Embed Size (px)
Citation preview
Lasers in Surgery and Medicine 5:291-296 (1985)
Complete Patency in Thrombus-Occluded Arteries Two Weeks After Liaser Recanalization
Jetan Marco, MD, Paul J. Silvernail, BA, Gerard Fournial, MD,
Daniel S.J. Choy, MD, Jean Fajadet, MD, and Robert 6. Case, MD
La'3oratory for Experimental Cardiology, St. Luke's-Roosevelt Hospital Center, New York (f).,l.S., D.S. J. C., R. B.C.), and Hopital Purpan, Centre Hospitalier Regional De Toulouse, Seivice De Cardiologie, Place Du Docteur Baylac, Toulouse, France (J. M., G. F., J. F.)
Thl: potential problem of rethrombosis after laser recanalization was studied in 16 thrombus-occluded canine femoral arteries. Ballooin de-end(ithelialization and thrombin-human blood injection produced adherent, c'ompletely occlusive thrombi 4 13 f 1.54 cm in length; laser exposure of the thrombi occurred at 18.35 22.1 hours. The argon laser catheter was introduced via a proximal arteriotomy and a power (43 .83 296.8'7 seconds. Follow-up period was 14 days. All arteries were patent immediately after and 14 days following lasing, ds demonstrated by angiography. There was no vessel perforation. Seven of the dogs were maintained on aspirin and dipyridamole 4 days before and throughout the study, but therc were no differences in thrombus length, laser power, or duration of laser exposure between these dogs and those receiving no anti-platelet therapy. Control thrombosed arteries (without laser energy applica- tion) showed n o autolysis within 14 days in all dogs and up to 95 days in three dogs followed for this period of' time.
These data show that rethrombosis of totally occluded, thrombosed arteries is not present up to 2 weeks later after laser recanalization, with or without the aid 01' anti-platelet therapy.
0.58 W delivered for 411.3
Klej P ords: rethrombosis, laser recanalization, argon laser
INTRODUCTION
Several investigators have demonstrated that an intravascular laser beam can creatl: a new lumen in an atherosclerotic artery 12-11. 151, thus opening the way for
Address reprint requests to Robert B . Case, MD, Laboratory for Experimeiital Cardiology, St. Lukc's Horpiral S&R 11, 114th St. and Amsterdam Avenue, New York, IVY 10025.
Accepted for publication Deccmber 10, 1084.
0 19%5 Alan H. Liss. Inc.
292 Marco et a1
revascularization of atherosclerotic arteries by a laser catheter provided that the three major potential problems of this techique-vessel wall perforation, distal emboliza- tion, and rethrombosis at the treated site-can be shown to be unimportant or can be dealt with effectively. Endothelial injury may initiate thrombosis [ 13,141, and a charred surface may be left following intravascular laser use [12,13]. To date, there has been little information in the experimental literature regarding rethrombosis after laser exposure. However, it is important to note that in the nine cases in which laser energy has been used successfully to recanalize human coronary arteries, there has been reocclusion in six of seven within 25 days [9,lO, unpublished observations]. One coronary artery remained open at 25-day follow-up, and another was excised immediately following laser recanalization. Also, it was stated at a recent meeting following presentation [ 161 of laser revascularization of three human femoral arteries that all had reoccluded. While it is possible that rethrombosis could have resulted from competitive flow within a bypass graft, or as a result of low flow within the newly laser-recanalized artery, the extent of this problem must be more clearly defined if laser revascularization is to become a reality. The present communication examines the incidence of rethrombosis over a period of 2 weeks after laser revascularization of obstructed large canine femoral arteries.
MATERIALS AND METHODS
This study was conducted by two teams working in Toulouse, France, and New York, New York. The investigators had undergone comparable training together in New York prior to the start of the experiments.
The model of arterial obstruction used for this study was the canine femoral artery that had been completely occluded by a fixed thrombus. We have previously described the technique for producing an occlusive adherent arterial thrombus [ 151. It may be summarized as follows: following anesthesia with chlorpromazine hydrochlo- ride ( 1 .O mg/kg, subcutaneously) and pentobarbitol sodium (29 mg/kg, intravenously) and an intramuscular injection of penicillin (1.2 X 106 units) 1 hour prior to surgery, both femoral areas were opened and the arteries dissected free for approximately 7 cm. In a clamp-isolated segment of dissected artery under direct vision, a balloon catheter was inserted to produce endothelial damage, followed by injection of a thrombin-human blood mixture. Following continued segment isolation for 2 hours, a completely occlusive thrombus resulted, which has remained totally occlusive for more than 3 months. The dogs were then returned to their cages. All laser-exposed thrombi in these studies were less than 3 days old and were completely occlusive, as demonstrated by angiography . Two dogs had both femoral arteries recanalized by laser energy. In the other 12 dogs, the artery contralateral to that undergoing laser recanalization was similarly thrombosed to serve as a control, but was not subject to laser energy. These control arteries were followed in the same manner as those undergoing laser recanalization.
Animal Groups Fourteen large (weight 12-32 kg, mean = 21.5 kg) healthy mongrel dogs were
used in the study. The animals were divided into two groups. Group I (n = 7, nine arteries laser treated) received no anti-platelet therapy, other than heparin during vascular repair, for the duration of the study. Group I1 (n = 7, seven arteries laser
Vessel Patency Following Laser Recanalization 293
treated) were started on dipyridamole (150 mg/day per 0s [P.o.]) and aspirin (130 mg/day p.0.) 4 days prior to thrombus formation and maintained on this drug regimen throughout the study.
Laser Protocol In both Toulouse and New York, identical protocols were followed by persons
well acquainted with this type of laser and the procedures described herein. The dogs were again anesthetized and the femoral wounds opened. They were given a 5.0-mg bolus injection of verapamil hydrochloride intravenously to prevent vascular spasm during the laser procedure. A proximal arteriotomy was made 1-2 cm from the thrombus. Two centimeters distal to the thrombus, a temporary, atraumatic ligature (umbilical tape) was placed to prevent retrograde flow of blood upon recanalization, thus allowing the thrombus to be lased in a clear field under normal saline.
The power output of the laser catheter was measured at the optical fiber tip before laser recanalization by directing the catheter perpendicularly to a Coherent Model 210 power meter with the tip 1.0 cm from the sensor. The minimum power used to recanalize was 3.0 W. The time needed for recanalization was recorded. Laser exposure was continued using a continuous mode until most of the thrombus had been vaporized, as demonstrated by visual observation, evidence of distal flow, and angiography.
The construction of the laser catheter has been described elsewhere [ 111. Briefly, it consists of an 85-pm silica fiber core with plastic cladding, bringing the total outer diameter to 125 pm. The optical fiber was passed through the balloon lumen of a Gruentzig 3F balloon dilatation catheter after the balloon assembly had been cut off, rendering the optical fiber eccentric relative to the center of the catheter. A Harvard peristaltic perfusion pump was attached to the fluid lumen of the catheter and 22 mll min of saline was infused during lasing. The laser used was a Coherent Model 1000 argon laser (Coherent Inc., Palo Alto, CA).
Prior to laser recanalization, an arteriogram was performed through the laser catheter. Following laser recanalization, a second arteriogram was performed after removal of the distal ligature. The animals were then given 5,000 units of heparin intravenously, and the arteriotomy repaired with 6-0 monofilament nylon sutures. The heparin was then reversed with 50 mg of protamine sulfate. The wounds were closed with 3-0 and 2-0 silk and the animals received penicillin (1.2 X lo6 units) intramuscularly 1 day following the procedure.
In the control vessels (ie, those not undergoing laser recanalization) the same procedures were used, except the laser power was never turned on. The laser catheter was left in situ for a comparable amount of time and maneuvered as if lasing were taking place.
Follow-up arteriograms were obtained at 7 days in five arteries and 14 days in fourteen arteries. The control arteries were similarly visualized angiographically at these time intervals. These angiograms were performed via a carotid arteriotomy; both lasered and unlasered arteries were visualized at each time interval.
RESULTS
With laser energy we recanalized 16 thrombosed femoral arteries in 14 dogs. 1.54 cm). They were 4.5- The thrombi ranged from 1.5 to 7.0 cm (mean = 4.13
294 Marco et a1
72 hours old (mean = 18.35 k 22.1 hours) at the time of laser treatment. In all cases the thrombi were totally occlusive as demonstrated by angiography prior to laser exposure. The laser powers used ranged from 3.0 to 5.0 W (mean = 3.83 +_ 0.58 W). The duration of exposure (using a continuous mode of laser energy delivery) ranged from 55 to 1140 seconds (mean = 411.3 + 296.87 seconds) (Table I). There were no trends among those dogs on anti-platelet therapy (Group 11) and those on no medication (Group I) concerning any of the above parameters.
None of the 14 control arteries in the 16 dogs of groups I and I1 underwent self- lysis within 14 days. Three of the group I1 dogs were followed for 95 days, and similarly, there was no thrombus autolysis.
No vessel perforation was observed visually, and there were no incidents of dye extravasation during angiography in arteries undergoing laser recanalization.
Follow-up arteriograms immediately after laser treatment and at 7 and 14 days afterward always showed a patent, remarkably unobstructed arterial lumen with no evidence of residual thrombus (Table 11). Visual inspection of arteries excised at 14 days revealed a patent lumen with little evidence of thrombus. Some arteries were not tested at 7 or 14 days owing to technical problems.
DISCUSSION
The concept of using laser energy to recanalize thrombus- or plaque-occluded arteries has received considerable attention since its initial description in 1980 [ 1,2]. The most important questions regarding the safety and efficacy of the use of lasers intravascularly are starting to be answered.
Gessman et a1 [6] found an absence of filterable debris when laser treating a single cadaver coronary artery under saline attached to a model. We have confirmed these findings in this laboratory by finding an absence of distal embolization in laser- recanalized, living canine, thrombus-occluded femoral arteries [ 151 and human ca- daver carotid arteries (unpublished observations). Hence, it appears that distal embo- lization is not a significant risk when recanalizing thrombus- or plaque-occluded arteries with laser energy.
Of equal importance is the question of rethrombosis in a vessel after undergoing laser recanalization. To date, little experimental information is available on this aspect of laser recanalization. Choy et al [9, 10, unpublished observations] have reported that six of seven human coronary arteries recanalized with an argon laser during coronary artery bypass surgery reoccluded within 25 days of the procedure, which could be due to competition between the newly laser-recanalized coronary artery and the vein bypass graft. Similarly, it was stated following presentation at the IX European Congress of Cardiology meeting in July 1984 that three of three human femoral arteries recanalized with laser energy reoccluded [16]. Ginsburg et al [8] reported that a patient undergoing laser recanalization of a totally occluded superficial femoral artery and a 95% stenotic deep femoral artery had only leg fatigue after walking 2-3 blocks, and no nocturnal or rest pain 6 months after the recanalization procedure, but no data on follow-up arteriograms have been reported. The patient was maintained on aspirin (325 mg/day) after recanalization. The above represent all clinical trials of laser revascularization performed to date.
The success or failure of preventing rethrombosis in laser-recanalized vessels depends on many factors-laser operator experience and ability to minimize wall
Vessel Patency Following Laser Recanalization 295
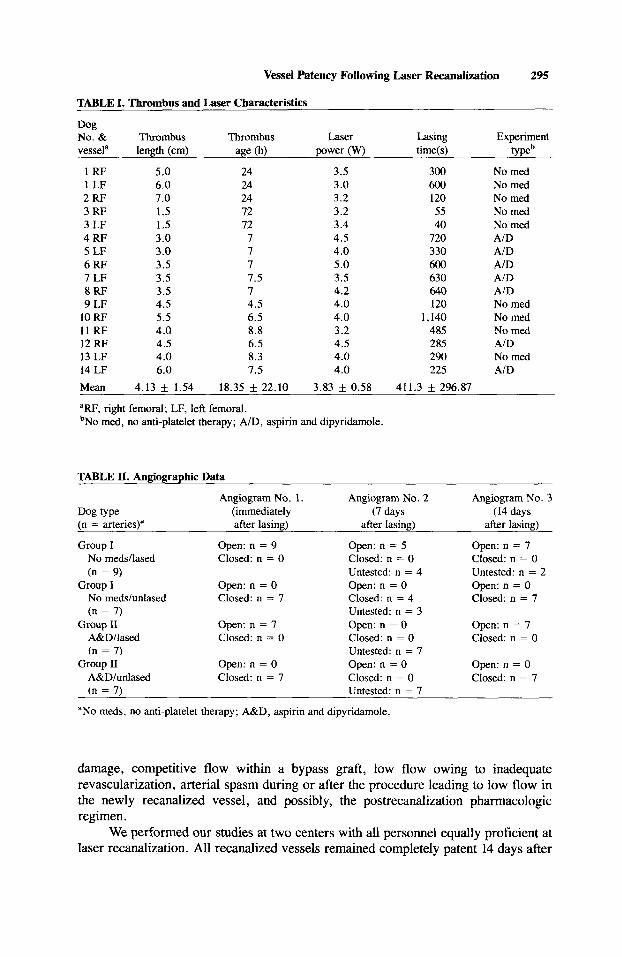
TABLE I. Thrombus and Laser Characteristics
Dog No. & Thrombus Thrombus Laser Lasing Experiment vessela length (cm) age (h) power (w) time(s) typeb
1 RF 5.0 24 3.5 300 No med 1 LF 6.0 24 3.0 600 No rned 2 RF 7.0 24 3.2 120 No med 3 RF 1.5 72 3.2 55 No med 3 LF 1.5 72 3.4 40 No med 4 RF 3.0 7 4.5 720 A/D 5 LF 3.0 7 4.0 330 AID 6 RF 3.5 7 5.0 600 AID 7 LF 3.5 7.5 3.5 630 AID 8 RF 3.5 7 4.2 640 A/D 9 LF 4.5 4.5 4.0 120 No rned
10 RF 5.5 6.5 4.0 1,140 No med 11 RF 4.0 8.8 3.2 485 No med 12 RF 4.5 6.5 4.5 285 AID 13 LF 4.0 8.3 4.0 290 No med 14 LF 6.0 7.5 4.0 225 AID Mean 4.13 i 1.54 18.35 22.10 3.83 k 0.58 411.3 & 296.87
'RF, right femoral; LF, left femoral. bNo rned, no anti-platelet therapy; AID, aspirin and dipyridamole.
TABLE 11. Angiographic Data
Dog type (immediately (7 days (14 days (n = arteries)a after lasing) after lasing) after lasing)
Angiogram No. 1. Angiogram No. 2 Angiogram No. 3
Group I No meds/lased (n = 9)
No rneds/unlased (n = 7)
A&D/lased (n = 7)
A&D/unlased (n = 7)
Group I
Group I1
Group I1
Open: n = 9 Closed: n = 0
Open: n = 0 Closed: n = 7
Open: n = 7 Closed: n = 0
Open: n = 0 Closed: n = 7
Open: n = 5 Closed: n = 0 Untested: n = 4 Open: n = 0 Closed: n = 4 Untested: n = 3 Open: n = 0 Closed: n = 0 Untested: n = 7 Open: n = 0 Closed: n = 0 Untested: n = 7
Open: n = 7 Closed: n = 0 Untested: n = 2 Open: n = 0 Closed: n = 7
Open: n = 7 Closed: n = 0
Open: n = 0 Closed: n = 7
"No meds, no anti-platelet therapy; A&D, aspirin and dipyridamole.
damage, competitive flow within a bypass graft, low flow owing to inadequate revascularization, arterial spasm during or after the procedure leading to low flow in the newly recanalized vessel, and possibly, the postrecanalization pharmacologic regimen.
We performed our studies at two centers with all personnel equally proficient at laser recanalization. All recanalized vessels remained completely patent 14 days after
296 Marco et a1
the procedure regardless of the presence or absence of anti-platelet drug therapy. No vessels were perforated during the procedure. This is noteworthy because the length of laser-treated thrombus in these studies far exceeded that found in the clinical setting of acute coronary thrombosis. Also, the model of vascular obstruction resembles the clinical presentation of deep vein thrombosis, but there are no reports to date of clinical laser recanalization of thrombosed veins.
CONCLUSIONS
We conclude that laser recanalization of thrombus-occluded vessels can be achieved without concern of rethrombosis within 2 weeks after laser treatment. However, given prior data in human studies, application of laser energy to athero- sclerotic vessels warrants more investigation before laser recanalization can achieve clinical relevance.
REFERENCES
1 . Choy DSJ: Fiberoptic laser tunneling device. Presented at the International Conference on Lasers: “Digest of Technical Papers.” Beijing: May 1980, p 149.
2. Macruz R, Martins JRM, Tupinamba A, Lopes EA, Vargas H, Penaaf DE, Carvalaho VB, Armelin E, De’Court LV: Therapeutic possibilities of laser beams in atheromas. Arq Bras Cardiol 34:9-12, 1980.
3. Abela G, Cohen D, Feldman RL, Geiser EA, Normann S, Conti CR: Use of laser radiation to recanalize stenosed arteries in a live animal model. Circulation 66(11):366, 1982.
4. Abela GS, Cohen D, Feldman RL, Normann S, Conti CR, Pepine CJ: Use of laser radiation to recanalize arteries in live rabbits. Clin Res 31(2):458A, 1983.
5 . Abela GS, Normann S, Feldman RL, Conti CR, Pepine CJ: A new model for evaluation of transluminal recanalization: human atherosclerotic coronary artery heterografts. Circulation 66(III):5, 1982.
6. Gessman LJ, Reno CW, Hastie R: Model for testing coronary angioplasty by laser catheter. J Am Coll Cardiol 1(2):690, 1983.
7. Choy DSJ, Stertzer SH, Quilici P, Wallsh E, Bruno MS, Loubeau JM, Kaminow I, Rotterdam H: Argon laser angioplasty in cadaver and animal models. J Am Coll Cardiol 1(2):690, 1983.
8. Ginsburg R, Kim DS, Guthaner D, Toth J, Mitchell RS: Salvage of an ischemic limb by laser angioplasty: Description of a new technique. Clin Cardiol 754-58, 1984.
9. Choy DSJ, Stertzer SH, Myler RK, Marco J, Fournial G: Human coronary laser recanalization. Clin Cardiol 7:377-381, 1984.
10. Choy DSJ, Stertzer SH, Case RB, Marco J, Fournial G, Silvernail PI, Myler RK: Update on laser recanalization. Lasers Surg Med 3(4):357, 1984.
11. Choy DSJ, Stertzer SH, Rotterdam HZ, Sharrock N, Kaminow IP: Laser coronary catheter angio- plasty. Am J Cardiol50: 1206-1209, 1982.
12. Gerrity RG, Loop FD, Golding LAR, Ehrhart LA, Argenyi ZB: Arterial response to laser operation for removal of atherosclerotic plaques. J Thorac Cardiovasc Surg 85:409-421, 1983.
13. Sanborn TA, Faxon DP, Haudenschild CC, Gottsman SB, Ryan TJ: Angiographic and histopatho- logic consequences of in vivo laser radiation of atherosclerotic lesions. Circulation AHA 56th Scientific Sessions (abstract #577), 1983.
14. Salazar AE: Induction of coronary thrombosis in the intact closed-chest dog. Circ Res 9: 1351-1356, 1961.
15. Case RB, Choy DSJ, Dwyer EM, Silvernail PJ: Absence of distal emboli during in vivo laser recanalization. Lasers Surg Med 5:281-289, 1985.
16. Geschwind H, Boussignac G, Teisseire B, Vieilledent C, Gaston, Becquemin JP, Mayiolini P: Percutaneous transluminal laser angioplasty in man. Lancet I:844, 1984.