
INDEPENDENT:1. Monitor vital signs and cardiacrhythm.R: to note
any changes and/orcomplications.2. Note respiratory rate,
depth,pursed-lip breathing; and areas ofpallor/cyanosis; for
example,peripheral (nailbeds).R: to assess
respiratoryinsufficiency.3. Elevate head of bed/position
clientappropriately; provide airwayadjuncts, as indicated.
R: to maintain airway.4. Maintain adequate intake andoutput, but
avoid fluid overload.
After 5-10 minutes ofnursing care andintervention,
patientmaintained airwaypatency as evidencedby RR=30cpm. GOALWAS
PARTIALLYMET.
After 1-2days nursingcare and interventionsthe patient able
to:
Demonstrateimproved
ventilation andadequateoxygenation
-
8/8/2019 compilation of grand case
44/51
adequateoxygenationwithin clientsnormal limits andabsence
ofsymptoms ofrespiratorydistress.
Participate intreatmentregimen (e.g.,
breathingexercises,effectivecoughing, anduse of oxygen)within
level ofability/ situation.
R: for mobilization of secretions.5. Provide adequate rest and
limitactivities to within client tolerance.Promote calm/ restful
environment.R: helps limit oxygen needs/consumption.6. Provide
psychological support,active-listen questions/concernsR: to reduce
anxiety.7. Keep environmentallergen/pollutant free
R: to reduce irritant effect of dustand chemicals on airways.8.
Emphasize the importance ofnutritionR: in improving stamina
andreducing the work of breathing.
COLLABORATIVE:1. Encourage frequent positionchanges and deep
breathing/coughing exercises.R: Promotes optimal chestexpansion and
drainage ofsecretions.2. Administer medications, asindicated (e.g.
bronchodilators)R: to treat underlying conditions.
3. Provide supplemental oxygen asindicated by laboratory results
andclient symptoms/situation.
within clientsnormal limitsand absence ofsymptoms
ofrespiratorydistress.
Participate intreatmentregimen (e.g.,breathingexercises,
effectivecoughing, anduse of oxygen)within level ofability/
situation.
-
8/8/2019 compilation of grand case
45/51
R: to improve respiratory function/oxygen-carrying capacity.
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSING DIAGNOSIS(Problem and Etiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
RISK FACTORS:
Febrile; Temp= 39.6C
Lowered resistance/suppressed inflammatoryresponse
Productive cough noted
Somnolence (lethargy)
Infection related toinadequate primarydefenses (decreasedciliary
action/stasis ofsecretions).
Short term:Within 30minutes to 1hour of nursing care
andintervention the patientwill be able to:
Maintain coretemperaturewithin normalrange.
Be afebrile.
Long term:Within 2-3days ofnursing care andintervention the
patientwill be able to:
Verbalizeunderstanding of
INDEPENDENT:1. Vital signs taken and recorded.R: to note any
changes and/orcomplications.2. Stress proper hand hygiene by
allcaregivers betweentherapies/clients.R: a first-line of defense
againsthealthcare-associated infections(HAI).3. Provide for
respiratory isolation,as indicated.R: reduces risk of
cross-contamination.4. Encourage early ambulation, deepbreathing,
coughing exercises, and
position changes.R: for mobilization of secretionsand prevention
of aspiration/
After 30minutes to 1hour of nursing care andintervention, the
patientmaintained a coretemperature withinnormal range, and
wasafebrile as evidenced bybody temperature of36.9C. GOAL
WASMET.
After 2-3days of nursingcare and intervention,GOAL WAS MET,
thepatient able to:
Verbalize
understanding ofindividualcausative/ risk
-
8/8/2019 compilation of grand case
46/51
individualcausative/ riskfactor(s).
Identifyinterventions toprevent/ reducerisk of infection.
respiratory infections.5. Maintain adequate hydration.R: to
avoid bladder distention/urinary stasis.
COLLABORATIVE:1. Administer/ monitor medicationregimen and note
clients response.R: to determine effectiveness oftherapy/ presence
of side effects.2. Emphasize necessity of taking
antivirals/ antibiotics, as directed(e.g., dosage and length of
therapy).R: premature discontinuation oftreatment when client
begins tofeel well may result in return ofinfection and potentates
drug-resistant strains.
factor(s).
Identifyinterventions toprevent/ reducerisk of infection.
-
8/8/2019 compilation of grand case
47/51
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSING DIAGNOSIS(Problem and
Etiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONSAND RATIONALE
EVALUATION
SUBJECTIVE:
Lisud e-ginhawa, asverbalized by the patient.
OBJECTIVES:
RR= 36 cpm
Pallor noted
with O2 inhalation of 2 LMPvi nasal cannula
productive cough noted withyellowish in color.
Ineffective Breathing
Pattern related toimbalance betweenoxygen supply anddemand.
Short term:
Within 2-3 hours ofNursing Care andinterventions, patient
will:
Establish a normaland effectiverespiratory pattern.
INDEPENDENT:
1. Auscultate chest, notingpresence and character of
breathsounds, presence of secretions.R: Note any
changes/complications.2. Elevate HOB as appropriate.R: to promote
physiological/psychological ease of maximalinspiration.3. Encourage
slower/deeperrespirations, use of purse-liptechnique, and so on.R:
to assist the client in takingcontrol of the situation.4. Maintain
a calm attitude whiledealing with the client and SO/s.R: to limit
the level of anxiety.
5. Assist the client in the use ofrelaxation techniques
andencourage position of comfort.
After 2-3 hours of
Nursing Care andinterventions, GOALWAS MET, patient wasable to
established anormal and effectiverespiratory pattern.
-
8/8/2019 compilation of grand case
48/51
R: Promotes optimal chestexpansion and drainage ofsecretions.6.
Assist client to learn breathingexercise; diaphragmatic,abdominal
breathing, inspiratoryresistive, as pursed-lip asindicated.
7. Encourage adequate restperiods between activities to
prevent fatigue.R: to meet increased metabolicdemands.
COLLABORATIVE::1. Administer oxygen at lowestconcentration
indicated forunderlying pulmonary conditionand respiratory
distress: O2inhalation regulated at 2 LPM vianasal cannula.R: to
offset increased oxygendemandsand consumption.
-
8/8/2019 compilation of grand case
49/51
NURSING CARE MANAGEMENT
ASSESSMENT DATA(Subjective and Objective
Cues)
NURSINGDIAGNOSIS
(Problem andEtiology)
GOALS ANDOBJECTIVES
NURSING INTERVENTIONS ANDRATIONALE
EVALUATION
SUBJECTIVE:Mag mata-mata ko usahay, diliko maka tulog dali sa
akongubo, as verbalized by thepatient.
OBJECTIVE:
inadequate hours of sleep:
Before admission: 6 8hours
During admission: 4 6hou
Disturbed SleepPattern related topresence of coughand fever.
Long term:Within 8 hours ofNursing Care andinterventions,
patientwill:
Achievesoptimalamounts ofsleep asevidenced
byrestedappearance,verbalizationof feelingrested,
andimprovement
in sleeppattern.
INDEPENDENT:1. Observe and/or obtain feedback fromclient and
SO/s regarding usual bedtime,rituals/routines, number of hours of
sleep,time of arising and environmental needs,to determine usual
sleep pattern andprovide comparative baseline.2. Identify
circumstances that interruptsleep and frequency.R: to be able to
provide baseline forcomparison.3. Arrange care to provide
foruninterrupted periods for rest.R: determines ability to
participate inplanning/ executing care.4. Provide quiet environment
and comfortmeasures.
R: helps limit oxygen needs/consumption.5. Recommend midmorning
nap if one is
After 8 hours ofNursing Care andinterventions, GOALWAS MET,
patient wasable to achieved anoptimal amounts ofsleep as evidenced
byrested appearance,verbalization of feelingrested andimprovement
in sleeppattern.
-
8/8/2019 compilation of grand case
50/51
required.R: Napping, especially in the afternoon,can disrupt
normal sleep patterns.
-
8/8/2019 compilation of grand case
51/51