Embed Size (px)
Citation preview

Concise Anatomyfor Anaesthesia

Concise Anatomyfor Anaesthesia
Andreas G ErdmannFellow in Pain ManagementLondonSpecialist Registrar in AnaesthesiaEast Anglian Deanery
London San Francisco
Greenwich Medical Media4th Floor, 137 Euston Road,LondonNW1 2AA
870 Market Street, Ste 720San FranciscoCA 94109, USA
ISBN 1841100692
First Published 2001
Apart from any fair dealing for the purposes of research or private study,or criticism or review, as permitted under the UK Copyright Designsand Patents Act 1988, this publication may not be reproduced, stored,or transmitted, in any form or by any means, without the priorpermission in writing of the publishers, or in the case of reprographicreproduction only in accordance with the terms of the licences issuedby the appropriate Reproduction Rights Organisations outside the UK.Enquiries concerning reproduction outside the terms stated here shouldbe sent to the publishers at the London address printed above.
The rights of Andreas Erdmann to be identified as author of this workhave been asserted by him in accordance with the Copyright Designsand Patents Act 1988.
The publisher makes no representation, express or implied, with regardto the accuracy of the information contained in this book and cannotaccept any legal responsibility or liability for any errors or omissions thatmay be made.
A catalogue record for this book is available from the British Library.
Distributed worldwide by Plymbridge Distributors Ltd and in the USAby Jamco Distribution
Typeset by Phoenix Photosetting, Chatham, KentPrinted by The Alden Group, Oxford
v
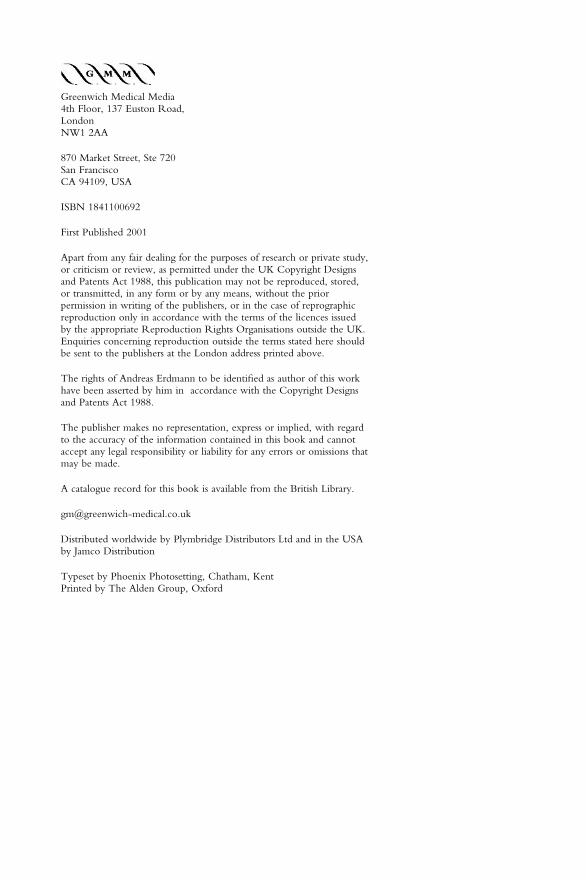
Foreword viiPreface ix
Respiratory System1. The mouth 22. The nose 43. The pharynx 64. The larynx 85. The trachea 146. The bronchi and bronchial
tree 167. The pleura and mediastinum 188. The lungs 209. The diaphragm 22
Sample questions 24
Cardiovascular System10. The heart 2611. The great vessels 30
Aorta 30Great arteries of the neck 30Arteries of the limbs 32Major veins 34
12. Fetal circulation 38Sample questions 40
Nervous System13. The brain 4214. The spinal cord 4415. The spinal meninges and
spaces 4716. The spinal nerves 5017. The nervous plexuses 52
Cervical 52Brachial 52
Lumbar 54Sacrococcygeal 56
18. The major peripheral nerves 60Upper limb 60Lower limb 62Abdominal wall 66Intercostal nerves 66
19. The autonomic nervous system 70Sympathetic 70Parasympathetic 72
20. The cranial nerves 76
Appendices1. Dermatomes of arm 882. Dermatomes of leg 893. Dermatomes of trunk 90Sample questions 91
Vertebral Column21. The vertebrae 9422. The vertebral ligaments 100Sample questions 101
Areas of Special Interest23. The base of the skull 10424. The thoracic inlet 10825. The intercostal space 11226. The abdominal wall 11427. The inguinal region 11628. The antecubital fossa 11829. The large veins of the neck 12030. The axilla 12231. The eye and orbit 124Sample questions 128
Index 137
Contents

vii
When I first started my anaesthesia job, itdid not take me long to realise that I wasgoing to have to relearn a lot of anatomythat had been implanted in my short-term memory during the second MB. Iwas, incorrectly, under the impressionthat anatomy was the sole preserve of thesurgeon.
From the moment that a career inanaesthesia is started, anatomy plays apart. Dr Andreas Erdmann decided towrite this book following his experiencesduring the final FRCA examination. Theidea is a simple one, combining simpleline diagrams and succinct text to coverall of the areas of anatomy essential to
modern anaesthetic practice. It will beinvaluable as a revision text for theFRCA, but will also help anaesthetists toretain anatomy knowledge throughouttheir careers. It will be useful forconsultants teaching trainees and also forother theatre personnel to understand theprocedures carried out by anaesthetists.
I am sure that generations of anaesthetistswill be grateful to Dr Erdmann forproviding such a simple andcomprehensive review of an essentialsubject.
Richard Griffiths MD FRCAPeterborough, June 2001
Foreword

ix
The origin of this concise book ofanatomy results from many commentsfrom FRCA examination candidates.Anatomy has always played an importantrole in the examination syllabus, as wellas being of great practical importance inthe everyday practice of anaesthesia. It isalso a subject that appears to demand adisproportionately large amount of timeduring examination preparation.However, neglect of the anatomicalsubject-matter is perilous and leads to theloss of valuable ‘easy’ marks.
The idea behind this book is to present aconcise and easily digestible outline ofanatomy that has been extensively basedon the current FRCA examinationsyllabus. I have attempted to present thecore anatomical knowledge required forthe Primary and Final FRCAexaminations in a simple andstraightforward manner. There arenumerous diagrams to illustrate thesubject matter, as well as additional spacefor the addition of personal notes. It is,however, impossible within the
constraints of this book to provide in-depth detail and this should be obtainedby reference to some of the largertextbooks. Sample questions are includedat the end of each section, and includequestions similar to those asked inprevious examinations.
It is hoped that this book may also be ofhelp to those teaching anatomy toFRCA candidates, as well as to allpractising anaesthetists wishing to ‘brushup’ on some forgotten anatomical detail.Nurses, operating theatre practitionersand other healthcare professionals willalso find this book of use when gaining apractical understanding of appliedanatomy.
Finally, all errors and omissions are myresponsibility, and any comments andadvice for improvement will be gratefullyaccepted.
Andreas ErdmannJune 2001
Preface
RespiratorySystem
DESCRIPTION
The mouth extends from the lips(anterior) to the isthmus of the fauces(posterior). There are two sections:
Vestibule – slit-like cavity betweenthe cheeks/lips and gingivae/teethOral cavity – from the teeth to theoropharyngeal isthmus
RELATIONS
Roof – hard and soft palateFloor – tongue and reflection of the gum
mucous membranePosterior – isthmus separates the oral
cavity from the oropharynx
POINTS OF INTEREST
● Papilla – a papilla for the opening ofthe parotid duct is present on thecheek opposite the upper secondmolar tooth
● Midline frenulum – under the tongue,has two papillae for the submandibularduct openings and the sublingual fold(of mucous membrane) for numeroustiny sublingual duct openings
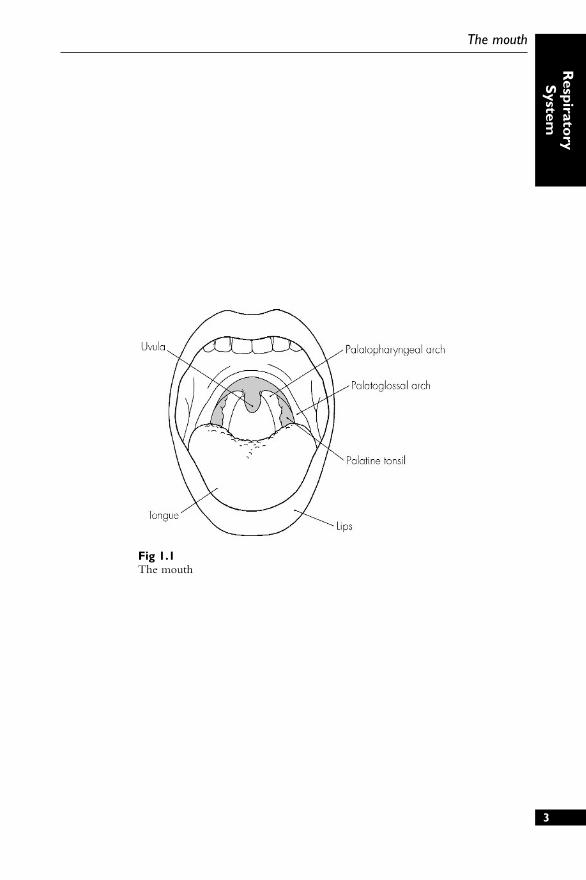
● Isthmus – contains three structures:the palatoglossal folds (anterior), thepalatine tonsils (middle) and thepalatopharyngeal folds (posterior). It isbounded by the soft palate above
● Hard palate – created by the maxilla(palatine process) anteriorly andpalatine bone posteriorly
● Soft palate – a suspended ‘curtain’from the hard palate with a midlineuvula; a fibrous palatine aponeurosisforms the skeleton of the soft palate
VASCULAR SUPPLY
1. Vestibule – facial artery (via superiorand inferior labial branches)
2. Teeth – maxillary artery (via superiorand inferior alveolar branches)
3. Tongue – lingual artery (venous vialingual vein into internal jugular)
4. Palate – mixed supply from facial,maxillary and ascending pharyngealarteries
NERVE SUPPLY
● Vestibule:● Sensory from the branches of the
trigeminal nerve (V2 and V3)● Motor from the facial nerve (VII)
● Tongue:● Taste – anterior two-thirds via the
facial nerve (VII via chordatympani), posterior one-third viathe glossopharyngeal nerve (IX)
● Motor from the hypoglossal nerve(XII)
● Palate:● Sensory and motor from the
trigeminal nerve (V2)● Taste from the facial nerve
2
1 The mouth
3
The mouth
Respirato
ryS
ystem
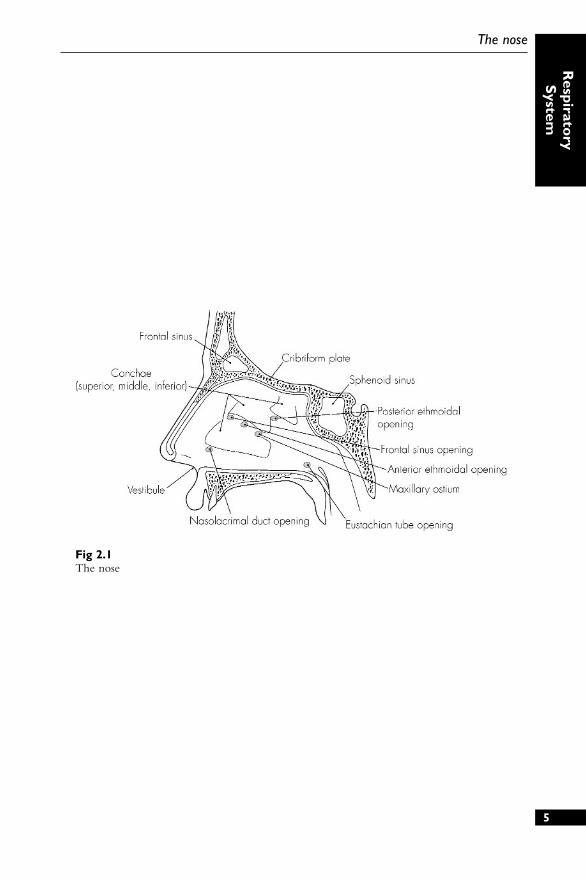
Fig 1.1The mouth
DESCRIPTION
A pyramidal structure of bone, cartilageand the nasal cavities. A midline nasalseptum divides the nasal cavity into twoseparate areas, which open anteriorly viathe nares and posteriorly via the choanae.
RELATIONS
Roof – arch-like, nasal cartilages andnasal bones anteriorly, cribriform plate(of ethmoid) in the middle, andsphenoid and clivus (occipital) bonesposteriorly
Floor – horizontal plate of the palatinebone, palatine process of the maxilla
Medial wall – nasal septum (cartilage andethmoid/vomer)
Lateral wall – bony framework(ethmoid/maxilla/palatine bone) andbony conchae (superior, middle andinferior)
POINTS OF INTEREST
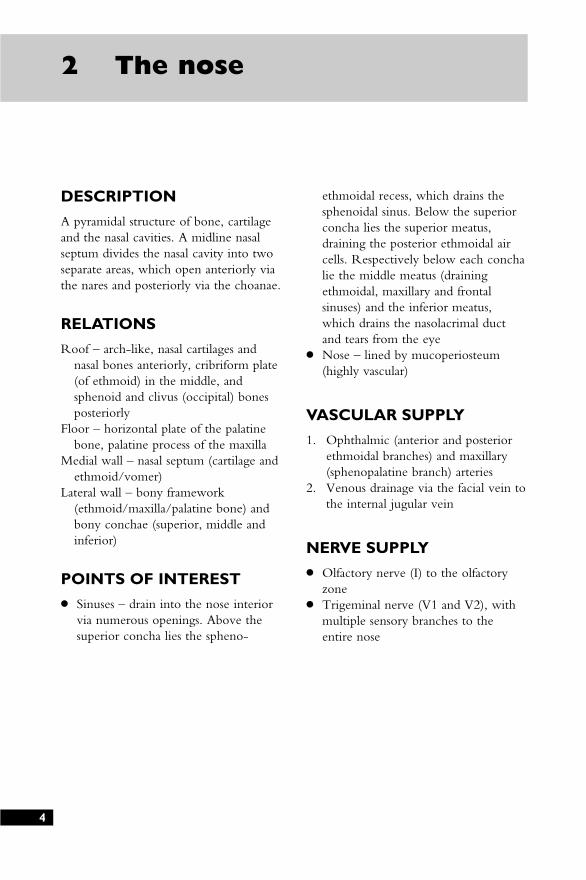
● Sinuses – drain into the nose interiorvia numerous openings. Above thesuperior concha lies the spheno-
ethmoidal recess, which drains thesphenoidal sinus. Below the superiorconcha lies the superior meatus,draining the posterior ethmoidal aircells. Respectively below each conchalie the middle meatus (drainingethmoidal, maxillary and frontalsinuses) and the inferior meatus,which drains the nasolacrimal ductand tears from the eye
● Nose – lined by mucoperiosteum(highly vascular)
VASCULAR SUPPLY
1. Ophthalmic (anterior and posteriorethmoidal branches) and maxillary(sphenopalatine branch) arteries
2. Venous drainage via the facial vein tothe internal jugular vein
NERVE SUPPLY
● Olfactory nerve (I) to the olfactoryzone
● Trigeminal nerve (V1 and V2), withmultiple sensory branches to theentire nose
4
2 The nose
5
The nose
Respirato
ryS
ystem
Fig 2.1The nose
DESCRIPTION
A midline muscular tube that provides acommon pathway for the ingestion offood and for respiration. It arises fromthe base of skull and ends at C6. It isdivided into three sections: naso-, oro-and laryngopharynx. The wall has fourlayers: mucosa, submucosa (tough fascia),muscular and loose connective tissue.
RELATIONS
Anterior – nose and mouthPosterior – retropharyngeal space,
prevertebral fascia and upper sixcervical vertebrae
Superior – sphenoid (body) and occipital(basilar region) bones
Inferior – becomes continuous with theoesophagus
POINTS OF INTEREST
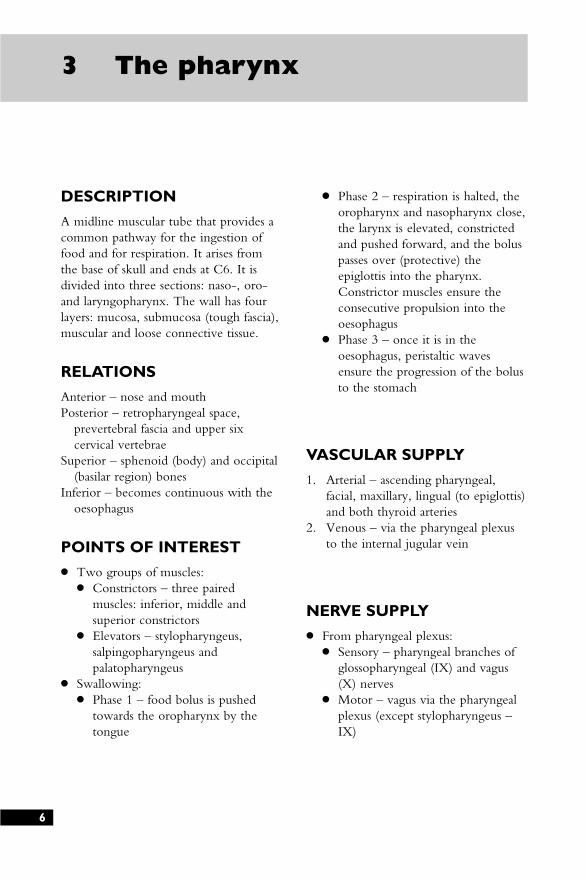
● Two groups of muscles:● Constrictors – three paired
muscles: inferior, middle andsuperior constrictors
● Elevators – stylopharyngeus,salpingopharyngeus andpalatopharyngeus
● Swallowing:● Phase 1 – food bolus is pushed
towards the oropharynx by thetongue
● Phase 2 – respiration is halted, theoropharynx and nasopharynx close,the larynx is elevated, constrictedand pushed forward, and the boluspasses over (protective) theepiglottis into the pharynx.Constrictor muscles ensure theconsecutive propulsion into theoesophagus
● Phase 3 – once it is in theoesophagus, peristaltic wavesensure the progression of the bolusto the stomach
VASCULAR SUPPLY
1. Arterial – ascending pharyngeal,facial, maxillary, lingual (to epiglottis)and both thyroid arteries
2. Venous – via the pharyngeal plexusto the internal jugular vein
NERVE SUPPLY
● From pharyngeal plexus:● Sensory – pharyngeal branches of
glossopharyngeal (IX) and vagus(X) nerves
● Motor – vagus via the pharyngealplexus (except stylopharyngeus –IX)
6
3 The pharynx
7
The pharynx
Respirato
ryS
ystem
Fig 3.1The pharynx

DESCRIPTION
The larynx forms a functional protectivesphincter of the respiratory tract as wellas containing the vocal apparatus. Itconsists of a complex arrangement ofmuscles, cartilage, membranes andligaments. It extends from C3 to C6 inthe midline (adult).
RELATIONS
Anterior – superficial structure, iscovered by the fascia (deep andsuperficial), platysma and skin
Posterior – pharynx, prevertebral musclesand cervical vertebrae
Superior – pharynxInferior – becomes continuous with the
trachea
STRUCTURE
1. Hyoid bone (at C3) – not strictly partof the larynx but firmly attachedabove it
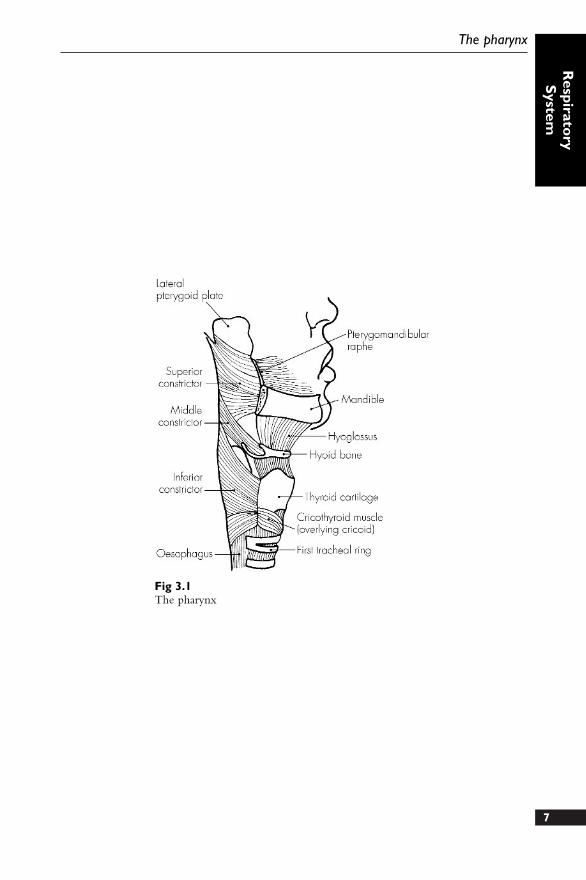
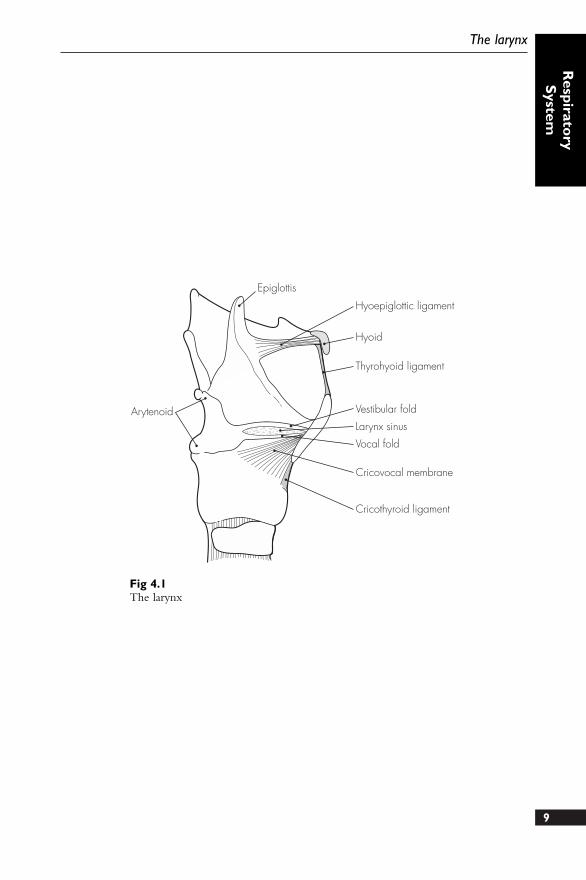
2. Cartilages (nine) – three unpaired andsix paired:● Epiglottis (elastic) – ‘leaf’-shaped;
the lower, narrower end isattached to the thyroid cartilage bythe thyro-epiglottic ligament, andthe upper broader end is free toproject superiorly
● Thyroid cartilage (hyaline) – like a‘shield’. It is the largest of thelaryngeal cartilages and a midlinestructure. Upper (at C4) andlower (at C5) borders carry cornua(horns) posteriorly – inferior
cornu also has a facet forarticulation with the cricoidcartilage
● Cricoid cartilage (hyaline) –‘signet ring’-shaped and situated atthe C6 level. It articulates on itslateral border with the thyroidcornua, and on its upper borderwith the arytenoid cartilages(paired)
● Arytenoid cartilages (paired) –pyramidal in shape, each with alateral muscular process (forinsertion of both crico-arytenoidmuscles) and an anterior vocalprocess (being the posteriorattachment of the vocal ligament)
● Corniculate cartilages (paired) andcuneiform cartilages (paired) –these provide attachments forsome intrinsic laryngeal musclesand are both found within thearyepiglottic folds (the fibro-elasticmembrane between the epiglottisand arytenoids – lower border ofwhich is free and forms thevestibular ligament or false cord)
3. Ligaments – four extrinsic and minorintrinsic (small synovial capsules):● Thyrohyoid membrane – between
the upper border of the thyroidand the hyoid bone. Strengthenedanteriorly and laterally
● Hyo-epiglottic ligament –connects the hyoid bone to thelower part of the epiglottis
● Cricothyroid ligament – betweenthe thyroid above and the cricoidbelow, the preferred site forcricothyrotomy8
4 The larynx
9
The larynx
Respirato
ryS
ystem
Epiglottis
Hyoepiglottic ligament
Hyoid
Thyrohyoid ligament
Vestibular fold
Larynx sinus
Vocal fold
Cricovocal membrane
Cricothyroid ligament
Arytenoid
Fig 4.1The larynx
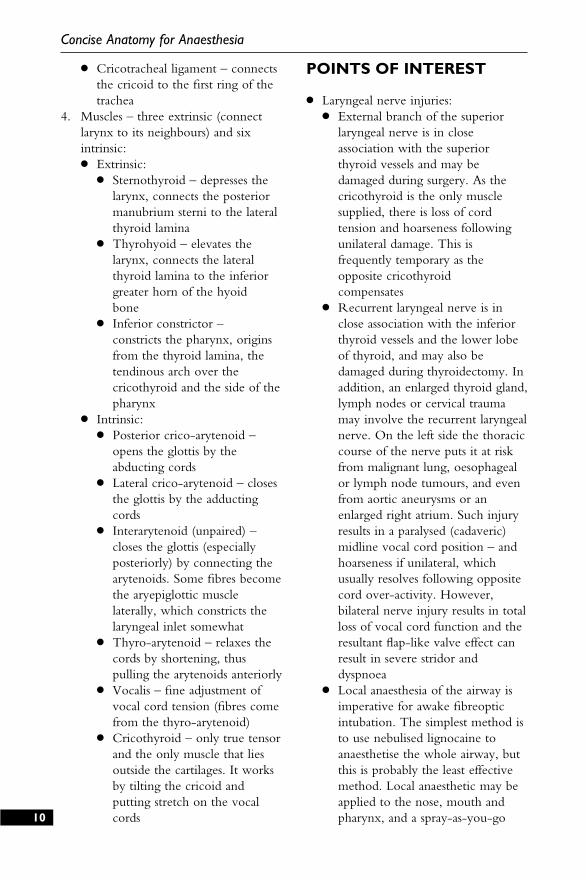
● Cricotracheal ligament – connectsthe cricoid to the first ring of thetrachea
4. Muscles – three extrinsic (connectlarynx to its neighbours) and sixintrinsic:● Extrinsic:
● Sternothyroid – depresses thelarynx, connects the posteriormanubrium sterni to the lateralthyroid lamina
● Thyrohyoid – elevates thelarynx, connects the lateralthyroid lamina to the inferiorgreater horn of the hyoid bone
● Inferior constrictor –constricts the pharynx, originsfrom the thyroid lamina, thetendinous arch over thecricothyroid and the side of thepharynx
● Intrinsic:● Posterior crico-arytenoid –
opens the glottis by theabducting cords
● Lateral crico-arytenoid – closesthe glottis by the adductingcords
● Interarytenoid (unpaired) –closes the glottis (especiallyposteriorly) by connecting thearytenoids. Some fibres becomethe aryepiglottic musclelaterally, which constricts thelaryngeal inlet somewhat
● Thyro-arytenoid – relaxes thecords by shortening, thuspulling the arytenoids anteriorly
● Vocalis – fine adjustment ofvocal cord tension (fibres comefrom the thyro-arytenoid)
● Cricothyroid – only true tensorand the only muscle that liesoutside the cartilages. It worksby tilting the cricoid andputting stretch on the vocalcords
POINTS OF INTEREST
● Laryngeal nerve injuries:● External branch of the superior
laryngeal nerve is in closeassociation with the superiorthyroid vessels and may bedamaged during surgery. As thecricothyroid is the only musclesupplied, there is loss of cordtension and hoarseness followingunilateral damage. This isfrequently temporary as theopposite cricothyroid compensates
● Recurrent laryngeal nerve is inclose association with the inferiorthyroid vessels and the lower lobeof thyroid, and may also bedamaged during thyroidectomy. Inaddition, an enlarged thyroid gland,lymph nodes or cervical traumamay involve the recurrent laryngealnerve. On the left side the thoraciccourse of the nerve puts it at riskfrom malignant lung, oesophagealor lymph node tumours, and evenfrom aortic aneurysms or anenlarged right atrium. Such injuryresults in a paralysed (cadaveric)midline vocal cord position – andhoarseness if unilateral, whichusually resolves following oppositecord over-activity. However,bilateral nerve injury results in totalloss of vocal cord function and theresultant flap-like valve effect canresult in severe stridor anddyspnoea
● Local anaesthesia of the airway isimperative for awake fibreopticintubation. The simplest method isto use nebulised lignocaine toanaesthetise the whole airway, butthis is probably the least effectivemethod. Local anaesthetic may beapplied to the nose, mouth andpharynx, and a spray-as-you-go10
Concise Anatomy for Anaesthesia
11
The larynx
Respirato
ryS
ystem
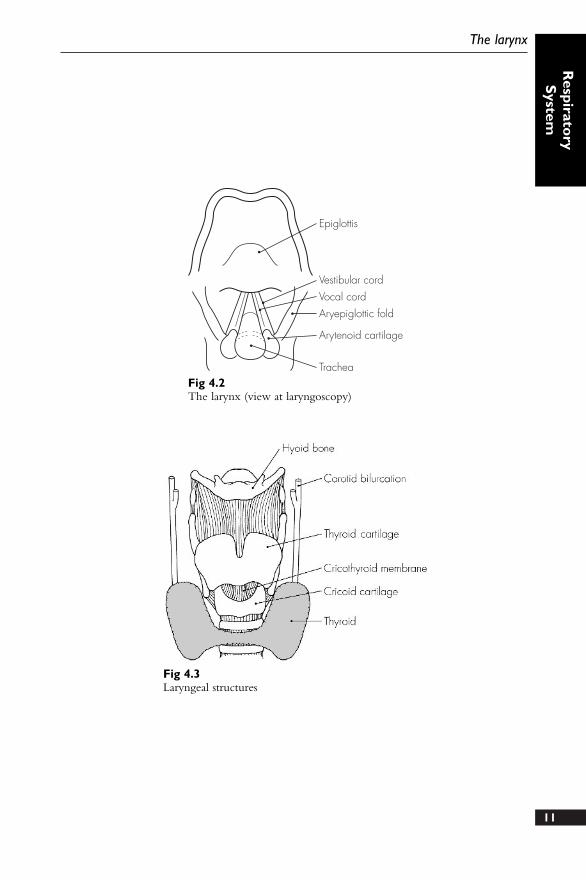
Epiglottis
Vestibular cordVocal cordAryepiglottic fold
Arytenoid cartilage
TracheaFig 4.2The larynx (view at laryngoscopy)
Fig 4.3Laryngeal structures
12
Concise Anatomy for Anaesthesia
technique is used (under directvision) for the laryngeal structures.This can be supplemented by acricothyroid membrane puncturewith an intratracheal spray of localanaesthetic. Individual blockade ofthe external branch of the superiorlaryngeal nerve (at the greater hornof the hyoid) and of its internalbranch (in the piriform fossa) hasbeen arguably superseded by theprior methods
VASCULAR SUPPLY
1. Arterial:● Superior laryngeal (from superior
thyroid artery) – accompanies theinternal branch of the superiorlaryngeal nerve
● Inferior laryngeal (from inferiorthyroid artery) – accompanies therecurrent laryngeal nerve
2. Venous – into the correspondingsuperior and inferior thyroid veins
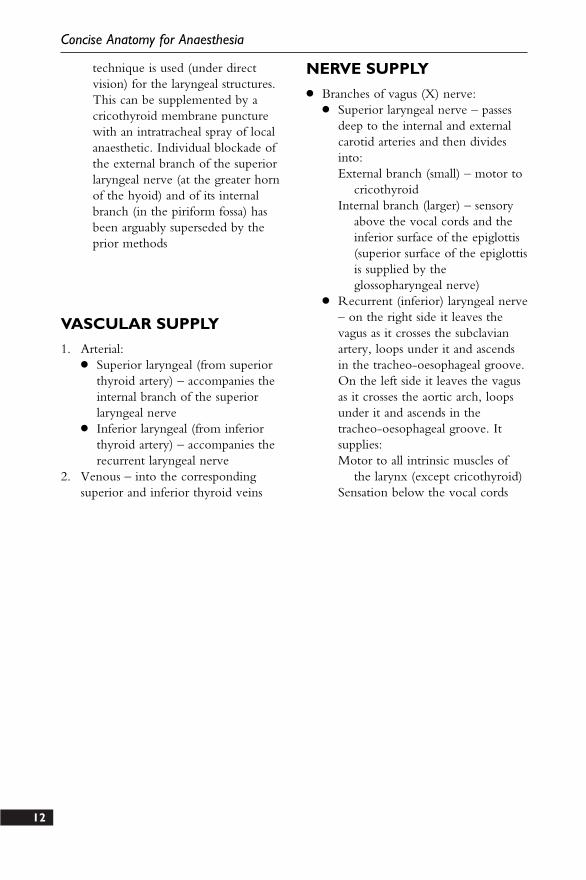
NERVE SUPPLY
● Branches of vagus (X) nerve:● Superior laryngeal nerve – passes
deep to the internal and externalcarotid arteries and then dividesinto:External branch (small) – motor to
cricothyroidInternal branch (larger) – sensory
above the vocal cords and theinferior surface of the epiglottis(superior surface of the epiglottisis supplied by theglossopharyngeal nerve)
● Recurrent (inferior) laryngeal nerve– on the right side it leaves thevagus as it crosses the subclavianartery, loops under it and ascendsin the tracheo-oesophageal groove.On the left side it leaves the vagusas it crosses the aortic arch, loopsunder it and ascends in thetracheo-oesophageal groove. Itsupplies:Motor to all intrinsic muscles of
the larynx (except cricothyroid)Sensation below the vocal cords
Vagus nerve
Superior laryngealnerve
Internal carotidartery
Subclavian artery
Recurrentlaryngeal nerve
External carotid artery
Internal laryngeal nerve
Thyrohyoid muscle
External laryngeal nerve
Cricothyroid muscle
13
The larynx
Respirato
ryS
ystem
Fig 4.4Nerve supply of the larynx
DESCRIPTION
It is a roughly midline structure thatextends from C6 (at the lower edge ofthe cricoid cartilage) to the carinalbifurcation at T4. It is 15 cm long in theadult and has up to 20 C-shapedcartilages joined by fibro-elastic tissuethat is deficient posteriorly. The trachealismuscle closes the posterior border.
RELATIONS
In the neck:Anterior – skin, superficial and deep
fascia, thyroid isthmus (over secondto fourth rings), sternothyroid andsternohyoid muscles (lower neck)and the anterior jugular veincommunications and thyroidea imaartery (also lower neck)
Posterior – oesophagus and recurrentlaryngeal nerves
Laterally – lateral lobes of the thyroidand carotid sheath (with internaljugular vein, common carotid arteryand vagus nerve)
In the thorax:Anterior (in caudad direction) –
inferior thyroid veins, sternothyroidorigins, thymus remnants,brachiocephalic artery, left commoncarotid artery and aortic arch. Thepulmonary bifurcation lies behindthe carina
Posterior – oesophagus and leftrecurrent laryngeal nerve
Laterally:● Right – pleura, azygos vein and
right vagus nerve
● Left – pleura, left commoncarotid, left subclavian artery,aortic arch and left vagus
POINTS OF INTEREST
● Tracheostomy:● Positioning – all important. With
full extension of the head and neckit is achieved by using a sandbagunder the patient’s shoulders.Keeping strictly to the midlineminimises the risk of major vesseldamage. During formaltracheostomy the skin incision isdeepened by blunt dissection, thethyroid isthmus is retracted ordivided, and a window is openedin the trachea between the secondand fourth rings. Higher placementmay result in an increasedincidence of tracheal stenosis. Thelargest tracheostomy tube for acomfortable fit is then inserted
● Percutaneous techniques – requireless dissection, but the sameprinciple of keeping strictly to themidline also applies
VASCULAR SUPPLY
1. Arterial – inferior thyroid arteries2. Venous – inferior thyroid veins
NERVE SUPPLY
● Recurrent laryngeal branch of thevagus and sympathetic branches of themiddle cervical ganglion14
5 The trachea
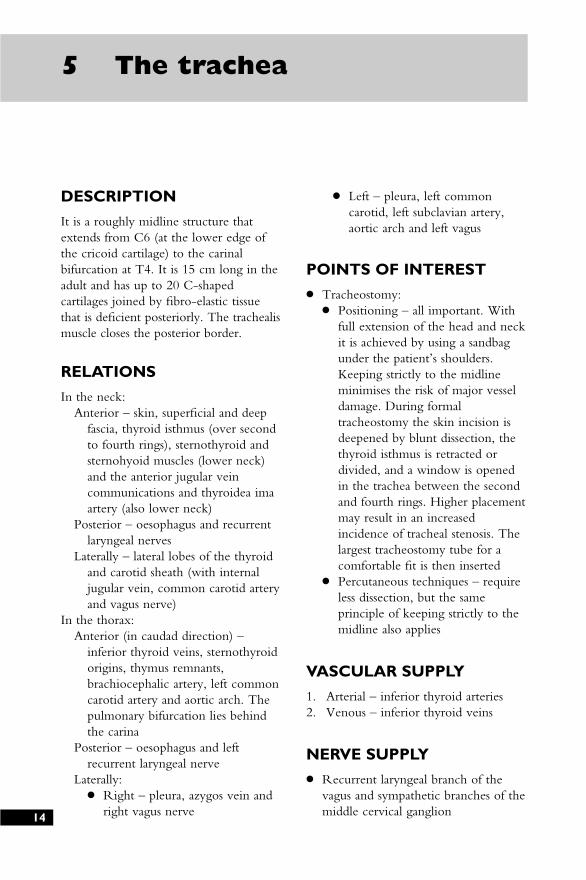
Pretracheal fascia(contains trachea,thyroid, oesophagus,recurrent nerve)
Sympatheticchain
Body of C6
Anterior jugular vein
Sternomastoid
Externaljugularvein
Carotid sheath(containing internal jugular vein,
common carotid artery and vagus)
15
The trachea
Respirato
ryS
ystem
Fig 5.1The trachea (cross-section)
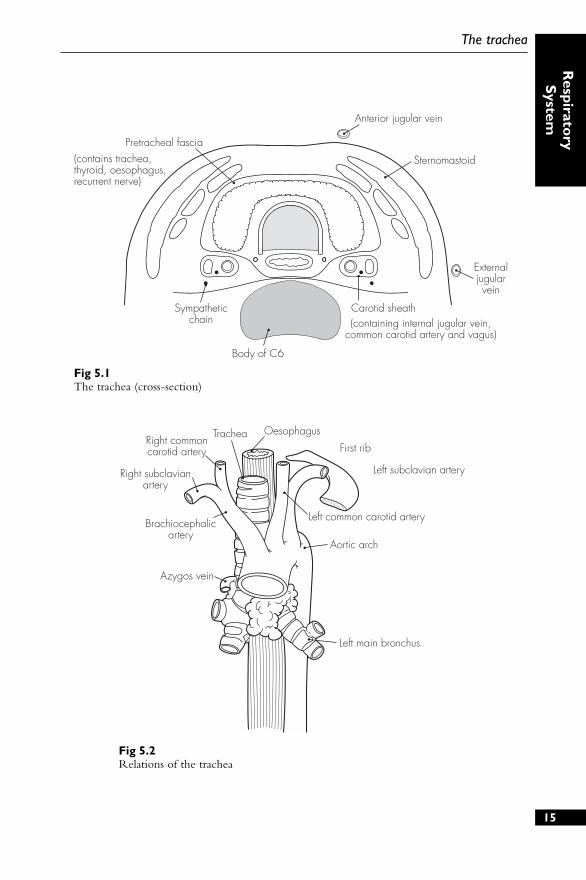
OesophagusTracheaRight commoncarotid artery
Right subclavianartery
Brachiocephalicartery
Azygos vein
First rib
Left subclavian artery
Left common carotid artery
Aortic arch
Left main bronchus
Fig 5.2Relations of the trachea
16
6 The bronchi andbronchial tree
DESCRIPTION
The trachea bifurcates at the T4 levelinto the right and left main bronchi. Thelast tracheal ring is wider and larger, andforms a ridge called the carina.
The right main bronchus is shorter,wider and more vertical than the left(25°). After 2.5 cm, it gives off the rightupper bronchus. The left main bronchusis more angled (45°) and is 5 cm long.
RELATIONS
Right main bronchus – passes under theazygos vein arch and lies above andthen behind the right pulmonaryartery
Left main bronchus – passes under theaortic arch, in front of the oesophagus,thoracic duct and descending aorta,and lies below and then behind the leftpulmonary artery
STRUCTURE
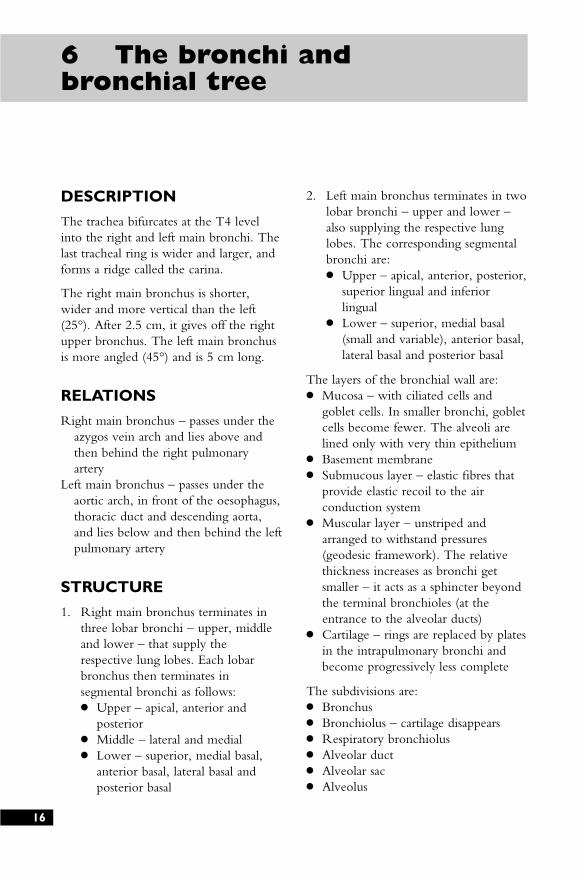
1. Right main bronchus terminates inthree lobar bronchi – upper, middleand lower – that supply therespective lung lobes. Each lobarbronchus then terminates insegmental bronchi as follows:● Upper – apical, anterior and
posterior● Middle – lateral and medial● Lower – superior, medial basal,
anterior basal, lateral basal andposterior basal
2. Left main bronchus terminates in twolobar bronchi – upper and lower –also supplying the respective lunglobes. The corresponding segmentalbronchi are:● Upper – apical, anterior, posterior,
superior lingual and inferiorlingual
● Lower – superior, medial basal(small and variable), anterior basal,lateral basal and posterior basal
The layers of the bronchial wall are:● Mucosa – with ciliated cells and
goblet cells. In smaller bronchi, gobletcells become fewer. The alveoli arelined only with very thin epithelium
● Basement membrane● Submucous layer – elastic fibres that
provide elastic recoil to the airconduction system
● Muscular layer – unstriped andarranged to withstand pressures(geodesic framework). The relativethickness increases as bronchi getsmaller – it acts as a sphincter beyondthe terminal bronchioles (at theentrance to the alveolar ducts)
● Cartilage – rings are replaced by platesin the intrapulmonary bronchi andbecome progressively less complete
The subdivisions are:● Bronchus● Bronchiolus – cartilage disappears● Respiratory bronchiolus● Alveolar duct● Alveolar sac● Alveolus
17
The bronchi and bronchial tree
Respirato
ryS
ystem
Fig 6.1The bronchial tree

18
7 The pleura andmediastinum
DESCRIPTION
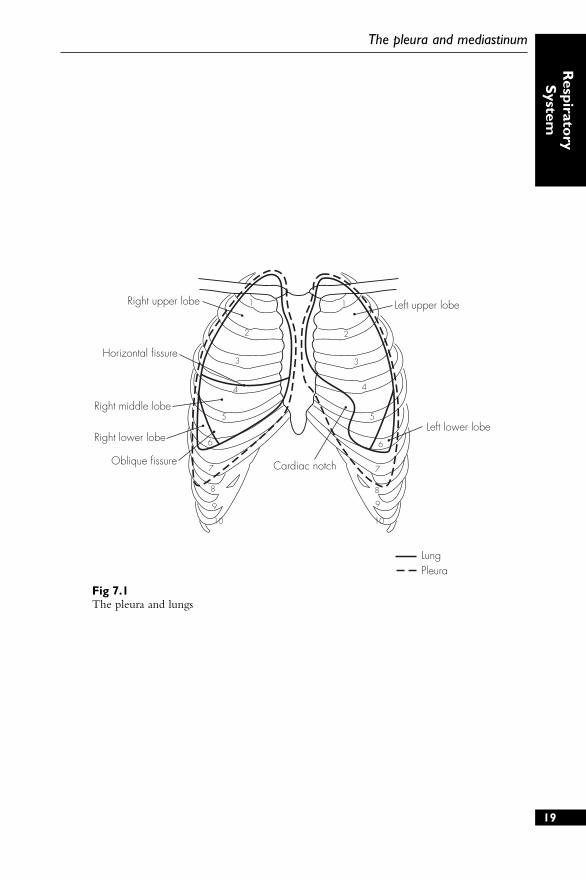
The lungs are enveloped in a twin-walled serous sac – two layers of thepleura – that meet at the hilum to formthe pulmonary ligament. A potentialspace exists between the two pleurallayers (visceral and parietal), whichcontains a thin film of serous fluid.
The mediastinum is the space betweenthe two pleural sacs and is divided intofour regions by the pericardium:
Superior (below thoracic inlet)Middle (contains pericardial contents)Anterior (behind sternum)Posterior (above diaphragm)
POINTS OF INTEREST
● Lines of pleural reflection (surfacemarkings):● Apex – lies 4 cm above the clavicle● Behind the sternoclavicular joint● Behind the sternum at the second
costochondral junction● On the left – lateral sternal edge at
the fourth cartilage● On the right – down to the
costoxiphoid angle● Eighth rib – mid-clavicular line● Tenth rib – mid-axillary line● Twelfth rib – posterior to the
costovertebral angle
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Horizontal fissure
Right middle lobe
Right lower lobe
Right upper lobe
Oblique fissure Cardiac notch
Left upper lobe
Left lower lobe
LungPleura
19
The pleura and mediastinum
Respirato
ryS
ystem
Fig 7.1The pleura and lungs
20
8 The lungs
DESCRIPTION
The lungs are enclosed within the pleuralsacs and separated by the mediastinalstructures. Each lung has an apex, base,hilum, three surfaces and three borders.
RELATIONS
Apex – extends into the root of theneck. The suprapleural membrane andpleural cupola are superior and thesubclavian artery leaves a groove onthe mediastinal surface of the lung
Base – concave in shape. The right lungis more concave (a higher diaphragmon the right due to the liver’s position)
Hilum – structures enter and leave thelung. It is formed mainly by thebronchi, pulmonary arteries, pulmonaryveins, bronchial arteries and veins,nerve plexuses, and lymph nodes:● On the right – superior vena cava
and right atrium lie anterior to thehilum, and the azygos vein archesover it
● On the left – thoracic aorta isposterior to the hilum; the aorticarch is superior
● On both sides – phrenic nerve,anterior nerve plexuses and minorvessels lie anteriorly, the vagusnerves and posterior nerve plexuseslie posteriorly
STRUCTURE
1. Lungs are divided into lobes – threeon the right and two on the left. Eachlobe is subdivided into triangularbronchopulmonary segments that
correspond to the individualsegmental bronchi (see above).
2. Right lung has two fissures:● Oblique – separates the middle
and lower lobes (follows the linefrom the second vertebral spine tothe sixth costochondral junction)
● Horizontal (transverse) – separatesthe upper and middle lobes(follows the line from the fourthcostochondral junction to join theoblique fissure in the axillary line)
3. Left lung has only one fissure –oblique fissure separating the upperand lower lobes
POINTS OF INTEREST
● Bronchoscopic anatomy – tracheaappears as a glistening tube structurewith a red mucosa and regularconcentric white tracheal rings. Thecarina is seen as a sharp ridge and liesslightly to the left of the midline:● Right main bronchus is wider and
easier to enter:Upper lobe bronchus – 2.5 cm
from the carina (three o’clockposition)
Middle lobe bronchus – 4.5 cmfrom the carina (12 o’clock)
Lower lobe bronchus – 4.5 cm (sixo’clock)
● Left main bronchus is longer (at 5cm) and narrower:Upper lobe bronchus – 5 cm (nine
o’clock) with lingular branchcentrally at 5.5 cm
Lower lobe bronchus – 6 cm (sixo’clock)
VASCULAR SUPPLY
1. Pulmonary artery – provides acapillary network for the exchange ofthe respiratory gases. The pulmonaryartery and divisions are concernedsolely with alveolar gas exchange andclosely follow the bronchial treedivisions. The capillaries in turn feedinto the pulmonary veins, which tendto run between the lung segments.The two main pulmonary veins drainseparately into the left atrium
2. Bronchial arteries – provide theblood supply to the lungs, bronchi,pleura and lymph nodes. They supplythe actual stroma of the lung. Thereare usually three (variable): one forthe right lung and two for the left.They originate from the descendingaorta (on the left) and variably fromthe aorta, an intercostal, internalthoracic or right subclavian artery (onthe right). There are two bronchialveins on each side draining into theazygos (right) or hemi-azygos (left)veins. Together with the Thebesianveins of the heart, the bronchialblood flow makes up the‘physiological shunt’
NERVE SUPPLY
● Tracheobronchial tree and lung:● Sensory – vagus (X), recurrent
laryngeal● Motor – vagus (X)
(bronchoconstriction) andsympathetic fibres from T2 to T4(bronchodilation and minorvasoconstriction)
● Pleura:● Parietal sensory – phrenic and
intercostal nerves● Visceral sensory – autonomic
supply
LYMPHATIC DRAINAGE
1. Superficial plexus drains visceralpleura
2. Deep plexus drains bronchi (as far asalveolar ducts)
Both drain into the bronchopulmonarylymph nodes – then into thetracheobronchial nodes – then into theright and left bronchomediastinal trunks.Variable termination – either directlyinto great veins of neck, or into thoracicduct (left) and right lymph duct (right).
21
The lungs
Respirato
ryS
ystem
22
9 The diaphragm
DESCRIPTION
The diaphragm separates the thoracic andabdominal cavities and is the mainmuscle of respiration. It consists of acentral tendinous portion and aperipheral muscular area. It is dome-shaped in structure and reaches a higherlevel on the right (fifth rib) than on theleft (fifth intercostal space) during end-expiration.
RELATIONS
Central trefoil tendon – blends with thefibrous pericardium above
Muscle – has a complex origin:● Costal origin – from the tips of the
last six costal cartilages● Xiphoid origin – from the two
small attachments to the posteriorsurface
● Arcuate ligaments (three):● Medial – psoas fascial thickening● Lateral – quadratus lumborum
fascial thickening● Median – fibrous arch between
two crura● Crura:
● Left – from the first and secondlumbar vertebral bodies
● Right – from the first, secondand third lumbar vertebralbodies
POINTS OF INTEREST
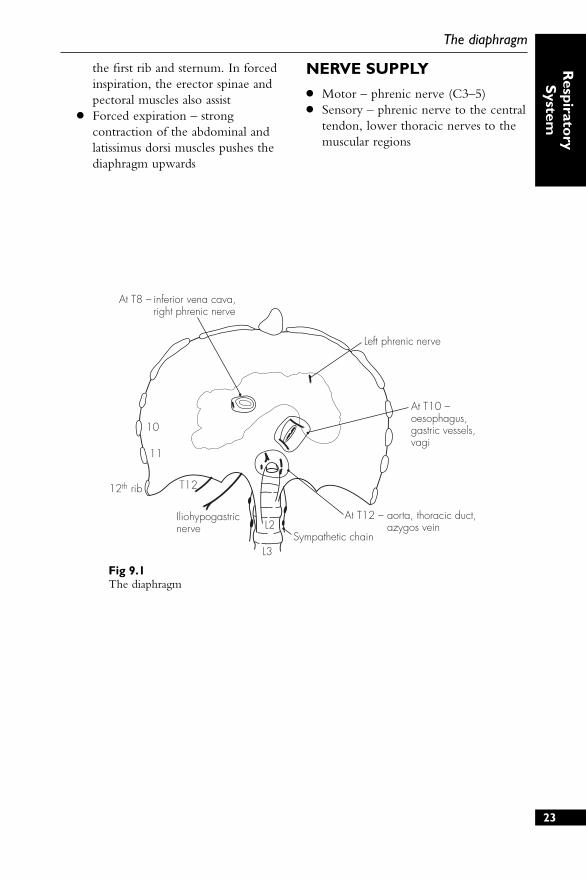
● Three major openings allow for thepassage of structures between thethorax and abdomen:
● At T8 – inferior vena cava(sometimes right phrenic nerve)
● At T10 – oesophagus, vagi, and leftgastric artery and vein
● At T12 – aorta, thoracic duct andazygos vein
● Further openings transmit:● Superior epigastric vessels –
between the costal and xiphoidorigins
● Lymphatic vessels – between thecostal and xiphoid origins
● Sympathetic trunk – behind themedial arcuate ligament
● Right phrenic nerve – pierces thecentral tendon close to the inferiorvena caval opening
● Left phrenic nerve – pierces musclejust lateral to the pericardialattachment
● Respiration:● Diaphragm – moves downwards
during inspiration and thus enlargesthe thoracic cavity. On expirationit relaxes (and the elastic recoil ofthe chest wall causes expiration).During quiet breathing thediaphragm is the dominantfunctioning muscle on inspiration
● Intercostal muscles – also known tocontract on inspiration. Thisapproximates the ribs, and elevatesand everts the rib cage increasingthe intrathoracic volume.Contraction is also seen on forcedexpiration (this is presumed to aidrib fixation)
● Scalene muscles – play a role ininspiration, especially whenrespiration is deeper. They elevate
At T8 – inferior vena cava, right phrenic nerve
T12
Iliohypogastricnerve L2
L3Sympathetic chain
At T12 – aorta, thoracic duct, azygos vein
At T10 –oesophagus,gastric vessels,vagi
Left phrenic nerve
10
11
12th rib
23
The diaphragm
Respirato
ryS
ystem
Fig 9.1The diaphragm
the first rib and sternum. In forcedinspiration, the erector spinae andpectoral muscles also assist
● Forced expiration – strongcontraction of the abdominal andlatissimus dorsi muscles pushes thediaphragm upwards
NERVE SUPPLY
● Motor – phrenic nerve (C3–5)● Sensory – phrenic nerve to the central
tendon, lower thoracic nerves to themuscular regions

24
Sample questions –respiratory system
1. Outline your technique forpercutaneous tracheostomy withparticular reference to the anatomyinvolved. List the possiblecomplications of this procedure.
2. Draw a simple diagram of the viewof the larynx at direct laryngoscopy.
3. What are the effects of damage to thenerve supply of the larynx?
4. Make a simple drawing, with labels,to show the trachea and the main andsegmental bronchi.
5. How may the airway be anaesthetisedfor awake fibreoptic intubation?
6. How may nerve blockade be used toprovide pain relief following chestwall trauma?
7. Describe the view seen duringbronchoscopic examination.
8. Give a brief account, with a simplediagram, of the anatomy of thediaphragm.
CardiovascularSystem
DESCRIPTION
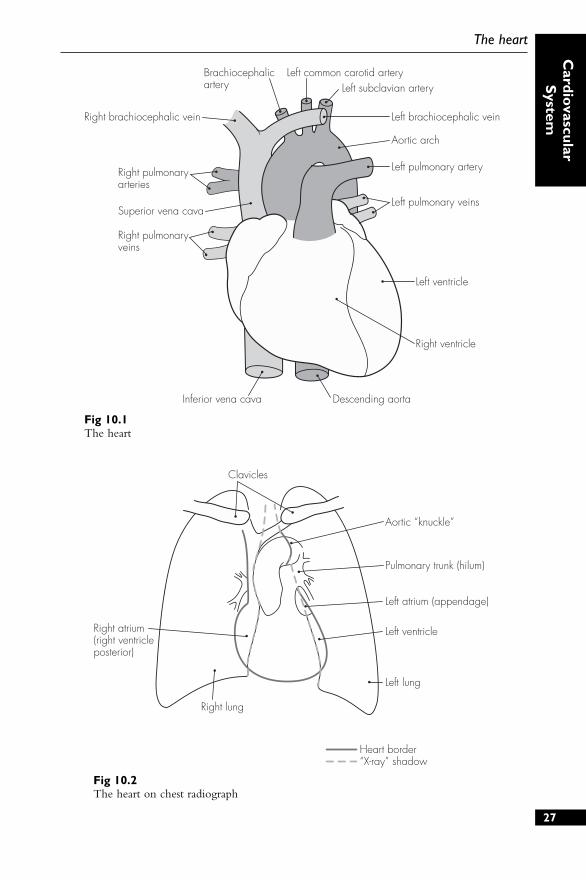
The heart is a four-chambered, conical,muscular pump in the middlemediastinum. Its borders are:
Right border – right atriumLeft border – left auricular appendage
and left ventricleAnterior surface – right ventricle
predominantlyDiaphragmatic surface – right and left
ventricles (right atrium)Posterior surface – left atrium (right
atrium)
The surface markings follow aquadrilateral shape (distances frommidline): third right costal cartilage (2cm), second left costal cartilage (3 cm),fifth left intercostal space (7 cm) andsixth right costal cartilage (2 cm).
STRUCTURE
The heart consists of four chambers:
1. Right atrium – receivesdeoxygenated blood from the bodyvia the venae cavae (inferior andsuperior). The outflow of bloodoccurs through the tricuspid valveinto the right ventricle. The sino-atrial node is situated in the upperpart of the right atrium, and theatrioventricular node lies near thebase of the tricuspid valve
2. Right ventricle – receives blood fromthe right atrium and expels it throughthe pulmonary valve and trunk.Some of the rough internal wall
muscle fibres (trabeculae) specialiseinto papillary muscles, which attachto the tricuspid valve cusps (in asimilar fashion to the mitral valve onthe left side of the heart). Thepulmonary valve is tricuspid and leadsinto the pulmonary trunk
3. Left atrium – receives oxygenatedblood from the lungs via the fourpulmonary veins, which opensuperoposteriorly. The blood thenpasses through the mitral (bicuspid)valve into the left ventricle
4. Left ventricle – thickest-walledchamber that distributes blood to thebody via the aorta. The aortic valve istricuspid – with right, left andposterior cusps. Small sinuses lieabove the cusps that give rise to thetwo coronary arteries – right and leftrespectively
POINTS OF INTEREST
● Conducting system:● Sino-atrial node – in the superior
right atrial wall (near the superiorvena caval opening) and initiatesconduction impulse. The node isin direct contact with the atrialcells and causes a wave ofdepolarisation, resulting incontraction of both atria
● Atrioventricular node – at the baseof the right atrial septal wall (nearthe tricuspid valve) and receivesimpulses from the atrialdepolarisation. There is no directneural route between the twonodes, which allows for a slight26
10 The heart
Brachiocephalicartery
Left common carotid artery
Left brachiocephalic veinRight brachiocephalic vein
Aortic arch
Left pulmonary artery
Left pulmonary veins
Left ventricle
Right ventricle
Descending aortaInferior vena cava
Left subclavian artery
Right pulmonaryveins
Right pulmonaryarteries
Superior vena cava
27
The heart
Cardio
vascularS
ystem
Fig 10.1The heart
Heart border“X-ray” shadow
Right atrium(right ventricleposterior)
Clavicles
Aortic “knuckle”
Pulmonary trunk (hilum)
Left atrium (appendage)
Left ventricle
Left lung
Right lung
Fig 10.2The heart on chest radiograph

delay and prevents simultaneousatrial and ventricular contraction
● Bundle of His – nerve fibre bundle(AV bundle) that receives theelectrical impulse from the AVnode and continues within theinterventricular septum. At the baseit divides into two terminal bundlebranches (right and left). Thesecontinue in the walls of theirrespective ventricles, terminating inPurkinje fibres, which penetratethe muscular walls and initiateventricular contraction
● Pericardium:● Heart is enveloped within a conical
fibroserous sac – the pericardium.The outer layer is attached to thefollowing structures:Adventitia of the great vesselsSternopericardial ligament – to the
posterior sternumCentral tendon of diaphragm –
where it is fused inferiorly● Outer fibrous layer is a tough
fibrous structure with openings toallow the aorta, pulmonary trunkand superior vena cava to passthrough
● Serous pericardium has twocomponents:Outer parietal pericardium – lines
the inner surface of the fibroussac and becomes continuouswith the visceral layer aroundthe great vessels
Inner visceral pericardium – indirect contact with the heartand forms a potential spacebetween the pericardial layers
● During embryological folding,sinuses develop in the pericardium:Transverse sinus (superiorly) –
behind the aorta/pulmonarytrunk and in front of superiorvena cava
Oblique sinus (inferiorly) – behindthe left atrium (bordered by the
inferior vena cava andpulmonary veins)
VASCULAR SUPPLY
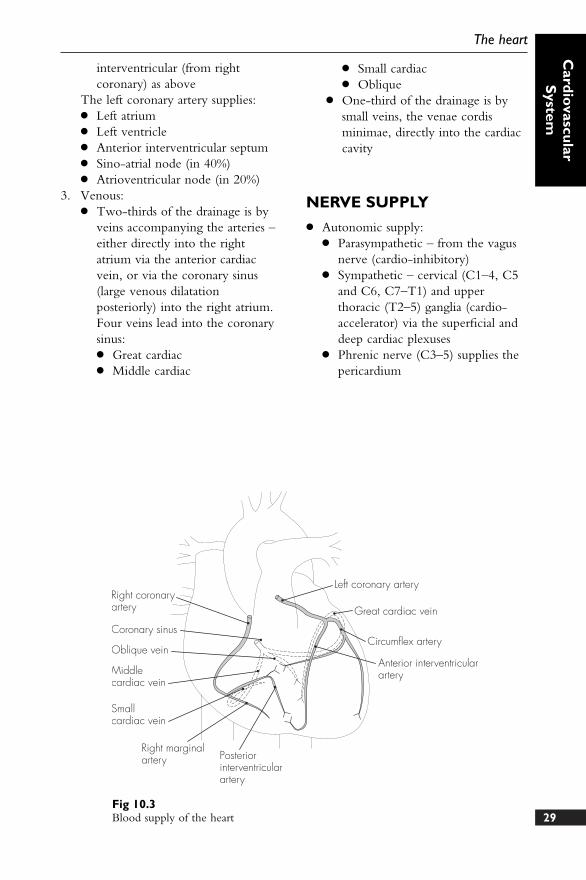
1. Arterial:● Right coronary artery – from the
right aortic sinus (previouslyanterior) and descends betweenthe pulmonary trunk and rightatrium to run in the anterioratrioventricular groove. Inferiorly,it anastomoses with the leftcoronary (circumflex) at theinferior interventricular groove. Inaddition to small atrial andventricular branches, it gives offtwo main branches:
● Right marginal branch – lowerborder of the heart
● Posterior interventricular branch –anastomoses with the anteriorinterventricular branch of the leftcoronary
The right coronary artery supplies:● Right atrium● Part of the left atrium● Right ventricle● Posterior interventricular septum● Sino-atrial node (in 60%)● Atrioventricular node (in 80%)
2. Left coronary artery – from the leftaortic sinus (previously left posterior)and it lies behind and then lateral tothe pulmonary trunk. It also gives offsmall atrial and ventricular branches,and divides immediately into twomain branches:● Circumflex artery – runs laterally
around the left atrioventriculargroove (anastomoses with rightcoronary as above). This also givesoff the left marginal branch
● Anterior interventricular artery(formerly left anterior descending)– runs down the anteriorinterventricular groove toanastomose with the posterior28
Concise Anatomy for Anaesthesia
29
The heart
Cardio
vascularS
ystem
Right coronaryartery
Coronary sinus
Oblique vein
Middlecardiac vein
Smallcardiac vein
Right marginalartery Posterior
interventricularartery
Left coronary artery
Great cardiac vein
Circumflex artery
Anterior interventricularartery
Fig 10.3Blood supply of the heart
interventricular (from rightcoronary) as above
The left coronary artery supplies:● Left atrium● Left ventricle● Anterior interventricular septum● Sino-atrial node (in 40%)● Atrioventricular node (in 20%)
3. Venous:● Two-thirds of the drainage is by
veins accompanying the arteries –either directly into the rightatrium via the anterior cardiacvein, or via the coronary sinus(large venous dilatationposteriorly) into the right atrium.Four veins lead into the coronarysinus:● Great cardiac● Middle cardiac
● Small cardiac● Oblique
● One-third of the drainage is bysmall veins, the venae cordisminimae, directly into the cardiaccavity
NERVE SUPPLY
● Autonomic supply:● Parasympathetic – from the vagus
nerve (cardio-inhibitory)● Sympathetic – cervical (C1–4, C5
and C6, C7–T1) and upperthoracic (T2–5) ganglia (cardio-accelerator) via the superficial anddeep cardiac plexuses
● Phrenic nerve (C3–5) supplies thepericardium
AORTA
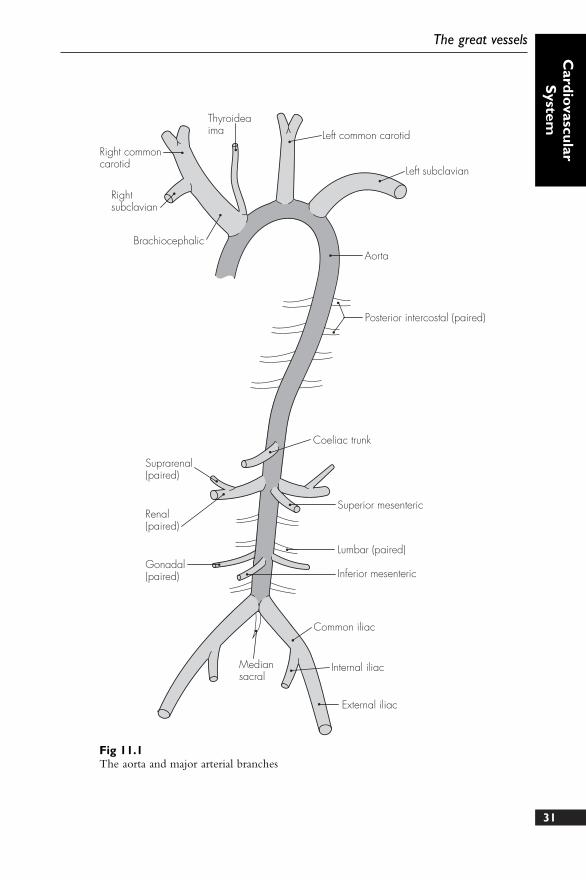
Commences at the aortic valve andterminates at its bifurcation into thecommon iliac arteries (L4 level). Thereare four parts:
1. Ascending – 5 cm long, posterior tosternum. It gives off:● Right coronary artery● Left coronary artery
2. Arch – runs upwards, backwards andto the left. It gives off:● Brachiocephalic, which divides
into:● Right common carotid● Right subclavian
● Left common carotid● Left subclavian● Thyroidea ima (occasionally)
3. Descending thoracic aorta – starts atlevel T4 and runs down to the aorticopening in the diaphragm (T12). Itgives off:● Visceral branches – pericardial,
bronchial, oesophageal,mediastinal and phrenic
● Somatic branches – posteriorintercostals, dorsal, muscular,lateral cutaneous and mammary
4. Abdominal aorta – starts at the aorticopening in the diaphragm and ends atthe common iliac bifurcation. It givesoff:● Lumbar arteries (paired)● Visceral arteries (paired) – inferior
phrenic, suprarenal, renal andgonadal
● Midline (unpaired) arteries:● Celiac trunk – supplies the
foregut (via left gastric,
common hepatic and splenic)● Superior mesenteric – supplies
the midgut (via inferiorpancreaticoduodenal, jejunal,ileal, ileocolic, right and middlecolic)
● Inferior mesenteric – suppliesthe hindgut (via left colic,sigmoid and superior rectal)
GREAT ARTERIES OF THE NECK
1. Brachiocephalic artery – first andlargest branch of the aortic arch. Itusually gives off no branches anddivides into the right commoncarotid and right subclavian behindthe right sternoclavicular joint
2. Right common carotid artery –ascends within the carotid sheath todivide (opposite the upper border ofthe thyroid cartilage, C4) into theinternal and external carotid arteries
3. Right subclavian artery – runs (overthe cervical pleura and lung apex) tothe lateral border of the first rib(grooved) where it becomes the rightaxillary artery. It gives off fivebranches: vertebral, internal thoracic,thyrocervical, costocervical and dorsalscapular
4. Left common carotid artery – secondbranch of the aortic arch and ascendsinitially towards the left and thenbehind the left sternoclavicular joint.It usually has no branches
5. Left subclavian artery – third branchof the aortic arch, and as on the rightside, it grooves the first rib30
11 The great vessels
31
The great vessels
Cardio
vascularS
ystem
Right commoncarotid
Thyroideaima Left common carotid
Left subclavian
Aorta
Posterior intercostal (paired)
Coeliac trunk
Superior mesenteric
Lumbar (paired)
Inferior mesenteric
Common iliac
Internal iliac
External iliac
Mediansacral
Gonadal(paired)
Renal(paired)
Suprarenal(paired)
Rightsubclavian
Brachiocephalic
Fig 11.1The aorta and major arterial branches
posteriorly before terminating at itslateral border to become the leftaxillary artery. It also has fivebranches (see above)
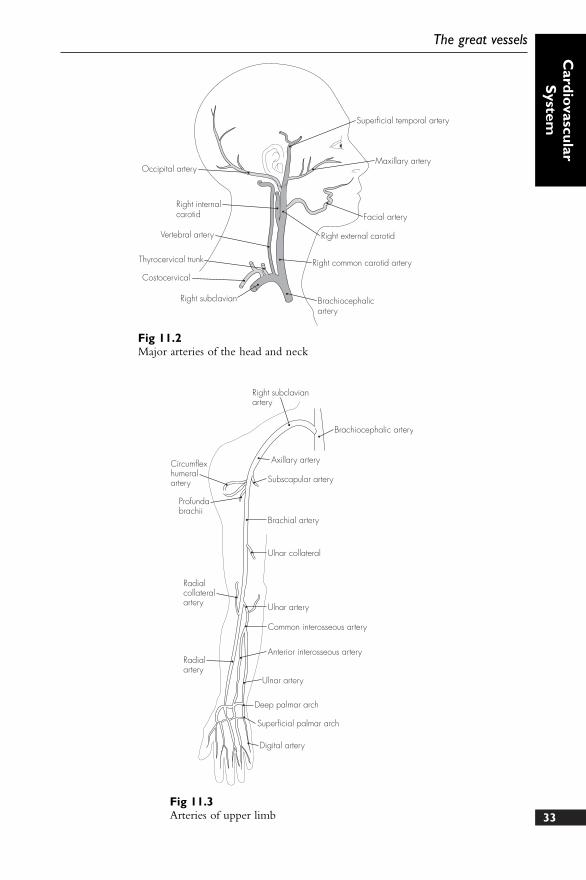
6. External carotid artery – main bloodsupply to the head and neck andgives off six branches beforebifurcating within the parotid gland:● Superior thyroid● Ascending pharyngeal● Lingual● Facial● Occipital● Posterior auricular● Superficial temporal (terminal
branch)● Maxillary (terminal branch)
7. Internal carotid artery – main bloodsupply to the intracranial contentsand lies initially posterior and lateralto the external carotid (beforebecoming medial at C2), shortly afterwhich it enters the skull through thecarotid canal. There are no cervicalbranches, but there are 10 brancheswithin the skull:● Caroticotympanic and pterygoid
(within petrous area)● Cavernous, hypophyseal and
meningeal (within cavernous area)● Ophthalmic● Anterior cerebral● Middle cerebral● Posterior communicating● Anterior choroidal
ARTERIES OF THE LIMBS
Upper limb
1. Axillary artery – continuation of thesubclavian artery and proceeds tobecome the brachial artery at thelower border of teres major. It givesoff:● Superior thoracic● Thoraco-acromial● Lateral thoracic
● Subscapular● Circumflex humeral (anterior and
posterior)2. Brachial artery – extends from the
teres major to the lower margins ofthe antecubital fossa, bifurcating intothe radial and ulnar arteries. Thebranches are:● Profunda brachii● Ulnar collateral (superior and
inferior)● Nutrient to humerus
3. Radial artery – lies on the radiusalong the medial border of thebrachioradialis, and it enters to thelateral aspect of the wrist (goingthrough anatomical snuffbox) toterminate in the deep palmar arch.The branches are:● Radial recurrent● Muscular● Carpal● Metacarpal● Superficial and deep palmar arch
4. Ulnar artery – accompanies the ulnarnerve and lies on the flexordigitorum profundus (lateral to ulnarnerve) before entering the wrist(superficial to flexor retinaculum) andterminating in the superficial palmararch. The branches are:● Ulnar recurrent● Common interosseous (divides
into anterior and posterior)● Muscular● Carpal● Superficial and deep palmar arch
Lower limb
1. Common iliac – from the aorticbifurcation at L4
2. External iliac – main continuation ofthe common iliac and travels down,anteriorly and laterally, deep to themid-inguinal point and becomes thefemoral artery in the thigh. Thebranches are:32
Concise Anatomy for Anaesthesia
33
The great vessels
Cardio
vascularS
ystem
Occipital artery
Right internalcarotid
Vertebral artery
Thyrocervical trunk
Right subclavian
Costocervical
Brachiocephalicartery
Right common carotid artery
Right external carotid
Facial artery
Maxillary artery
Superficial temporal artery
Fig 11.2Major arteries of the head and neck
Right subclavianartery
Brachiocephalic artery
Axillary artery
Subscapular artery
Brachial artery
Ulnar collateral
Ulnar artery
Ulnar artery
Deep palmar arch
Superficial palmar arch
Digital artery
Common interosseous artery
Anterior interosseous arteryRadialartery
Radialcollateralartery
Profundabrachii
Circumflexhumeralartery
Fig 11.3Arteries of upper limb
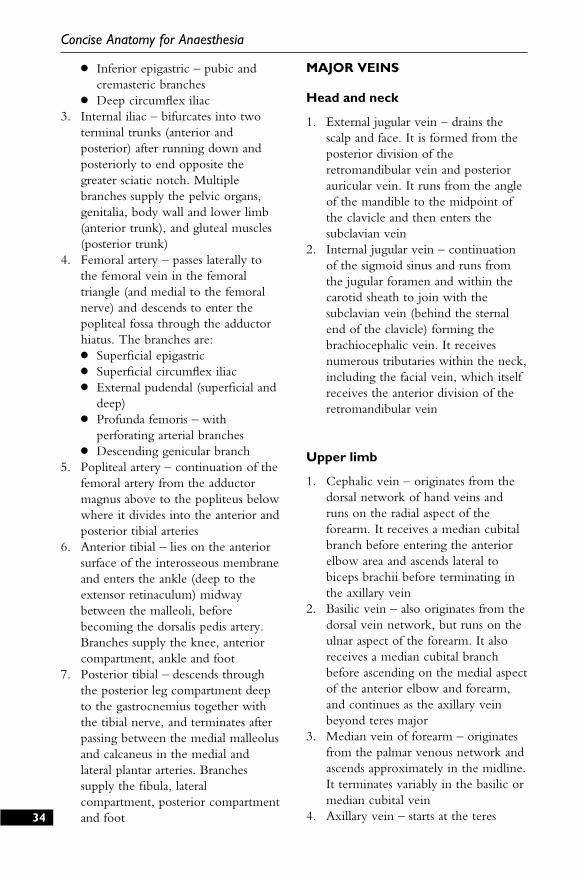
● Inferior epigastric – pubic andcremasteric branches
● Deep circumflex iliac3. Internal iliac – bifurcates into two
terminal trunks (anterior andposterior) after running down andposteriorly to end opposite thegreater sciatic notch. Multiplebranches supply the pelvic organs,genitalia, body wall and lower limb(anterior trunk), and gluteal muscles(posterior trunk)
4. Femoral artery – passes laterally tothe femoral vein in the femoraltriangle (and medial to the femoralnerve) and descends to enter thepopliteal fossa through the adductorhiatus. The branches are:● Superficial epigastric● Superficial circumflex iliac● External pudendal (superficial and
deep)● Profunda femoris – with
perforating arterial branches● Descending genicular branch
5. Popliteal artery – continuation of thefemoral artery from the adductormagnus above to the popliteus belowwhere it divides into the anterior andposterior tibial arteries
6. Anterior tibial – lies on the anteriorsurface of the interosseous membraneand enters the ankle (deep to theextensor retinaculum) midwaybetween the malleoli, beforebecoming the dorsalis pedis artery.Branches supply the knee, anteriorcompartment, ankle and foot
7. Posterior tibial – descends throughthe posterior leg compartment deepto the gastrocnemius together withthe tibial nerve, and terminates afterpassing between the medial malleolusand calcaneus in the medial andlateral plantar arteries. Branchessupply the fibula, lateralcompartment, posterior compartmentand foot
MAJOR VEINS
Head and neck
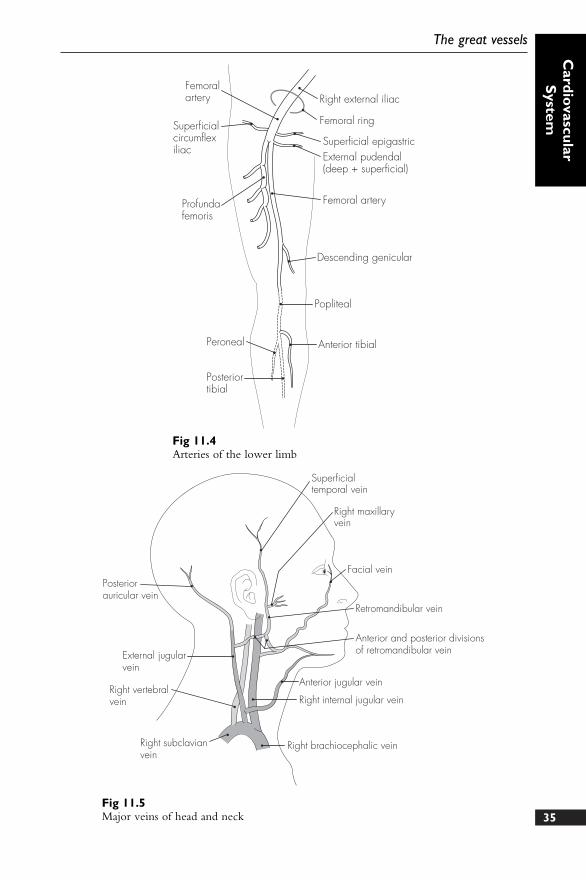
1. External jugular vein – drains thescalp and face. It is formed from theposterior division of theretromandibular vein and posteriorauricular vein. It runs from the angleof the mandible to the midpoint ofthe clavicle and then enters thesubclavian vein
2. Internal jugular vein – continuationof the sigmoid sinus and runs fromthe jugular foramen and within thecarotid sheath to join with thesubclavian vein (behind the sternalend of the clavicle) forming thebrachiocephalic vein. It receivesnumerous tributaries within the neck,including the facial vein, which itselfreceives the anterior division of theretromandibular vein
Upper limb
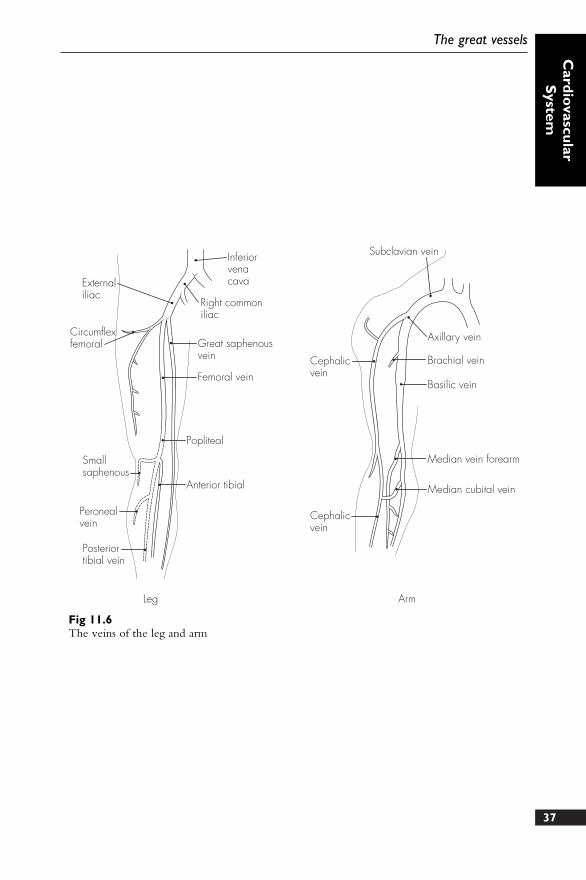
1. Cephalic vein – originates from thedorsal network of hand veins andruns on the radial aspect of theforearm. It receives a median cubitalbranch before entering the anteriorelbow area and ascends lateral tobiceps brachii before terminating inthe axillary vein
2. Basilic vein – also originates from thedorsal vein network, but runs on theulnar aspect of the forearm. It alsoreceives a median cubital branchbefore ascending on the medial aspectof the anterior elbow and forearm,and continues as the axillary veinbeyond teres major
3. Median vein of forearm – originatesfrom the palmar venous network andascends approximately in the midline.It terminates variably in the basilic ormedian cubital vein
4. Axillary vein – starts at the teres34
Concise Anatomy for Anaesthesia
35
The great vessels
Cardio
vascularS
ystem
Femoralartery
Superficialcircumflexiliac
Profundafemoris
Right external iliac
Femoral ring
Superficial epigastricExternal pudendal(deep + superficial)
Femoral artery
Descending genicular
Popliteal
Anterior tibialPeroneal
Posteriortibial
Fig 11.4Arteries of the lower limb
Superficialtemporal vein
Right maxillaryvein
Facial vein
Retromandibular vein
Anterior and posterior divisionsof retromandibular vein
Anterior jugular vein
Right internal jugular vein
Right brachiocephalic veinRight subclavianvein
Right vertebralvein
External jugularvein
Posteriorauricular vein
Fig 11.5Major veins of head and neck

major and ends opposite the first ribto continue as the subclavian vein
Thorax
1. Brachiocephalic vein (bilateralvenous, unilateral arterial) – formedfrom the junction of the internaljugular and subclavian veins behindthe sternal clavicle. The longer leftand shorter right brachiocephalicveins join behind the first costalcartilage to become the superior venacava (drains blood from abovediaphragm)
Abdomen
1. External iliac – continuation of thefemoral vein (draining the leg) and isjoined by the internal iliac (drainingthe pelvis) to form the common iliacvein in front of the sacroiliac joint
2. Common iliac – left and right ascendand unite at the L5 level to form the
inferior vena cava (drains blood frombelow diaphragm)
Lower limb
1. Great saphenous vein – from themedial aspect of the foot and in frontof the medial malleolus. It ascends onthe medial side to the knee and up tothe thigh where it enters thesaphenous foramen and joins thefemoral vein
2. Small saphenous vein – from thelateral aspect of the foot and behindthe lateral malleolus. It ascends in themidline posteriorly and joins thepopliteal vein after running betweenthe two heads of the gastrocnemius
3. Posterior tibial vein – runs with theposterior tibial artery and unites withthe anterior tibial vein to form thepopliteal vein
4. Femoral vein – continuation of thepopliteal vein as it emerges from theadductor canal and enters the femoraltriangle
36
Concise Anatomy for Anaesthesia
37
The great vessels
Cardio
vascularS
ystem
Inferiorvenacava
Right commoniliac
Externaliliac
Circumflexfemoral
Smallsaphenous
Peronealvein
Posteriortibial vein
Popliteal
Anterior tibial
Great saphenousvein
Femoral vein
Subclavian vein
Cephalicvein
Axillary vein
Cephalicvein
Brachial vein
Basilic vein
Median vein forearm
Median cubital vein
Leg Arm
Fig 11.6The veins of the leg and arm
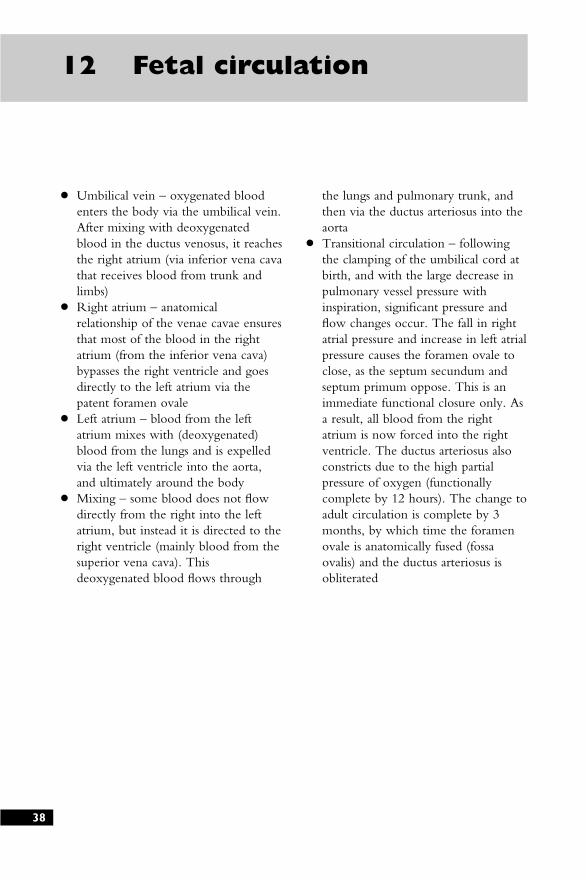
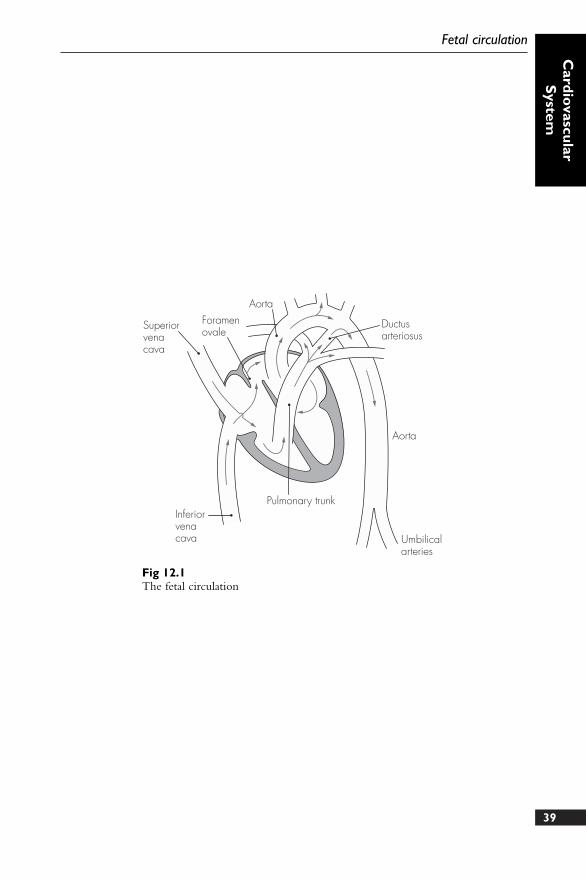
● Umbilical vein – oxygenated bloodenters the body via the umbilical vein.After mixing with deoxygenatedblood in the ductus venosus, it reachesthe right atrium (via inferior vena cavathat receives blood from trunk andlimbs)
● Right atrium – anatomicalrelationship of the venae cavae ensuresthat most of the blood in the rightatrium (from the inferior vena cava)bypasses the right ventricle and goesdirectly to the left atrium via thepatent foramen ovale
● Left atrium – blood from the leftatrium mixes with (deoxygenated)blood from the lungs and is expelledvia the left ventricle into the aorta,and ultimately around the body
● Mixing – some blood does not flowdirectly from the right into the leftatrium, but instead it is directed to theright ventricle (mainly blood from thesuperior vena cava). Thisdeoxygenated blood flows through
the lungs and pulmonary trunk, andthen via the ductus arteriosus into theaorta
● Transitional circulation – followingthe clamping of the umbilical cord atbirth, and with the large decrease inpulmonary vessel pressure withinspiration, significant pressure andflow changes occur. The fall in rightatrial pressure and increase in left atrialpressure causes the foramen ovale toclose, as the septum secundum andseptum primum oppose. This is animmediate functional closure only. Asa result, all blood from the rightatrium is now forced into the rightventricle. The ductus arteriosus alsoconstricts due to the high partialpressure of oxygen (functionallycomplete by 12 hours). The change toadult circulation is complete by 3months, by which time the foramenovale is anatomically fused (fossaovalis) and the ductus arteriosus isobliterated
38
12 Fetal circulation
39
Fetal circulation
Cardio
vascularS
ystem
Foramenovale
Aorta
Ductusarteriosus
Aorta
Umbilicalarteries
Pulmonary trunkInferiorvenacava
Superiorvenacava
Fig 12.1The fetal circulation

1. Describe, with the aid of a simplediagram, the blood supply of theheart. Briefly indicate the areas ofmyocardium supplied by thecoronary arteries and their mainbranches.
2. Give an account of the arterial supplyof the upper limb. List thecomplications of intra-arterial cannula
insertion and indicate the precautionsrequired prior to insertion.
3. Describe the venous drainage of theleg.
4. Using a simple diagram, indicate thespecial features of the fetal circulationand the subsequent changes followingbirth.
40
Sample questions –cardiovascular system
Nervous System
DESCRIPTION
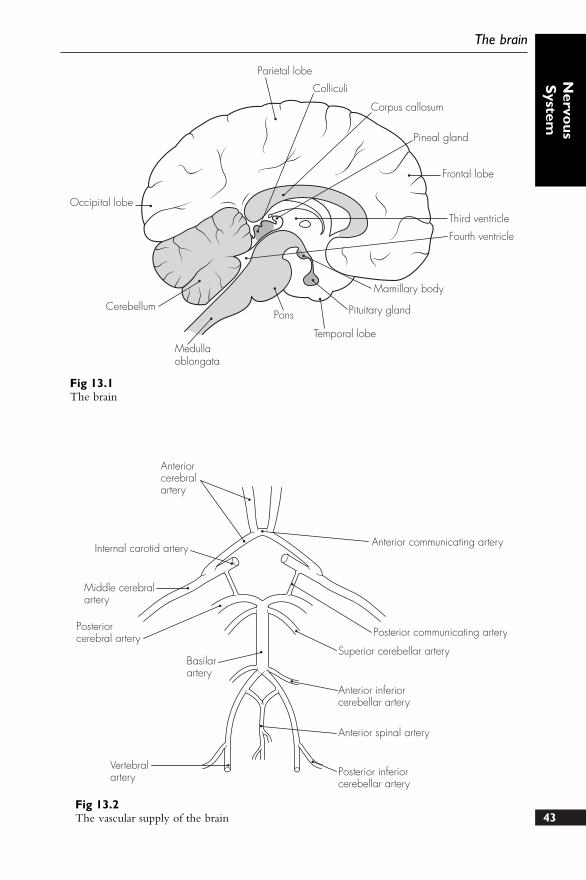
There are three main parts of the brain:
Forebrain:● Telencephalon – consists of the
two cerebral hemispheresseparated by a longitudinalfissure. The cortex of eachhemisphere is made up of gyriand sulci and is separated intolobes. Four major lobes arecommonly recognised: frontal,parietal, occipital and temporal
● Diencephalon – lies between thecerebral hemispheres andmidbrain. It contains thethalamus and the hypothalamus
Midbrain – connects the forebrain tothe hindbrain
Hindbrain – consists of the pons, themedulla oblongata (which exits thecranial cavity through the foramenmagnum) and the cerebellum
VASCULAR SUPPLY
1. Arterial – arterial supply to the braincomes from four arteries: the pairedinternal carotid arteries and the pairedvertebral arteries. These form thecircle of Willis from which theanterior, middle and posteriorcerebral arteries arise
2. Venous – venous drainage of thebrain is via the numerous duralvenous sinuses, which drain into theinternal jugular vein
42
13 The brain
43
The brain
Nervo
usS
ystem
Occipital lobe
Parietal lobe
Colliculi
Corpus callosum
Pineal gland
Frontal lobe
Third ventricle
Fourth ventricle
Mamillary body
Pituitary gland
Temporal lobe
Pons
Medullaoblongata
Cerebellum
Fig 13.1The brain
Anteriorcerebralartery
Internal carotid artery
Middle cerebralartery
Posteriorcerebral artery
Basilarartery
Vertebralartery Posterior inferior
cerebellar artery
Anterior spinal artery
Anterior inferiorcerebellar artery
Superior cerebellar artery
Posterior communicating artery
Anterior communicating artery
Fig 13.2The vascular supply of the brain
DESCRIPTION
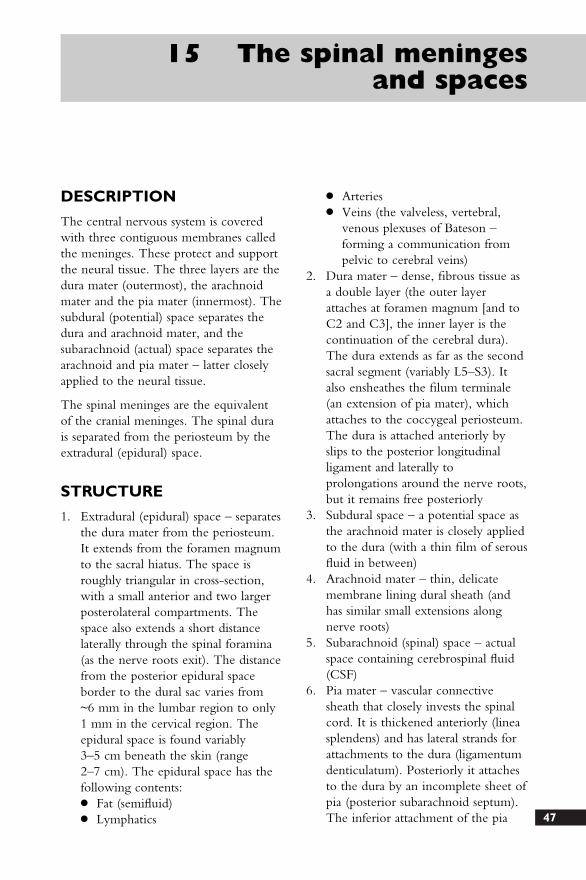
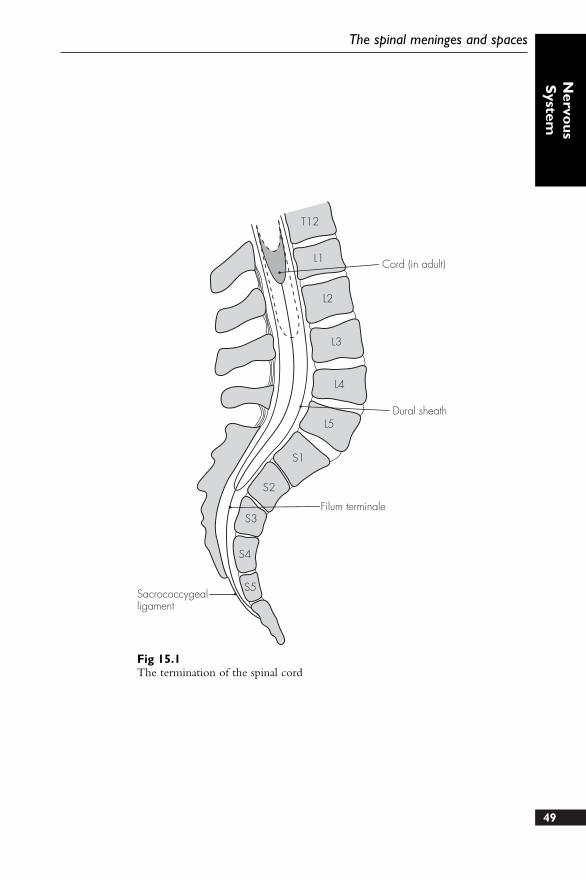
The spinal cord is ~45 cm long in theadult and has an approximatelycylindrical shape, which is flattenedsomewhat in the lumbar region. Itextends from the cervical area as anextension of the medulla oblongata andcontinues to the lumbar region, where itterminates in the conus medullaris. Athin thread called the filum terminalecontinues to attach to the coccyx.
There are normally 31 pairs of spinalnerve roots: eight cervical, 12 thoracic,five lumbar, five sacral and onecoccygeal. The elongation of the lumbarand sacral nerve roots, prior to their exitfrom the intervertebral foramina, formsthe cauda equina. There is a widevariation in the relations of the cordthroughout the course of life. The spinalcord ends, on average, between L1 andL2 in the adult – and in the newborn itmay end at the lower border of L3.However, individual variation betweenT12 and L3 in the adult is notuncommon.
STRUCTURE
The spinal cord is roughly circular incross-section, flattened in theanterior–posterior aspect. There are twomajor indentations: an anterior medianfissure and a posterior median sulcus(which extends further to form theposterior median septum). Furtherposterolateral sulci exist, along which theposterior nerve roots are seen to exit.
The anterior nerve roots, however, exitwithout a corresponding groove.
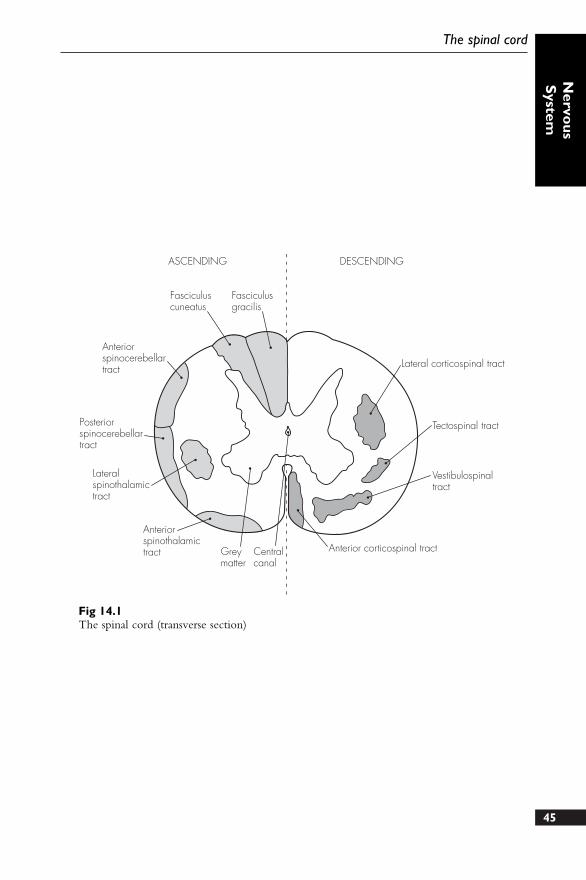
The following structures can be seen oncross-section:
1. Central canal – travels downwardfrom the fourth ventricle. It iscontinuous throughout the cord andis slightly dilated in the region of theconus medullaris
2. Grey matter – forms the ‘H-like’structure in the central regions of thecord. The lateral limbs of grey matterare joined by the transversecommissure. The limbs have ananterior (wider) column or horn anda posterior (narrower) column. Theposterior horn has a group ofspecialised nerve cells, the substantiagelatinosa, at its tip. A lateral greycolumn can also be seen in thethoracic and upper lumbar area(containing spinal sympatheticcells)
3. White matter – consists oflongitudinal nerve fibres divided intothe following major tracts:● Descending lateral corticospinal
tract – major motor tract (fibrescross the midline in the medulla –pyramidal decussation)
● Descending anterior corticospinaltract – small motor tract (fibres donot decussate until reaching thedistal anterior horn cells)
● Ascending posterior column –divided into the fasciculus gracilisand cuneatus. These subserve finetouch and proprioception (largelyuncrossed)44
14 The spinal cord
45
The spinal cord
Nervo
usS
ystem
Fasciculusgracilis
Fasciculuscuneatus
Anteriorspinocerebellartract
Posteriorspinocerebellartract
Lateralspinothalamictract
Anteriorspinothalamictract Grey
matterCentralcanal
Anterior corticospinal tract
Vestibulospinaltract
Tectospinal tract
Lateral corticospinal tract
ASCENDING DESCENDING
Fig 14.1The spinal cord (transverse section)
46
Concise Anatomy for Anaesthesia
● Ascending spinothalamic tracts –lateral (pain and temperature –cross midline) and anterior/dorsal(touch/deep pain – remainuncrossed)
● Ascending spinocerebellar tracts –anterior and posterior (sensoryproprioception to the cerebellum)
VASCULAR SUPPLY
1. Arterial:● Anterior spinal artery – formed by
the union of the vertebral arteriesat the foramen magnum. It runson the anterior median fissure andsupplies the larger part of theanterior spinal cord
● Posterior spinal arteries (one ortwo on each side) – formed fromthe posterior cerebellar arteries.These are smaller and reinforcedby spinal branches from a numberof nearby vessels
● Radicular arteries also providefurther blood supply to both the
anterior and posterior spinalarteries. These arise from thecervical, thoracic and lumbarregions (usually number betweenthree and six larger vessels). Onevessel is often particularly large –arteria radicularis magna. It usuallyarises distally and from the left,and may provide the dominantsupply to the lower two-thirds ofthe spinal cord
Despite the extensive origin, thearterial blood supply of the spinalcord is vulnerable. The anterior andposterior spinal arteries do not havedirect anastomoses and cordinfarction is possible after thrombosis,hypotension, surgical occlusion,trauma, and vasoconstriction.
2. Venous:● By a series of venous plexuses or
channels (anterior, posterior andlateral), which in turn drain intosegmental veins, including thevertebral, azygos, lumbar andlateral sacral veins
47
DESCRIPTION
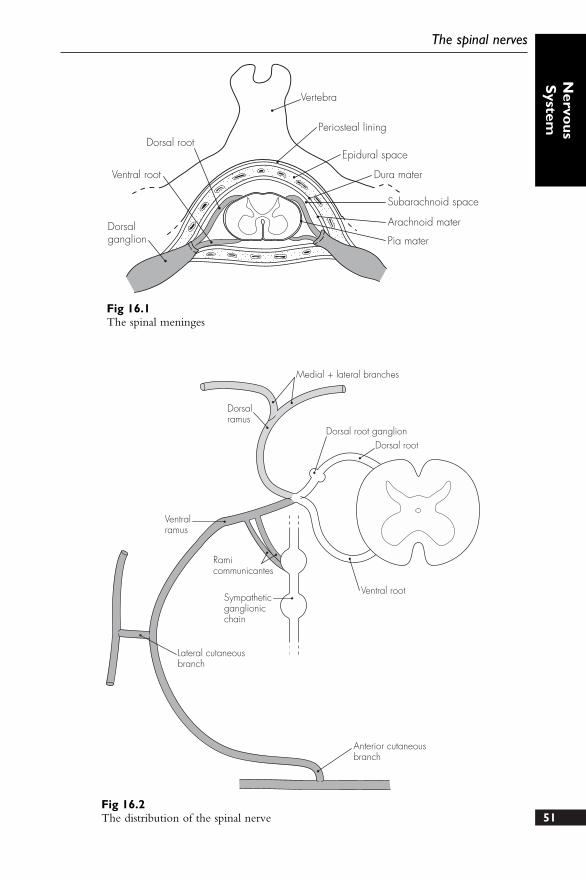
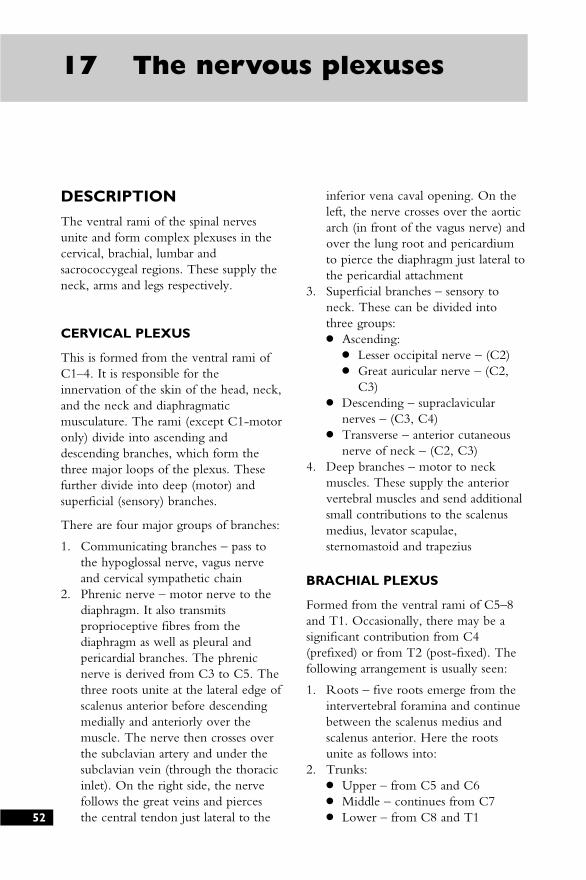
The central nervous system is coveredwith three contiguous membranes calledthe meninges. These protect and supportthe neural tissue. The three layers are thedura mater (outermost), the arachnoidmater and the pia mater (innermost). Thesubdural (potential) space separates thedura and arachnoid mater, and thesubarachnoid (actual) space separates thearachnoid and pia mater – latter closelyapplied to the neural tissue.
The spinal meninges are the equivalentof the cranial meninges. The spinal durais separated from the periosteum by theextradural (epidural) space.
STRUCTURE
1. Extradural (epidural) space – separatesthe dura mater from the periosteum.It extends from the foramen magnumto the sacral hiatus. The space isroughly triangular in cross-section,with a small anterior and two largerposterolateral compartments. Thespace also extends a short distancelaterally through the spinal foramina(as the nerve roots exit). The distancefrom the posterior epidural spaceborder to the dural sac varies from~6 mm in the lumbar region to only1 mm in the cervical region. Theepidural space is found variably3–5 cm beneath the skin (range2–7 cm). The epidural space has thefollowing contents:● Fat (semifluid)● Lymphatics
● Arteries● Veins (the valveless, vertebral,
venous plexuses of Bateson –forming a communication frompelvic to cerebral veins)
2. Dura mater – dense, fibrous tissue asa double layer (the outer layerattaches at foramen magnum [and toC2 and C3], the inner layer is thecontinuation of the cerebral dura).The dura extends as far as the secondsacral segment (variably L5–S3). Italso ensheathes the filum terminale(an extension of pia mater), whichattaches to the coccygeal periosteum.The dura is attached anteriorly byslips to the posterior longitudinalligament and laterally toprolongations around the nerve roots,but it remains free posteriorly
3. Subdural space – a potential space asthe arachnoid mater is closely appliedto the dura (with a thin film of serousfluid in between)
4. Arachnoid mater – thin, delicatemembrane lining dural sheath (andhas similar small extensions alongnerve roots)
5. Subarachnoid (spinal) space – actualspace containing cerebrospinal fluid(CSF)
6. Pia mater – vascular connectivesheath that closely invests the spinalcord. It is thickened anteriorly (lineasplendens) and has lateral strands forattachments to the dura (ligamentumdenticulatum). Posteriorly it attachesto the dura by an incomplete sheet ofpia (posterior subarachnoid septum).The inferior attachment of the pia
15 The spinal meningesand spaces
48
mater to the coccyx is via itscontinuation – filum terminale
POINTS OF INTEREST
● Cerebrospinal fluid (CSF):● Volume – ~150 ml (roughly equal
to daily production), only 25 ml ofwhich is contained in thespinal/subarachnoid space
● Production – by the choroidplexuses of the lateral, third andfourth ventricles. It passes from thelateral ventricles to the thirdventricle via the pairedinterventricular foramina (ofMunro), and then via the cerebralaqueduct to the fourth ventricle.The CSF then flows from thefourth ventricle to thesubarachnoid spinal space throughthe paired lateral foramina of
Lushka and the median foramen ofMagendie
● Absorption – ~80% is absorbed viathe arachnoid villi (projections ofarachnoid mater) in the cerebralvenous sinuses. The remaining 20%is absorbed by spinal arachnoid villior by lymphatic drainage. The CSFpressure is gravity-dependent andranges from 6 to 10 cm (of CSF)when lying, to subatmosphericcervically and 20–40 cm in thelumbar area when sitting
● Composition – is approximately:Osmolality = 280 mOsmSpecific gravity = 1005pH 7.4Glucose = 1.5–4.0 mmol l–1
Sodium = 140–150 mmol l–1
Chloride = 120–130 mmol l–1
Bicarbonate = 25–30 mmol l–1
Protein = 0.15–0.3 g l–1
Cells = less than five lymphs mm–3
Concise Anatomy for Anaesthesia
49
The spinal meninges and spaces
Nervo
usS
ystem
T12
L1
L2
L3
L4
L5
S1
S2
S3
S4
S5
Cord (in adult)
Dural sheath
Filum terminale
Sacrococcygealligament
Fig 15.1The termination of the spinal cord
DESCRIPTION
These number 31 pairs in total: eightcervical, 12 thoracic, five lumbar, fivesacral and one coccygeal. The nerves aremixed (i.e. contain sensory and motorfibres) and are formed from the fusion ofventral (anterior) motor and dorsal(posterior) sensory roots. Unlike theventral roots, the dorsal sensory rootscontain a ganglion located just prior tothe fusion of the roots.
The spinal nerves exit from the vertebralcanal through the intervertebral foramina,and the nerve roots are sheathed inmeningeal membranes – dura extendingas far as the fusion to form the spinalnerve.
Once fused, the spinal nervesimmediately give off a small meningealbranch (which supplies the vertebralstructures) and then divide into twomajor nerves: the dorsal and ventral rami.There is also a branch that links to thesympathetic ganglionic chain – these arecalled the rami communicantes.
STRUCTURE
1. Dorsal (posterior) primary rami –generally smaller than the ventral
rami and divide into medial andlateral branches. They are concernedwith the innervation of the back(skin and muscles). The innervation ischaracteristically segmental ordermatomal in distribution. A fewdorsal rami are exceptional:● First cervical dorsal ramus is
entirely motor, larger and does nothave medial and lateral branches.It supplies the muscles of thesuboccipital triangle
● Second cervical dorsal ramus isalso large and divides into a largemedial branch (which becomesthe greater occipital nerve) and asmaller lateral (motor) branch
● Coccygeal dorsal ramus is verysmall, undivided and supplies theskin over the coccyx
2. Ventral (anterior) primary rami –generally larger, these supply the arm,leg and the anterior/lateral aspects ofthe torso. Some ventral rami uniteand form nerve plexuses: cervical,brachial and lumbosacral. These arediscussed below. The thoracicventral rami remain, however,independent of each other, separatedby the ribs. They, like the dorsalrami, innervate segmentally(dermatomal distribution)
50
16 The spinal nerves
51
The spinal nerves
Nervo
usS
ystem
Dorsalganglion
Ventral root
Dorsal root
Vertebra
Periosteal lining
Epidural space
Dura mater
Subarachnoid space
Arachnoid mater
Pia mater
Fig 16.1The spinal meninges
Dorsalramus
Medial + lateral branches
Dorsal root ganglionDorsal root
Ventralramus
Ventral root
Ramicommunicantes
Sympatheticganglionicchain
Lateral cutaneousbranch
Anterior cutaneousbranch
Fig 16.2The distribution of the spinal nerve
DESCRIPTION
The ventral rami of the spinal nervesunite and form complex plexuses in thecervical, brachial, lumbar andsacrococcygeal regions. These supply theneck, arms and legs respectively.
CERVICAL PLEXUS
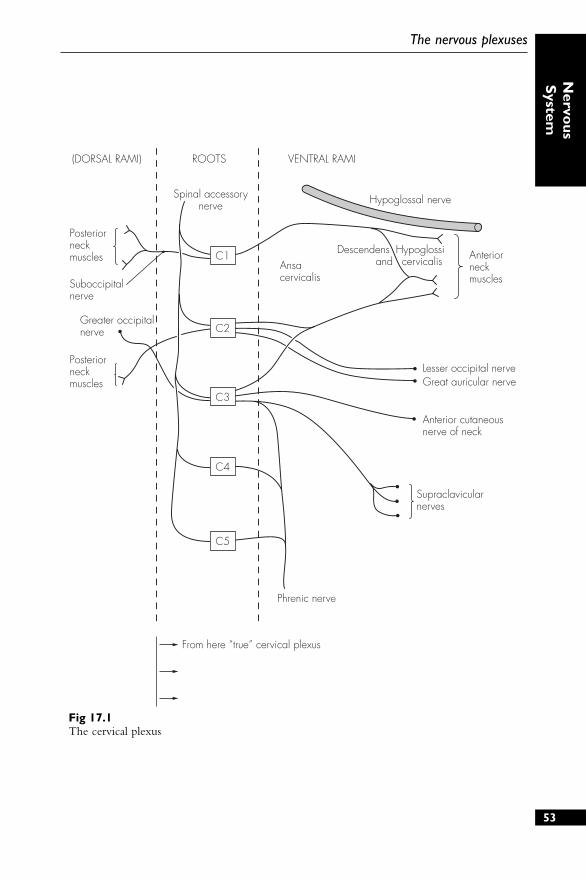
This is formed from the ventral rami ofC1–4. It is responsible for theinnervation of the skin of the head, neck,and the neck and diaphragmaticmusculature. The rami (except C1-motoronly) divide into ascending anddescending branches, which form thethree major loops of the plexus. Thesefurther divide into deep (motor) andsuperficial (sensory) branches.
There are four major groups of branches:
1. Communicating branches – pass tothe hypoglossal nerve, vagus nerveand cervical sympathetic chain
2. Phrenic nerve – motor nerve to thediaphragm. It also transmitsproprioceptive fibres from thediaphragm as well as pleural andpericardial branches. The phrenicnerve is derived from C3 to C5. Thethree roots unite at the lateral edge ofscalenus anterior before descendingmedially and anteriorly over themuscle. The nerve then crosses overthe subclavian artery and under thesubclavian vein (through the thoracicinlet). On the right side, the nervefollows the great veins and piercesthe central tendon just lateral to the
inferior vena caval opening. On theleft, the nerve crosses over the aorticarch (in front of the vagus nerve) andover the lung root and pericardiumto pierce the diaphragm just lateral tothe pericardial attachment
3. Superficial branches – sensory toneck. These can be divided intothree groups:● Ascending:
● Lesser occipital nerve – (C2)● Great auricular nerve – (C2,
C3)● Descending – supraclavicular
nerves – (C3, C4)● Transverse – anterior cutaneous
nerve of neck – (C2, C3)4. Deep branches – motor to neck
muscles. These supply the anteriorvertebral muscles and send additionalsmall contributions to the scalenusmedius, levator scapulae,sternomastoid and trapezius
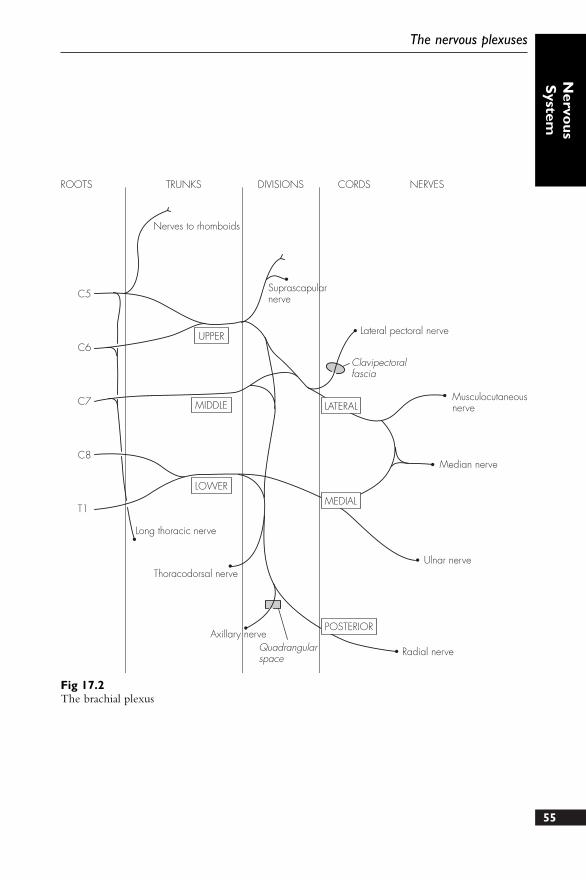
BRACHIAL PLEXUS
Formed from the ventral rami of C5–8and T1. Occasionally, there may be asignificant contribution from C4(prefixed) or from T2 (post-fixed). Thefollowing arrangement is usually seen:
1. Roots – five roots emerge from theintervertebral foramina and continuebetween the scalenus medius andscalenus anterior. Here the rootsunite as follows into:
2. Trunks:● Upper – from C5 and C6● Middle – continues from C7● Lower – from C8 and T152
17 The nervous plexuses
(DORSAL RAMI) ROOTS VENTRAL RAMI
Spinal accessorynerve
Posteriorneckmuscles
Posteriorneckmuscles
Greater occipitalnerve
Phrenic nerve
Supraclavicularnerves
Anterior cutaneous nerve of neck
Lesser occipital nerveGreat auricular nerve
Anteriorneckmuscles
Ansacervicalis
Descendens Hypoglossi and cervicalis
Hypoglossal nerve
Suboccipitalnerve
C1
C2
C3
C4
C5
From here “true” cervical plexus
53
The nervous plexuses
Nervo
usS
ystem
Fig 17.1The cervical plexus
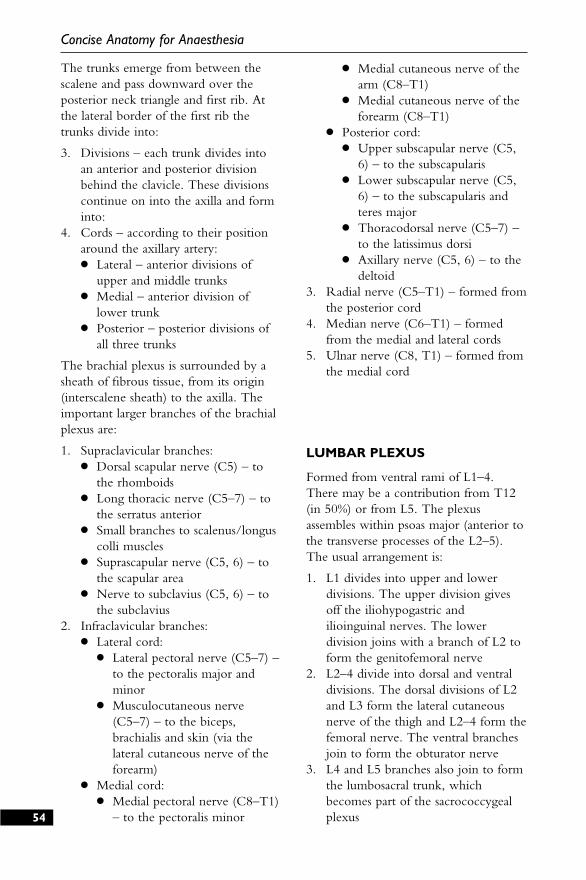
The trunks emerge from between thescalene and pass downward over theposterior neck triangle and first rib. Atthe lateral border of the first rib thetrunks divide into:
3. Divisions – each trunk divides intoan anterior and posterior divisionbehind the clavicle. These divisionscontinue on into the axilla and forminto:
4. Cords – according to their positionaround the axillary artery:● Lateral – anterior divisions of
upper and middle trunks● Medial – anterior division of
lower trunk● Posterior – posterior divisions of
all three trunks
The brachial plexus is surrounded by asheath of fibrous tissue, from its origin(interscalene sheath) to the axilla. Theimportant larger branches of the brachialplexus are:
1. Supraclavicular branches:● Dorsal scapular nerve (C5) – to
the rhomboids● Long thoracic nerve (C5–7) – to
the serratus anterior● Small branches to scalenus/longus
colli muscles● Suprascapular nerve (C5, 6) – to
the scapular area● Nerve to subclavius (C5, 6) – to
the subclavius2. Infraclavicular branches:
● Lateral cord:● Lateral pectoral nerve (C5–7) –
to the pectoralis major andminor
● Musculocutaneous nerve(C5–7) – to the biceps,brachialis and skin (via thelateral cutaneous nerve of theforearm)
● Medial cord:● Medial pectoral nerve (C8–T1)
– to the pectoralis minor
● Medial cutaneous nerve of thearm (C8–T1)
● Medial cutaneous nerve of theforearm (C8–T1)
● Posterior cord:● Upper subscapular nerve (C5,
6) – to the subscapularis● Lower subscapular nerve (C5,
6) – to the subscapularis andteres major
● Thoracodorsal nerve (C5–7) –to the latissimus dorsi
● Axillary nerve (C5, 6) – to thedeltoid
3. Radial nerve (C5–T1) – formed fromthe posterior cord
4. Median nerve (C6–T1) – formedfrom the medial and lateral cords
5. Ulnar nerve (C8, T1) – formed fromthe medial cord
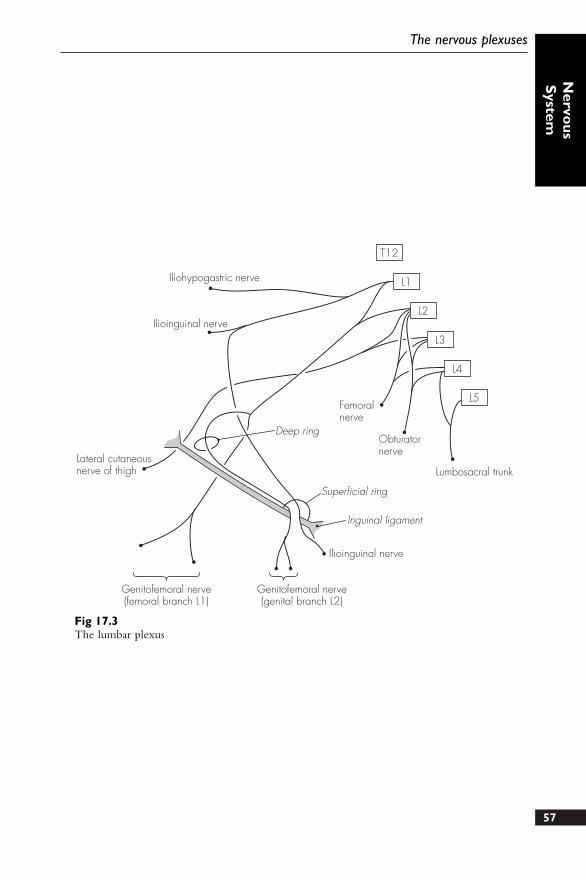
LUMBAR PLEXUS
Formed from ventral rami of L1–4.There may be a contribution from T12(in 50%) or from L5. The plexusassembles within psoas major (anterior tothe transverse processes of the L2–5).The usual arrangement is:
1. L1 divides into upper and lowerdivisions. The upper division givesoff the iliohypogastric andilioinguinal nerves. The lowerdivision joins with a branch of L2 toform the genitofemoral nerve
2. L2–4 divide into dorsal and ventraldivisions. The dorsal divisions of L2and L3 form the lateral cutaneousnerve of the thigh and L2–4 form thefemoral nerve. The ventral branchesjoin to form the obturator nerve
3. L4 and L5 branches also join to formthe lumbosacral trunk, whichbecomes part of the sacrococcygealplexus54
Concise Anatomy for Anaesthesia
55
The nervous plexuses
Nervo
usS
ystem
ROOTS TRUNKS DIVISIONS CORDS NERVES
Nerves to rhomboids
UPPER
MIDDLE
LOWER
Long thoracic nerve
Thoracodorsal nerve
Axillary nerve
Radial nerve
Ulnar nerve
Median nerve
Musculocutaneousnerve
Lateral pectoral nerve
Clavipectoralfascia
SuprascapularnerveC5
C6
C7
C8
T1
Quadrangularspace
LATERAL
MEDIAL
POSTERIOR
Fig 17.2The brachial plexus

SACROCOCCYGEAL PLEXUS
There is a wide variation in constitution.The sacral plexus is formed from L4–5and S1–4. The coccygeal part is formedfrom S4, S5 and the coccygeal nerve:
1. L4 and L5 form the lumbosacraltrunk at the medial border of psoasmajor. This travels over the pelvicbrim and joins S1
2. Ventral rami of S1–4, with S5 andCo. 1 join the plexus within thepelvis
The sacral plexus has numerous vesselspassing in between the nerve trunks.These are the inferior gluteal, superiorgluteal, iliolumbar and internal pudendalvessels. The most important nervebranches are:
1. Superior gluteal nerve (L4 and L5,S1)
2. Inferior gluteal nerve (L5, S1 and S2)3. Posterior femoral cutaneous nerve
(S1–3)4. Perforating cutaneous nerve (S2 and
S3)5. Pudendal nerve (S2–4)6. Sciatic nerve (S2–4) – largest nerve in
the body and supplies (together withthe femoral nerve) the lower limb
The coccygeal part of the plexus is small.S4, S5 and Co. 1 join to form theanococcygeal nerve, and this supplies theskin over the coccyx.
POINTS OF INTEREST
● Regional anaesthetic blockade ispossible by injecting a localanaesthetic solution around the nervesof a plexus. Brachial plexus blockadeis the most commonly performedmajor peripheral nerve block, but thecervical and lumbar plexuses may alsobe targeted
● Brachial plexus block – large numberof techniques described, but each fallsinto one of four groups:● Interscalene● Supraclavicular● Axillary● Infraclavicular
● No one technique is demonstrablybetter than the others, and each hasdifferent benefits and complications.The more common complicationsinclude pneumothorax, phrenic nervepalsy, stellate ganglion block,recurrent laryngeal nerve palsy,subarachnoid injection and vertebralartery injection. The details of how toperform these blocks are welldescribed in the many excellent textsof regional anaesthesia
● Cervical plexus block – provides goodanalgesia of the skin of the occipitalregion, posterior neck and shoulders.The superficial branches of the plexusprovide the sensory supply. These arebest located by turning the patient’shead slightly away from the side to beblocked. The point of needle entry istaken from a line drawn laterally fromthe cricoid cartilage where it meetsthe posterior border of thesternomastoid. A needle inserted atthis point at right angles to the skinwill pop through the cervical fascia,where 10 ml local anaesthetic is theninjected
● Lumbar plexus block – providesanalgesia to the lower abdominal skin,the skin over the hip and the proximallower limb:● Classically, the original approach
was paravertebral. This involvedthe patient lying prone, and a point4 cm lateral to the spinal process ofL3 used as the entry point. Thetransverse process is contacted at~5 cm depth, at which point theneedle is directed slightly cephaladand medially, and ‘walked off’ the56
Concise Anatomy for Anaesthesia
57
The nervous plexuses
Nervo
usS
ystem
Iliohypogastric nerve
Ilioinguinal nerve
Lateral cutaneousnerve of thigh
Deep ring
Femoralnerve
Obturatornerve
Lumbosacral trunk
Ilioinguinal nerve
Superficial ring
Inguinal ligament
Genitofemoral nerve(genital branch L2)
Genitofemoral nerve(femoral branch L1)
T12
L1
L2
L3
L4
L5
Fig 17.3The lumbar plexus

process for a further 2 cm. Solution(30 ml) is then injected
● Direct lumbar plexus blocktechnique is identical, except thatthe needle is not angled medially,only cephalad, once the transverseprocess is contacted
● Modified three-in-one techniquemay also be used. This relies onthe spread of the solution withinthe inguinal canal reaching thelumbar roots, and consequentlyhigher volumes of solution arerequired
58
Concise Anatomy for Anaesthesia
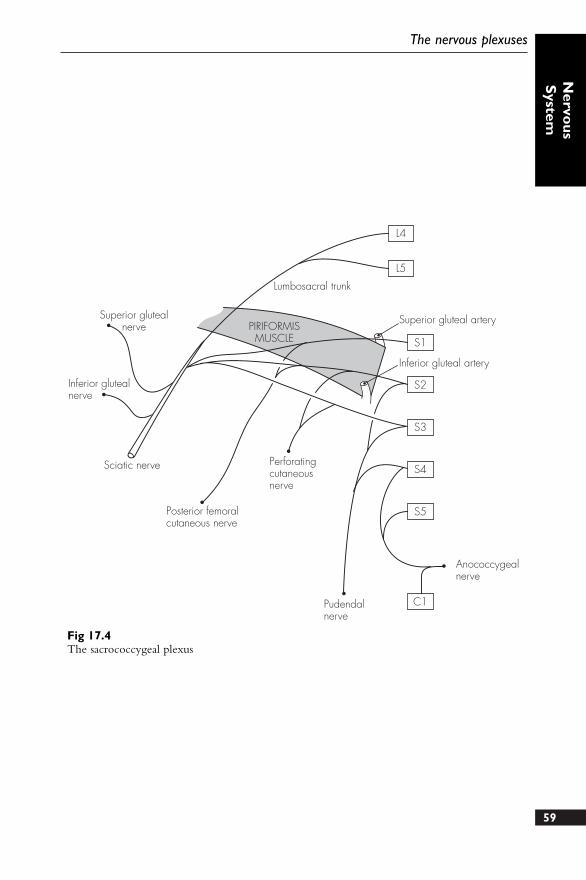
59
The nervous plexuses
Nervo
usS
ystem
Superior glutealnerve
Inferior glutealnerve
Sciatic nerve
Posterior femoralcutaneous nerve
Perforatingcutaneousnerve
Pudendalnerve
Lumbosacral trunk
Superior gluteal artery
Inferior gluteal artery
PIRIFORMISMUSCLE
Anococcygealnerve
L4
L5
S1
S2
S3
S4
S5
C1
Fig 17.4The sacrococcygeal plexus
These are divided into groups accordingto the area of supply.
UPPER LIMB
1. Radial nerve – continuation of theposterior cord of the brachial plexus(C5–T1). It descends posterior to theaxillary and brachial arteries andcrosses the tendons of latissimus dorsiand teres major. It passes between thelong and medial heads of triceps(accompanying profunda brachiivessels) before running posteriorlyaround the spiral groove of thehumerus. It then pierces the lateralintermuscular septum and runsforward between brachioradialis andbrachialis muscles. It terminates overthe lateral epicondyle in twobranches – superficial radial nerveand posterior interosseous nerve. Theradial nerve supplies:● Muscular branches to – triceps,
anconeus, brachialis,brachioradialis and extensor carpiradialis longus
● Cutaneous branches – posteriorcutaneous nerve of the arm,posterior cutaneous nerve of theforearm and lower lateralcutaneous nerve of the arm
● Posterior interosseous nerve –entirely motor to the extensors ofthe forearm and hand, and runsthrough the supinator muscle
● Superficial radial nerve – entirelysensory and runs underbrachioradialis (with radial artery)before dividing above the wrist
into digital branches. It suppliesthe dorsal thumb base, radial sideof back of hand and the back ofthe radial three and a half digits
2. Musculocutaneous nerve – arisesfrom the lateral cord (C5–7). It runsfrom behind the pectoralis minor(lateral to axillary artery) and descendsbetween the biceps and brachialis. Itterminates in the lateral cutaneousnerve of the forearm. It supplies:● Muscular branches to –
coracobrachialis, biceps andbrachialis
● Sensory branches – from thelateral cutaneous nerve of theforearm, supplying the skin overthe lateral forearm and wrist
3. Median nerve – arises from themedial and lateral cords (C6–T1).Initially anterior to the axillary artery,it then runs laterally and crosses thebrachial artery at the mid-humeruslevel to become medial in theantecubital fossa. Running oncoracobrachialis and brachialis, itpasses under the bicipital aponeurosisand enters the forearm between theflexor digitorum profundus andflexor digitorum superficialis. Itemerges laterally at the wrist to rununder the flexor retinaculum (in thecarpal tunnel) and terminates in twobranches (medial and lateral). Themedian nerve supplies:● Muscular branches to – pronator
teres, flexor carpi ulnaris, palmarislongus, flexor digitorumsuperficialis, three thenar musclesand lateral two lumbricals60
18 The major peripheralnerves
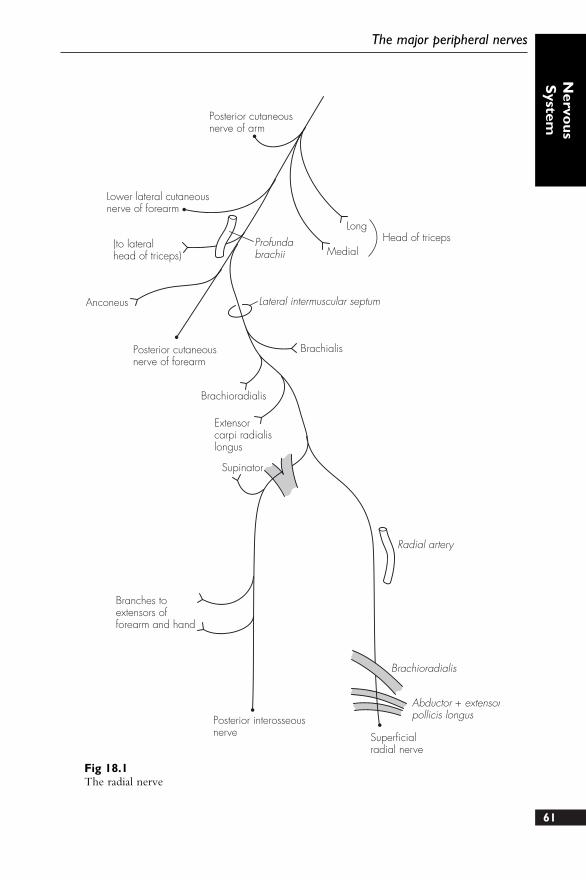
61
The major peripheral nerves
Nervo
usS
ystemPosterior cutaneousnerve of arm
Lower lateral cutaneousnerve of forearm
(to lateralhead of triceps)
Profundabrachii
Long
MedialHead of triceps
Lateral intermuscular septum
Brachialis
Anconeus
Posterior cutaneousnerve of forearm
Brachioradialis
Extensorcarpi radialislongus
Supinator
Radial artery
Branches toextensors offorearm and hand
Brachioradialis
Abductor + extensorpollicis longus
Superficialradial nerve
Posterior interosseousnerve
Fig 18.1The radial nerve
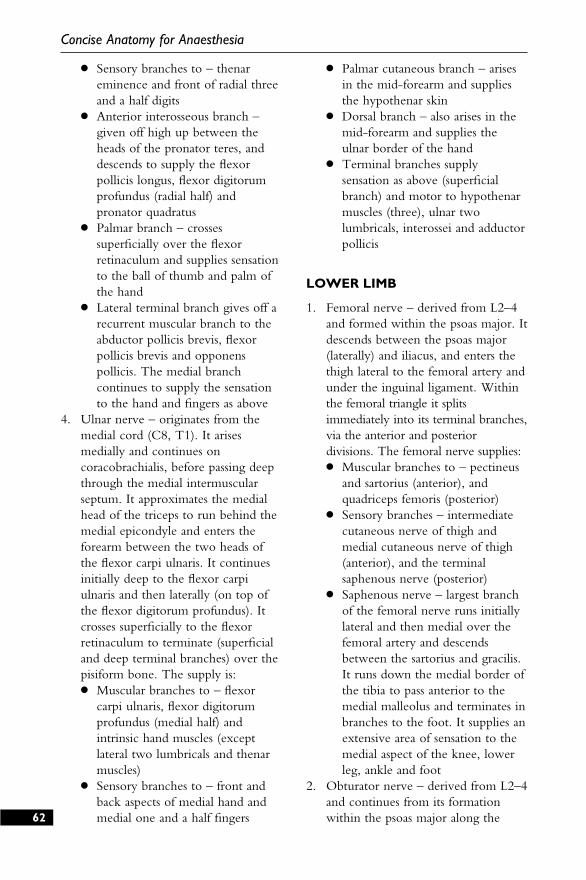
● Sensory branches to – thenareminence and front of radial threeand a half digits
● Anterior interosseous branch –given off high up between theheads of the pronator teres, anddescends to supply the flexorpollicis longus, flexor digitorumprofundus (radial half) andpronator quadratus
● Palmar branch – crossessuperficially over the flexorretinaculum and supplies sensationto the ball of thumb and palm ofthe hand
● Lateral terminal branch gives off arecurrent muscular branch to theabductor pollicis brevis, flexorpollicis brevis and opponenspollicis. The medial branchcontinues to supply the sensationto the hand and fingers as above
4. Ulnar nerve – originates from themedial cord (C8, T1). It arisesmedially and continues oncoracobrachialis, before passing deepthrough the medial intermuscularseptum. It approximates the medialhead of the triceps to run behind themedial epicondyle and enters theforearm between the two heads ofthe flexor carpi ulnaris. It continuesinitially deep to the flexor carpiulnaris and then laterally (on top ofthe flexor digitorum profundus). Itcrosses superficially to the flexorretinaculum to terminate (superficialand deep terminal branches) over thepisiform bone. The supply is:● Muscular branches to – flexor
carpi ulnaris, flexor digitorumprofundus (medial half) andintrinsic hand muscles (exceptlateral two lumbricals and thenarmuscles)
● Sensory branches to – front andback aspects of medial hand andmedial one and a half fingers
● Palmar cutaneous branch – arisesin the mid-forearm and suppliesthe hypothenar skin
● Dorsal branch – also arises in themid-forearm and supplies theulnar border of the hand
● Terminal branches supplysensation as above (superficialbranch) and motor to hypothenarmuscles (three), ulnar twolumbricals, interossei and adductorpollicis
LOWER LIMB
1. Femoral nerve – derived from L2–4and formed within the psoas major. Itdescends between the psoas major(laterally) and iliacus, and enters thethigh lateral to the femoral artery andunder the inguinal ligament. Withinthe femoral triangle it splitsimmediately into its terminal branches,via the anterior and posteriordivisions. The femoral nerve supplies:● Muscular branches to – pectineus
and sartorius (anterior), andquadriceps femoris (posterior)
● Sensory branches – intermediatecutaneous nerve of thigh andmedial cutaneous nerve of thigh(anterior), and the terminalsaphenous nerve (posterior)
● Saphenous nerve – largest branchof the femoral nerve runs initiallylateral and then medial over thefemoral artery and descendsbetween the sartorius and gracilis.It runs down the medial border ofthe tibia to pass anterior to themedial malleolus and terminates inbranches to the foot. It supplies anextensive area of sensation to themedial aspect of the knee, lowerleg, ankle and foot
2. Obturator nerve – derived from L2–4and continues from its formationwithin the psoas major along the62
Concise Anatomy for Anaesthesia
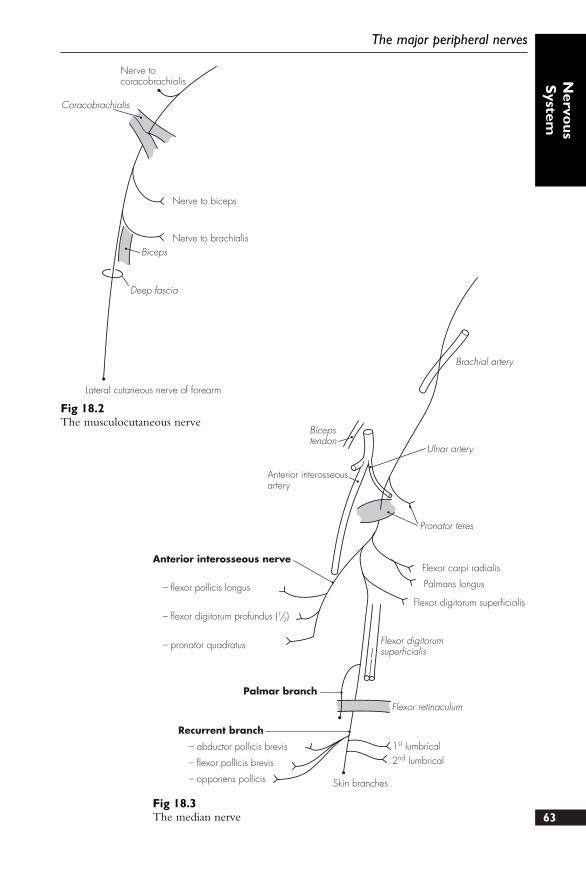
63
The major peripheral nerves
Nervo
usS
ystem
Bicepstendon
Brachial artery
Anterior interosseousartery
Anterior interosseous nerve
Palmar branch
– flexor pollicis longus
– flexor digitorum profundus (1/2)
– pronator quadratus
Recurrent branch
– abductor pollicis brevis
– flexor pollicis brevis
– opponens pollicis Skin branches
Flexor retinaculum
Flexor digitorumsuperficialis
1st lumbrical2nd lumbrical
Flexor digitorum superficialis
Palmans longus
Flexor carpi radialis
Pronator teres
Ulnar artery
Fig 18.3The median nerve
Nerve tocoracobrachialis
Nerve to biceps
Nerve to brachialisBiceps
Deep fascia
Lateral cutaneous nerve of forearm
Coracobrachialis
Fig 18.2The musculocutaneous nerve
pelvic sidewall and posterior to thecommon iliac vessels. After passingover the pelvic brim, it enters theobturator canal and divides intoanterior and posterior divisions. Itsupplies:● Muscular branches to – adductor
longus and brevis, pectineus andgracilis (anterior), and obturatorexternus and half adductor magnus(posterior)
● Sensory branches to – hip jointand medial skin over thigh(anterior) and knee joint(posterior)
3. Sciatic nerve – formed from L4 andL5 and S1–3 (on pyriformis) andpasses back through the greater sciaticforamen and lies deep to the gluteusmaximus. It runs down on thegemellus superior and inferior, andlies initially posterior to theacetabulum. From a point midwaybetween the greater trochanter andischial tuberosity, it runs directlydown on the quadratus femoris andadductor magnus. It passes betweenthe two heads of the biceps femorisand continues in the posteriormidline of the thigh. It terminates inthe common peroneal and tibialnerves above the knee. The sciaticnerve supplies:● Muscular branches to –
semitendinosus,semimembranosus, adductormagnus (half) and biceps femoris
● Nerve to quadratus femoris – alsoinferior gemellus and sensory tothe hip joint
● Nerve to obturator internus – alsosuperior gemellus
4. Tibial nerve – arises in the lowerthird of the thigh as the terminalbranch of the sciatic nerve. It passesdown through the popliteal fossa,deep to and between thesemimembranosus and biceps femoris.
It leaves the fossa between the headsof the gastrocnemius to run on thetibialis posterior in the calf, graduallysloping medially. It winds behind themedial malleolus (with the posteriortibial artery medially and flexorhallucis longus tendon laterally) toenter the foot under the flexorretinaculum, and terminates into themedial and lateral plantar nerves. Thenerve supplies:● Muscular branches to – popliteus,
gastrocnemius, soleus and plantaris(in popliteal fossa), and tibialisposterior, flexor digitorum longus,flexor hallucis longus and soleus(in the calf and foot)
● Sensory branches to – sural nerve(in popliteal fossa) and medialcalcaneal nerve (foot)
● Sural nerve – arises from thepopliteal fossa and becomessuperficial to run laterally downthe lower leg. It passes behind thelateral malleolus to supplysensation to the lateral foot
● Terminal branches supply the footvia the medial and lateral plantarbranches. The sensory supply is tothe medial two-thirds of the soleof the foot and plantar medialthree and a half toes (medialplantar) and lateral one-third ofthe sole of the foot and plantarlateral one and a half toes (lateralplantar). Together with thebranches of the common peronealnerve they supply the intrinsicmuscles of the foot
5. Common peroneal nerve – derivedfrom the sciatic nerve in the lowerthird of the thigh. It runs in thelateral part of the popliteal fossabefore winding around the neck ofthe fibula. It then divides (deep toperoneus longus) into two branches –superficial peroneal and deepperoneal nerves. It supplies:64
Concise Anatomy for Anaesthesia
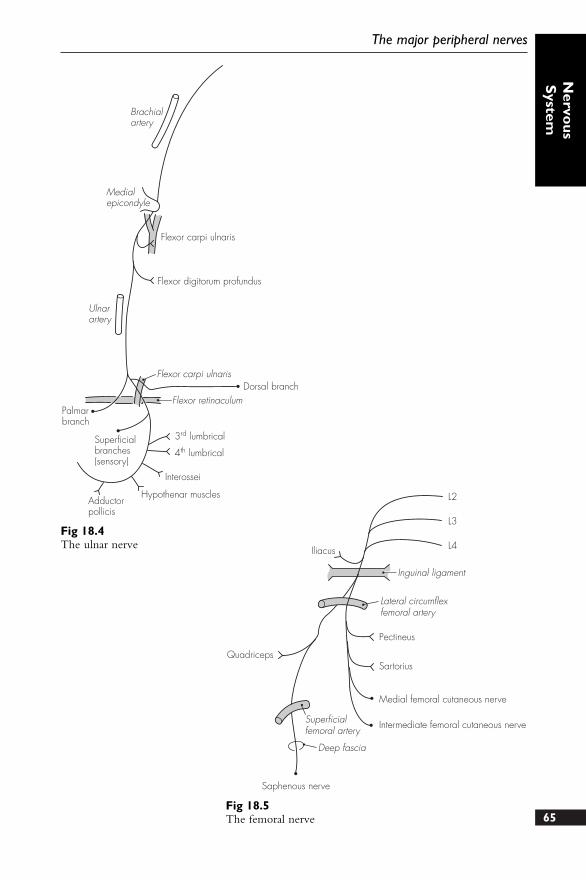
65
The major peripheral nerves
Nervo
usS
ystemBrachialartery
Flexor carpi ulnaris
Flexor digitorum profundus
Ulnarartery
Palmarbranch
Flexor carpi ulnaris
Flexor retinaculumDorsal branch
Superficialbranches(sensory)
3rd lumbrical
4th lumbrical
Interossei
Hypothenar musclesAdductorpollicis
Medialepicondyle
Fig 18.4The ulnar nerve Iliacus
L2
L3
L4
Inguinal ligament
Lateral circumflexfemoral artery
Pectineus
Sartorius
Medial femoral cutaneous nerve
Intermediate femoral cutaneous nerve
Saphenous nerve
Deep fascia
Superficialfemoral artery
Quadriceps
Fig 18.5The femoral nerve
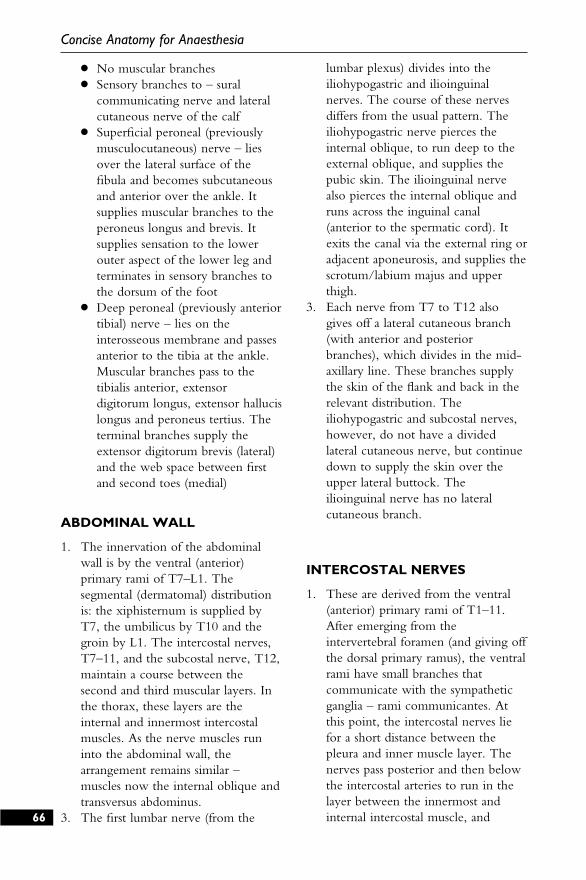
● No muscular branches● Sensory branches to – sural
communicating nerve and lateralcutaneous nerve of the calf
● Superficial peroneal (previouslymusculocutaneous) nerve – liesover the lateral surface of thefibula and becomes subcutaneousand anterior over the ankle. Itsupplies muscular branches to theperoneus longus and brevis. Itsupplies sensation to the lowerouter aspect of the lower leg andterminates in sensory branches tothe dorsum of the foot
● Deep peroneal (previously anteriortibial) nerve – lies on theinterosseous membrane and passesanterior to the tibia at the ankle.Muscular branches pass to thetibialis anterior, extensordigitorum longus, extensor hallucislongus and peroneus tertius. Theterminal branches supply theextensor digitorum brevis (lateral)and the web space between firstand second toes (medial)
ABDOMINAL WALL
1. The innervation of the abdominalwall is by the ventral (anterior)primary rami of T7–L1. Thesegmental (dermatomal) distributionis: the xiphisternum is supplied byT7, the umbilicus by T10 and thegroin by L1. The intercostal nerves,T7–11, and the subcostal nerve, T12,maintain a course between thesecond and third muscular layers. Inthe thorax, these layers are theinternal and innermost intercostalmuscles. As the nerve muscles runinto the abdominal wall, thearrangement remains similar –muscles now the internal oblique andtransversus abdominus.
3. The first lumbar nerve (from the
lumbar plexus) divides into theiliohypogastric and ilioinguinalnerves. The course of these nervesdiffers from the usual pattern. Theiliohypogastric nerve pierces theinternal oblique, to run deep to theexternal oblique, and supplies thepubic skin. The ilioinguinal nervealso pierces the internal oblique andruns across the inguinal canal(anterior to the spermatic cord). Itexits the canal via the external ring oradjacent aponeurosis, and supplies thescrotum/labium majus and upperthigh.
3. Each nerve from T7 to T12 alsogives off a lateral cutaneous branch(with anterior and posteriorbranches), which divides in the mid-axillary line. These branches supplythe skin of the flank and back in therelevant distribution. Theiliohypogastric and subcostal nerves,however, do not have a dividedlateral cutaneous nerve, but continuedown to supply the skin over theupper lateral buttock. Theilioinguinal nerve has no lateralcutaneous branch.
INTERCOSTAL NERVES
1. These are derived from the ventral(anterior) primary rami of T1–11.After emerging from theintervertebral foramen (and giving offthe dorsal primary ramus), the ventralrami have small branches thatcommunicate with the sympatheticganglia – rami communicantes. Atthis point, the intercostal nerves liefor a short distance between thepleura and inner muscle layer. Thenerves pass posterior and then belowthe intercostal arteries to run in thelayer between the innermost andinternal intercostal muscle, and66
Concise Anatomy for Anaesthesia
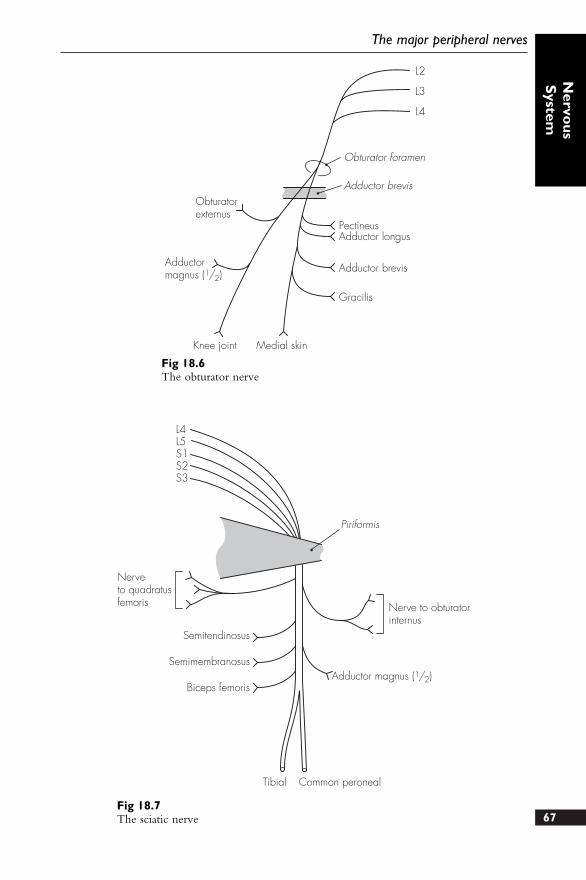
67
The major peripheral nerves
Nervo
usS
ystem
L2
L3
L4
Obturator foramen
Adductor brevis
PectineusAdductor longus
Adductor brevis
Gracilis
Knee joint Medial skin
Adductormagnus (1/2)
Obturatorexternus
Fig 18.6The obturator nerve
L4L5S1S2S3
Piriformis
Nerveto quadratusfemoris
Semitendinosus
Semimembranosus
Biceps femoris
Tibial Common peroneal
Adductor magnus (1/2)
Nerve to obturatorinternus
Fig 18.7The sciatic nerve
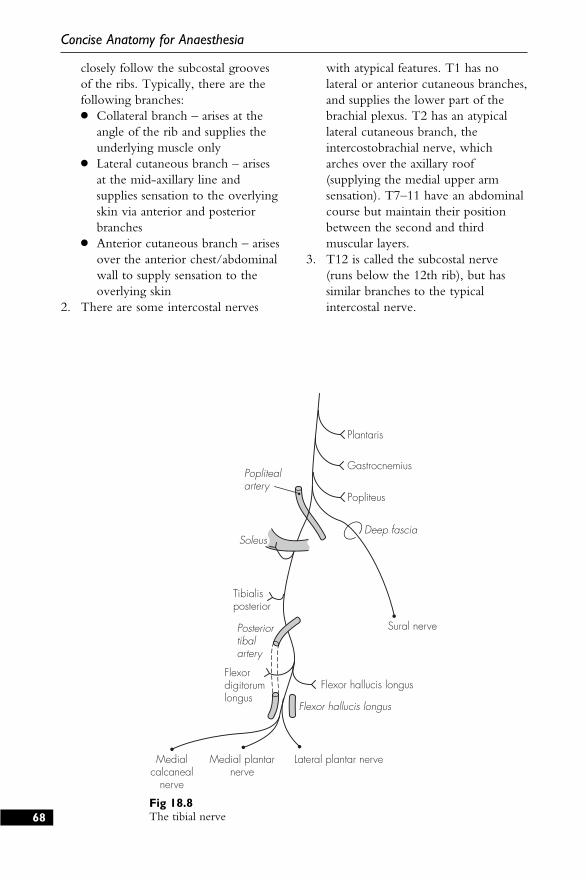
closely follow the subcostal groovesof the ribs. Typically, there are thefollowing branches:● Collateral branch – arises at the
angle of the rib and supplies theunderlying muscle only
● Lateral cutaneous branch – arisesat the mid-axillary line andsupplies sensation to the overlyingskin via anterior and posteriorbranches
● Anterior cutaneous branch – arisesover the anterior chest/abdominalwall to supply sensation to theoverlying skin
2. There are some intercostal nerves
with atypical features. T1 has nolateral or anterior cutaneous branches,and supplies the lower part of thebrachial plexus. T2 has an atypicallateral cutaneous branch, theintercostobrachial nerve, whicharches over the axillary roof(supplying the medial upper armsensation). T7–11 have an abdominalcourse but maintain their positionbetween the second and thirdmuscular layers.
3. T12 is called the subcostal nerve(runs below the 12th rib), but hassimilar branches to the typicalintercostal nerve.
68
Concise Anatomy for Anaesthesia
Plantaris
Gastrocnemius
Popliteus
Poplitealartery
Tibialisposterior
Sural nervePosteriortibalartery
Flexor hallucis longus
Flexor hallucis longus
Flexordigitorumlongus
Medialcalcaneal
nerve
Medial plantarnerve
Lateral plantar nerve
SoleusDeep fascia
Fig 18.8The tibial nerve
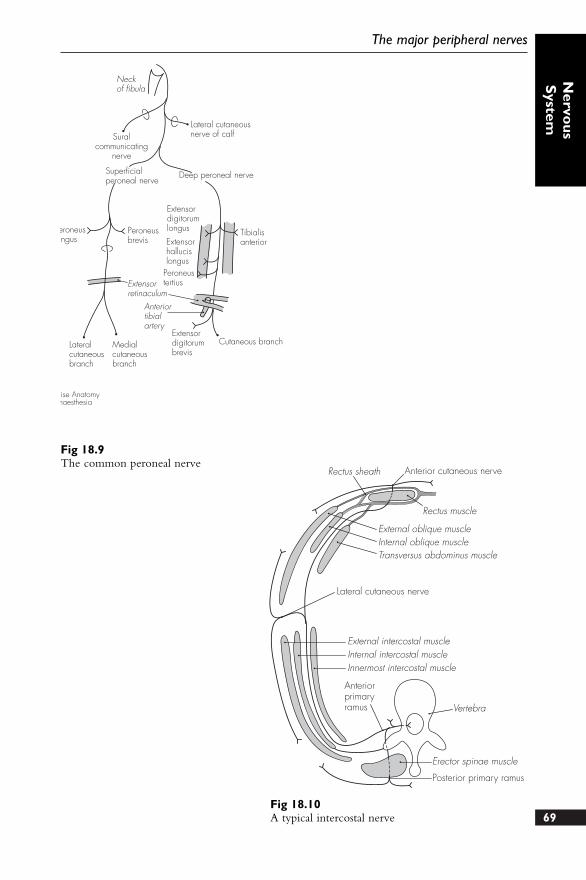
69
The major peripheral nerves
Nervo
usS
ystem
Suralcommunicating
nerve
Lateral cutaneousnerve of calf
Neckof fibula
Superficialperoneal nerve
Deep peroneal nerve
eroneusngus
Peroneusbrevis
Tibialisanterior
Extensordigitorumlongus
Extensorhallucislongus
PeroneustertiusExtensor
retinaculum
Lateralcutaneousbranch
Medialcutaneousbranch
Anteriortibialartery
Extensordigitorumbrevis
Cutaneous branch
ise Anatomynaesthesia
Fig 18.9The common peroneal nerve
Rectus sheath Anterior cutaneous nerve
Rectus muscle
External oblique muscleInternal oblique muscleTransversus abdominus muscle
Lateral cutaneous nerve
External intercostal muscleInternal intercostal muscleInnermost intercostal muscle
Anteriorprimaryramus Vertebra
Erector spinae muscle
Posterior primary ramus
Fig 18.10A typical intercostal nerve
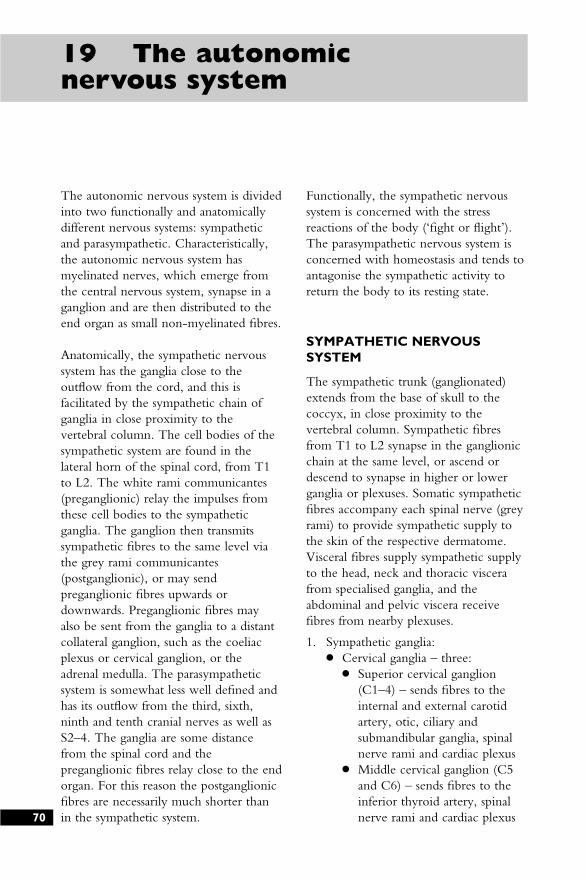
The autonomic nervous system is dividedinto two functionally and anatomicallydifferent nervous systems: sympatheticand parasympathetic. Characteristically,the autonomic nervous system hasmyelinated nerves, which emerge fromthe central nervous system, synapse in aganglion and are then distributed to theend organ as small non-myelinated fibres.
Anatomically, the sympathetic nervoussystem has the ganglia close to theoutflow from the cord, and this isfacilitated by the sympathetic chain ofganglia in close proximity to thevertebral column. The cell bodies of thesympathetic system are found in thelateral horn of the spinal cord, from T1to L2. The white rami communicantes(preganglionic) relay the impulses fromthese cell bodies to the sympatheticganglia. The ganglion then transmitssympathetic fibres to the same level viathe grey rami communicantes(postganglionic), or may sendpreganglionic fibres upwards ordownwards. Preganglionic fibres mayalso be sent from the ganglia to a distantcollateral ganglion, such as the coeliacplexus or cervical ganglion, or theadrenal medulla. The parasympatheticsystem is somewhat less well defined andhas its outflow from the third, sixth,ninth and tenth cranial nerves as well asS2–4. The ganglia are some distancefrom the spinal cord and thepreganglionic fibres relay close to the endorgan. For this reason the postganglionicfibres are necessarily much shorter thanin the sympathetic system.
Functionally, the sympathetic nervoussystem is concerned with the stressreactions of the body (‘fight or flight’).The parasympathetic nervous system isconcerned with homeostasis and tends toantagonise the sympathetic activity toreturn the body to its resting state.
SYMPATHETIC NERVOUSSYSTEM
The sympathetic trunk (ganglionated)extends from the base of skull to thecoccyx, in close proximity to thevertebral column. Sympathetic fibresfrom T1 to L2 synapse in the ganglionicchain at the same level, or ascend ordescend to synapse in higher or lowerganglia or plexuses. Somatic sympatheticfibres accompany each spinal nerve (greyrami) to provide sympathetic supply tothe skin of the respective dermatome.Visceral fibres supply sympathetic supplyto the head, neck and thoracic viscerafrom specialised ganglia, and theabdominal and pelvic viscera receivefibres from nearby plexuses.
1. Sympathetic ganglia:● Cervical ganglia – three:
● Superior cervical ganglion(C1–4) – sends fibres to theinternal and external carotidartery, otic, ciliary andsubmandibular ganglia, spinalnerve rami and cardiac plexus
● Middle cervical ganglion (C5and C6) – sends fibres to theinferior thyroid artery, spinalnerve rami and cardiac plexus70
19 The autonomicnervous system
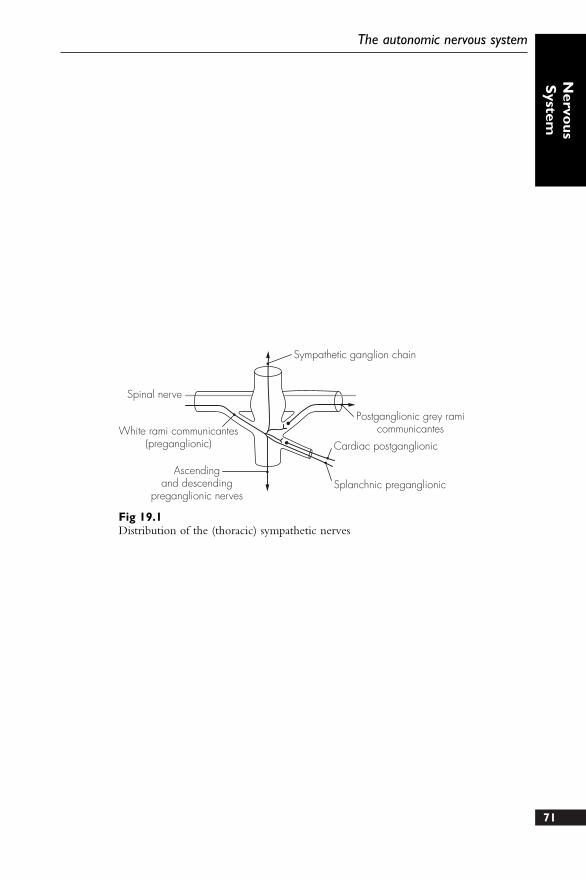
71
The autonomic nervous system
Nervo
usS
ystem
Spinal nerve
Sympathetic ganglion chain
White rami communicantes(preganglionic)
Ascendingand descending
preganglionic nerves
Postganglionic grey ramicommunicantes
Cardiac postganglionic
Splanchnic preganglionic
Fig 19.1Distribution of the (thoracic) sympathetic nerves
● Inferior cervical ganglion (C7and C8) – sends fibres to thevertebral artery, spinal nerverami and cardiac plexus.However, in 80% of cases, it isfused with T1 to form thestellate ganglion
● Stellate ganglion – formed fromC7 to T1. It has a closeanatomical relationship with thelower sympathetic chain. It ispositioned anterior and betweenthe transverse process of T7 andthe first rib, and lies behind thevertebral artery. Stellate ganglionblockade may be performed withthe head in full extension. Thetransverse process of C7 is usuallyeasily palpated with firm pressure3 cm above the sternoclavicularjoint. The needle is inserted atright angles to the skin, and withthe sternomastoid muscle andcarotid artery retracted laterally,the transverse process is met ~3cm from the skin. The localanaesthetic is then injected, aftercareful aspiration
● Thoracic ganglia – usually 12.They supply fibres to the aorta,spinal nerve rami, three splanchnicnerves (greater, lesser, lowest) andthe cardiac, pulmonary andoesophageal plexuses
● Lumbar ganglia – usually four.Branches go to the aortic andhypogastric plexuses, and lumbarspinal nerves
● Sacral ganglia – four. Supply pelvicplexuses and sacral spinal nerves
2. Sympathetic plexuses:● Cardiac plexus:
● Deep cardiac plexus lies infront of the tracheal bifurcationand receives branches from thecervical and upper four thoracicganglia as well as the vagalbranches
● Superficial cardiac plexus liesanterior to the pulmonaryartery and under the aorticarch. It receives the upper rightcervical ganglion branches andthe left vagus lower cardiacbranch
● Coeliac plexus – largestsympathetic plexus. It is found as adense network of fibres anterior tothe aorta, around the origin of thecoeliac artery (at L1). It liesbehind the superior border of thepancreas and the stomach. Itreceives the greater, lesser andlowest splanchnic nerves and thecoeliac branch of the right vagus.Some fibres relay directly to theadrenal medulla, and theremainder descend down the aortato form the aortic plexus. Theceliac plexus may be also beblocked, usually with the patientprone. A long spinal needle isinserted ~6 cm from the midline,at the lower costal margin. Theneedle is angled towards the firstlumbar vertebral body and ‘slippedoff’ anteriorly for a short distance.Careful aspiration should precedethe injection (the aortic pulsationcan frequently be felt)
● Hypogastric plexus – lies on thesacral promontory between thecommon iliac arteries. It receivesthe presacral nerves (from lumbartrunks and aortic plexus) and thesympathetic nerves spread furtherto the pelvis plexuses
PARASYMPATHETIC NERVOUSSYSTEM
The parasympathetic nervous system hascranial and sacral components:
1. Cranial – conveyed in cranial nervesIII, VII, IX and X. The functions72
Concise Anatomy for Anaesthesia
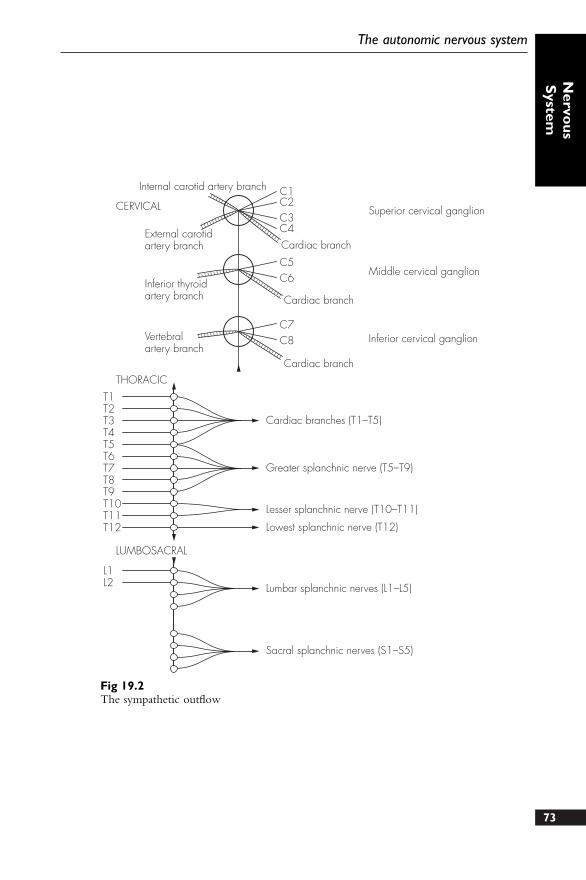
73
The autonomic nervous system
Nervo
usS
ystem
T1T2T3T4T5T6T7T8T9T10T11T12
L1L2
C1C2C3
C5C6
C7C8
C4
Internal carotid artery branch
External carotidartery branch
Inferior thyroidartery branch
Cardiac branch
Cardiac branch
Cardiac branch
Vertebralartery branch
Superior cervical ganglion
Middle cervical ganglion
Inferior cervical ganglion
Cardiac branches (T1–T5)
Greater splanchnic nerve (T5–T9)
Lesser splanchnic nerve (T10–T11)
Lowest splanchnic nerve (T12)
Lumbar splanchnic nerves (L1–L5)
Sacral splanchnic nerves (S1–S5)
CERVICAL
THORACIC
LUMBOSACRAL
Fig 19.2The sympathetic outflow
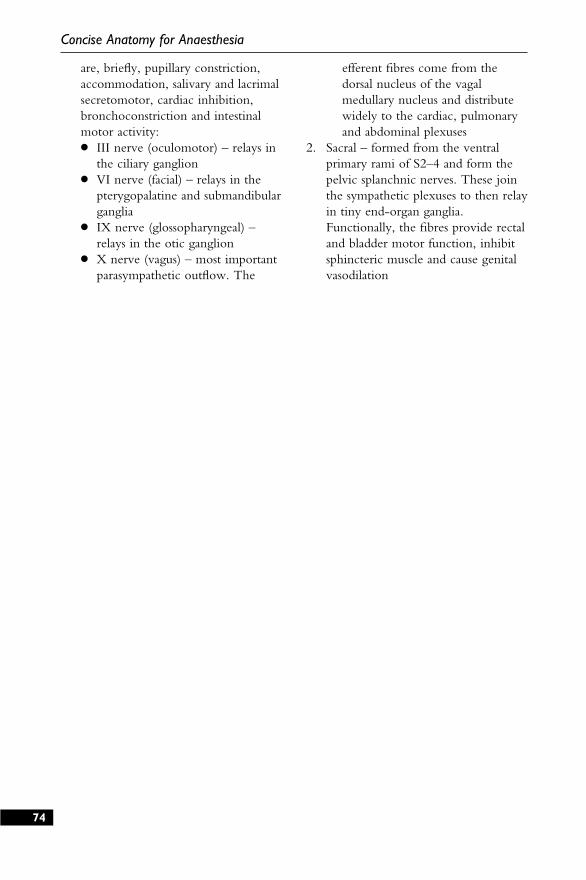
are, briefly, pupillary constriction,accommodation, salivary and lacrimalsecretomotor, cardiac inhibition,bronchoconstriction and intestinalmotor activity:● III nerve (oculomotor) – relays in
the ciliary ganglion● VI nerve (facial) – relays in the
pterygopalatine and submandibularganglia
● IX nerve (glossopharyngeal) –relays in the otic ganglion
● X nerve (vagus) – most importantparasympathetic outflow. The
efferent fibres come from thedorsal nucleus of the vagalmedullary nucleus and distributewidely to the cardiac, pulmonaryand abdominal plexuses
2. Sacral – formed from the ventralprimary rami of S2–4 and form thepelvic splanchnic nerves. These jointhe sympathetic plexuses to then relayin tiny end-organ ganglia.Functionally, the fibres provide rectaland bladder motor function, inhibitsphincteric muscle and cause genitalvasodilation
74
Concise Anatomy for Anaesthesia
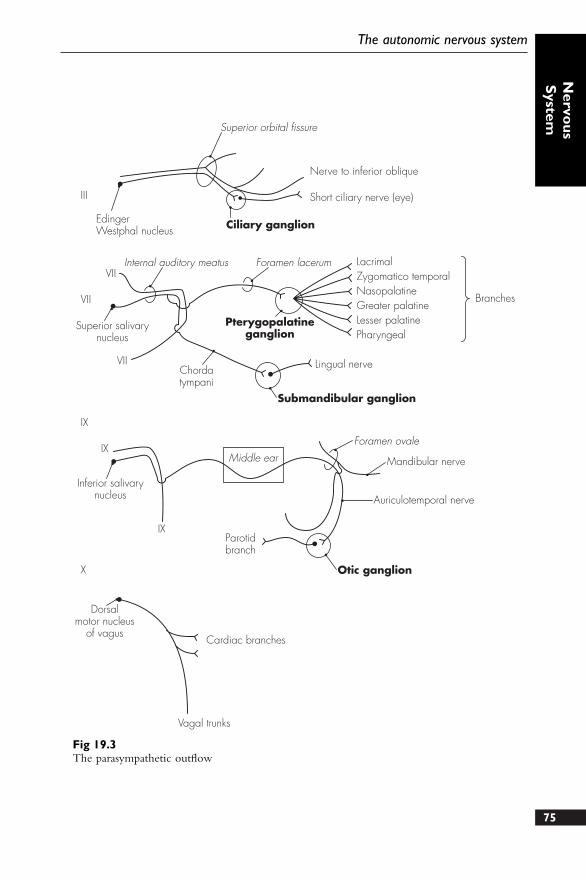
75
The autonomic nervous system
Nervo
usS
ystem
Superior orbital fissure
Nerve to inferior oblique
Short ciliary nerve (eye)
Ciliary ganglionEdingerWestphal nucleus
Internal auditory meatus
Superior salivarynucleus
Chordatympani
Pterygopalatineganglion
Foramen lacerum LacrimalZygomatico temporalNasopalatineGreater palatineLesser palatinePharyngeal
Branches
Lingual nerve
Submandibular ganglion
Inferior salivarynucleus
Middle ear
Foramen ovale
Mandibular nerve
Auriculotemporal nerve
Otic ganglion
Parotidbranch
Dorsalmotor nucleus
of vagusCardiac branches
Vagal trunks
III
VII
VII
VII
IX
IX
IX
X
Fig 19.3The parasympathetic outflow

The cranial nerves can be thought of asthe peripheral nerves of the brain. Theseoriginate from cranial nerve nuclei,which are situated in the pons andmedulla (the embryological hindbrain).There are 12 cranial nerves, of whichtwo are somewhat atypical: the olfactorynerve (formed by extended olfactorysensory processes) and optic nerve (a tractdrawn out from the brain duringdevelopment).
1. Olfactory nerve (I) – consists of anolfactory tract with directconnections to the anterior part ofthe brain. The cribriform plate allowsthe olfactory sensory cells to passthrough, and these synapse with theolfactory bulb. The bulb leads to theolfactory tract, which runs on theinferior surface of the frontal lobe
2. Optic nerve (II) – fibres pass fromthe retina via the optic disc to theoptic nerve. This passes through theorbit within the muscle cone, andgoes through the optic foramen (inthe sphenoid bone), above theophthalmic artery, into the middlecranial fossa. Here it lies medial tothe anterior clinoid process beforerunning laterally and then superior tothe sella turcica. The optic chiasma isformed here, with the temporal fieldscrossing to the opposite side. Thenerves continue on each sidebetween the temporal uncus and thecerebral peduncle to reach the lateralgeniculate body (in the thalamus).Some fibres also extend to reach thesuperior colliculus, subserving the
ocular and papillary reflexes. Thelateral geniculate body then sendsfibres via the optic radiation to theoccipital cortex
3. Oculomotor nerve (III) – emergesmedial to the cerebral peduncle toreach the middle cranial fossa. It thenruns forward, close to the posteriorcommunicating artery, and piercesthe dura to enter the cavernous sinussuperiorly and laterally. It descendsmedial to the trochlear nerve andenters the orbit within the tendinousring and through the superior orbitalfissure. It divides into two divisions:● Superior – supplying superior
rectus and levator palpebraesuperioris
● Inferior – supplying medial rectus,inferior rectus and inferior oblique
In addition to the above muscularsupply, the oculomotor nerve alsocarries preganglionic fibres (topupillary sphincter and ciliary muscle)from the Edinger–Westphalparasympathetic nucleus. These relayin the ciliary ganglion situated in thelateral orbit
4. Trochlear nerve (IV) – emerges (afterdecussating in the midbrain) lateral tothe superior cerebellar peduncle. Itruns into the mid-cranial fossa,between the superior cerebellar andposterior cerebral arteries, and entersthe cavernous sinus laterally. Here itlies below, and is crossed medially by,the III nerve. It runs through thesuperior orbital fissure and terminatesby supplying the superior obliquemuscle76
20 The cranial nerves
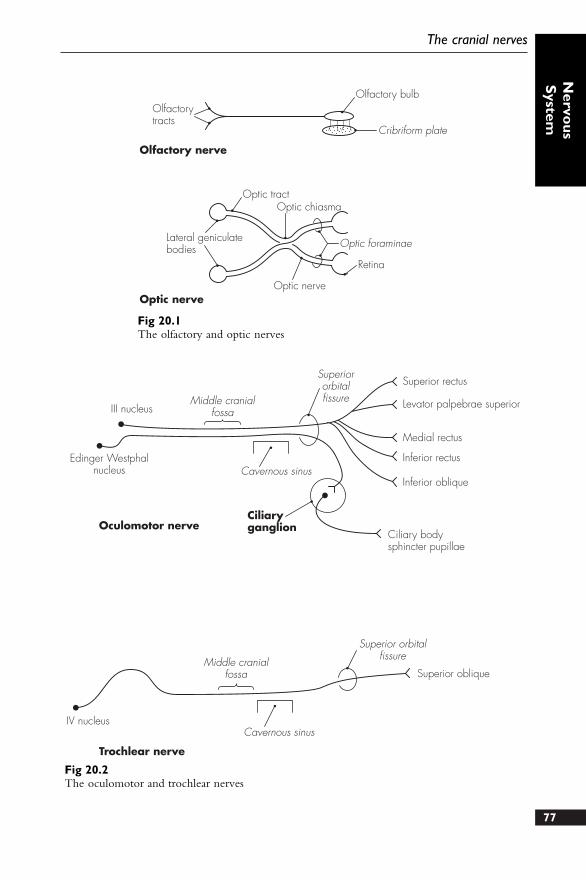
77
The cranial nerves
Nervo
usS
ystem
Olfactorytracts
Olfactory bulb
Cribriform plate
Olfactory nerve
Optic nerve
Optic tractOptic chiasma
Optic foraminae
Retina
Optic nerve
Lateral geniculatebodies
Fig 20.1The olfactory and optic nerves
III nucleusMiddle cranial
fossa
Middle cranialfossa
Superiororbitalfissure
Superior orbitalfissure
Superior rectus
Levator palpebrae superior
Medial rectus
Inferior rectus
Inferior oblique
Ciliary bodysphincter pupillae
Edinger Westphalnucleus Cavernous sinus
CiliaryganglionOculomotor nerve
Trochlear nerve
IV nucleus
Superior oblique
Cavernous sinus
Fig 20.2The oculomotor and trochlear nerves
5. Trigeminal nerve (V) – largest cranialnerve. It has a small motor and alarge sensory root and is associatedwith four autonomic ganglia. It isresponsible for the majority ofsensory supply to the face, nose,mouth and orbit, and supplies motorfibres to the muscles of mastication,posterior digastric, mylohyoid, tensorpalati and tensor tympani. It alsocommunicates with the ciliary,pterygopalatine, submandibular andotic ganglia. The motor nucleus issituated in the upper pons, just belowthe floor of the fourth ventricle. Thesensory nucleus is divided into threeparts: mesencephalic (high mid-brain), superior (upper pons) andspinal tract (runs parallel to the ponsand medulla nuclei). These nucleieach subserve different sensory inputs.The combined roots of the trigeminalnerve emerge from the ventrolateralaspect of the pons. The larger lateralsensory root develops a swelling after1 cm – the trigeminal ganglion:● Trigeminal ganglion – lies near
the apex of the petrous temporalbone (slightly hollowed). Themotor root of the trigeminal nerveruns beneath it, above it lies thetemporal lobe. Medially lie theposterior cavernous sinus andinternal carotid artery. Fibres passposteriorly below the superiorpetrosal sinus to reach the pons,and anteriorly the nerve dividesinto three divisions: ophthalmic,maxillary and mandibulardivisions. During local nerveblockade of the ganglion, theneedle is introduced below theposterior zygomatic bone andbehind the pterygoid plate. Theforamen ovale is locatedradiologically, and the needleadvanced through this to a furtherdepth of 1 cm. Dural puncture is
possible and careful aspiration isrequired, prior to injection
The three divisions of the trigeminalnerve are:
● Ophthalmic nerve – smallest ofthe three divisions. It providessensation only to the superiorface and anterior scalp. Prior toentering the orbit, theophthalmic nerve divides intothree branches – all of whichpass through the superiororbital fissure:Frontal nerve – divides into the
supra-orbital nerve (suppliesthe upper eyelid and scalp)and supratrochlear nerve(supplies the skin of theforehead)
Nasociliary nerve – branchesare long ciliary nerves(eyeball), ganglionic (ciliary),ethmoidal nerves (ethmoidand nasal cavity) andinfratrochlear nerve (lacrimalsac and eyelid)
Lacrimal nerve – supplies thelacrimal gland and uppereyelid
● Maxillary nerve – also purelysensory, to the mid-facialregion. It passes through theforamen rotundum into thepterygopalatine fossa and viathe fissure into theinfratemporal fossa. It exitsthrough the inferior orbitalfossa and continues as the infra-orbital nerve. The maxillarynerve has numerous branchesduring its course:Meningeal branches – within
the cranium (dura mater)Ganglionic branches – within
the pterygopalatine fossa (tothe pterygopalatine ganglion)
Zygomatic nerve – within thepterygopalatine fossa into78
Concise Anatomy for Anaesthesia
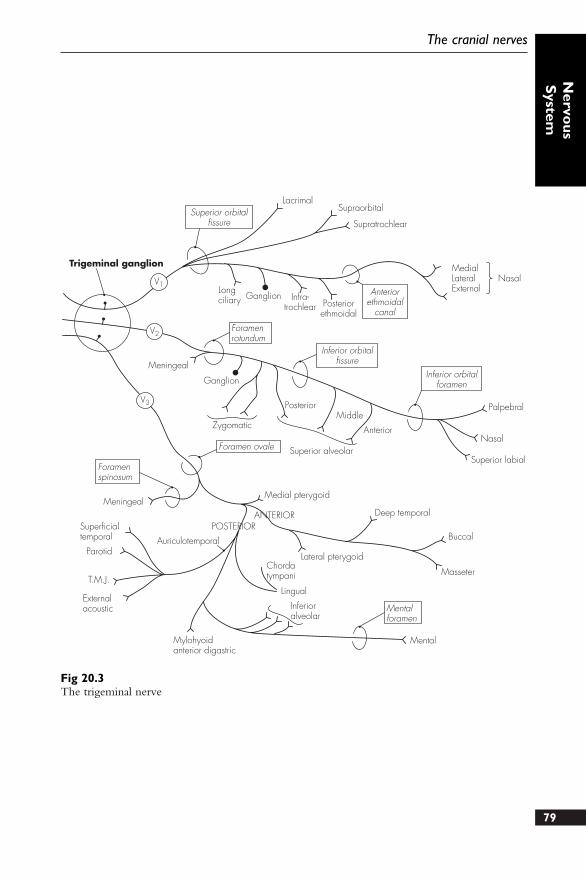
79
The cranial nerves
Nervo
usS
ystem
Trigeminal ganglion
Superior orbitalfissure
LacrimalSupraorbital
Supratrochlear
Longciliary Ganglion Infra-
trochlear Posteriorethmoidal
Anteriorethmoidal
canal
MedialLateralExternal
Nasal
Meningeal
Foramenrotundum
Ganglion
Foramenspinosum
Zygomatic
PosteriorMiddle
Anterior
Superior alveolarForamen ovale
Meningeal
Superficialtemporal
Parotid
T.M.J.
Externalacoustic
Mylohyoidanterior digastric
Chordatympani
Auriculotemporal
POSTERIORANTERIOR
Medial pterygoid
Deep temporal
Lateral pterygoid
Lingual
Inferioralveolar
Mentalforamen
Mental
Buccal
Masseter
Superior labial
Nasal
Palpebral
Inferior orbitalforamen
Inferior orbitalfissure
V1
V2
V3
Fig 20.3The trigeminal nerve
two branches (-facial and -temporal – to the cheek andtemple)
Posterior superior alveolarnerve – within thepterygopalatine fossa (to themaxillary sinus, maxillarymolar, cheek and gums)
Middle superior alveolar nerve– from the infra-orbitalnerve (to the maxillary sinusand upper premolar tooth)
Anterior superior alveolar nerve– from the infra-orbitalnerve (to the maxillary sinusand canine and incisor teeth)
Infra-orbital nerve (terminal) –divides into the palpebral,nasal and superior labialbranches
● Mandibular nerve – sensoryand motor. The nerve exitsthrough the foramen ovale andgives off two branches (sensoryto the dura mater, motor to themedial pterygoid muscle),before bifurcating into theanterior (small) and posterior(large) trunks:Anterior trunk – gives off:
Buccal nerve (sensory to thecheek)
Masseteric nerve (motor tothe masseter)
Deep temporal nerves(motor to the temporalis)
Nerve to lateral pterygoidPosterior trunk – gives off:
Auriculotemporal nerve (fiveterminal branches supplythe acoustic meatus andear fibres,temporomandibular joint,temporal skin and parotidparasympathetic)
Lingual nerve (joined by thechorda tympani (VII),sensory to the mucous
membrane of the mouth,tongue and gums)
Inferior alveolar nerve (lowerteeth and gums, thenthrough the mentalforamen to supply thelower lip/chin, also givesoff the nerve to themylohyoid)
6. Abducent nerve (VI) – emerges fromthe lower border of the pons andcrosses the pontine basal cisternbefore piercing the dura inferolateralto the sella turcica. Arching over thepetrous temporal bone, it runs on themedial wall of the cavernous sinusand lateral to the internal carotidartery. It enters the orbit through thesuperior orbital fissure to supply thelateral rectus muscle
7. Facial nerve (VII) – mixed nervewith complex arrangements. Itsupplies motor fibres to the musclesof expression, carries parasympatheticinnervation to the salivary, palatineand lacrimal glands, taste from theanterior two-thirds of the tongue andsensation to the external auditorymeatus, tympanic membrane and ear.It emerges from the pontomedullaryjunction as two roots – a visceralefferent root and a mixed nervusintermedius. It runs (together withthe VIIIth nerve) into the internalauditory meatus (in the posteriorpetrous bone), and runs in the facialcanal and then in the lateral middleear. A sharp bend in the tortuouscourse of the facial nerve (at themedial wall between the inner andmiddle ear) marks the site of thegeniculate (facial) ganglion. Thenerve continues down in thetympanic cavity posteriorly and exitsthrough the stylomastoid foramen.After winding laterally around thestyloid process, the facial nerve divesinto the posterior part of the parotid80
Concise Anatomy for Anaesthesia
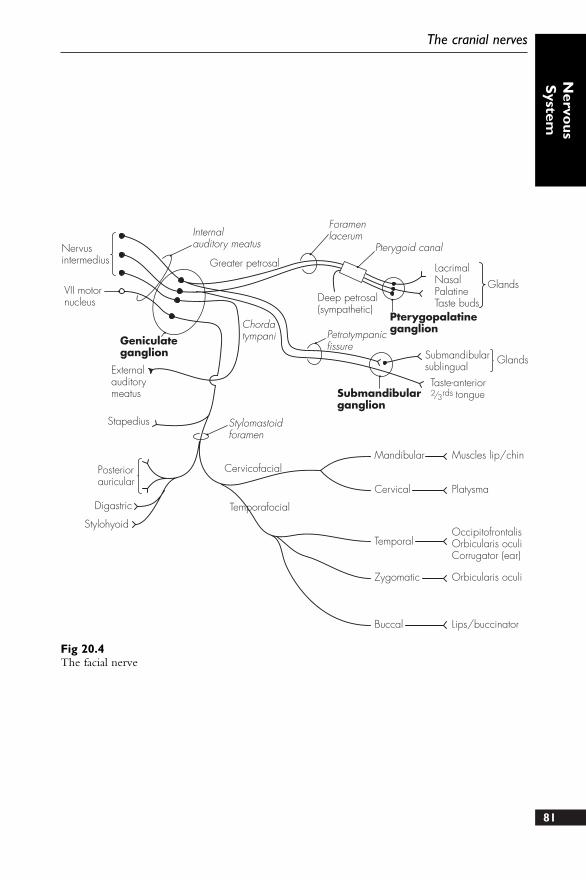
81
The cranial nerves
Nervo
usS
ystem
Nervusintermedius
VII motornucleus
Internalauditory meatus
Greater petrosal
Foramenlacerum
Pterygoid canal
LacrimalNasalPalatineTaste buds
GlandsDeep petrosal(sympathetic)
PterygopalatineganglionPetrotympanic
fissure
ChordatympaniGeniculate
ganglion
Externalauditorymeatus
Stapedius Stylomastoidforamen
Posteriorauricular
Digastric
Stylohyoid
Cervicofacial
Temporafocial
Submandibularganglion
Submandibularsublingual
Glands
Taste-anterior2/3rds tongue
Mandibular
Cervical
Temporal
Zygomatic
Buccal
Muscles lip/chin
Platysma
OccipitofrontalisOrbicularis oculiCorrugator (ear)
Orbicularis oculi
Lips/buccinator
Fig 20.4The facial nerve
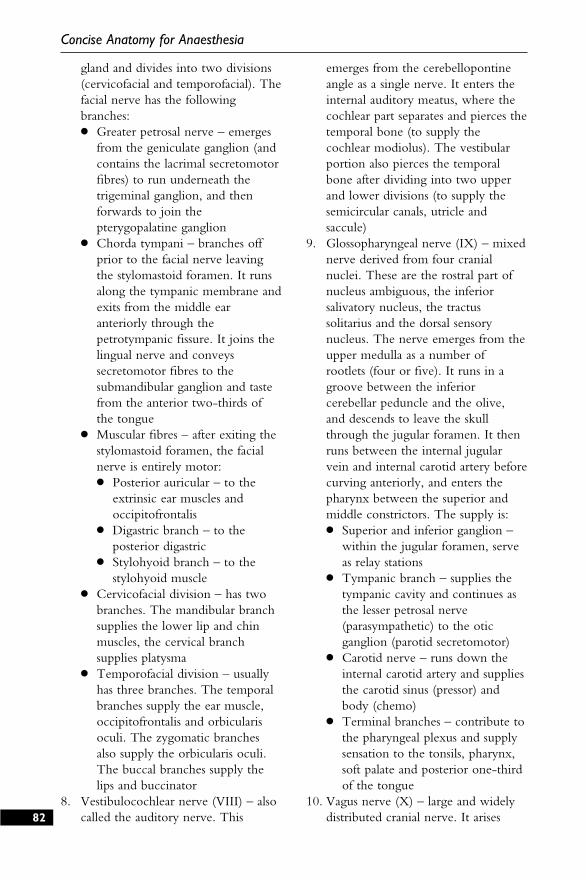
gland and divides into two divisions(cervicofacial and temporofacial). Thefacial nerve has the followingbranches:● Greater petrosal nerve – emerges
from the geniculate ganglion (andcontains the lacrimal secretomotorfibres) to run underneath thetrigeminal ganglion, and thenforwards to join thepterygopalatine ganglion
● Chorda tympani – branches offprior to the facial nerve leavingthe stylomastoid foramen. It runsalong the tympanic membrane andexits from the middle earanteriorly through thepetrotympanic fissure. It joins thelingual nerve and conveyssecretomotor fibres to thesubmandibular ganglion and tastefrom the anterior two-thirds ofthe tongue
● Muscular fibres – after exiting thestylomastoid foramen, the facialnerve is entirely motor:● Posterior auricular – to the
extrinsic ear muscles andoccipitofrontalis
● Digastric branch – to theposterior digastric
● Stylohyoid branch – to thestylohyoid muscle
● Cervicofacial division – has twobranches. The mandibular branchsupplies the lower lip and chinmuscles, the cervical branchsupplies platysma
● Temporofacial division – usuallyhas three branches. The temporalbranches supply the ear muscle,occipitofrontalis and orbicularisoculi. The zygomatic branchesalso supply the orbicularis oculi.The buccal branches supply thelips and buccinator
8. Vestibulocochlear nerve (VIII) – alsocalled the auditory nerve. This
emerges from the cerebellopontineangle as a single nerve. It enters theinternal auditory meatus, where thecochlear part separates and pierces thetemporal bone (to supply thecochlear modiolus). The vestibularportion also pierces the temporalbone after dividing into two upperand lower divisions (to supply thesemicircular canals, utricle andsaccule)
9. Glossopharyngeal nerve (IX) – mixednerve derived from four cranialnuclei. These are the rostral part ofnucleus ambiguous, the inferiorsalivatory nucleus, the tractussolitarius and the dorsal sensorynucleus. The nerve emerges from theupper medulla as a number ofrootlets (four or five). It runs in agroove between the inferiorcerebellar peduncle and the olive,and descends to leave the skullthrough the jugular foramen. It thenruns between the internal jugularvein and internal carotid artery beforecurving anteriorly, and enters thepharynx between the superior andmiddle constrictors. The supply is:● Superior and inferior ganglion –
within the jugular foramen, serveas relay stations
● Tympanic branch – supplies thetympanic cavity and continues asthe lesser petrosal nerve(parasympathetic) to the oticganglion (parotid secretomotor)
● Carotid nerve – runs down theinternal carotid artery and suppliesthe carotid sinus (pressor) andbody (chemo)
● Terminal branches – contribute tothe pharyngeal plexus and supplysensation to the tonsils, pharynx,soft palate and posterior one-thirdof the tongue
10. Vagus nerve (X) – large and widelydistributed cranial nerve. It arises82
Concise Anatomy for Anaesthesia
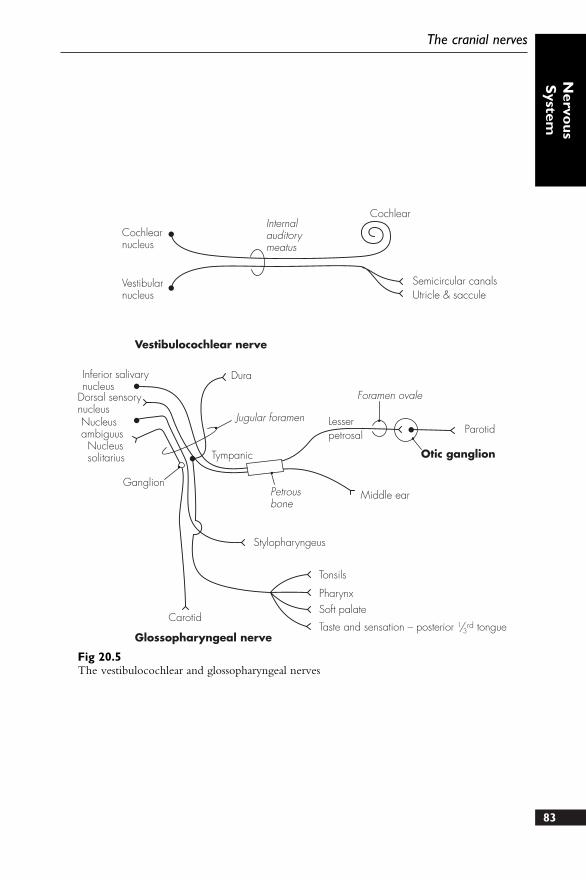
83
The cranial nerves
Nervo
usS
ystem
Cochlearnucleus
Vestibularnucleus
Internalauditorymeatus
Cochlear
Semicircular canalsUtricle & saccule
Vestibulocochlear nerve
Inferior salivarynucleus
Dorsal sensorynucleusNucleusambiguusNucleussolitarius
Dura
Jugular foramen
Tympanic
Ganglion
Lesserpetrosal
Foramen ovale
Parotid
Otic ganglion
Middle earPetrousbone
Stylopharyngeus
Tonsils
PharynxSoft palate
Taste and sensation – posterior 1/3rd tongue
Carotid
Glossopharyngeal nerve
Fig 20.5The vestibulocochlear and glossopharyngeal nerves
from three cranial nuclei: dorsalnucleus of vagus, nucleus ambiguusand nucleus of the tractus solitarius. Itemerges from the upper medullaalongside the glossopharyngeal nerveas a set of rootlets (nine or ten), andcontinues similarly in theposterolateral groove. The vagus soonforms a single trunk and exits theskull through the jugular foramen.Two small ganglia are present on thevagus nerve within the jugularforamen: superior (with cell bodiesfrom the ear and dura) and inferior(other afferents). The cranial part ofthe accessory nerve fuses with thevagus just below the jugular foramen.The distal course of the vagus nervediffers somewhat on each side. Bothvagi descend within the carotidsheath and lie in front of the cervicalsympathetic chain. On the right, thevagus descends in front of the rightsubclavian artery and gives off theright recurrent laryngeal nerve.Passing behind the rightbrachiocephalic vein, it descends intothe thorax against the trachea andbehind the root of the right lung. Itgives branches to the right posteriorpulmonary and oesophageal plexuses,and enters the abdomen behind theoesophageal hiatus. It proceeds togive branches to the upper stomachbefore forming the coeliac branch (tothe coeliac plexus). The left vagusruns down between the left carotidand left subclavian artery to passbehind the left brachiocephalic vein.It crosses over the aortic arch, givingoff the left recurrent nerve, anddescends into the thorax behind theleft lung root. Branches are also givento the posterior pulmonary andoesophageal plexuses, but the nervenow runs anteriorly and close to the
oesophagus through the oesophagealhiatus. Apart from branches to thelower stomach and pylorus, a hepaticbranch is also given off. The branchesof the vagus nerve are:● In jugular foramen – meningeal
and auricular branches● In neck – pharyngeal branch,
superior laryngeal nerve, rightrecurrent laryngeal nerve andcardiac branches
● In thorax – cardiac branches, leftrecurrent laryngeal nerve,pulmonary, pericardial andoesophageal branches
● In abdomen – gastric, hepatic andcoeliac branches
11. Accessory nerve (XI) – derived fromtwo roots, a cranial (from nucleusambiguus) and a spinal root (from C1to C5). After emerging as numerousrootlets behind the olive, the nervefuses with the spinal root (havingascended through foramen magnum)and exits the skull through thejugular foramen. The cranial rootjoins the vagus, and the spinal rootdescends laterally in front of the atlasto supply motor fibres to thesternocleidomastoid and trapezius
12. Hypoglossal nerve (XII) – emerges asa series of small rootlets from theanterolateral medulla. These fusealong their course behind thevertebral artery and into thehypoglossal canal. It emergesanteriorly and laterally to the neckvessels, before passing over the hyoidgreater cornu, and terminates underthe submandibular gland. Thehypoglossal nerve supplies motorfibres to the intrinsic muscles of thetongue, hyoglossus, genioglossus andstyloglossus (as well as receiving fibresfrom the cervical ventral rami fordistribution to the neck muscles)
84
Concise Anatomy for Anaesthesia
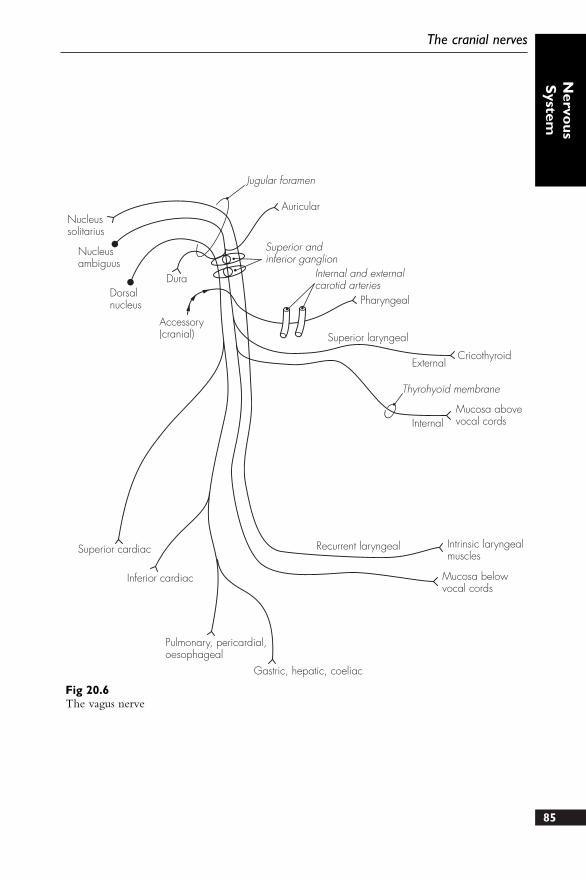
85
Nervo
usS
ystemThe cranial nerves
Nucleussolitarius
Nucleusambiguus
Dorsalnucleus
Jugular foramen
Auricular
Dura
Accessory(cranial)
Superior andinferior ganglion
Internal and externalcarotid arteries
Pharyngeal
Superior laryngeal
External
Internal
Thyrohyoid membrane
Mucosa abovevocal cords
Superior cardiac
Inferior cardiac
Pulmonary, pericardial,oesophageal
Gastric, hepatic, coeliac
Recurrent laryngeal Intrinsic laryngealmuscles
Mucosa belowvocal cords
Cricothyroid
Fig 20.6The vagus nerve
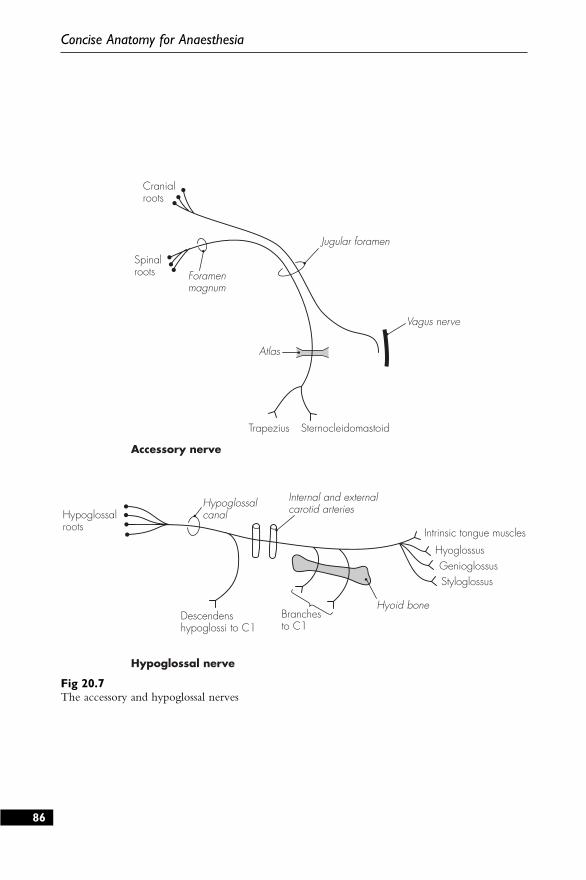
86
Concise Anatomy for Anaesthesia
Cranialroots
Spinalroots Foramen
magnum
Jugular foramen
Atlas
Vagus nerve
Trapezius Sternocleidomastoid
Accessory nerve
Hypoglossal nerve
Hypoglossalroots
Hypoglossalcanal
Internal and externalcarotid arteries
Intrinsic tongue muscles
HyoglossusGenioglossusStyloglossus
Hyoid boneBranchesto C1
Descendenshypoglossi to C1
Fig 20.7The accessory and hypoglossal nerves

Appendices
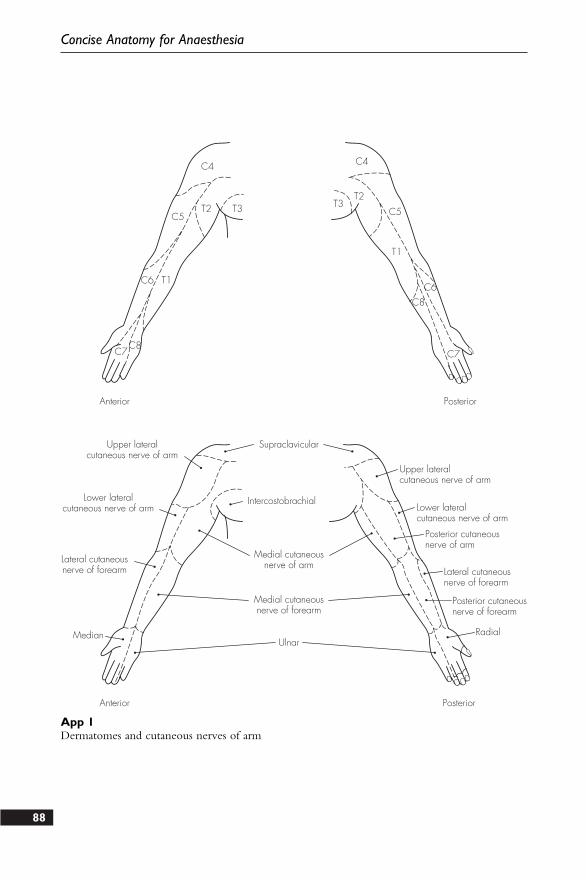
88
Concise Anatomy for Anaesthesia
C7C8
C6 T1C6
C8
C7
T1
C5 C5T2T2
T3 T3
C4 C4
Anterior
Anterior
Posterior
Posterior
SupraclavicularUpper lateralcutaneous nerve of arm
Lower lateralcutaneous nerve of arm
Lateral cutaneousnerve of forearm
Intercostobrachial
Medial cutaneousnerve of arm
Medial cutaneousnerve of forearm
UlnarMedian
Upper lateralcutaneous nerve of arm
Lower lateralcutaneous nerve of arm
Posterior cutaneousnerve of arm
Lateral cutaneousnerve of forearm
Posterior cutaneousnerve of forearm
Radial
App 1Dermatomes and cutaneous nerves of arm
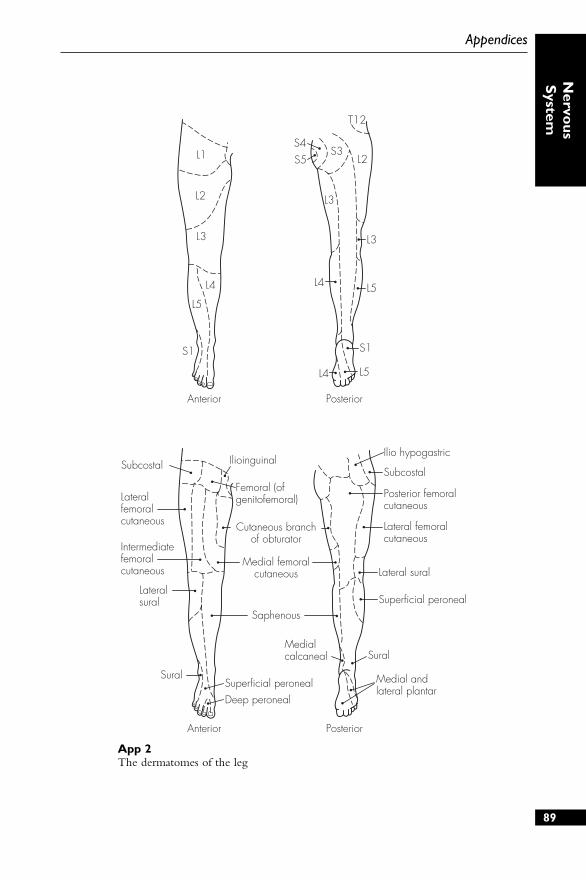
L1
L2
L3
L5
S1
L4
L4 L5
S1
L5L4
L3
L3
S5S4
S3
T12
L2
Anterior Posterior
Anterior Posterior
Subcostal
Lateralfemoralcutaneous
Intermediatefemoralcutaneous
Lateralsural
Sural
Deep peronealSuperficial peroneal
Ilioinguinal
Femoral (ofgenitofemoral)
Cutaneous branchof obturator
Medial femoralcutaneous
Saphenous
Medialcalcaneal Sural
Medial andlateral plantar
Superficial peroneal
Lateral sural
Lateral femoralcutaneous
Posterior femoralcutaneous
Subcostal
Ilio hypogastric
89
Appendices
Nervo
usS
ystem
App 2The dermatomes of the leg
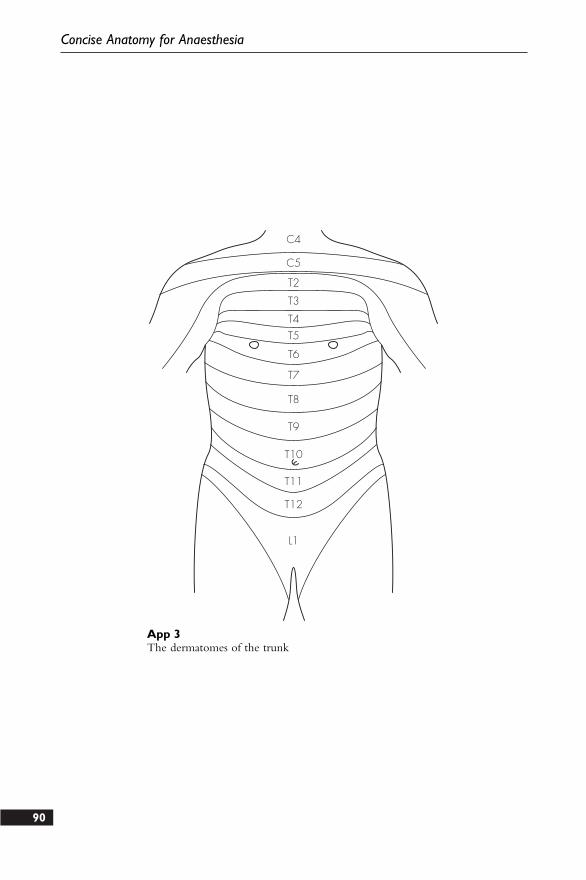
90
Concise Anatomy for Anaesthesia
C4
C5
T2
T3
T4T5
T6
T7
T8
T9
T10
T11
T12
L1
App 3The dermatomes of the trunk

91
1. Describe, with the aid of a diagram,the blood supply to the brain.
2. Using a simple diagram, detail thepath of a typical intercostal nervefrom its origin to its terminalbranches.
3. What is the nerve supply of theabdominal wall?
4. Draw a cross-sectional labelleddiagram of the spinal column toillustrate the relationships of theepidural space.
5. Discuss, in point form, the anatomyof the brachial plexus. Brieflydescribe one method of performing abrachial plexus nerve block.
6. Describe how you would carry outan axillary brachial plexus nerveblock.
7. Draw a labelled diagram of therelations of the stellate ganglion.How is it blocked and what are thepossible complications?
8. Describe your technique for a coeliacplexus block with reference to theimportant anatomical features.
9. How is an ankle block performed?Explain how the sensory innervationof the foot is related to individualnerves.
10. Describe the course of thefemoral/sciatic nerve. How do youperform a femoral/sciatic nerveblock?
11. Draw a labelled diagram of theanterior aspect of the wrist. Howmay this knowledge be of use inanaesthetic practice?
Sample questions –nervous system

91
1. Describe, with the aid of a diagram,the blood supply to the brain.
2. Using a simple diagram, detail thepath of a typical intercostal nervefrom its origin to its terminalbranches.
3. What is the nerve supply of theabdominal wall?
4. Draw a cross-sectional labelleddiagram of the spinal column toillustrate the relationships of theepidural space.
5. Discuss, in point form, the anatomyof the brachial plexus. Brieflydescribe one method of performing abrachial plexus nerve block.
6. Describe how you would carry outan axillary brachial plexus nerveblock.
7. Draw a labelled diagram of therelations of the stellate ganglion.How is it blocked and what are thepossible complications?
8. Describe your technique for a coeliacplexus block with reference to theimportant anatomical features.
9. How is an ankle block performed?Explain how the sensory innervationof the foot is related to individualnerves.
10. Describe the course of thefemoral/sciatic nerve. How do youperform a femoral/sciatic nerveblock?
11. Draw a labelled diagram of theanterior aspect of the wrist. Howmay this knowledge be of use inanaesthetic practice?
Sample questions –nervous system
VertebralColumn
1. Vertebral column – midline structureextending from the base of the skullabove to the pelvis below. It providesprotection for the spinal cord andtransfers weight through the pelvis, aswell as having an extensive area formuscular attachment. It consists ofbony vertebrae connected byintervertebral fibrocartilaginous discs
2. Twenty-four true vertebrae – sevencervical, 12 thoracic and five lumbar.There are nine false vertebrae, whichconsist of the sacrum (five fusedvertebrae) and the vestigial coccyx(four fused vertebrae)
3. Vertebral column – also has anumber of curved segments. In theadult, there are two areas that areconvex anteriorly: cervical andlumbar curvatures. The thoracic andsacral areas show anteriorly concavecurvatures
DESCRIPTION
A typical vertebra has an anterior bodyand a posterior neural arch. The lumbarbodies are the largest, having to supportproportionately more weight. Thevertebral bodies are each separated by atough fibrocartiligenous disc. The neuralarch is connected to the vertebral bodyby two strong pedicles of bone. Thepedicles each have articular facets(superior and inferior), which articulatewith similar facets of the adjacentvertebra as a synovial joint (facet joint).The neural arch is completed posteriorlyby the two bony laminae joining to forma spinous process. A transverse process on
each side projects laterally and providesadditional surface area for muscularattachment. There are also two costalprocesses on each vertebral body, whichare well developed in the thoracic area.The detailed structure of the individualvertebrae varies considerably:
Cervical vertebrae – the typicalcervical vertebra is found from C3 toC6. It has a relatively small and widebody, and has two lateral processes (forthe synovial joints of Lushka) on thesuperior surface of the body. Thetransverse processes also contain aforamen (transversarium) for thepassage of the vertebral artery, venousand sympathetic plexuses. The spinalnerve exits from the vertebral columnvia a shallow neural groove, betweenthe anterior and posterior tubercle ofthe transverse processes. The laminaeare flat and long, and terminate inbifid spinous processes (often single atC6). The neural canal is roughlytriangular in cross-section and widestat C5. The atypical cervical vertebraeare:● Atlas (C1) – has no true body and
essentially consists of a ring of bone.It supports the weight of the skulland articulates with the occipitalcondyles on its superior articularfacets. The inferior facets articulatewith the axis below. It also has arounded facet on the anterior archfor articulation with the odontoidpeg of the axis. The skull rocksbackward and forward on theatlas94
21 The vertebrae
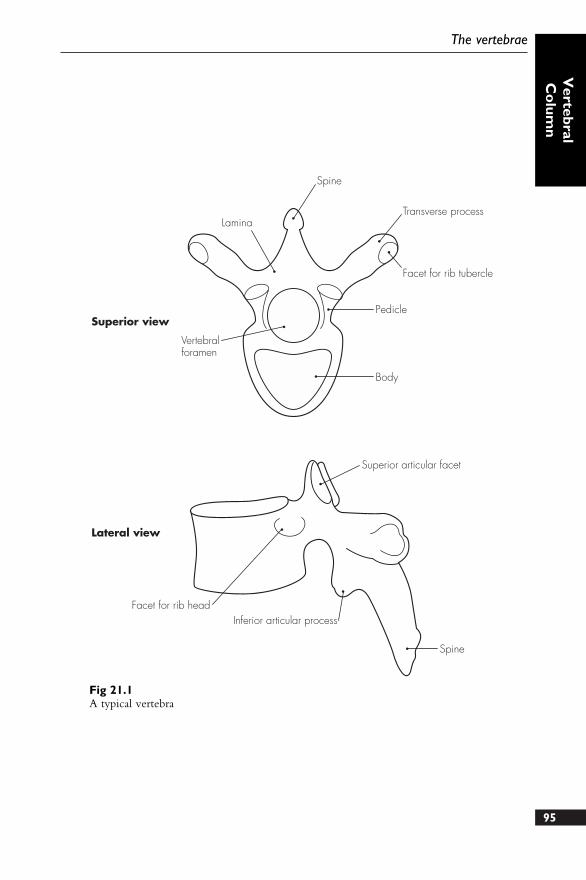
95
The vertebrae
Vertebral
Co
lumn
Lamina
Spine
Transverse process
Facet for rib tubercle
Pedicle
Vertebralforamen
Superior view
Lateral view
Body
Superior articular facet
Spine
Inferior articular processFacet for rib head
Fig 21.1A typical vertebra
● Axis (C2) – allows the head torotate. It is also somewhat ring-likein shape. It has a projection of bonefrom the body – odontoid peg ordens, which is attached to theoccipital bone by apical ligaments.The laminae are particularly strongand the transverse processes short
● Vertebra prominens (C7) – largestcervical vertebra. It has aparticularly large spinous processand is transitional between thecervical and thoracic vertebrae.Occasionally, a cervical rib may alsobe seen, extending from thetransverse process
Thoracic vertebrae – have articularfacets on the vertebral bodies andtransverse processes for articulationwith the head and neck of the rib.The vertebral bodies are somewhatheart-shaped and have lateral half-facets (superiorly and inferiorly) for thearticulation of the head of the rib. Thetransverse processes are directedbackwards and laterally, and carryfacets on the anterior aspect forarticulation with the tubercle of therib. The spinous processes aregenerally slender, long and aredirected caudad. The atypical vertebraeare:● T1 – similar to C7, with a broader
and wider body. The upper costalfacet is complete for articulationwith the first rib and a transverseprocess facet placed moreanteriorly. An articular shelf is alsopresent, providing additionalsupport to prevent backwarddisplacement of C7 on T1
● T9 and T10 – may only showsingle costal articular facets
● T11 and T12 – transitional betweenthe thoracic and lumbar vertebrae(being stronger and having smallertransverse processes)
Lumbar vertebrae – largest vertebraeand lack foramina transversaria andcostal facets. The bodies are large andkidney-shaped, the pedicles short andstrong, and the transverse processesrelatively small. The superior andinferior articular facets are verticallyorientated. The body of L5 is wedge-shaped – thicker posteriorly thananteriorly.
Sacrum – formed by the fusion of thefive sacral vertebrae. It forms thecentral axis of the pelvic girdle, andarticulates above with the fifth lumbarvertebra, on the sides with theinnominate bone (at the sacroiliacjoints), and below with the coccyx. Itis concave anteriorly and roughlywedge-like in shape, and has four pairsof foramina for the exit of the ventralspinal nerves posteriorly.
The sacral canal is within the sacrum,with anterior and posterior marginscreated by the fused sacral vertebrae. Itcontains:● Cauda equina● Filum terminale● Meninges (spinal)● Coccygeal/sacral nerves● Epidural fat and veins
The lower part of the sacrum showsthat the fifth sacral laminae frequentlyfail to fuse. This is called the sacralhiatus. The hiatus is bounded aboveby the fused fourth sacral laminae,laterally by the deficient laminamargins of S5 (bearing the sacralcornua) and below by the posteriorbody of S5.
The hiatus is covered over by thesacrococcygeal ligament, and thisprovides a convenient entry route intothe caudal epidural space. The cornuaare identified with a fingertip, and aneedle introduced at 45° to the skin.Once the sacral canal is entered, the96
Concise Anatomy for Anaesthesia
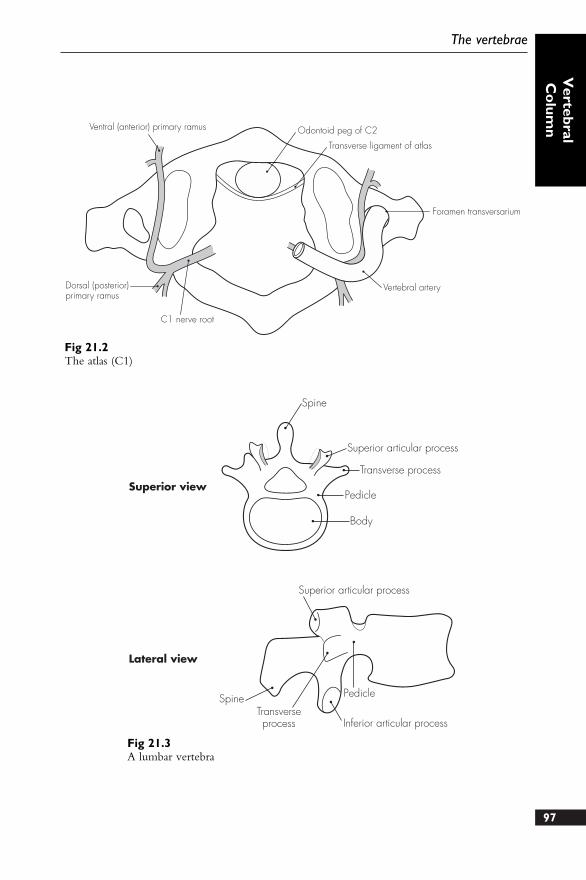
97
The vertebrae
Vertebral
Co
lumnVentral (anterior) primary ramus Odontoid peg of C2
Transverse ligament of atlas
Dorsal (posterior)primary ramus
C1 nerve root
Foramen transversarium
Vertebral artery
Fig 21.2The atlas (C1)
Spine
Superior articular process
Transverse process
Pedicle
Body
Superior articular process
SpineTransverseprocess
Pedicle
Inferior articular process
Superior view
Lateral view
Fig 21.3A lumbar vertebra

needle is advanced a short distance andthe solution injected. Care must betaken to avoid entering the subduralspace, especially in children where thedural sac may end unusually low.
Coccyx – formed from the fusion offour small and rudimentary coccygealvertebrae. The surfaces provideattachment for nearby pelvic andgluteal muscles
98
Concise Anatomy for Anaesthesia
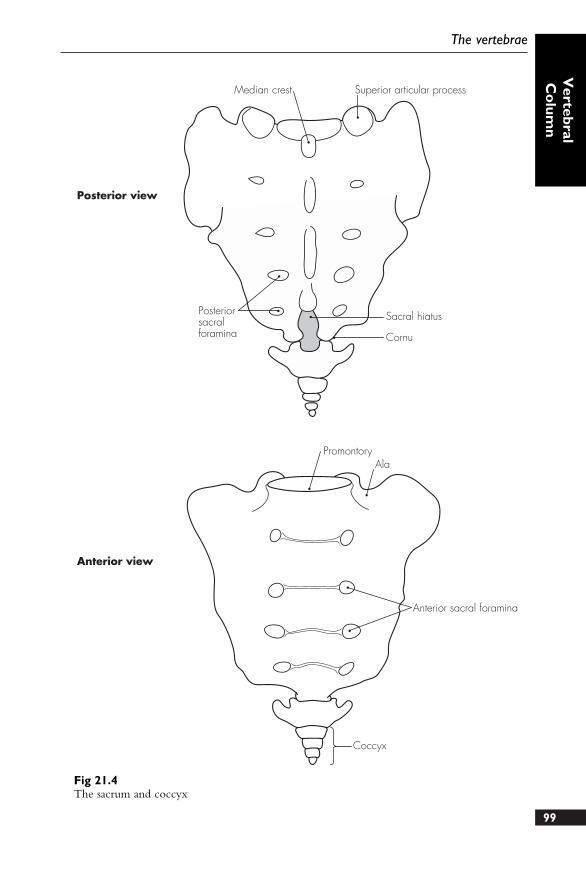
99
The vertebrae
Vertebral
Co
lumn
Posterior view
Anterior view
Median crest Superior articular process
Posteriorsacralforamina
Sacral hiatus
Cornu
PromontoryAla
Anterior sacral foramina
Coccyx
Fig 21.4The sacrum and coccyx
DESCRIPTION
There is a complicated series of ligamentsand joints that connect the variouscomponents of the vertebral column.These may be summarised as follows:
Intervertebral discs – connect thevertebral bodies and make up 25%of the height of the spinal column.These consist of an outer annulusfibrosus and an inner annuluspulposus. The superior and inferiorsurfaces of the vertebral bodies arealso lined with hyaline cartilage,which allow adhesion to theintervertebral discs
Anterior longitudinal ligament – runsalong the anterior surface of thevertebral bodies, from C2 to thesacrum. It adheres to the anteriorsurface of the vertebral bodies andthe discs
Posterior longitudinal ligament –extends along the posterior aspect ofthe vertebral bodies and discs
Ligamenta flava – series of thick,elastic, vertical fibres that connectadjacent vertebral laminae
Interspinous ligaments – connect theshafts of the spinous processes
Supraspinous ligaments – tough fibrouscolumn that connects the tips of thespinous processes
Ligamentum nuchae – superiorextension of the supraspinousligaments and extends from C7 tothe occiput
POINTS OF INTEREST
● The epidural space may be entered byinserting a needle between the spinalvertebral laminae, either directly inthe midline, or via a para-midlineapproach. The needle will passthorough the following structures as itadvances:● Skin● Subcutaneous tissue and fat● Supraspinous ligaments (tough)● Interspinous ligaments (thin)● Ligamentum flavum (tough)● Epidural space (and contents)
100
22 The vertebral ligaments

1. Describe the anatomical structuresthough which the spinal needle passesduring a lumbar puncture.
2. How do you perform a caudal block?Detail the important relations of the
caudal canal with the aid of a simplediagram.
3. Draw and label a cross-sectionaldiagram of the epidural space.
Sample questions –vertebral column
101

Areas of SpecialInterest

The skull provides protection to theintracranial contents and the face, andconsists of the neurocranium and anteriorfacial (splanchnocranium) structures. Thebrain rests on the base of the skull, whichitself can be divided into three areas orcranial fossae: posterior, middle andanterior.
1. Posterior cranial fossa – largest anddeepest fossa. The sphenoid, temporaland basi-occipital bones bound itanteriorly, and the occipital bonelaterally and posteriorly. Posteriorly,the transverse sinuses create deepgrooves, which pass laterally, and theoccipital prominence lies centrally.This extends to form the internaloccipital crest, which attaches to thefalx cerebelli. The posterior fossahouses the medulla, pons andcerebellum below and the occipitallobes above (separated by thehorizontal tentorium cerebelli). Thefollowing openings transmit variousstructures:● Internal acoustic meatus – situated
in the posterior petrous part of thetemporal bone, and transmits thefacial and vestibulocochlear nervesand labyrinthine vessels
● Jugular foramen – lies just belowthe internal auditory meatus. Ittransmits the sigmoid and inferiorpetrosal sinuses, and theglossopharyngeal, vagus andaccessory nerves
● Hypoglossal canal – transmits thehypoglossal nerve and meningealbranches of the ascending
pharyngeal artery. It lies justanterior to the foramen magnum
● Foramen magnum – largest skullopening and transmits the medullaoblongata and meninges, as well asthe vertebral arteries and the spinalaccessory nerve
2. Middle cranial fossa – houses thetemporal lobes of the brain. It isbounded by the wings of thesphenoid bone anteriorly, thetemporal bone laterally, and thepetrous temporal crests posteriorly.The sphenoid body houses thehypophyseal fossa centrally (for thepituitary gland) and has two smallposterior clinoid processes forattachment to the tentoriumcerebelli. The middle cranial fossacommunicates with the orbit throughtwo structures: optic canal and thesuperior orbital fissure. These andother openings transmit the followingstructures:● Optic canal – placed anteriorly,
this transmits the optic nerve andophthalmic artery
● Superior orbital fissure – transmitsall the other structures from theorbit
● Ophthalmic nerve● Oculomotor, trochlear and
abducens nerves● Ophthalmic veins● Foramen rotundum – lies
anteriorly in the greater wing ofthe sphenoid bone. It transmits themaxillary division of thetrigeminal nerve
● Foramen ovale – placed just104
23 The base of the skull
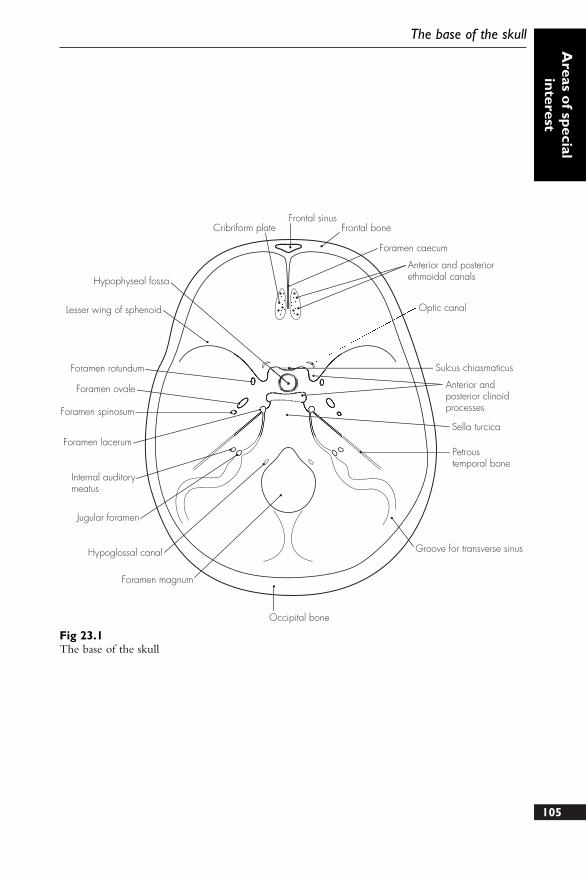
105
The base of the skullA
reas of special
interest
Frontal sinusFrontal boneCribriform plate
Foramen caecum
Anterior and posteriorethmoidal canals
Optic canal
Sulcus chiasmaticus
Anterior andposterior clinoidprocesses
Sella turcica
Petroustemporal bone
Groove for transverse sinus
Occipital bone
Foramen magnum
Hypoglossal canal
Jugular foramen
Internal auditorymeatus
Foramen lacerum
Foramen spinosum
Foramen ovale
Foramen rotundum
Hypophyseal fossa
Lesser wing of sphenoid
Fig 23.1The base of the skull

behind the foramen rotundum andtransmits the mandibular division(trigeminal), and the lesser petrosalnerve
● Foramen spinosum – placedfurther posterolateral to the above,and contains the middle meningealvessels, and the meningeal branchof the mandibular nerve
● Foramen lacerum – at the junctionbetween the sphenoid andtemporal bones posteriorly. Ittransmits small meningeal branches(of ascending pharyngeal artery)and emissary veins
● Carotid canal – allows the internalcarotid artery (and accompanyingsympathetic plexus) entrance to thecranium. The artery runs throughits large intracranial opening to runanteriorly and medially, lateral tothe sphenoid body
● Stylomastoid foramen – has anopening only present on theunderside of the skull base. Thistransmits the facial nerve andbranch of the posterior auricularartery and these enter the facialcanal
3. Anterior cranial fossa – houses thefrontal lobes and is bounded by thefrontal bone anteriorly and the lesserwings of sphenoid posteriorly. Thefloor of the fossa is made of theethmoid bone centrally and this has aprojection – the crista galli – for theattachment to the falx cerebri. Thelesser wings of the sphenoid projectlaterally and terminate medially in theanterior clinoid processes (attach tothe tentorium cerebelli). Between theanterior clinoid processes is a slightlyindented plateau of bone upon whichthe optic chiasma lies (sulcuschiasmatus). The following openingsare present:● Foramen caecum – anterior to the
crista galli and transmits anemissary vein
● Cribriform plate – transmits theolfactory sensory nerves
● Anterior ethmoidal canal – justlateral to the cribriform plate andfor the passage of anteriorethmoidal nerves and vessels
● Posterior ethmoidal canal – for theposterior ethmoidal vessels
106
Concise Anatomy for Anaesthesia

The thoracic inlet is the area where theneck and thorax meet, and is filled witha large number of important structures. Itis roughly kidney-shaped and is boundedby the superior manubrium anteriorly,the anterior surface of the first vertebralbody posteriorly, and the first ribs andcartilages laterally. The lung apicesproject above the clavicle for ~3 cm,covered over by the pleura and thesuprapleural membrane. The lungs aregrooved anteriorly by the subclavianvessels and posteriorly by the stellateganglion, superior intercostal artery andthe first thoracic ventral nerve ramus.
The scalenus muscles and the first rib areuseful structures to understand therelationships in this area:
1. Scalenus muscles – three: scalenusanterior, scalenus medius and scalenusposterior. The scalenus anteriororiginates from the anterior tuberclesof C3–6, and passes down andlaterally, to attach to the scalenetubercle of the first rib. It lies behindthe sternomastoid muscle. Thefollowing structures are related to thescalenus anterior:● Anteriorly:
● Phrenic nerve● Thoracic duct (on left)● Carotid sheath – superiorly
only; inferiorly only theinternal jugular vein is anterior(others medial)
● Subclavian vein● Posteriorly:
● Subclavian artery (divided intoparts)
● Brachial plexus roots● Medially:
● First part of subclavian arteryand branches (vertebral,internal thoracic, thyrocervical,costocervical)
● Common carotid artery(inferiorly)
● Vagus nerve (inferiorly)● Sympathetic trunk
2. First rib – shortest, flattest and mostcurved of the ribs. It has a head, afacet for the body of T1, a neck anda tubercle for the transverse processof T1. There are a number ofgrooves and tubercles on the superiorsurface of the first rib and these willbe described from posterior toanterior:● Insertion for scalenus medius – on
the long neck of the first rib andprovides for the attachment of themuscle. Immediately in front ofthe muscle lie the trunks of thebrachial plexus
● Groove for subclavian artery – justanterior to the scalenus mediusmuscle groove. It is grooved forthe lower trunk of the brachialplexus (posterior) and thesubclavian artery (anterior)
● Tubercle for scalenus anterior –on the inner medial curve of thefirst rib, anterior to the subclaviangroove
● Groove for subclavian vein – justanterior to the insertion ofscalenus anterior. The subclavianvein runs over this groove andbehind the clavicle108
24 The thoracic inlet
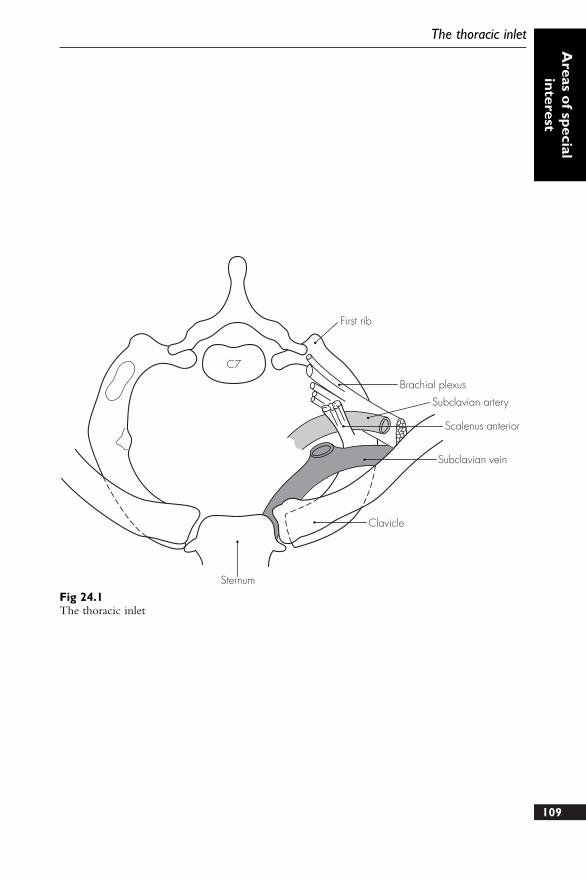
109
The thoracic inletA
reas of special
interest
First rib
Brachial plexus
Scalenus anterior
Subclavian vein
Clavicle
Sternum
Subclavian artery
C7
Fig 24.1The thoracic inlet
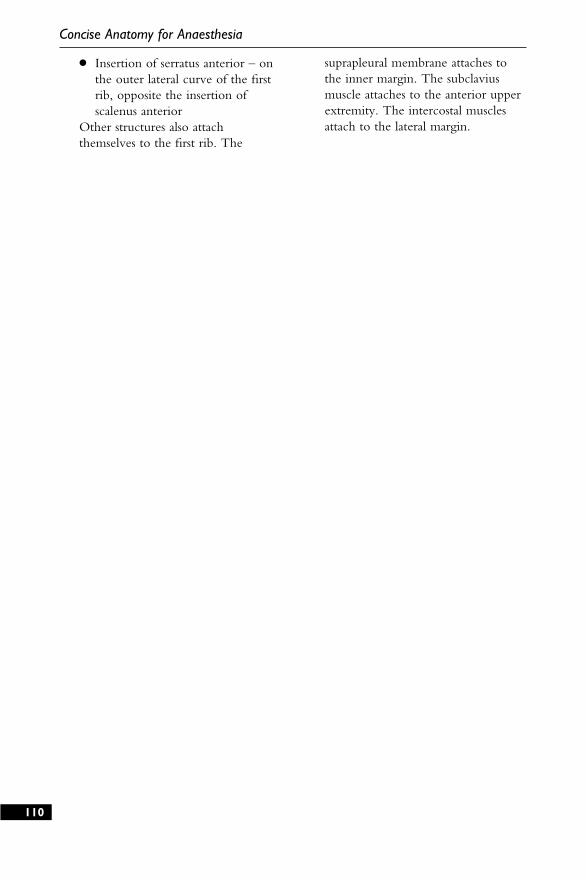
● Insertion of serratus anterior – onthe outer lateral curve of the firstrib, opposite the insertion ofscalenus anterior
Other structures also attachthemselves to the first rib. The
suprapleural membrane attaches tothe inner margin. The subclaviusmuscle attaches to the anterior upperextremity. The intercostal musclesattach to the lateral margin.
110
Concise Anatomy for Anaesthesia
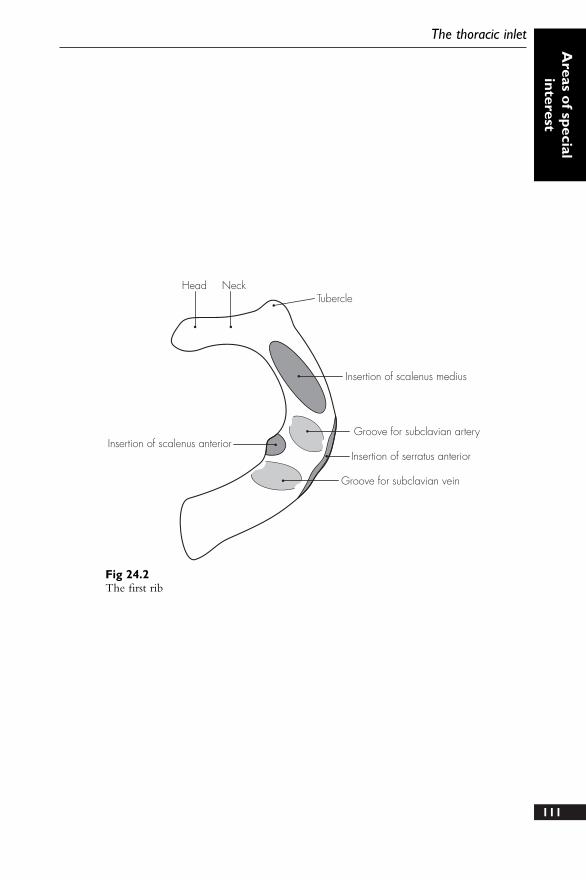
111
The thoracic inletA
reas of special
interest
Head NeckTubercle
Insertion of scalenus medius
Groove for subclavian artery
Insertion of serratus anterior
Groove for subclavian vein
Insertion of scalenus anterior
Fig 24.2The first rib
The spaces between the ribs are filled bylayers of muscle and fibrous tissue,between which are the vessels, nervesand lymphatics.
1. Muscles:● External intercostals (11 pairs) –
these outermost muscles pass fromthe lower border of the upper ribto the upper border of the lowerrib. They extend anteriorlytowards the costochondral junctionbecoming gradually more fibrous,and merge into the external(anterior) intercostal membrane
● Internal intercostals (11 pairs) –run deep, and with the fibresrunning at right angles, to theexternal intercostals. They extendfrom the sternum, laterally aroundto the angle of the rib, where theybecome fibrous and merge toform the internal (posterior)intercostal membrane
● Innermost intercostal – largelyincomplete and consist ofnumerous slips of muscle tissue.They are individually named asthe transversus thoracis(anteriorly), intracostal (laterally)and subcostalis (posteriorly)muscles. These are bound togetherby a continuous sheet of fascia.The innermost muscles are alsoseparated from the parietal pleuraby a further layer of fascia, theendothoracic fascia
2. Neurovascular bundles – each consistof (from above down) a vein, anartery and a nerve. They lie between
the innermost and internal intercostalmuscle layers for almost their entirecourse:● Veins – have complex
terminations and consist of theposterior and anterior intercostalveins. The posterior veinseventually drain into the superiorvena cava via the azygos andhemi-azygos systems, and theanterior veins drain into themusculophrenic vein (lowerspaces), or the internal thoracicvein (upper spaces)
● Arteries – the posterior andanterior intercostal arteries. Theposterior intercostal arteries arisedirectly from the thoracic aortafrom T3 to T11, and from thesuperior intercostal artery (T1 andT2). The anterior intercostalarteries (T1–9) are derived fromthe two internal thoracic arteries,which themselves are branches ofthe subclavian artery, and runbehind and just lateral to thesternal edge. The last twointercostal spaces are supplied bythe posterior intercostal arteriesonly. The anterior intercostalseventually anastomose with theposterior intercostal arteries
● Nerves – ventral (anterior) rami ofthe thoracic nerves from T1 toT11. The lower five nerves fromT7 to T11 continue to supply theabdominal wall and maintain theirposition between the innermostand internal muscle layers (theinternal oblique and transversus112
25 The intercostal space
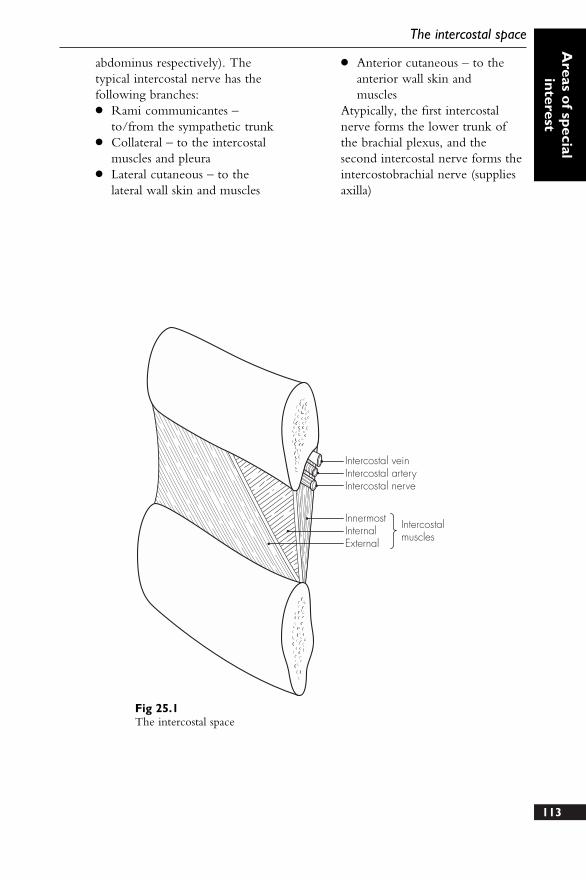
113
The intercostal spaceA
reas of special
interest
Intercostal veinIntercostal arteryIntercostal nerve
InnermostInternalExternal
Intercostalmuscles
Fig 25.1The intercostal space
abdominus respectively). Thetypical intercostal nerve has thefollowing branches:● Rami communicantes –
to/from the sympathetic trunk● Collateral – to the intercostal
muscles and pleura● Lateral cutaneous – to the
lateral wall skin and muscles
● Anterior cutaneous – to theanterior wall skin and muscles
Atypically, the first intercostalnerve forms the lower trunk ofthe brachial plexus, and thesecond intercostal nerve forms theintercostobrachial nerve (suppliesaxilla)

This extends from the xiphoid process (atthoracic level T9) and subcostal marginsuperiorly to the iliac crest, inguinalligament and pubic symphysis inferiorly.The umbilicus is a convenient centralpoint to divide the abdomen into upperand lower, and right and left, quarters. Itis positioned opposite the third lumbarvertebra (and has dermatomal nervesupply from T10). A line joining the iliaccrests passes through the body of thefourth lumbar vertebra, and this is also auseful point of reference when performingan epidural or spinal procedure.
The anterior abdominal wall is essentiallya layered fibromuscular sheet and has itsown blood and nerve supply. Inferiorly,the inguinal region contains numerousstructures of importance.
1. Muscles● Rectus abdominus – band-like
central pair of muscles arising fromthe pubic crest and inserting intothe fifth, sixth, and seventh costalcartilages. The muscle has at leastthree horizontal fibrous bands onthe anterior surface (preventingeasy spread of local anaestheticsolution anteriorly). Each muscleis enclosed by the rectus sheath,which is formed by the splitting ofthe inferior oblique aponeurosis.This is further reinforced behindby the transversus abdominusaponeurosis and in front by theexternal oblique aponeurosis. Theposterior part of the rectus sheathis deficient superiorly at the costalmargin (muscular insertions), and
inferiorly below the arcuate line(where the aponeuroses all passanteriorly to the rectus muscle). Inthe central region the rectussheath lies directly onextraperitoneal fat andperitoneum. The rectus sheathcontains the rectus abdominus, thesuperior and inferior epigastricvessels, the terminal branches ofthe intercostal nerves T7–11, andthe subcostal vessels and nerves
● External oblique – outermostabdominal wall muscle andextends from the lateral edge ofthe rectus abdominus (linea alba),pubis and anterior iliac crest to therib insertions. The fibres rundownward and medially
● Internal oblique – lies deep to theexternal oblique and is continuouswith the internal intercostalmuscles above. The fibres passupwards and laterally
● Transversus abdominus –innermost muscle and its fibrespass horizontally
2. Blood supply – extensive, and themain supply comes from the inferiorepigastric (from the external iliacartery) and superior epigastric(terminal branch of the internalthoracic artery) arteries. Thecorresponding veins carry the bloodaway and also lie within the rectussheath
3. Nerve supply – from the ventral(anterior) primary rami of T7 to L1.The details of supply have beendescribed earlier.114
26 The abdominal wall
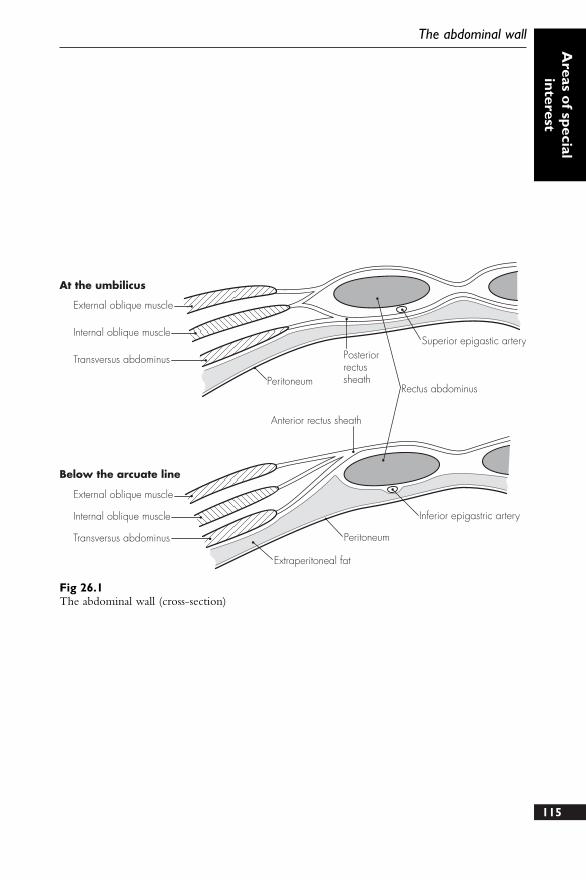
115
The abdominal wallA
reas of special
interest
Superior epigastic arteryPosteriorrectussheath
Rectus abdominusPeritoneum
Anterior rectus sheath
Peritoneum
Inferior epigastric artery
External oblique muscle
Internal oblique muscle
Transversus abdominus
External oblique muscle
At the umbilicus
Below the arcuate line
Internal oblique muscle
Transversus abdominus
Extraperitoneal fat
Fig 26.1The abdominal wall (cross-section)

The inguinal canal is obliquely placed,passing through the lower part of theanterior abdominal wall. It extends fromthe deep inguinal ring (transversalis fasciaopening), down and medially to thesuperficial ring (external obliqueaponeurosis opening). It lies above andfollows the inguinal ligament. Theinguinal ligament is the rolled-up edge ofthe external oblique, which runs fromthe pubic tubercle to the anteriorsuperior iliac spine. The boundaries ofthe inguinal canal are:● Anterior – aponeurosis of the external
oblique● Posterior – fascia transversalis, and
conjoint tendon in the medial third
(common tendon of internal obliqueand transversus muscles)
● Floor – inguinal ligament, and lacunarligament medially
● Roof – arching fibres of thetransversus abdominus and internaloblique
The inguinal canal has the followingcontents:● Male – ilioinguinal nerve and
spermatic cord (containing the vasdeferens, testicular, deferens andcremasteric arteries, pampiniformplexus, sympathetic plexus and genitalbranch of genitofemoral nerve)
● Female – ilioinguinal nerve and roundligament
116
27 The inguinal region
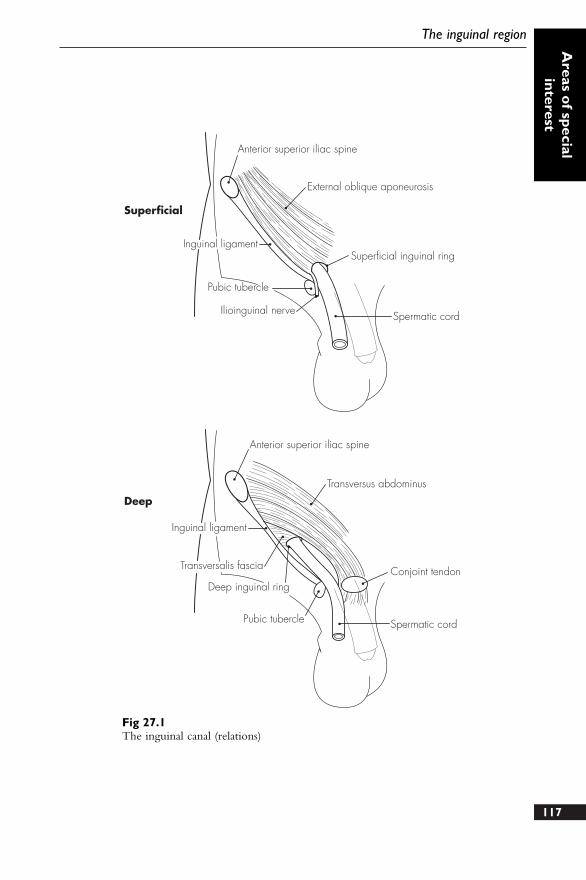
117
The inguinal regionA
reas of special
interest
Anterior superior iliac spine
Anterior superior iliac spine
External oblique aponeurosis
Superficial inguinal ring
Spermatic cordIlioinguinal nerve
Pubic tubercle
Inguinal ligament
Transversus abdominus
Conjoint tendon
Spermatic cordPubic tubercle
Deep inguinal ring
Transversalis fascia
Inguinal ligament
Superficial
Deep
Fig 27.1The inguinal canal (relations)
DESCRIPTION
This is the triangular hollowed area onthe anterior aspect of the elbow. Itcontains a number of vessels and nervesthat enter and exit the forearm, andwhich can easily be damaged.
RELATIONS
Inferomedial – pronator teresInferolateral – brachioradialisSuperior – a line joining the two
epicondyles of the humerus (medialand lateral)
Roof – deep fascia (reinforced bybicipital aponeurosis). Lying superficialto the fascia are the median cubitalvein and the medial cutaneous nerveof the forearm, and the basilic vein(medial) and cephalic vein (lateral)
Floor – supinator (laterally) and brachialis(medially)
CONTENTS
From medial to lateral:
● Median nerve● Brachial artery – considerable
variations may occur. The artery maybifurcate high in the upper arm, andsuperficial radial and ulnar branchesmay also be found. The superficialulnar artery variation (found in 2%) isat particular risk during antecubitalvenepuncture attempts
● Biceps tendon● Radial nerve (with posterior
interosseous branch)
SUPERFICIAL VEINS
These also show considerable variation:
1. Cephalic vein – drains the radialforearm
2. Basilic vein – drains the ulnarforearm
3. Medial cubital vein – joins the basilicand cephalic vein to form an ‘H’arrangement. It frequently receivesthe median vein of the forearm, andmay bifurcate to form an ‘M’arrangement
118
28 The antecubital fossa
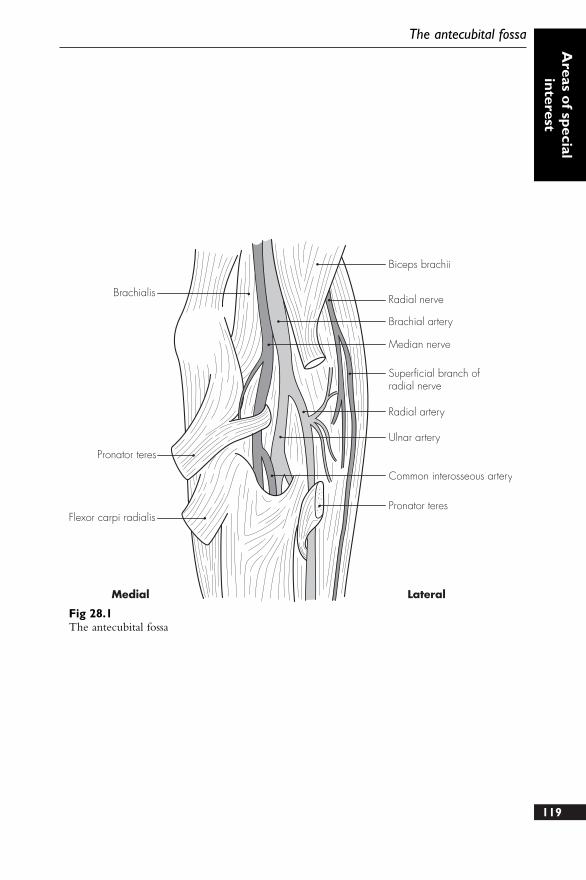
119
The antecubital fossaA
reas of special
interest
Brachialis
Pronator teres
Flexor carpi radialis
Biceps brachii
Radial nerve
Brachial artery
Median nerve
Superficial branch ofradial nerve
Radial artery
Ulnar artery
Common interosseous artery
Pronator teres
Medial Lateral
Fig 28.1The antecubital fossa

These have been briefly discussed earlier,and a more detailed description follows.
1. Internal jugular vein – runsdownwards from the jugular foramen(draining the sigmoid sinus) and joinsthe subclavian vein behind the sternalclavicle to form the brachiocephalicvein. It lies lateral to the internalcarotid artery, and lower down, thecommon carotid artery, within thecarotid sheath. The vagus nerve liesjust behind and between the twomajor vessels, within the sheath. Thesympathetic chain runs immediatelyposterior to the carotid sheath andthe relations of these two nerves andtwo vessels are thus similar. Theinternal jugular vein receives thefollowing tributaries:● Pharyngeal veins● Common facial vein● Thyroid veins (superior and middle)● Lingual vein
2. External jugular vein – receives theposterior division of theretromandibular vein (the anteriordivision joins the facial vein) andcrosses anterior to the sternomastoidin the neck. It passes deep to theneck fascia above the clavicle andenters the subclavian vein (not theinternal jugular vein)
3. Anterior jugular vein – drains theanterior neck and passes over thethyroid isthmus, diving deep to thesternomastoid, to enter the externaljugular vein
4. Subclavian vein – continuation of theaxillary vein, and extends from thefirst rib outer border to the scalenusanterior medial border. It joins theinternal jugular vein to form thebrachiocephalic vein behind thesternoclavicular joint. It runs overand grooves the first rib in its arch-like course. It also receives thethoracic duct on the left
5. Brachiocephalic vein – formed by theinternal jugular and subclavian veins.It receives inferior thyroid, internalthoracic and vertebral veins. The leftbrachiocephalic vein is 6 cm long andruns behind the manubrium sterni toterminate in forming the superiorvena cava (with the rightbrachiocephalic vein), behind the firstcostal cartilage. It runs in front of thebrachiocephalic artery, trachea andleft common carotid artery, andsuperior to the aortic arch. The rightbrachiocephalic vein is 3 cm long andruns vertically down behind the rightborder of the manubrium sterni toform the superior vena cava (asabove)
120
29 The large veins ofthe neck
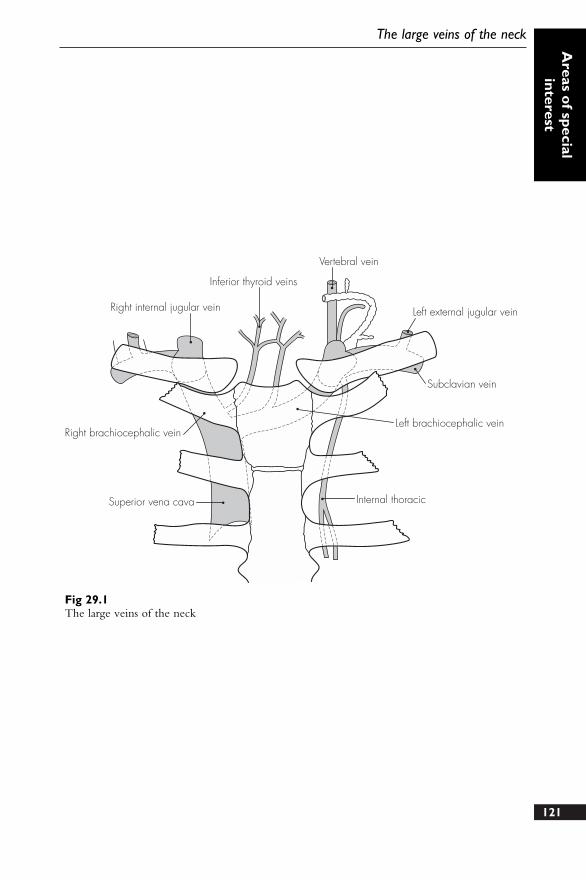
121
The large veins of the neckA
reas of special
interest
Inferior thyroid veins
Vertebral vein
Left external jugular vein
Subclavian vein
Left brachiocephalic vein
Internal thoracicSuperior vena cava
Right brachiocephalic vein
Right internal jugular vein
Fig 29.1The large veins of the neck

DESCRIPTION
This is roughly pyramidal in shape andallows major structures to pass from theneck to the upper limb. The roofextends into the neck and is bounded bythe clavicle in front and the scapulabehind. The base is bounded by theanterior pectoralis major, the posteriorteres major and medially by the chestwall (and serratus anterior muscle), and iscovered over by a layer of skin.
RELATIONS
Anterior wall – pectoralis major andminor muscles, and clavipectoralfascia
Posterior wall – subscapularis, latissimusdorsi and teres major muscles
Medial wall – serratus anterior muscle,and upper five ribs and spaces
Lateral wall – coracobrachialis and bicepsbrachii muscles
CONTENTS
● Axillary artery – continuation of thesubclavian artery and becomes thebrachial artery at the lower border ofteres major. It is invested in aconnective tissue sheath – axillarysheath. The pectoralis minor dividesthe axillary artery into three parts
● Axillary vein – receives the upperlimb venous drainage and becomesthe subclavian vein. It lies mediallyalong the axillary artery
● Brachial plexus – cords of the brachialplexus surround the axillary arterywithin the axillary sheath. Initially allcords lie above the axillary artery (inits first part), but take their respectivepositions (medial, lateral and posterior)in relation to the more distal secondpart of the artery
● Axillary lymph nodes – these drainthe lateral breast and chest wall, andthe upper limb. There are six groupsthat drain into the thoracic duct onthe left and the right lymphatic truckon the right
122
30 The axilla
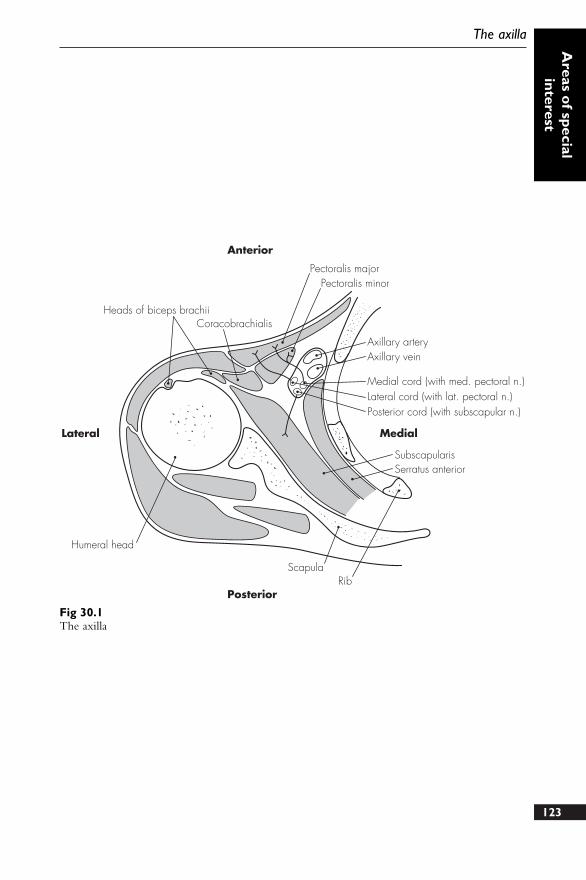
123
The axillaA
reas of special
interest
ScapulaRib
Humeral head
Heads of biceps brachii
Lateral
Posterior
Anterior
Medial
Coracobrachialis
Pectoralis majorPectoralis minor
Axillary arteryAxillary vein
Medial cord (with med. pectoral n.)Lateral cord (with lat. pectoral n.)Posterior cord (with subscapular n.)
SubscapularisSerratus anterior
Fig 30.1The axilla

DESCRIPTION
The orbit is roughly conical in shape,with the apex directed posteriorly andslightly medially towards the middlecranial fossa. The base is directed towardsthe face and has strong bony margins toprotect the orbital contents. The marginsare formed as follows:
Superior – frontal bone (with supra-orbital notch)
Lateral – frontal process of thezygomatic bone
Inferior – frontal process of thezygomatic bone (laterally) andanterior lacrimal crest of the maxilla(medially)
Medial – frontal bone (superiorly),posterior lacrimal crest of thelacrimal bone (inferiorly)
The lacrimal apparatus is containedwithin a fossa on the medial wall of theorbit, and between the anterior andposterior lacrimal crests.
RELATIONS
Each orbit has the following boundaries:
Roof – formed from the orbital plateof the frontal bone (anteriorly) andlesser wing of the sphenoid bone(posteriorly). The optic canal is inthe posterior roof and transmits theoptic nerves, meninges andophthalmic artery
Medial wall – formed from the orbitallamina of the ethmoid bone, frontalprocess of the maxilla, lacrimal boneand body of the sphenoid. The
lacrimal fossa is formed between thetwo lacrimal crests on the medialwall. Anterior and posteriorethmoidal foramina on the medialwall transmit ethmoidal nerves andvessels
Floor – formed from the orbitalsurface of the maxilla and orbitalprocess of the palatine bone. Theinferior orbital fissure transmits theinfra-orbital artery and nerve
Lateral wall – formed from the frontalprocess of the zygomatic bone infront and the greater wing of thesphenoid behind. The superiororbital fissure lies between the roofand lateral wall, and transmits thecranial nerves III, IV and VI, theophthalmic divisions of thetrigeminal nerve (V), and thesuperior ophthalmic vein.
CONTENTS
● Fat● Lacrimal apparatus● Optic nerve● Orbital vessels● Eyeball – spherical structure
occupying the anterior half of theorbit. It has three coats: an exteriorfibrous coat (opaque sclera andtransparent cornea), a middle vascular,pigmented coat (choroid, ciliary bodyand iris), and an inner, delicate, retinalcoat. Within the eyeball are therefractive structures: lens, aqueoushumour and vitreous body. A thinfascial sheath surrounds the eyeball,except the cornea. This bulbar sheath124
31 The eye and orbit
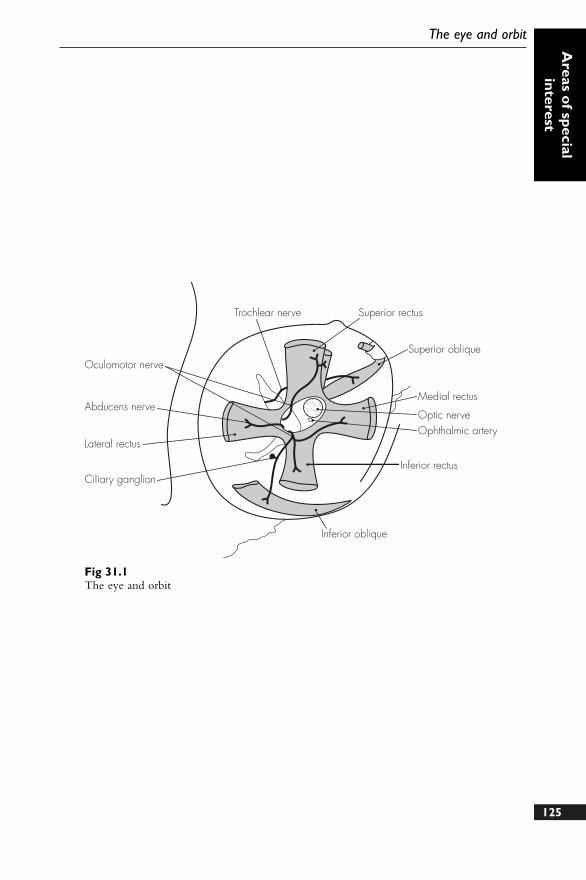
125
The eye and orbitA
reas of special
interest
Trochlear nerve Superior rectus
Oculomotor nerve
Abducens nerve
Lateral rectus
Ciliary ganglion
Inferior oblique
Inferior rectus
Ophthalmic arteryOptic nerve
Medial rectus
Superior oblique
Fig 31.1The eye and orbit
(or Tenon’s capsule) separates theeyeball from the surrounding fat andorbital structures. The extra-ocularmuscles attach to the corneoscleraljunction, and six muscles areresponsible for the movement of theeyeball. There are four rectus muscles(medial, lateral, superior, inferior) thatarise from a tendinous ring encirclingthe optic canal and nerve. The tworemaining oblique muscles, superiorand inferior, arise from the sphenoidbone and orbital surface of themaxilla. Levator palpebrae superiorisalso arises from the tendinous ring andinserts into and elevates the uppereyelid.
VASCULAR SUPPLY
1. Arterial:● Ophthalmic artery – provides the
major blood supply to the orbitand eye. It arises from the internalcarotid artery (near the cavernoussinus) and enters the orbit throughthe optic canal. It gives off anumber of branches:
● Lacrimal artery● Posterior ciliary arteries● Muscular arteries and anterior
ciliary branches● Supra-orbital, supratrochlear, nasal
and posterior ethmoidal branches● Central artery of the retina
2. Venous:● Superior ophthalmic vein – passes
over the optic nerve and throughthe superior orbital fissure toterminate in the cavernous sinus.It also anastomoses with the facialvein
● Inferior ophthalmic vein – passesunder the optic nerve and throughthe inferior orbital fissure to
terminate in the superiorophthalmic vein or the cavernoussinus
● Central vein of the retina – usuallypasses directly to the cavernoussinus (occasionally joining thesuperior ophthalmic vein)
NERVE SUPPLY
May be divided into three groups:● Motor nerves:
● Abducens – within the tendinousring to supply the lateral rectus
● Trochlear – outside the tendinousring to supply the superior oblique
● Oculomotor – inside the tendinousring to supply other intra-ocularmuscles
● Sensory nerves:● Optic nerve (as discussed above)● Frontal nerve – from the
ophthalmic division of thetrigeminal nerve to supply the skinof the upper eyelid, forehead andscalp
● Lacrimal nerve – sensory only tothe gland
● Nasociliary nerve – sensory to theeyeball via numerous branches,including the long and short (alsoautonomic) ciliary nerves
● Autonomic fibres:● Maxillary fibres from the
pterygopalatine ganglion –secretomotor to the lacrimal gland
● Oculomotor nerve – posteriordivision carries preganglionicparasympathetic fibres to the ciliaryganglion
● Short ciliary nerves – carrypostganglionic fibres from theciliary ganglion to the sphincterpupillae and ciliary muscles
126
Concise Anatomy for Anaesthesia
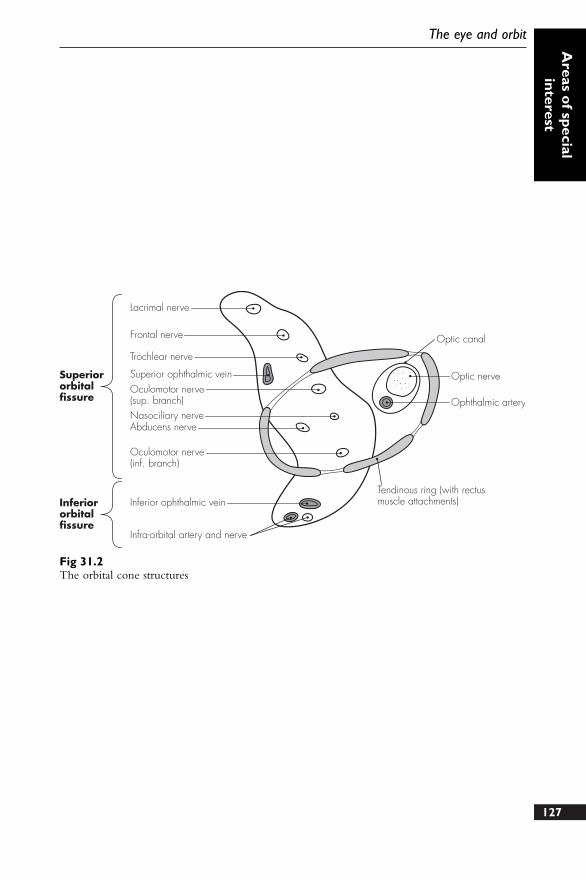
127
The eye and orbitA
reas of special
interest
Lacrimal nerve
Frontal nerve
Trochlear nerve
Superior ophthalmic veinSuperiororbitalfissure
Inferiororbitalfissure
Oculomotor nerve(sup. branch)Nasociliary nerveAbducens nerve
Oculomotor nerve(inf. branch)
Inferior ophthalmic vein
Infra-orbital artery and nerve
Tendinous ring (with rectusmuscle attachments)
Ophthalmic artery
Optic nerve
Optic canal
Fig 31.2The orbital cone structures

1. Using the skull/diagram provided,describe the foraminae marked andlist the structures that pass throughthem.
2. Describe the anatomy of the firstrib.
3. What are the important relations andboundaries of the antecubital fossa?What structures may be damagedduring attempts at venepuncture inthis area?
4. Make a simple diagram, labelled toshow the anatomical structures
associated with the right jugular vein.List the complications of cannulationof this vessel, mentioning how eachmay be avoided.
5. Describe the anatomy of the inguinalcanal. How may nerve blockade beused to allow surgery under localanaesthesia?
6. What are the bony components ofthe orbit? Which structures may bedamaged during peribulbar andretrobulbar nerve blockade for eyesurgery?
128
Sample questions – areas ofspecial interest

129
Notes

130
Notes
131
Notes

132
Notes

133
Notes

134
Notes

135
Notes

136
Notes
Index
Note: a. = artery/ies; l. = ligament/s; m. = muscle/s; n. = nerve/s; v. = vein/s
138
Index
abdominal wall 114–15blood supply 36, 114muscles 114nerve supply 114
abducent n. 80, 125–7accessory n. 84, 86acoustic meatus 104acoustic n. 79adductor brevis m. 64, 67adductor longus m. 64, 67adductor magnus m. 64, 67airway anaesthesia 10alveolar n. 79, 80anconeus m. 60–1anococcygeal n. 56antecubital fossa 118–19anterior interosseus n. 62–3anterior tibial (deep peroneal) n. 66aorta 30–1
abdominal 30aortic arch 15, 27aortic sinus 28knuckle 27major branches 30–1
appendices 87–91arachnoid mater 47, 51arcuate ligaments 22arm see upper limbarteries 30–5
head 33lower limbs 32, 34, 35neck 30–2, 33upper limbs 32, 33see also named arteries
aryepiglottic folds 11arytenoid cartilage 8–9, 11atlas vertebra 94, 94–6, 97atrioventricular node 26auditory (vestibulocochlear) n. 82, 83auricular n. 81–2, 85auriculotemporal n. 75, 79–80
autonomic nervous system 70–5parasympathetic ns 72, 74, 75sympathetic ns 70–2
axilla 122–3axillary a. 32–3, 54, 122–3axillary lymph nodes 122–3axillary n. 55axillary v. 34–6, 37, 122–3azygos v. 14–15, 20, 22–3
basilic v. 34, 37, 118biceps femoris m. 64, 67brachial a. 32–3brachial plexus 52, 54, 55, 109, 122–3brachial plexus block 56brachial v. 37brachialis m. 60–1, 119brachiocephalic a. 15, 27, 30–1, 33brachiocephalic v. 27, 35, 36, 37, 120–1brachioradialis m. 60–1brain 42–3
cranial n. 76–86vascular supply 42–3
bronchi and bronchial tree 16–17, 20lymphatic drainage 21vascular supply 21
buccal n. 79–80bundle of His 28
calcaneal n. 64, 68cardiac n. 84–5cardiac notch 19cardiac plexus 72cardiac postganglionic n. 71cardiac v. 29cardiovascular system 25–40carotid a. 11, 13, 15, 30–2, 43
bifurcation 11cervical ganglia 73
carotid canal 106carotid n. 82–3
139
IndexIndex
cavernous sinus, brain 77cephalic v. 34, 37, 118cerebellar a. 43cerebral a. 43cerebrospinal fluid 48cervical ganglia 70–3cervical n. 81cervical plexus 52, 53cervical plexus block 56cervical vertebrae 94–6, 97cervicofacial n. 81chorda tympani 75, 81–2ciliary a. 126ciliary ganglion 75, 125–6ciliary n. 126circumflex a. 28–9circumflex femoral v. 37circumflex iliac a.
deep 34superficial 35
clavicle 109clavipectoral fascia 55coccygeal n. 56coccygeal vertebrae 98, 99coeliac plexus 72, 84coeliac trunk 31common interosseous a. 119common peroneal n. 64, 66, 69communicating a. 43conjoint tendon 116–17constrictors, pharynx 6–7coracobranchialis m. 123corniculate cartilage 8coronary a. 26, 28–9corrugator m. 81corticospinal tract 44–5costocervical a. 30, 33costochondral junction 18costoxiphoid angle 18cranial fossae 104–6cranial nerves 72–4, 76–86
orbit 125–7cribriform plate 4–5, 105–6cricoarytenoid m. 10cricoid cartilage 8–9, 11cricothyroid l. 8–9cricothyroid m. 7, 10, 13cricothyroid membrane 11
puncture 12crura 22cubital v. 118cuneus fasciculus 44–5
cutaneous n.lower limb 89upper limb 88
deep peroneal n. 66, 69dermatomes
lower limb 89trunk 90upper limb 88
diaphragmcentral trefoil tendon 22, 28muscles 22nerve supply 23respiration movements 22–3
diencephalon 42dorsal root ganglion 51ductus arteriosus 38–9dura mater 47, 49, 51
Edinger–Westphal nucleus 75, 76elbow, antecubital fossa 118–19epidural space 47, 51epigastric vessels 22, 115epiglottis 8–9, 11ethmoid bone 4–5ethmoidal a. 126ethmoidal canal 79, 105–6eye and orbit 124–7
nerve supply 126orbital cone 127vascular supply 126
facial a. 32–3facial (geniculate) ganglion 80–1facial n. 74, 80–2facial v. 35, 120fasciculus cuneus and gracilis 44–5femoral a. 34–5femoral cutaneous n. 56femoral n. 62, 65femoral v. 37fetal circulation 38–9filum terminale 49foramen caecum, skull 105–6foramen lacerum, skull 105–6foramen magnum 104–5foramen ovale
heart 38–9skull 104–5
foramen rotundum, skull 104–5foramen spinosum, skull 105–6frenulum 2
frontal n. 78–9, 126–7
gastrocnemius m. 64, 68geniculate bodies 77geniculate ganglion 80–1genitofemoral n. 57glossopharyngeal n. 12, 74, 82, 83gluteal a. 59gluteal n. 56, 59gracilis fasciculus 44–5gracilis m. 64, 67great vessels 30–7
head arteries 30, 33head veins 34, 35heart 26–9
autonomic nerve supply 29blood supply 29cardiac notch 19chest radiograph 27fetal circulation 38–9great vessels 30–7vascular supply 28–9
Thebesian v. 21hepatic n. 84–5hilum 18, 20hyoepiglottic l. 9hyoglossus m. 7hyoid, pharynx 6–7hypogastric plexus 72hypoglossal canal 105hypoglossal n. 53, 84, 86
iliac a. 31, 32, 34–5iliac crests, and lumbar vertebrae 114iliac v. 36–7iliohypogastric n. 23, 57, 66ilioinguinal n. 57, 66, 116–17inferior vena cava 27, 36infraclavicular n. 54inguinal canal 116–17inguinal l. 57inguinal region 116–17interarytenoid m. 10intercostal a. 31, 112–13intercostal m. 22, 66, 69, 112–13intercostal n. 66–9, 112–13intercostal space 112–13
neurovascular bundles 112–13intercostal v. 112–13intercostobrachial n. 68, 113interosseous a. 32–3, 62–3, 119
intervertebral discs 100isthmus 2–3
jugular foramen 104–5jugular v.
anterior 15, 34–5, 120–1internal and external 15, 34–5, 120–1
lacrimal glands 81lacrimal n. 78–9, 126laryngeal n. 12–13, 84–5
injuries 10larynx 8–13
laryngoscopy view 11vascular supply 12
latissimus dorsi 23ligamenta flava 100ligamentum nuchae 100lingual n. 75, 79–80lingual v. 120liver, vagus n. 84–5longus colli m. 54lower limb
arteries 32, 34, 35cutaneous n. 89dermatomes 89nerves 57, 62–8veins 36–7
lumbar ganglia 72–3lumbar n. 66lumbar plexus 54, 57lumbar plexus block 56–8lumbar vertebrae 96, 97
and iliac crests 114lumbosacral trunk 57lungs 18–19, 20–21
bronchial supply 17cardiac notch 19fissures 19–20lobes 19–20lymphatic drainage 21nerve supply 21vagus n. 84–5vascular supply 21
lymphatic drainagebronchial tree 21pleura 21
mamillary body 43mandibular n. 75, 79, 80, 81mandibular v. 35masseteric n. 79–80140
Concise Anatomy for Anaesthesia
141
IndexIndex
maxillary a. 32–3maxillary n. 78–9median n. 55, 60, 62, 63, 119median v., upper limb 34mediastinum 18–19meningeal n. 50, 79, 84meninges 47–9, 51mental n. 79–80mesenteric a. 31middle ear, nerve supply 83mouth 2–3
nerve supply 2vascular supply 2
musculocutaneous n. 55, 60, 63, 66mylohyoid digastric n. 79
nasal glands 81nasal n. 79nasociliary n. 78–9, 126–7neck a. 30–3neck v. 15, 34, 35, 120–1nose/nasal cavity 4–5
nerve supply 4vascular supply 4
oblique m., orbit 125–6obturator n. 57, 62, 64occipital a. 32–3occipital lobe 43occipital n. 53occipitofrontalis m. 81oculomotor n. 74, 76, 77, 125–7oesophagus, vagus n. 84–5olfactory n. 76, 77ophthalmic a. 125–7ophthalmic n. 78–9ophthalmic v. 126–7optic canal 79, 105–6optic chiasma 76–7optic n. 76, 77, 125–7orbiculoris oculi m. 81orbit
cranial nerves 125–7rectus m. 125–6
orbital cone 127otic ganglion 75, 83
palate 2–3, 5nerve supply 2, 83vascular supply 2
palatine glands 81palatoglossal arch and folds 2–3
palatopharyngeal arch and folds 2–3palmar n. 63palpebral n. 79parasympathetic ns 72, 74, 75parotid n. 75, 79pectineus m. 62, 65pectoral n. 54–5perforating cutaneous n. 56, 59pericardium 28peripheral nerves 60–9
abdominal wall 66intercostal 66, 68–9lower limb 62–9upper limb 60–2
peroneal n. 64, 66, 69peroneal v. 37petrosal n. 81–3petrotympanic fissure 81–2petrous temporal bone 105pharyngeal v. 120pharynx 6–7
nerve supply 6, 83, 85vascular supply 6
phrenic n. 20, 22–3, 29, 52–3physiological shunt 21pia mater 47, 51pineal gland 43piriformis m. 59, 67pituitary gland 43plantar n. 64, 68plantaris m. 64, 68platysma m. 81pleura 18–19
lymphatic drainage 21nerve supply 21
plexuses 52–9brachial 52, 54, 55cervical 52, 53lumbar 54, 57sacrococcygeal 56, 59
popliteal a. 34–5, 68popliteal v. 36–7popliteus m. 64, 68pronator teres 119psoas major 62pterygoid n. 79pterygomandibular raphe 7pterygopalatine ganglion 75, 78, 81, 126pubic tubercle 117pudendal n. 56, 59pulmonary vascular supply 20, 21, 27Purkinje fibres 28
pyramidal decussation 44
questionsareas of special interest 128cardiovascular system 40nervous system 91respiratory system 24vertebrae 102
radial a. 32–3, 119radial n. 54–5, 60–2, 119radicular a. 46rami communicantes 51rectus abdominis 114–15rectus m., orbit 125–6recurrent laryngeal n. 10, 12, 13, 14, 84–5respiratory system 1–24retromandibular v. 35rib cage 19
axilla 123first rib 108–110, 111
saccule, nerve supply 83sacral ganglia 72–3sacral vertebrae 96, 99sacrococcygeal l. 49, 96sacrococcygeal plexus 54, 56, 59salivary nucleus 75saphenous n. 62, 65saphenous v. 36–7sartorius m. 62, 65scalenus m. 22–3, 54, 108–9sciatic n. 56, 59, 64, 67semicircular canals 83semimembranosus m. 64, 67semitendinosus m. 64, 67septum primum/secundum 38–9serratus anterior m. 110, 123sinoatrial node 26sinuses, nose/nasal cavity 4–5skull base 104–6
anterior cranial fossa 106middle cranial fossa 104, 106posterior cranial fossa 104
soleus m. 64, 68spermatic cord 116–17spinal a. 43, 46spinal accessory n. 53spinal cord 44–6
termination 44, 49vascular supply 46
spinal meninges and spaces 47–9, 51spinal cord termination 49
spinal nerves 50–1distribution 51dorsal and ventral rami 50–1roots 44spinal meninges 51
spinal plexuses 52–9spinocerebellar tract 45–6spinothalamic tract 45–6splanchnic n. 73splanchnic preganglionic n. 71stapedius m. 81stellate ganglion 72sternocleidomastoid n. 86sternohyoid m. 10sternopericardial l. 28stylohyoid m. 81stylomastoid foramen 81–2, 106stylopharyngeus m. 83subarachnoid space 47subclavian a. 13, 27, 108–9subclavian v. 35, 37, 108–9, 120–1subcostal n. 68subdural space 47submandibular ganglion 75, 81suboccipital n. 53subscapular n. 54subscapularis m. 123sulcus chiasmaticus 105superficial peroneal n. 66, 69superior orbital fissure 79superior vena cava 20, 27, 121supraclavicular n. 53, 54suprapleural membrane 110suprascapular n. 54–5swallowing 6sympathetic nerve supply 15, 70–2
sympathetic ganglia 51, 70, 72, 73sympathetic plexuses 72
telencephalon 42temperofacial n. 81temporal a. 32–3temporal n. 79, 81temporal v. 35Tenon’s capsule 126Thebesian v., heart 21thoracic ganglia 72–3thoracic inlet 108–11thoracic n., long 55thoracic sympathetic nerve supply 71142
Concise Anatomy for Anaesthesia
143
IndexIndex
thoracic v. 121thoracic vertebrae 96thoracodorsal n. 55thorax, v.s 36thyroarytenoid m. 10thyrocervical trunk 33thyrohyoid l. 9thyrohyoid m. 10, 13thyrohyoid membrane 8thyroid cartilage 8–9thyroid gland 11thyroid v. 120–1thyroidea ima 31tibial a. 34–5, 68tibial (deep peroneal) n. 64, 66, 68tibial v. 36, 37tongue
nerve supply 2, 83, 86vascular supply 2
tonsil 3nerve supply 83
trachea 14–15bifurcation 16cartilages 16nerve supply 14–15, 21vascular supply 14
tracheostomy 14trapezius n. 86trigeminal ganglion 78, 79trigeminal n. 78, 79trochlear n. 76–77, 125–7trunk, dermatomes 90
ulnar a. 32–3, 119ulnar n. 54, 55, 62, 65
umbilical a. 39umbilical n. 66umbilical v. 38upper limb
arteries 32, 33cutaneous n. 88dermatomes 88nerves 54, 60–3veins 34, 36, 37
utricle, nerve supply 83
vagus n. 13, 20, 74, 82–5vas deferens 116–17veins
abdomen 36head and neck 34, 35, 120–1lower limb 36–7thorax 36upper limb 34, 36, 37
venae cordis minimae 29vertebrae 94–102vertebral a. 32–3, 43, 94, 97vertebral l. 100vertebral v. 35vestibular cord 11vestibular n. 83vestibule, mouth 2–3vestibulocochlear n. 82, 83vestibulospinal tract 44–5vocal folds 9, 11, 85
xiphisternal n. 66xiphoid, diaphragm m. 22
zygomatic n. 78–9, 81