Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
International Journal of Law and Psychiatry 30 (2007) 539–545
Compulsory treatment with clozapine: A retrospectivelong-term cohort study
Peter F.J. Schulte a,⁎, Juan J. Stienen b, Jan Bogers c, Dan Cohen a,d, Daniel van Dijk e,Wendell H. Lionarons f, Sophia S. Sanders g, Adolph H. Heck h
a Department De Dijk, Mental Health Services North-Holland North, Kennemerstraatweg 464, 1851 NG Heiloo, The Netherlandsb Department of Psychiatry, Red Cross Hospital, Beverwijk, The Netherlands
c Department Haagstreek, Mental Health Services Rivierduinen, Leidschendam, The Netherlandsd Department of Clinical Epidemiology, University Medical Centre Groningen, Groningen, The Netherlands
e Psychiatric Hospital Dijk en Duin, Castricum, The Netherlandsf Altrecht Mental Health, Utrecht, The Netherlands
g Department Amstelveen, Mental Health Services Buiten Amstel-De Geestgronden, Amstelveen, The Netherlandsh Psychiatric Hospital Symfora Group, Amersfoort, and Forensic Psychiatric Hospital Veldzicht, Balkbrug, The Netherlands
Abstract
Background: Clozapine is the gold standard in treatment of treatment-resistant psychotic patients. We know little about the effectsof compulsory treatment in patients unwilling to accept the necessary treatment.Aims: To assess the effectiveness, tolerability and safety of compulsory treatment with clozapine (CTC).Method: A cohort of 17 consecutive patients given compulsory treatment with clozapine were rated retrospectively by their treatingpsychiatrists on the basis of their case notes.Results: CGI-S decreased significantly over time until last observation after a mean of more than 15 months. No patientdeteriorated as measured by CGI-I. At last observation as many as ten of the 11 patients still on clozapine were classified as muchto very much improved. The degree of custodial restriction at last observation showed improvement in 11 patients and no change insix. No serious adverse events were observed.Conclusion: A trial of compulsory treatment with clozapine showed this treatment to be feasible, effective, safe and well tolerated.© 2007 Elsevier Inc. All rights reserved.
Keywords: Clozapine; Schizophrenia; Treatment refusal; Treatment outcome
1. Introduction
Even after the advent of the new atypical antipsychotics, clozapine is still the gold standard in treatment of treatment-resistant and partially responsive schizophrenia and schizoaffective disorder (American Psychiatric Association, 2004;Schulte, 2001). It shows a superior effect on aggression and suicidality (Meltzer et al., 2003; Volavka et al., 2004).Clozapine should therefore always be offered to patientswith serious treatment–refractory psychotic illness. Unfortunatelylack of insight leading to rejection of antipsychotic medication is a frequent phenomenon amongst psychotic patients,
⁎ Corresponding author. Tel.: +31 72 531 2300; fax: +31 72 531 2391.E-mail address: [email protected] (P.F.J. Schulte).
0160-2527/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.ijlp.2007.09.003

540 P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
especially under the most seriously affected. A literature search revealed only two publications on compulsory restart ofclozapine after refusal (Lokshin, Lerner, Miodownik, Dobrusin, & Belmaker, 1999; McLean & Juckes, 2001).
We intended to investigate the effectiveness, tolerability and safety of CTC in patients without earlier treatment withclozapine. A prospective randomised trial in this severely ill, uncooperative and often incapable patient group with ahigh risk for violence and suicide did not seem feasible and would have been open to severe ethical objections. Even anactive control group with a nonclozapine antipsychotic seemed impracticable since clozapine was judged the onlyappropriate drug in these patients, mainly because of refractory psychotic illness. We therefore decided to evaluate acohort of CTC patients retrospectively, by chart review.
2. Methods
2.1. Design and inclusion criteria
All psychiatrists of the ClozapinePlusCollaborationGroup (CPCG), a Dutch group for study and consultation with regard toclozapine and therapy–refractory psychotic patients, were asked whether they had treated patients compulsorily with clozapine.Under Dutch legislation, compulsory treatment can be administered when patients pose a serious threat to themselves, others or theirenvironment. These patients are normally assaultive or suicidal, mutilate themselves or are seriously deteriorating undercircumstances considered to be inhuman. Due to the risk of agranulocytosis, in Europe the therapeutic indication of clozapine has beenrestricted mainly to schizophrenic patients resistant or intolerant to other antipsychotics. Agranulocytosis occurs in less than 1% ofexposed patients (Alvir, Lieberman, Safferman, Schwimmer, & Schaaf, 1993; Munro et al., 1999). On the other hand clozapine has aspecific antisuicidal effect and may decrease suicide and suicide attempts substantially (Duggan, Warner, Knapp, & Kerwin, 2003;Hennen & Baldessarini, 2005). Furthermore, clozapine has unique antiaggressive features independent of its antipsychotic effect(Krakowski, Czoborm, Citrome, Bark, & Cooper, 2006; Volavka et al., 2004). Psychiatrists in the ClozapinePlusCollaborationGrouphave therefore assessed clozapine's benefit/risk ratio as being favourable for highly selected patients. In the Netherlands compulsorytreatment is only possible in patients under judicially forced hospitalization (court order). If a psychiatrist had been unable to convincea patient of the necessity of treatment with clozapine and had subsequently given the patient the choice of taking clozapine orally orotherwise being given an injection with clozapine, we defined this patient's treatment as compulsory, even if in the end the patient haddecided to swallow the medication. There were no exclusion criteria. The treating psychiatrists were asked to fill out a questionnairedeveloped by the CPCG for each patient, on the basis of the individual case notes and from their memory. Since CTC is not an ordinarytreatment they remembered those cases very well. The questionnaire recorded clinical characteristics of the patient, aspects ofdecision-making (duration and clinical weighing), kind of coercion and practical issues of CTC, including whether treatment withclozapine could ultimately be continued or not.
2.2. Effectiveness
The primary measure of effectiveness was the change from baseline (T0) until the end of the acute-treatment phase (T1) and lastobservation (T2) with Clinical Global Impression—Severity (CGI-S) and Clinical Global Impression—Improvement (CGI-I) (Guy,1976). Response was defined as a CGI-I of 1 (very much improved) or 2 (much improved). The point taken as the end of the acute-treatment phase with clozapine was determined by the treating psychiatrist's clinical judgement, since this duration may vary widelyinterindividually (Wilson, 1996). The point of last observation was the last available evaluation of the patient whether on or offclozapine. We were interested in the long-term progress of the patients for several reasons: there was a possibility that someresponders would not sustain their initial improvement, for example due to adherence problems after prolonged clozapine treatment.On the other hand, some positive effects of clozapine – especially on negative and cognitive symptoms –may take several months todevelop (Buchanan, Holstien, & Breier, 1994; Rosenheck et al., 1999). Moreover, we wanted to evaluate whether a putativedetrimental effect of coercion at T1 would last until T2.
As a secondary measure, the amount of custodial restriction at T0 and T2 was noted. We constructed a scale from the mostrestrictive to the least restrictive environment, ranging from restraint/separation, closed ward, open ward with 24-hour nursing staffor 16-hour nursing staff, sheltered accommodation, nursing staff on request, to private accommodation.
Since compulsory treatment is an intervention which may be traumatic and detrimental to the patient, we asked about theretrospective subjective judgement (positive/negative/neutral) of the patient on the effect of the compulsory treatment at T2. Theoverall judgements of the family and treating psychiatrist integrating all positive and negative effects of CTC were also evaluated.
2.3. Tolerability and safety
Tolerability of clozapine injections was evaluated by Clinical Global Impression Scale—Tolerance (CGI-T, a rating scale from 1(excellent) to 5 (discontinuation necessary) (Guelfi, Payan, Fermanian, Pedarriosse, & Manfredi, 1992). Every adverse event was to be

Table 1Demographic and clinical characteristics of subjects treated compulsorily with clozapine
Characteristic Total group (N=17)
N or mean %
Age, years: mean (S.D.) 40.6 (12.8)Sex
Male 10 59Female 7 41
RaceWhite 13 76Black 1 6Other 3 18
Diagnosis (DSM-IV)Schizophrenia, paranoid type a 12 71Schizophrenia, undifferentiated type 2 12Schizophrenia, disorganised type 0 0Schizophrenia, catatonic type 0 0Schizoaffective disorder 3 18
Duration of illness since onset (years)Zero to one 0 0One to two 0 0Two to five 2 12Five to ten 3 18More than ten 12 71
IncapacityWith respect to illness/treatment 9 53General incapacity 5 29
Reasons for compulsory treatment with clozapine b
Treatment-resistant disease 16 94Serious suffering of patient 16 94Serious suffering of surrounding 5 29Suicidality 2 12Assaultiveness 10 59Automutilation 2 12Self-neglect/anorexia 5 29Risk of permanent hospitalization 1 6a One patient was also mentally retarded.b Several reasons possible.
541P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
registered if the treating psychiatrist considered the relation with intramuscular clozapine as “very probable” according to the followingdefinition: an adverse event which is mentioned as a possible side effect in the clozapine product information and which cannot beexplained by other reasons such as concomitant medication or concomitant diseases. Safety was evaluated by registration of all seriousadverse events during treatment with clozapine injections, irrespective of causation. Serious adverse events were defined as those thatresulted in death or were life-threatening, required hospitalization or prolongation of hospitalization, resulted in persistent or significantdisability or incapacity, or resulted in a congenital anomaly or birth defect. Serious adverse events were evaluated for duration andpossible relation to the study drug.
3. Results
Seven psychiatrists reported on 17 patients who had been treated compulsorilywith clozapine in the period from January 1998 to July2003. There were no other psychiatrists in the CPCGwho had had experiencewith this situation. The seven reporting psychiatrists statedthat they were quite sure that they remembered all patients to whom they had given compulsory treatment with clozapine during theabove-mentioned period and had evaluated the effects of this treatment. Therefore the patient group forms a complete cohort of allrelevant cases. Eleven cases were reported within one month after T2, four cases within a year and one two years later.
Demographic and clinical characteristics are presented for the 17 subjects who met the inclusion criteria in Table 1. 10 patientswere male (59%). The mean (S.D.) age of the group was 40.6 (12.8). 14 (82%) were diagnosed with schizophrenia and 3 (18%) withschizoaffective disorder. At the beginning of the period all patients were hospitalized in closed wards, seven patients in seclusionrooms. The majority of the patients had been ill for more than 10 years. The psychiatrists rated severity of illness in all patients as

Table 2Course of CGI-S with CTC at T0, T1 and T2
a
Patient T0 T1 T2
A 6 3 5B 7 3 3C 6 4 4D 6 4 3E 6 4 3F 6 4 4G 7 7 7Hb 7 7 7I 6 4 4J 7 4 4K 6 6 4L 7 4 4M 7 6 4N 6 4 4O 6 4 6P 6 4 6Q 7 6 4
a Figures in italics: patient off clozapine.b This patient was at T2 (after 7 months) still in the acute-treatment phase.
542 P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
“very ill” or “one of the most ill patients”. 14 patients (82%) were judged to be incapable, at least in respect to treatment decisions.The severity of illness in this population is highlighted by the reasons which led to CTC (Table 1): treatment-resistance combinedwith serious suffering, suicidality, automutilation, assaultiveness, self-neglect, anorexia, or risk of permanent hospitalization. Therewere always several reasons leading to the decision to give compulsory treatment, with one exception: a patient in whose caseassaultiveness was the only reason. The duration of the decisional process (discussion with the patient, his or her family and thenursing staff) was 2 days in one case (6%), three to four weeks in four cases (19%), six to twelve weeks in four cases (19%), and sixto eight months in seven cases (44%). CTC was thus not an emergency intervention but the result of a thorough and carefulconsideration.
3.1. Characteristics of coercion and clozapine injection treatment
The most serious form of coercion, physical constraint, was necessary in only three patients (18%). Five patients (29%)collaborated after intimidation by heavy nursing presence. In all other patients the firmly stated choice of taking clozapine orally orotherwise being given an injection with clozapine was sufficient. In 7 patients (41%) no injection was necessary, and 10 patients(59%) were given at least one injection. Duration of injection treatment was one to four days for four patients (40%), seven to elevendays for three patients (30%), and one to three months for three patients (30%). The maximum daily dosage of IM clozapine, given inone or two injections, was 12.5 to 25 mg for four patients, and 50 mg, 150 mg, 200 mg, 225 mg, 300 mg and 500 mg for six patientsrespectively. Reasons for termination of clozapine were side-effects in two patients (leucopenia with IM clozapine and impaired liverfunction tests with oral clozapine in one patient each), and continuous injection treatment of 90 days without perspective of a switchto oral treatment in one. One patient's treatment had to be discontinued because of further psychic and somatic deterioration andswelling at the injection site. Another patient recovered to such an extent that he could convince the commission for complaints thatcompulsory treatment should be stopped. He was in a relapse at T2 but was treated successfully with a second course of CTC later on.The last patient convinced the locum to return to compulsory treatment with haloperidoldecanoate and stopped his hunger strike.
3.2. Effectiveness
The course of CGI-S scores shows a favourable time effect of CTC (see Table 2). Mean CGI-S decreased significantly from 6.4before initiation of clozapine to 4.6 at the end of the acute-treatment phase (T1, mean (S.D.) 7.8 (6.8) weeks after baseline) and 4.5 atlast observation (T2, mean 15.7 (17.3) months after baseline) (Friedman's nonparametric test: Chi-square 21.06; df 2; pb .0001).This interpretation is substantiated by mean CGI-I: 2.5 (moderately improved) between T0 and T1 and 2.3 (much improved) betweenT0 and T2. The slight improvement between T2 and T1 as shown by CGI-S is reflected by a mean CGI-I of 3.4 between these pointsin time. Eight of 17 patients with CTC (47%) were considered to be responders (CGI-I of 1 (very much improved) or 2 (muchimproved) at the end of the acute-treatment phase. At last observation as many as ten of the 11 patients still on clozapine (59% of thetotal cohort) were classified as much improved or very much improved, although the patients on clozapine were followed up (T2) for

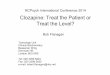
Fig. 1. Retrospective overall judgement of CTC in absolute numbers.
543P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
a mean of 15.2 months. At T2 eight patients were taking clozapine voluntarily (mean CGI-I: 1.9), while three still needed somecoercion (mean CGI-I: 1.3). The remaining six patients had returned to other antipsychotics than clozapine; half of them were takingtheir medication voluntarily (mean CGI-I: 3.0), the other half compulsorily (mean CGI-I: 3.7).
The degree of custodial restriction at T2 showed improvement in 11 patients (65%) and no change in six (35%). No patientneeded more custodial restriction at T2 in comparison to T0.
Fig. 1 shows retrospective judgements on the positive and negative overall effects of the compulsory treatment by patient, familyand psychiatrist. Even in this difficult-to-treat patient population there were more satisfied than dissatisfied patients. Families andpsychiatrists were even more positive on the outcome of CTC: only in one case (6%) was there a negative judgement on the overalleffects of the treatment while nearly all other cases were judged as positive.
3.3. Tolerability and safety
Seven patients (70%) tolerated the injection treatment very well or showed only minor side effects (CGI-T of 1 or 2). Sialorrhoeawas reported in two patients, and somnolence and speech disorder in one patient. Two patients with a dosage of 150 mg and 225 mgrespectively developed local swelling and one patient backflow of clozapine solution at the injection site. Transient leucopenia wasseen in one patient and led to cessation of CTC (CGI-T of 5). No serious adverse events were observed.
4. Discussion
4.1. Good effect of CTC in the majority of patients
The results of this naturalistic long-term study show that in a clozapine naive cohort of 17 patients with seriouschronic psychotic disorders a compulsory trial with clozapine turned out to be feasible, effective, safe and well tolerated.
The amount of coercion was rather low. Seven patients never needed to be given an injection. Only three patientsrequired physical constraint to administer the clozapine injection. Eight out of 17 patients (47%) were consideredresponders at the end of the acute-treatment phase with CTC.
At last observation, after a mean of 15.7 months, the CGI-S had significantly decreased by almost two points. At thattime, ten out of 17 patients (59%) showed a favourable response to clozapine. This is in agreement with findings inpatients with treatment–refractory schizophrenia or schizoaffective disorder, where clozapine shows a 69% responserate if the plasma level is above the necessary threshold (Schulte, 2003). Recently the outcome of compulsoryantipsychotic treatment was shown to be no poorer than that of voluntary treatment in a comparison group (Steinert &Schmidt, 2004). Our results may point in the same direction for clozapine.
4.2. No deterioration in others
No patient at any time point in our study was rated as having deteriorated in comparison to the baseline assessedby CGI-I. Thus we conclude that CTC had a positive treatment effect on the whole group treated and that it had no

544 P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
deleterious psychopathological effects on individuals. This result is in agreement with findings in psychiatricpatients that only 24% of all posttraumatic stress symptoms were related to hospitalization and coercion, while 69%were related to terrifying psychotic experiences (Meyer, Taiminen, Vuori, Äijälä, & Helenius, 1999). Judging by aCGI-qualification of improved or very much improved, ten of eleven patients staying on clozapine until lastobservation were responders. Clozapine may – even if treated compulsorily – reduce liability to posttraumaticstress symptoms by ameliorating hallucinations and paranoia. The positive results quantified by the CGI-scalesare sustained by the declining need of restrictive environments. Thus in our cohort CTC ultimately led to lesscoercion.
It is remarkable that at last observation only three patients were negative about their CTC, while five were positiveand seven neutral. Eight of 17 patients chose to continue clozapine voluntarily. Most studies of patients' retrospectiveattitudes towards their compulsory treatment indicate that while the majority are positive, there is a substantial minoritywith a negative attitude (Adams & Hafner, 1991; Finzen, Haug, Beck, & Lüthi, 1993; Greenberg et al., 1996; Naber,Kircher, & Hessel, 1996; Svensson & Hansson, 1994) . On the other hand, in our sample 85% of the families and 88%of the psychiatrists were retrospectively satisfied with the overall effects of CTC. Therefore, on the whole our resultsindicate a favourable effect of CTC despite the necessity of coercion.
The total number of reported adverse events due to clozapine injection in our study is lower than might be expectedfrom the literature on oral or injection treatment with clozapine (Dev & Krupp, 1995; Lokshin et al., 1999). In a study of59 patients treated with clozapine injections 32% complained of mild side effects other than sedation: constipation(12%), headache (10%) or a dry mouth (4%). In this study no changes in laboratory measures were observed. Wepresume that in our study the treating psychiatrists noted in their case notes only those adverse events which were moresevere than those normally expected with oral clozapine or which were clinically significant and led to cessation ofclozapine treatment. We conclude that clozapine injections do not appear to be much less tolerable or safe than the oraltreatment.
4.3. Limitations of this study
Wemust acknowledge several shortcomings of our approach. Firstly, the fact that the retrospective evaluations madeby the treating psychiatrists were not tested for reliability may have biased the results. Next, the use of CGI rather thanspecific psychopathological scales for psychosis and posttraumatic symptoms impairs insight into the domain ofpsychopathological change. Lack of a comparison group obscures the interpretation of our results; however, thesubstantial improvement in the majority of patients could not have been expected without clozapine in this long-standing and seriously ill, treatment-resistant population. The same holds true for safety and tolerability: data had notbeen registered in a systematic way and there was no comparison. Side effects can easily be underreported. Because ofthese shortcomings our results should be viewed with caution and will bear further study. Nonetheless, our study is toour knowledge the first report on CTC in patients without earlier treatment with clozapine. The positive result of theCGI is sustained by improvement of degree of custodial restriction and positive retrospective evaluation by families inmany cases. In addition we presume that serious adverse events occurring during IM treatment with clozapine wouldhave been reported in the case notes.
5. Conclusion
In assessing the long-term efficacy of medication, randomised placebo-controlled trials are generally considered themost robust method. In a population like our cohort of severely ill, uncooperative and often incapable patients with ahigh risk for violence and suicide, it is not very probable that such a study will be conducted in the near future. Even aprospective naturalistic study will be hampered by difficulties in obtaining informed consent for a study of compulsorytreatment. While a retrospective study has its limitations, we feel that since the positive effects of clozapine intreatment-resistant psychotic illness have been shown over and over again, naturalistic studies such as ours may sufficeto show that this effect is not impeded by the compulsory nature of a trial in this most seriously affected group ofpatients.
Unfortunately Novartis has terminated the production of clozapine ampoules. Hopefully the positive results of CTCpresented here will encourage them to reconsider this decision. Otherwise a pharmacist may be asked to prepare aclozapine solution suited for injection.

545P.F.J. Schulte et al. / International Journal of Law and Psychiatry 30 (2007) 539–545
Acknowledgments
We would like to thank Mrs M.A. Nugter, M.A., Ph.D., for her help and advice with statistical calculations and MrR. Jokhoe, M.D., for registration of data for one patient.
References
Adams, N., & Hafner, R. (1991). Attitudes of psychiatric patients and their relatives to involuntary treatment. Australian and New Zealand Journal ofPsychiatry, 25, 231−237.
Alvir, J. M., Lieberman, J. A., Safferman, A. Z., Schwimmer, J. L., & Schaaf, J. A. (1993). Clozapine-induced risk factors in the United States. TheNew England Journal of Medicine, 329, 162−167.
American Psychiatric Association. (2004). Practice guideline for the treatment of patients with schizophrenia, second edition. American Journal ofPsychiatry, 161 (suppl.).
Buchanan, R. W., Holstein, C., & Breier, A. (1994). The comparative efficacy and long-term effect of clozapine treatment on neuropsychological testperformance. Biological Psychiatry, 36, 717−725.
Dev, V. J., & Krupp, P. (1995). Adverse event profile and safety of clozapine. Review of Contemporary Pharmacotherapy, 6, 197−208.Duggan, A., Warner, A., Knapp, J., & Kerwin, M. (2003). Modelling the impact of clozapine on suicide in patients with treatment-resistant
schizophrenia in the UK. British Journal of Psychiatry, 182, 505−508.Finzen, A., Haug, H. J., Beck, A., & Lüthi, D. (1993). Hilfe wider Willen. Bonn: Psychiatrie Verlag.Greenberg, W., Moore-Duncan, L., & Herron, R. (1996). Patients' attitudes towards having been forcibly medicated. Bulletin American Academy of
Psychiatry and the Law, 24, 513−524.Guelfi, J. D., Payan, C., Fermanian, J., Pedarriosse, A. M., & Manfredi, R. (1992). Moclobemide versus clomipramine in endogenous depression. A
double-blind randomised clinical trial. British Journal of Psychiatry, 160, 519−524.Guy, W. (Ed.). (1976). ECDEU Assessment Manual for Psychopharmacology: Publication ADM 76-338 (pp. 218−222). Washington, DC: US
Department of Health, Education, and Welfare.Hennen, J., & Baldessarini, R. J. (2005). Suicidal risk during treatment with clozapine: A meta-analysis. Schizophrenia Research, 73, 139−145.Krakowski, M. I., Czoborm, P., Citrome, L., Bark, N., & Cooper, T. B. (2006). Atypical antipsychotic agents in the treatment of violent patients with
schizophrenia and schizoaffective disorder. Archives of General Psychiatry, 63, 622−629.Lokshin, P., Lerner, V., Miodownik, C., Dobrusin, M., & Belmaker, R. H. (1999). Parenteral clozapine: Five years of experience (letter). Journal of
Clinical Psychopharmacology, 19, 479−480.McLean, G., & Juckes, L. (2001). Parenteral clozapine (clozaril) (letter). Australasian Psychiatry, 9, 371.Meltzer, H. Y., Alphs, L., Green, A. I., Altamura, A. C., Anand, R., Bertoldi, A., et al. (2003). Clozapine treatment for suicidality in schizophrenia:
International Suicide Prevention Trial (InterSePT). Archives of General Psychiatry, 60, 82−91 (Erratum in: Archives of General Psychiatry, 60, 735).Meyer, H., Taiminen, T., Vuori, T., Äijälä, A., & Helenius, H. (1999). Post-traumatic stress disorder symptoms related to psychosis and acute
involuntary hospitalisation in schizophrenic and delusional patients. Journal of Nervous and Mental Disorders, 187, 343−352.Munro, J., O'Sullivan, D., Andrews, C., Arana, A., Mortimer, A., & Kerwin, R. (1999). Active monitoring of 12760 clozapine recipients in the UK
and Ireland. British Journal of Psychiatry, 175, 576−580.Naber, D., Kircher, T., & Hessel, K. (1996). Schizophrenic patients' retrospective attitudes regarding involuntary psychopharmacological treatment
and restraint. European Psychiatry, 11, 7−11.Rosenheck, R., Dunn, L., Peszke, M., Cramer, J., Xu, W., Thomas, J., et al. (1999). Impact of clozapine on negative symptoms and on the deficit
syndrome in refractory schizophrenia. American Journal of Psychiatry, 156, 88−93.Schulte, P. F. J. (2001). The place of clozapine in the treatment of schizophrenia. Tijdschrift voor Psychiatrie, 43, 715−720.Schulte, P. F. J. (2003). What is an adequate trial with clozapine? Therapeutic drug monitoring and time to response in treatment–refractory
schizophrenia. Clinical Pharmacokinetics, 42, 607−618.Steinert, T., & Schmidt, P. (2004). Effect of voluntariness of participation in treatment on short-term outcome of inpatients with schizophrenia.
Psychiatric Services, 55, 786−791.Svensson, B., & Hansson, L. (1994). Patient satisfaction with inpatient psychiatric care. The influence of personality traits, diagnosis and perceived
coercion. Acta Psychiatrica Scandinavica, 90, 379−384.Volavka, J., Czobor, P., Nolan, K., Sheitman, B., Lindenmayer, J. P., Citrome, L., et al. (2004). Overt aggression and psychotic symptoms in patients
with schizophrenia treated with clozapine, olanzapine, risperidone, or haloperidol. Journal of Clinical Psychopharmacology, 24, 225−228.Wilson, W. (1996). Time required for initial improvement during clozapine treatment of refractory schizophrenia. American Journal of Psychiatry,
15, 951−952.