Embed Size (px)
Citation preview
CiEKR
O
M
R
C
AoRrtiadth
C
CG
W
P
Outcomes
omprehensive Quality-of-life Outcomesn the Setting of a Multidisciplinary,qual Access Prostate Cancer Clinic
evin Rice, Jane Hudak, Kimberly Peay, Sally Elsamanoudi, Judith Travis,obbin Lockhart, Jennifer Cullen, Libby Black, Susan Houge, and Stephen Brassell
BJECTIVES To identify racial and demographic factors that influence treatment choice and its resultingimpact on health-related quality of life (HRQoL) for prostate cancer patients.
ETHODS Patients presenting to an equal access, military, multidisciplinary prostate cancer clinic com-posed the study group. The Expanded Prostate Cancer Index Composite (EPIC), EPIC Demo-graphic, and Medical Outcomes Study Short Form 36 were the instruments used. Evaluation wasperformed before treatment and every 3 months after treatment.
ESULTS The study group comprised 665 patients. Caucasians were 3-fold more likely to choosesurgery (radical prostatectomy [RP]) over external beam radiation therapy (EBRT). Patientswho earned more than $100 000 annually disproportionately chose RP (P �.0001). Simi-larly, those having a graduate school degree disproportionally chose RP (P �.0001). Patientsundergoing RP had the greatest risk of urinary function decline (P �.0001) and sexualbother (P � .0003). African Americans (AA) had a greater risk of urinary function declineirrespective of treatment choice. Patients undergoing EBRT had equivalent urinary functionto expectant management (EM) at 12 months (P �.0001). Brachytherapy was the onlytreatment that posed an increased risk of urinary bother decline when compared with EM (P �.0217). EBRT alone did not show significant decrement in sexual function when comparedwith EM.
ONCLUSIONS RP was chosen by patients of Caucasian ethnicity and patients with higher income andeducation level, despite providing the greatest risk of HRQoL decline. EBRT had no significantimpact on urinary function, sexual function, or sexual bother scores at 12 months. EBRT may beoffered to older patients with minimal HRQoL impact. Pretreatment counseling of HRQoLoutcomes is essential to overall prostate cancer management. UROLOGY 76: 1231–1239, 2010.
Published by Elsevier Inc.HcphpcoobTtcmtfuis
ssessing impact of treatment on patient satisfac-tion has long been a concern of physicians.Unfortunately, quantitative measures of these
utcomes often lag behind other clinical parameters.ecently, emphasis has been further focused on health-
elated quality of life (HRQoL) after prostate cancerreatment. A seminal meeting of the American Urolog-cal Association practice guidelines panel to determineppropriate endpoints for prostate cancer treatment mo-alities identified HRQoL as being of equal importanceo more traditional clinical outcome measures.1 Othersave echoed this conclusion, stating that the impact of
ompeting interest: Study partially funded by GlaxoSmithKline.From the Urology Service, Department of Surgery, Walter Reed Army Medical
enter, Washington, DC; Center for Prostate Disease Research, Washington, DC; andlaxoSmithKline; Research Triangle Park, North CarolinaReprint requests: Kevin R. Rice, M.D., 6900 Georgia Avenue, NW, Building 2,
rard 56, Washington, DC 20307. E-mail: [email protected]: December 2, 2009, accepted (with revisions): March 5, 2010
ublished by Elsevier Inc.
RQoL on clinical decision making is so critical that aancer trial is incomplete without it.2 As multidisci-linary clinics become the standard of care for compre-ensive counseling of patients newly diagnosed withrostate cancer, providers must incorporate HRQoL out-omes into their discussion of available managementptions. In this way, patients can be made cognizant notnly of the oncological results of each treatment modalityut also of their associated health-related side effects.hese discussions should be tailored to each individual,
aking into account age, race/ethnicity, education, in-ome, and other salient demographic factors to opti-ize communication and avoid unrealistic expecta-
ions. Our goal was to characterize HRQoL outcomesor a variety of treatment choices in patients who havendergone standardized multidisciplinary counselingn an equal access medical center. Furthermore, weought to characterize how demographic factors were
elated to treatment choice in this setting.0090-4295/10/$36.00 1231doi:10.1016/j.urology.2010.03.087

M
PPmnoHuccocrpneai
ltmpSbtqu
pwU1ttmresd7tg4ohpupEcCataft
SPcl
DHradiFm(tem
aseHl1omisfidW
ROgtawCFdlt(ayw6iE
RWtd(oitCsmd
1
ATERIAL AND METHODS
atients and Proceduresatients presenting to our institution, an equal access militaryedical center, for counseling and management of newly diag-osed prostate cancer between June 2003 and June 2008 wereffered enrollment into an institutional review board–approvedRQoL database study before treatment. Each patient then
nderwent evaluation in our multidisciplinary prostate cancerlinic. This clinic consists of several counseling blocks to in-lude an attending urological oncologist (60 minutes), radiationncologist (60 minutes), andrologist (60-minute group lecture),linical psychologist (30 minutes), nurse educator (30 minutes),esearch personnel (30 minutes), and a combined session of theatient, spouse, and above providers (15 minutes). Patients areot required or expected to make management decisions by thend of the multidisciplinary clinic visit. Follow-up clinic visitsnd phone consults are provided to all patients at 1-monthntervals until a treatment decision is reached.
The HRQoL database was established for the prospective col-ection of patient reported HRQoL outcomes at regular intervals torend these dynamic measures over time. The instruments used toeasure HRQoL were the Expanded Prostate Cancer Index Com-
osite (EPIC), EPIC Demographic, and Medical Outcomes Studyhort-Form 36 (SF-36). Patients received a baseline evaluationefore prostate biopsy and at 3, 6, 9, 12, 18, 24 and 36 monthshereafter. Chi-square testing was used to compare treatment fre-uencies by race, income, and education level. Student’s t test wassed to compare mean HRQoL outcomes.
For patients choosing surgery, radical prostatectomy (RP) waserformed using the technique described by Walsh.3 All RPsere performed by 1 of 2 urological oncologists with Society ofrologic Oncology (SUO) certification who perform at least
00 RPs annually. Nerve sparing was determined by preopera-ive parameters and intraoperative judgment. None of the pa-ients who underwent RP received neoadjuvant hormone treat-ent (NHT). Patients who received adjuvant or salvage
adiation were not included in this analysis. Patients choosingxternal beam radiation therapy (EBRT) received three-dimen-ional conformal intensity-modulated radiotherapy in 2.0-Gyaily fractions administered 5 days per week until a total dose of6 Gy was reached. Patients treated with neoadjuvant hormoneherapy before EBRT (EBRT � NHT) were given 10.8 mgoserelin acetate injection at 3-month intervals for a total of-28 months as determined by pretreatment clinical parametersf their disease state, with longer duration being reserved forigh-risk disease. For patients choosing brachytherapy, a trans-erineal approach using transrectal ultrasound guidance wassed to deliver a 160-Gy dose by iodine-125 implants. Noatients were subsequently treated with a further boost byBRT. Patients who chose hormone therapy alone (HT) re-eived 10.8 mg goserelin acetate injections every 3 months.ombined androgen blockade with 50 mg bicalutamide was
lso added for some patients at the providers’ discretion. Pa-ients in the expectant management (EM) group were defineds those patients who, after extensive counseling, chose toorego definitive or palliative treatment and received no furtherherapy during the study time frame.
tatistical Analysisatients enrolled in the study were asked to complete a surveyontaining questions regarding their race/ethnicity, highest
evel of education, marital status, and annual household income. s232
emographic information, disease characteristics, and results ofRQoL measures from the study sample were examined. With
egard to level of education, patients were divided into those withcollege degree or less versus patients with professional or graduateegrees. Annual household income was used to divide patientsnto those earning less than $100 000 versus those earning more.requencies were reported for categorical patient features, whereaseasures of central tendency (mean and median) and dispersion
standard deviation and range) were reported for continuous pa-ient features. Student’s t test and analysis of variance were used toxamine the association between HRQoL scores and patient de-ographic and disease features.Using multivariable regression, a series of models were ex-
mined for each of the function and bother outcomes (urinary,exual, bowel, and hormonal). Two additional models werexamined for 2 SF-36 outcomes, Mental Health and Physicalealth. For each model, HRQoL change over time was calcu-
ated by subtracting a subject’s baseline HRQoL score from his2-month follow-up HRQoL score, for each of the 10 HRQoLutcomes. The same list of covariates was included in eachodel, including age, race/ethnicity, education, marital status,
ncome, prostate-specific antigen (PSA) at diagnosis, clinical Ttage, and Gleason score. Estimates of risk, corresponding con-dence intervals, and P values are presented for these longitu-inal findings. All data analysis was conducted in SAS 9.1 forindows (SAS Institute, Cary, NC).
ESULTSf the 935 patients enrolled, 665 comprised the study
roup with at least 12-months of follow-up. Analyses forhe study group were performed at baseline and at 3, 6, 9,nd 12 months of follow-up. In all, 95% of the patientsho presented to the CPDR Multidisciplinary Prostateancer Clinic accepted enrollment into the HRQoL study.or the patients who elected not to enroll, no definitiveemographic or clinic trends could be identified. Table 1ists the demographic and clinical characteristics. The pa-ients are notable for 202 (30.5%) being African AmericanAA), 542 (82.3%) being married, and 328 (50.3%) havinggraduate or professional school degree. Median age was 62ears; mean PSA was 8.0. A total of 447 patients (67.4%)ere clinical T1c, and 455 (69.2%) had a Gleason score ofor less. RP was chosen by 55.5% of patients, EBRT alone
n 23.1%, EBRT � NHT in 8.1%, brachytherapy in 4.1%,M, in 6.5% and HT alone in 2.7%.
ace, Treatment Choice, and HRQoLhen comparing clinical characteristics between pa-
ients of AA and Caucasian race, there were no statisticalifferences in clinical stage, PSA, Gleason score, or ageTable 2). The EPIC Questionnaire collects informationf the number of medical comorbidities. A comorbidityndex was created to categorize patients based on whetherhey reported 0, 1, 2, or �3 comorbidities. AA andaucasians were compared across these four groups. Chi-
quare analysis revealed no significant differences in co-orbidities among AA and Caucasians. Table 2 gives a
etailed description of treatment groups by race. Cauca-
ians comprised 80.5% of the EM group, with AA makingUROLOGY 76 (5), 2010

uC.cpmP
bCscRtac
DWtwlEedmw
mAutffg.f(pu
o.asEftF(tp
bissatst
CPaadilc“lt
U
p the remaining 19.5%. When adjusted for population,aucasians still chose EM twice as frequently as AA (P �
0033). Caucasians were also 3 times more likely tohoose RP over EBRT (59.1% vs 19.1%). AA dispro-ortionately chose EBRT alone over all other treat-ents compared with Caucasians (31.7% vs 19.1%,� .003).At baseline, AA had worse urinary function, bowel
other, hormonal bother, and physical function scores thanaucasians. At 12 months, AA who underwent EBRT had
ignificantly lower mean urinary function scores than Cau-asians undergoing EBRT (P �.05), whereas AA choosingP had significantly lower mean physical function scores
han Caucasians undergoing RP (P �.05). In multivariablenalysis, AA had the greatest risk of urinary function de-
Table 1. Demographic and clinical characteristics ofstudy sample
Characteristic N (%)
Race/ethnicityAfrican American 202 (30.5)Caucasian 431 (65.1)Hispanic 14 (2.1)Asian 7 (1.1)Other 11 (1.6)
Marital statusMarried 542 (82.3)Divorced/separated 73 (11.1)Widowed 23 (3.5)Never married 21 (3.2)
Employment statusFull-time 377 (57.3)Retired 226 (34.4)Part-time/searching 72 (10.8)
Income ($)0-30,000 33 (5.1)30,001-100,000 301 (46.8)�100 000 309 (50.3)
EducationHigh school/technical school 75 (11.5)College 249 (38.2)Graduate/professional school 328 (50.3)
SmokingNo 610 (92.6)Yes 49 (7.4)
Clinical stageT1 447 (67.4)T2 202 (30.5)T3 14 (2.1)
Gleason scoreWell differentiated (Gleason 2-6) 455 (69.2)Moderately differentiated (Gleason 7) 142 (21.6)Poorly differentiated (Gleason 8-10) 61 (9.3)
Mean (�SD)PSA 8.0 (� 16.7)Age
Surgery 58.0 (� 8.0)EBRT 67.0 (� 8.9)EBRT � NHT 69.8 (� 8.5)Brachytherapy 62.9 (� 8.2)EM 69.3 (� 9.9)HT 74.0 (� 9.4)
line regardless of treatment choice (P � .0083). l
ROLOGY 76 (5), 2010
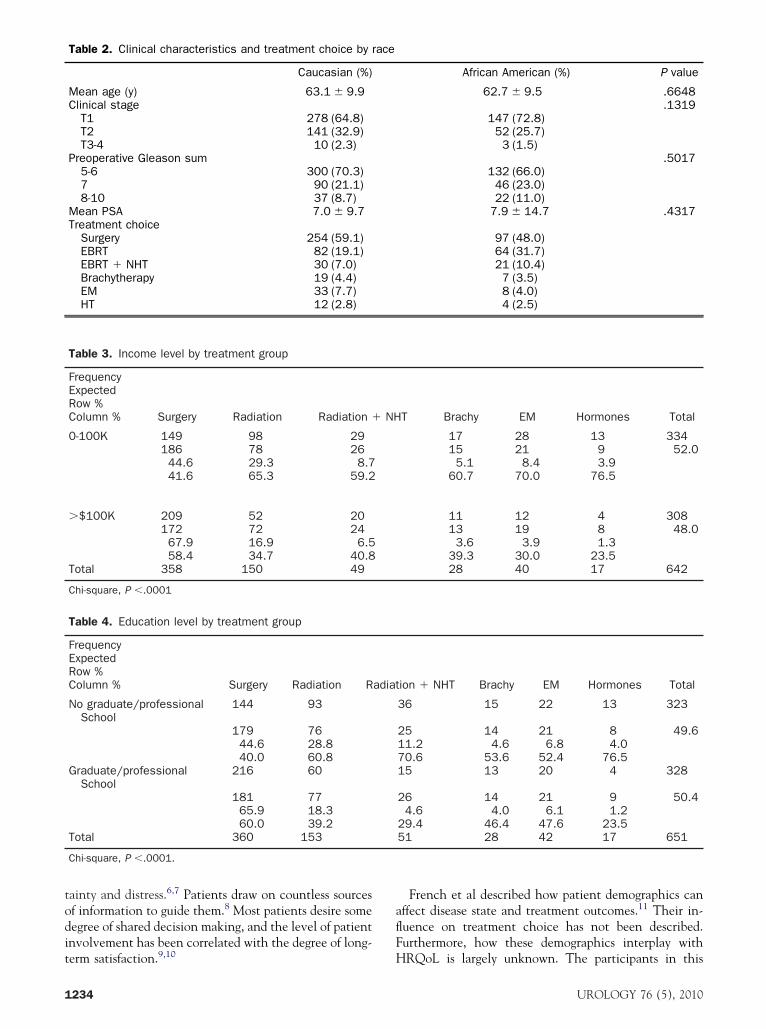
emographics, Treatment Choice, and HRQoLhen comparing income, patients who earned more
han $100,000 annually disproportionately chose RP,hereas those earning less than $100,000 were more
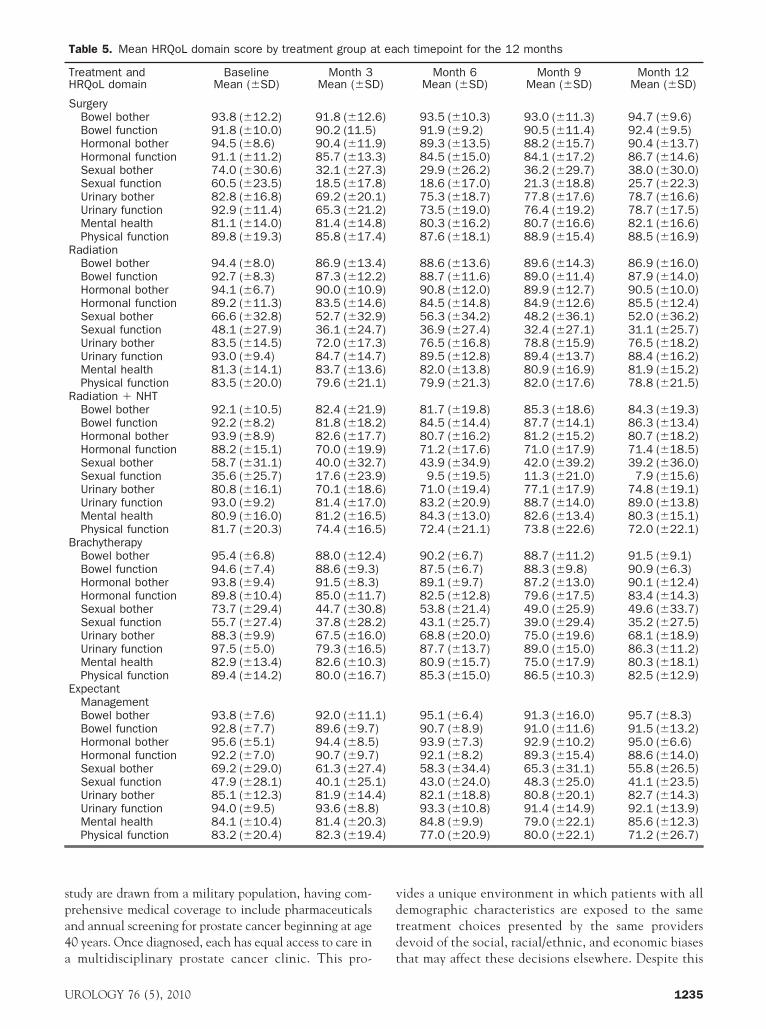
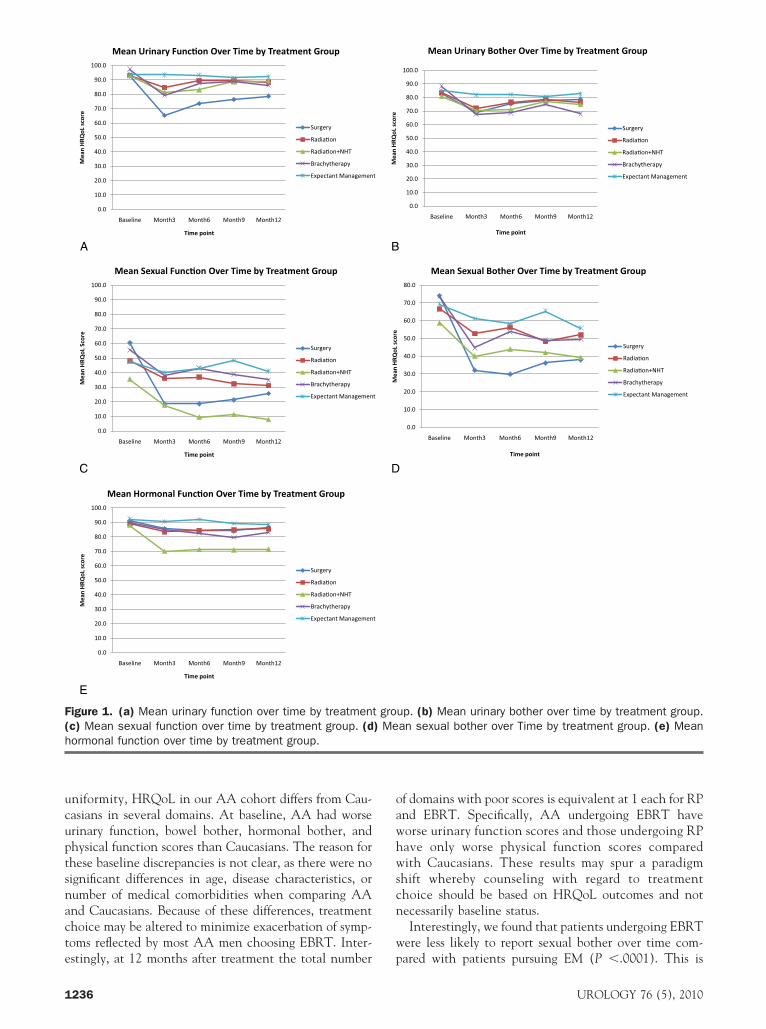
ikely to choose one of the other treatment modalities orM (P �.0001); (Table 3). A similar trend was noted forducation, with patients having a graduate school degreeisproportionally choosing RP, whereas the other treat-ent options were disproportionally represented in thoseith college education or less (P �.0001; Table 4).Table 5 demonstrates the HRQoL domains for all treat-ent modalities at baseline and through 1-year follow-up.s shown in Figure 1a, the strongest predictor of change in
rinary function over time was treatment choice, with pa-ients undergoing RP having the highest risk of urinaryunction decline (P �.0001). Age also affected urinaryunction to a lesser extent, with older age groups having areater risk of decline regardless of treatment choice (P �0308). Patients undergoing EBRT had equivalent urinaryunction to EM at 12 months but worse bowel botherP �.0001). Brachytherapy was the only treatment thatosed an increased risk of urinary bother decline with EMsed as the referent group (P � .0217; Fig. 1b).
The strongest predictors of change in sexual functionver time were treatment (P �.0001) and PSA (P �0178). To this end, patients undergoing RP, brachyther-py, and EBRT � NHT showed statistically significantexual function decline using EM as the referent group.BRT alone did not show significant decrement in sexual
unction compared with EM (Fig. 1c). RP was the onlyreatment to predict change in sexual bother (P � .0003,ig. 1d). Gleason sum (P � .0016) and EBRT � NHTP � .0032) were the only predictors of hormonal func-ion decline (Fig. 1e). Hormonal bother over time wasredicted only by Gleason sum (P �.0001).Using multivariable analysis to evaluate the relationship
etween smoking status, marital status, education level,ncome, and employment and HRQoL outcomes, only 2tatistically significant associations were found. Currentmokers reported less decline in bowel function (P � .0122)nd bowel bother (P � .0124) over time regardless ofreatment choice. Patients who completed graduate/profes-ional school were noted to have greater sexual bother overime (P � .0064) regardless of treatment choice.
OMMENTatients faced with the initial diagnosis of prostate cancerre challenged not only with an emotional burden thatny cancer diagnosis imparts, but also with the difficultecision-making process where definitive data are lack-ng. To date, no well-designed clinical trial has estab-ished the superiority of one definitive therapy for clini-ally localized prostate cancer.4,5 In the absence of astandard” therapy, patients will continue to face thisife-altering decision with suboptimal information. Givenhe potential impact on long-term health and quality of
ife, this decision can be a source of tremendous uncer-1233
todit
aflF
1
ainty and distress.6,7 Patients draw on countless sourcesf information to guide them.8 Most patients desire someegree of shared decision making, and the level of patientnvolvement has been correlated with the degree of long-
Table 2. Clinical characteristics and treatment choice by r
Caucasian (%)
Mean age (y) 63.1 � 9.9Clinical stage
T1 278 (64.8)T2 141 (32.9)T3-4 10 (2.3)
Preoperative Gleason sum5-6 300 (70.3)7 90 (21.1)8-10 37 (8.7)
Mean PSA 7.0 � 9.7Treatment choice
Surgery 254 (59.1)EBRT 82 (19.1)EBRT � NHT 30 (7.0)Brachytherapy 19 (4.4)EM 33 (7.7)HT 12 (2.8)
Table 3. Income level by treatment group
FrequencyExpectedRow %Column % Surgery Radiation Radiation �
0-100K 149 98 29186 78 2644.6 29.3 8.741.6 65.3 59.2
�$100K 209 52 20172 72 2467.9 16.9 6.558.4 34.7 40.8
Total 358 150 49
Chi-square, P �.0001
Table 4. Education level by treatment group
FrequencyExpectedRow %Column % Surgery Radiation R
No graduate/professionalSchool
144 93
179 7644.6 28.840.0 60.8
Graduate/professionalSchool
216 60
181 7765.9 18.360.0 39.2
Total 360 153
Chi-square, P �.0001.
erm satisfaction.9,10 H
234
French et al described how patient demographics canffect disease state and treatment outcomes.11 Their in-uence on treatment choice has not been described.urthermore, how these demographics interplay with
African American (%) P value
62.7 � 9.5 .6648.1319
147 (72.8)52 (25.7)3 (1.5)
.5017132 (66.0)46 (23.0)22 (11.0)
7.9 � 14.7 .4317
97 (48.0)64 (31.7)21 (10.4)7 (3.5)8 (4.0)4 (2.5)
T Brachy EM Hormones Total
17 28 13 33415 21 9 52.05.1 8.4 3.9
60.7 70.0 76.5
11 12 4 30813 19 8 48.03.6 3.9 1.3
39.3 30.0 23.528 40 17 642
ion � NHT Brachy EM Hormones Total
36 15 22 13 323
25 14 21 8 49.611.2 4.6 6.8 4.070.6 53.6 52.4 76.515 13 20 4 328
26 14 21 9 50.44.6 4.0 6.1 1.2
29.4 46.4 47.6 23.551 28 42 17 651
ace
NH
adiat
RQoL is largely unknown. The participants in this
UROLOGY 76 (5), 2010
spa4a
vdtd
U
tudy are drawn from a military population, having com-rehensive medical coverage to include pharmaceuticalsnd annual screening for prostate cancer beginning at age0 years. Once diagnosed, each has equal access to care in
Table 5. Mean HRQoL domain score by treatment group a
Treatment andHRQoL domain
BaselineMean (�SD)
Month 3Mean (�SD
SurgeryBowel bother 93.8 (�12.2) 91.8 (�12.Bowel function 91.8 (�10.0) 90.2 (11.5)Hormonal bother 94.5 (�8.6) 90.4 (�11.Hormonal function 91.1 (�11.2) 85.7 (�13.Sexual bother 74.0 (�30.6) 32.1 (�27.Sexual function 60.5 (�23.5) 18.5 (�17.Urinary bother 82.8 (�16.8) 69.2 (�20.Urinary function 92.9 (�11.4) 65.3 (�21.Mental health 81.1 (�14.0) 81.4 (�14.Physical function 89.8 (�19.3) 85.8 (�17.
RadiationBowel bother 94.4 (�8.0) 86.9 (�13.Bowel function 92.7 (�8.3) 87.3 (�12.Hormonal bother 94.1 (�6.7) 90.0 (�10.Hormonal function 89.2 (�11.3) 83.5 (�14.Sexual bother 66.6 (�32.8) 52.7 (�32.Sexual function 48.1 (�27.9) 36.1 (�24.Urinary bother 83.5 (�14.5) 72.0 (�17.Urinary function 93.0 (�9.4) 84.7 (�14.Mental health 81.3 (�14.1) 83.7 (�13.Physical function 83.5 (�20.0) 79.6 (�21.
Radiation � NHTBowel bother 92.1 (�10.5) 82.4 (�21.Bowel function 92.2 (�8.2) 81.8 (�18.Hormonal bother 93.9 (�8.9) 82.6 (�17.Hormonal function 88.2 (�15.1) 70.0 (�19.Sexual bother 58.7 (�31.1) 40.0 (�32.Sexual function 35.6 (�25.7) 17.6 (�23.Urinary bother 80.8 (�16.1) 70.1 (�18.Urinary function 93.0 (�9.2) 81.4 (�17.Mental health 80.9 (�16.0) 81.2 (�16.Physical function 81.7 (�20.3) 74.4 (�16.
BrachytherapyBowel bother 95.4 (�6.8) 88.0 (�12.Bowel function 94.6 (�7.4) 88.6 (�9.3Hormonal bother 93.8 (�9.4) 91.5 (�8.3Hormonal function 89.8 (�10.4) 85.0 (�11.Sexual bother 73.7 (�29.4) 44.7 (�30.Sexual function 55.7 (�27.4) 37.8 (�28.Urinary bother 88.3 (�9.9) 67.5 (�16.Urinary function 97.5 (�5.0) 79.3 (�16.Mental health 82.9 (�13.4) 82.6 (�10.Physical function 89.4 (�14.2) 80.0 (�16.
ExpectantManagementBowel bother 93.8 (�7.6) 92.0 (�11.Bowel function 92.8 (�7.7) 89.6 (�9.7Hormonal bother 95.6 (�5.1) 94.4 (�8.5Hormonal function 92.2 (�7.0) 90.7 (�9.7Sexual bother 69.2 (�29.0) 61.3 (�27.Sexual function 47.9 (�28.1) 40.1 (�25.Urinary bother 85.1 (�12.3) 81.9 (�14.Urinary function 94.0 (�9.5) 93.6 (�8.8Mental health 84.1 (�10.4) 81.4 (�20.Physical function 83.2 (�20.4) 82.3 (�19.
multidisciplinary prostate cancer clinic. This pro- t
ROLOGY 76 (5), 2010
ides a unique environment in which patients with allemographic characteristics are exposed to the samereatment choices presented by the same providersevoid of the social, racial/ethnic, and economic biases
ch timepoint for the 12 months
Month 6Mean (�SD)
Month 9Mean (�SD)
Month 12Mean (�SD)
93.5 (�10.3) 93.0 (�11.3) 94.7 (�9.6)91.9 (�9.2) 90.5 (�11.4) 92.4 (�9.5)89.3 (�13.5) 88.2 (�15.7) 90.4 (�13.7)84.5 (�15.0) 84.1 (�17.2) 86.7 (�14.6)29.9 (�26.2) 36.2 (�29.7) 38.0 (�30.0)18.6 (�17.0) 21.3 (�18.8) 25.7 (�22.3)75.3 (�18.7) 77.8 (�17.6) 78.7 (�16.6)73.5 (�19.0) 76.4 (�19.2) 78.7 (�17.5)80.3 (�16.2) 80.7 (�16.6) 82.1 (�16.6)87.6 (�18.1) 88.9 (�15.4) 88.5 (�16.9)
88.6 (�13.6) 89.6 (�14.3) 86.9 (�16.0)88.7 (�11.6) 89.0 (�11.4) 87.9 (�14.0)90.8 (�12.0) 89.9 (�12.7) 90.5 (�10.0)84.5 (�14.8) 84.9 (�12.6) 85.5 (�12.4)56.3 (�34.2) 48.2 (�36.1) 52.0 (�36.2)36.9 (�27.4) 32.4 (�27.1) 31.1 (�25.7)76.5 (�16.8) 78.8 (�15.9) 76.5 (�18.2)89.5 (�12.8) 89.4 (�13.7) 88.4 (�16.2)82.0 (�13.8) 80.9 (�16.9) 81.9 (�15.2)79.9 (�21.3) 82.0 (�17.6) 78.8 (�21.5)
81.7 (�19.8) 85.3 (�18.6) 84.3 (�19.3)84.5 (�14.4) 87.7 (�14.1) 86.3 (�13.4)80.7 (�16.2) 81.2 (�15.2) 80.7 (�18.2)71.2 (�17.6) 71.0 (�17.9) 71.4 (�18.5)43.9 (�34.9) 42.0 (�39.2) 39.2 (�36.0)9.5 (�19.5) 11.3 (�21.0) 7.9 (�15.6)
71.0 (�19.4) 77.1 (�17.9) 74.8 (�19.1)83.2 (�20.9) 88.7 (�14.0) 89.0 (�13.8)84.3 (�13.0) 82.6 (�13.4) 80.3 (�15.1)72.4 (�21.1) 73.8 (�22.6) 72.0 (�22.1)
90.2 (�6.7) 88.7 (�11.2) 91.5 (�9.1)87.5 (�6.7) 88.3 (�9.8) 90.9 (�6.3)89.1 (�9.7) 87.2 (�13.0) 90.1 (�12.4)82.5 (�12.8) 79.6 (�17.5) 83.4 (�14.3)53.8 (�21.4) 49.0 (�25.9) 49.6 (�33.7)43.1 (�25.7) 39.0 (�29.4) 35.2 (�27.5)68.8 (�20.0) 75.0 (�19.6) 68.1 (�18.9)87.7 (�13.7) 89.0 (�15.0) 86.3 (�11.2)80.9 (�15.7) 75.0 (�17.9) 80.3 (�18.1)85.3 (�15.0) 86.5 (�10.3) 82.5 (�12.9)
95.1 (�6.4) 91.3 (�16.0) 95.7 (�8.3)90.7 (�8.9) 91.0 (�11.6) 91.5 (�13.2)93.9 (�7.3) 92.9 (�10.2) 95.0 (�6.6)92.1 (�8.2) 89.3 (�15.4) 88.6 (�14.0)58.3 (�34.4) 65.3 (�31.1) 55.8 (�26.5)43.0 (�24.0) 48.3 (�25.0) 41.1 (�23.5)82.1 (�18.8) 80.8 (�20.1) 82.7 (�14.3)93.3 (�10.8) 91.4 (�14.9) 92.1 (�13.9)84.8 (�9.9) 79.0 (�22.1) 85.6 (�12.3)77.0 (�20.9) 80.0 (�22.1) 71.2 (�26.7)
t ea
)
6)
9)3)3)8)1)2)8)4)
4)2)9)6)9)7)3)7)6)1)
9)2)7)9)7)9)6)0)5)5)
4)))7)8)2)0)5)3)7)
1))))4)1)4))3)4)
hat may affect these decisions elsewhere. Despite this
1235
ucuptsnacte
oawhwscn
w
F(h
1
niformity, HRQoL in our AA cohort differs from Cau-asians in several domains. At baseline, AA had worserinary function, bowel bother, hormonal bother, andhysical function scores than Caucasians. The reason forhese baseline discrepancies is not clear, as there were noignificant differences in age, disease characteristics, orumber of medical comorbidities when comparing AAnd Caucasians. Because of these differences, treatmenthoice may be altered to minimize exacerbation of symp-oms reflected by most AA men choosing EBRT. Inter-
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Baseline Month3 Month6 Month9 Month12
Mea
n H
RQoL
sco
re
Time point
Mean Urinary Func�on Over Time by Treatment Group
Surgery
Radia�on
Radia�on+NHT
Brachytherapy
Expectant Managemen
A
C
E
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Baseline Month3 Month6 Month9 Month12
Mea
n H
RQoL
Sco
re
Time point
Mean Sexual Func�on Over Time by Treatment Group
Surgery
Radia�on
Radia�on+NHT
Brachytherapy
Expectant Managemen
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Baseline Month3 Month6 Month9 Month12
Mea
n H
RQoL
sco
re
Time point
Mean Hormonal Func�on Over Time by Treatment Group
Surgery
Radia�on
Radia�on+NHT
Brachytherapy
Expectant Managemen
igure 1. (a) Mean urinary function over time by treatmenc) Mean sexual function over time by treatment group. (dormonal function over time by treatment group.
stingly, at 12 months after treatment the total number p
236
f domains with poor scores is equivalent at 1 each for RPnd EBRT. Specifically, AA undergoing EBRT haveorse urinary function scores and those undergoing RPave only worse physical function scores comparedith Caucasians. These results may spur a paradigm
hift whereby counseling with regard to treatmenthoice should be based on HRQoL outcomes and notecessarily baseline status.Interestingly, we found that patients undergoing EBRT
ere less likely to report sexual bother over time com-
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Baseline Month3 Month6 Month9 Month12
Time point
Mean Urinary Bother Over Time by Treatment Group
Surgery
Radia�on
Radia�on+NHT
Brachytherapy
Expectant Management
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
Baseline Month3 Month6 Month9 Month12
Mea
n H
RQoL
sco
re
Time point
Mean Sexual Bother Over Time by Treatment Group
Surgery
Radia�on
Radia�on+NHT
Brachytherapy
Expectant Management
up. (b) Mean urinary bother over time by treatment group.an sexual bother over Time by treatment group. (e) Mean
t
Mea
n H
RQoL
sco
re
B
D
t
t
t gro) Me
ared with patients pursuing EM (P �.0001). This is
UROLOGY 76 (5), 2010

mwpfowmfaadsa
scHtfpsdwacttbghbbd
HradoeTapEcww
wdamdcbgt
mlnv
daHUodHti
pTtwpm
CHmpcwt
R
1
U
ost likely due to immaturity of the data in this area asell as to the extensive pretreatment counseling that ouratients undergo, setting expectations for post-treatmentunctional status. This phenomenon has been previ-usly characterized in a generalized cancer populationhere emphasis on patient’s perception of post-treat-ent HRQoL affects future domain scores despite worse
unctional outcomes.12,13 Initial investigation into thepplicability of this model to prostate cancer has beenttempted, but further study is warranted to limit theisparity between anticipated outcomes and actual re-ults.14 In addition, age and likelihood of accepting ther-py from patients’ providers could be factors as well.
Patients who chose RP tended to be younger, Cauca-ian, and of higher income and educational level. Thisohort chose the option with the greatest impact onRQoL, which provides evidence that patients with
hese demographic characteristics may emphasize otheractors in their treatment decisions, such as avoidance ofrolonged daily treatments, definitive pathologic analy-is, and the peace of mind associated with the rapidecline in PSA associated with extirpative therapy. Weould expect continued improvement in sexual functionnd bother as well as urinary function and bother withontinued follow-up in this group. Therefore, some ofhese declines may be reversible. It is tempting to assumehat the younger patients who chose surgery had higheraseline scores and thus were more likely to exhibitreater declines with intervention. This appears toave played only a role only in the sexual function andother domains, but not the urinary function andother domains, where a baseline difference was notemonstrated.Older patients tended to choose EBRT, EBRT withT, HT, or EM. These patients are more likely to choose
adiation therapy for several reasons. First, radiation ther-py is noninvasive and carries fewer medical risks thanoes surgery under general or epidural anesthesia. Sec-nd, most of these patients are retired and are moreasily able to commit to 7 weeks of daily treatments.hird, the patients are counseled that erectile functionnd continence outcomes tend to be worse in olderatients.15 Older patients are more likely to chooseM, as their shorter life expectancy decreases thehances that their disease will progress to the point athich intervention would be required or symptomsould develop.This study group contained a large number of patients
ith high incomes as well as patients with professionalegreases. Approximately 50% of patients reported annnual household income of � $100 000, and approxi-ately 50% of patients reported graduate or professional
egrees. With a 95% study enrollment rate, these findingsannot be explained by a study selection bias. This maye partially explained by the high cost of living in thereater Washington, DC metropolitan area. In addi-
ion, the vast majority of these patients are retiredROLOGY 76 (5), 2010
ilitary beneficiaries, meaning that they have had ateast 20 years of active duty military service and areow collecting a military pension in addition to theirocational income.Finally, recent attention has been focused on the
etriments of prostate cancer screening in older mennd how treatment has a significant adverse impact onRQoL. In keeping with practice patterns in thenited States, most men in this age group would be
ffered EBRT if they desired active treatment. Ourata indicate that EBRT and EM differ in only 1RQoL domain— bowel bother. Therefore, we believe
hat EBRT can be offered to older patients with min-mal HRQoL impact.
Recent large-scale studies have called widespreadrostate cancer screening and treatment into question.herefore, it is imperative that we examine the effect
hat definitive treatments have on HRQoL comparedith nonintervention. To our knowledge, this is the firstrostate cancer HRQoL study to compare various treat-ent modalities with EM.
ONCLUSIONSRQoL is an important component of prostate canceranagement. By using HRQoL outcomes combined with
atient demographics, more comprehensive counselingan be administered in a multidisciplinary setting. In thisay, future treatment recommendations can be tailored
o best match a patient’s HRQoL expectations.
eferences1. Schellhammer P, Cockett A, Boccon-Gibod L, et al. Assessment of
endpoints for clinical trials for localized prostate cancer. Urology.1997;49:27-38.
2. Altwein J, Ekman P, Barry M, et al. How is quality of life in prostatecancer patients influenced by modern treatment? The WallenbergSymposium. Urology. 1997;49:66-76.
3. Walsh PC. Anatomic radical retropubic prostatectomy. In: RetikAB, Vaughan ED, Wein AJ, eds. Campbell’s Urology, Vol. 4 Phil-adelphia, PA: W. B. Saunders; 2002:3107-3128.
4. Middleton RG, Thompson IM, Austenfeld MS, et al. ProstateCancer Clinical Guidelines Panel summary report on the manage-ment of clinically localized prostate cancer. The American Uro-logical Association. J Urol. 1995;154:2144-2148.
5. Thompson I, Thrasher JB, Aus G, et al. Guideline for the man-agement of clinically localized prostate cancer: 2007 update. J Urol.2007;177:2106-2131.
6. Burke MA, Lowrance W, Perczek R. Emotional and cognitiveburden of prostate cancer. Urol Clin North Am. 2003;30:295-304.
7. Steginga SK, Occhipinti S, Gardiner RA, et al. Prospective study ofmen’s psychological and decision-related adjustment after treat-ment for localized prostate cancer. Urology. 2004;63:751-756.
8. Brawley OW. Nonmedical factors in treatment selection. Urol ClinNorth Am. 2003;30:331-335.
9. Benbassat J, Pilpel D, Tidhar M. Patients’ preferences for partici-pation in clinical decision making: a review of published surveys.Behav Med. 1998;24:81-88.
0. Davison BJ, Degner LF, Morgan TR. Information and decision-making preferences of men with prostate cancer. Oncol Nurs Fo-
rum. 1995;22:1401-1408.1237

1
1
1
1
1
ETqloia
mcAscs
a9aHcec
ohtctibsilwp
lpisbi
cdm
stmtsadoc
BUW
R1
2
3
dU
RWtbbbecwhftrntrtttrd1hbs
Hfmtff
1
1. French DB, Jones LA. Minority issues in prostate disease. Med ClinNorth Am. 2005;89:805-816.
2. Wan GJ, Counte MA, Cella DF. The influence of personal expec-tations on cancer patients’ reports of health-related quality of life.Psychooncology. 1997;6:1-11.
3. Carr AJ, Gibson B, Robinson PG. Measuring quality of life: isquality of life determined by expectations or experience? BMJ.2001;322:1240-1243.
4. Symon Z, Daignault S, Symon R, et al. Measuring patients’ ex-pectations regarding health-related quality-of-life outcomes as-sociated with prostate cancer surgery or radiotherapy. Urology.2006;68:1224-1229.
5. Stanford JL, Feng Z, Hamilton AS, et al. Urinary and sexualfunction after radical prostatectomy for clinically localized pros-tate cancer: the Prostate Cancer Outcomes Study. JAMA.2000;283:354-360.
DITORIAL COMMENThis study represents a prospective analysis on health-relateduality of life (HRQOL) outcomes after various treatments forocalized prostate cancer. It is a strong effort to measure theseutcomes; but, similar to most all publications in this domain,t fails to adhere to the necessary study design requirements forccurate outcomes analysis.
aValidated HRQOL surveys should be initiated before treat-ent, as done in this study. However, the surveys should be
ompleted anonymously, which was not done in this study.nonymity entails completion at home, without nursing or
tudy coordinator phone assistance; mailing to a third party dataenter; and no treating institution or patient name on theurvey.1
aThe attrition rate in this study was very high, at least 30%,nd likely much higher. Based on entry dates, almost all of the35 men should have reached the 2-year follow-up, yet theuthors use the 1-year survey endpoint, with only 665 men. InRQOL studies, there exists a strong bias toward adverse out-
omes in the nonresponders. Response rates of less than 90%,ven in large studies, will usually result in falsely better out-omes.
aSexual health domain analysis should always be predicatedn pretreatment scores. Men with high pretreatment sexualealth scores are much more likely to diminish their scores withreatment than men with low pretreatment scores. Comparinghanges in overall mean treatment scores in the total popula-ion, as was done in this study, can mask the true negativempact of treatment on sexual health in men functioning wellefore treatment. Ideally, the endpoint that should be used forexual health analysis in men functioning well before treatments an actual return to baseline (not “percentage return to base-ine”).1,2 This does tend to result in less than ideal outcomesith all treatments, which is likely why it is never used inublished HRQOL studies to date.In the Urinary and Bowel domains, the major flaw in pub-
ished studies is in defining success. The only appropriate end-oint, with all treatments, is again return to actual baseline, andn the urinary domain additionally being pad-free. It has beenhown that even men wearing 1 liner per day rarely return toaseline in urinary function, and should not be considered asndicating “success.”1
Based on optimal study design, we (urologists, radiation on-ologists, and medical oncologists) have failed in accuratelyefining HRQOL outcomes in our patients undergoing treat-
ents for localized prostate cancer. With the recent evidence s238
trongly supporting the fact that outcomes vary not only byreatment but also by the actual physician provider, we musteet this challenge.3 Future HRQOL studies for localized pros-
ate cancer should be published only if performed using optimaltudy design and with clear and accurate data analysis, usingppropriate endpoints. It is only with this close adherence toesign and analysis that we can accurately counsel our patientsn expectations when undergoing treatment for localized car-inoma of the prostate.
ruce L. Dalkin, M.D., F.A.C.S., Department of Urology,niversity of Washington School of Medicine, Seattle,ashington
eferences. Dalkin BL, Christopher B, Shawler D. Health related quality of life
outcomes after radical prostatectomy: accuracy through study design.Urol Oncol Semin Orig Investig. 2006;24:1:24-32.
. Dalkin BL, Christopher B. Potent men undergoing radical prosta-tectomy: a prospective study of changes in sexual health outcomesand the impact of erectile dysfunction treatments. Urol Oncol SeminOrig Investig. 2008;26:281-285.
. Bianco F, Vickers A, Cronin A, et al. Variations among experiencedsurgeons in cancer control after open radical prostatectomy. J Urol.2010;183:977-983.
oi:10.1016/j.urology.2010.03.088ROLOGY 76: 1238, 2010. © 2010 Elsevier Inc.
EPLYe appreciate the thoughtful interpretation and critique of
his study. We attempted to establish true unbiased HRQoLaseline scores by administering questionnaires not onlyefore treatment (as the editorial comments suggest) butefore biopsy. This was done in an effort to minimize theffect that a cancer diagnosis might have on patients’ per-eptions of their HRQoL. Follow-up HRQoL questionnairesere mailed to patients to be completed anonymously atome and mailed back to research coordinators at the Center
or Prostate Disease Research. The completed forms werehen faxed to a third-party data collection center, whereesults were entered into the HRQoL database. If question-aires were not received in 30 days, data managers contactedhe patients by phone and asked them to complete andeturn their questionnaires. Using this system, we were ableo keep the attrition rate relatively low at 12% rather thanhe 30% suggested by the preceding editorial comments. Theime that transpired during data analysis, manuscript prepa-ation, submission, and peer review accounts for the seemingiscrepancy in the relative number of patients with at least2 months of follow-up. We agree that patient attrition canave a biased effect on statistical analysis of outcomes. Weelieve that our 88% compliance rate is acceptable for atudy of this size.
With regard to sexual function outcomes, we used validatedRQoL instruments before diagnosis and at regular points of
ollow-up. We then compared mean scores for the differentanagement strategies. The editorial comments indicate that
his strategy does not account for the effect that pretreatmentunction may have on patients’ perceptions of changes resultingrom intervention. The relatively high standards of deviation
upport the assertion that mean values alone do not account forUROLOGY 76 (5), 2010





























