Embed Size (px)
Citation preview

Genetic Brief
Complete Mitochondrial DNA Sequence Analysis in a Familywith Early-Onset Dystonia and Optic Atrophy
Michael D. Brown, PhD,1* Seyed Hosseini, PhD,2 Israel Steiner, MD,3 Douglas C. Wallace, PhD,4
and Isabelle Korn-Lubetzki, MD5
1Division of Basic Medical Sciences, Mercer University School of Medicine, Macon, Georgia, USA2Department of Pathology, Emory University School of Medicine, Atlanta, Georgia, USA
3Department of Neurology, Hadassah University Hospital, Jersusalem, Israel4MAMMAG, University of California Irvine, Irvine, California, USA
5Neurological Service, Bikur Cholim Hospital, Jerusalem, Israel
Abstract: The combination of optic atrophy and dystonia hasbeen etiologically associated with mitochondrial DNA(mtDNA) mutations. We report here on the complete mtDNAsequence from the proband of a consanguineous family exhib-iting “mitochondrial-like” optic atrophy and dystonia. A can-didate tRNAGly mutation was identified that was unique to thefamily. However, the mutation was homoplasmic in both af-
fected and unaffected family members and we were unable todemonstrate a biochemical defect in patient mitochondria.Hence, it is unlikely that a mtDNA mutation accounts for thephenotype in this family. © 2003 Movement Disorder Society
Key words: mitochondria; dystonia; optic atrophy; mtDNAmutations
Three different mitochondrial DNA (mtDNA) mis-sense mutations have been associated with the co-occur-rence of optic atrophy and dystonia. A heteroplasmic Gto A mutation at nucleotide position 14459 of the ND6gene precipitates a severe reduction in mitochondrialcomplex I (NADH dehydrogenase) activity, resulting inthe segregation of Leber’s hereditary optic atrophy(LHON) and/or a severe, generalized, early-onset dysto-nia in Hispanic, Caucasian, and African American fam-ilies.1,2 Clinically, 14459A-positive pediatric dystoniapatients display a range of neurological dysfunctionsfrom pure dystonia with normal cognition to a morecomplex neurological disease featuring dystonia,pseudobulbar signs, corticospinal tract dysfunction, and
mental retardation.2,3 Optic atrophy onset and progres-sion is typical for LHON.4 Neuroradiologically, 14459A-positive patients exhibit bilateral basal ganglia lesionsinvolving primarily the putamen and caudate nuclei.2 Asevere complex I deficiency associated with a heteroplas-mic 11696G and a homoplasmic 14596A mtDNA muta-tion was reported subsequently in a large, maternallyinherited Dutch family with a very similar phenotype.5
Hence, optic atrophy with dystonia is not an unrecog-nized or unusual clinical manifestation of mitochondrialdisease.
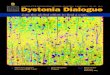
More recently, we have reported a consanguineous Is-raeli family with clinical and neuroradiological similaritiesto the above cases (Fig. 1).6 Like the mtDNA-based cases,this family featured: (1) early-onset uni- or bilateral dysto-nia (average age of onset; 7 years); (2) bilateral opticatrophy (age of onset in the second to third decade) char-acterized by reduced visual acuity and optic disc pallor,although no peripapillary telangiectasias were noted; and(3) bilateral and symmetric putaminal lesions with addi-tional but variable involvement of the caudate nucleus.
*Correspondence to: Dr. Michael D. Brown, Division of BasicMedical Sciences, Mercer University School of Medicine, Macon, GA31207. E-mail: [email protected]
Received 7 June 2003; Accepted 31 July 2003DOI 10.1002/mds.10646
Movement DisordersVol. 19, No. 2, 2004, pp. 235–237© 2003 Movement Disorder Society
235

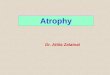
Although affected children from an unaffected motherand non-transmission from affected males are character-istic of pathogenic mtDNA mutation inheritance, it is notpossible to discern between mitochondrial/maternal, au-tosomal recessive, or X-linked transmission of the dis-ease in our Israeli family by pedigree analysis alone.Marked clinical similarities, however, between the Is-raeli family and the “mitochondrial” optic atrophy-dys-tonia families raised the possibility that a mtDNA muta-tion may be relevant to the family’s neurological disease.In our original report, we tested multiple family membersfor the 14459A mutation and several other LHONmtDNA mutations.6 Although all screens were negative,it did not rule out the possibility of a new mtDNAmutation. Thus, we completely sequenced lymphoblastmtDNA from the proband of the Israeli optic atrophy-dystonia family. Automated sequence analysis identified12 homoplasmic mutations (263G, 750G, 1438G,4769G, 8860G, 9995C, 11447G, 12528A, 14215C,15326G, 15724G, and 16189C) relative to the revisedCambridge reference sequence.7 Three of these, 9995Cin the tRNAGly gene, 12528A in the ND5 gene, and14215C in the ND6 gene, are newly described variants.The 12528A and 14215C polymorphisms do not changean amino acid and hence are not considered candidatemutations. Further, the absence of the 7028T and10398G polymorphisms characterizes unambiguouslythe proband mtDNA as belonging to European haplo-group H. Haplogroup H is the most common of ninephylogenetic lineages that comprise European-derivedmtDNA variation, and is found in roughly 40% of Eu-ropean mtDNAs.8,9 The 9995C tRNAGly mutation altersa non-phylogenetically conserved nucleotide and dis-rupts an A-T base pair in the tRNA acceptor stem (Fig.2). A mutation-specific polymerase chain reaction-re-striction fragment length polymorphism (PCR-RFLP)
test was developed to confirm the presence and ho-moplasmic state of the mutation. For this test, one PCRprimer contained an A to G mismatch at nucleotideposition 9998. The presence of this mismatched base andthe 9995C variant creates an Eco57I restriction endonu-clease site in the PCR product, permitting rapid identi-fication of 9995C-containing mtDNAs. Using this ap-proach, we verified 9995C homoplasmy in the probandmtDNA and further demonstrated that the mutation washomoplasmic in 8 affected and unaffected maternallyrelated family members. A screen of haplotype-matchedcontrol mtDNAs indicated that the mutation was notpresent in 63 haplogroup H controls. Furthermore, the9995C variant has not been reported as either a diseasemutation or a polymorphism in the human mtDNA da-tabase, MITOMAP (online at http://mitomap.org).Hence, the 9995C tRNAGly mutation has only beenfound in our optic atrophy-dystonia family.
Respiration studies were carried out on mitochondriaisolated from proband lymphoblasts to assess the functionalsignificance of the 9995C mutation. No reduction in com-plex I- or complex II-linked respiration rates (state III, state
FIG. 1. Partial pedigree of Israeli family exhibiting early-onset dys-tonia and optic atrophy. Shaded symbols indicate individuals manifest-ing both dystonia and optic atrophy. Arrow indicates proband. Noteconsanguinity in first generation. Some unaffected males have pro-duced unaffected offspring.
FIG. 2. Schematic of tRNAGly showing position of the T to C mutationat nucleotide position 9995. The 9995C mutation disrupts an A-T basepair in the tRNAGly acceptor stem.
236 M.D. BROWN ET AL.
Movement Disorders, Vol. 19, No. 2, 2004

IV, or uncoupled), state III ratios,10 or ADP/O ratios werefound in comparison with 21 control lymphoblasts (data notshown). These findings corroborate preliminary results de-scribed in the original report on this family in that noreduction in complex I, II, III, or IV or in citrate synthase-specific enzyme activity was found in biopsied skeletalmuscle from an affected family member.6 The 9995C mu-tation constitutes a candidate mutation for the optic atrophy-dystonia phenotype exhibited in this family because it dis-rupts a base pair in the tRNAGly acceptor stem (thuspotentially perturbing tRNA charging, mitochondrial trans-lation, or both) and it has not been found in either literaturecontrols or in a large group of mtDNA haplotype-matchedcontrols. Homoplasmy for a pathogenic mtDNA tRNAmutation would be unprecedented, however, particularlywhen the same homoplasmic mutation is found in unaf-fected, maternally related family members. Moreover, wewere unable to detect a respiration defect in proband lym-phoblast mitochondria, suggesting that mitochondrial func-tion is not compromised. Thus, these data indicate that thematernal transmission of the 9995C mutation is unlikely tobe etiologically relevant and suggest that either an autoso-mal recessive or X-linked genetic mechanism is responsiblefor the optic atrophy-dystonia in the Israeli family.
Acknowledgments: This work was supported by the Na-tional Institutes of Health (NEI 014393 to M.D.B. and NS21328 to D.C.W.). We thank Dr. V. Mayorov and Mr. J. Allenfor their assistance.
REFERENCES
1. Jun AS, Brown MD, Wallace DC. A mitochondrial DNA mutationat nucleotide pair 14459 of the NADH dehydrogenase subunit 6gene associated with maternally inherited Leber hereditary opticneuropathy and dystonia. Proc Natl Acad Sci USA 1994;91:6206–6210.
2. Shoffner JM, Brown MD, Stugard C, et al. Leber’s hereditary opticatrophy plus dystonia is caused by a mitochondrial DNA pointmutation. Ann Neurol 1995;38:163–169.
3. Novotny EJ, Singh G, Wallace DC. Leber’s disease and dystonia:a mitochondrial disease. Neurology 1986;36:1053–1060.
4. Kerrison JB, Newman NJ. Clinical spectrum of Leber’s hereditaryoptic neuropathy. Clin Neurosci 1997;4:295–301.
5. De Vries DD, Went LN, Bruyn GW, Scholte HR, Hofstra RM,Bolhuis PA, van Oost BA. Genetic and biochemical impairment ofmitochondrial complex I activity in a family with Leber hereditaryoptic neuropathy and hereditary spastic dystonia. Am J Hum Genet1996;58:703–711.
6. Korn-Lubetzki I, Blumenfeld A, Gomori JM, Soffer D, Steiner I.Progressive dystonia with optic atrophy in a Jewish-Iraqi family.J Neurol Sci 1997;151:57–63.
7. Andrews RM, Kubacka I, Chinnery PF, Lightowlers RN, TurnbullDM, Howell N. Reanalysis and revision of the Cambridge refer-ence sequence for human mitochondrial DNA. Nat Genet 1999;23:147.
8. Finnila S, Lehtonen MS, Majamaa K. Phylogenetic network forEuropean mtDNA. Am J Hum Genet 2001;68:1474–1484.
9. Torroni A, Huoponen K, Francalacci P, et al. Classification ofEuropean mtDNAs from an analysis of three European popula-tions. Genetics 1996;144:1835–1850.
10. Brown MD, Starikovskaya E, Derbeneva O, et al. The role ofmtDNA background in disease expression: a new primary LHONmutation associated with the Western Eurasian haplogroup J. HumGenet 2000;110:130–138.
EARLY-ONSET DYSTONIA AND OPTIC ATROPHY 237
Movement Disorders, Vol. 19, No. 2, 2004