Embed Size (px)
Citation preview

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 1
Complementary Medicine: Exploring the Issues
Dr Ken Harvey MB BS, FRCPA
http://www.medreach.com.au
Short Course (2 of 3 sessions), Nov 2014, Multicultural Hub
• What is complementary &/or alternative medicine?
• Who uses it, why and what for?
• Regulation of products and practitioners;
• The current review of the private health insurance rebate for natural therapies;
• How do we know if it works: what is evidence?
• Evidence for and against specific products &/or therapies for certain conditions;
• Sources of good information about complementary medicine, and
• Using complementary medicine wisely.
Issues that could be explored
2

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 2
But first a new video from the TGA
3http://www.tga.gov.au/consumers/education-consumers.htm
Regulation of practitioners
44

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 3
Regulation of practitioners
Academy of Applied Hypnosis
Alexander Technique
Association of Massage Therapists Ltd
Association of Remedial Masseurs
Australasian Association of Ayurveda Inc
Australian Acupuncture & Chinese Medicine Association Ltd
Australian Feldenkrais Guild Inc
Australian Homœopathic Association
Australian Hypnotherapists Association
Australian Kinesiology Association
Australian Natural Therapists Association Ltd
Australian Naturopathic Practitioners Association
Australian Register of Homoeopaths Ltd.
Australian Society of Teachers of the Alexander Technique
Australian Traditional‐Medicine Society Ltd
Australian Association of Professional Homeopaths
Bowen Association of Australia
Bowen Therapist Federation of Australia
Buteyko Institute of Breathing & Health
Complementary Medicine Association
Dietitians Association of Australia
Endeavour College of Natural Health
Hypnotherapy Council of Australia
Institute of Registered Myotherapists
Institute of Registered Myotherapists of Australia
International Aromatherapy & Aromatic Medicine Association
International Iridology Practitioners Association
International Yoga Teachers' Association Inc
Massage Association of Australia
Natural Herbalists Association of Australia
Pilates Alliance Australasia
Pilates Method Association in Australia
Reflexology Association of Australia Ltd
Shiatsu Therapy Association of Australia
Tai Chi for Health Institute and Tai Chi Association of Australia
The International Institute of Psychosomatic Medicine
Regulation of practitioners
• National registration of some health professions(AHPRA) aims to ensure a minimal level of education and training, appropriate standards of professional behaviour and effective and efficient complaint mechanisms.
• Naturopaths and many other complementary medicine (CM)practitioners have not achieved national registration, in part because of division in their ranks, but also because of their varied training.
• CM practitioners may be members of professional associations but this does not necessarily ensure evidence‐based practice, continuing professional education or good complaint handling processes.
• State based health complaints entities and/or the ACCC are available for complaints about unregistered practitioners but have problems.
6

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 4
Regulation of practitioners
7
Regulation of practitioners
8

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 5
Options for unregistered practitioners, 2011
9
AHMAC Standing Council on Health, August 2013
• Ministers agreed to strengthen state and territory health complaints mechanisms via:– a single national Code of Conduct for unregistered health
practitioners to be made by regulation in each state and territory, and statutory powers to enforce the Code by investigating breaches and issuing prohibition orders;
– a nationally accessible web based register of prohibition orders; and
– mutual recognition of state and territory issued prohibition orders.
• AHMAC will undertake a public consultation on the terms of the first national Code of Conduct and proposed policy parameters to underpin nationally consistent implementation of the Code, for consideration by Ministers.
10

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 6
Code of conduct for unregistered health practitioners (NSW)
3. Health practitioners to provide services in safe and ethical manner
(a) A health practitioner must maintain the necessary competence in his or her field of practice,
(d) A health practitioner must recognise the limitations of the treatment he or she can provide and refer clients to other competent health practitioners in appropriate circumstances.
11. Health practitioners required to have clinical basis for treatments
A health practitioner must not diagnose or treat an illness or condition without an adequate clinical basis.
12. Health practitioners not to misinform their clients
(3) A health practitioner must not make claims, either directly or in advertising or promotional material, about the efficacy of treatment or services provided if those claims cannot be substantiated.
11
A National Code of Conduct for health care workers, 2014
• Clause 11 of the NSW Code and Clause 10 of the SA Code states:– ‘A health practitioner must have an
adequate clinical basis for treatment’.
• This clause has not been included in the draft National Code.
• However, clause 9 (c) states: – a health care worker must not make claims
either directly to clients or in advertising or promotional materials about the efficacy of treatment or services he or she provides if those claims cannot be substantiated.
12

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 7
• What is complementary &/or alternative medicine?
• Who uses it, why and what for?
• Regulation of products and practitioners;
• The current review of the private health insurance rebate for natural therapies;
• How do we know if it works: what is evidence?
• Evidence for and against specific products &/or therapies for certain conditions;
• Sources of good information about complementary medicine, and
• Using complementary medicine wisely.
Issues that could be explored
13
Natural Therapy Review Advisory Committee
• The review’s purpose is to ensure that taxpayer funds that are paid through the private health insurance rebate to subsidise natural therapies are underpinned by a credible evidence base that demonstrates their clinical efficacy, cost effectiveness and safety and quality.
• The Natural Therapy Review Advisory Committee (NTRAC) will use the NHMRC review of natural therapies and will make recommendations to as to which therapies are underpinned by a credible evidence base.
14http://www.health.gov.au/internet/main/publishing.nsf/Content/phi-natural-therapies

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 8
Private Health Insurance (PHI)
• The government (all taxpayers) currently provides a rebate to the cost of PHI to around 50% of the population who choose (or can afford) PHI.
15
Private Health Insurance (PHI)
• Many private health insurance (PHI) funds provide ancillary (extras) cover for a range of natural therapies.
• The ancillary benefits provided by different funds are currently a commercial decision; they take no account of clinical effectiveness and vary widely with respect to the services covered and the maximum money refunded per service per person per year.
16

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 9
Private Health Insurance: Natural therapies covered
17
Natural Therapy Review Advisory Committee
• While natural therapies only provide a relatively small proportion (6.5 per cent) of all ancillary benefits paid, they are growing at a much greater rate than other services.
• For example, between September 2000 and September 2013, the number of dental services funded doubled whereas natural therapies services increased nine fold.
18
http://phiac.gov.au/wp-content/uploads/2014/02/benefitsAUS.zip

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 10
NHMRC Natural TherapiesWorking Committee
• The NHMRC are currently reviewing the evidence for the effectiveness of “natural therapies” such as massage, aromatherapy, homeopathy, naturopathy, reflexology, rolfing and western herbalism for NTRAC.
• They are undertaking a systematic review of available evidence on their effectiveness in treating a variety of clinical conditions in humans and also assess evidence provided by stakeholders.
http://www.nhmrc.gov.au/your-health/complementary-and-alternative-medicines 19
Types of evidence
20
Meta-analysis

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 11
NHMRC assessment of evidence
• Randomised controlled clinical trials– the medicine is compared with a substance
that has no effect (placebo) in a group of people with the health condition (placebo‐controlled trial), or the medicine is compared with an effective standard treatment (controlled trial).
– each participant is given either the medicine or the placebo/other treatment at random (randomised trial) .
– participants and researchers do not know whether they are taking the medicine or the placebo/other treatment until the study is finished (double‐blinded trial).
21
NHMRC assessment of evidence
• Randomised controlled clinical trials (cont.)– there are enough participants to be reasonably
confident that, if there is a bigger change in the health condition in one group, this is not just due to chance.
– the correct statistical methods are used to analyse the results and ascertain whether the results could have been caused by chance.
– independent of vested interests (low bias).
– peer reviewed.
– published in reputable journals.
– replicated. 22

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 12
NHMRC assessment of evidence
• The results of individual studies need to be replicated in other independent studies, to make sure the effects seen were not just due to chance.
• The most reliable information comes from research that combines the results of all available similar studies (systematic reviews) and analyses the results together (meta‐analysis).
23
What is a systematic review?
A collation of all the evidence that fits pre‐specified eligibility criteria in order to answer a specific research question. It uses:• A clearly stated set of objectives with pre‐defined
eligibility criteria for including studies;
• An explicit, reproducible methodology;
• A systematic search that attempts to identify all studies that would meet the eligibility criteria;
• An assessment of the validity of the findings of the included studies, for example through the assessment of risk of bias; and
• A systematic presentation, and synthesis, of the characteristics and findings of the included studies
including meta‐analysis of the data. 24

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 13
NHMRC First Report: Homeopathy
• The NHMRC was concerned that unconventional products and procedures are often promoted to improve people’s health when there is little or no evidence of their benefit, except for the benefits people experience when they believe that a treatment is effective (the placebo effect).
• Sometimes patients may be misled into rejecting practices and treatments that are proven to be effective.
• There is disagreement about whether homeopathy is effective 25
Why?
Homeopathy
26
The New Melbourne Homeopathic Hospital 1885-1934St Kilda Road, Melbourne
(In 1934 it became Prince Henry’s allopathic hospital)
Samuel Hahnemann (1755-1843): The Father of Homeopathy

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 14
10:23 Campaign AgainstHomeopathy ‐Melbourne
27https://www.youtube.com/watch?v=kvgRMcfo0Yk
NHMRC First Report: Homeopathy
• Three main sources of information:– published systematic reviews,
– information provided by homeopathy interest groups and the public
– clinical practice guidelines and government reports on homeopathy published in other countries.
• The assessment was guided by a committee of experts appointed in 2012 (The NHMRC Homeopathy Working Committee).
28

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 15
NHMRC First Report: Homeopathy
• For each health condition, all the available evidence was grouped together to form a body ofevidence on that condition.
• A body of evidence was considered more reliable if it included studies that were high quality, well designed and with enough participants to make its results meaningful.
• A body of evidence was considered less reliable if there were very few studies, or if the studies were poor quality, badly designed, or included too few participants.
• The quality of evidence found was generally low.
29
NHMRC First Report: Homeopathy
• The NHMRC concluded that there were no health conditions for which there was reliable evidence that homeopathy was effective.
• This conclusion is similar to that of a 2010 UK House of Commons Science and Technology Select Committee, which also looked at the scientific evidence and stated:
– “In our view, the systematic reviews and meta‐analyses conclusively demonstrate that homeopathic products perform no better than placebos”.
30
http://consultations.nhmrc.gov.au/public_consultations/homeopathy_health

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 16
Industry response
• Australian homoeopathic organisations expressed concern at the limitations of the NHMRC evaluation which considered only systematic reviews of homeopathy rather than searching for all published studies of homeopathy.
• They were concerned that the NHMRC evaluation excluded observational and outcomes studies that examined effectiveness of treatments in real‐world conditions.
• The noted that although this evidence may in some instances be of a lower quality, it did not support a conclusion that homoeopathic treatment equates to placebo treatment.
• They also emphasised that, “the absence of evidence does not mean absence of effect”.
31http://www.asbrm.com.au/images/ASBRM_News_LetterV5_June2014.pdf
Possible Implications
32

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 17
Possible implications: Products & the TGA
HCG Diet Products Are Illegal• The Food and Drug Administration (FDA) is
advising consumers to steer clear of these "homeopathic" human chorionic gonadotropin (HCG) weight‐loss products. They are sold in the form of oral drops, pellets and sprays and can be found online and in some retail stores.
• FDA and the Federal Trade Commission (FTC) have issued seven letters to companies warning them that they are selling illegal homeopathic HCG weight‐loss drugs that have not been approved by FDA, and that make unsupported claims
http://www.biomedicals.com.auThe acronym hCG is for human Chorionic Gonadotrophin.
Homeopathic Drops for Weight lossLoose Weight Fast & Easily
Complaint sent to TGAProduct no longer sold in
Australia
Possible Implications
34
Ingredients: Arnica Montana (Leopard’s Bane) - 30C: Bellis Perennis(Daisy) - 30C: Chamomilla (Wild Cham o mile) - 30C: Ipecacuanha
(Ipecac) - 30C: Lycopodium (Clubmoss) - 30C
The Advertising Standards Authority (ASA) of New Zealand has upheld a complaint regarding advertising of the homeopathic product “No-Jet-Lag / Jet-Ease” in an Auckland pharmacy. The complaint lodged by the Society for Science Based
Healthcare in July 2014, alleged that the advertisement’s claims about the product that “It Really Works” for “Homeopathic Jet Lag Prevention” were unsubstantiated and
misleading.

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 18
Possible Implications
35
Possible Implications
36
HLT60612 - Advanced Diploma of Homoeopathy (Release 1)

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 19
Possible Implications
37
Possible Implications
38http://www.youtube.com/watch?v=p2FT8kNCYMs

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 20
Possible Implications
Natural Therapy Review Advisory Committee
• Services subsidised under Medicare by health professionals regulated by AHPRA under the National Registration and Accreditation Scheme (NRAC) will not be affected by the review.
• These include Chinese Traditional Medicine, Chiropractic and Osteopathy.
http://www.health.gov.au/internet/main/publishing.nsf/Content/phi-natural-therapies 40

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 21
Should AHPRA registered practitioners be exempt?
41
Should AHPRA registered practitioners be exempt?
42http://www.universalhealth.com.au/services/pdf/chiropractic_paediatric.pdf
http://www.malchiro.com.au/testimonials.html

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 22
Should AHPRA registered practitioners be exempt?
43
The National Law (s.133) prohibits advertising that:
• Is false, misleading or deceptive or is likely to be so,
• Offers a gift, discount or other inducement to attract a user of the health service without stating the terms and conditions of the offer,
• Uses testimonials or purported testimonials,
• Creates an unreasonable expectation of beneficial treatment, and/or
• Encourages the indiscriminate or unnecessary use of health services.

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 23
• What is complementary &/or alternative medicine?
• Who uses it, why and what for?
• Regulation of products and practitioners;
• The current review of the private health insurance rebate for natural therapies;
• How do we know if it works: what’s evidence?
• Evidence for and against specific products &/or therapies for certain conditions;
• Sources of good information about complementary medicine, and
• Using complementary medicine wisely.
Issues that could be explored
45
What’s evidence?
• Friends, colleagues, social media (and testimonials) might say, “It worked for me”.
• But the plural of anecdote is not evidence.
• There are a number of reasons why consumers (and practitioners) convince themselves that a treatment is effective when it is not including:
– Placebo effect (patient’s expectation regarding an intervention),
– The natural history of disease (symptoms may wax and wane) ,
– Confirmation bias (seeing what you expect to see),
– Cognitive dissonance (ignoring results not in accord with expectations),
– Endorsement by “celebrities” who receive multi‐million payments (be especially suspicious).
• In short, personal evaluation is quick, convincing and often wrong, while blinded, controlled clinical trials are slow, complex, and costly.
• However, the latter are important as they often show that initially promising results are not replicated by larger and better conducted studies.
46

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 24
Types of evidence
47
Meta-analysis
The Age 23/06/2014
48

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 25
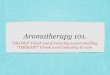
J Clin Psychopharmacol. 2009 Aug; 29(4):378‐82
• We conducted a randomized, double‐blind, placebo‐controlled efficacy and tolerability trial of Matricaria recutita (chamomile) extract therapy in patients with mild to moderate generalized anxiety disorder (GAD).
• Sixty‐one outpatients with mild to moderate GAD were enrolled, and 57 were randomized to either double‐blind chamomile extract (n = 28) or placebo therapy (n = 29) for 8 weeks. The study was powered to detect a statistically significant and clinically meaningful group difference in change over time in total Hamilton Anxiety Rating (HAM‐A) scores.
• We observed a significantly greater reduction in mean total HAM‐A score during chamomile versus placebo therapy (P = 0.047). One patient in each treatment group discontinued therapy for adverse events.
• This is the first controlled clinical trial of chamomile extract for GAD. The results suggest that chamomile may have modest anxiolytic activity in patients with mild to moderate GAD. Future studies are needed to replicate these observations.
49
New drug development
• Pre‐clinical– Animal studies (toxicology)
• Human clinical trials– Phase I
• Healthy human volunteers; dose finding; small numbers (typically 6–60)
– Phase II• In patients; safety/efficacy; dose confirmation
– Phase III• In patients; randomized against placebo or the current standard treatment; safety/efficacy; larger numbers (typically 1000–3000)
• Marketing application (Therapeutic Goods Administration)
• Product licensed for marketing– Phase IV
• Post‐marketing; compared against active treatments, considered for subsidy (PBS). 50

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 26
Problem reporting
Properly evaluated AUST R CMs?
http://www.tga.gov.au/industry/cm-basics-regulation-evaluation.htm 52

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 27
• Of the 25 products on the list most are unremarkable: Iron, Calcium, Vitamin D, Psyllium fibre and Ispaghula husk for constipation, Clove oil for toothache.
• More innovative products are:– IBEROGAST (Flordis). A specific nine herb mixture, “for the
treatment of functional dyspepsia and irritable bowel syndrome”.
– KALOBA (Schwabe) containing a specific extract of Pelargonium sidoides (EPs 7630) for “for the treatment of acute bronchitis and sinusitis” (an alternative to prescribing an antibiotic).
– FLEXAGIL (Blackmores). A specific extract of Symphytum officinale(Comfrey) for topical application for the “relief of lower back pain, painful joints and strains”.
TGA list of evaluated registered CMs
http://www.tga.gov.au/industry/cm-basics-regulation-evaluation.htm 53
Flordis Iberogast registration dossier
• 14,200 pages Clinical data
• 7000 pages Toxicological data
• 5,600 pages Quality data
• 105 pages Local data
Total: 27,455 pages
$150,000 submission cost
Iberogast is a clinically proven nine herb mixture for functional dyspepsia and irritable
bowel syndrome (AUST R: 168967)

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 28
www.mediadoctor.org.au
Problems: media
• Many media stories about new medicines– Overstate benefits
– Understate risks
– Understate costs
– Fail to disclose relevant financial ties.
• 207 stories from 1994 to 1998– 40% did not report benefits quantitatively
• Of those that did, 83% reported only relative benefits
– 53% did not mention potential harm
– 70% did not mention cost of therapy
– 39% disclosed ties where it was relevant.55Moynihan R et al. NEJM 2000;342:1645–50
Relative and absolute benefits / risks
• WHI ‐ Risks and benefits of HRT in healthy post‐menopausal women (JAMA 2002; 288: 321–33)
• A randomized, placebo‐controlled, primary prevention trial (planned duration, 8.5 years) in which 16,608 postmenopausal women aged 50‐79 years (the majority over 60 years) with an intact uterus at baseline were recruited by 40 US clinical centres in 1993‐1998.
• It reported the risk of invasive breast cancer increased by 26% (relative risk) with HRT which triggered wide‐spread panic and many women ceased HRT.
• In fact, the risk only increased by 8 cases per 10,000 person years (38 versus 30 per 10 000 person‐years) and absolute risk increase of 0.08%.
• Always ask for the absolute numbers involved, not just the percentage risk or benefit. 56

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 29
Evidence: questions to ask
• How strong is the evidence to support the claims being made about the therapy:– levels of evidence?
– trials registered?
– results published?
– replicated by others?
• Could the therapy be shonky?– glowing testimonials but no trial results?
– do those promoting it profit from it?
– listed in Quackwatch?
– complaints upheld by the CRP?
– product removed from the ARTG by the TGA? 57
Evidence: questions to ask
• What’s the size of the potential benefit and risk offered by the therapy, and for what types of patients:– statistically significant?
– clinically significant?
– absolute benefits and risks (not relative)?
– Numbers needed to treat?
– Numbers needed to harm?
• What are the costs of the therapy and are the potential risks and benefits worth the cost?
58
http://www.thennt.com/

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 30
Evidence: questions to ask
• What are the alternatives to the therapy being offered:– watchful waiting?
• research is always progressing.
– non‐drug options such as physiotherapy?
– evidence‐based complementary therapies?
• What do reputable patient support groups and their medical advisors say?
• In short, while there are many ethical responsible and knowledgeable health practitioners and therapeutic goods companies out there….
• I reiterate, ask for (and evaluate) the evidence.
59
• What is complementary &/or alternative medicine?
• Who uses it, why and what for?
• Regulation of products and practitioners;
• The current review of the private health insurance rebate for natural therapies;
• How do we know if it works: what is evidence?
• Evidence for and against specific products &/or therapies for certain conditions;
• Sources of good information about complementary medicine, and
• Using complementary medicine wisely.
Last session
60

Complementary Medicine: Exploring the Issues U3A Short Course (2 of 3 sessions), Nov 2014
Dr Ken Harvey Page 31
Last session: Evidence for specific products &/or therapies
61