Embed Size (px)
Citation preview

10/15/2016
1
Severe Sepsis and Septic Shock:Diagnosis and Management
Review and Update 2016
Emanuel Rivers , MD MPH
The Sunshine Act of Medical Transparency
No Disclosures
Saving patients from sepsis is a race against timeCDC calls sepsis a medical emergency;
encourages prompt action for prevention, earlyrecognition
Tuesday, August 23, 2016, 1:00 p.m. ET

10/15/2016
2
(Crit Care Med 2016; 44:1353–1360)
The Financial Impact

10/15/2016
3
33.164 Billionor
8.7% of aggregatehospital costs
What is Sepsis?:The Early Pathogenesis
Global TissueHypoxia and
OrganDysfunction
Organism
Multiple OrganDysfunction and
Refractory Hypotension
Diffuse endothelialdisruption and
microcirculation defects
Systemic Inflammationor Inflammatory
Response
Septic Shock
Sepsis: A Complex and Dynamic Landscape
Severe Sepsis
EmergencyDepartment
Intensive CareUnit
Out PatientSetting
At Home orResidence
SepsisSource
Systemic Inflammatory Response Syndrome (SIRS)A clinical response arising from a nonspecific insult,including ≥2 of the following:
• Temperature ≥38oC or ≤36oC
• HR ≥90 beats/min
• Respirations ≥20/min
• WBC count ≥12,000/mm3 or≤4,000/mm3 or >10% bands
• PaCO2 < 32mmHg
General PracticeFloors
ORand Recovery

10/15/2016
4
The Morbidity Impact
Morbidity orDisabilities
PsychiatricDisease
Chronic HeartFailure
Disabilities(Amputations)
Chronic LungDisease (ARDS)
Kidney Failureand Dialysis
NeuromuscularDisorders
The Realities of CurrentSepsis Management:
Need for Improving ASystem of Care and Disease

10/15/2016
5
Sepsis Care - 2016A Systems Approach To Poor Sepsis Care
Early Recognition (SIRS)+
Risk Stratification(Lactate)
Recognition ofpoor sepsis carein the US ED’s
HemodynamicOptimization
AndImmuomodulation
Cultures,Antibiotics andSource Control
Recognition ofGlobal TissueHypoxia and
Cryptic Shock
ContinuousQuality
Improvement
1955 2001
A Need to Change theParadigm of
Current Sepsis Management

10/15/2016
6
Cases/year Mortality (%)
Stroke 591,996 6-7
AMI 540,891 10
Trauma 697,025 5-16
Sepsis 859,858 15-20
Severe Sepsis 791,000 27-40
Septic Shock 200,000 36-47
Pneumonia 1,187,180 5-9
What AboutGuidelines for Sepsis?

10/15/2016
7
2004, 2008, 2012
• Maintains international data base representing over 40,000
patients to date.
• Consultant to CMS and NQF
• Continued refinement of sepsis best practice.
80-110to 150
Golden Hours
Silver Day
Bundles
NEJM, 2014
NEJM, 2014
NEJM, 2015

10/15/2016
8
Early GoalDirectedTherapy
UsualCare
Treatment EffectSIRS
LactateFluid Challenge
AntibioticsEarly ICU admission
Unblinded CareSteroids
Protective lung strategiesGlucose Control
Pre-existing Sepsis ProtocolsDiminishing Mortality
2001
2016
Mortality > 46.5%
Mortality <20%
NEJM, 2014
NEJM, 2014
NEJM, 2015
2001-
October 1, 2015
Joint Commission CMSAHRQ

10/15/2016
9
1. Measure lactate
2. Blood cultures/appropriate cultures
3. Give broad spectrum antibiotics
4. Fluid Challenge of 30 cc/ kg if (hypotension/lactate > 4mM/L)
3H
ou
rB
un
dle
6H
our
Bu
nd
le
5. If persistent hypotension– vasopressor to maintain MAP > 65 mmHg
6. Document perfusion:
7. Re-measure lactate within 6 hours
InvasiveCVP
ScvO2
UltrasoundIVCTEETTE
Dynamic Assessment ofVolume Responsivenessto Fluid Challenge or PLR
SVVSLR
Bioimpedence
Physical ExamPeripheral Pulses
Capillary Refill (<2 secs)Skin Turgor
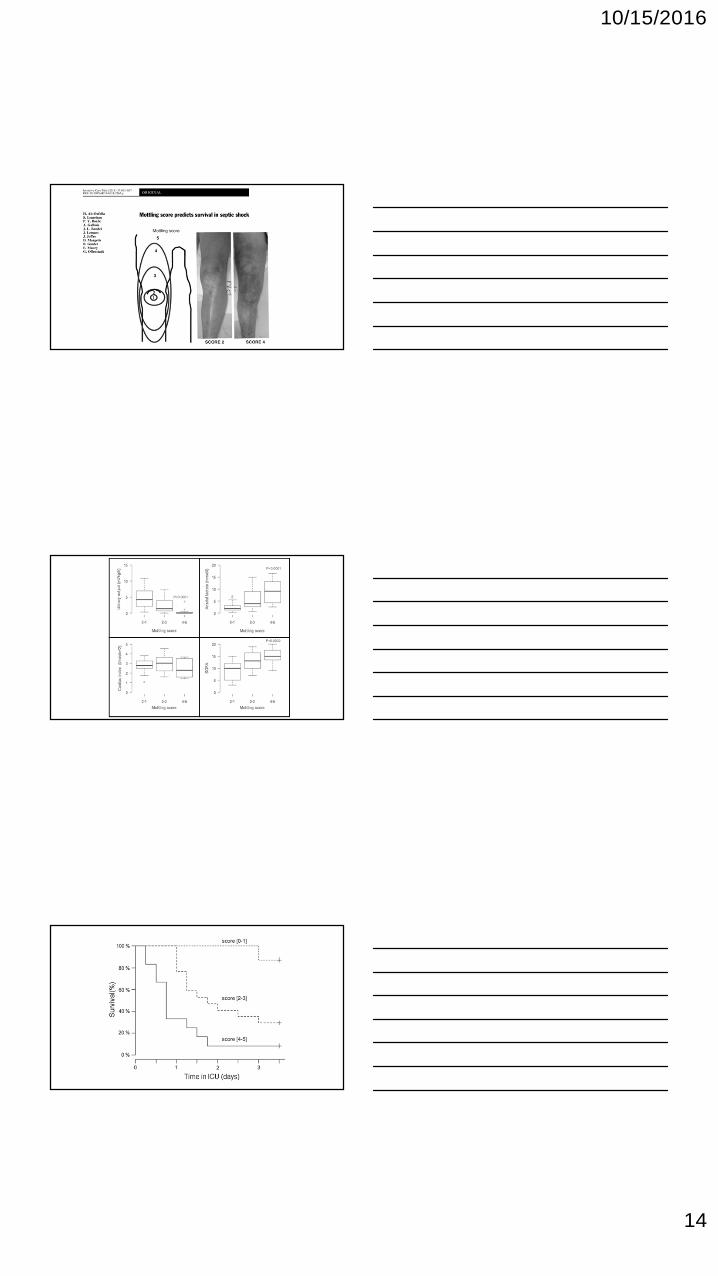
Mottling ScoreShock Index
Diagnosing Severe Sepsis andSeptic Shock
The Origin of SIRS
1991

10/15/2016
10
SIRS in the Emergency Department
Tuttle A, Nowak Rm, Grzybowski M, Rivers EP, Dereczyk BE, Morris DC, Jaggi FM, Ander DS, Tomlanovich MC:The systemic inflammatory response syndrome at triage: prevalence and association with hospital admissions.
Acad Emergency Medicine 1996, 3(478).
Pneumonia and Creatinine of 4.2 mg/dl
isSevere Sepsis

10/15/2016
11

10/15/2016
12
The prognostic ability of qSOFAwas similar to that of SOFA andAPACHE II but slightly inferior to
that of MEDS.
The performance of qSOFA inpredicting ICU admission was
similar to that of SOFA,MEDS, and APACHE II.
Super SIRSSuspected Infection
Two or more:
• Temperature ≥38.3oC or ≤36oC
• HR ≥120 beats/min
• Respirations ≥24/min
• Systolic < 90 mmHg
10/15/2016
13
What are the physicalexamination findings of sepsis?
10/15/2016
14

10/15/2016
15
Antibiotic Therapy
Crit Care Med,2014
Crit Care Med,2014
8.5% Increase in Mortality

10/15/2016
16
Importance of Blood Cultures andAdequacy of Antibiotics
5,715 patients,Retrospective,
Multicenter
52%10.3% 9.45

10/15/2016
17

10/15/2016
18
The Importance ofSource Control

10/15/2016
19
Crit Care Med, 2004
Sigmoid Perforation in Association with Colonoscopy
Lu A, Aronowitz P. N Engl J Med 2012;366:744-744.
Every hour of delay from admission to surgery was associated with an adjusted2.4% decreased probability of survival compared with the previous hour.
10/15/2016
20
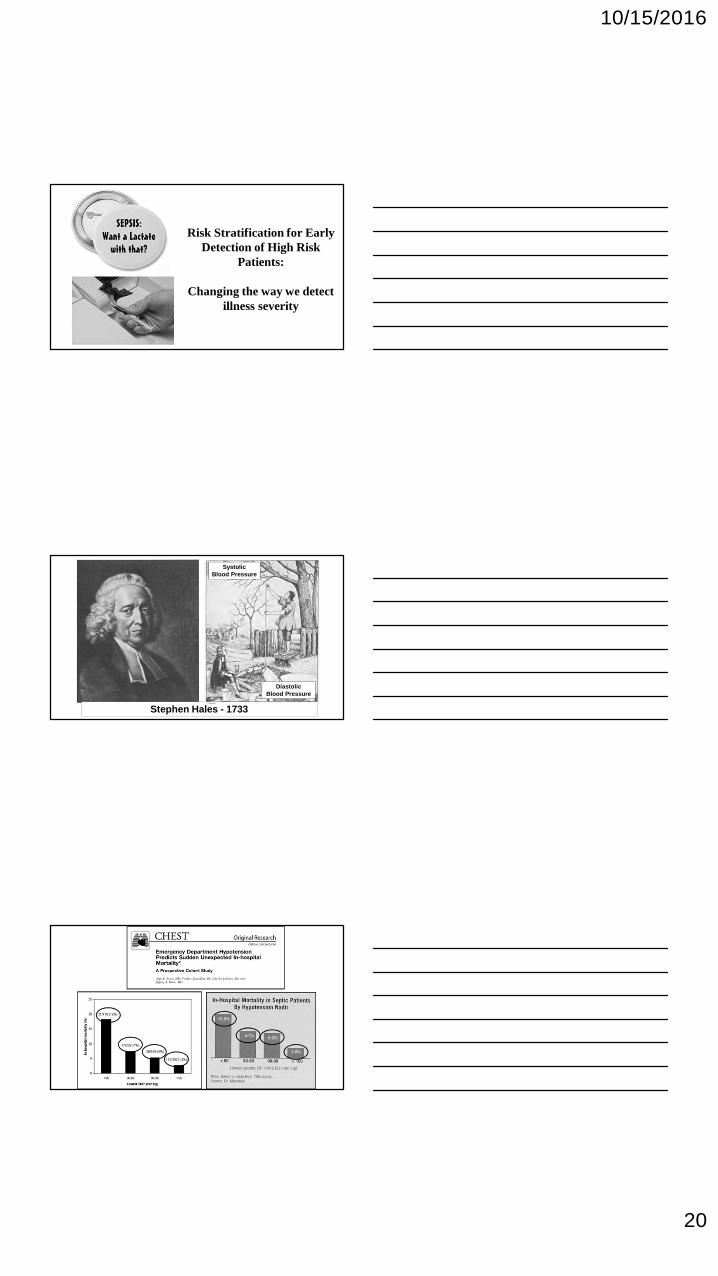
Risk Stratification for EarlyDetection of High Risk
Patients:
Changing the way we detectillness severity
Stephen Hales - 1733
SystolicBlood Pressure
DiastolicBlood Pressure
10/15/2016
21
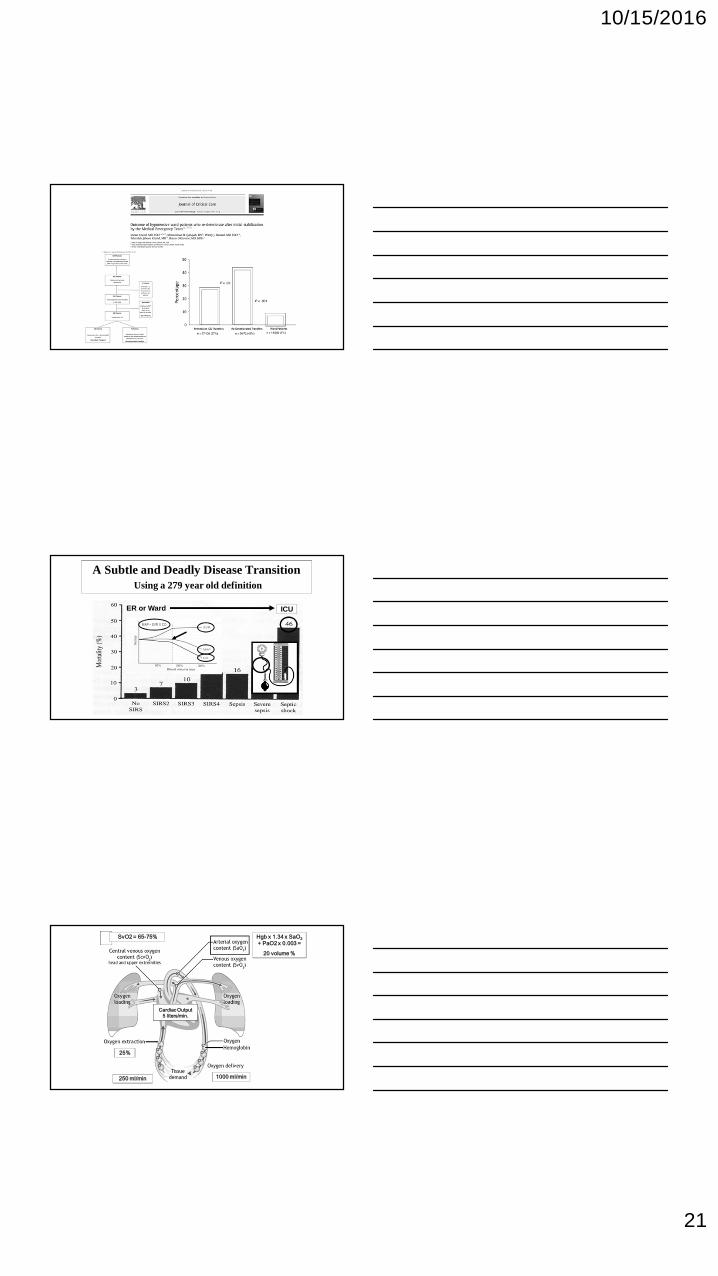
A Subtle and Deadly Disease TransitionUsing a 279 year old definition
ER or Ward ICU
MAP ~ SVR X CO
250 ml/min
25%
1000 ml/min
SvO2 = 65-75% Hgb x 1.34 x SaO2
+ PaO2 x 0.003 =
20 volume %
Cardiac Output5 liters/min.

10/15/2016
22
70-75%
VO2
• Stress
• Pain
• Hyperthermia
• Shivering
• Work of breathing
DO2
• SaO2/PaO2
• Hgb
• Cardiac Output
- +
ScvO2 SvO2
Global Tissue Hypoxia:A More Sensitive Measure of Shock
OXYGENBALANCE
Global TissueHypoxia
OXYGENDEMAND
OXYGENDELIVERY
Lactic Acid> 4 mM/L
Where did a Lactate cut point of 4 come from?
56 patients with clinical signs of shock:Hypovolemia (17), Sepsis (9), cardiac failure (7),neural dys. & endocrine def. (4), vascular obs. (2),mixed (9), unclassified (8)
Broder G, Weil MH.Science 1964;143:1457-1459
Seminal Lactate Studies

10/15/2016
23
Screening for Severe IllnessInfection and Lactate (LA > 4 mM/L)
#SIRS SIRSWard (%)
SIRS + LAWard (%)
SIRS + LAICU
0 11.6 33.3 0
1 14.7 15.4 0
2 34.6 40.0 62.5
3 55.4 84.6 94.5
4 70.0 100 100
≥ 2 of the following is SIRS:
– Temperature ≥38oC or ≤36oC
– HR ≥ 90 beats/min
– Respirations ≥ 20/min
– WBC count ≥12,000/mm3
or ≤4,000/mm3
or >10% bands
– PaCO2 < 32mmHg
Grzybowski M, Tuttle A, Nowak R, Rivers EP, Dereczyk BE, Tomlanovich MC: : Systemic inflammatory response syndromecriteria and lactic acidosis in the detection of critical illness among patients presenting to the emergency department.
Chest 1996, 110:145S.
Lactate > 4 mM/L
28%
Low ScvO223%
Hypotension
28%
46% 51%
56%
35%
Crit Care Med, 2014

10/15/2016
24
Cardiovascular Insufficiency and Global Tissue Hypoxia:The Most Common Cause of Death in the First 24 hours
TachycardiaHypotension
Global TissueHypoxia
Brun-Buisson, C., F. Doyon, et al. (1995)."Incidence, risk factors, and outcome of severe sepsisand septic shock in adults.A multicenter prospectivestudy in intensive care units. French ICU Group for
Severe Sepsis." JAMA 274(12): 968-74.
Cryptic ShockSudden
CardiopulmonaryComplications
ED
Floors
20%
Check Initial and Repeat Lactate?
Case
• 78 year old female
• 2 weeks after AAA
• T – 39o C
• Cough
• Brown sputum
• Right sided chestpain
SvO24 mM/L

10/15/2016
25
12.1% of AllCardiac ArrestsAre pnuemonia
Repeat Lactate:The Implications ofLactate Clearance

10/15/2016
26
Quartiles of Lactate Clearance
Initial Lactate minus Later LactateInitial Lactate
Bad Good
Lactate
Sudden CardiopulmonaryComplications
Is there anequivalent number of
interventions?

10/15/2016
27
10/15/2016
28
How Do I Lactate Clearance Clinically?
• Be careful with alactemic septic shock
– 25-50% of patients have lactate < 2.0 mmol/L.
• Lactate can be influenced by:
– Inadequate source control, dead bowel
– Inadequate delivery (corrected by ScvO2)
– Overuse of vasopressors
– Liver disease
– Thiamine deficiency, metformin, protease
• Identification
– Suspect infection (SIRS)
• Initiation
• Cultures, Antibiotics
– Source Control
• Risk Stratification
– Fluid challenge
– Lactate (Initial and Repeat)
• Hemodynamic Optimization
– Preload
– Afterload
– Contractility
– Balance DO2 & VO2
• Immunomodulation (steroids)

10/15/2016
29
• Mechanical Ventilation
• Quality Initiatives
• Economics
• Outcome Benefits
• ProCESS, ARISE and ProMISe
• Future of Sepsis Management
The Hemodynamics ofSeptic Shock
Increased Metabolic Demands:Fever, Tachypnea Hypovolemia,Vasodilation &
Myocardial Depression
Microvascular Alterations:Impaired Tissue Oxygen
Utilization
Inflammatory Mediators Produce Cardiovascular Insufficiency
Cytopathic Tissue Hypoxia
Fink, Crit Care Clin, 2002

10/15/2016
30
MAP CVP
Cardiac Index ScvO2
ProCESS,ProMISe
and ARISe
Oxygen Debt: To Pay or Not to Pay

10/15/2016
31
Optimization Trials“A Closer Look”
Mortality
(Boyd, New Horiz, 1996)
Early
Late
(Kern, Crit Care Med, 2002)
10/15/2016
32
Task Force of the American College ofCritical Care Medicine
Practice parameters for hemodynamicsupport of sepsis in adult patients in
sepsis.
Crit Care Med 1999 ;27:639-60
Fluids Vasopressors
Hematocrit of 30%
SvO2
LactateInotropes
Importance of the Fluid Challenge
10/15/2016
33
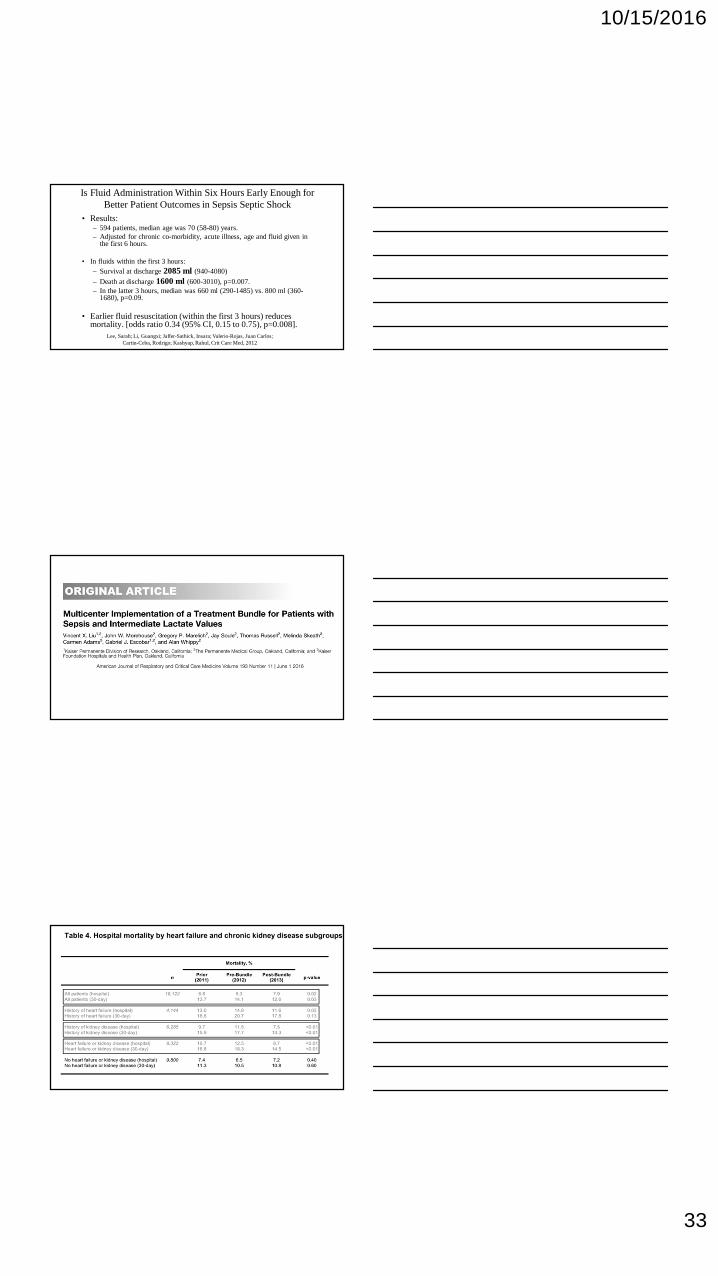
Is Fluid Administration Within Six Hours Early Enough forBetter Patient Outcomes in Sepsis Septic Shock
• Results:– 594 patients, median age was 70 (58-80) years.– Adjusted for chronic co-morbidity, acute illness, age and fluid given in
the first 6 hours.
• In fluids within the first 3 hours:
– Survival at discharge 2085 ml (940-4080)
– Death at discharge 1600 ml (600-3010), p=0.007.– In the latter 3 hours, median was 660 ml (290-1485) vs. 800 ml (360-
1680), p=0.09.
• Earlier fluid resuscitation (within the first 3 hours) reducesmortality. [odds ratio 0.34 (95% CI, 0.15 to 0.75), p=0.008].
Lee, Sarah; Li, Guangxi; Jaffer-Sathick, Insara; Valerio-Rojas, Juan Carlos;Cartin-Ceba, Rodrigo; Kashyap, Rahul, Crit Care Med, 2012

10/15/2016
34
4981
3499
“The earlier fluid resuscitation may account for the lack ofoutcome differences in the trial and may have contributedto the overall low 60-day in-hospital mortality rate of 19%.”
You want to pick a fight?Just mention CVP

10/15/2016
35
Late
Early
999,949
203,481
10/15/2016
36
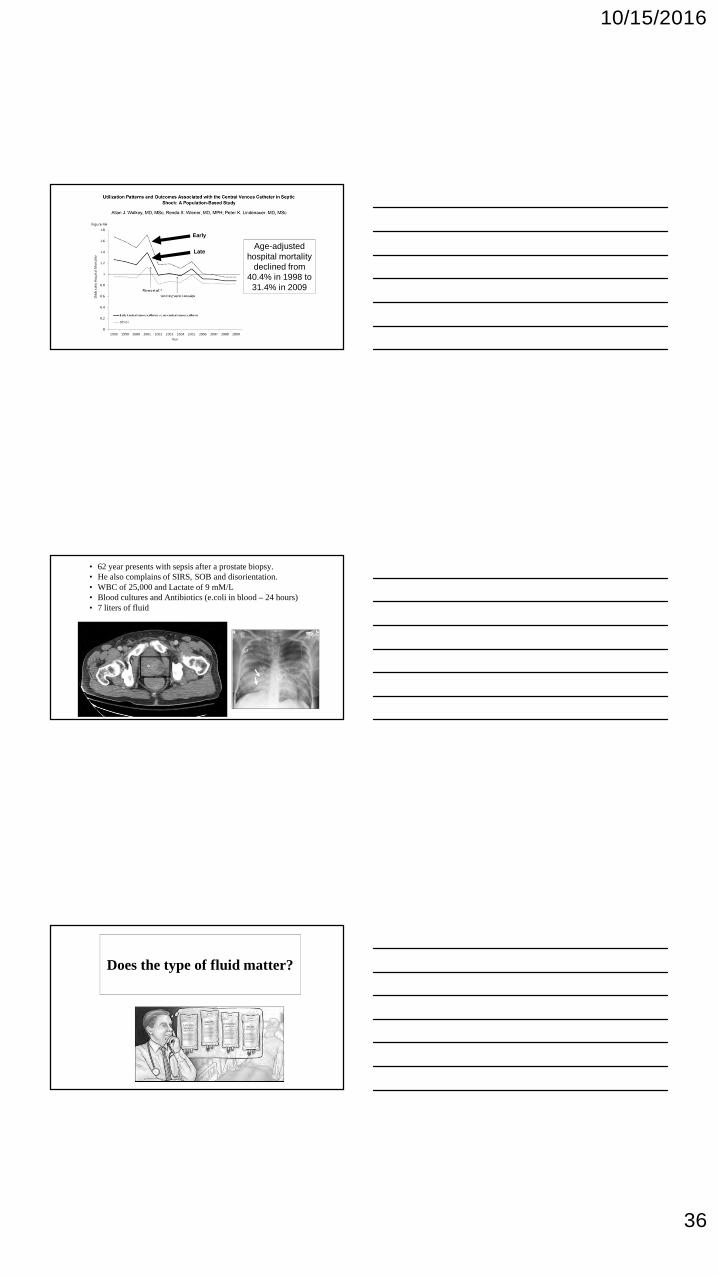
Early
LateAge-adjusted
hospital mortalitydeclined from
40.4% in 1998 to31.4% in 2009
• 62 year presents with sepsis after a prostate biopsy.• He also complains of SIRS, SOB and disorientation.• WBC of 25,000 and Lactate of 9 mM/L• Blood cultures and Antibiotics (e.coli in blood – 24 hours)• 7 liters of fluid
Does the type of fluid matter?

10/15/2016
37
Severe Sepsis

10/15/2016
38
10/15/2016
39
• In critically ill septic patients manifesting hyperchloremia (Cl=110mEq/L) on ICU admission
• Higher Cl levels and within-subject worsening hyperchloremia at 72hours of ICU stay were associated with all-cause hospital mortality.
• These associations were independent of base deficit, cumulative fluidbalance, acute kidney injury, and other critical illness parameters.
Crit Care Med, 2015
Adjuncts to TitratingFluid Therapy

10/15/2016
40
Vasopressor Therapy
10/15/2016
41
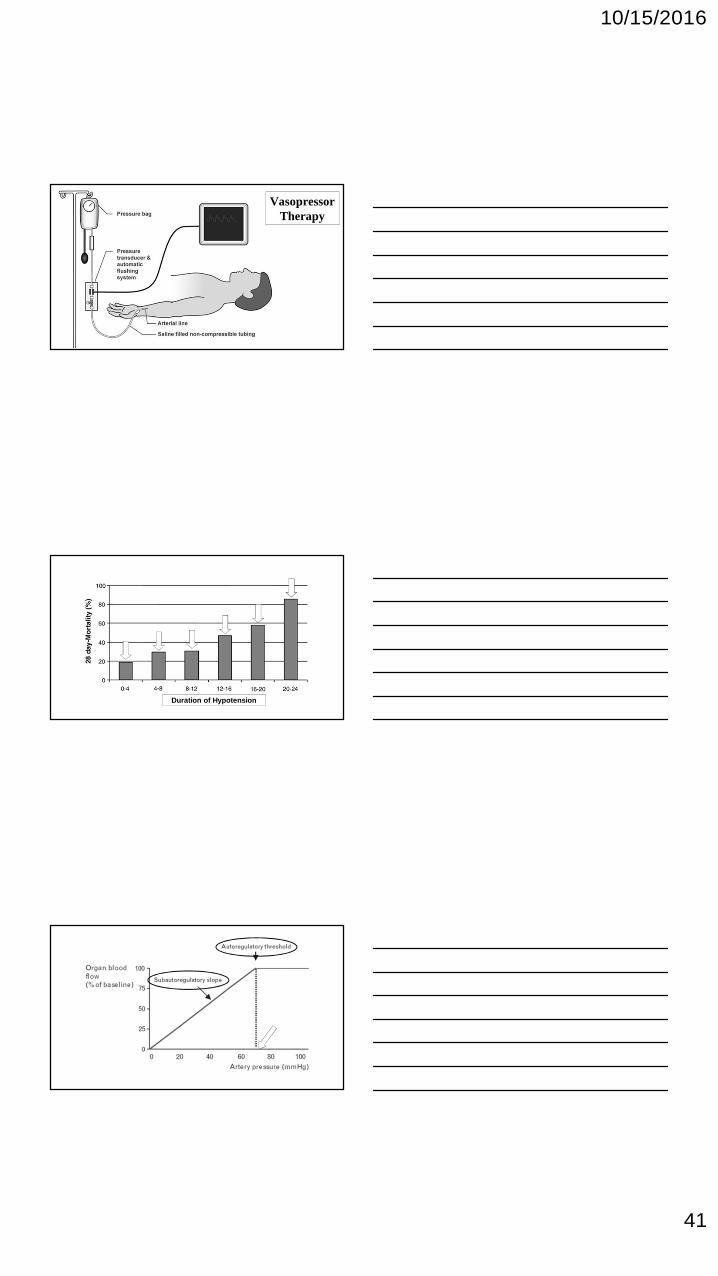
VasopressorTherapy
Duration of Hypotension

10/15/2016
42
March, 2014

10/15/2016
43
The Choice of a Vasopressor
Hypotensive
Tachycardic Patient
Hypotensive
Bradycardic Patient

10/15/2016
44
Early – Ebb PhaseResuscitation
Late – Flow PhaseDe-Resuscitation
Optimal FluidMaintenance
Inadequate Fluid(Hydrophobia)Tissue Hypoxia
Cardiopulmonary EventsInflammationOrgan Failure
Too Much Fluid(Hydrophilia)
Volume OverloadOrgan Failure
Increased Ventilator DaysHemodialysis
Co
mp
licat
ion
s

10/15/2016
45
Complications of Vasopressors
Critical Care Medicine, 2014
• If vasoactive drugs were given in the first hour:
– Higher pressures
– Less fluids were given
• Pharmacologic vasoconstriction and hypovolemia:
– impairs organ perfusion
– increased mortality
• “cold septic shock” is simply hypoperfusion in patients with acirculating volume insufficient to cope with their dilatedcapacitance vessels

10/15/2016
46
Critical Care Medicine, 2014
• Patients become “warm” after administration of adequatevolume of fluids
• These findings support previously shown benefits ofaggressive early fluid resuscitation.
• It may be detrimental to start vasoactive agents withinthe first hour after shock onset.
– Delaying them for at least one hour while the fluid resuscitationis begun.
What do these individuals havein common?
Macrophage
Migration
Inhibition
Factor
(Reichlin, NEJM, 1993)(Chrousos, NEJM, 1995)(Soni, Am J Med, 1995)
(Beishuizen, J Clin Endo & Meb, 2001)
Surgery and
TraumaDrugs
Infection (Sepsis)Intense heat/cold
AdrenalInsufficiency
ContemporaryAdrenal Dysfunction

10/15/2016
47
• The effects of low or high APACHE II score and early or latehydrocortisone initiation are additive (<9 hours).
• High APACHE score (>19), the early initiation ofhydrocortisone increased the survival rate from19.8% to 41.2% (p = 0.021).
• Low APACHE score (< 19), early initiation of hydrocortisoneincreased the survival rate from 55.0% to 83.3%.

10/15/2016
48
14.5% Reductionin Vasopressor
Use if Optimizedwith EGDT
Hold steroid useuntil the patient
has beenresuscitated andendpoints met
(6-8 hours)
CST is optionaland consider a
baseline cortisol

10/15/2016
49
• This was a prospective, multi-centre, observational study conductedover a one-year period in ten French ICUs.
• ScvO2 was measured upon and 6 hours later (H6), by blood sampling.
• More than 25% of septic patients had ScvO2 < 70% in the first hoursafter ICU admission hours after ICU admission..
• 10% higher mortality.

10/15/2016
50
What if my patientis anemic?
NEJM, 2014
NEJM, 2014

10/15/2016
51
NEJM, 2014
Myocardial Suppression andInotropic Therapy

10/15/2016
52
Global TissueHypoxia
InflammatoryMediators
Parillo, JClin.Invest, 1985
Difference in Lactate Levels and Cardiac Function Among Three Septic PatientGroups Stratified By Initial Central Venous Oxygen Saturation Levels
Nakamura, Masataka; Coopersmith, Craig; Greg, Martin; McConnell, Kevin; Kandiah, Prem;Still, Mary; Nicholls, Matthew; Oda, Shigeto; Hirasawa, Hiroyuki; Buchman, Timothy
Critical Care Medicine 2012;40 (12) :1-328
NCardiacDisease
Mortality
Low ScvO2 (<70%) 108 38.7% 41.2%
Normal ScvO2 (70-80%) 119 25.0% 24.1%
High ScvO2 (>80%) 78 16.7% 30.8%

10/15/2016
53
Ms. Peterson
• Infected foot – clostridium Perf (anaerobe)
• Lactate of 10 and oliguric
• BNP -3467
• BUN-77 and creatinine 4.3
• CXR
• Ultrasound
Venous Hyperoxia in Sepsis
Pope, Annals of Emerg Med, 2009
< 70% 70 - 90% > 90%

10/15/2016
54
The Microcirculation
Mechanical Ventilation
10/15/2016
55
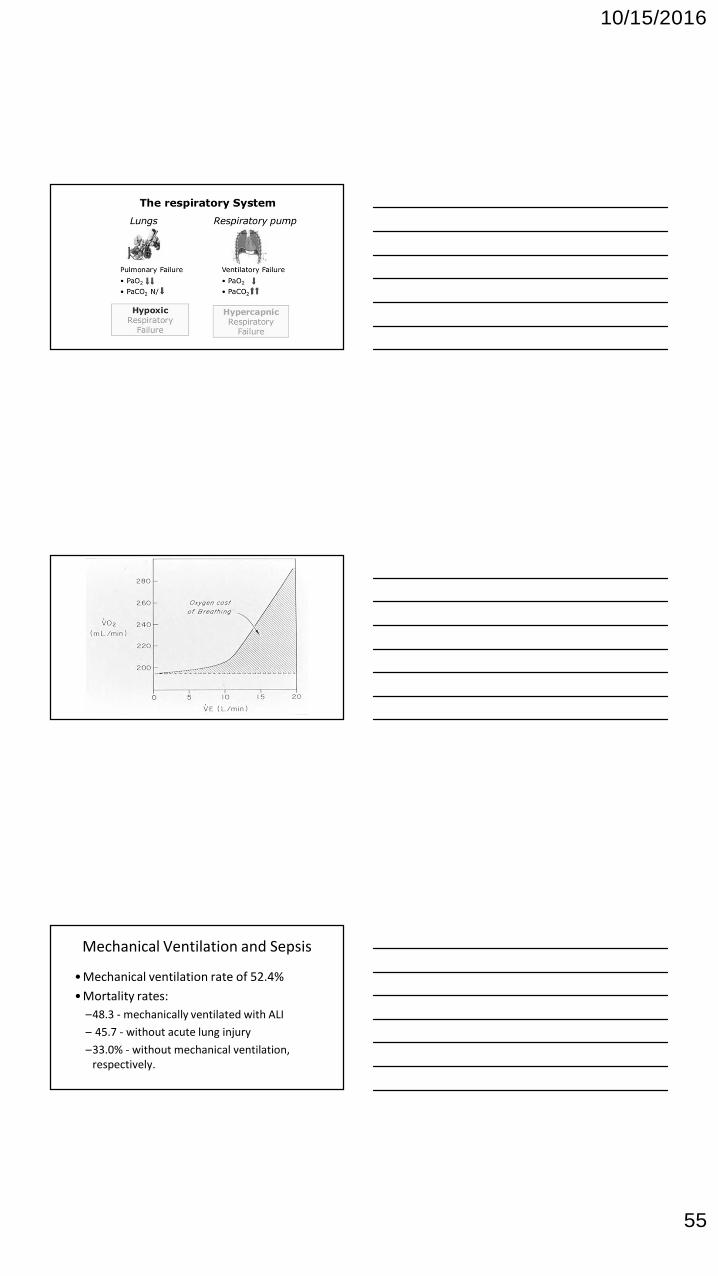
Mechanical Ventilation and Sepsis
• Mechanical ventilation rate of 52.4%
• Mortality rates:
–48.3 - mechanically ventilated with ALI
– 45.7 - without acute lung injury
–33.0% - without mechanical ventilation,respectively.

10/15/2016
56
• Reduction in hospital mortality
• Reduction in baro-trauma
• Reduction in ventilator free days

10/15/2016
57
Early versus LateSepsis Care

10/15/2016
58
2011
How can we over comethe constipation in
sepsis management?
Continuous QualityImprovement
StructureProcess
FeedbackEducation
Outcomes
Donabedian A. Continuity and change in the quest for quality.Clin Perform Qual Health Care. 1993;1:9-16.

10/15/2016
59
Sepsis Guidelines Saves Lives
EGDT after a DecadeNEJM, 2001
Mor
tali
ty%
Pre-EGDT Control EGDT
51%
46%
30%
November 8, 2001
20%
2015

10/15/2016
60
JAMA. 2016;315(8):775-787
Before (Control) After (Treatment) Total
Studies/Patient level data N % Mortality SD N % Mortality SD N
Randomized Control (13) 2776 46.36 20 2831 36.0 15 5607
Quasi experimental (4) 379 45.78 12 741 28.5 12 1120
Prospective observational (33) 25945 40.03 11 36315 26.7 11 62260
Prospective with historical controls (9) 957 45.51 13 1293 29.6 12 2250
Retrospective (19) 1050 41.15 13 1133 24.7 9 2183
Summary of All Studies 31107 42.47 14 42313 28.7 12 73420

10/15/2016
61
March 6, 2013
Joint Commission CMS AHRQ
1. Measure lactate
2. Blood cultures/appropriate cultures
3. Give broad spectrum antibiotics
4. Fluid Challenge of 30 cc/ kg if (hypotension/lactate > 4mM/L)
3H
our
Bu
nd
le6
Ho
ur
Bu
nd
le
5. If persistent hypotension– vasopressor to maintain MAP > 65 mmHg
6. Document perfusion:
7. Re-measure lactate within 6 hours
InvasiveCVP
ScvO2
UltrasoundIVCTEETTE
Dynamic Assessment ofVolume Responsivenessto Fluid Challenge or PLR
SVVSLR
Bioimpedence
Physical ExamPeripheral
PulsesCapillary Refill
(<2 secs)Skin Turgor
• Identification
– Suspect infection (SIRS)
• Initiation (8%)
– Cultures, Antibiotics (6%)
– Source Control (2-16%)
• Risk Stratification
– Fluid challenge (3-5%)
– Lactate (10-12%)
• Hem. Optimization (9-10.4%)
– Preload (CVP)
– Afterload
– Contractility
– Balance DO2 & VO2
• Immunomodulation (8%)





























