1. Dr. Mohan Lal Associate Professor Department of Community
Medicine Govt. Medical College ,Amritsar
2. Iceberg Phenomenon of Disease Major submerged portion
consists of :- Subclinical cases Carriers Undiagnosed cases
(apparently healthy individuals) Constitute a mass of unrecognized
disease in the community. Responsible for the constant prevalence
of disease . Detection and a control is challenge .
3. 1 Diseased, diagnosed & controlled 2 Diagnosed,
uncontrolled 3 Undiagnosed or wrongly diagnosed disease 4 Risk
factors for disease 5 Free of risk factors Diagnosed disease
Undiagnosed or wrongly diagnosed disease
4. Defined as the search for unrecognized disease or defect by
means of rapidly applied test, examination or other procedures in
apparently healthy individuals
5. Detection programmes should be restricted to those
conditions in which there is considerable time lag between disease
onset and usual time of diagnosis Lead time is advantage gained by
screening i.e. period between diagnosis by early detection and
diagnosis by other means
6. Aims To sort out those having the disease and those not
having the disease from a group of apparently healthy
individuals.
7. Objectives To provide treatment to those detected persons,
so that the disease is controlled in community
8. Considerations of Screening Screening must be applied to
those people most likely to benefit. Selection must be based on the
persons age, sex, medical history, occupation, family history, etc.
Test with greater accuracy may be more expensive and time
consuming, so choice of test is based on compromise.
9. Screening should be integrated in to existing health
services The risks as well as expected benefits must be explained
to people to be screened Regular patient follow up is also
important
10. Criteria for Screening Public health importance
Recognizable early stage Disease can be diagnosed before the onset
of signs and symptoms Facilities available to confirm diagnosis
Must be effective treatment Disease with treatment , Good
prognosis
11. Screening Disease Important Public health problem- High
Prevalence & Serious outcome Recognized in early/ latent phase
Natural history well understood- Early detection and treatment can
affect the course of disease Test Safe, Accurate, Cost effective,
Suitable & Acceptable Treatment Diagnostic Test Agreed policy
& Treatment Cost Cost of screening< Cost of medical care
Continuing process and not a "once for all" project.
12. Problem of borderline In screening for disease, a prior
decision is made about the cut off point The following factors are
take into consideration: Disease prevalence: when the prevalence is
high in the community, its screening level is set at lower level,
which will increase sensitivity The disease: if the disease is very
lethal and early detection markedly improves prognosis, a greater
degree of sensitivity, even at the expense of specificity, is
desired
13. Uses of Screening Case detection (Prescriptive screening)
Control of the disease(Prospective screening) Research purpose
Educational purpose
14. Case detection It is also known as prescriptive screening.
Defined as presumptive identification of unrecognized disease which
does not arise from patients request. e.g. neonatal screening.
Diseases sought include breast cancer, cervical cancer, diabetes,
tuberculosis, HDN etc. Initiated by medical and public health
personnel, they are under special obligation to make sure that
appropriate treatment is started early.
15. Control of the disease Also known as prospective screening.
People are examined for benefit of others. e.g. screening of
immigrants from infectious diseases such as tuberculosis, syphilis,
streptococcal infection etc. The screening programme may, by
leading to early diagnosis permit more effective treatment and
reduce the spread of infectious disease and/or mortality from the
disease.
16. Educational opportunities Screening programs provide
opportunities for creating public awareness and for educating
health professionals. eg screening for diabetes.
17. Research purposes Screening helps in obtaining basic
knowledge about natural history of chronic diseases. Initial
screening provides prevalence estimate and subsequent screening, an
incidence figure. Where screening is done for research purposes,
the investigator should inform the study participant that no follow
up therapy will be available.
18. DISEASE The disease to be screened should fulfill the
following criteria before its considered suitable for screening 1)
The condition sought should be an important health problem. 2)
There should be a recognizable latent or early asymptomatic stage.
3) The natural history of the condition, including development from
latent to declared disease, should be adequately understood.
19. Flow Chart Apparently healthy Screening test Probably have
disease Diagnostic test Probably do not have disease Have disease
Do not have disease Given treatment Under surveillance Periodic
screening (Screening)
20. Types of Screening Mass screening High risk screening
Multipurpose screening Multiphase screening Opportunistic
screening
21. Mass screening Means screening of the whole population or a
sub group It is offered to all irrespective of particular risk
individual may run of contracting disease in question.
Indiscriminate mass screening is not a useful preventive measure
unless backed up by suitable treatment that will reduce duration of
illness or alter final outcome.
22. High risk or selective screening Screening is most
productive if applied selectively to high risk groups, groups
defined on epidemiological research. Diseases tend to aggregate in
family so screening other members of family can detect additional
cases. Epidemiologists have extended concept of screening to risk
factors.
23. Multi phasic screening Defined as application of two or
more screening test in combination to large number of people at one
time than to carry out separate screening test for single diseases.
Procedure includes health questionnaire, clinical examination and
range of measurements and investigations. E.g. chemical and
hematological tests on blood and urine, lung function assessment,
audiometry etc.
24. Recently multi phasic screening has not shown any benefit
to population in terms of mortality and morbidity reduction. Rather
it has increased the cost of health services without any observable
benefit.
25. Thus screening test divides the apparently healthy
population in to two groups Those probably having the disease Those
probably not having disease
26. The first group is then further subjected to history taking
,clinical examination and diagnostic tests Which divides this group
into two sub- groups Those who have the disease , requiring
treatment Those not having the disease ,requiring Surveillance and
periodic screening
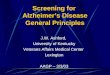
27. Population (1) Examination of urine sugar Persons with
negative result Persons with positive result (2) Examination of
random blood for sugar level Persons with blood glucose level 120
mgm % (3) Oral glucose tolerance test Blood sugar 180 mgm% 2 hrs
after glucose Non- diabetic Impaired glucose tolerance
diabetic
28. Screening differs from periodic health examination o
Capable of wide application o Relatively inexpensive and o Requires
little physician- time
29. Screening test Diagnostic test Done on apparently healthy
people Done on sick people Done on groups Done on individual cases
Done by the epidemiologist Done by the physician Test results are
final Diagnosis is not final but based on other criteria such as
history and clinical findings The purpose is to do community
diagnosis ,to launch a control programme The purpose is to make a
diagnosis in the patient to give treatment Less expensive More
expensive Initiative is from the epidemiologist Initiative is from
patient
30. Criteria for screening test Should be Simple, Safe cheap
and rapidly applied Acceptable by the people Reliable (repeatable
or reproducible)
31. Some Screening Tests Pregnancy Infancy Anemia Hypertension
Toxemia Rh status Syphilis Cardiovascular disease Neural tube
defects Down syndrome HIV Congenital heart disease Spina bifida
visual defects Hypothyroidism Haemoglobinopathies Sickle cell
anemia Middle-aged men and women Elderly hypertension cancer
Diabetes mellitus Serum cholesterol Nutritional disorders Cancer
Glaucoma Cataract
32. SCREENING TEST The test must satisfy the criteria of:
Acceptability Repeatability Validity besides other such as yield,
simplicity, safety, rapidity, ease of administration and cost
also.
33. ACCEPTABILITY Since a high rate of cooperation is
necessary, its important that the test should be acceptable to the
people at whom it is aimed. REPEATABILITY The test must give
consistent results when repeated more than once. It depends on 3
major factors: -- Observer variation -- Biological (Subject)
variation -- Errors relating to technical methods
34. Variations Observer variations A) Intra-observer B)
Inter-observer Biological Variations Mechanical variations Valid
(accurate)
35. OBSERVER VARIATIONS These are of 2 types: a) Intra-observer
variations If a single observer takes two measurements (e.g. BP
& Chest expansion) in the same subject, at the same time and
each time he obtains a different result, this is termed as
intra-observer or within-observer variation. b) Inter-Observer
variation this is variation b/w diff. observers on the same subject
or material, also known as Between-observer variation.
36. BIOLOGICAL (SUBJECT) VARIATIONS There is a biological
availability associated with many physiological variables such as
BP, Blood sugar, Serum cholesterol etc. The fluctuation in the
variate measured in the same individual may be due to: a) Changes
in the parameters observed. E.g. Cervical smears taken from the
same woman may be normal one day, and abnormal on other day.
37. b) Variations in the way patients perceive their symptoms
and answers. c) Regression to mean : There is tendency for values
at the extreme of distribution, to regress toward the mean or
average on repeat measurements.
38. Contd. E.g. elevated serum cholesterol is associated with
high risk of developing coronary heart disease. In this way
preventive measures can be applied before the disease occurs.
39. ERRORS RELATING TO TECHNICAL METHODS: Repeatability may be
affected by variations inherent in the method. e.g. -- Defective
instruments -- Erroneous calibration -- Faulty reagents -- Test
inappropriate or unreliable
40. VALIDITY (ACCURACY) The term Validity refers to what extent
the test accurately measures which it purports to measure. In other
words, validity expresses the ability of a test to separate or
distinguish those who have the disease from those who do not.
41. Diagnosis (screening test results) Diseased Not diseased
Total Positive (True positive ) a (False positive) b (Total
positive) a+b Negative (False negative) c (True negative) d (Total
negative) c+d Total (Total disease) a+c (Total non diseased) b+d
(Grand total) a+b+c+d
42. Validity has two components: Sensitivity Specificity When
assessing the accuracy of a diagnostic test, one must consider both
these components. Both measurements are expressed in percentages.
Sensitivity & Specificity are usually determined by applying
the test, to one group of persons having disease, and to a
reference group not having the disease.
43. Evaluation of screening test
44. Indicators To evaluate screening test: Sensitivity
Specificity Predictive value of positive test Predictive value of
negative test Percentage of false negatives Percentage of false
positives
45. Sensitivity Introduced by Yerushalmy as statistical index
of diagnostic accuracy. Defined as the ability of test to identify
correctly all those who have the disease, that is true
positive.
46. a Sensitivity = x100 a+c Percentage of diseased persons
,showing the test result positive Ability of a test to correctly
identify those having disease (true positive )
47. d Specificity= x100 b+d Ability of the test to correctly
identify those not having the disease Percentage of non-diseased
persons showing the negative results
48. Combination of tests Two or more tests can be used in
combination to enhance specificity or sensitivity of screening. For
example syphilis screening (RPR test) has high sensitivity, yet
will yield false positives. However, all those positive to RPR are
then submitted to FTA-ABS which is more specific test and the
resultant positives now truly have syphilis.
49. Predictive accuracy Performance of screening test is
measured by its predictive value which reflects diagnostic power of
test. Predictive accuracy depends upon sensitivity, specificity and
disease prevalence. More prevalent a disease in a given population,
more accurate will be the predictive value of a positive screening
test.
50. a Predictive value ( + test)= x100 a+b Percentage of
positive probably having the disease
51. d Predictive value (-test)= x100 c+d Percentage of negative
probably not having the disease
52. False positives Means patients who do not have the disease
are told that they have. It causes inconvenience, discomfort,
anxiety and expense to normal healthy people. Screening test with
high specificity will have few false positives
53. b False positive = x100 b+d Percentage of non-diseased
persons wrongly identified as having a disease
54. False negatives Means patients who actually have the
disease are told that they do not have the disease. So patient
might ignore the development of signs and symptoms and may postpone
the treatment. A screening test which is very sensitive has few
false negatives. Lower the sensitivity, larger the number of false
negatives.
55. False negative = x100 Percentage of diseased persons
wrongly identified as not having the disease C a+c
56. That is, a proportion of false positives is tolerable but
not false negatives. On the other hand, in a prevalent disease like
diabetes for which treatment does not markedly alter outcome,
specificity must be high and false positives should be
limited.
57. Yield It is the amount of previously unrecognized disease
that is diagnosed as a result of screening effort. It depend on
sensitivity and specificity of the test, prevalence of the disease
and participation of individuals in the detection program.
58. Gratitude for all authors and sources whose material has
been used for this Presentation